

Abstract
Background and aims:
Immunogenicity with formation of anti-drug antibodies (ADA) to biologics is an important reason for treatment failure in inflammatory bowel disease (IBD). Our aim was to assess the rate of ADA, the effect of combination therapy with immunomodulators on ADA and the influence of ADA on efficacy and safety of biologics for IBD treatment.
Methods:
MEDLINE, Embase and Cochrane Central Register of Controlled Trials (CENTRAL) were searched from inception to April 2020 for trials of biologics that assessed immunogenicity. The overall certainty of evidence was evaluated using Grading of Recommendations, Assessment, Development and Evaluations (GRADE). The primary outcome was rate of ADA. Secondary outcomes included efficacy and safety outcomes among patients with detectable versus undetectable ADA. For dichotomous outcomes, pooled risk ratios (RR) and 95% confidence intervals (CI) were calculated.
Results:
Data from 68 studies were analysed and 33 studies (5850 patients) were included in the meta-analysis. Pooled ADA rates for biologic monotherapy were 28.0% for infliximab, 7.5% for adalimumab, 3.8% for golimumab, 10.9% for certolizumab, 6.2% for ustekinumab and 16.0% for natalizumab. Pooled ADA rates were 8.4% for vedolizumab and 5.0% for etrolizumab for combo- and monotherapy combined. In all biologics, ADA rates were underestimated by use of drug sensitive ADA assays and higher dose and/or frequency. ADA rate was significantly reduced in patients treated with combination therapy for infliximab (RR 0.52; 95% CI 0.44, 0.62), adalimumab (RR: 0.31; 95% CI 0.14, 0.69), golimumab (RR: 0.29; 95% CI 0.10, 0.83), certolizumab pegol (RR: 0.30; 95% CI 0.14, 0.67) and natalizumab (RR: 0.20; 95% CI 0.11, 0. 39). ADA to infliximab were associated with lower clinical response rates (RR: 0.75; 95% CI 0.61, 0.91) and higher rates of infusion reactions (RR: 2.36; 95% CI 1.85, 3.01).
Conclusions:
Differences in analytical methods to detect ADA hamper comparison of true ADA rates across biologics in IBD. Use of combination therapy with immunomodulators appeared to reduce ADA positivity for most biologics. For infliximab, ADA were associated with reduced drug efficacy and increased adverse events.
1. Introduction
Although biologics were first introduced for the treatment of inflammatory bowel disease (IBD) in the late nineties guidelines regarding their optimal use are still evolving. Over the last several decades IBD-related healthcare costs have increased significantly due to increased utilization of tumor necrosis factor-alpha (TNF-α) antagonists and other biologics [1, 2]. Accordingly, optimal use of biologics is necessary to enhance efficacy, reduce adverse effects and manage costs.
The TNF-α antagonists infliximab, adalimumab, golimumab and certolizumab pegol act by targeting and inhibiting TNF-α, a pro-inflammatory cytokine that has a central role in mucosal inflammation in IBD [3, 4]. Ustekinumab binds to the common p40 subunit of the pro-inflammatory cytokines interleukin (IL)-12 and IL-23 which are also known to play a role in the pathophysiology of IBD [5]. Natalizumab binds to the α4 subunit of the α4β1 and α4β7 integrin, thereby blocking the binding to respectively vascular cell adhesion molecule 1 (VCAM-1) and mucosal vascular addressin cell adhesion molecule 1 (MAdCAM-1) and inhibiting the migration of mononuclear leukocytes to different tissues, predominantly the gut and central nervous system [6]. Vedolizumab recognizes a conformational epitope of the heterodimer α4β7 which blocks binding to MAdCAM-1, thereby inhibiting the migration of gut-selective leukocytes [7]. Etrolizumab tartgets the β7 unit of the heterodimeric integrins α4β7 and αEβ7, thereby inhibiting migration of gut-selective leukocytes [8].
A major concern when treating patients with biologics is the development of anti-drug antibodies (ADA), since ADA are associated with lower serum drug concentrations, loss of response, and adverse effects such as infusion and injection site reactions [9–11]. Several strategies for prevention of ADAs formation have been investigated. Combination therapy comprised of a biologic with an immunomodulator prevents ADA formation [12, 13]. Higher anti-TNF dosing is associated with less ADA detection [14, 15]. Pre-treatment with hydrocortisone has also been shown to prevent ADA formation and infusion reactions; however, data supporting this strategy are limited [16]. There is also some evidence that a decline in ADA may be achieved by adding or switching immunomodulators [17, 18].
