

Abstract
Adolescence is a developmental period when peer network structure is associated with mental health. However, how networks relate to distress for youth at different intersecting racial/ethnic and gender identities is unclear. Using National Longitudinal Study of Adolescent to Adult Health survey data, cross-sectional models examine peer network cohesion predicting adolescent depressive levels for racial/ethnic and gender groups. The analytic sample is N=13,055, average age 15.3 years, 50.2% female, 68.8 % White, 17.2% Black, 9.7% Hispanic, and 4.2% Asian. The results indicate that average cohesion, depressive levels, and cohesion associated with depressive levels differ by race/ethnicity and gender, with the greatest benefits for White and Black girls. This work clarifies patterns of adolescent networks and mental health by race/ethnicity and gender.
Keywords: Social Networks, Intersectionality, Mental Health, Peers
Introduction
Peer networks are an important developmental resource for adolescent health (Umberson et al. 2010). However, it is unclear if networks relate to mental health in the same way for all youth. Intersectional perspectives (Andersen & Hill Collins 2016) suggest that overlapping identities create distinct multiplicative experiences of (dis)advantage for health (Homan et al., 2021). As a result, how peer networks relate to adolescent mental health likely differs by race/ethnicity and gender. This study uses nationally representative data on adolescents in the United States to cross-sectionally examine differences across racial/ethnic and gender groups. This study examines eight groups (Asian females, Asian males, Black females, Black males, Hispanic females, Hispanic males, White females, and White males) in levels of peer network cohesion, depressive symptoms, and how cohesion relates to depressive symptoms. In doing so, this work contributes to research on adolescent peer networks and intersectional health.
Adolescent Peer Network Cohesion
Adolescence is a period of socio-cognitive development in the life course when same-age peers play a key role in healthy development (Johnson et al., 2011). From the social networks perspective, peer networks provide foundational structures that shape mental health (Bearman & Moody 2004). While many studies examine network composition, such as the race/ethnicity of adolescents’ best friends (Kao & Joyner, 2004), network structure is also salient for mental health (Falci & McNeely, 2009).
One important aspect of peer network structure is whether or not one’s friends are cohesively interconnected (Walker, 2015). Peer cohesion is measured through structural patterns of network connections that represent existing ties compared to possible ties within one’s friendship group (Haynie, 2001). For example, densely interconnected groups where friends are friends with each other are highly cohesive, whereas an adolescent who spans different groups of disconnected friends experiences low cohesion.
Greater cohesion supports interaction and common identity (Haynie, 2001) and trust and shared norms (McGloin et al., 2014). As a result, cohesion can be a critical resource for mental well-being (Walker, 2015). However, high cohesion can increase over-regulation of behavior (Haynie, 2001) and enforced conformity (McGloin et al., 2014). High cohesion can also spur vicarious stress (Kornienko et al., 2013), all factors that can harm mental health. Results for how cohesion relates to distress are thus mixed, with some research suggesting that the impact of cohesion depends on social characteristics, such as gender (Falci & McNeely, 2009).
Gender and Cohesion
The developmental trade-offs model theorizes that gender socialization processes lead to the gendered structuring of adolescents’ peer relations, the relational content of friendships, and the emotional and behavioral consequences of friendships (Rose & Rudolph, 2006). Girls typically maintain smaller, more cohesive friend groups compared to boys’ larger activity-based friend groups (Molloy et al., 2014). Women and girls are also socialized to invest greater self-salience in interpersonal relationships than men and boys (Rosenfield 2012), resulting in greater efforts to maintain close relationships and social standing, and larger effects of relationships and social evaluation on girls’ mental health (Kornienko & Santos, 2014). Girls’ friendships are typically marked by high emotional disclosure and socioemotional support (Rose & Rudolph, 2006). Whereas boys often face social pressure against such behavior among peers, due to masculine norms that sanction seeking support or expressing mental distress (Kornienko & Santos, 2014).
For girls, this salience of peer networks and tendency toward support means that higher cohesion is typically beneficial for girls’ mental well-being (Falci & McNeely, 2009). Girls also usually have higher levels of cohesion from which to benefit (Molloy et al. 2014), so gender differences in cohesion related to mental health are exacerbated by differences in levels of cohesion. Conversely, adolescent boys tend to have less cohesive friend groups and are less likely to benefit from cohesion, in some cases experiencing increased mental distress from cohesion (Falci & McNeely, 2009).
Race/Ethnicity and Cohesion
Compared to the gender differences delineated by the developmental trade-offs model, how peer network structure and related consequences differ across racial/ethnic groups is understudied (Graham & Echols, 2018). Assumed benefits of networks may not generalize across race/ethnicity given that samples of peer networks have typically examined mostly White adolescents (Pagano & Hirsch, 2007). One of the few studies to consider how structural features of adolescent friendships vary by race/ethnicity shows in descriptive statistics that rates of reciprocated same-sex best friendships vary by race, with the lowest reciprocity for Black boys and the highest for White girls (Vaquera & Kao, 2008). However, whether these differences extend to other structures beyond best friend reciprocity or to how networks relate to mental health remains unclear.
Despite this research gap, there are several ways that macro-level racism likely affects adolescent networks and mental health. Systemic racism unequally exposes people of color to stressors that strain relationships and can increase risks of mental distress (Umberson et al., 2014). Research indicates that Black, Hispanic, and Asian youth have greater depressive symptoms than White youth from adolescence into early adulthood (Hargrove et al., 2020).
Systemic racism also shapes the hegemonically White cultural school context, limiting access to social resources for youth of color (Stanton-Salazar, 1997). For example, Latino youth experience lower support and greater disconnection from school peers, leading to less benefit from peer integration (Stanton-Salazar & Spina, 2005). Research also finds that Asian youth report fewer friends than other groups, perhaps due to less emphasis on fictive kin or to parents discouraging leisure time spent with peers (Way et al., 2005).
Adolescent school social networks are also typically patterned by racial/ethnic homophily, where same-race ties are more likely than cross-race ties (Moody 2001). As a result, social ties may further concentrate advantages among privileged groups, so that greater cohesion yields greater access to status and power for White youth compared to other racial/ethnic groups (Stanton-Salazar 1997). In sum, although specific questions about peer cohesion across racial/ethnic groups have yet to be explored, there is reason to believe that differences in cohesion may exist and that these differences may pattern mental health outcomes.
An Intersectional Perspective
Despite research focusing on social characteristics separately, gender and race/ethnicity simultaneously shape individuals’ lives. Intersectional perspectives indicate the joint, contingent importance of overlapping systems of oppression (Crenshaw, 1991), where positions at the nexus of multiple axes of identity create combinatory (dis)advantage beyond the sum of constituent components (Andersen & Hill Collins, 2016). These multiple social hierarchies affect health so health inequalities are both racialized and gendered (Homan et al., 2021). For example, women of color face both racism and sexism that harm health (Hargrove et al., 2020), whereas White men have privileged racial/ethnic and gender identities. Accordingly, Black and Hispanic women tend to have the greatest depressive symptoms across the life course, and White men the least (Hargrove et al., 2020).
