

Abstract
Introduction:
As renal development and maturation processes begin in utero and continue through early childhood, sensitive developmental periods arise during which metal exposures can program subclinical nephrotoxicity that manifests later in life. We used novel dentine biomarkers of established nephrotoxicants including arsenic (As), cadmium (Cd), lead (Pb), chromium (Cr), and lithium (Li), and their mixtures, to identify critical windows of exposure-associated kidney function alterations in preadolescents.
Methods:
Participants included 353 children in the Programming Research in Obesity Growth, Environment and Social Stressors (PROGRESS) longitudinal birth cohort study based in Mexico City. Estimated glomerular filtration rate (eGFR) was assessed in 8–12 year old children using serum cystatin C measures. Pre- and postnatal metal(loid) concentrations were assessed in weekly increments by analyzing deciduous teeth with laser ablation-inductively coupled plasma-mass spectrometry. We used reverse distributed lag models (rDLMs) and lagged Weighted Quantile Sum (L-WQS) regression to examine time-varying associations between weekly perinatal metal(loid) exposure or metal(loid) mixtures and preadolescent eGFR while adjusting for age, sex, BMI z-score, SES and prenatal tobacco smoke exposure.
Results:
We identified a critical window of susceptibility to Pb exposure, in the late 3rd trimester (5 weeks prior to birth) during which higher Pb exposure was associated with children’s increased eGFR. When all elements were assessed as a mixture, we identified late 2nd/early 3rd trimester (weeks 8–17 of gestation) as a window of vulnerability associated with decreased eGFR, with Li and Cr contributing the greatest weights to the association. When stratified by sex, we observed stronger effects among boys than girls.
Conclusions:
Using tooth-matrix biomarkers, we identified discrete developmental exposure windows wherein Pb and metal(loid) mixtures were associated with altered preadolescent kidney function.
Keywords: Metals, Nephrotoxicity, Tooth, Kidney function, Critical windows, Perinatal
1. Introduction
The developing kidney is especially vulnerable to environmental insults compared to the mature adult kidney. Nephrogenesis begins at 4 weeks of gestation and is largely complete by birth in full term infants. In the second and third trimesters, the majority of branching morphogenesis occurs (between 11 and 14 weeks’ gestation) (Sampogna et al., 2015) and 90% of nephron formation is completed (between 26 and 36 weeks’ gestation) (Hinchliffe et al., 1991; Benz and Amann, 2010; Solhaug et al., 2004). Early childhood also reflects windows of renal maturation that can increase susceptibility to environmental insults as homeostatic processes (e.g. renal blood flow and glomerular filtration) continue to mature (Veille et al., 1998; Gubhaju et al., 2014). Exposure to environmental toxicants during these periods of in utero and postnatal susceptibility may result in low nephron endowment (the number of mature nephrons at birth) or altered filtration and reabsorptive processes, established risk factors for chronic kidney disease (CKD) and hypertension (Solhaug et al., 2004; Brenner et al., 1988; Ingelfinger, 2008; Sanders et al., 2018; Luyckx and Brenner, 2020; Gurusinghe et al., 2017). Thus, in order to protect against risk of later life CKD, it is imperative to prevent in utero and early postnatal insults.
Environmental metal(loid)s such as arsenic (As), lead (Pb), cadmium (Cd), lithium (Li) and chromium (Cr) are nephrotoxicants associated with CKD (Goyer, 1993; Wedeen and Qian, 1991; Lee et al., 2020; Kessing et al., 2015) and kidney injury in adults (Tsai et al., 2017; Navas-Acien et al., 2009). Concomitant exposure to these ubiquitous metals in pregnancy and during early childhood is common, due to a variety of dietary and environmental sources, including natural local geology, air pollution, smoking, pharmaceuticals, and industrial, agricultural and domestic emissions (Tchounwou et al., 2012; Anke et al., 2003). These metals can cross the placenta and infants are particularly vulnerable to environmental metal exposures due to underdeveloped metabolic systems and behaviours such as hand-to-mouth activities (Landrigan et al., 2004). Toxic metal(loid)s can disrupt nephrogenesis as well as primary renal developmental processes vital for maintaining nutrient and waste product homeostasis. In population-based studies, children’s Pb, Cd, and Cr exposure are associated with decreased kidney function (Fadrowski et al., 2010), as well as elevated levels of protein biomarkers of tubular dysfunction such as kidney injury molecule-1 (KIM-1) and beta 2 microglobulin (B2M) (Cárdenas-González et al., 2016; Zheng et al., 2017). Yet, there are limited data on timing of perinatal environmental risk factors, as exposures captured at single time points do not provide adequate resolution to assess exposure occurring throughout the nuanced stages of kidney development and maturation.
Tooth-based biomarkers offer important advantages to studying how the perinatal environment contributes to later life diseases such as CKD and hypertension. Pb, As and Cr accumulate in hard tissue including bones and teeth (Rodríguez and Mandalunis, 2018). Indeed, teeth serve as excellent matrices to assess concomitant metal(loid)s exposure during early life (Arora and Austin, 2013). Deciduous (baby) teeth begin forming in utero and mineralize following an incremental pattern (akin to growth rings) (Berkovitz et al., 2009). Metals accumulate in the mineralizing tooth as it grows, creating an archive of fetal and postnatal exposure (Arora et al., 2014; Arora et al., 2012). Microspatial sampling of metal distribution in teeth has been used to construct fine-scale temporal profiles of exposure at nearly weekly resolution beginning in the 2nd trimester through to early childhood (Claus Henn et al., 2018; Horton et al., 2018; Arora et al., 2017; Müller et al., 2019; Dean et al., 2019).
In this study, we set out to identify critical windows of perinatal toxic metal(loid) exposures leveraging the fine scale (1–2 weeks) resolution of the tooth biomarker with preadolescent kidney function assessed at ages 8–12 years. To our knowledge this is the first longitudinal study to examine time-varying associations of nephrotoxic metal(loid)s exposure with kidney function parameters in healthy children.
2. Methods
2.1. PROGRESS cohort description:
Our analysis included 353 participants from the Programming Research in Obesity, Growth, Environment and Social Stressors (PROGRESS) cohort from Mexico City. PROGRESS is a prospective, ongoing, NIH-funded birth cohort study in Mexico City founded in 2007. Pregnant women receiving care through the Mexican Social Security Institute were enrolled between July 2007 and February 2011. All mothers provided informed and written consent and children provided assent at the 8–12 year-age visit. The study protocols were approved by the institutional review boards of the Brigham and Women’s Hospital, the Icahn School of Medicine at Mount Sinai and the National Institute of Public Health in Mexico.
Women were eligible for enrollment if they were 18 years or older, pregnant at fewer than 20 weeks’ gestation, had access to a telephone, planned to reside in Mexico City for the following three years, were free of heart or kidney disease, did not use steroids or anti-epilepsy drugs, or consume alcohol on a daily basis (Braun et al., 2014). Analyses excluded children born preterm (less than 37 weeks gestation) and post term (>42 weeks gestation), based on gestational age at delivery which was calculated using maternal report of last menstrual period and confirmed with Capurro physical examination at birth (Sanders et al., 2015). Participants provided naturally shed deciduous teeth during the regular study visits which were then stored at room temperature. Of 948 mother-infant pairs assessed, a total of 581 preadolescents attended the 8–12 year-age visit. At the visit, fasting blood samples were collected in vacutainer tubes, according to the standard protocol by a trained phlebotomist. Serum samples were stored at −80 °C until subsequent laboratory analyses for cystatin C and eGFR calculation. The study participants for this analysis were restricted to the 353 participants who had complete data including measures of serum cystatin C, weekly tooth measures and covariates of interest.
