

Abstract
Increased participation and duration in sport has become commonplace for women with their involvement often including the transition to motherhood in the peak of their athletic careers. No rehabilitation models that assess the full spectrum of pregnancy to postpartum have been developed for women to assist in safe exercise progressions that reduce postpartum symptoms and optimize performance during the return to full activity. Referral to physical therapy both in the prenatal and postnatal period is currently not considered standard of care to reduce prevalence of symptoms such as musculoskeletal pain, diastasis recti, and pelvic floor dysfunction which may ultimately interfere with physical activity and performance. This commentary presents a timeline and suggested progression for exercise participation to improve awareness of the musculoskeletal changes that occur after labor and delivery. The concepts covered may increase the understanding of how to manage pregnant and postpartum athletes from a musculoskeletal perspective and serve as a starting point for establishing appropriate and guided rehabilitation for safe return to sport after childbirth.
Keywords: pregnancy, postpartum, physical therapy, strength and conditioning, female athlete
INTRODUCTION
Musculoskeletal parameters in pregnancy and postpartum care have been an area of much debate and scrutiny, with continuous changes in these recommendations being inconsistent at best and conflicting at worst. The ability to stay active during and after pregnancy provides significant physiological benefits, regardless of prior training status.1–5 From a medical perspective, physical activity during pregnancy decreases risk of developing conditions such as gestational diabetes, pre-eclampsia, hypertension, depression, and both prenatal and postpartum incontinence.1 Physical activity also been shown to not increase the likelihood of adverse outcomes including low birth weight, miscarriage, or perinatal mortality.1 Despite the known benefits of physical activity in this population, there is little guidance on how to safely progress programming during pregnancy or how to return to sport performance postpartum.6,7 The six-week postpartum check is largely agreed upon as a point where medical clearance to return to normal activity occurs – however, it is becoming more clear that appropriate musculoskeletal interventions could safely begin in the immediate postpartum period. Discussions with the mother surrounding what types of exercise are safe to perform and what symptoms are normal/abnormal are not commonly included at this time, and musculoskeletal exams are rarely performed despite pregnancy and delivery being both medical and musculoskeletal events.8,9 Delaying guided rehabilitation until the six-week postpartum mark may compromise safe return to activity as many women work to navigate this phase independently. Currently, no peer-reviewed return to sport protocols for postpartum women exist despite the fact that 75% of postpartum runners return to running within eight weeks after delivery.10 Thus, women may be missing the benefit of guided rehabilitation and targeted exercise in a time frame where they can minimize postpartum symptoms and adequately prepare for return to sport.
Peak athletic performance has been shown to coincide with the predicted peak fertility years.1 As such, female athletes frequently sustain careers spanning these years, which often includes managing the physical transition from pregnancy to motherhood. Prevalent postpartum conditions including musculoskeletal pain, urinary incontinence, abdominal separation, and pelvic organ prolapse are factors that may limit physical performance and safe return to sport.11 Christopher et al. and de Mattos Lourenco et al. have found that more than one-third of postpartum runners experience pain upon their return as well as some form of urinary incontinence.10,12 While these symptoms may be present prior to or immediately upon return to activity, they may also demonstrate a delayed onset over time, as return to exercise may not consider the potential for dysfunctional pelvic floor and/or abdominal musculature. In addition, postpartum symptoms such as urinary incontinence or hip and knee pain appearing with return to activity may be dismissed as “normal”, potentially leading to continued deferral of treatment until the athlete is often several years postpartum. The lack of distinction between common versus normal symptoms in the first three months postpartum often delays appropriate management despite evidence that physical therapy can be beneficial in preventing and resolving these symptoms.13–15
Exercise guidance through the postpartum period is warranted for athletes to return to full activity safely and effectively. This clinical commentary proposes and outlines guidelines to encourage recreational and other elite athletes to engage in early physical activity in a progressive manner. Safe return to sport guidelines would allow women to address the facets of the musculoskeletal system that have been affected by pregnancy and return to sport and impact activity safely, using the first six weeks to their advantage.
Adaptations to pregnancy and postpartum
A wide variety of physiologic changes occur during pregnancy, which often can be managed with thorough musculoskeletal assessment and intervention. Weight gain, ligamentous laxity, postural changes, and center of gravity changes that occur during pregnancy all require different demands on strength, endurance, and postural control. The abdominal musculature is stretched to 115% of its resting length by 38 weeks of pregnancy.16 Cardiac output increases by 30-50%, (driven by increasing heart rate and stroke volume) by mid-pregnancy, along with a 10-20% increase in baseline oxygen consumption. Together, these cardiovascular alterations result in decreased available oxygen for aerobic activity.17,18 Pregnant athletes are often still anecdotally encouraged to stay below a target heart rate (formerly recommended as <140 bpm) and avoid lifting more than 25 pounds, conflicting with the more recent evidence that indicates these heart rate monitoring and absolute limits on weight lifting are no longer appropriate restrictions for low risk pregnancies.4,5
During labor and delivery, pelvic floor musculature is stretched to 250% of its resting length during delivery.9 Recovery of the pelvic floor muscles (levator ani and associated connective tissue) is thought to be maximized by four to six months postnatal, although unrestricted clearance to activity is typically obtained well before this point.9 Bladder neck mobility postpartum remains higher than when measured at 37 weeks gestation and can require increased musculoskeletal support to limit symptoms such as incontinence.19 With cesarean section delivery, uterine scar thickness is still increased at the six-week postnatal point indicating continued remodeling despite the fact that many women are told that they may begin unrestricted activity at this point, and notable pelvic floor dysfunction including weakness or difficulty with coordination may also still be present associated with the pressure of the growing uterus throughout pregnancy.20
“Core canister” health and dysfunction
