

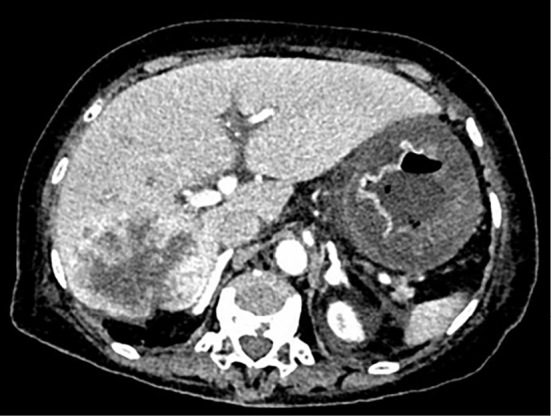
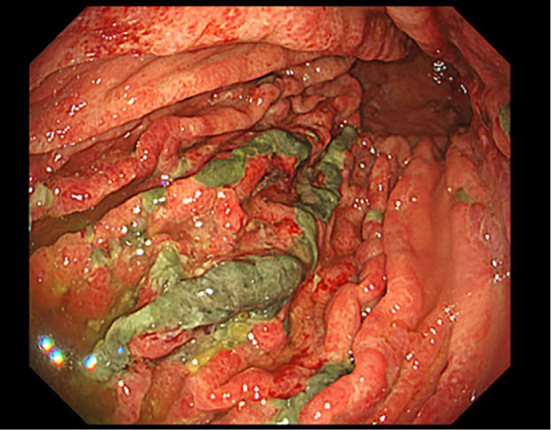
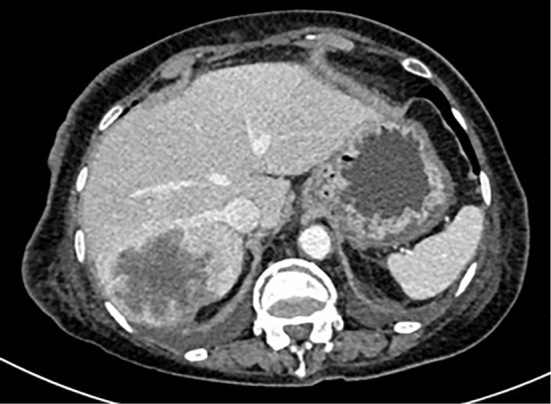
An 84-year-old woman was receiving chemotherapy for small-cell lung cancer with liver metastasis. She developed post-chemotherapy febrile neutropenia and then presented with systemic hypoperfusion due to septic shock and gastrointestinal bleeding. Contrast-enhanced computed tomography (CT) showed the absence of contrast enhancement of the mucosa at the greater curvature of the gastric body and diffuse thickening of the gastric wall (Picture 1). Esophagogastroduodenoscopy revealed multiple gastric erosions and pale inflamed mucosa in the greater curvature of the gastric body (Picture 2). We diagnosed her with gastric ischemia and continued treatment for septic shock, administering an intravenous proton pump inhibitor. Contrast-enhanced CT three days after the onset showed the recovery of the blood flow and improvement of the wall thickening in the stomach (Picture 3). Gastric ischemia is uncommon because of the rich collateral blood supply to the stomach (1,2). Endoscopy and CT play an important role in the diagnosis of gastric ischemia (3).
Picture 1.
Picture 2.
Picture 3.
The authors state that they have no Conflict of Interest (COI).
References
- 1.Tang SJ, Daram SR, Wu R, Bhaijee F. Pathogenesis, diagnosis, and management of gastric ischemia. Clin Gastroenterol Hepatol 12: 246-252, 2014. [DOI] [PubMed] [Google Scholar]
- 2.Herman J, Chavalitdhamrong D, Jensen DM, Cortina G, Manuyakorn A, Jutabha R. The significance of gastric and duodenal histological ischemia reported on endoscopic biopsy. Endoscopy 43: 365-368, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sharma A, Mukewar S, Chari ST, Wong Kee, Song LM. Clinical features and outcomes of gastric ischemia. Dig Dis Sci 62: 3550-3556, 2017. [DOI] [PubMed] [Google Scholar]