These overlapping systems of oppression and privilege likely also affect social relations. Although girls tend to benefit from peer cohesion, this may differ across racial/ethnic identities. For example, racialized expectations of femininity for Hispanic girls may increase pressure to provide support in friendships (Stanton-Salazar & Spina, 2005) that taxes girls’ own mental health. Additional behavior regulation in school due to racist stereotypes may socially sanction Black girls’ tight-knit peer groups (Morris, 2007). Young Asian women may face gendered racism from peers through expectations of compliance or submissiveness (Ahn et al., 2021) that can similarly affect the benefits of cohesion to mental health.
Young men of color may experience additional disadvantages associated with their race/ethnicity that exacerbate potential detriments of cohesion for boys. Racialized hypermasculine stereotypes (Connell & Messerschmidt, 2005) may further limit friends from becoming supportive resources (Lindsey et al., 2010). Racialized gendered stereotypes of boys of color as violent or confrontational (Morris, 2007) may also shape perceptions of racial/ethnic minority boys’ peer groups, leading to potential sanctions for tight-knit groups.
Conversely, White youth may experience combinatory returns to privileged statuses that advantage health, perpetuating gendered and racialized health disparities (Link & García, 2021). Hegemonic norms of White emphasized femininity prioritize emotional expressiveness, sensitivity, and passivity (Rosenfield, 2012), which may increase cohesion and the benefits of cohesion to mental health for White girls. White boys may face pressure to maintain masculinity that limits support-seeking in friendships, but they may avoid racialized hypermasculine stereotypes faced by boys of color (Connell & Messerschmidt, 2005). Thus, social experiences, norms, and stressors at the intersection of race/ethnicity and gender may shape peer cohesion, mental health, and how cohesion relates to mental health for distinct groups.
Factors Related to Networks and Mental Health
In addition to racial/ethnic and gender differences, other characteristics and conditions affecting social life may shape both networks and mental health. Adjusting for such features is important when examining the association between networks and mental distress. For example, peer networks (Molloy et al., 2014) and mental health (Gregory et al., 2020) vary with age over the course of adolescent development. Socioeconomic status often relates to race/ethnicity and to mental health (Adkins et al., 2009). Characteristics of the school context, such as school size, may shape peer networks by providing different-sized pools of potential friends or qualitatively different social experiences (Cheadle & Goosby, 2012). Moreover, some youth may spend their social energy outside of school networks and having non-school friends or how non-school friends relate to mental health may differ by gender and race/ethnicity (Way & Chen, 2000). Adjusting for these known factors related to adolescent peer relations and distress enables a more precise view of peer cohesion and mental health across racial/ethnic and gender groups.
The Current Study
Prior work demonstrates associations between adolescent networks and mental health, as well as the importance of intersecting identities, but it is unclear whether peer networks relate to mental health differently based on distinct racial/ethnic and gender identities. Existing literature expects higher cohesion that is more salient to mental health for girls and that networks provide greater returns to White youth, but the lack of research on network structure at intersecting racial/ethnic and gender identities means that prior work does not support specific expectations for each group. Consequently, in lieu of hypotheses, this study explores two research questions: Does peer cohesion differ across racial/ethnic and gender groups, and do associations between cohesion and depressive symptoms differ across racial/ethnic and gender groups? This study addresses these questions by examining eight distinct racial/ethnic gender groups (Asian females, Asian males, Black females, Black males, Hispanic females, Hispanic males, White females, and White males) cross-sectionally1 across the range of adolescence, for individuals in Grades 7–12 (average age = 15.3). As other social factors may affect both social relations and mental health, analyses adjust for age, parental education, family structure, school size, and the number of out of school friends.
Methods
Data and Participants
Data come from the National Longitudinal Study of Adolescent to Adult Health (Add Health, Harris, 2013). This nationally representative survey of United States adolescents was collected from students in grades 7–12 in 1994–95. A stratified sample of 80 high schools based on school type, size, racial/ethnic composition, urbanicity, and region, plus one feeder school for each high school, yielded a nationally representative sample of 90,118 students in 132 schools. The Wave I response rate was 79%. Social networks were from the Wave I in-school survey where respondents were asked to, “list your closest male (female) friends,” with up to 5 male and 5 female friends. Nominations with a uniquely identifiable sender and receiver were matched to create networks of school friendships (n=119 networks, Carolina Population Center, 2001).
Analyses included respondents in schools with network data who were measured on their depressive symptoms in Wave I and had valid survey weights (n=13,435). Analyses excluded cases with missing race or gender information (n=380) for a final analytic sample of 13,055 respondents (weighted average age 15.3 years, 50.2 % female, 68.8 % White). This study refrained from further sample restrictions (such as limiting to a smaller age range) to prioritize adequate sample sizes of racial/ethnic and gender groups, as discussed further below.
Depressive Symptoms
The outcome of depressive symptoms was assessed using the 5-item Center for Epidemiological Studies-Depression scale (Radloff, 1977) indicated when assessing depression across racial/ethnic groups (Perreira et al., 2005). Responses were summed to create a scale ranging from 0–15. The Cronbach’s alpha for this scale suggests high reliability (alpha =.78).
Cohesion
Cohesion was measured as effective ego-network density. Density measures the proportion of existing ties to possible ties (Valente, 2010), based on sent and received friendship nominations, following prior work (Guan & Kamo, 2016; Haynie, 2001; Reynolds & Crea, 2015). This measure indicates the tight-knittedness of an adolescent’s peer connections. This measure was then adjusted for the survey cap at nominating 10 close friends to measure effective density adjusted for survey design, calculated as
where, S=sum of ties in the sent/received (directed) ego-network, N =number of nodes in sent/receive ego-network, and 10 indicates the maximum sent nominations. Respondents with zero friends or only one friend had a zero for cohesion.
Racial/ethnic and gender groups
Racial/ethnic and gender groups were defined using a four-category measure of race/ethnicity constructed as recommended for the dataset (Harris, 2013) for non-Hispanic White, non-Hispanic Black, Hispanic, and non-Hispanic Asian, and a two-category measure of gender (male, female), creating eight separate race/ethnicity gender groups. With this categorical measure, results are presented using the reference category (White girls) that best aids coefficient interpretation (Johfre & Freese, 2021), but alternative comparisons are discussed.
Age
Age was captured at Wave I and ranges from 11–21, with 99% of the sample 19 years old or younger (and results are robust to limiting the sample to age 19 or under, discussed below).
Parental Education
Models included an ordinal variable of highest parental education (1=less than high school, 2=high school diploma, 3=some college, 4=college completion) as a proxy for socioeconomic status.
Biological Parents
Models included a dichotomous variable indicating whether the respondent reported living with two biological parents at Wave I (1=yes, 0=no) as a proxy for family structure.
School Size
Models adjusted for school size, measured by the number of students in a school, standardized.
Out of School Friends
Models included the number of out of school friends, measured by the number of individuals a respondent nominated as a close friend who did not attend the respondent’s school.