Pregnant and postpartum women may have limited education on their own bodies and the musculoskeletal adaptations that occur. They may also not realize that many of the symptoms that they may experience in pregnancy and postpartum are common but not normal. In the United States, pelvic floor rehabilitation is not currently recommended for women as a standard of care requiring many to self-advocate for such treatment. Prevalence of pelvic floor dysfunction (urinary stress incontinence, urgency urinary incontinence, overactive bladder, pelvic organ prolapse, and fecal or anal incontinence) is high, with over one in four women experiencing at least one of these conditions.21 The presence of incontinence during pregnancy may be indicative of the presence of incontinence in postpartum. Those who have persistent incontinence at three months postpartum have a significantly greater likelihood of continued incontinence at the five-year postpartum mark compared to the general population.22 Postpartum urinary incontinence creates a barrier to exercise, and may limit athletes from completing their desired sport or exercise program.13 The total number of women including female athletes who will undergo surgery for correction of pelvic organ prolapse alone is expected to increase by ~48% over the next four decades.23 Despite many of the commonly experienced signs and symptoms of pelvic floor dysfunction being improved or prevented with rehabilitation, there is little discussion of a guided protocol to limit the likelihood of onset such dysfunction during pregnancy and postpartum.19,24–27
As would be expected, given the duration and intensity of change imparted upon the pelvic floor musculature, followed by the largely musculoskeletal event of labor and delivery, the pelvic floor muscles are typically dysfunctional postpartum with regard to strength, motor control, and endurance.9 For many women who were unaware of how to utilize pelvic floor muscles appropriately prior to delivery or for women who have had multiple babies without adequate rehabilitation and recovery, there may be significant dysfunction in attempts to self-train these muscles.2 Recommendations for musculoskeletal intervention postpartum vary from no activity until medical consult to full clearance to self-guided exercise at six weeks, suggesting discussions of varying types of delivery and tearing or injury may not be included when assessing return to activity/sport.25 When prescribed appropriately, performance of deep core exercises during pregnancy results in significantly fewer incontinence symptoms during late pregnancy and the postpartum period.8
Demands of returning to sport
Running is a specialized skill requiring very specific muscular endurance and strength demands. While it is common to use physical therapy to restore running mechanics in the post-operative and post-injury populations, the use of physical therapy in postpartum women looking to safely return to running is less commonly utilized. Optimizing postnatal recovery is a critical factor given the pregnant and postpartum musculoskeletal changes that occur as physical therapist’s accommodate these athletes and their desire to return to previous levels of activity.
There is considerable demand on the pelvic floor musculature during a task such as running. High impact activities are associated with a sudden rise in intra-abdominal pressure as well as ground reaction forces of 1.6-2.5x bodyweight.28,29 Given the structure and location of the pelvis as a force transmission site from the lower to the upper body, it is expected that the attaching musculature would be required to quickly contract and relax repeatedly throughout a task such as running. If the pelvic floor musculature is unable to contract and relax on demand in a supervised setting such as pelvic floor rehabilitation, it would be expected that the ability to perform that role during an often subconscious task such as running would be diminished and as such could result in potential activity-related dysfunction associated with that lack of ability including incontinence and prolapse.28
High impact exercise has been found to increase risk of pelvic floor dysfunction nearly five-fold as compared to low impact exercise, further warranting additional healing time prior to resuming high impact tasks.12 Just as physical therapists typically defer return to running in post-operative cases where notable anatomical healing must occur, perhaps physical therapists should also advocate for a return to running protocol that corresponds both to a time and criterion-based approach in the postpartum phase.25 A recommendation of this nature was initially made by Goom and colleagues,2 who advised that return to running be considered at or around the three months postpartum period. Based on the baseline demands of running as a power, endurance, and strength movement, the aim of the following recommendations is to restore asymptomatic tolerance for return to running. For most athletes, clearance for return to running readies them to participate in a more sport-specific training program as desired.
REHABILITATION TIMELINE RECOMMENDATIONS
In the absence of absolute or relative contraindications, pregnant women should be encouraged to participate in a regular, moderate intensity exercise program supported by the American College of Sports Medicine (ACSM) as well as the American College of Obstetricians and Gynecologists (ACOG) guidelines.5,30 General physicians have self-reported that they do not typically feel that they have adequate training in postpartum exercise prescription, and variations in regards to anecdotal recommendations are common.31 From a physical therapy perspective, Table 1 outlines a rehabilitation timeline with suggested goals and criterion for exercise participation to encourage a timely and safe full return to sport. As with any protocol, parameters may be adjusted to some extent depending on the individual, but these are best adjusted under the guidance of an appropriately trained professional.32 Such professionals should be well versed in the warning signs during exercise as well as contraindications to exercise when working with pregnant and postpartum clients.5,31
Table 1. Goals for Prenatal and Postnatal Performance.5,31,34.
| Stage | Goals | Example Criterion |
|---|---|---|
| First Trimester |
|
|
| Second Trimester |
|
|
| Third Trimester |
|
|
| Postpartum Weeks 0-2 |
|
|
| Postpartum Weeks 3-4 |
|
|
| Postpartum Weeks 5-6 |
|
|
| Postpartum Weeks 7-12 |
|
|
| Postpartum Weeks 13+ |
|
|
Each phase of the following protocol should ideally be monitored by a pelvic health physical therapist who can best make determinations on readiness to progress to the next phase and ensure that the pelvic floor muscles are contracting and relaxing correctly. Working with trained individuals in the area of pelvic health may also help to reduce fear avoidance behaviors and increase compliance during the pregnancy period.33 Understanding that high-impact tasks like running are necessary and appropriate for maximizing performance allows increased focus on safe movement with core and pelvic floor control, posture, and mobility.
Table 2. Musculoskeletal Protocol for Pregnancy through Return to Sport.7,31,34,36.