2.2. Tooth metal(loid) determination by LA-ICP-MS:
We analyzed deciduous teeth (incisors, canines and molars) that were free of obvious defects such as caries, fillings and extensive tooth wear. Dentine As, Cd, Cr, Li and Pb were measured using laser ablation-inductively coupled plasma-mass spectrometry (LA-ICP-MS) after sectioning teeth along the labio-lingual/buccal-lingual plane, as described in prior studies (Arora and Austin, 2013; Austin et al., 2013; Hare et al., 2011). Briefly, we identify the neonatal line (a histological feature formed in enamel and dentine at birth) and daily growth incremental markings to assign temporal information to sampling points. The laser ablation unit used was an ESI NWR-193 system with an excimer argon-fluoride laser emitting a nanosecond laser pulse at a wave-length of 193 nm, and a two volume ablation chamber. An approximately 40 cm length of Tygon® tubing (i.d. 3 mm) connected the laser ablation unit and the Agilent Technologies 8800 ICP-MS. The instrument was fitted with a ‘s’ lens system for enhanced sensitivity. As part of the daily performance, the system was tuned for sensitivity using NIST SRM 612 (trace elements in glass). Typical oxide formation, as measured by 232Th+/232Th16O+ was consistently under 0.3 % and fractionation was minimal (232Th+/238U+ 100 ± 5 %). Samples were ablated in raster mode in mantle dentine adjacent to the enamel-dentine junction. Depending on tooth type, the line ablated covered a timeline from the start of the second trimester (14 weeks gestation) through up to one year of age. Laser and ICP-MS conditions are recorded in Supplemental Table 1. A pre-ablation line (50 μm spot, 100 μm/s, 5 Hz, 1 J/cm2) was run first to remove surface contamination. Metal(loid) intensities were normalized to average calcium (43Ca) per tooth to control for any variations in mineral content within a tooth and between tooth type and individuals. Data were analyzed as Metal(loid)-Isotope:43Ca ratios.
2.3. Serum cystatin C and creatinine assessment:
Cystatin C was measured in serum samples using the Quantikine Enzyme-Linked Immunosorbent Assay (ELISA) Human Cystatin C Immunoassay (R&D Systems, Minneapolis, MN). Optical density was measured by a microplate reader (Synergy HT, BioTek Instruments, Inc., Winooski, VT) set to 450 nm. Each plate contained an internal control with inter-assay coefficients of variability (precision between plates) less than 5%. The limit of detection was 60 pg/mL with a linear range between 62.5 and 2000 pg/mL. Serum creatinine was measured using Creatinine FS reagent and Respons 910 (both by DiaSys, Holzheim, Germany), based on Jaffe’s kinetic method without deproteinization. The detection limit was 0.2 mg/dL. All standards, samples and controls were analyzed in duplicate with intra-assay coefficients of variability less than 5%.
2.4. Estimated glomerular filtration rate (eGFR):
eGFR was calculated according to two validated formulae for children, as previously described (Saylor et al., 2022). These included the CKiD cystatin C-based equation [Eqn (1)] (Schwartz et al., 2012) and the Schwartz equation [Eqn (2)] (Schwartz et al., 2009) and:
| (1) |
with cystatin C in mg/L (Schwartz et al., 2012);
| (2) |
where k = 0.55 for children younger than 13 years (Schwartz et al., 2009);
We present eGFRCysC2012 in our main models as cystatin C-derived estimates are suggested to more closely estimate the measured GFR in pediatric populations (Ng et al., 2018; Aggarwal et al., 2012), since cystatin C is produced by all mononucleated cells and less subject to variation with muscle mass and BMI compared to serum creatinine (Gerchman et al., 2009).
2.5. Covariates
Child height and weight were measured with a professional digital scale and stadiometer (InBody230, InBody, Seoul, Korea) with the head in the Frankfort plane. Weight and height were used to calculate BMI categories according to the WHO z-scores for age and sex, defined as obesity (z-score > 2), overweight (1 < z-score ≤ 2), normal weight (−2 < z-score ≤ 1) and underweight (z-score ≤ −2) (de Onis and Lobstein, 2010; WHO Multicentre Growth Reference Study Group, 2006). In regression analyses, participants in the underweight category (n = 2) were included in the normal weight category. Information on maternal socioeconomic status (SES) and environmental tobacco exposure were collected at the 2nd trimester visit using a standardized questionnaire. Prenatal household environmental tobacco smoke exposure was dichotomized as yes/no based on the mother’s report that at least one household member smoked during the pregnancy. The SES index during pregnancy was calculated based on the 1994 Mexican Association of Intelligence Agencies Market and Opinion (AMAI) rule 13 * 6. The index classifies families into 6 levels based on 13 questions related to the characteristics of the household. The majority of families were middle or low SES. Thus, the 6 resultant levels were further collapsed into 3 SES categories: lower, medium, and higher.
2.6. Statistical analysis
In single chemical analyses, we conducted reverse distributed lagged models (rDLMs) adjusted for covariates including child age, sex, BMI z-score categorized according to WHO guidelines, prenatal tobacco smoke in the home and SES. rDLMs utilized a truncated power function spline with best possible knot placement with positions in 4 clusters over a grid of values with optimization based on minimizing the sum of squared error. Regressions were initially performed using directionally unrestricted models with further assessment exploring both positively constrained and negatively constrained directions individually.
To evaluate the potential for a time-varying mixture effect of the 5 nephrotoxic metal(loid)s, we conducted lagged weighted quatile sum (WQS) regression (Gennings et al., 2020). As we previously reported, L-WQS is an extension of WQS strategy that accommodates time-varying effects similar to rDLMs, but in the context of predictive mixtures. Here, L-WQS models included directionally unconstrained analyses with additional analyses constrained to the positive direction only and the negative direction only. Critical windows were identified as time zones where the Holm-Bonferroni 95% confidence intervals did not cross zero. Next, we investigated interaction effects with lagged stratified interaction WQS regression [Equation (3)]. The strata-specific WQS models [Equations (4) and (5)] consisted of the lagged model which permitted for strata-specific weights and beta parameters for children who were exposed (household indoor tobacco smoke exposure) versus those who were not. To set general notation, let I be an indicator for group 0 (reference level) and group 1.
| (3) |
For group 0, the model is:
| (4) |
so that β1(t) denotes the time-varying association for group 0 between WQS(t) and Y.
For group 1, the model is:
| (5) |
so that β1(t) + β12(t) is the time-varying association for group 1, β12 is the difference in the association between the two groups and β2 is the difference in the intercept due to the covariate.
These analyses permit different metal(loid) weights per strata and different beta coefficients per strata in the interaction model. Here, we performed the regressions with β2 that was not time-varying: sex (male served as referent) and prenatal household indoor tobacco smoke exposure. We hypothesized sex-specific differences and that children with prenatal tobacco smoke exposure would have increased metal(loid) burden (e.g. Pb and Cd) and associated kidney function decline.
3. Results
Demographic characteristics of the 353 preadolescents with complete data at the 8–12 year-old visit are shown in Table 1. Age and sex of participants did not differ significantly from the parent cohort, although a higher proportion of participants who contributed tooth samples were overweight, obese and of ‘middle’ SES compared to those who did not (data not shown). Majority participants were considered lower SES and 30% of mothers reported exposure to secondhand tobacco smoke in the home. The average age of kidney function assessment was 10 years ranging between 8 and 12 years; 50% were boys. Approximately half of the children were normal weight, and 27% and 23% were considered overweight or with obesity respectively. Four children had eGFRCKiD2012 values less than 75 mL/min, a level potentially indicative of adolescent kidney function decline (Delanaye et al., 2019). Dentine-metal-to-calcium ratios measured between the 2nd trimester and 12 months of age (Seupplmental Fig. 1) were generally not associated with child sex, age at kidney function assessment, BMI, prenatal tobacco smoke, or SES.
