

Abstract
We report the country-level prevalence of awareness about electronic cigarette use, and ‘dual use’ and its association with age, sex, country income, and e-cigarette regulatory status. We analyzed the most recent Global Youth Tobacco Surveys done on nationally representative samples of school-going youth aged 13–15 years in 75 countries/territories. The weighted prevalence of ‘awareness’ (heard about e-cigarettes), ‘ever use’ (even tried a few puffs), ‘current use’ (during the last 30 days), and ‘dual use’ (e-cigarette use and cigarette smoking during the last 30 days) were estimated. Awareness was > 80% in 13 countries mostly from Europe Poland being the highest at 95.8% (95% CI 94.8- 96.6). In seven countries, 30–50% of the youth had ever used an e-cigarette, Italy was the highest at 55.1% (95%CI 51–3,58.9). In 30 countries, current e-cigarette use was > 10%, the highest of 35.1% (95%CI 32.4–38.0) in Guam. Awareness and use were highest in the European region (74.6% and 34.5%) and HIC (83.6% and 39.4%). Youth from HIC (compared to lMIC) and countries having restrictive e-cigarette regulations (compared to NRP) had 2.4 times (aOR 2.2.4, 95% CI 2.2, 2.7) and 1.8 times (aOR 1.8, 95% CI 1.6, 2.0) higher odds of being current e-cigarette users respectively. Youth in countries with the most restrictive e-cigarette regulations (compared to NRP) had 0.6 times lower odds of being current e-cigarette users (aOR 0.6, 95% CI 0.6, 0.7). Awareness and e-cigarette use varied by sex, country income level, and region. Continued global surveillance of youth e-cigarette use is needed for the formulation of e-cigarette regulatory policy. Awareness and use of e-cigarettes were higher among boys, in countries in Europe and America regions, and among those with higher income and restrictive policies, whereas it was lower in countries having the most restrictive policies. Higher awareness is strongly correlated with a trial and current use of e-cigarettes. E-cigarette marketing should be restricted, and continued surveillance of e-cigarette use is needed. Most restrictive policies such as the ban on e-cigarettes appear to reduce e-cigarette use among the youth.
Subject terms: Epidemiology, Medical research
Introduction
Tobacco use is a major risk factor contributing to the preventable disease burden1. Global efforts guided by the Framework Convention for Tobacco Control2 resulted in the decline of tobacco use among adults3,4. Lifelong nicotine addiction if initiated at a younger age5 (this part seems incomplete) makes it imperative to prevent the uptake of smoking among the youth as a key strategy to end the tobacco epidemic6. Analysis from the Global Youth Tobacco Survey (GYTS) has shown that tobacco use excluding electronic cigarettes (e-cigarettes) among school-going youth aged 13–15 years still remains substantial7. E-cigarette use also known as ‘vaping’ is increasing among the youth particularly in high-income countries (HIC)8. Increased use of e-cigarettes by youth has raised concerns about the “trying out” of e-cigarettes and then taking up cigarette smoking, often referred to as the ‘gateway to smoking9,10. E-cigarette use has led to plateauing or decline in youth cigarette smoking in some countries11,12. Nevertheless, recent reports of increasing rates of ‘dual use’ (both cigarette smoking and e-cigarettes) suggests a higher level of dependence13,14. Data on medium- and long-term effects of e-cigarette use are lacking but evidence about potentially harmful health effects is growing15,16. This warrants public health actions to prevent the impending epidemic of e-cigarette use17.
Epidemiologic surveillance of e-cigarette use among youth through regular, nationally representative, comparable household surveys helps monitor the changes in the prevalence and patterns of e-cigarette use and provide information to regulate e-cigarette use and evaluate strategies to control use, as appropriate18. Yet only about one third of all the countries have comprehensive tobacco use surveillance systems19. GYTS provides a feasible, cost-effective, global surveillance method for youth tobacco use through regular school-based surveys7. Questions about e-cigarette use introduced in 2014 provides important data for surveillance of e-cigarette use among youth worldwide18. A narrative review summarised the prevalence of awareness, ever use, past 30-days use, and regular use up to year 20148 while a systematic review of e-cigarette use among youth aged ≤ 20 years primarily comprising HIC, provides prevalence estimates of ‘ever’, ‘current’ and ‘occasional’ use20. A study based on 17 European GYTS sites provides estimates of current e-cigarette use only21. Sun et al. reported the prevalence of e-cigarette use in the past 30 days among youth in 68 GYTS countries, while Chan et al.; have also reported e-cigarette use in the past 30 days in 44 GYTS countries. In addition the current literature on e-cigarette use among youth is not comparable across countries because of heterogeneity of measurements and reporting of e-cigarette use8,22. To-date GYTS-based reports have not provided estimates of ‘awareness’, ‘ever use’ and have not analysed estimates by e-cigarette regulatory status. As tobacco companies expand their markets beyond HIC, data about e-cigarettes in low-and-middle-income countries (LMIC) are particularly lacking for surveillance purposes. To address this data gap, we report the most comprehensive, comparable country-level estimates to date of e-cigarette awareness, stand-alone e-cigarette use, and ‘dual use’ with conventional cigarettes among youth in 75 countries. We describe the distribution of pooled estimates of e-cigarette awareness, ‘ever e-cigarette use’, ‘current e-cigarette use’, and ‘dual use’ by age, sex, and contextual factors (e-cigarette regulatory policy status, WHO regions, and World Bank income group). We also explored if awareness correlated with ever and current e-cigarette use and if ‘current use’ of e-cigarettes was associated with age, sex, cigarette smoking, and contextual factors.
Methods
Design and data sources
We conducted a secondary analysis of the most recent data from 75 GYTS countries/territories that have collected data on e-cigarette use and asked at least one question. This study was conducted in accordance with the Declaration of Helsinki and followed all relevant guidelines and regulations. The detailed methodology of GYTS is available on the US Centers for Disease Control and Prevention (CDC) website. GYTS was reviewed by the National Ethical Committee and parental consent was obtained. GYTS, uses a two-stage cluster sampling method in which schools are selected by probability proportional to their enrolment size. Classes in each selected school are randomly selected until the required sample size was achieved. Students of all ages attending school on the day of the survey answered a standard self-administered core questionnaire with closed ended responses and a set of optional questions adapted by countries according to local needs and priorities. The questionnaires were translated and back translated into the local languages of each country to verify accuracy, and CDC validated and approved the questionnaires at the country level. The core questionnaire covers areas such as tobacco use, exposure to second-hand smoke, attempts to quit smoking, exposure to tobacco product advertising in the media, access to tobacco products, and knowledge, and attitudes towards tobacco use23. The number of questions on e-cigarettes in the optional module varied by country and survey year. Countries that included at least one question about ‘awareness’(69/75), ‘ever use’ (54/75) and ‘current use’(67/75) e-cigarettes were included in the analyses.
Outcome variables
Outcome variables based on questions asked in GYTS were defined as follows; 1) ‘Awareness about e-cigarettes’ was defined as having ever heard about e-cigarettes. 2) ‘Ever e-cigarette use’ was defined as youth who had ever tried or experimented with even one or two puffs or used e-cigarette on at least one day during their lifetime. 3) ‘Current e-cigarette use’ was defined as youth who had used e-cigarette on at least one day during the past 30 days prior to survey date. 4) ‘Current cigarette smoking’ was defined as smoking a cigarette on at least one day during the last 30 days prior to survey date. 6) ‘Dual use’ was defined as youth who had used e-cigarette as well as smoked cigarettes on at least one day over the previous 30 days prior to survey date.