Analyses
Models assessed the relationship between cohesion and depressive symptoms at Wave I using ordinary least squares (OLS) regression. Models then interacted the racial/ethnic and gender groups with cohesion to test if any association of cohesion with depressive symptoms differs across groups. Study covariates were either complete (school size, out of school friends) or missingness was below 5% (maximum parental education, age). However, the measure of two biological parents had a higher missingness at 28%. Analyses used multiple imputation with chained equations (MICE) and 20 iterations to adjust for variable missingness, as well as survey weights to adjust for survey sampling design.
Results
Descriptive statistics for the weighted sample by each racial/ethnic and gender group are shown in Table 1. For average depressive symptoms in adolescence, Hispanic females had the greatest symptoms, followed by Black females, Asian females, and then White females. Even White females, who had the lowest depressive levels among females, had higher depressive levels than any male group. Among males, Asian males had the highest depressive levels, followed by Black males, Hispanic males, and White males. These results follow expectations for mental health by gender and race/ethnicity, with female adolescents typically having higher depressive levels than males, and students of color experiencing greater distress than White students.
Table 1.
Descriptive Statistics (Weighted) by Race/Ethnicity and Gender; National Longitudinal Study of Adolescent to Adult Health (N=13,055)
| White male | White female | Black male | Black female | Hispanic male | Hispanic female | Asian male | Asian female | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean or % | SD | Mean or % | SD | Mean or % | SD | Mean or % | SD | Mean or % | SD | Mean or % | SD | Mean or % | SD | Mean or % | SD | |
| Depressive Symptoms (0–15) | 1.95 | 0.06 | 2.53 | 0.07 | 2.38 | 0.09 | 3.11 | 0.13 | 2.24 | 0.13 | 3.52 | 0.18 | 2.45 | 0.18 | 3.08 | 0.21 |
| Cohesion | 0.19 | 0.01 | 0.21 | 0.01 | 0.13 | 0.01 | 0.16 | 0.01 | 0.15 | 0.01 | 0.17 | 0.01 | 0.17 | 0.01 | 0.17 | 0.01 |
| Age | 15.37 | 0.15 | 15.16 | 0.15 | 15.52 | 0.26 | 15.42 | 0.23 | 15.38 | 0.27 | 15.30 | 0.24 | 15.51 | 0.28 | 15.47 | 0.29 |
| Maximum Parent Education | ||||||||||||||||
| Less than High School | 7.21% | 7.95% | 10.31% | 13.61% | 31.60% | 32.38% | 9.68% | 11.79% | ||||||||
| High School | 32.37% | 31.88% | 37.64% | 39.70% | 30.76% | 29.92% | 23.37% | 20.63% | ||||||||
| Some College | 22.58% | 24.19% | 20.07% | 21.88% | 15.29% | 19.58% | 12.48% | 18.88% | ||||||||
| College | 37.84% | 35.98% | 31.98% | 24.81% | 22.35% | 18.12% | 54.48% | 48.70% | ||||||||
| Two Biological Parents | 80.29% | 78.20% | 55.33% | 64.88% | 74.43% | 73.61% | 88.13% | 84.07% | ||||||||
| Number Out of School Friends | 1.13 | 0.11 | 1.47 | 0.07 | 0.92 | 0.07 | 1.70 | 0.12 | 1.08 | 0.12 | 1.53 | 0.15 | 1.16 | 0.20 | 1.60 | 0.24 |
| School Size | 855.94 | 66.12 | 833.92 | 69.19 | 863.28 | 80.88 | 966.00 | 107.14 | 1317.97 | 190.47 | 1334.81 | 205.14 | 1214.74 | 190.06 | 1250.19 | 181.83 |
Gender differences were less stark for average cohesion, illustrated in Figure 1. White females had the highest average cohesion, at .21, indicating that a little over 20% of all possible ties were observed in their close friend networks. White males had the second highest cohesion levels, at .19. Black females, Hispanic females, and Asian males and females all had similar levels of peer cohesion, though significantly lower than those of White youth. Hispanic males had the second lowest cohesion, below levels for White adolescents and Hispanic females. Black males had the least cohesion compared to any other group in the sample, with about 13% of possible ties present in their close friend groups. These patterns indicate that levels of cohesion differed across race/ethnicity gender groups, with White girls experiencing the highest cohesion on average, followed by White boys, while Black boys experienced the least cohesion.
Fig. 1.
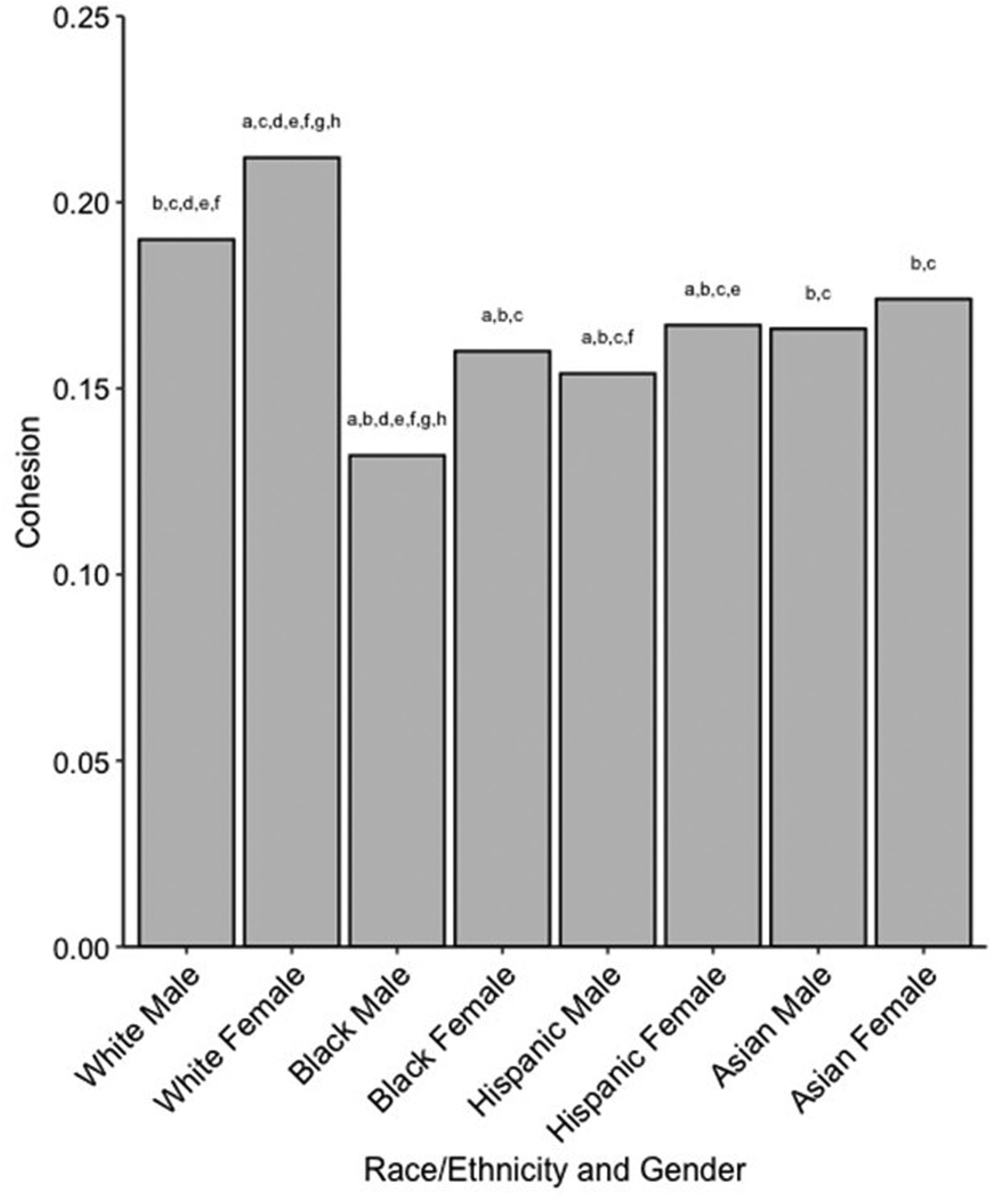
Average Cohesion by Race/Ethnicity and Gender (weighted). Note: a = significantly different than White males; b = significantly different than White females; c = significantly different than Black males; d = significantly different than Black females; e = significantly different than Hispanic males; f = significantly different than Hispanic females; g = significantly different than Asian males; h = significantly different than Asian females
Model 1 in Table 2 examines predicted depressive symptoms for each race/ethnicity gender group, compared to the reference category of White females. After adding covariates, patterns from descriptive statistics persist. Black, Hispanic, and Asian females had significantly higher depressive levels than White females, while every male group had significantly lower depressive levels than White females. In Model 1, cohesion predicted lower depressive levels, indicating that higher cohesion generally relates to fewer depressive symptoms. The coefficient of −1.026 indicates that for every additional .10 of cohesion (an additional 10% of possible ties present in one’s close friend group) there was a decrease of about .10 in depressive symptoms.