| Stage | Focus | Recommendations |
|---|---|---|
| First Trimester | Cardiovascular activity |
|
| Neuromuscular activity |
|
|
| Strength Training |
|
|
| Pelvic floor |
|
|
| Modifications for this phase |
|
|
| Second Trimester | Cardiovascular activity |
|
| Neuromuscular activity |
|
|
| Pelvic Floor |
|
|
| Strength Training |
|
|
| Modifications for this phase |
|
|
| Third Trimester | Cardiovascular activity |
|
| Neuromuscular activity |
|
|
| Strength Training |
|
|
| Pelvic Floor |
|
|
| Modifications for this phase |
|
|
| Postpartum Weeks 0-2 | Cardiovascular activity |
|
| Neuromuscular activity |
|
|
| Pelvic Floor |
|
|
| Postpartum Weeks 3-4 | Cardiovascular activity |
|
| Neuromuscular activity |
|
|
| Pelvic Floor |
|
|
| Postpartum Weeks 5-6 | Cardiovascular activity |
|
| Neuromuscular activity |
|
|
| Pelvic Floor/Strength |
|
|
| Postpartum Weeks 7-12 | Cardiovascular activity |
|
| Neuromuscular activity |
|
|
| Pelvic Floor |
|
|
| Strength |
|
|
| Impact-Specific Markers for Readiness for Progression |
|
|
| Functional Testing Options |
||
| Postpartum Weeks 13+ | Cardiovascular activity |
|
| Strength/Power |
|
First to third trimester
Initially, cardiovascular activity should be kept at a conversational pace, but is no longer limited to the 140 beats per minute metric.7 When a patient is self-assessing intensity, clinicians should discuss how to use the rate of perceived exertion (RPE) modified scale (0-10), aiming for between 1-4 for light to moderate.22 Occasional higher intensity cardiovascular tasks may be completed for short time periods, but time spent exceeding the RPE ranges of 5-7 should be limited due to the added pressure on the pelvic floor muscles as a fetus develops. Exercises may include running, stationary biking, low impact aerobics, step aerobics, swimming, or walking may be encouraged, which may vary day to day with specific symptoms of the mother.5,31 Contact sports, activities that increase likelihood of falls (horseback riding, cycling, downhill skiing, etc.), scuba diving, and/or hot yoga should be avoided.1,2,36 Incorporation of rest periods throughout cardiovascular effort (walking, stopping, stretching, etc.) should be considered to reflect the metabolic needs of the mother as pregnancy progresses.
Risk versus benefit analysis should be performed with continued impact work, as some athletes will be able to continue running and jumping during this phase but should closely monitor symptoms to determine whether this should be modified or eliminated. In similar fashion, running may be continued but duration can be reduced to limit the amount of stress on the pelvic floor and changes to gait with changing posture and growing fetus. Incline jogging/running and interval runs, for example, can be encouraged in bouts to reduce the volume of repetitive impact and assist with maintenance of running if desired. For athletes training for an upcoming race or needing to return quickly to an elite athlete level, continued safe impact work may be warranted and monitored closely. Other forms of cardiorespiratory activity that are lower impact and encourage more full body strength training and could potentially encourage a faster return to running and sport in the postnatal phase.
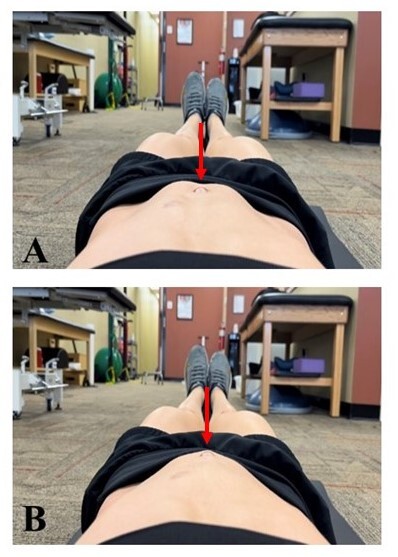
The importance of transversus abdominis control should be established, and challenging this control in a variety of positions including supine, sitting, and standing is important for function. Coordinating this movement with diaphragmatic breathing is also important as encouraging patients to perform this movement as they exhale can assist with control and pelvic floor coordination. Awareness and modifications around activities that cause coning would indicate limited tension management through the linea alba and as such should be modified until the patient is able to perform appropriately to help load the affected tissue safely. If the athlete is unable to modify this movement without the presence of continuous or repetitive coning, the movement may need to be eliminated to decrease severity of potential diastasis recti (Figure 1). As pregnancy progresses, repeated lumbar flexion movements should be limited and instead focus on stability movements of the core/spine such as anti-rotation, anti-extension, and anti-rotation drills with modifications as needed to avoid and manage abnormal tension at the linea alba. In the final months of pregnancy, breath work and coordination of pelvic floor relaxation should be focused upon, in order to increase the ability to relax the pelvic floor musculature during both deep inhalation and exhalation to prepare for delivery. Increased focus should be placed on postural endurance and mobility as the center of gravity shifts forward to include thoracic extensors, thoracic rotators, transversus abdominis, internal/external obliques, and hip flexors and extensors.
Figure 1. Normal (A) vs. abnormal/coning (B) management of tension at linea alba with leg lifting in early pregnancy.
Work that includes power movements of a barbell across the abdomen (i.e., snatches) should be modified as posture and bar path change. Movements such as this can be broken down into smaller multi- or single-joint exercises (deadlift, overhead press). Dumbbells may be substituted for bar exercises depending on the need and desires of the individual. Supine work may also be modified on an as needed basis dependent on symptoms such as pallor, increased heart rate, increased blood pressure, or generally feeling unwell. Such symptoms may indicate potential compression and can be quickly managed by moving the patient to at least a 30 degree reclined position.37 Positions that require stretching of the pelvic floor stretches such as deep squatting, child’s pose, and hip adductor stretching may be integrated to assist with muscular down-training techniques. Perineal massage techniques can be discussed around the 34-week mark for integration at home. Labor and delivery positions can be discussed in preparation for birth to include quadruped, deep squatting, or side-lying. Options should also be discussed for mothers who prefer to have epidurals as positioning may be more limited but may include side-lying with a peanut ball or rolling a towel around the tailbone/sacrum to allow opening at the pelvic outlet during the push phase.
Internal muscle exam is typically deferred in the first trimester due to the likelihood of miscarriage being highest in the first trimester. While an internal muscle exam is not correlated with any increase in this likelihood, potential association with miscarriage should be avoided if possible. It is also important to note that internal exam may not be necessary for assessment of the pelvic floor muscles as there are external techniques to determine pelvic floor muscle function, and that any addition of internal assessment does increase risk for potential infection. If desired by the athlete being treated by an individual trained in internal muscle examination, internal pelvic floor muscle exam may be completed in second or third trimester to assess baseline function of pelvic floor muscles and address associated deficits. It is important to ensure that this exam is performed in agreeance with the athlete’s medical team in addition to ensuring appropriate informed consent to the athlete.