Explanatory variables
We reviewed the data available on three web resources on regulations about e-cigarette (online supplement 1). E-cigarette regulatory policy status in each country was classified based on the information available from the websites of global tobacco control (https://www.globaltobaccocontrol.org/e-cigarette/domain-classification), global state of harm reduction (https://gsthr.org/countries) and the Tobacco Control Laws (https://www.tobaccocontrollaws.org/legislation). E-cigarette regulatory status for each country was grouped as 1) Most restrictive policies (MRP)- ban of e-cigarettes, 2) Restrictive policies (RP)- regulations on nicotine and/or other contents only, 3) Less restrictive policies (LRP)-allowed selling of e-cigarettes but provided sales restrictions/regulations, and 4) No regulatory policies (NRP)- no reliable information was available24. World Bank country classification (based on Gross national income) for the year of the survey was used to classify countries as 1) low, (LIC) 2) lower-middle, (lMIC) 3) upper-middle, (uMIC) and 4) high-income (HIC) using data available at https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed 30/1/2022). GATS countries/territories were grouped according to the WHO regions, namely Africa (AFR), Americas (AMR), Europe (AMR), Eastern Mediterranean (EMR), Western Pacific (WPR) and South-east Asia (SEAR).
Statistical analyses
Using microdata of each country, weighted prevalence estimates (%) and their 95% confidence intervals (95% CI) were estimated for awareness, ‘ever e-cigarette use’, ‘current e-cigarette use’, and ‘dual use’. The survey weights were adjusted for school, class, and student as per the multistage sampling process of GYTS. The microdata for all 75 countries were combined irrespective of the survey year. On the pooled data set, we calculated pooled estimates of each outcome by age, sex, WHO regions, World Bank income groups, and e-cigarette regulatory status. In the pooled data each survey participant (students) is nested within the school; each school is nested within the country. To account for this multi-level data binary logistic regression models with a random intercept at schools (first level) and country (second level) were used. To explore the factors associated with current e-cigarette use adjusted odds ratios (aOR), their 95% CI, random-effects parameters, and likelihood test ratios were estimated. Age, sex, current cigarette smoking, at the individual level (model 1); e-cigarette regulatory status, and World Bank income group as country-level (model 2) were entered into the models. We explored the relationship of awareness with ever use and current use of e-cigarettes using aggregate data (country-level estimates). We did two-way scatter plots and Spearman’s rank correlation test. Stata version 15/SE (Stata Corp, College Station, Texas, USA) was used for all statistical analyses.
Ethical approval
This study was based on analyses of publicly available de-identified GYTS data so a separate ethical approval was not required from the author’s institutions.
Results
Survey characteristics and sample description
A total of 264, 490 (male = 128,581, female = 135,909) youth surveyed in 75 countries during 2014–2019 was analyzed. Survey samples varied from 163 (Niue) to 9992 (Indonesia). Most GYTS countries were middle income countries (MIC) (uMIC-32, lMIC-22), 20 were HIC. In 23 countries there was no reliable information about e-cigarette regulatory policies (NRP). In 15 countries most restrictive policies (MRP) were in place, 28 countries had restrictive policies (RP), and nine countries had least restrictive policies (LRP). Prevalence of current cigarette smoking among youth was < 3% in six countries, the lowest being in Cambodia (0.9%, 95% CI 0.5, 1.7) and it was > 20% in six countries of which Bulgaria had the highest prevalence (22.8%, 95% CI 18.8, 27.3). Except for seven countries in AMR and EUR, the male-to-female (m-t-f ratio) of current cigarette smoking was > 1 (online supplement 1).
Country-wise estimates of awareness about and use of e-cigarettes and ‘dual use’
Country-wise prevalence estimates are shown in Table 1. Weighted prevalence of awareness about e-cigarettes in 69 countries varied from 9.4% (95%CI, 7.4, and 11.9) in Cambodia to 95.8% (95% CI 94.8, 96.6) in Poland and it was > 80% in 13 countries most of which were in Europe region (EUR). ‘Ever e-cigarette use’ in 54 countries ranged from 2.3% (95% CI 1.7, 3.1) in Cambodia to 55.1% (95% CI 51.3, 58.9) in Italy. In 7/54 countries, about third to half the youth had ever used e-cigarette. Prevalence of ‘current e-cigarette use’ (67 countries) was lowest in Togo 1.2% (95% CI 0.8, 1.9] and highest in Guam 35.1% [95% CI 32.4, 38.0]. In 30/67 countries, ‘current e-cigarette use’ was > 10%. Prevalence of ‘dual use’ (67 countries) ranged from 0.1% (95% CI 0.0,0.2) in Cambodia to 13.6% (95% CI 12.2, 15.2) in Poland followed by Italy 10.0% (95% CI 8.1,12.2). In 15/67 countries ‘dual use’ was > 5% (Table 2).
