

Abstract
Rapid, convenient, and full access to personal electronic health records is a key part of empowering patients to manage their health and collaborate with healthcare, argue Maria Hägglund and colleagues
The need for digital health solutions to manage health and care became more apparent than ever during the covid-19 pandemic.1 Patient empowerment is essential in such a health crisis. Empowerment requires both access to information and the tools and competence to make informed decisions.
During the pandemic, digital provision of information and access to care was implemented and adopted at rates never seen before. Having online access to personal health records has proved an important tool for patient empowerment.2 3 4 To cope with social distancing measures, use of telemedicine soared and use of patient portals increased rapidly. In some health systems, platforms for telemedicine visits were offered only through logging into a portal, so patient access to online health records was spurred by video visits.1 Patients were also asked to report covid-19 symptoms through various mobile apps and to carry digital proof of vaccination and covid-19 test results.
In parallel with this increased use of digital health solutions, the importance of accessible and structured health data was also emphasized by policy makers internationally. In the United States, a federal rule from the 21st Century Cures Act mandated US healthcare providers to offer patients access to all the health information in their electronic medical records without charge.5 In Europe, the European Health Data Space was proposed in May 2022, with the aim to empower people to control and use their health data in their home country or in other member states and to offer “a consistent, trustworthy, and efficient framework to use health data for research, innovation, policy making, and regulatory activities, while ensuring full compliance with the European Union’s high data protection standards.”6 In South Korea, the MyHealthWay app was launched in February 2021,7 designed to give people control of their personal medical data with the plan to store all personal health records in a single app; by 2023 all medical records and health records, including data from personal “wearable” medical devices, are expected to be integrated and saved into the app.7
There has been progress in many, mainly high income, countries in providing patients with access to their clinical records, but even in these countries not everyone can access their health records online (box 1). We argue that there are good reasons to offer patients immediate and full access to their records to increase patient empowerment.
Box 1. Implementing access to patient records in three countries.
England
Adult patients in England can register for online services through a variety of providers.8 Although 46.6% of patients had registered for online services and were able to access at least one online service in March 2022, only 13% were able to see their detailed coded record. The coded record provides basic health information held in their GP record but does not include free text consultation entries or record attachments such as hospital letters.9 In March 2022 around 40% of patients were registered to book appointments online, and 46% were able to order repeat prescriptions online. Which parts of the primary care record are visible to patients is currently under the control of the GP surgery, although NHS England and NHS Improvement have announced plans to enable full prospective access by default to the primary care record in November this year. It is generally not possible for patients to access their secondary care hospital records online because progress away from paper based records has been slow.10
New Zealand
New Zealand has several different patient portals that provide electronic access to approximately 70% of primary care practices. Most people who sign up use them to make GP appointments or request repeat prescriptions, but, as in England, the degree of access to their health information through the portal is under the control of the individual general practice. There is generally no electronic access to hospital held healthcare information owing to the complexity and inconsistency of electronic records,11 although the Ministry of Health has released a strategy to develop nationally consistent electronic access to personal health information.
Sweden
A national patient portal provides Swedish patients with several online services. In contrast to England and New Zealand, the national portal includes appointment booking, prescription renewals, and full online access to electronic health records from both primary and secondary care, including free text notes and lab results. Record access was launched in one of Sweden’s 21 regions in 2012 and has since spread throughout the country. Over 1.85 million people use the online health record every month, with over six million logins a month.
Impact of covid-19 pandemic on patients accessing their records
The implementation of digital health solutions during the pandemic was rapid, and we can only hypothesize why adoption was so much quicker than previous attempts. Before the pandemic, individual patients were the most likely to benefit from having access to digital health solutions such as online records and telemedicine. During the pandemic, however, the urgent societal need ensured that resources were quickly allocated to digital health. Healthcare professionals also had more incentives to use digital solutions that allowed communication of test results and for them to see patients without requiring a physical meeting to reduce the spread of covid-19. Patients across the globe were asked to provide data on their health, symptoms, and vaccinations on a magnitude never seen before.