Table 2.
OLS regression predicting Wave I Depression; National Longitudinal Study of Adolescent to Adult Health (N=13,055)
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| Variable | Coef | SE | Coef | SE |
| Race/Ethnicity Gender Groups | ||||
| White Female (ref.) | ||||
| White Male | −0.596 *** | 0.069 | −0.817 *** | 0.163 |
| Black Male | −0.353 ** | 0.118 | −0.703 ** | 0.217 |
| Black Female | 0.367 * | 0.151 | 0.453 | 0.302 |
| Hispanic Male | −0.529 ** | 0.149 | −0.966 *** | 0.255 |
| Hispanic Female | 0.739 *** | 0.174 | −0.051 | 0.380 |
| Asian Male | −0.074 | 0.185 | −0.440 | 0.328 |
| Asian Female | 0.515 * | 0.205 | 0.159 | 0.376 |
| Cohesion | −1.032 ** | 0.315 | −1.883 ** | 0.640 |
| Race/Ethnicity Gender Groups * Cohesion | ||||
| White Female (ref.)*Cohesion | ||||
| White Male*Cohesion | 1.059 | 0.765 | ||
| Black Male*Cohesion | 2.130 | 1.210 | ||
| Black Female*Cohesion | −0.818 | 1.413 | ||
| Hispanic Male*Cohesion | 2.487 * | 1.127 | ||
| Hispanic Female*Cohesion | 4.470 * | 1.761 | ||
| Asian Male*Cohesion | 1.940 | 1.432 | ||
| Asian Female*Cohesion | 1.838 | 1.474 | ||
| Age | 0.120 *** | 0.017 | 0.121 *** | 0.017 |
| Maximum Parent Education (ref: Less than High School) | ||||
| High School | −0.369 ** | 0.119 | −0.377 ** | 0.119 |
| Some College | −0.642 *** | 0.132 | −0.643 *** | 0.131 |
| College | −0.830 *** | 0.118 | −0.833 *** | 0.118 |
| Two Biological Parents | −0.406 *** | 0.096 | −0.403 *** | 0.096 |
| Number Out of School Friends | 0.048 * | 0.018 | 0.046 * | 0.018 |
| School Size | −0.016 | 0.047 | −0.009 | 0.047 |
p<.05
p<.01
p<.001
Model 2 in Table 2 includes interactions between cohesion and each racial/ethnic and gender group. Here, even among youth with peer cohesion at zero, White, Black, and Hispanic males experienced significantly lower depressive levels compared to White females. For White females, cohesion still predicted lower depressive levels, but interactions indicate that cohesion was significantly less protective for Hispanic males and females in comparison to White females.
To better understand how cohesion relates differently to depressive levels for each group rather than just in relation to White females, Figure 2 provides the average marginal effects of cohesion by race/ethnicity and gender groups. Table 3 presents corresponding values for average marginal effects and denotes significant differences between all groups. Here, results show that higher cohesion predicted lower depressive levels for White females and Black females, and to a lesser extent, White males. For White females and Black females, an additional .10 of cohesion corresponded with decreases in depressive symptoms of .19 and .27, respectively. For White males, an additional .10 of cohesion corresponded with a reduction of .08 in depressive symptoms. No other group showed significant associations between cohesion and depressive levels. Thus, while only Hispanic males and females significantly differ from White females in Model 2 (and from Black females in Table 3), cohesion also did not significantly predict depressive symptoms for Asian males, Asian females, or Black males. Although Model 1 suggests that cohesion relates to better mental health, this association was only for White females, Black females, and White males.
Fig. 2.