Table 1.
Country-wise overall estimates (%) and their 95% CI of awareness about e-cigarettes, ever and current use of e-cigarettes and dual use for the data available in 75 GYTS countries.
| Country | Awareness€ | Ever use£ | Current use¥ | Dual® | ||||
|---|---|---|---|---|---|---|---|---|
| High income | ||||||||
| Antigua & Barbuda | 49.6 | [45.9,53.3] | – | – | 5.1 | [4.1,6.3] | 1.0 | [0.6,1.5] |
| Bahrain | 60.3 | [55.7,64.7] | 19.9 | [15.8,24.8] | – | – | – | – |
| Cook Islands | 45.2 | [45.2,45.2] | 16 | [16.0,16.0] | 9.4 | [9.4,9.4] | 4.1 | [4.1,4.1] |
| Czech Republic | 95.3 | [94.4,96.1] | 26.2 | [23.3,29.3] | 11.1 | [9.4,13.1] | 7.3 | [6.0,8.9] |
| Guam | 82.6 | [80.5,84.4] | 48.2 | [44.6,51.8] | 35.1 | [32.4,38.0] | 7.7 | [6.4,9.2] |
| Italy | – | – | 55.1 | [51.3, 58.9] | 18.3 | [15.7,21.2] | 10 | [8.1,12.2] |
| Kuwait | 81.3 | [77.3,84.8] | 23.6 | [19.7,28.0] | – | – | – | – |
| Latvia | – | – | 52.4 | [49.0, 55.8] | 18.5 | [16.6,20.6] | 8.6 | [7.3,10.2] |
| Macao | 70.9 | [67.4,74.1] | – | – | 2.7 | [1.7,4.3] | 0.8 | [0.4,1.6] |
| Niue | 71.5 | [63.9,78.0] | 36.5 | [26.9,47.3] | 22.5 | [15.8,31.0] | 8.0 | [4.3,14.3] |
| Oman | 44.4 | [38.9,50.1] | – | – | 6.3 | [4.3,9.0] | 0.8 | [0.5,1.3] |
| Panama | 45.2 | [40.0,50.5] | 7.7 | [6.2,9.5] | 6.8 | [5.4,8.5] | 1.2 | [0.7,2.1] |
| Poland | 95.8 | [94.8,96.6] | 44.5 | [42.0,47.1] | 26.9 | [24.8,29.2] | 14 | [12.2,15.2] |
| Qatar | 60.9 | [56.9,64.7] | 17.2 | [14.0,20.9] | 10.8 | [8.6,13.5] | 2.1 | [1.3,3.2] |
| San Marino | 29.0 | [23.6,35.0] | 24 | [19.3,29.5] | 10.7 | [7.7,14.6] | 4.1 | [2.6,6.6] |
| Seychelles | 38.0 | [35.0,41.2] | 11.9 | [10.1,13.9] | 7.4 | [6.0,9.1] | 2.8 | [2.0,3.8] |
| Slovakia | – | – | – | – | 8.1 | [6.5,9.9] | 5.0 | [3.8,6.4] |
| Slovenia | 84.9 | [82.2,87.3] | 16.8 | [14.0,20.1] | – | – | 0 | – |
| Trinidad & Tobago | 71.9 | [69.3,74.4] | 26.9 | [24.1,29.9] | 15.7 | [13.9,17.8] | 3.7 | [2.7,4.9] |
| Uruguay | – | – | 25.3 | [20.6, 30.1] | 14.2 | [9.8,20.1] | 3.6 | [1.5,8.5] |
| Upper middle income | – | – | – | – | – | – | – | |
| Albania | 64.7 | [60.3,68.9] | – | – | 6.8 | [5.8,8.0] | 2.4 | [1.7,3.5] |
| Argentina | 76.1 | [68.2,82.5] | 15.7 | [11.3,21.3] | 8.2 | [5.7,11.7] | 4.1 | [3.0,5.5] |
| Belarus | 81.9 | [78.0,85.2] | – | – | – | – | 0 | – |
| Belize | 33.6 | [29.0,38.7] | 7.7 | [6.0,10.0] | 6.3 | [5.0,7.9] | 2.2 | [1.5,3.3] |
| Bosnia & Herzegovina | 90.5 | – | – | – | 12.1 | [10.6, 13.6] | 5.8 | [4.7, 6.9] |
| Bulgaria | 88.5 | [84.8,91.4] | 21.6 | [19.4,24.0] | 10.9 | [8.7,13.5] | 5.8 | [4.2,8.1] |
| Croatia | 91.1 | [89.1,92.9] | 22.1 | [17.8,27.2] | 10.8 | [8.6,13.6] | 6.0 | [4.2,8.3] |
| Cuba | 49.7 | [44.0,55.5] | – | – | 6.0 | [4.4,8.2] | 2.5 | [1.6,3.9] |
| Dominican Republic | 67.3 | [62.3,71.8] | 20.7 | [17.2,24.6] | 10.6 | [8.5,13.1] | 1.7 | [1.1,2.5] |
| Ecuador | 50.2 | [42.2,58.2] | 17.3 | [12.0,24.3] | 10.8 | [8.5,13.5] | 3.6 | [2.6,4.9] |
| Fiji | 33.9 | [31.1,36.9] | 12.5 | [9.4,16.3] | 12.6 | [9.9,15.9] | 3.2 | [2.3,4.5] |
| Grenada | 44.9 | [40.4,49.6] | – | – | 7.6 | [6.1,9.5] | 2.1 | [1.5,2.9] |
| Guyana | 22.7 | [19.8,25.9] | 8.0 | [5.8,10.8] | 8.3 | [5.8,11.7] | 2.3 | [1.5,3.5] |
| Indonesia | 71.3 | [68.3,74.1] | 22.9 | [20.8,25.1] | 14.4 | [13.0,15.9] | 8.5 | [7.5,9.6] |
| Iraq | 53.9 | [47.8,59.9] | 16.1 | [12.6,20.3] | 9.2 | [6.4,13.1] | 4.5 | [2.6,7.5] |
| Jamaica | 44.0 | [44.0,44.0] | 16.2 | [16.2,16.2] | 12.5 | [12.5,12.5] | 3.9 | [3.9,3.9] |
| Kazakhstan | 45.5 | [35.3,56.0] | 3.4 | [2.1,5.7] | 2.0 | [1.2,3.4] | 0.4 | [0.2,1.0] |
| Maldives | 58.9 | [55.9,61.8] | 18.8 | [16.5,21.3] | 0 | |||
| Marshall Islands | 28.1 | [26.0,30.4] | – | – | 18.7 | [16.7,21.0] | 7.9 | [6.8,9.3] |
| Mauritius | 54.2 | [47.2,61.0] | – | – | 11.3 | [8.5,15.0] | 5.7 | [4.0,8.0] |
| Macedonia | 68.7 | [66.0,71.2] | – | – | 4.1 | [3.3,5.2] | 1.7 | [1.2,2.3] |
| Montenegro | 81.6 | [79.0,83.9] | – | – | – | – | 0 | – |
| Paraguay | 77.4 | [66.3,85.6] | 23.3 | [18.2, 28.4] | 11.3 | [9.6,13.2] | 1.6 | [1.2,2.2] |
| Peru | 52.7 | [47.4,58.0] | 13.5 | [11.8, 15.1] | 6.9 | [5.7,8.3] | 2.3 | [1.8,3.0] |
| Romania | 19.6 | [17.6,21.7] | 14.3 | [12.8,15.8] | 7.6 | [6.5,8.9] | 2.9 | [2.4,3.6] |
| Saint Lucia | 47.5 | [42.4,52.7] | 15.7 | [13.4,18.3] | 10.7 | [8.5,13.3] | 2.9 | [2.1,4.1] |
| Saint Vincent | 39.2 | – | – | – | 7.5 | [6.0, 9.1] | 1.9 | [1.2,2.6] |
| Samoa | 27.6 | [23.8,31.7] | 12.2 | [9.9,15.0] | 12.7 | [10.5,15.3] | 4.1 | [3.1,5.4] |
| Serbia | – | – | 23.4 | [22.0, 24.7] | 7 | [7.0,7.0] | 3.4 | [3.4,3.4] |
| Srpska (Is this wrongly spelled?) | 86.6 | [84.4,88.5] | – | – | – | – | 0 | – |
| Suriname | 41.3 | [36.4,46.5] | – | – | 5.7 | [4.4,7.3] | 2.1 | [1.5,3.0] |
| Thailand | 38.6 | [32.5,45.0] | 5.4 | [3.9,7.5] | 3.4 | [2.5,4.7] | 1.8 | [1.4,2.5] |
| Lower middle income | ||||||||
| El Salvador | 31.5 | [27.6,35.7] | 8.0 | [6.1, 10.0] | 3.1 | [2.5,3.9] | 1.6 | [1.2,2.1] |