Postpartum (weeks 0-6)
Immediately postpartum, minimizing excessive musculoskeletal stress is important as healing begins. Household ambulation is encouraged in small bouts as tolerated but should not be an area of great concern. General intensity should remain in the RPE 0-2 ranges to allow for appropriate healing. As comfort increases, a walking program may be initiated with focus on shorter duration performance (<10-15 minutes) and increasing frequency as tolerated. Symptoms should be monitored over the 24-48 hours after completion of these bouts of walking to determine musculoskeletal response prior to increasing frequency as some indicators of pelvic floor dysfunction such as prolapse may be delayed. Incline walking and/or gradually increasing speed (below jogging) and duration (<20-30 minutes) is acceptable so long as symptoms are not noted during or after performance. If symptoms present, these should be discussed with a qualified provider to determine whether they are a normal response to new loading of affected tissue or if they are an indicator of dysfunction.
In the early postpartum period, initial focus should be on reconnecting with diaphragmatic breathing to restore thoracic and lumbar mobility as well as to increase on-demand neuromuscular connection of the pelvic floor musculature. Initiation of gentle transversus abdominis work may begin with tasks such as pelvic tilts. Gentle lumbar and thoracic mobility such as lumbar rotation (Figure 2, A, B) and the side-lying “open book” exercise (Figure 2, C, D) within pain-free range may be performed to limit stiffness and encourage safe range of motion.
Figure 2. Range of motion exercises for lumbar mobility.
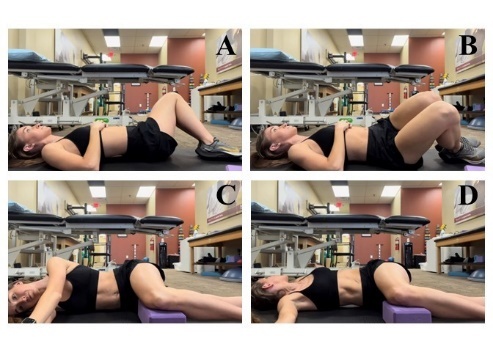
Lumbar rotation to the left (A) and right (B) with knees returning to center/neutral; side-lying “open book” exercise beginning (C) to end position (D) with knees supported at ninety-degree angle.
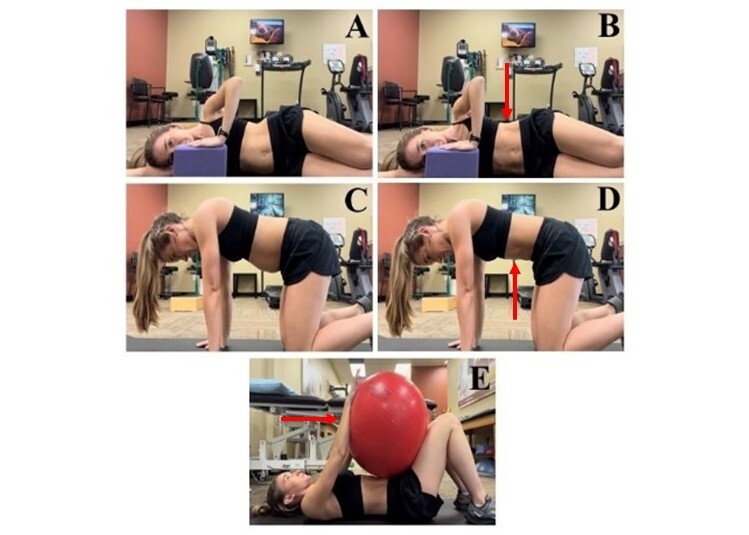
Light pelvic floor contract/relax movements may be initiated but deferred if symptomatic. As recovery progresses, independence in diaphragmatic breathing and anterior/posterior pelvic tilting should occur. Transversus abdominis stability drills may be initiated, preferably with less reliance on pelvic tilting. This should be coordinated with breath work to include supine, side-lying, and quadruped positions (Figure 3). Pelvic floor contractions and relaxations can be incorporated in this timeframe but may be deferred until internal muscle examination if pain occurs with performance.
Figure 3. Side-lying transverse abdominis isometric contraction (B) coordinated by pushing into block and drawing in ribs followed by relaxation (A) and exhalation. Quadruped transverse abdominis contraction (C) by drawing in of the umbilicus and relaxation (D). Hook-lying ball press (E) conducted by pushing arms into ball while exhaling.
Exercises focused on postural strength and endurance are important, as this is an area many new mothers have difficulty with due to nursing and holding the baby. Coordination of the transversus abdominis in functional positions such as sitting, standing, and high plank positions may also be initiated at this point if asymptomatic. Gentle open kinetic chain (OKC) movements may be integrated to increase hip strength and begin improving function associated with pregnancy postural changes. Appropriate pelvic floor contract/relax should be integrated into these movements to include light functional movements such as sit to stand or step ups.
Postpartum (weeks 7-12)
A walking program may continue, increasing speed and duration as tolerated. As there is a wide amount of variation in readiness for impact at this phase, adding short <20 second jogging bouts may be appropriate at the eight-week postnatal mark for athletes dependent on labor duration, degree of tearing, and other biopsychosocial factors to include sleep, hormone changes, and nursing status. It is recommended that if jogging is added during this phase, initial work:recovery intervals should be 1:2 ratio of time. This interval impact training should begin with no more than 20 minutes total duration, followed by monitoring, to ensure no symptom increase in the 48 hours after completion. If no symptom increase is present, duration may be slowly increased both in length of the activity interval as well as length of total duration of training. Impact “readiness” should be indicated by implementation of impact drills and response to initiation of a running program.