Table 1.
Participant demographics for n = 353 child-mother pairs in the PROGRESS cohort included in this analysis.
| Arithmetic mean (SD) or % | |
|---|---|
| Age, years | 9.72 (0.73) |
| Male, % | 50% |
| Socioeconomic status+ | |
| Lower | 51% |
| Medium | 41% |
| Higher | 8% |
| Exposure to secondhand smoke (yes/no) | 30% |
| Child BMI+ | |
| Underweight (z-score ≤ −2)* | 0.4% |
| Normal Weight (z-score > −2, ≤ 1) | 49.5% |
| Overweight (z-score > 1, ≤ 2) | 26.5% |
| Obese (z-score > 2) | 23.6% |
| Serum Cystatin C (mg/L) | 0.71 (0.16) |
| Serum Creatinine (mg/dL) | 0.42 (0.09) |
| eGFRSchwartz (mL/min/1.73 m2) | 183.67 (41.33) |
| eGFRCySC2012 (mL/min/1.73 m2) | 101.25 (22.3) |
In regression analyses using categorical BMI z-score, underweight participants (n = 2) were included in the normal weight category.
Note: Two-sample t-tests and chi-squared tests were used to compare the demographic information of the study subset with participants in the parent cohort that did not contribute teeth. SES and child BMI z-score were statistically different from each other via these statistical tests.
3.1. Single metal(loid) analyses identified windows of prenatal Pb exposure associated with eGFR
Using rDLMs, we examined associations between individual dentine metal(loid)s and preadolescent eGFR. We found that prenatal Pb exposure in the 5 weeks prior to birth was associated with increased eGFR (Fig. 1). No significant associations were observed between single-metal (loid) exposure to As, Cd, Li, or Cr and eGFR.
Fig. 1. rDLMs of single-metal(loid) As, Cd, Cr, Li, or Pb exposures and cystatin C-based eGFR at age 9 years.
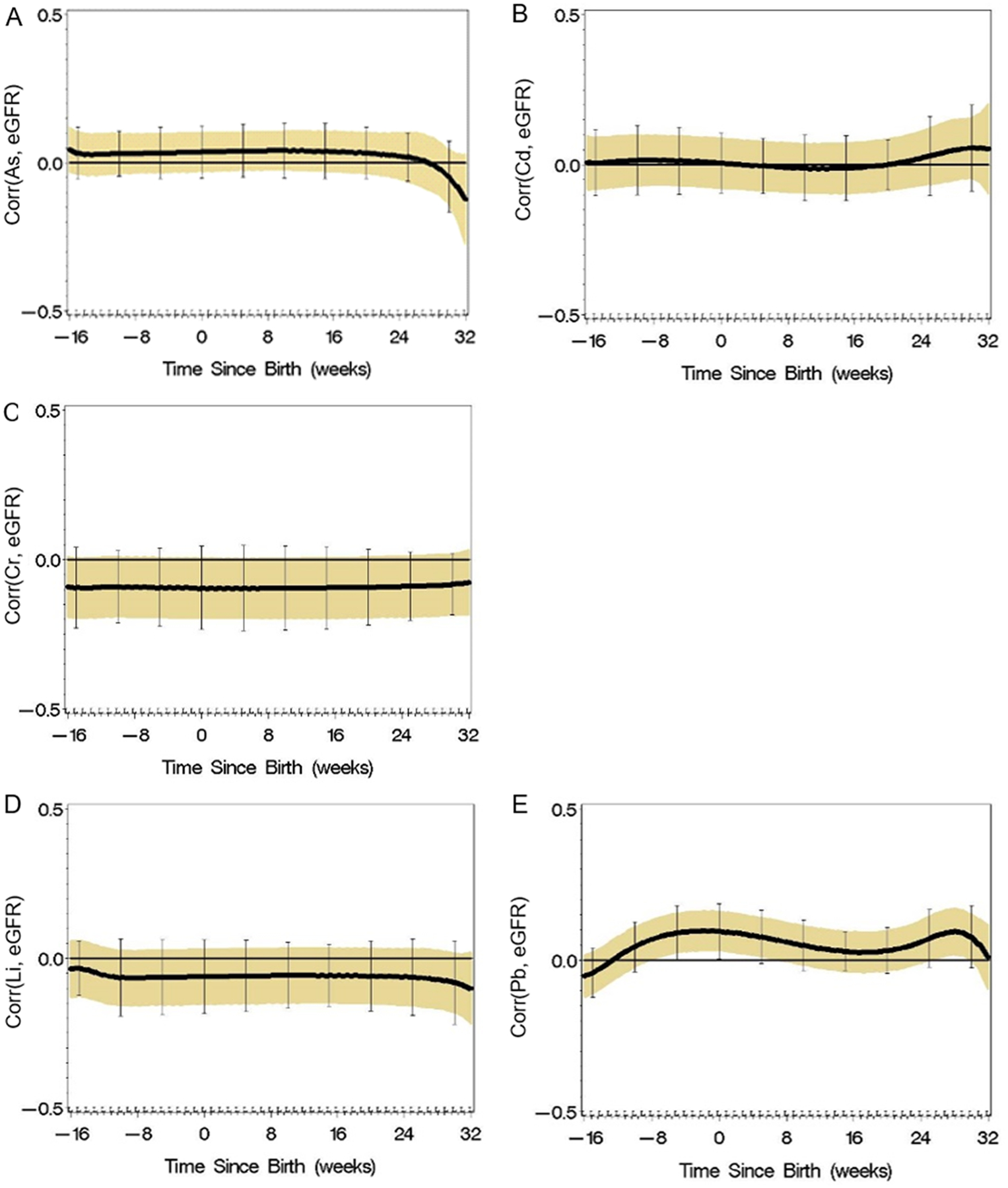
The solid black line represents the smoothed, time-varying association between dentine concentrations and eGFR; shaded region indicates 95% confidence limits and error bars are Holm-Bonferroni correction for multiple comparisons. A significant window from birth to about 5 weeks prior, was identified for Pb exposure.
3.2. Windows of perinatal metal(loid) mixtures associated with reduced preadolescent eGFR
We used L-WQS to examine the time-varying associations between perinatal co-exposure to As, Cd, Cr, Pb, and Li with eGFR. When constrained in the positive direction, the mixture was associated with increased eGFR after 24 postnatal weeks, with Li as the main contributor. However, this association was not statistically significant. When constrained in the negative direction, we observed that prenatally, between 8 and 17 weeks prior to birth, metal(loid) mixture exposure was associated with decreased eGFR at 9 years (Fig. 2). The highest weighted metal(loid)s contributing to the association in this window were Cr and Li.
Fig. 2. Associations of time-varying perinatal metal(loid) mixture exposures and cystatin C-based eGFR at age 9 years.