| Bolivia | 48.6 | [44.4,52.9] | 12.8 | [10.8,15.0] | 8.4 | [7.2,9.7] | 3.1 | [2.5,3.8] |
| Cambodia | 9.4 | [7.4,11.9] | 2.3 | [1.7,3.1] | 2.4 | [1.9,2.9] | 0.1 | [0.0,0.2] |
| Congo | 37.0 | [33.1,41.0] | 9.5 | [7.1,12.7] | 5.5 | [3.7,8.2] | 1.2 | [0.8,1.7] |
| Georgia | 78.9 | [73.4,83.5] | – | – | 12.4 | [9.6,15.9] | 3.3 | [2.3,4.8] |
| Ghana | 14.3 | [11.6,17.4] | 8.7 | [6.1,12.2] | 5.8 | [3.9,8.4] | 1.2 | [0.6,2.2] |
| Guatemala | 39.8 | [35.1,44.7] | 11.4 | [9.7,13.4] | 6.1 | [4.7,7.7] | 3.2 | [2.5,4.1] |
| Kiribati | 25.5 | [23.4,27.8] | 11.7 | [9.7, 13.6] | 11.2 | [9.5,13.3] | 4.9 | [3.7,6.4] |
| Kosovo | 37.0 | [33.6,40.5] | 7.6 | [6.7,8.5] | 4.5 | [3.8,5.5] | 1.1 | [0.8,1.6] |
| Kyrgyzstan | 41.0 | [36.4,45.7] | 5.3 | [4.1, 6.6] | 2.9 | [2.2,3.9] | 0.5 | [0.3,0.9] |
| Lao republic | 16.7 | [13.9,19.8] | 8.6 | [7.3, 10.1] | 4.9 | [3.7,6.3] | 1.4 | [1.0,1.9] |
| Mauritania | 33.5 | [29.7,37.5] | – | – | 18.7 | [13.8,24.8] | 6.7 | [4.1,10.6] |
| Republic of Moldova | 87.7 | [85.6,89.6] | 32.1 | [29.3,35.1] | 12.8 | [11.3,14.5] | 3.4 | [2.6,4.4] |
| Mongolia | 52.4 | [47.5,57.2] | 9.9 | [8.0,12.0] | 3.4 | [2.5,4.6] | 1.0 | [0.6,1.6] |
| Morocco | 44.1 | [38.1,50.2] | – | – | 5.4 | [4.0,7.3] | 0.8 | [0.5,1.3] |
| Nicaragua | – | – | 14.5 | [12.2, 16.9] | 8.6 | [7.7,9.6] | 3.1 | [2.7,3.7] |
| Papua New Guinea | 20.4 | [18.3,22.8] | – | – | 18 | [15.0,21.3] | 7.4 | [5.6,9.7] |
| Philippines | 43.3 | [39.1,47.6] | 12.1 | [10.0,14.5] | – | – | 0 | – |
| Tunisia | 54.6 | [50.5,58.7] | 6.4 | [5.3,7.6] | 4.8 | [3.9,6.0] | 1.7 | [1.1,2.5] |
| Ukraine | 93.2 | [91.1,94.8] | 36.3 | [32.8,40.0] | 17.4 | [14.8,20.4] | 3.7 | [2.6,5.3] |
| Vanuatu | 21.3 | [18.4,24.5] | 10.7 | [8.4,13.6] | 7.2 | [5.5,9.4] | 4.7 | [3.4,6.4] |
| Yemen | 29.5 | [23.7,36.1] | 14.4 | [12.1,17.1] | 13.9 | [11.8,16.4] | 2.3 | [1.5,3.5] |
| Low income | ||||||||
| Togo | 16.3 | [11.3,22.9] | – | – | 1.2 | [0.8,1.9] | 0.4 | [0.2,0.8] |
€ -69 countries, £- 54 countries, ¥- 67 countries, ®-67 countries.
Table 2.
Pooled estimates and their 95% CI of awareness about e-cigarette, ever and current e-cigarette use, and ‘dual use’ among the youth by their age, sex, and contextual factors (WHO regions, World Bank taxonomy, and regulatory policy status).
| Awareness | Ever use | Current use | Dual use | |||||
|---|---|---|---|---|---|---|---|---|
| P (%) | 95% CI | P (%) | 95% CI | P (%) | 95% CI | P (%) | 95% CI | |
| Total | 56.7 | [55.2,58.2] | 20.2 | [19.2,21.3] | 10.9 | [10.3,11.6] | 4.6 | [4.1,5.1] |
| Age | ||||||||
| ≤ 11 years* | 53.2 | [47.7,58.7] | 25 | [19.9,31.0] | 17.6 | [13.6,22.5] | 10.3 | [7.1,14.8] |
| 12 years | 49.9 | [46.9,53.0] | 16.1 | [13.9,18.6] | 8.7 | [7.2,10.5] | 3.0 | [2.2,4.0] |
| 13 years | 52.4 | [50.0,54.8] | 16.1 | [14.7,17.7] | 8.3 | [7.5,9.2] | 3.1 | [2.6,3.7] |
| 14 years | 57.0 | [55.0,58.9] | 19.9 | [18.4,21.6] | 10.8 | [9.9,11.8] | 4.4 | [3.8,5.2] |
| 15 years | 57.6 | [55.4,59.8] | 21.7 | [20.3,23.3] | 11.1 | [10.2,12.1] | 4.6 | [4.1,5.3] |
| 16 years | 63.3 | [60.6,65.9] | 24.9 | [23.2,26.8] | 14.2 | [12.7,15.7] | 6.6 | [5.7,7.5] |
| ≥ 17 years* | 63.8 | [60.3,67.1] | 24.8 | [22.8,27.0] | 14.6 | [12.9,16.4] | 7.3 | [5.8,9.2] |
| Sex | ||||||||
| Male | 61.5 | [59.9,63.1] | 28.5 | [26.8,30.3] | 16 | [14.8,17.3] | 7.6 | [6.7,8.7] |
| Female | 51.9 | [50.1,53.6] | 11.8 | [10.8,12.8] | 5.6 | [5.2,6.1] | 1.6 | [1.4,1.8] |
| WHO regions (number of countries) | ||||||||
| AFR (6) | 19.1 | [16.9,21.5] | 8.8 | [6.4,12.0] | 5.7 | [4.4,7.5] | 1.4 | [1.0,2.0] |
| AMR (21) | 58.1 | [55.4,60.8] | 18.7 | [16.6,21.0] | 8.2 | [7.4,9.1] | 2.8 | [2.5,3.1] |
| EMR (8) | 46.4 | [43.8,49.0] | 14.3 | [12.4,16.3] | 8.2 | [7.1,9.5] | 2.2 | [1.6,3.2] |
| SEAR (3) | 66.9 | [64.4,69.3] | 20.5 | [18.7,22.5] | 12.9 | [11.7,14.3] | 7.6 | [6.7,8.5] |
| WPR (14) | 38.2 | [34.7,41.8] | 15.3 | [13.5,17.2] | 4.4 | [3.9,4.9] | 0.2 | [0.2,0.3] |
| EUR (23) | 74.6 | [72.1,76.9] | 34.5 | [32.5,36.5] | 15.5 | [14.4,16.6] | 6.7 | [6.0,7.3] |
| World Bank taxonomy (number of countries) | ||||||||
| Low (1) | 16.3 | [11.3,22.9] | – | – | 1.2 | [0.8,1.9] | 0.4 | [0.2,0.8] |
| Lower Middle (12) | 40.6 | [38.6,42.7] | 16.5 | [15.3,17.8] | 7.6 | [6.9,8.3] | 1.3 | [1.1,1.5] |
| Upper Middle (32) | 64.0 | [62.1,65.9] | 19.4 | [18.0,20.9] | 11.2 | [10.3,12.2] | 5.8 | [5.1,6.5] |
| High (20) | 83.6 | [82.3,84.8] | 39.4 | [37.0,41.8] | 18.5 | [17.2,20.0] | 9.0 | [8.0,10.0] |
| E-cigarette regulatory policy status (number of countries) | ||||||||
| NRP (23) | 46.2 | [43.1,49.4] | 13.2 | [10.9,15.9] | 6.8 | [6.0,7.7] | 1.6 | [1.3,1.9] |
| LRP (9) | 48.5 | [44.7,52.4] | 19.9 | [17.6,22.5] | 15.4 | [13.4,17.5] | 3.1 | [2.3,4.0] |
| RP ((28) | 65.2 | [63.0,67.4] | 22.4 | [21.0,23.8] | 13.4 | [12.4,14.5] | 6.9 | [6.2,7.6] |
| MRP (15) | 47.5 | [42.1,53.0] | 17.2 | [14.9,19.8] | 5.6 | [4.6,6.7] | 2.4 | [1.9,2.9] |
All bivariate comparisons were statistically significant p < 0.001 by Chi-square statistic. *GYTS questionnaire did not collect exact age of those aged ≤ 11 years and ≥ 17 years.