As people began to see the benefits of having access to their health data, new opportunities for patient empowerment through health data access emerged. In New Zealand, the population was encouraged to sign up to a national covid tracer app (with both QR codes and Bluetooth available for tracing contacts only after a positive covid-19 case is detected) and following that, to a “My Covid Record” digital health account.12 This account provides access to personal covid-19 vaccination records, a smartphone vaccine pass, covid-19 test results, and more recently the ability to upload self-testing covid-19 results. Approximately, 64% of the New Zealand population now has a digital health account.
In England, the percentage of people who were registered for and able to access at least one online service increased rapidly during 2021 when vaccination passes were introduced. But record access did not noticeably increase in the same way over the same period ( fig 1 ).
Fig 1.
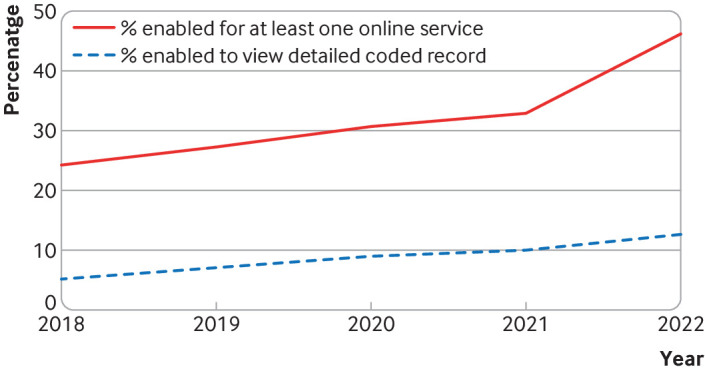
Increase in people registered for and able to access at least one online service in England.8
In Sweden, where all patients already had online access to their records before the pandemic, the increase in use was substantial (box 2). Having immediate online access to covid-19 test results was essential in empowering people to make informed decisions about their health and to take action to reduce the risk of spreading the virus.
Box 2. Impact of covid-19 pandemic on use of record access in Sweden.
In April 2022, 6.2 million citizens (of the total population of 10.2 million) had logged into their online health records at least once, compared with 3.4 million in January 2020. This suggests that patients’ motivation to access their health records online had increased, to access covid-19 test results for example, and that a greater proportion of the population were accessing their records than ever before.
Benefits of patients’ online access to their records
Patients who have access to their records report using them to become more involved in their care, to follow up on doctor visits, and for an overview of their healthcare visits, test results, and treatment history.2 Beyond the advantages of access during the pandemic, multiple surveys show that most patients who access their online records (including clinical notes) are positive about the experience, reporting many benefits, such as understanding their care plans better,3 greater trust in their provider,13 enhanced control in managing their health,2 3 14 including doing a better job taking their medications.15
In a US survey with responses from 21 664 patients, 96% of the respondents reported that they understood all or nearly all of their notes.16 Patients in a New Zealand study also emphasized that, despite the risk that they might not understand everything, patients should still be granted access out of respect and because the information is about them.11 In a Swedish study, 84% of patients agreed or strongly agreed that having access to their records online improved their communication with clinicians.2
It is not uncommon for patients to find errors in their records; 21.1% (n=4830) of note readers in a US study found a mistake in their notes.13 Although this might sound troubling, patients and their families have the potential to contribute to improved patient safety when given access to their full records.17 An analysis of 20 randomized clinical trials related to sharing clinical notes, involving 17 387 patients, concluded that sharing electronic health records could improve patient safety.18 This was also a conclusion reached by the US National Academy of Medicine in 2016, which recommended patients’ access to their records as a mechanism to improve diagnostic accuracy by closing feedback loops on care with more engaged patients.19
In addition to patients’ positive experiences and the potential to improve patient safety, a meta-analysis of 20 randomized controlled trials found a beneficial effect on haemoglobin A1c reduction for patients with type 2 diabetes.18 They also identified small studies showing improved effectiveness for outcomes such as blood pressure, anxiety, cardiac symptoms, and low density lipoprotein cholesterol.18
Risks of patients’ online access to their records
Despite generally positive experiences reported by patients, there are risks and unintended consequences of giving patients access to their records. In a small qualitative study in England, patients described finding unexpected information in the record that they had difficulty interpreting. GPs reported spending extra time on documentation to reduce potential misunderstandings and on administration of record access and sometimes excluding information to prevent worrying patients.20 In Norway, clinicians, especially in psychiatric care, reported keeping shadow records to prevent patients from accessing and potentially being harmed by the content of their records.21
Other concerns arise around the language used by clinicians. A large US based study in three centers found that 11% (n=2411) of patients who accessed their notes felt judged or offended by what they read, which included errors, surprises, forms of labeling, and disrespectful wording.22 Linguistic analyses of documentation in the US recently found that stigmatizing language was significantly more common in notes written about black patients than notes about white patients,23 24 and among patients with diagnoses of diabetes,24 substance abuse disorders, or chronic pain.