A sample return to running program can also be found in Table 3 with the initial suggested 1:2 work:rest ratio. These guidelines are focused on duration as opposed to distance with the understanding that pace will vary significantly dependent on the individual athlete as well as type of birth and associated tissue injury. It is important to note that this is only a sample program, and work, rest, and total time parameters may each be adjusted up or down to meet the individual needs of each athlete. Based on a combination of guidelines with varying recommendations of return to run timeframes, this particular protocol suggests that running should begin no sooner than eight weeks postpartum, only after the athlete is able to walk a minimum of 30 minutes without symptoms, in addition to being able to tolerate the six tasks in the Run Readiness Scale (step ups, wall sits, single leg squats, double leg squats, and a plank hold – each lasting one minute) without symptoms.25,36,38 When initiating the return to running program, each portion should be completed twice with 48 hours of rest between completions to ensure that no delayed symptom onset occurs. In the absence of an increase in symptoms 48 hours after the completion of the second trial of each week, the athlete should progress to the next phase until continuous running of desired distances is achieved. Increased symptoms during or after running should be discussed with a pelvic health physical therapist and progression to the next phase should be restricted to allow for a more individualized assessment regarding the source of those symptoms. It is also important to note that running with a stroller will result in postural changes and increased energy expenditure. If running with a stroller, the two-handed method proposed by Goom et al is most commonly suggested as this resulted in the speed and stride length closest to the baseline of each athlete.25
Table 3. Sample Return to Running Program.
| Week of Program | Work Phase (jog/run) |
Rest Phase
(walk) |
Maximum Total Time |
|---|---|---|---|
| 1 | 1 min | 2 min | 20 min |
| 2 | 1 min | 1 min | 20 min |
| 3 | 1 min | 2 min | 30 min |
| 4 | 1 min | 1 min | 30 min |
| 5 | 2 min | 2 min | 20 min |
| 6 | 2 min | 1 min | 20 min |
| 7 | 2 min | 2 min | 30 min |
| 8 | 2 min | 1 min | 30 min |
| 9 | 3-5 min | 2 min | 30 min |
| 10 | 3-5 min | 2 min | 45 min |
| 11 | 5-10 min | 2 min | 30 min |
| 12* | 10-15 min | 2 min | 45 min |
*Beyond week 12, desired factors (i.e. intensity, duration) may increase or decrease dependent on athlete goals. If the client desires to increase shorter duration speed work, this program may be more heavily focused on the earlier components with increasing intensity of the work phase.
Awareness and improvement of postural changes that have occurred during pregnancy and that often persist postpartum (limited thoracic rotation, improving degree of excessive anterior/posterior pelvic tilting) should all continue to be addressed as appropriate for each individual patient. An internal muscle exam should be performed if desired by patient to determine need for focused up-training vs. down-training at the pelvic floor once the individual is cleared for internal muscle examination by their OBGYN. Pelvic floor muscle focus should be on achieving full range of motion, quick flicks (strength), and endurance holds without compensations to encourage carryover into the functional tasks mentioned below.
Closed kinetic chain (CKC) strength tasks such as squatting, lunging, heel raises, or step ups to mimic movements that would be required in running or sport may also be integrated at this point. As tolerated, movement should progress from single-leg to double-leg to improve tolerance to this position. In addition, towards the end of this phase the speed of these movements may increase (i.e., quick step ups or quick sit to stand) to prepare musculature for more power-based movement. Approaching end of this phase may also include more horizontal impact work such as mountain climbers or plank hop outs in preparation for more upright impact work in the next phase. While this horizontal impact work may require less strength and coordination of the pelvic floor muscles, it does require increased control of the core and thus the incline may be modified to meet the needs of the athlete as both areas are heavily affected during the postnatal recovery period.
Cadence in running should range between 160-180 bpm to limit excessive force through the lower extremities as even a 10% increase in cadence has been shown to decrease mechanical stress at the knee joint.39 Running gait should also be individually assessed to limit likelihood of injury. Factors such as peak hip and knee adduction and knee stiffness may demonstrate more notable compensations in the postpartum phase with a comprehensive guide to 2D running analysis provided by Souza and colleagues.40
Postpartum (weeks 13+)
Mileage may be increased gradually, increasing speed in short bouts while incorporating walking, jogging and rest into the run as needed. As cardiovascular output increases, cross training (weightlifting, complimentary cardiorespiratory modalities) should also increase to have an athletically balanced approach to increasing intensity and duration. Symptoms should be monitored during and post training to make the necessary adjustments in training variables.
Impact work can be slowly graded from horizontal to upright as tolerated without symptoms. Initial attempts at running may be performed on slight incline to assist the pelvic floor musculature from a postural perspective and slowly decreased to 0% as tolerated. This slight incline limits excessive anterior pelvic tilt that many new mothers note postpartum to assist with muscular function at the pelvic floor. As new mothers can better control these habitual postures acquired during pregnancy, incline can be decreased to promote flat road running. Full clearance for return to running and sport should be assessed weekly as training volume slowly increases per ACSM guidelines (2-10%/week).
Additional Considerations
It is important to note that with this suggested timeline that there are common misconceptions surrounding regular pelvic floor contractions (Kegels) during pregnancy for pelvic floor strength. Many women are anecdotally instructed to focus on repeated pelvic floor contractions in order to strengthen the pelvic floor muscles for labor and delivery without being instructed on the need for relaxation of these muscles to encourage improved ease of delivery. Many athletes may suffer from the overactivity of their musculature both in pregnancy and postpartum, and symptoms can be made worse by performing repeated and regular muscle contractions at the pelvic floor when not indicated.41 The ability of a trained pelvic floor physical therapist to perform an internal muscle examination both during pregnancy and postpartum can ensure that the pelvic floor musculature is achieving appropriate range of motion and that contractions are being performed correctly. Any symptoms of pelvic floor dysfunction should serve as indicators for lack of readiness for progression to the next phase and may require additional visits to allow for safety in these progressions.