Pooled prevalence estimates of awareness, e-cigarette use, and dual use and their distribution
Pooled prevalence estimate, overall and by age, sex, WHO regions, World Bank taxonomy, and e-cigarette regulatory policy status are shown in Table 2. Overall pooled estimates were 56.7% (95% CI 55.2, 58.2) for awareness of e-cigarette, the estimates for ‘ever use’, current use’, and ‘dual use’ were 20.2%, (95% CI 55.2, 58.2), 10.9% (95% CI 19.2, 21.3) and 4.6% (95% CI 4.1, 5.1) respectively. Youth from EUR (74.6%) and HIC (83.6%) had the highest e-cigarette awareness. Boys, higher age, and youth from countries with RP had a higher e-cigarette awareness. A similar pattern was observed for ‘ever’ use’, and ‘current use’ of e-cigarettes and ‘dual use’. Current e-cigarette use was also threefold higher (1.6% vs. 5.6%) while ‘dual use’ was fivefold higher (7.6% vs. 1.6%) among boys compared to girls, and prevalence also increased with age (Table 3). Notably, among those aged 11 years and less, ever (25.0%) and current (17.6%) e-cigarette use, and ‘dual use’ (10.3%) was higher than in the other ages. On bivariate comparisons, all the differences in pooled estimates were statistically significant (p < 0.001).
Table 3.
Socio-demographic and contextual factors associated with current e-cigarette use among youth by multi-level regression analyses.
| Univariate analyses | Multi-level model 1 | Multi-level model 2 | ||||
|---|---|---|---|---|---|---|
| Crude OR (95% CI) | Adj. OR (95% CI) | Adj. OR (95% CI) | ||||
| Age groups (in years) | ||||||
| 11–13 | 1 | < 0.001 | 1 | < 0.001 | 1 | < 0.001 |
| 14 | 1.3 (1.1, 1.4) | 1.2 (1.2, 1.3) | 1.2 (1.2, 1.3) | |||
| 15 | 1.3 (1.1, 1.5) | 1.3 (1.2, 1.34) | 1.3 (1.2, 1.3) | |||
| ≥ 16 | 1.7 (1.49, 2.0.) | 1.3 (1.3, 1.4) | 1.3 (1.2, 1.4) | |||
| Sex | ||||||
| Female | 1 | 1 | < 0.001 | 1 | < 0.001 | |
| Male | 3.2 (2.9, 3.6) | < 0.001 | 1.7 (1.6, 1.7) | 1.7 (1.6, 1.7) | ||
| Current cigarette smoker | ||||||
| No | 1 | 1 | < 0.001 | 1 | < 0.001 | |
| Yes | 12.4 (11.2, 13.7) | < 0.001 | 9.9 (9.6,10.4) | 9.9 (9.5, 10.3) | ||
| Contextual factors | ||||||
| E-cigarette regulatory policy status | ||||||
| NRP | 1 | 1 | ||||
| LRP | 2.5 (2.0, 3.1) | < 0.001 | 0.9 (0.8, 1.1) | 0.401 | ||
| RP | 2.2 (1.8, 2.5) | < 0.001 | 1.8 (1.6, 2.0) | < 0.001 | ||
| MRP | 0.8 (0.6, 1.0) | 0.069 | 0.6 (0.6, 0.7) | < 0.001 | ||
| World Bank taxonomy | ||||||
| lMIC | 1 | 1 | ||||
| uMIC | 1.6 (1.3, 1.8) | < 0.001 | 1.1 (1.0, 1.2) | 0.011 | ||
| HIC | 2.8 (2.4, 3.2) | < 0.001 | 2.4 (2.2, 2.7) | < 0.001 | ||
| Random-effects parameters | ||||||
| School level | SD | 0.00000003 | 0.00000002 | |||
| SE | 0.000664 | 0.0004885 | ||||
| Country level | SD | 0.8746556 | 0.6879336 | |||
| SE | 0.208748 | 0.0182421 | ||||
| Model comparison | ||||||
| Likelihood | Chi-square statistic | 4384.7 | 2552.8 | |||
| Ratio testa | P value | 0.0000 | 0.0000 | |||
aBased on the results on likelihood ratio tests, estimates of multilevel logistic regression were preferred than fixed effect models.
SD-standard deviation, SE-standard error.
*Ages 11–13 and ≥ 16 were merged owing to small numbers.
Sex-differentials
Sex-wise estimates in each country are shown in online supplement 2. Country-wise, in nearly all countries male-to-female (m-t-f) ratio for e-cigarette use was marginally above 1. However, both ‘ever e-cigarette use’, and ‘current e-cigarette use’ m-t-f ratio was > 1 in most countries the largest m-t-f ratio being 6.7 for ‘ever use’ (Indonesia) and 6.8 for ‘current use’ (Qatar). The m-t-f ratio for ‘dual use’ was diverse. It was < 1 in four countries (Ghana, Mauritania, Paraguay, and Slovenia), and among the countries with a magnitude of m-t-f ratio > 1 the highest ratio was in Morocco (31.0) and Qatar (28.2). Generally, the magnitude of the m-t-f ratio (> 1) for ‘current cigarette smoking’ (online supplement 1) was higher than that for ‘current e-cigarette use’. However, in 25 countries (mainly in 10 countries of EUR) m-t-f ratio for ‘current e-cigarette’ use was larger than that of current cigarette smoking. Notably, in some SEAR and EMR countries, the m-t-f ratio was > 1 but the magnitude of m-t-f ratio for e-cigarette use was smaller than that for cigarette smoking. In Uruguay, Antigua and Barbuda, and Argentina, the m-t-f ratio for e-cigarette were > 1 for e-cigarette and < 1 for cigarette smoking (online supplement 2).
Factors associated with e-cigarette use
Awareness about e-cigarettes was positively correlated with ‘ever use’ (r = 0.731, (95%CI 0.566 to 0.839, p < 0.001) (Fig. 1) as well as ‘current use’ (r = 0.333, 95% CI 0.089 to 0.540, p = 0.009) (Fig. 2). The correlations were consistent and statistically significant among boys (r = 0.717, 95% CI 0.546 to 0.831, p < 0.001 and r = 0.347 95% CI 0.097 to 0.555, p = 0.008) and girls (r = 0.549, 95% CI 0.319 to 0.718, p < 0.001 and r = 0.281 95% CI 0.027 to 0.501, p = 0.031). Higher age, being a boy, current cigarette smoking, higher country income and restrictive e-cigarette regulations had higher odds of being a ‘current e-cigarette user’. For instance, after adjusting for other factors, boys had about 1.7 times higher odds of being a current e-cigarette user (aOR 1.7 95%CI 1.6, 1.7), and youth who currently smoked cigarettes had 10 times higher odds of being current e-cigarette users (aOR 9.9, 95% CI 9.5, 10.3). Youth from a HIC compared to lMIC and a country having restrictive e-cigarette regulations compared to NRP had 2.4 times (aOR 2.4, 95% CI 2.2, 2.7) and 1.8 times (aOR 1.8, 95% CI 1.6, 2.0) higher odds of being current e-cigarette users respectively (Table 3) respectively. Youth in countries with most restrictive e-cigarette regulations compared to NRP had 0.6 times lower odds of being current e-cigarette users (aOR 0.6, 95% CI 0.6, 0.7).
Figure 1.