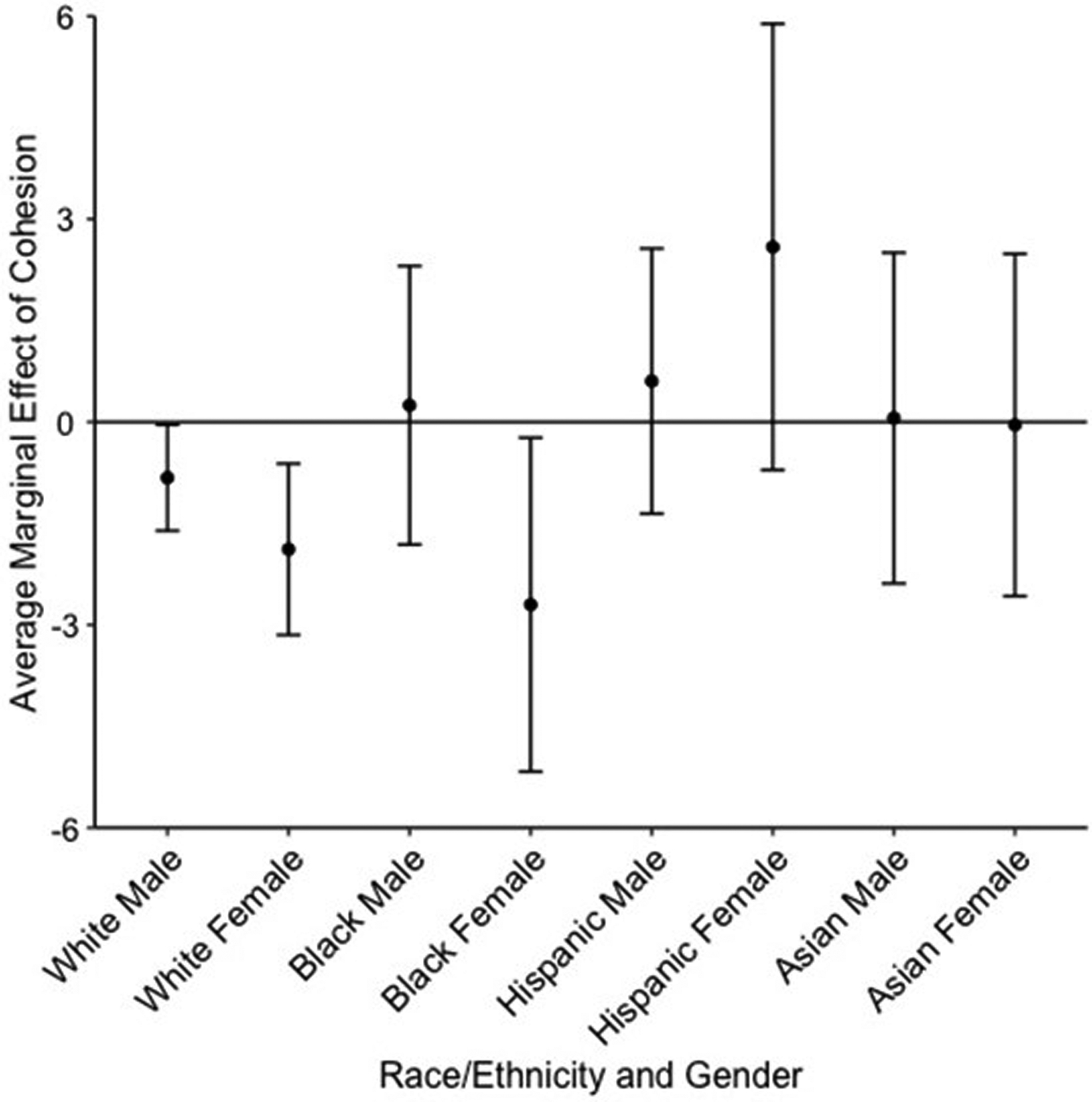
Average marginal effects of cohesion predicting depressive symptoms across Race/Ethnicity and Gender
Table 3.
Average Marginal Effects of Cohesion predicting Depressive Symptoms by Race/Ethnicity and Gender; National Longitudinal Study of Adolescent to Adult Health (N=13,055)
| Average Marginal Effect | 95% Confidence Interval | Significant Differences (p<.05) | |
|---|---|---|---|
| White Male | −0.823 * | [−1.607, −0.040] | f |
| White Female | −1.883 ** | [−3.149, −0.616] | e,f |
| Black Male | 0.247 | [−1.812, 2.306] | |
| Black Female | −2.701 * | [−5.170, −0.232] | e,f |
| Hispanic Male | 0.605 | [−1.355, 2.565] | b,d |
| Hispanic Female | 2.588 | [−0.711, 5.887] | a,b,d |
| Asian Male | 0.058 | [−2.388, 2.503] | |
| Asian Female | −0.044 | [−2.575, 2.487] |
Note: a= significantly different than White males; b= significantly different than White females; c= significantly different than Black males; d= significantly different than Black females; e= significantly different than Hispanic males; f= significantly different than Hispanic females; g= significantly different than Asian males; h= significantly different than Asian females
p<.05
p<.01
p<.001
To further investigate the role of cohesion for White males, White females, and Black females, Figure 3 plots predicted depressive symptoms by cohesion (holding all other covariates at their mean values) and the average cohesion level for these groups. This figure shows that although the effect of cohesion appeared strongest for Black females, their relatively higher depressive levels means that Black females exhibited greater depressive symptoms than White males across most levels of cohesion.
Fig. 3.
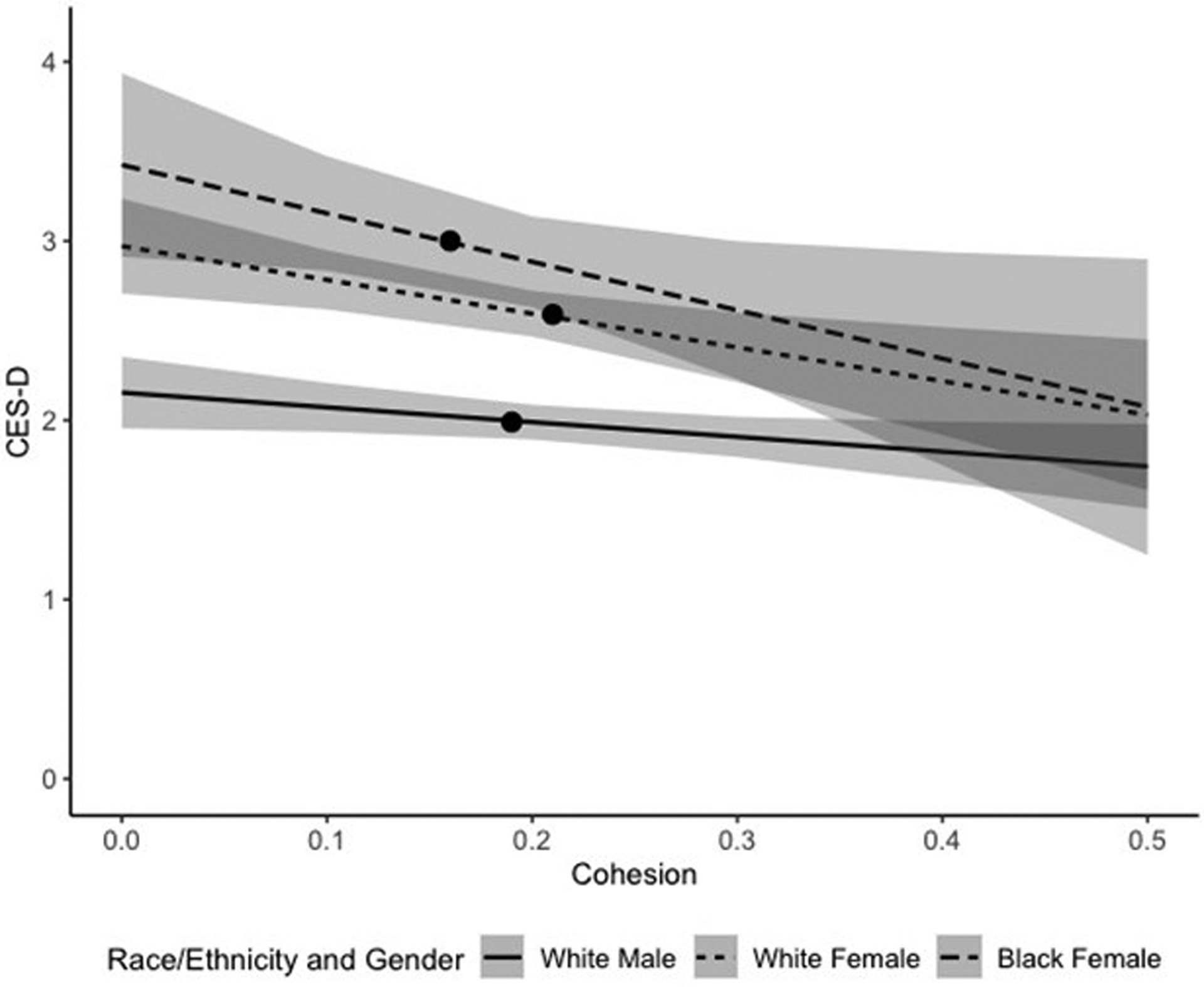
Depressive Symptoms by Cohesion for White Males, White Females, and Black Females. Note: Black circle denotes average cohesion for each group
Results were robust to many alternate specifications. The depressive symptoms scale used here as an outcome was not assessed in the prior in-school survey wave, but this prior wave did include a one-item proxy for depression. Results of an additional model adjusting for this proxy measure (Appendix A) were substantively similar to those shown here, particularly for Black females and White males, although the association between cohesion and depressive symptoms fell to marginal significance (p<.10) for White females. This pattern could indicate that for White females, cohesion may have a stronger association with contemporaneous rather than subsequent distress in a way that differs from Black females and White males, who saw a persistent association with subsequent depressive symptoms net of prior depression.
