

Abstract
Potatoes are commonly consumed food item that contributes key nutrients to the diet including vitamin C, potassium, and dietary fiber. Despite their nutritional value, potato tuber may harm human health by virtue of their toxic glycoalkaloids (solanine). Acute solanine poisoning can happen from ingesting green or sprouted potatoes. The toxicity of Gas in humans causes mainly gastrointestinal disturbances such as vomiting, diarrhea, and abdominal pain. However, at higher doses, the toxicity of Gas in humans produces more severe symptoms, including fever, rapid pulse, low blood pressure, rapid respiration, and neurological disorders. Though potatoes are widely consumed, their toxicity is relatively rare. We came across a suspected case of poisoning by raw potato ingestion in an 11 years old Saudi boy who suffered cardiovascular complications, and was managed conservatively in pediatric ICU. The diagnosis was made based on history and clinical presentation. The patient recovered completely and was discharged with counseling.
Keywords: Glycoalkaloids, solanine, Saudi Arabia, toxicity
Introduction
Despite their economic and nutritional value, potato may harm human health by virtue of their toxic glycoalkaloids (GAs), Alpha solanine and Alpha-chaconine.[1,2] that exhibit strong lytic properties and inhibiting acetyl cholinesterase (AChE) and butyryl cholinesterase activities.[3] Acute solanine poisoning can happen from ingesting green or sprouted potatoes that have not been stored properly.[4] At lower doses, it causes gastrointestinal disturbances that mimics common microbial gastroenteritis, and may easily be missed by the general practitioner. At higher doses, it produces severe symptoms, including fever, tachypnea, low blood pressure, rapid respiration, and neurological disorders.[5] Fatal cases of solanine toxicity are rare.[6,7,8]
Case History
We report the case of an eleven years old Saudi boy, who initially presented to the emergency ward of the general hospital in one of the suburban towns of Southwest Saudi Arabia with a history of acute generalized, colicky abdominal pain and vomiting for a few hours duration. The vomitus was greenish in color and non-projectile. Mother of the boy reported that the boy had been asking her for food while she was busy elsewhere. In desperation he consumed some raw potatoes in her absence from the kitchen. There was no history of food consumed from outside and no contact with any sick patient.
Rest of the history was not significant.
On physical examination, blood pressure was100/70 mmHg, pulse 98 ppm, respiration rate 30 ppm, SpO2 96%, and temperature was 37.1°C. The boy was conscious; with no signs of respiratory distress, dehydration, jaundice. Head and neck examination was normal- no lymph node enlargement, throat congestion, and good oral hygiene. The abdominal exam was normal except for increased bowel sounds No other abnormality was detected on systemic examination.
The patient was admitted as a case of probable gastroenteritis. Routine investigations and blood culture was sent and patient was started on supportive treatment with intravenous fluids, hydration, and antiemetic. However, the patient did not show any improvement over the next couple of hours and his condition started to deteriorate. He developed cyanosis and bradycardia with a heart rate dropping to less than 60 beats per minute. His oxygen saturation dropped, and he was placed on oxygen through a non-rebreathing face mask at the rate of 10 liters per minute. The differential diagnosis was revised and the patient was admitted to PICU as a suspected case of solanine poisoning. He was kept nil orally. Continuous neuro-vital and cardiopulmonary monitoring was done. The patient was evaluated for cardiac, liver, and kidney function along with electrolytes, arterial blood gas, and acid-base study. Direct Bilirubin and blood glucose were slightly raised and creatinine and sodium levels were nominally lower than normal. All other parameters were found normal. ECG findings showed sinus bradycardia with normal QT interval, normal axis and normal PR interval [Figure 1: ECG findings]. The blood sample was sent for a toxic screen to the regional toxicology lab in Khamis Mushayt. No exposure to any of the common drugs was reported by the family. Nevertheless we tested for salicylate as it is a common, over the counter drug.[9] No test for glycoalkaloid was available in the lab and the toxicity screen was reported negative.
Figure 1.
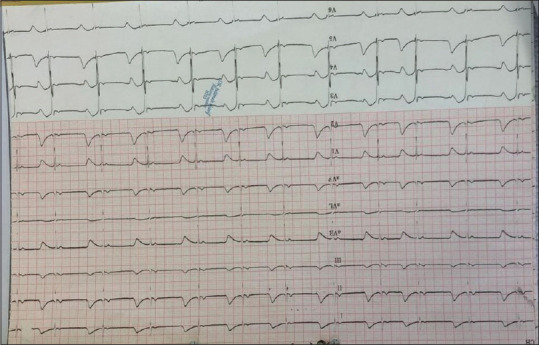
ECG showing bradycardia
The patient remained stable but continued with bradycardia and low oxygen saturation for two days before he started to develop fever on day 3 and a third-generation cephalosporin was added intravenously to his ongoing symptomatic treatment regime (Omeprazole, ondansetron, iv fluid). The patient started to improve from day 5 and a soft oral diet was started. All labs registered improvement. The patient was shifted to the male pediatric ward and kept under observation until day 8 when he was finally discharged.