Other considerations as the athlete returns to running include timing of nursing with recommendations to empty the breasts just prior to running to limit discomfort and potential clogged ducts associated with full breasts. Athletes should be educated that exercise has not been shown to limit breastmilk production so long as appropriate hydration status and caloric intake is maintained.42 Sports bra fitting should provide appropriate support without being overly compressive and professional fitting of the bra is highly recommended, noting that previously worn breast support garments may no longer be adequate.43,44
While highly variable among individuals, foot size and shape can also change during pregnancy because of increased laxity of the ligaments in the feet. As such, a postnatal footwear assessment should be performed to ensure that running shoes are providing adequate support in addition to the intrinsic foot strengthening suggested within this protocol and others.38 While there are theories that the relaxin hormone responsible for this laxity may increase likelihood for injury, there are no studies that currently support this.45
CONCLUSION
Women in the pregnant and postpartum periods have lacked adequate guidance regarding appropriate exercise prescription. The proposed timeline of rehabilitation is proposed to facilitate improved quality of life, increased likelihood of full and safe return to sport, and less medical care requirements for postpartum symptoms. Understanding the intricacies of the female athlete during this time may assist clinicians and coaches with guidance to assist in safe return to sport. Without a slow and graded return to exercise which is commonplace for other musculoskeletal events, the current paradigm may unintendedly be overly conservative in some respects (during pregnancy) while not addressing dysfunction during the postpartum recovery.46,47
Despite evidence regarding the effectiveness of pelvic floor physical therapy,24,48,49 no specific rehabilitation guidelines currently exist to assist clinicians in determining appropriate frequency or progression of exercise for the pregnant and postpartum athlete. This commentary presents suggestions regarding graded activity during pregnancy and rehabilitation during post-partum recovery that may decrease the likelihood complications. The importance of this commentary lies not only in the outline of a preventative approach to postpartum care, but in the recommendation of continuous reassessment of the changing body throughout pregnancy and the early postpartum period as athletes perform and return to activities of daily living, work, exercise activity, and sport participation. As musculoskeletal health has been largely unstudied in this population, this protocol may provide guidelines for the prevention of common musculoskeletal dysfunction in the pregnant and postpartum athlete and spark future research.
COI Statement
The authors of this study report no conflicts of interest with regard to this manuscript or its contents.
References
- Mottola Michelle F, Davenport Margie H, Ruchat Stephanie-May, Davies Gregory A, Poitras Veronica J, Gray Casey E, Jaramillo Garcia Alejandra, Barrowman Nick, Adamo Kristi B, Duggan Mary, Barakat Ruben, Chilibeck Phil, Fleming Karen, Forte Milena, Korolnek Jillian, Nagpal Taniya, Slater Linda G, Stirling Deanna, Zehr Lori. British Journal of Sports Medicine. 21. Vol. 52. BMJ; 2019 Canadian guideline for physical activity throughout pregnancy; pp. 1339–1346. [DOI] [PubMed] [Google Scholar]
- Exercise and pregnancy in recreational and elite athletes: 2016 evidence summary from the IOC expert group meeting, Lausanne. Part 2—the effect of exercise on the fetus, labour and birth. Bø Kari, Artal Raul, Barakat Ruben, Brown Wendy, Dooley Michael, Evenson Kelly R, Haakstad Lene A H, Larsen Karin, Kayser Bengt, Kinnunen Tarja I, Mottola Michelle F, Nygaard Ingrid, van Poppel Mireille, Stuge Britt, Davies Gregory A L, IOC Medical Commission Oct 12;2016 British Journal of Sports Medicine. 50(21):1297–1305. doi: 10.1136/bjsports-2016-096810. doi: 10.1136/bjsports-2016-096810. [DOI] [PubMed] [Google Scholar]
- Clinical guidelines for occupational lifting in pregnancy: evidence summary and provisional recommendations. MacDonald Leslie A., Waters Thomas R., Napolitano Peter G., Goddard Donald E., Ryan Margaret A., Nielsen Peter, Hudock Stephen D. Aug;2013 American Journal of Obstetrics and Gynecology. 209(2):80–88. doi: 10.1016/j.ajog.2013.02.047. doi: 10.1016/j.ajog.2013.02.047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Summary of international guidelines for physical activity after pregnancy. Evenson Kelly R., Mottola Michelle F., Owe Katrine M., Rousham Emily K., Brown Wendy J. Jul;2014 Obstetrical & Gynecological Survey. 69(7):407–414. doi: 10.1097/ogx.0000000000000077. doi: 10.1097/ogx.0000000000000077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ACOG Committee opinion. Number 267, January 2002: exercise during pregnancy and the postpartum period. Practice A.C.O. 2002Obstet Gynecol. 99(1):171–173. doi: 10.1016/s0029-7844(01)01749-5. [DOI] [PubMed] [Google Scholar]
- Running during pregnancy and postpartum, part A: Why do women stop running during pregnancy and not return to running in the postpartum period? James Megan L., Moore Isabel S., Donnelly Gráinne M., Brockwell Emma, Perkins Joanna, Coltman Celeste E. Jan 18;2022 Journal of Women's Health Physical Therapy. 46(3):111–123. doi: 10.1097/jwh.0000000000000228. doi: 10.1097/jwh.0000000000000228. [DOI] [Google Scholar]
- Reframing return-to-sport postpartum: the 6 Rs framework. Donnelly Gráinne M, Moore Isabel S, Brockwell Emma, Rankin Alan, Cooke Rosalyn. 2022British Journal of Sports Medicine. 56(5):244–245. doi: 10.1136/bjsports-2021-104877. doi: 10.1136/bjsports-2021-104877. [DOI] [PubMed] [Google Scholar]