Adding outdegree or total degree to control for individuals’ social activity or general friendliness (which may affect both networks and distress) did not change results. Measuring cohesion as effective ego-network density based only on sent ties (Appendix B), as sent ties indicate friendships from ego’s perspective that may be more relevant to ego’s outcomes, produced similar results to those shown here. Measuring cohesion as effective ego-network density based only on reciprocal ties (Appendix C), as reciprocal ties are often used as a proxy for high-quality, close friendships, produced somewhat similar results to those shown here; cohesion remained significant for Black females (p<.01), and cohesion became marginally significant (p<.10) for White females and non-significant for White males. This pattern may indicate that cohesion among strong, close friendships may be most important for Black females, while White teens may see more beneficial associations with mental health from weaker ties. To remain consistent with prior work measuring cohesion based on sent and received ties in these data (Guan & Kamo, 2016; Haynie, 2001; Reynolds & Crea, 2015) and research indicating the differential importance of sent and received ties for adolescent mental health (Kamis and Copeland 2020), main models operationalized cohesion based on sent and received ties.
As prior work indicates the importance of the social context’s racial and gender composition, additional models tested several composition measures. Controlling for school racial and gender composition, such as the percentage of White students or the degree of racial and gender segregation in the overall school network, did not change results. Controlling for ego-network composition through the racial heterogeneity of individuals’ friend groups and the proportion of friends that are female marginally impacted results: the difference between White females and Hispanic males in cohesion predicting depressive levels fell to p<.10 significance. Finally, although analyses prioritize retaining sample size to adequately capture race/ethnicity and gender groups, analyses (available upon request) restricting the sample to those who were aged 19 or younger at Wave I (N=13,032) had consistent results with those shown here.
Discussion
In adolescence, peer networks become highly salient for mental health (Falci & McNeely, 2009), yet it is unclear if networks relate to mental health in the same way for all youth. Gender is a socializing factor shaping peer networks and how networks relate to mental health (Rose & Rudolph, 2006). However, intersectional perspectives suggest that overlapping dimensions of race/ethnicity and gender lead to distinct experiences of (dis)advantage in social systems (Andersen & Hill Collins, 2016). Both social relations (Umberson et al. 2014) and mental health (Hargrove et al., 2020) differ by race/ethnicity and gender, meaning that adolescent peer cohesion and how it relates to mental health may also differ for racial/ethnic and gender groups.
Results here indicate that levels of cohesion do in fact differ by race/ethnicity and gender. White girls experienced significantly higher cohesion than other groups, and Black boys experienced significantly lower cohesion than others. White boys had lower cohesion than White girls, but significantly higher cohesion than all other groups. Black girls, Hispanic boys and girls, and Asian boys and girls had middling levels of cohesion.
As little research has systematically described how peer network structures may differ across racial/ethnic groups (Graham & Echols, 2018), this finding is an important one. These gaps in cohesion would likely not be visible without separately examining racial/ethnic groups, indicating that generalizability regarding cohesion in typical, predominantly White samples may be limited for youth of color who have significantly different peer cohesion experiences.
Next, consistent with past research (Hargrove et al., 2020), results show that depressive levels also differed across racial/ethnic and gender groups. Girls of color experienced the most and White boys the fewest depressive symptoms. These patterns mirror typical gender differences observed in adolescent mental health, with higher distress among girls, as even the least depressive female group (White girls) had higher depressive levels than the most depressive male group (Asian boys). Results here extend evidence of mental health differences by showing that within each gender group, White youth exhibited the lowest depressive levels.
Finally, results indicate that how cohesion relates to depressive symptoms differs across groups. Model 2 shows that cohesion predicted fewer depressive symptoms for only White girls, Black girls, and to a lesser extent, White boys. These results indicate associations, not causal effects, meaning that higher cohesion for White youth and Black girls may benefit mental health, or mental health may affect cohesion, for example, if depressive friends induce conflict or emotional demands that strain tight-knit friendships (Rose & Rudolph, 2006). Regardless, results here indicate that associations of cohesion with depressive levels are not generalizable to all youth, but only maintained for White girls, Black girls, and White boys. Results of average marginal effects, shown in Figure 2, indicate that for all other groups, cohesion did not significantly predict depressive levels. Associations for Hispanic youth were significantly different from those for White girls, with Hispanic youth seeing comparatively less of a beneficial association between cohesion and depressive symptoms.
Taken together, results indicate that White girls had both a beneficial association between cohesion and mental health and the most cohesion from which to benefit (or to garner as a beneficial return to mental well-being). In contrast, Black girls saw beneficial associations between depressive levels and cohesion, but they had significantly less cohesion at their disposal and greater average depressive symptoms. While White boys saw a smaller beneficial association between cohesion and depressive levels, they had the lowest initial depressive levels and higher levels of cohesion from which to benefit compared to all other groups except White girls. In this way, White youth are privileged compared to other groups when considering the combined experiences of higher cohesion, lower depressive symptoms, and significant beneficial associations between cohesion and depressive levels. These results also mirror broader patterns of mental health disparities based on race/ethnicity and gender. Levels of peer cohesion and the extent to which that cohesion is beneficially associated with mental health may be one more aspect of social life in which White individuals garner privilege that translates to better mental health outcomes to perpetuate mental health disparities.
Comparing results from Models 1 and 2 indicates that failing to disaggregate experiences of distinct racial/ethnic and gender groups would suggest that cohesion was associated with lower depressive levels for all adolescents, while this finding only reflects the experience of a few groups. The higher levels of peer cohesion and beneficial associations with depressive levels for White youth suggest that aspects of systemic racism in the school social environment may condition experiences of peer network structure in relation to mental health for many racial/ethnic minority adolescents. For example, some Hispanic youth may have many peer ties, but experience less support or social capital from them, creating barriers to beneficial associations between cohesive friendships and mental health (Stanton-Salazar & Spina, 2005). Hispanic girls (Stanton-Salazar & Spina, 2005) and Asian girls (Ahn et al., 2021) may face racialized gendered stereotypes regarding behaviors and social demands in peer relationships that limit the benefits of cohesion to mental health.