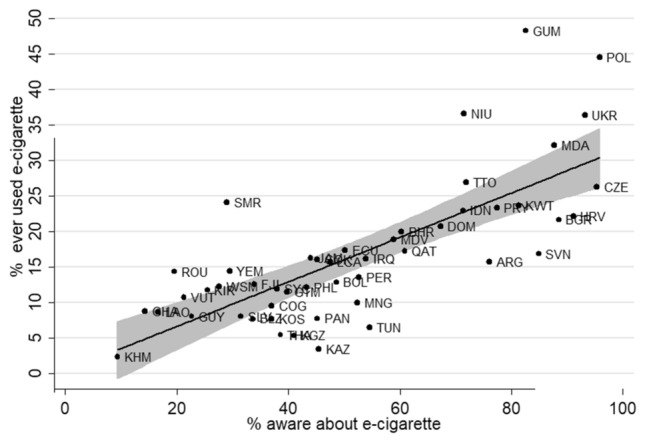
Two-way scatter plots between the prevalence of awareness and ever e-cigarette use (both sexes) in 49 countries. Cambodia- KHM, Ghana-GHA, Lao republic-LAO, Romania-ROU, Vanuatu-VUT, Guyana-GUY, Kiribati-KIR, Samoa-WSM, San Marino-SMR, Yemen-YEM, El Salvador-SLV, Belize-BLZ, Fiji-FJI, Kosovo-KOS, Congo-COG,Seychelles-SYC,Thailand-THA,Guatemala-GTM,Kyrgystan-KGZ,Philippines-PHL,Jamaica-JAM,Panama-PAN,Cook islands-COK, Kazakhstan-KAZ, Saint Lucia-LCA,Bolivia-BOL,Ecuador-ECU,Mongolia-MNG,Peru-PER,Iraq-IRQ, Tunisia-TUN, Maldives-MDV, Bahrain-BHR, Qatar-QAT, Dominican Republic-DOM, Indonesia-IDN, Niue-NIU, Trinidad and Tobago-TTO, Argentina-ARG, Paraguay-PRY, Kuwait-KWT, Guam-GUM, Slovenia-SVN, Republic of Moldova-MDA, Bulgaria-BGR, Croatia-HRV, Ukraine-UKR, Czech republic-CZE, Poland-POL. (Spacing after the comma should be consistently applied).
Figure 2.
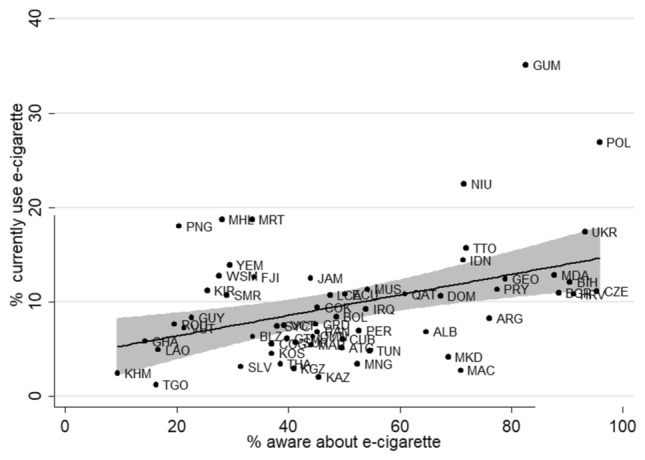
Two-way scatter plots between the prevalence of awareness and current EC use (both sexes) in 61countries. Congo-COG, Ghana-GHA, Mauritania-MRT, Mauritius-MUS, Seychelles-SYC, Togo-TGO, Antigua and Barbuda-ATG, Argentina-ARG, Belize-BLZ, Bolivia-BOL, Cuba-CUB, Dominican republic-DOM, Ecuador-ECU, El Salvador-SLV, Grenada-GRD, Guatemala-GTM, Guyana-GUY, Jamaica-JAM, Panama-PAN, Paraguay-PRY, Peru-PER, Saint Lucia-LCA, Suriname-SUR, Trinidad and Tobago-TTO, Yemen-YEM, Iraq-IRQ,Morocco-MAR,Oman-OMN,Qatar-QAT,Tunisia-TUN,Thailand-THA,Indonesia-IDN,Vanuatu-VUT,Cambodia-KHM, Cook islands-COK, Fiji-FJI, Guam-GUM, Kiribati-KIR, Lao republic-LAO, Macao-MAC, Marshall islands-MHL, Mongolia-MNG, Niue-NIU, Papua new guinea-PNG, Samoa-WSM, Ukraine-UKR, Albania-ALB, Bulgaria-BGR, Croatia-HRV, Czech republic-CZE, Georgia-GEO, Kazakhstan-KAZ, Kosovo-KOS, Kyrgyzstan-KGZ, Macedonia-MKD, Poland-POL, Moldova, Republic of-MDA, Romania-ROU, San Marino-SMR, Bosnia-BIH, Saint Vincent and The Grenadines-VCT. (Spacing after the comma should be consistently applied).
Discussion
Amid growing concern about increasing e-cigarette use among the youth particularly in HIC, and a relative scarcity of data for LMIC, our report provides the most up-to-date reliable estimates using comparable GYTS data. Our analyses of GYTS microdata showed that nearly half of the youth are aware of e-cigarettes and one third of them have used e-cigarette in their lifetime. Stand-alone e-cigarettes use and ‘dual use’ were several times higher among boys than girls. E-cigarette use was high among the youth in European countries and HIC. In some countries, up to half of the youth had used an e-cigarette in their lifetime and one third to one quarter of them were current e-cigarette users. In countries with a higher prevalence of e-cigarette use ‘dual use’ was common.
Strengths and limitations of this study
A standardized survey methodology, questionnaire and acceptable response rates in GYTS provide comparable estimates25. Compared with the current literature8,18,20,21, we provide estimates for more uMIC and lMIC in which regulatory policies are weak or absent26. Our study is the first to report on the distribution of e-cigarette use among the youth by age, sex, country income groups, and e-cigarette regulatory status to inform public health policy and assess the impact of existing regulations27. Existing reports on estimates of e-cigarette use only report about ever, current, and occasional e-cigarette use20,21. However this report provides estimates of e-cigarette awareness and ‘dual use’. Several limitations should be considered while interpreting our results. Self-reported behaviors are subject to reporting bias particularly in middle-income countries. Regardless, current use on one or more days in the 30 days before the survey date is known to reduce information bias and is a reliable indicator of current use28. Our pooled estimates do not represent global prevalence or prevalence estimates for World Bank income groups and WHO regions. The number of countries in which GYTS included optional questions on e-cigarette use was smaller than the number of countries covered by GYTS. The question on e-cigarette use did not distinguish between electronic nicotine delivery systems (ENDS) and electronic non-nicotine delivery systems (ENNDS)23. Therefore, we were unable to provide estimates for these two types i.e. ENDS and ENNDS29. Our estimates for 2014 to 2019, are not very up-to-date because e-cigarette use patterns among youth are evolving rapidly due to aggressive marketing strategies by tobacco companies.
Interpretation and comparison with related studies
Our findings are consistent with published reports that e-cigarette use varies across countries8,17,21, based on the different indicators used to define e-cigarette use22. The cross national difference in e-cigarette use are due to the different regulatory frameworks for e-cigarettes26,30. The very high prevalence of awareness is consistent with studies from HIC in which exposure to e-cigarettes through online media31,32. or witnessing of e-cigarette use by youth among peers, family, or in public is common. A significant correlation between estimates of awareness and ever use of e-cigarette use supports the argument that increased awareness through aggressive advertising and marketing has led to experimentation with e-cigarette (to try them out) and subsequent regular use33. Higher rates of e-cigarette use in HIC may be attributed to higher disposable income among youth compared to their peers in uMIC or lMIC34. Higher pocket money among the youth led to higher odds of them being e-cigarette use in a European study21. Tobacco company strategies such as advertising attractive flavors, sleek models, and online sales have increased e-cigarette use in HIC21,35 however such data are lacking for uMIC and lMIC. The distribution of pooled estimates by WHO region is consistent with existing reports from the EUR and AMR8,20,21,36.