But, when reflecting on the potential risks of access, we should also be mindful of the alternative—keeping the record and notes inaccessible to patients. When patients are unable or not encouraged to read their health information, they might miss out on important opportunities to support understanding and interpretation of their diagnosis and treatment plan.25 Many patients report feeling anxious as they await test results, and instant access can reduce those concerns. Access to records might prevent results inadvertently being missed or not followed up by clinicians, particularly in transitions of care (from secondary to primary care, for example). As surveys show, patients who are more vulnerable to communication breakdowns in face-to-face visits might have the most to gain from access. In short, not offering patients access might also incur negative consequences for care that must be balanced against access.
Challenges in implementing patients’ online health record access
Despite the benefits reported by patients, implementation of online record access is often slow and challenging.26 27 In England, for example, the proportion of patients that can currently view their detailed coded record is low (13%).8 The percentage of patients with access to all the data in their primary care record is likely to be much lower, although this information is not in the public domain.
Clinician concerns
Barriers or resistance among clinicians often relate to concerns about malpractice,28 technical challenges, fears of contributing to workload, increases in patient confusion and anxiety, safeguarding risks, or changes to current work practices.29 Some concerns might be justified, especially with respect to rapid access to test results. A study in the US, for example, found that, after implementation of mandatory patient accessibility to their online health record, there was a doubling in the number of messages sent by patients within six hours of reviewing a test result.30 Moreover, healthcare professionals’ concerns are strikingly similar across different countries.21 31
Interoperability
Poor interoperability between electronic health record systems and other data sources remains a problem, causing fragmentation and frustration.32 A comparison between implementation in Sweden and the Netherlands found that clinician resistance and technical challenges were common barriers.27 Even when national regulations allow or mandate patient access, that might not be enough to guarantee patients easy access to their full health records.33 Poor usability, challenging registration processes, and accessibility requirements can also be barriers to adoption,4 which can, in turn, be used as an argument to not pursue further implementation as patients are not inclined to use the service.
Inequality
When offered, the extent to which patients access their records varies. Studies in Sweden2 and Norway14 have shown that older people, people with lower levels of education, and those with lower socioeconomic status are less likely to read their records online. Reduced rates of access might be due to lower digital or health literacy (or both) or lack of other resources such as broadband connection at home.
In a US study, patients with a lower socioeconomic status were less likely to read their records, but those who did, reported higher benefits than other users.3 Perhaps these patients are offered less information initially in person, have more difficulty processing the information, or ask fewer questions, making the written information in the record all the more important.34
In qualitative studies from Norway and England, patients who chose not to read their records reported that they found them impersonal, unnecessary, best left to healthcare professionals, and incomprehensible.4 35 A UK study among families with a teenager who was treated for cancer found a connection between coping strategy and use of a patient controlled electronic health record,36 indicating that patients or families with an avoidance coping strategy showed lower motivation to read their records. The choice to read will always be that of the individual patient. But for all patients to be able to make an informed decision and reap the potential benefits of reading their records, it’s essential to lower the barriers for accessing records and to ensure that all patients are informed and encouraged to read.