Results for Black boys (who have the lowest peer cohesion) align with theories of racialized masculinity (Connell & Messerschmidt 2005), suggesting that Black boys may face the greatest social sanctions against facets of friendships that can make groups more cohesive and yield beneficial associations from cohesion. This finding supports research suggesting that Black boys’ mental health may face particular risks, given their likelihood to experience both high-stress environments and low network support (Lindsey et al., 2010).
Results here are consistent with expectations of White students facing fewer stigmatizing barriers in the peer environment. White girls may experience positive reinforcement between perceptions of how girls should enact social relationships aligned with hegemonic ideas of White emphasized femininity (Rosenfield, 2012). This reinforcement may lead to both the greatest cohesion and strongest association between cohesion and mental health for White girls (Rose & Rudolph, 2006).
Notably, Black girls have different patterns than other racial/ethnic minority groups, with a beneficial association between mental health and cohesion. This pattern highlights the importance of distinguishing experiences of distinct groups, as Black boys see no benefit from cohesion, but Black girls do. This result aligns with prior work noting Black girls’ strengths in maintaining close, supportive kin ties (Pagano & Hirsch, 2007), extending this pattern to suggest that peer ties may be another important source of support for Black girls’ well-being. Bolstering tight-knit peer groups for Black girls may be an important resource for healthy development.
Results should be considered in light of several limitations. Data are collected nearly thirty years ago and provide one snapshot of in-school friendships. Future work should consider processes described here using contemporary data that can provide a more holistic view of adolescents’ peers. Models here are cross-sectional given data limitations, and ancillary analyses using a one-item measure of prior depressive symptoms suggest that the timing of associations between cohesion and depressive levels may differ by group. Future work should consider patterns described here over time to better disentangle reciprocal effects of cohesion and mental health for different groups. Models here consider network structure, and although results are robust to considering composition, future work should study the moderating role of composition in how structure relates to mental health, as well as additional network features that relate to different relational processes. Small sample sizes limit examining additional groups, with adequate samples of only four racial/ethnic categories and a binary measure of gender. Small sample sizes also limit analyses of additional identities that likely matter for peers and health, such as class, sexuality, gender identity, or nativity, which should be considered in future work.
Adolescence captures a wide-ranging developmental period in which associations between networks and mental health likely differ as youth age. Ancillary analyses (available upon request) suggest that as adolescents age, depressive levels increase and cohesion decreases. However, analyses here cannot distinguish differences across early, middle, or late adolescence for all racial/ethnic and gender groups with present sample sizes. Analyses assessing patterns across different adolescent stages for the larger groups where sample size permits (only White and Black respondents) suggested that density may be more predictive of depressive symptoms for Black females in mid to late (compared to early) adolescence. Future work with larger samples of racial/ethnic minority youth across ages should consider how patterns observed here might differ with age or at specific stages of adolescence. Despite limitations, these data provide the current best opportunity to examine peer network structure in a nationally representative sample of adolescents.
Conclusion
Despite research indicating the importance of peer networks for adolescent mental health, whether beneficial associations between peer cohesion and mental health extend across distinct racial/ethnic and gender groups is unclear. This study addresses this gap by applying an intersectional lens to social networks, finding that White youth have relatively higher and Black boys significantly lower levels of peer cohesion compared to others. Mental health is also patterned by gender and race, with the highest depressive levels for racial/ethnic minority girls. Moreover, cohesion is only beneficially associated with lower depressive levels for White and Black girls, and to a lesser extent, White boys. Consequently, White adolescents are advantaged by having both beneficial associations between cohesion and mental health and the highest levels of cohesion. Stakeholders working with youth should invest in fostering tight-knit friend groups for all youth by reducing stigma or other barriers that limit cohesion or benefits of cohesion for many racial/ethnic minority youth. Future research should examine why cohesion does not relate to mental health for some adolescents, with an eye toward remedying gaps in past research for particularly understudied racial/ethnic minority groups, as well as potential opportunities for intervention in the links between peer networks and mental health. By demonstrating racial/ethnic and gender group differences in peer network structure, depressive levels, and the association of networks with depressive levels, this study contributes to research on intersectional health and adolescent peer networks to highlight how social networks can contribute to mental health disparities in adolescence.
Supplementary Material
Acknowledgments
Thank you to Allison Stolte, Jessica S. West, and Scott Lynch for their helpful comments.
Footnotes
Longitudinal social network data in Add Health are only collected in a subset of 16 schools, meaning longitudinal analyses do not have a sufficient sample size to examine distinct racial/ethnic and gender groups.
References
- Adkins DE, Wang V, Dupre ME, van den Oord EJCG, & Elder GH (2009). Structure and Stress: Trajectories of Depressive Symptoms across Adolescence and Young Adulthood. Social Forces, 88(1), 31–60. 10.1353/sof.0.0238 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahn LH, Keum BT, Meizys GM, Choudry A, Gomes MA, & Wang L (2021). Second-generation Asian American Women’s Gendered Racial Socialization. Journal of Counseling Psychology. 10.1037/cou0000575 [DOI] [PubMed] [Google Scholar]
- Andersen ML, & Hill Collins P (2016). Why Race, Class, and Gender Still Matter. In Andersen ML & Collins PH (Eds.), Race, Class, Gender: An Anthology (9th ed., p. 516). Cengage Learning. [Google Scholar]
- Bearman PS, & Moody J (2004). Suicide and Friendships among American Adolescents. American Journal of Public Health, 94(1), 89–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carolina Population Center. (2001). National Longitudinal Study of Adolescent Health: Network Variables Code Book.