Higher e-cigarette use rates among boys than girls, is comparable to sex difference reported about cigarette smoking37. The ratio of boys to girls for cigarette smoking > 1 is consistent with the existing literature7,37. In most countries the difference between boys and girls is greater for e-cigarette use compared to cigarette smoking. In some EMR countries and SEA, where female smoking is culturally unacceptable38. The difference was narrow i.e. m-t-f for e-cigarette indicates that e-cigarette use among girls may be higher. The higher rates of e-cigarette use among 11–13 years old suggests that the age at initiation for e-cigarette use was lower5 as in Europe and America21,39. The results suggest that experimentation with e-cigarette occur at a very young age, which warrants stricter policies regarding the minimum age for e-cigarette purchase39,40. Evidence from a few countries suggests that ‘dual use’ of cigarette smoking and e-cigarette use among the youth is on the rise13,14. There is growing evidence that e-cigarette use at younger ages leads to subsequent initiation of cigarette smoking9,41 and a lifelong nicotine dependence42. Exposing youth to nicotine at a young age is a ploy by tobacco companies to entice them to smoke cigarettes33. However, in the absence of detailed information we cannot preclude if the youth had initiated cigarette smoking or e-cigarette or switched between these during the previous 30 days. Adult smokers have been reported to use e-cigarettes for cigarette smoking cessation43. E-cigarette questions included in GYTS did not inquire about the purpose of e-cigarette use as youth are unlikely to be using e-cigarettes to quit smoking44.
Implications of the results on policy and future research
Understanding the distribution of e-cigarette use across these socio-demographic groups is useful for policy-making on e-cigarette regulations27. Our results provide deeper insights into the age and sex distribution of e-cigarette use among youth to assist formulation of age-gender-specific e-cigarette regulatory policies37. However, we were unable to examine the distribution of e-cigarette use by youth’s income status because GYTS does not gather such data consistently across countries. However, the results of previous studies indicate that higher income is a determinant of e-cigarette use among youth and adults21,45. Our report showed that e-cigarette use is substantial among the youth in uMIC countries not just in HIC. Our findings call for continued monitoring at HIC and expansion of monitoring to additional uMIC and lMIC countries for surveillance using standardized survey methods and indicators of e-cigarette use46. GYTS results presented in this report could serve as a benchmark for future surveillance. Although surveys typically collect data on types of e-cigarette (ENDS/ENNDS), flavors and designs, surveillance should cover basic indicators of e-cigarette use behaviors covering recommended indicators46.
Conclusion
Prevalence of e-cigarette use among the youth varied by income groups and WHO regions in World bank countries. E-cigarette was highest in HIC and those in EUR and AMR regions. To better understand the determinants of e-cigarette use and formulate future e-cigarette regulatory policies, an expanded and standardized surveillance system is needed. E-cigarettes need to be regulated in the MIC to prevent escalation of its use as in HIC.
Supplementary Information
Author contributions
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. Sreeramareddy CT conceptualised and designed the analyses and Acharya K performed the statistical analyses, Anusha M prepared the results, tables and graphs and interpreted the results, Sreeramareddy CT wrote first draft of the manuscript. All authors contributed to the review and editing of the manuscript, approved the final draft of the manuscript for submission and agree to be accountable for all aspects of the work.
Data availability
The datasets used and/or analysed during the current study available on the website of Centre for Disease Control, Atlanta, USA. The data sets and Stata code used for analyses are available from the corresponding author on reasonable request.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
The online version contains supplementary material available at 10.1038/s41598-022-25594-4.
References
- 1.Reitsma MB, Kendrick PJ, Ababneh E, Abbafati C, Abbasi-Kangevari M, Abdoli A, Gorini G. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. The Lancet. 2021;397(10292):2337–2360. doi: 10.1016/S0140-6736(21)01169-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.World Health Organization. WHO framework convention on tobacco control. World Health Organization (2003).
- 3.Ngo A, Cheng KW, Chaloupka FJ, et al. The effect of MPOWER scores on cigarette smoking prevalence and consumption. Prev. Med. 2017;105:S10–S14. doi: 10.1016/j.ypmed.2017.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.World Health Organization. WHO report on the global tobacco epidemic, 2017: monitoring tobacco use and prevention policies. World Health Organization (2017).
- 5.Reitsma MB, Flor LS, Mullany EC, Gupta V, Hay SI, Gakidou E. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and initiation among young people in 204 countries and territories, 1990–2019. The Lancet Public Health. 2021;6(7):e472–e481. doi: 10.1016/S2468-2667(21)00102-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.McDaniel PA, Smith EA, Malone RE. The tobacco endgame: A qualitative review and synthesis. Tob. Control. 2016;25(5):594–604. doi: 10.1136/tobaccocontrol-2015-052356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ma C, Xi B, Li Z, et al. Prevalence and trends in tobacco use among adolescents aged 13–15 years in 143 countries, 1999–2018: findings from the Global Youth Tobacco Surveys. The Lancet Child & Adolesc. Health. 2021;5(4):245–255. doi: 10.1016/S2352-4642(20)30390-4. [DOI] [PubMed] [Google Scholar]
- 8.Greenhill R, Dawkins L, Notley C, Turner JJ. Adolescent awareness and use of electronic cigarettes: A review of emerging trends and findings. J. Adolesc. Health. 2016;59(6):612–619. doi: 10.1016/j.jadohealth.2016.08.005. [DOI] [PubMed] [Google Scholar]
- 9.Ö'Brien D, Long J, Quigley J, et al. Association between electronic cigarette use and tobacco cigarette smoking initiation in adolescents: A systematic review and meta-analysis. BMC Public Health. 2021;21(1):1–10. doi: 10.1186/s12889-021-10935-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chan GC, Stjepanovi-ç D, Lim C, et al. Gateway or common liability? A systematic review and meta-analysis of studies of adolescent É-cigarette use and future smoking initiation. Addiction. 2021;116(4):743–756. doi: 10.1111/add.15246. [DOI] [PubMed] [Google Scholar]
- 11.Hammond, D., Reid, J.L., Rynard, V.L. et al. Prevalence of vaping and smoking among adolescents in Canada, England, and the United States: Repeat national cross sectional surveys. Bmj 365 (2019). [DOI] [PMC free article] [PubMed]
- 12.Walker N, Parag V, Wong SF, et al. Use of e-cigarettes and smoked tobacco in youth aged 14–15 years in New Zealand: Findings from repeated cross-sectional studies (2014–19) The Lancet Public Health. 2020;5(4):e204–e212. doi: 10.1016/S2468-2667(19)30241-5. [DOI] [PubMed] [Google Scholar]
- 13.Bowe AK, Doyle F, Stanistreet D, et al. E-cigarette-only and dual use among adolescents in Ireland: Emerging behaviours with different risk profiles. Int. J. Environ. Res. Public Health. 2021;18(1):332. doi: 10.3390/ijerph18010332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cerrai S, Potente R, Gorini G, Gallus S, Molinaro S. What is the face of new nicotine users? 2012–2018 e-cigarettes and tobacco use among young students in Italy. Int. J. Drug Policy. 2020;86:102941. doi: 10.1016/j.drugpo.2020.102941. [DOI] [PubMed] [Google Scholar]
- 15.Gotts, J.E., Jordt, S.E., McConnell, R. et al. What are the respiratory effects of e-cigarettes? Bmj 366 (2019). [DOI] [PMC free article] [PubMed]
- 16.Marques P, Piqueras L, Sanz MJ. An updated overview of e-cigarette impact on human health. Respir. Res. 2021;22(1):1–14. doi: 10.1186/s12931-021-01737-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.US Department of Health and Human Services. E-Cigarette Use Among youth and young adults: A Report of the Surgeon General-Executive Summary (2016).