- Effect of pelvic muscle exercise on transient incontinence during pregnancy and after birth. Sampselle C M, Miller J M, Mims B L, Delancey J O, Ashton-Miller J A, Antonakos C L. Mar;1998 Obstetrics & Gynecology. 91(3):406–412. doi: 10.1016/s0029-7844(97)00672-8. doi: 10.1016/s0029-7844(97)00672-8. [DOI] [PubMed] [Google Scholar]
- How much does the levator hiatus have to stretch during childbirth? Svabík K, Shek KL, Dietz HP. Sep 1;2009 BJOG. 116(12):1657–1662. doi: 10.1111/j.1471-0528.2009.02321.x. doi: 10.1111/j.1471-0528.2009.02321.x. [DOI] [PubMed] [Google Scholar]
- What are the biopsychosocial risk factors associated with pain in postpartum runners? Development of a clinical decision tool. Christopher Shefali Mathur, Cook Chad E., Snodgrass Suzanne J. Aug 12;2021 PLoS One. 16(8):e0255383. doi: 10.1371/journal.pone.0255383. doi: 10.1371/journal.pone.0255383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blyholder Liga, Chumanov Elizabeth, Carr Kathleen, Heiderscheit Bryan. Sports Health: A Multidisciplinary Approach. 1. Vol. 9. SAGE Publications; Exercise behaviors and health conditions of runners after childbirth; pp. 45–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Urinary incontinence in female athletes: a systematic review. de Mattos Lourenco Thais Regina, Matsuoka Priscila Katsumi, Baracat Edmund Chada, Haddad Jorge Milhem. Mar 19;2018 International Urogynecology Journal. 29(12):1757–1763. doi: 10.1007/s00192-018-3629-z. doi: 10.1007/s00192-018-3629-z. [DOI] [PubMed] [Google Scholar]
- Is urinary incontinence a barrier to exercise in women? Nygaard Ingrid, Girts Tammy, Fultz Nancy H., Kinchen Kraig, Pohl Gerhardt, Sternfeld Barbara. Aug;2005 Obstetrics & Gynecology. 106(2):307–314. doi: 10.1097/01.aog.0000168455.39156.0f. doi: 10.1097/01.aog.0000168455.39156.0f. [DOI] [PubMed] [Google Scholar]
- Physical therapy is an important component of popartum care in the fourth trimester. Critchley Claire J C. Feb 25;2022 Phys Ther. 102(5) doi: 10.1093/ptj/pzac021. doi: 10.1093/ptj/pzac021. [DOI] [PubMed] [Google Scholar]
- Hip, knee, and foot pain during pregnancy and the postpartum period. Vullo V.J., Richardson J.K., Hurvitz E.A. 1996J Fam Pract. 43(1):63–68. [PubMed] [Google Scholar]
- Structure and function of the abdominal muscles in primigravid subjects during pregnancy and the immediate postbirth period. Gilleard Wendy L, Brown J Mark. Jul 1;1996 Physical Therapy. 76(7):750–762. doi: 10.1093/ptj/76.7.750. doi: 10.1093/ptj/76.7.750. [DOI] [PubMed] [Google Scholar]
- Maternal heart rate patterns under resting conditions in late pregnancy. Odendaal Hein, Groenewald Coen, Myers Michael M., Fifer William P. 2018Trends in Research. 1(3) doi: 10.15761/tr.1000116. doi: 10.15761/tr.1000116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aerobic exercise during pregnancy. Special considerations. Sady S.P., Carpenter M.W. 1989Sports Med. 7(6):357–375. doi: 10.2165/00007256-198907060-00002. [DOI] [PubMed] [Google Scholar]
- Postpartum recovery of levator hiatus and bladder neck mobility in relation to pregnancy. Stær-Jensen Jette, Siafarikas Franziska, Hilde Gunvor, Benth Jūratė Šaltytė, Bø Kari, Engh Marie Ellström. Mar;2015 Obstetrics & Gynecology. 125(3):531–539. doi: 10.1097/aog.0000000000000645. doi: 10.1097/aog.0000000000000645. [DOI] [PubMed] [Google Scholar]
- Ultrasound evaluation of the uterine scar after cesarean delivery: a randomized controlled trial of one- and two-layer closure. Ceci Oronzo, Scioscia Marco, Bettocchi Stefano, Cantatore Clementina, Nardelli Claudia, Laera Annafranca, Vimercati Antonella. Feb;2008 Obstetrics & Gynecology. 111(2 Pt 1):452; author reply 452. doi: 10.1097/aog.0b013e318163c90b. doi: 10.1097/aog.0b013e318163c90b. [DOI] [PubMed] [Google Scholar]
- The epidemiology of pelvic floor disorders and childbirth: An update. Hallock Jennifer L., Handa Victoria L. Mar;2016 Obstetrics and Gynecology Clinics of North America. 43(1):1–13. doi: 10.1016/j.ogc.2015.10.008. doi: 10.1016/j.ogc.2015.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The risk of stress incontinence 5 years after first delivery. Viktrup L., Lose G. Jul;2001 American Journal of Obstetrics and Gynecology. 185(1):82–87. doi: 10.1067/mob.2001.114501. doi: 10.1067/mob.2001.114501. [DOI] [PubMed] [Google Scholar]
- Predicting the number of women who will undergo incontinence and prolapse surgery, 2010 to 2050. Wu Jennifer M., Kawasaki Amie, Hundley Andrew F., Dieter Alexis A., Myers Evan R., Sung Vivian W. Sep;2011 American Journal of Obstetrics and Gynecology. 205(3):230 e231–235. doi: 10.1016/j.ajog.2011.03.046. doi: 10.1016/j.ajog.2011.03.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- A randomized controlled trial of pelvic floor muscle training for stages I and II pelvic organ prolapse. Hagen Suzanne, Stark Diane, Glazener Cathryn, Sinclair Lesley, Ramsay Ian. 2009International Urogynecology Journal. 20(1):45–51. doi: 10.1007/s00192-008-0726-4. doi: 10.1007/s00192-008-0726-4. [DOI] [PubMed] [Google Scholar]
- Donnelly G., Brockwell E., Goom T. Physiotherapy. Vol. 107. Elsevier BV; Return to running postnatal - guideline for medical, health and fitness professionals managing this population; pp. e188–e189. [DOI] [Google Scholar]
- The lower extremity functional scale (LEFS): Scale development, measurement properties, and clinical application. Binkley J.M., Stratford P.W., Lott S.A., Riddle D.L. 1999North American orthopaedic rehabilitation research network. Phys Ther. 79(4):371–383. [PubMed] [Google Scholar]
- Short forms to assess life quality and symptom distress for urinary incontinence in women: The incontinence impact questionnaire and the urogenital distress inventory. Uebersax John S., Wyman Jean F., Shumaker Sally A., McClish Donna K., Fantl J.A. 1995Neurourology and Urodynamics. 14(2):131–139. doi: 10.1002/nau.1930140206. doi: 10.1002/nau.1930140206. [DOI] [PubMed] [Google Scholar]