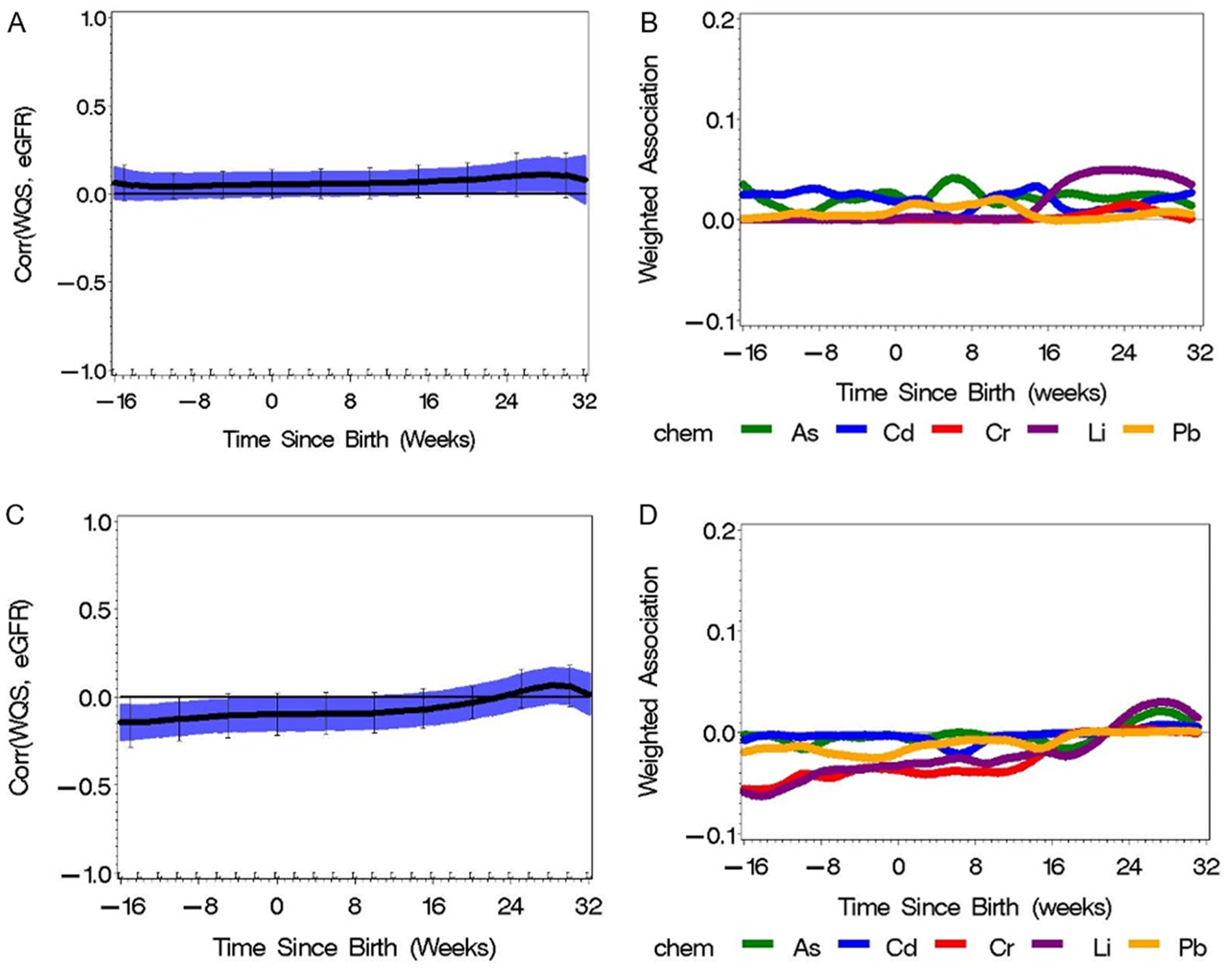
(a) L-WQS constrained in the positive direction and (b) associated weights. Li was the highest weighted metal(loid) contributing to a positive association with eGFR after 24 weeks postnatal but this is not significant. (c) L-WQS constrained in the negative direction. Prenatal metal(loid) mixture exposure 8–17 weeks before birth was associated with decreased eGFR. (d) The highest weighted metal(loid)s contributing to the association in this window were Li and Cr. The solid black line represents the smoothed, time-varying association between the metal(loid) mixture and eGFR; shaded region indicates 95% confidence limits and error bars are Holm-Bonferroni correction.
3.3. Evidence of sex specific effects
To evaluate whether there was evidence of interaction effects by sex, we conducted stratified L-WQS regression (Figs. 3 and 4) which includes time-varying interaction parameters. When the confidence interval on the interaction parameter excludes 0, there is a significant sex-specific difference. Constrained in the negative direction we observed an inverse association between eGFR and metal(loid) mixture at 8–16 weeks before birth and from 15 weeks postnatally in boys (Fig. 3). This association was primarily driven by Li, Cr and As in the prenatal window, and Pb and Cd in the postnatal window. We tested the differences in effect estimates between sexes using stratified L-WQS and found the difference was greatest from about 24 weeks postnatally, but this was not statistically significant. In girls, Cr and Pb were the biggest contributors to the association between the metal(loid) mixture and eGFR from about 24 weeks, though the associated weights are much smaller than observed in boys. When constrained in the positive direction, we did not observe a difference between sexes, but we did observe differences in the time-varying weights for each mixture (Fig. 4). In preliminary models stratified by BMI z-score categories, we did not observe evidence of effect modification.
Fig. 3. Stratified L-WQS to assess sex differences in the metal(loid)-mixture association with eGFR at 9 years, constrained in the negative direction.
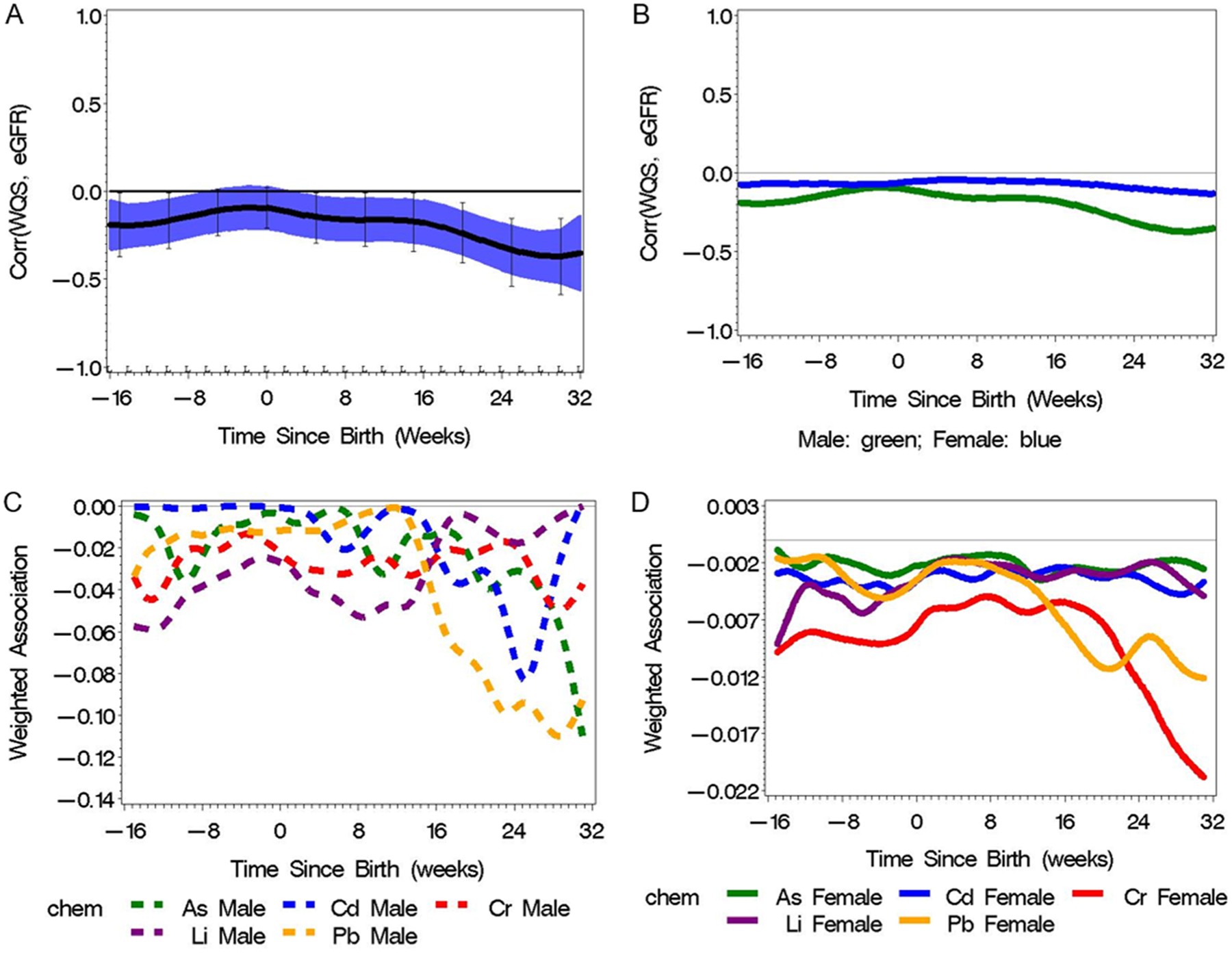
(a) L-WQS in boys, (b) time-varying differences between boys and girls, (c) time-varying weights of metal(loid) mixture in boys, (d) time-varying weights of metal-mixture in girls. We observed an inverse association between eGFR and metal(loid) mixture at 8–16 weeks before birth and from 15 weeks postnatally in boys (3a). This association was primarily driven by Li, Cr and As in the prenatal window, and Pb and Cd in the postnatal window (3c). The differences in effect estimates between sexes was greatest after 24 weeks postnatally (3b), but this was not statistically significant.