Conclusion
During the covid-19 pandemic, patients became more accustomed to remote and electronic methods of accessing care. Use of patient portals increased, including access to online health records. Yet, uptake remains low in some contexts—especially where barriers to access remain. These barriers are often related to prolonged and cumbersome processes to gain access or systems in which record access is not the default. Transitioning to record access by default might lead to an increase in workload for clinicians in the short term but is likely to reduce workload in the longer term and make access more uniform and useful for patients. Studies have found that limitations in information access are a common cause of frustration for users of patient portals.4 37
To overcome these barriers, resources are needed to implement record access and to facilitate the process of gaining access. The default should be enabling record access while implementing flexible functionality to ensure access can be delayed or blocked in high risk situations. In England, for example, records access will become the default in November 2022, and GPs will need to choose when to restrict access and be able to justify why access should be restricted.
Granting access to records for patients will require education interventions to support clinicians and encourage more confidence in sharing notes and in writing notes that patients will read, as well as greater guidance about the benefits and risks of note reading among patients. Patients need greater support for digital literacy, which is now considered a social determinant of health. Education of users will, however, never be enough unless we also improve the design of online solutions to access health records to make them useful for patients without overburdening healthcare professionals.
As health systems around the world digitize, developing systems that will enable patients to access their patient records will become an increasingly important way of empowering patients to make decisions about their health and care.
Key recommendations.
Decision makers globally are encouraged to ensure their populations have easy online access to their health records
-
Investments are required in several areas:
technical infrastructure, including interoperability of health data
support in legislation
education of both patients and healthcare professionals
well designed patient portals with high usability, including support for patients (eg, how to use the portal, explanations of content and functionality, glossary of medical terms)
We recommend learning from current implementations, in which default patient access increases patient adoption and use, but flexible solutions to delay or block access can be used in high risk situations.
Key messages.
During the covid-19 pandemic, patient adoption and use of online health services, including access to health records, greatly increased
Research from high income countries has shown that patients have positive and empowering experiences
Although record access has been shown to have positive effects on some clinical outcomes, further research is needed
Patients with lower education and socioeconomic status may benefit the most from having record access
Access is not without challenges, including clinician resistance, lack of digital literacy, and poor usability, that need to be tackled.
Acknowledgments
This work was partly supported by NordForsk through the funding to Nordic eHealth for Patients: Benchmarking and Developing for the Future (NORDeHEALTH), project number 100477, and by FORTE through the funding to Beyond Implementation of eHealth (2020- 01229). CB reports support from a Keane Scholar Award. BM is funded by the National Institute for Health and Care Research (NIHR Award ref: NIHR300887). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Contributors and sources: The guarantor of the article is MH, an expert in digital healthcare who has conducted long term research into patients’ access to their health records online within Sweden and internationally. BM is an NIHR advanced fellow at the Centre for Primary Care and Health Services Research, a practicing general practitioner, and a registered health psychologist. His research interests include the use of digital technology and psychological theory to improve patients’ experiences of primary care. RW is a public health physician and clinical director of innovation in the New Zealand health service. She is a long term researcher in digital health, and has conducted research with patients around their access to and use of their health information. CB is a philosopher of medicine and healthcare ethicist at Beth Israel Deaconess Medical Center, Harvard Medical School, who has led multiple surveys and ethical explorations of patient access to their clinical notes.
Patient involvement: We did not seek input from patients beyond the authors, however, MH uses the Swedish patient accessible electronic health record system to manage both her hypertension and other chronic conditions, and as a relative, in relation to her children. RW’s contribution is based on her work with patients at the Waitemata District Health Board including surveys, research projects, and consumer panels.
Competing interests: We have read and understood BMJ policy on declaration of interests and have the following interests to declare: The authors declare no conflicts of interest.
This article is part of a series commissioned by The BMJ for the World Innovation Summit for Health (WISH) 2022. Funding for the articles, including open access fees, was provided by WISH, which is an initiative of the Qatar Foundation. The BMJ peer reviewed, edited, and made the decisions to publish. The series, including open access fees, is funded by WISH. The steering committee members were Angela Coulter, Mark Barone, Michael Barry, Maria Hägglund, Karina Dahl Steffensen, and Mowafa Househ. Richard Hurley and Paul Simpson were the lead editors for The BMJ.