- Evaluation of pelvic floor muscle activity during running in continent and incontinent women: An exploratory study. Leitner Monika, Moser Helene, Eichelberger Patric, Kuhn Annette, Radlinger Lorenz. 2017Neurourology and Urodynamics. 36(6):1570–1576. doi: 10.1002/nau.23151. doi: 10.1002/nau.23151. [DOI] [PubMed] [Google Scholar]
- Ground reaction forces during downhill and uphill running. Gottschall Jinger S., Kram Rodger. Mar;2005 Journal of Biomechanics. 38(3):445–452. doi: 10.1016/j.jbiomech.2004.04.023. doi: 10.1016/j.jbiomech.2004.04.023. [DOI] [PubMed] [Google Scholar]
- American College of Sports Medicine L G. ACSM's guidelines for exercise testing and prescription. Wolters Kluwer; Philadelphia: [Google Scholar]
- Primary care physician perceptions of female pelvic floor disorders. Wong J.W., Kaneshiro B.E., Oyama I.A. 2019Hawaii J Med Public Health. 78(4):132–136. [PMC free article] [PubMed] [Google Scholar]
- Association A.P.T. Description of specialty practice: Women’s health physical therapy. Alexandria; [Google Scholar]
- The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Louw Adriaan, Zimney Kory, Puentedura Emilio J., Diener Ina. Jun 28;2016 Physiotherapy Theory and Practice. 32(5):332–355. doi: 10.1080/09593985.2016.1194646. doi: 10.1080/09593985.2016.1194646. [DOI] [PubMed] [Google Scholar]
- Guidelines of the American college of obstetricians and gynecologists for exercise during pregnancy and the postpartum period. Artal R, O'Toole M. Feb 1;2003 British Journal of Sports Medicine. 37(1):6–12; discussion 12. doi: 10.1136/bjsm.37.1.6. doi: 10.1136/bjsm.37.1.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Considerations for the Postpartum Runner. Mihevc Edwards Kate. Feb;2020 Strength Cond J. 42(1):45–52. doi: 10.1519/ssc.0000000000000453. doi: 10.1519/ssc.0000000000000453. [DOI] [Google Scholar]
- An examination of step frequency and the running readiness scale as predictors of running-related injury in collegiate cross-country athletes. Payne Shelley, D'Errico Jenna, Williams D. S. Blaise. Oct;2019 Journal of Sports Medicine and Allied Health Sciences: Official Journal of the Ohio Athletic Trainers' Association. 5(2) doi: 10.25035/jsmahs.05.02.04. doi: 10.25035/jsmahs.05.02.04. [DOI] [Google Scholar]
- Krywko D.M., King K.C. Aortocaval compression syndrome. StatPearls Publishing; Treasure Island (FL): [PubMed] [Google Scholar]
- Rehabilitation of the postpartum runner: a 4-phase approach. Christopher Shefali Mathur, Gallagher Sandra, Olson Amanda, Cichowski Sara, Deering Rita E. Feb 17;2022 Journal of Women's Health Physical Therapy. 46(2):73–86. doi: 10.1097/jwh.0000000000000230. doi: 10.1097/jwh.0000000000000230. [DOI] [Google Scholar]
- Effects of step rate manipulation on joint mechanics during running. Heiderscheit BRYAN C., Chumanov ELIZABETH S., Michalski MAX P., Wille CHRISTA M., Ryan MICHAEL B. Feb;2011 Med Sci Sports Exerc. 43(2):296–302. doi: 10.1249/mss.0b013e3181ebedf4. doi: 10.1249/mss.0b013e3181ebedf4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- An Evidence-Based Videotaped Running Biomechanics Analysis. Souza Richard B. Feb;2016 Physical Medicine and Rehabilitation Clinics of North America. 27(1):217–236. doi: 10.1016/j.pmr.2015.08.006. doi: 10.1016/j.pmr.2015.08.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Recognition and management of nonrelaxing pelvic floor dysfunction. Faubion Stephanie S., Shuster Lynne T., Bharucha Adil E. Feb;2012 Mayo Clinic Proceedings. 87(2):187–193. doi: 10.1016/j.mayocp.2011.09.004. doi: 10.1016/j.mayocp.2011.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Exercise and lactation: are they compatible? Carey Gale B., Quinn Timothy J. Feb 1;2001 Canadian Journal of Applied Physiology. 26(1):55–75. doi: 10.1139/h01-004. doi: 10.1139/h01-004. [DOI] [PubMed] [Google Scholar]
- Breast elevation and compression decrease exercise-induced breast discomfort. McGhee DEIRDRE E., Steele JULIE R. Jul;2010 Med Sci Sports Exer. 42(7):1333–1338. doi: 10.1249/mss.0b013e3181ca7fd8. doi: 10.1249/mss.0b013e3181ca7fd8. [DOI] [PubMed] [Google Scholar]
- Bra-breast forces generated in women with large breasts while standing and during treadmill running: Implications for sports bra design. McGhee Deirdre E., Steele Julie R., Zealey William J., Takacs George J. Jan;2013 Applied Ergonomics. 44(1):112–118. doi: 10.1016/j.apergo.2012.05.006. doi: 10.1016/j.apergo.2012.05.006. [DOI] [PubMed] [Google Scholar]
- Peripheral joint laxity increases in pregnancy but does not correlate with serum relaxin levels. Schauberger Charles W., Rooney Brenda L., Goldsmith Laura, Shenton David, Silva Paul D., Schaper Ana. Feb;1996 American Journal of Obstetrics and Gynecology. 174(2):667–671. doi: 10.1016/s0002-9378(96)70447-7. doi: 10.1016/s0002-9378(96)70447-7. [DOI] [PubMed] [Google Scholar]
- Principles of postoperative anterior cruciate ligament rehabilitation. Saka Tolga. 2014World Journal of Orthopedics. 5(4):450. doi: 10.5312/wjo.v5.i4.450. doi: 10.5312/wjo.v5.i4.450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baumgarten Keith M., Vidal Armando F., Wright Rick W. Sports Health: A Multidisciplinary Approach. 2. Vol. 1. SAGE Publications; Rotator Cuff Repair Rehabilitation: A Level I and II Systematic Review; pp. 125–130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Can pelvic floor muscle training improve sexual function in women with pelvic organ prolapse? A randomized controlled trial. Brækken Ingeborg H., Majida Memona, Ellström Engh Marie, Bø Kari. Feb;2015 The Journal of Sexual Medicine. 12(2):470–480. doi: 10.1111/jsm.12746. doi: 10.1111/jsm.12746. [DOI] [PubMed] [Google Scholar]
- Bø Kari. EAU Update Series. 3. Vol. 1. Elsevier BV; Is there still a place for physiotherapy in the treatment of female incontinence? pp. 145–153. [DOI] [Google Scholar]