Fig. 4. Stratified L-WQS to assess sex differences in the metal(loid)-mixture association with eGFR at 9 years, constrained in the positive direction.
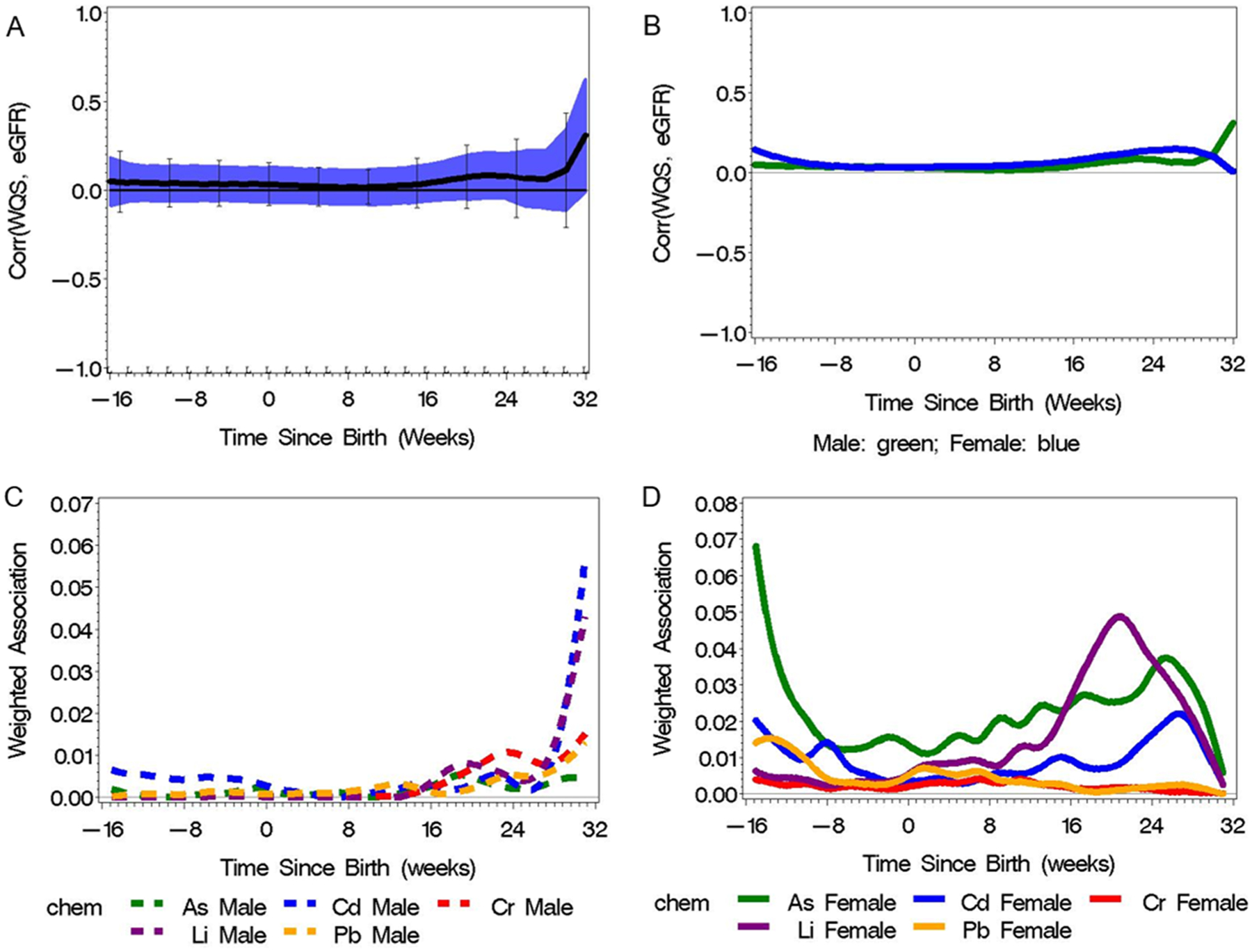
(a) L-WQS in boys, (b) time-varying differences between boys and girls, (c) time-varying weights of metal(loid) mixture in boys, (d) time-varying weights of metal(loid)-mixture in girls. We did not observe a difference between sexes, but we did observe differences in the time-varying weights for each mixture.
3.4. Effect modification by prenatal tobacco smoke exposure
When stratified by prenatal tobacco smoke exposure status, we did not observe statistically significant differences between children exposed prenatally to tobacco smoke in the home (Supplementary Fig. 2). However, we observed evidence of the association among children without environmental tobacco exposure. Speficially, we observed an inverse association between the metal(loid) mixture and eGFR during the prenatal period and postnatally after about 12 weeks, in children not exposed to prenatal environmental tobacco smoke (ETS). Differences in the mixture weights were observed between the two groups, with Li and Cr driving the prenatal association and Pb driving the postnatal mixture effect in the non-ETS exposed group. Notably, these results suggest that the primary relationship between metal(loid) mixtures and eGFR observed in the main models were not related to ETS exposure status, or alternately, that ETS obscures the association with metal(loid)s.
4. Discussion
In this study, we observed critical windows of prenatal toxic metal (loid) exposure that predict later life altered preadolescent eGFR. We observed that prenatal Pb exposure 5 weeks prior to birth was associated with children’s increased eGFR. We also observed that prenatal exposure to metal(loid) mixtures 8–17 weeks before birth was associated with decreased eGFR with the metals Li and Cr contributing most to the association. The identified exposure windows have important significance in the context of kidney development as they overlap with the timing of branching morphogenesis (2nd trimester) and nephrogenesis (3rd trimester) (Hinchliffe et al., 1991; Benz and Amann, 2010; Solhaug et al., 2004).