Discussion
Epidemiology
Plants of the solanaceae family have been known to be toxic to humans since ancient times. In 399 BC, Socrates was sentenced to death by hemlock. A fatal case of solanine toxicity was reported in 1948, the causative agent was Solanum dulcamara (woody nightshade).[6] An outbreak of solanine poisoning linked to the ingestion of potatoes was reported in 1978.[7] wherein the case of 78 schoolboys became ill after eating potatoes that were leftover from the previous term at school. A Japanese research has reported a rising trend of toxicity associated with Solanum tuberosum.[8] Our case is an isolated incident of a young Saudi boy, previously healthy, presenting with characteristic signs of gastrointestinal poisoning. The suspicion of potato poisoning surfaced with his deterioration and development of cyanosis and cardiovascular symptoms. However, toxicity could not be confirmed due to lack of testing service for glycoalkaloids in the regional lab.
We compared our findings with those described in the UK study as our case belongs to the same age group and had a positive history of raw potato consumption.[7] Most of the findings reported in this study were replicated in our case, except for confusion.
Diagnosis
The diagnosis of solanine poisoning rests upon a high degree of suspicion and clinical acumen. Detailed food history revealed raw potato ingestion by the boy. To rule out any cardiac, gastrointestinal, and neurological causes, a complete and comprehensive investigation was done. A toxicity screen was run to exclude common toxicities in this region.[9]
Treatment
Symptomatic, supportive therapy. For managing the cyanosis and cardiovascular symptoms, oxygen therapy and watchful waiting were followed along with comprehensive evaluation.
Prognosis
Prognosis depends on the amount of toxin, age of patient, and time to treatment. Timely diagnosis, expulsion of stomach contents, and supportive treatment will lead to full recovery in 5 days to one week.[7]
Conclusions
This study provides valuable insight into how careful listening and consistent probing by primary care practitioners to identify the exact cause for a suspected case of gastroenteritis would save valuable time and resources. Considering that potatoes are a common food item across cultures, a high degree of suspicion for toxicity is warranted, especially in pediatric cases where smaller dose may cause harm to patient and cause undue burden on health services. Our case also emphasizes the need for drug and poison information centers and labs across Saudi Arabia to be strengthened.[10]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors are thankful to the parents for agreeing to publish this case with anonymity and providing a written consent for the same.
References
- 1.Beals K. Potatoes, nutrition and health. Am J Potato Res. 2018:96. [Google Scholar]
- 2.Schrenk D, Bignami M, Bodin L, Chipman JK, Del Mazo J, et al. EFSA Panel on Contaminants in the Food Chain (CONTAM) Risk assessment of glycoalkaloids in feed and food, in particular in potatoes and potato-derived products. EFSA J. 2020;18:e06222. doi: 10.2903/j.efsa.2020.6222. doi: 10.2903/j.efsa. 2020.6222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Krasowski MD, McGehee DS, Moss J. Natural inhibitors of cholinesterases:Implications for adverse drug reactions. Can J Anaesth. 1997;44:525–34. doi: 10.1007/BF03011943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rymuza K, Gugała M, Zarzecka K, Sikorska A, Findura P, Malaga-Toboła U, et al. The effect of light exposures on the content of harmful substances in edible potato tuber. Agriculture. 2020;10:139. doi: 10.3390/agriculture10050139. [Google Scholar]
- 5.Rayburn JR, Bantle JA, Friedman M. Role of carbohydrate side chains of potato glycoalkaloids in developmental toxicity. J Agric Food Chem. 1994;42:1511–5. [Google Scholar]
- 6.Alexander RF, Forbes GB, Hawkins ES. A fatal case of solanine poisoning. Br Med J. 1948;2:518. doi: 10.1136/bmj.2.4575.518. doi:10.1136/bmj. 2.4575.518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mcmillan M, Thompson JC. An outbreak of suspected solanine poisoning in schoolboys:Examination of criteria of solanine poisoning. Q J Med. 1979;48:227–43. [PubMed] [Google Scholar]
- 8.Toda M, Uneyama C, Kasuga F. Trends of plant toxin food poisonings during the past 50 years in Japan. Shokuhin Eiseigaku Zasshi. 2014;55:55–63. doi: 10.3358/shokueishi.55.55. [DOI] [PubMed] [Google Scholar]
- 9.Tobaiqy M, Asiri BA, Sholan AH, Alzahrani YA, Alkatheeri AA, Mahha AM, et al. Frequency and Management of Acute Poisoning Among Children Attending an Emergency Department in Saudi Arabia. Pharmacy. 2020;8:189. doi: 10.3390/pharmacy8040189. https://doi.org/10.3390/pharmacy8040189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Al Nasser K, AlQahtani Assessment of drug and poison information centers in Saudi Arabia. Toxicol Commun. 2019;3:43–6. [Google Scholar]