References
- 1. Blease C, Salmi L, Hägglund M, Wachenheim D, DesRoches C. Covid-19 and open notes: a new method to enhance patient safety and trust. JMIR Ment Health 2021;8:e29314. 10.2196/29314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Moll J, Rexhepi H, Cajander Å, et al. Patients’ experiences of accessing their electronic health records: national patient survey in Sweden. J Med Internet Res 2018;20:e278. 10.2196/jmir.9492 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Walker J, Leveille S, Bell S, et al. OpenNotes after 7 years: patient experiences with ongoing access to their clinicians’ outpatient visit notes. J Med Internet Res 2019;21:e13876. 10.2196/13876 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. McMillan B, Davidge G, Brown L, et al. A qualitative exploration of patients’ experiences, needs and expectations regarding online access to their primary care record. BMJ Open 2021;11:e044221. 10.1136/bmjopen-2020-044221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Salmi L, Blease C, Hägglund M, Walker J, DesRoches CM. US policy requires immediate release of records to patients. BMJ 2021;372:n426. 10.1136/bmj.n426 [DOI] [PubMed] [Google Scholar]
- 6.European Commission. A European Health Data Space for people and science. https://ec.europa.eu/commission/presscorner/detail/en/ip_22_2711
- 7.Jung J. South Korea’s My HealthWay: a “digital highway” of personal health records, but to where? The BMJ. 2021 https://blogs.bmj.com/bmj/2021/09/24/south-koreas-my-healthway-a-digital-highway-of-personal-health-records-but-to-where/
- 8.NHS Digital. Patient online management information (POMI). https://digital.nhs.uk/data-and-information/data-collections-and-data-sets/data-collections/pomi
- 9.NHS. Online health and prescription services. https://www.nhs.uk/nhs-services/gps/online-health-and-prescription-services/
- 10. Clarke A, Watt I, Sheard L, Wright J, Adamson J. Implementing electronic records in NHS secondary care organizations in England: policy and progress since 1998. Br Med Bull 2017;121:95-106. 10.1093/bmb/ldw055 [DOI] [PubMed] [Google Scholar]
- 11. Dobson R, Baty C, Best G, et al. Digital solutions for providing patients access to hospital-held health information: what are the design issues that need to be addressed? N Z Med J 2022;135:114-23. [PubMed] [Google Scholar]
- 12.New Zealand Ministry of Health. My covid record. https://mycovidrecord.health.nz/
- 13. Bell SK, Delbanco T, Elmore JG, et al. Frequency and types of patient-reported errors in electronic health record ambulatory care notes. JAMA Netw Open 2020;3:e205867. 10.1001/jamanetworkopen.2020.5867 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Zanaboni P, Kummervold PE, Sørensen T, Johansen MA. Patient use and experience with online access to electronic health records in Norway: results from an online survey. J Med Internet Res 2020;22:e16144. 10.2196/16144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Blease C, Dong Z, Torous J, Walker J, Hägglund M, DesRoches CM. Association of patients reading clinical notes with perception of medication adherence among persons with serious mental illness. JAMA Netw Open 2021;4:e212823-212823. 10.1001/jamanetworkopen.2021.2823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Leveille SG, Fitzgerald P, Harcourt K, et al. Patients evaluate visit notes written by their clinicians: a mixed methods investigation. J Gen Intern Med 2020;35:3510-6. 10.1007/s11606-020-06014-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Blease CR, Bell SK. Patients as diagnostic collaborators: sharing visit notes to promote accuracy and safety. Diagnosis (Berl) 2019;6:213-21. 10.1515/dx-2018-0106 [DOI] [PubMed] [Google Scholar]
- 18. Neves AL, Freise L, Laranjo L, Carter AW, Darzi A, Mayer E. Impact of providing patients access to electronic health records on quality and safety of care: a systematic review and meta-analysis. BMJ Qual Saf 2020;29:1019-32. 10.1136/bmjqs-2019-010581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.National Academies of Sciences, Engineering, and Medicine. Improving diagnosis in health care. 2015. https://www.nap.edu/catalog/21794/improving-diagnosis-in-health-care