To our knowledge, this is the first study to report time-varying perinatal metal(loid) exposures associated with preadolescent kidney function. However prior studies that assessed Pb concentrations in urine and blood have reported mixed associations with eGFR in children [as reviewed in (Zheng et al., 2017)]. For example, in a prospective cohort study of 391 North Americans between ages 1 and 19 years, blood Pb concentrations were associated with a decrease in eGFR although the findings did not reach statistical significance (Fadrowski et al., 2010), potentially due to the wide age range of participants. Further, a cross-sectional study of 83 Mexican children ages 5–12 reported that dose-dependent urine Cr and high As levels were associated with increased kidney injury molecule-1 (KIM-1) and other kidney function biomarkers; they reported no significant associations with urine Pb, Cd or fluoride concentrations (Cárdenas-González et al., 2016). One potential explanation of inconsistent prior observations may be that previous studies could not measure time-varying effects and therefore may have missed critical windows. It is not surprising then that we observed contrasting directionality of effect estimates in windows of susceptibility for prenatal Pb exposure with increased filtration and metal(loid) mixtures with decreased filtration. This is because the earliest signs of Pb-associated kidney perturbations can include glomerular hyper-perfusion and hypertrophy that may precede kidney function decline. Thus, our findings suggest that a hyper- vs. hypofiltration state may be dependent on the timing, duration and level of predominant metal(loid) exposure that fluctuates throughout early life. Moreover, the tooth biomarker adds critically relevant time-varying exposure information and is an important improvement over traditional exposure assessments measured at discrete pre- or postnatal time points.
Nephron endowment, the number of new nephrons at birth, can range between 0.2 and 2 million nephrons per kidney due to developmental platsticity (Hughson et al., 2003; Puelles et al., 2011). Nephro-toxic exposures during the perinatal period through early childhood may cause permanent loss of nephrons resulting in low nephron endowment or number. As these are established risk factors for CKD, it is imperative to maximize nephron endowment and limit nephrotoxic exposures. Sources of Pb and Li exposure in Mexico City are largely dietary and therefore intervenable factors. As Pb-glazed ceramics are widely used in Mexico for food preparation (Pantic et al., 2018; Sanders et al., 2018), Pb ingestion is common (Kupsco et al., 2019). Drinking water is considered the major source of environmental Li exposure, with notable dietary contributions as well, and Li exposure varies considerably by geography (Anke et al., 2003). In Mexico, Li water levels in the north and center of the country are higher compared to US levels (Lindsey et al., 2021; Rubio-Arias et al., 2007; Padilla-Reyes et al., 2012). A small study of mother-infant pairs in Argentina showed Li is transported across the placenta with no saturation effect, and that exclusively breastfed infants had significantly lower urinary Li than non-exclusively breastfed infants up to 4 months of age (Harari et al., 2012). As this is an observational study, we did not investigate specific mechanistic pathways of prenatal exposures to Pb or metal(loid) mixtures that may affect preadolescent glomerular function. Future toxicological work will aim to disentangle potential mechanisms and pathways.
Compared to the overall population, we observed a stonger association between metal(loid) mixtures and eGFR in children not exposed to ETS during pregnancy compared to exposed children. A similar phenomenon was oberserved in a study of NHANES participants which showed a stronger association between urinary Cd and periodontal disease among a low-tobacco-exposed group compared to the overall population (Arora et al., 2009). It may be that other factors associated with prenatal ETS obscure the relationship between the metal(loid)s studied here and kidney function.
Our study has many strengths. PROGRESS is an established prospective birth cohort with well-characterized demographic and covariate data, as well as simultaneous exposures. Dentine metal(loid) levels were measured blinded to preadolescent eGFR, and therefore cannot be biased with respect to eGFR assessment. We assessed 5 prioritized nephrotoxicant metal(loid)s using the tooth-based biomarker at weekly intervals beginning in the second trimester through roughly ~9 months after birth. The tooth-metals biomarker has been validated against other biomarkers and environmental measures collected at specific time points (Arora et al., 2012, 2014; Arora and Hare, 2015; Austin et al., 2013, 2017). Teeth are one of the few matrices that provide fine scale, repeated measures of fetal metal uptake. While prior studies largely relied on maternal blood and urine metals assessment, these maternal matrices may not be an accurate proxy for fetal exposure due to placental regulation of many environmental chemicals, and repeated measures are not be feasible in short time frames such as every week. The weekly tooth measures enable the identification of critical windows of susceptibility, which could otherwise be masked when using blood or urine matrices that are collected only once and over a wide time frame. The identification of critical windows can provide insight into the possible mechanisms of action and targets for preventative measures.
We applied two common eGFR estimating equations that included separately cystatin C- and serum creatinine-based formulae for children. Historically, decrements in kidney function have been historically assessed by clinically used serum creatinine-based equations yet, changes in serum creatinine may not become clinically appearant until substantial kidney impairment or nephron loss is present. The cystatin C univariate equation for children has advantages over other estimating equations for children as it may have less delayed sensitivity to kidney damage (Gerchman et al., 2009). As eGFR was assessed at preadolescence (with an average age of 9 years), we did not account for maturation status. Future studies should assess kidney parameter trajectories through the adolescent and pubertal period.
Our study had limitations. The metanephric kidney begins forming around 4 weeks of gestation, and tooth development begins forming after the first trimester therefore we cannot determine associations with first trimester exposures using this biomarker. While studies that combine additional media such as blood or urine measures in the first trimester may be informative, we also recognize the importance of the 2nd and 3rd trimester windows for kidney development. Some metal (loid)s (e.g. Cd and As) were generally not above detection limits in this study. The deposition of metal(loid)s is unequal across all matrices and it is possible the null findings observed may be due to low detection levels in teeth rather than lack of a true association. Urine As and Cd, along with blood Pb remain the gold standard biomarkers for assessment, yet collection of weekly or monthly samples to achieve a similar temporal resolution as reported herein is cost-prohibitive in large population-based studies and few participants woud likely agree to the burden-some protocol. By focusing our study in the PROGRESS cohort, based in Mexico City, we reduced confounding due to sociodemographic factors, however, this may limit generalizability to other populations. Compared to the overall cohort, participants that donated a tooth were more likely to be overweight, obese and of ‘middle’ SES. While models were adjusted for these variables, it is possible that individuals who did not contribute teeth, which were more likely to be lower SES, may have had different exposure profiles, including higher exposures to Pb (Whitehead and Buchanan, 2019). Exclusion of these individuals may have biased our results towards the null. We used BMI z-score categorized according to WHO guidelines and note that these rounded z-score cutoffs may introduce misclassification (Anderson et al., 2017). We assessed eGFR at a single time point in preadolescence. Further work investigating eGFR trajectories with longitudinal measures through the peripubertal period will be important to understanding the implications of these findings for later life risk of hypertension and kidney disease.
5. Conclusion
Identification of intervenable early life risk factors – such as dietary metal(loid) exposures and prenatal tobacco smoke exposure status – for CKD and hypertension could hold important potential in clinical and public health practice.
Supplementary Material
Acknowledgments
This work was supported in part by funding from the NIH: K99ES027508, R00ES027508, R00HD087523, R24ES028522, P30ES023515, R01ES013744, R01ES014930, R01ES026033, R35ES030435 and R01ES021357. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Appendix A. Supplementary material
Supplementary data to this article can be found online at https://doi.org/10.1016/j.envint.2022.107361.