- 18.Palipudi, K.M., Jones, C., Lee, K.A. et al. Awareness and use of electronic cigarettes among youth: Evidence from the Global Youth Tobacco Survey 2012–2015. Tobacco Induced Dis. 16(1) (2018).
- 19.World Health Organization. WHO report on the global tobacco epidemic, 2017: monitoring tobacco use and prevention policies. World Health Organization (2017).
- 20.Yoong SL, Hall A, Leonard A, et al. Prevalence of electronic nicotine delivery systems and electronic non-nicotine delivery systems in children and adolescents: A systematic review and meta-analysis. The Lancet Public Health. 2021;6(9):e661–e673. doi: 10.1016/S2468-2667(21)00106-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tarasenko, Y., Ciobanu, A., Fayokun, R. et al. Electronic cigarette use among adolescents in 17 European study sites: Findings from the Global Youth Tobacco Survey. Eur. J. Public Health (2021). [DOI] [PMC free article] [PubMed]
- 22.Echevarria C, Sinha IP. Heterogeneity in the measurement and reporting of outcomes in studies of electronic cigarette use in adolescents: A systematic analysis of observational studies. Tob. Control. 2017;26(3):247–253. doi: 10.1136/tobaccocontrol-2015-052881. [DOI] [PubMed] [Google Scholar]
- 23.World Health Organization, Centers for Disease Control and Prevention. Tobacco questions for surveys of youth (TQS-Youth): a subset of key questions from the Global Youth Tobacco Survey (GYTS). Tobacco questions for surveys of youth (TQS-Youth): A subset of key questions from the Global Youth Tobacco Survey (GYTS) (2019).
- 24.Gravely S, Driezen P, Ouimet J, et al. Prevalence of awareness, ever-use and current use of nicotine vaping products (NVPs) among adult current smokers and ex-smokers in 14 countries with differing regulations on sales and marketing of NVPs: Cross-sectional findings from the ITC Project. Addiction. 2019;114(6):1060–1073. doi: 10.1111/add.14558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Group TGC. The global tobacco surveillance system. Tobacco Control 15(Suppl 2):ii1 (2006). [DOI] [PMC free article] [PubMed]
- 26.Klein, D.E., Chaiton, M., Kundu, A. et al. A literature review on international e-cigarette regulatory policies. Curr. Addict. Rep. 1–11 (2020).
- 27.Palipudi KM, Mbulo L, Morton J, et al. Awareness and current use of electronic cigarettes in Indonesia, Malaysia, Qatar, and Greece: Findings from 2011–2013 global adult tobacco surveys. Nicotine Tob. Res. 2015;18(4):501–507. doi: 10.1093/ntr/ntv081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tavolacci MP, Vasiliu A, Romo L, et al. Patterns of electronic cigarette use in current and ever users among college students in France: A cross-sectional study. BMJ Open. 2016;6(5):e011344. doi: 10.1136/bmjopen-2016-011344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.World Health Organization. Electronic nicotine delivery systems and electronic non-nicotine delivery systems (ENDS/ENNDS) (2016).
- 30.Kennedy RD, Awopegba A, De Leon E, et al. Global approaches to regulating electronic cigarettes. Tob. Control. 2017;26(4):440–445. doi: 10.1136/tobaccocontrol-2016-053179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Beguinot E, Martinet Y. Tobacco industry strategies to attract new and young smokers. Rev. Prat. 2021;71(3):279–282. [PubMed] [Google Scholar]
- 32.US Department of Health and Human Services. Preventing tobacco use among youth and young adults: a report of the Surgeon General. 2012. Atlanta, GA: US Department of Health and Human Services, Centers for Disease. [PubMed]
- 33.Chen-Sankey, J.C., Unger, J.B., Bansal-Travers, M. et al. E-cigarette marketing exposure and subsequent experimentation among youth and young adults. Pediatrics 144(5) (2019). [DOI] [PMC free article] [PubMed]
- 34.Hartwell G, Thomas S, Egan M, et al. E-cigarettes and equity: A systematic review of differences in awareness and use between sociodemographic groups. Tob. Control. 2017;26(e2):e85–e91. doi: 10.1136/tobaccocontrol-2016-053222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Collins L, Glasser AM, Abudayyeh H, et al. E-cigarette marketing and communication: How e-cigarette companies market e-cigarettes and the public engages with e-cigarette information. Nicotine Tob. Res. 2019;21(1):14–24. doi: 10.1093/ntr/ntx284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kinnunen JM, Rimpel AH, Lindfors PL, et al. Electronic cigarette use among 14-to 17-year-olds in Europe. Eur. J. Pub. Health. 2021;31(2):402–408. doi: 10.1093/eurpub/ckaa145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Pampel FC. Global patterns and determinants of sex differences in smoking. Int. J. Comp. Sociol. 2006;47(6):466–487. doi: 10.1177/0020715206070267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Pathania, V.S. Women and the smoking epidemic: turning the tide. Bulletin of the World Health Organization 89, 162. SciELO Public Health (2011). [DOI] [PMC free article] [PubMed]
- 39.Foxon F, Selya AS. Electronic cigarettes, nicotine use trends and use initiation ages among US adolescents from 1999 to 2018. Addiction. 2020;115(12):2369–2378. doi: 10.1111/add.15099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Institute for global tobacco control. Minimum age. 2022. 12-1-2022.
- 41.Soneji S, Barrington-Trimis JL, Wills TA, et al. Association between initial use of e-cigarettes and subsequent cigarette smoking among adolescents and young adults: a systematic review and meta-analysis. JAMA Pediatr. 2017;171(8):788–797. doi: 10.1001/jamapediatrics.2017.1488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Goriounova NA, Mansvelder HD. Short-and long-term consequences of nicotine exposure during adolescence for prefrontal cortex neuronal network function. Cold Spring Harb. Perspect. Med. 2012;2(12):a012120. doi: 10.1101/cshperspect.a012120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hartmann-Boyce, J., McRobbie, H., Butler, A.R. et al. Electronic cigarettes for smoking cessation. Cochrane Data. Syst. Rev. (9) (2021). [DOI] [PMC free article] [PubMed]
- 44.Nicksic NE, Snell LM, Barnes AJ. Reasons to use e-cigarettes among adults and youth in the Population Assessment of Tobacco and Health (PATH) study. Addict. Behav. 2019;93:93–99. doi: 10.1016/j.addbeh.2019.01.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Sreeramareddy. Awareness about and e-cigarette use among adults in 15 low-and middle-income countries, 2014–2018 estimates from Global Adult Tobacco Surveys (2022). [DOI] [PubMed]
- 46.Pearson JL, Hitchman SC, Brose LS, et al. Recommended core items to assess e-cigarette use in population-based surveys. Tob. Control. 2018;27(3):341–346. doi: 10.1136/tobaccocontrol-2016-053541. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets used and/or analysed during the current study available on the website of Centre for Disease Control, Atlanta, USA. The data sets and Stata code used for analyses are available from the corresponding author on reasonable request.