- 20. Turner A, Morris R, McDonagh L, et al. Unintended consequences of patient online access to health records: a qualitative study in UK primary care. Br J Gen Pract 2022;72:e128-37. 10.3399/BJGP.2021.0426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kristiansen E, Johansen MA, Zanaboni P. Healthcare personnels’ experience with patients’ online access to electronic health records. Differences between professions, regions, and somatic and psychiatric healthcare. Linköping Electron Conf Proc 2019;161:93-8. [Google Scholar]
- 22. Fernández L, Fossa A, Dong Z, et al. Words matter: what do patients find judgmental or offensive in outpatient notes? J Gen Intern Med 2021;36:2571-8. 10.1007/s11606-020-06432-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Sun M, Oliwa T, Peek ME, Tung EL. Negative patient descriptors: documenting racial bias in the electronic health record. Health Aff (Millwood) 2022;41:203-11. 10.1377/hlthaff.2021.01423 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Himmelstein G, Bates D, Zhou L. Examination of stigmatizing language in the electronic health record. JAMA Netw Open 2022;5:e2144967. 10.1001/jamanetworkopen.2021.44967 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Blease C, Salmi L, Rexhepi H, Hägglund M, DesRoches CM. Patients, clinicians and open notes: information blocking as a case of epistemic injustice. J Med Ethics 2021;medethics-2021-107275. . 10.1136/medethics-2021-107275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Hägglund M, Scandurra I. Patients’ online access to electronic health records: current status and experiences from the implementation in Sweden. Stud Health Technol Inform 2017;245:723-7. [PubMed] [Google Scholar]
- 27. Cijvat CD, Cornet R, Hägglund M. Factors influencing development and implementation of patients’ access to electronic health records-a comparative study of Sweden and the Netherlands. Front Public Health 2021;9:621210. 10.3389/fpubh.2021.621210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Blease C, Cohen IG, Hoffman S. Sharing clinical notes: potential medical-legal benefits and risks. JAMA 2022;327:717-8. 10.1001/jama.2021.23179 [DOI] [PubMed] [Google Scholar]
- 29. de Lusignan S, Mold F, Sheikh A, et al. Patients’ online access to their electronic health records and linked online services: a systematic interpretative review. BMJ Open 2014;4:e006021. 10.1136/bmjopen-2014-006021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Steitz BD, Sulieman L, Wright A, Rosenbloom ST. Association of immediate release of test results to patients with implications for clinical workflow. JAMA Netw Open 2021;4:e2129553. 10.1001/jamanetworkopen.2021.29553 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Grünloh C, Cajander Å, Myreteg G. “The record is our work tool!”—physicians’ framing of a patient portal in Sweden. J Med Internet Res 2016;18:e167. 10.2196/jmir.5705 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Essén A, Scandurra I, Gerrits R, et al. Patient access to electronic health records: differences across ten countries. Health Policy Technol 2018;7:44-56 10.1016/j.hlpt.2017.11.003 [DOI] [Google Scholar]
- 33. Hägglund M, DesRoches C, Petersen C, Scandurra I. Patients’ access to health records. BMJ 2019;367:l5725. 10.1136/bmj.l5725 [DOI] [PubMed] [Google Scholar]
- 34. Blease C, Fernandez L, Bell SK, Delbanco T, DesRoches C. Empowering patients and reducing inequities: is there potential in sharing clinical notes? BMJ Qual Saf 2020;29:1-2. 10.1136/bmjqs-2019-010490 [DOI] [PubMed] [Google Scholar]
- 35. Valeur HS, Lie AK, Moen K. Patient rationales against the use of patient-accessible electronic health records: qualitative study. J Med Internet Res 2021;23:e24090. 10.2196/24090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Schneider H, Hill S, Blandford A. Patients know best: qualitative study on how families use patient-controlled personal health records. J Med Internet Res 2016;18:e43. 10.2196/jmir.4652 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Hägglund M, Scandurra I. Usability of the Swedish accessible electronic health record: qualitative survey study. JMIR Hum Factors 2022;9:e37192. 10.2196/37192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Turer RW, DesRoches CM, Salmi L, Helmer T, Rosenbloom ST. Patient perceptions of receiving covid-19 test results via an online patient portal: an open results survey. Appl Clin Inform 2021;12:954-9. 10.1055/s-0041-1736221 [DOI] [PMC free article] [PubMed] [Google Scholar]