References
- Aggarwal N, Porter AC, Tang IYS, Becker BN, Akkina SK, 2012. Creatinine-based estimations of kidney function are unreliable in obese kidney donors. J. Transplant 2012, 1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson LN, Carsley S, Lebovic G, Borkhoff CM, Maguire JL, Parkin PC, Birken CS, 2017. Misclassification of child body mass index from cut-points defined by rounded percentiles instead of Z-scores. BMC Res. Notes 10 (1). 10.1186/s13104-017-2983-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anke M, Schäfer U, Arnhold W In: Caballero B (Ed.), Encyclopedia of Food Sciences and Nutrition, second ed. Academic Press, Oxford, 2003, pp. 3589–3593. [Google Scholar]
- Arora M, Austin C, 2013. Teeth as a biomarker of past chemical exposure. Curr. Opin. Pediatr 25, 261–267. [DOI] [PubMed] [Google Scholar]
- Arora M, Hare DJ, 2015. Tooth lead levels as an estimate of lead body burden in rats following pre- and neonatal exposure. RSC Adv. 5 (82), 67308–67314. [Google Scholar]
- Arora M, Weuve J, Schwartz J, Wright RO, 2009. Association of environmental cadmium exposure with periodontal disease in U.S. Adults. Environ. Health Perspectives 117 (5), 739–744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arora M, Bradman A, Austin C, Vedar M, Holland N, Eskenazi B, Smith DR, 2012. Determining fetal manganese exposure from mantle dentine of deciduous teeth. Environ. Sci. Technol 46 (9), 5118–5125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arora M, Austin C, Sarrafpour B, Hernández-Ávila M, Hu H, Wright RO, Tellez-Rojo MM, Meliker J, 2014. Determining prenatal, early childhood and cumulative long-term lead exposure using micro-spatial deciduous dentine levels. PLoS ONE 9 (5), e97805. 10.1371/journal.pone.0097805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arora M, Reichenberg A, Willfors C, Austin C, Gennings C, Berggren S, Lichtenstein P, Anckarsäter H, Tammimies K, Bölte S, 2017. Fetal and postnatal metal dysregulation in autism. Nat. Commun 8 (1) 10.1038/ncomms15493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Austin C, Smith TM, Bradman A, Hinde K, Joannes-Boyau R, Bishop D, Hare DJ, Doble P, Eskenazi B, Arora M, 2013. Barium distributions in teeth reveal early-life dietary transitions in primates. Nature 498 (7453), 216–219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Austin C, Richardson C, Smith D, Arora M, 2017. Tooth manganese as a biomarker of exposure and body burden in rats. Environ. Res 155, 373–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benz K, Amann K, 2010. Maternal nutrition, low nephron number and arterial hypertension in later life. BBA 1802 (12), 1309–1317. [DOI] [PubMed] [Google Scholar]
- Berkovitz B, Holland G, Moxham B, 2009. Oral Anatomy, Histology and Embryology, fourth ed. Elsevier, London. [Google Scholar]
- Braun JM, Wright RJ, Just AC, Power MC, Tamayo y Ortiz M, Schnaas L, Hu H, Wright RO, Tellez-Rojo MM, 2014. Relationships between lead biomarkers and diurnal salivary cortisol indices in pregnant women from Mexico City: a cross-sectional study. Environ. Health: Global Access Sci. Source 13 (1). 10.1186/1476-069X-13-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brenner BM, Garcia DL, Anderson S, 1988. Glomeruli and blood pressure. Less of one, more the other? Am. J. Hypertens 1, 335–347. [DOI] [PubMed] [Google Scholar]
- Cárdenas-González M, Osorio-Yáñez C, Gaspar-Ramírez O, Pavković M, Ochoa-Martínez A, López-Ventura D, Medeiros M, Barbier OC, Pérez-Maldonado IN, Sabbisetti VS, Bonventre JV, Vaidya VS, 2016. Environmental exposure to arsenic and chromium in children is associated with kidney injury molecule-1. Environ. Res 150, 653–662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Claus Henn B, Austin C, Coull BA, Schnaas L, Gennings C, Horton MK, Hernández-Ávila M, Hu H, Téllez-Rojo MM, Wright RO, Arora M, 2018. Uncovering neurodevelopmental windows of susceptibility to manganese exposure using dentine microspatial analyses. Environ. Res 161, 588–598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Onis M, Lobstein T, 2010. Defining obesity risk status in the general childhood population: which cut-offs should we use? Int. J. Pediatr. Obes 5, 458–460. [DOI] [PubMed] [Google Scholar]
- Dean MC, Spiers KM, Garrevoet J, Le Cabec A, 2019. Synchrotron X-ray fluorescence mapping of Ca, Sr and Zn at the neonatal line in human deciduous teeth reflects changing perinatal physiology. Arch. Oral Biol 104, 90–102. [DOI] [PubMed] [Google Scholar]
- Delanaye P, Jager KJ, Bökenkamp A, Christensson A, Dubourg L, Eriksen BO, Gaillard F, Gambaro G, van der Giet M, Glassock RJ, Indridason OS, van Londen M, Mariat C, Melsom T, Moranne O, Nordin G, Palsson R, Pottel H, Rule AD, Schaeffner E, Taal MW, White C, Grubb A, van den Brand JAJG, 2019. CKD: a call for an age-adapted definition. J. Am. Soc. Nephrol.: JASN 30 (10), 1785–1805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fadrowski JJ, Navas-Acien A, Tellez-Plaza M, Guallar E, Weaver VM, Furth SL, 2010. Blood lead level and kidney function in US adolescents: the third national health and nutrition examination survey. Arch. Intern. Med 170, 75–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gennings C, Curtin P, Bello G, Wright R, Arora M, Austin C, 2020. Lagged WQS regression for mixtures with many components. Environ. Res 186, 109529. 10.1016/j.envres.2020.109529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gerchman F, Tong J, Utzschneider KM, Zraika S, Udayasankar J, McNeely MJ, Carr DB, Leonetti DL, Young BA, de Boer IH, Boyko EJ, Fujimoto WY, Kahn SE, 2009. Body mass index is associated with increased creatinine clearance by a mechanism independent of body fat distribution. J. Clin. Endocrinol. Metab 94 (10), 3781–3788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goyer RA, 1993. Lead toxicity: current concerns. Environ. Health Perspect 100, 177–187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gubhaju L, Sutherland MR, Horne RSC, Medhurst A, Kent AL, Ramsden A, Moore L, Singh G, Hoy WE, Black MJ, 2014. Assessment of renal functional maturation and injury in preterm neonates during the first month of life. Am. J. Physiol. Renal Physiol 307 (2), F149–F158. [DOI] [PubMed] [Google Scholar]
- Gurusinghe S, Tambay A, Sethna CB, 2017. Developmental origins and nephron endowment in hypertension. Front. Pediatr 5, 151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harari F, Ronco AM, Concha G, Llanos M, Grandér M, Castro F, Palm B, Nermell B, Vahter M, 2012. Early-life exposure to lithium and boron from drinking water. Reprod. Toxicol 34 (4), 552–560. [DOI] [PubMed] [Google Scholar]
- Hare D, Austin C, Doble P, Arora M, 2011. Elemental bio-imaging of trace elements in teeth using laser ablation-inductively coupled plasma-mass spectrometry. J. Dent 39 (5), 397–403. [DOI] [PubMed] [Google Scholar]
- Hinchliffe SA, Sargent PH, Howard CV, Chan YF, van Velzen D, 1991. Human intrauterine renal growth expressed in absolute number of glomeruli assessed by the disector method and Cavalieri principle. Lab. Invest 64, 777–784. [PubMed] [Google Scholar]