- Cheadle JE, & Goosby BJ (2012). The Small-school Friendship Dynamics of Adolescent Depressive Symptoms. Society and Mental Health, 2(2), 99–119. 10.1177/2156869312445211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connell RW, & Messerschmidt JW (2005). Hegemonic Masculinity: Rethinking the Concept. Gender & Society, 19(6), 829–859. 10.1177/0891243205278639 [DOI] [Google Scholar]
- Crenshaw K (1991). Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color. Stanford Law Review, 43(6), 1241–1299. 10.2307/1229039 [DOI] [Google Scholar]
- Falci C, & McNeely C (2009). Too Many Friends: Social Integration, Network Cohesion and Adolescent Depressive Symptoms. Social Forces, 87(4), 2031–2062. [Google Scholar]
- Graham S, & Echols L (2018). Race and Ethnicity in Peer Relations Research. In Burkowski WM, Laursen B, & Rubin KH (Eds.), Handbook of peer interactions, relationships, and groups (pp. 590–614). [Google Scholar]
- Gregory D, Turnbull D, Bednarz J, & Gregory T (2020). The Role of Social Support in Differentiating Trajectories of Adolescent Depressed Mood. Journal of Adolescence, 85, 11. [DOI] [PubMed] [Google Scholar]
- Guan W, & Kamo Y (2016). Contextualizing Depressive Contagion: A Multilevel Network Approach. Society and Mental Health, 6(2), 129–145. 10.1177/2156869315619657 [DOI] [Google Scholar]
- Hargrove TW, Halpern CT, Gaydosh L, Hussey JM, Whitsel EA, Dole N, Hummer RA, & Harris KM (2020). Race/Ethnicity, Gender, and Trajectories of Depressive Symptoms Across Early- and Mid-Life Among the Add Health Cohort. Journal of Racial and Ethnic Health Disparities, 7(4), 619–629. 10.1007/s40615-019-00692-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris KM (2013). The Add Health Study: Design and Accomplishments. 10.17615/C6TW87 [DOI] [Google Scholar]
- Haynie DL (2001). Delinquent Peers Revisited: Does Network Structure Matter? American Journal of Sociology, 106(4), 1013–1057. [Google Scholar]
- Homan P, Brown TH, & King B (2021). Structural Intersectionality as a New Direction for Health Disparities Research. Journal of Health and Social Behavior, 002214652110329. 10.1177/00221465211032947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johfre SS, & Freese J (2021). Reconsidering the Reference Category. Sociological Methodology. 10.1177/0081175020982632 [DOI] [Google Scholar]
- Johnson MK, Crosnoe R, & Elder GH (2011). Insights on Adolescence from a Life Course Perspective. Journal of Research on Adolescence, 21(1), 273–280. 10.1111/j.1532-7795.2010.00728.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kao G, & Joyner K (2004). Do Race and Ethnicity Matter Among Friends? The Sociological Quarterly, 45(3), 557–573. 10.1111/j.1533-8525.2004.tb02303.x [DOI] [Google Scholar]
- Kornienko O, Clemans KH, Out D, & Granger DA (2013). Friendship Network Position and Salivary Cortisol Levels. Social Neuroscience, 8(4), 385–396. 10.1080/17470919.2013.795500 [DOI] [PubMed] [Google Scholar]
- Kornienko O, & Santos CE (2014). The Effects of Friendship Network Popularity on Depressive Symptoms During Early Adolescence: Moderation by Fear of Negative Evaluation and Gender. Journal of Youth and Adolescence, 43(4), 541–553. 10.1007/s10964-013-9979-4 [DOI] [PubMed] [Google Scholar]
- Lindsey MA, Joe S, & Nebbitt V (2010). Family Matters: The Role of Mental Health Stigma and Social Support on Depressive Symptoms and Subsequent Help Seeking Among African American Boys. Journal of Black Psychology, 36(4), 458–482. 10.1177/0095798409355796 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Link BG, & García SJ (2021). Diversions: How the Underrepresentation of Research on Advantaged Groups Leaves Explanations for Health Inequalities Incomplete. Journal of Health and Social Behavior, 002214652110281. 10.1177/00221465211028152 [DOI] [PubMed] [Google Scholar]
- McGloin JM, Sullivan CJ, & Thomas KJ (2014). Peer Influence and Context: The Interdependence of Friendship Groups, Schoolmates and Network Density in Predicting Substance Use. Journal of Youth and Adolescence, 43(9), 1436–1452. 10.1007/s10964-014-0126-7 [DOI] [PubMed] [Google Scholar]
- Molloy LE, Gest SD, Feinberg ME, & Osgood DW (2014). Emergence of Mixed-Sex Friendship Groups during Adolescence: Developmental Associations with Substance Use and Delinquency. Developmental Psychology, 50(11), 2449–2461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moody J (2001). Race, School Integration, and Friendship Segregation in America. American Journal of Sociology, 107(3), 679–716. 10.1086/338954 [DOI] [Google Scholar]
- Morris EW (2007). “Ladies” or “Loudies”?: Perceptions and Experiences of Black Girls in Classrooms. Youth & Society, 38(4), 490–515. 10.1177/0044118X06296778 [DOI] [Google Scholar]
- Pagano ME, & Hirsch BJ (2007). Friendships and Romantic Relationships of Black and White Adolescents. Journal of Child and Family Studies, 16(3), 347–357. 10.1007/s10826-006-9090-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perreira KM, Deeb-Sossa N, Harris KM, & Bollen K (2005). What Are We Measuring? An Evaluation of the CES-D Across Race/Ethnicity and Immigrant Generation. Social Forces, 83(4), 1567–1602. [Google Scholar]
- Radloff LS (1977). The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement, 1(3), 385–401. 10.1177/014662167700100306 [DOI] [Google Scholar]
- Reynolds AD, & Crea TM (2015). Peer influence processes for youth delinquency and depression. Journal of Adolescence, 43, 83–95. 10.1016/j.adolescence.2015.05.013 [DOI] [PubMed] [Google Scholar]
- Rose AJ, & Rudolph KD (2006). A Review of Sex Differences in Peer Relationship Processes: Potential trade-offs for the emotional and behavioral development of girls and boys. Psychological Bulletin, 132(1), 98–131. 10.1037/0033-2909.132.1.98 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenfield S (2012). Triple jeopardy? Mental health at the intersection of gender, race, and class. Social Science and Medicine, 74(11), 1791–1801. 10.1016/j.socscimed.2011.11.010 [DOI] [PubMed] [Google Scholar]
- Stanton-Salazar RD (1997). A Social Capital Framework for Understanding the Socialization of Racial Minority Children and Youths. Harvard Educational Review, 67(1), 1–41. 10.17763/haer.67.1.140676g74018u73k [DOI] [Google Scholar]
- Stanton-Salazar RD, & Spina SU (2005). Adolescent Peer Networks as a Context for Social and Emotional Support. Youth & Society, 36(4), 379–417. 10.1177/0044118X04267814 [DOI] [Google Scholar]
- Umberson D, Crosnoe R, & Reczek C (2010). Social Relationships and Health Behavior Across the Life Course. Annual Review of Sociology, 36(1), 139–157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Umberson D, Williams K, Thomas PA, Liu H, & Thomeer MB (2014). Race, Gender, and Chains of Disadvantage: Childhood Adversity, Social Relationships, and Health. Journal of Health and Social Behavior, 55(1), 20–38. 10.1177/0022146514521426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valente TW (2010). Social Networks and Health: Models, Methods, and Applications. Oxford University Press. [Google Scholar]
- Vaquera E, & Kao G (2008). Do You Like Me as Much as I Like You? Friendship Reciprocity and its Effects on School Outcomes among Adolescents. Social Science Research, 37(1), 55–72. 10.1016/j.ssresearch.2006.11.002.Do [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker MH (2015). The Contingent Value of Embeddedness: Self-affirming Social Environments, Network Density, and Well-being. Society and Mental Health, 5(2), 128–144. 10.1177/2156869315574601 [DOI] [Google Scholar]
- Way N, & Chen L (2000). Close and General Friendships among African American, Latino, and Asian American Adolescents from Low-Income Families. Journal of Adolescent Research, 15(2), 274–301. 10.1177/0743558400152005 [DOI] [Google Scholar]
- Way N, Gingold R, Rotenberg M, & Kuriakose G (2005). Close friendships among urban, ethnic-minority adolescents. New Directions for Child and Adolescent Development, 2005(107), 41–59. 10.1002/cd.120 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.