- Horton MK, Hsu L, Claus Henn B, Margolis A, Austin C, Svensson K, Schnaas L, Gennings C, Hu H, Wright R, Rojo MMT, Arora M, 2018. Dentine biomarkers of prenatal and early childhood exposure to manganese, zinc and lead and childhood behavior. Environ. Int 121, 148–158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughson M, Farris AB, Douglas-Denton R, Hoy WE, Bertram JF, 2003. Glomerular number and size in autopsy kidneys: the relationship to birth weight. Kidney Int 63 (6), 2113–2122. [DOI] [PubMed] [Google Scholar]
- Ingelfinger JR, 2008. Disparities in renal endowment: causes and consequences. Adv. Chronic Kidney Dis 15 (2), 107–114. [DOI] [PubMed] [Google Scholar]
- Kessing LV, Gerds TA, Feldt-Rasmussen B.o., Andersen PK, Licht RW, 2015. Use of lithium and anticonvulsants and the rate of chronic kidney disease: a nationwide population-based study. JAMA Psychiatry 72 (12), 1182. 10.1001/jamapsychiatry.2015.1834. [DOI] [PubMed] [Google Scholar]
- Kupsco A, Kioumourtzoglou M-A, Just AC, Amarasiriwardena C, Estrada-Gutierrez G, Cantoral A, Sanders AP, Braun JM, Svensson K, Brennan KJM, Oken E, Wright RO, Baccarelli AA, Téllez-Rojo MM, 2019. Prenatal metal concentrations and childhood cardiometabolic risk using bayesian kernel machine regression to assess mixture and interaction effects. Epidemiology 30 (2), 263–273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landrigan PJ, Kimmel CA, Correa A, Eskenazi B, 2004. Children’s health and the environment: public health issues and challenges for risk assessment. Environ. Health Perspect 112 (2), 257–265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee J, Oh S, Kang H, Kim S, Lee G, Li L, Kim CT, An JN, Oh YK, Lim CS, Kim DK, Kim YS, Choi K, Lee JP, 2020. Environment-wide association study of CKD. Clin. J. Am. Soc. Nephrol.: CJASN 15 (6), 766–775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindsey BD, Belitz K, Cravotta CA, Toccalino PL, Dubrovsky NM, 2021. Lithium in groundwater used for drinking-water supply in the United States. Sci Total Environ 767, 144691. 10.1016/j.scitotenv.2020.144691. [DOI] [PubMed] [Google Scholar]
- Luyckx VA, Brenner BM, 2020. Clinical consequences of developmental programming of low nephron number. Anat Rec (Hoboken) 303 (10), 2613–2631. [DOI] [PubMed] [Google Scholar]
- Müller W, Nava A, Evans D, Rossi PF, Alt KW, Bondioli L, 2019. Enamel mineralization and compositional time-resolution in human teeth evaluated via histologically-defined LA-ICPMS profiles. Geochim. Cosmochim. Acta 255, 105–126. [Google Scholar]
- Navas-Acien A et al. , 2009. Blood cadmium and lead and chronic kidney disease in US adults: a joint analysis. Am. J. Epidemiol 170, 1156–1164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ng DK, Schwartz GJ, Schneider MF, Furth SL, Warady BA, 2018. Combination of pediatric and adult formulas yield valid glomerular filtration rate estimates in young adults with a history of pediatric chronic kidney disease. Kidney Int 94 (1), 170–177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Padilla-Reyes DA, Núñez-Peña EP, Escalona-Alcázar F.d.J., Bluhm-Gutíerrez J, 2012. Calidad del agua del acuífero Guadalupe-Bañuelos, Estado de Zacatecas, México. GEOS 32. [Google Scholar]
- Pantic I, Tamayo-Ortiz M, Rosa-Parra A, Bautista-Arredondo L, Wright R, Peterson K, Schnaas L, Rothenberg S, Hu H, Téllez-Rojo M, 2018. Children’s blood lead concentrations from 1988 to 2015 in Mexico City: the contribution of lead in air and traditional lead-glazed ceramics. Int. J. Environ. Res. Public Health 15 (10), 2153. 10.3390/ijerph15102153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Puelles VG, Hoy WE, Hughson MD, Diouf B, Douglas-Denton RN, Bertram JF, 2011. Glomerular number and size variability and risk for kidney disease. Curr. Opin. Nephrol. Hypertens 20 (1), 7–15. [DOI] [PubMed] [Google Scholar]
- Rodríguez J, Mandalunis PM, 2018. A review of metal exposure and its effects on bone health. J. Toxicol 2018, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubio-Arias H, Quintana CE, Wood K, Saucedo RA, Bautista-Margulis R, 2007. Vanadium and lithium contamination in freshwaters of the conchos river in Chihuahua, Mexico. Environ. Health Risk IV 11. [Google Scholar]
- Sampogna RV, Schneider L, Al-Awqati Q, 2015. Developmental programming of branching morphogenesis in the kidney. J. Am. Soc. Nephrol.: JASN 26 (10), 2414–2422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanders AP, Burris HH, Just AC, Motta V, Svensson K, Mercado-Garcia A, Pantic I, Schwartz J, Tellez-Rojo MM, Wright RO, Baccarelli AA, 2015. microRNA expression in the cervix during pregnancy is associated with length of gestation. Epigenetics: Official J. DNA Methylation Soc 10 (3), 221–228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanders AP, Svensson K, Gennings C, Burris HH, Oken E, Amarasiriwardena C, Basnet P, Pizano-Zarate ML, Schnaas L, Tamayo-Ortiz M, Baccarelli AA, Satlin LM, Wright RO, Tellez-Rojo MM, 2018. Prenatal lead exposure modifies the effect of shorter gestation on increased blood pressure in children. Environ. Int 120, 464–471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saylor C, Malin AJ, Tamayo-Ortiz M, Cantoral A, Amarasiriwardena C, Estrada-Gutierrez G, Tolentino MC, Pantic I, Wright RO, Tellez-Rojo MM, Sanders AP, 2022. Early childhood fluoride exposure and preadolescent kidney function. Environ. Res 204, 112014. 10.1016/j.envres.2021.112014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL, 2009. New equations to estimate GFR in children with CKD. J. Am. Soc. Nephrol.: JASN 20 (3), 629–637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz GJ, Schneider MF, Maier PS, Moxey-Mims M, Dharnidharka VR, Warady BA, Furth SL, Muñoz A, 2012. Improved equations estimating GFR in children with chronic kidney disease using an immunonephelometric determination of cystatin C. Kidney Int 82 (4), 445–453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Solhaug MJ, Bolger PM, Jose PA, 2004. The developing kidney and environmental toxins. Pediatrics 113, 1084–1091. [PubMed] [Google Scholar]
- Tchounwou PB, Yedjou CG, Patlolla AK, Sutton DJ In: Luch A (Ed.), Molecular, Clinical and Environmental Toxicology: Volume 3: Environmental Toxicology. Springer Basel, Basel, pp. 133–164. [Google Scholar]
- Tsai T-L, Kuo C-C, Pan W-H, Chung Y-T, Chen C-Y, Wu T-N, Wang S-L, 2017. The decline in kidney function with chromium exposure is exacerbated with co-exposure to lead and cadmium. Kidney Int. 92 (3), 710–720. [DOI] [PubMed] [Google Scholar]
- Veille JC, McNeil S, Hanson R, Smith N, 1998. Renal hemodynamics: longitudinal study from the late fetal life to one year of age. J. Maternal-fetal Investigation: Official J. French Soc. Ultrasound Med. Biol … [et al. ] 8, 6–10. [PubMed] [Google Scholar]
- WHO Multicentre Growth Reference Study Group, 2006. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatrica 95, 76–85. [DOI] [PubMed] [Google Scholar]
- Wedeen RP, Qian LF, 1991. Chromium-induced kidney disease. Environ. Health Perspect 92, 71–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitehead LS, Buchanan SD, 2019. Childhood lead poisoning: a perpetual environmental justice issue? J. Public Health Manage. Practice 25, S115–S120. [DOI] [PubMed] [Google Scholar]
- Zheng LY, Sanders AP, Saland JM, Wright RO, Arora M, 2017. Environmental exposures and pediatric kidney function and disease: a systematic review. Environ. Res 158, 625–648. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.