The incidence of immunogenicity varies considerably across studies and biologic agents. A critical factor related to this variability may be the sensitivity of the assay used to detect ADA [19, 20]. Qualitative terms are used to distinguish between drug ‘tolerant’ assays that are able to measure ADA in the presence of detectable drug concentrations, and drug ‘sensitive’ assays which are not. Drug tolerant assays are preferred for detecting ADA to assess the true ADA rate.
Strategies for optimal management of ADA formation are still evolving, and the exact influence of concomitant immunomodulator therapy on immunogenicity remains unclear. Therefore, the objectives of this systematic review were to determine the rate of ADA formation in patients on monotherapy or combination therapy, and the impact of ADA formation on the pharmacokinetics, efficacy and safety of biologics in patients with IBD.
2. Methods
This systematic review and meta-analysis was conducted using the methods described in the Cochrane Handbook of Systematic Reviews,[21] and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [22]. The review protocol was registered in the Cochrane Database of Systematic Reviews [23].
2.1. Eligibility criteria
Any trial of biologics that enrolled adult Crohn’s disease (CD) or ulcerative colitis (UC) patients (16 years or older) and assessed immunogenicity was eligible for inclusion. Interventions of interest included adalimumab, certolizumab pegol, golimumab, infliximab, natalizumab, vedolizumab, ustekinumab and etrolizumab administered alone or in combination with another agent (i.e. corticosteroids [including pre-medication], thiopurines, or methotrexate).
2.2. Comparisons and outcomes
The primary outcomes of interest were ADA formation and ADA concentration among patients treated with monotherapy compared to combination therapy. Secondary outcomes included drug serum concentration and rates of response (clinical, endoscopic or biochemical), remission (clinical, endoscopic or biochemical) and adverse events (including acute, delayed or injection site reactions) in patients with detectable versus undetectable ADA. Response and remission rates were pooled for analysis irrespective of the definition employed in the original study.
2.3. Search strategy
MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) were searched from inception to April 21, 2020 (Supplementary Appendix 1). No language or date restrictions were applied. The bibliographies of relevant articles and conference proceedings from Digestive Disease Week and United European Gastroenterology Week (2013 to 2020) were hand searched to identify additional studies.
2.4. Screening and data extraction
Two authors (SB and NVC) independently screened search results and extracted information on study design, participants, intervention, comparison, outcomes, and risk of bias using a standardized data collection form. Secondary outcome data were only collected if immunogenicity data were reported. Disagreements were resolved through discussion with a third author (JFB or CEP). For unclear or missing data, an attempt was made to contact the original study authors for clarification.
2.5. Risk of bias assessment
The Cochrane risk of bias tool was used to assess the methodological quality of randomized controlled trials (RCTs) [24]. The Newcastle-Ottawa Quality Assessment Scale (NOS) was used for quality assessment of the observational studies [25].
2.6. Heterogeneity
Heterogeneity was assessed using the Chi2 test (p ≤0.10 was considered statistically significant) and the I2 statistic.[26] I2 values of 0%, <50%, ≥50% and ≥75% were interpreted as indicating no, low, moderate and high heterogeneity, respectively [26].
2.7. Data synthesis and analysis
Data from individual trials were pooled for meta-analysis if the intervention(s), population, and outcomes were sufficiently similar (determined by consensus). Data were not pooled for analysis if there was a high degree of heterogeneity (I2 >75%).
For dichotomous outcomes, the risk ratio (RR) and corresponding 95% confidence interval (CI) were calculated. If outcome data were reported at multiple timepoints, the primary timepoint defined by the original study authors was used. A fixed-effect model was used to pool data, however, we planned to use a random-effects model in the case of significant, unexplained heterogeneity. Review Manager (RevMan 5.4; The Nordic Cochrane Centre for The Cochrane Collaboration, Copenhagen, Denmark) was used to perform data analysis according to the intention-to-treat principle.
2.8. Sensitivity and subgroup analyses
Sensitivity analyses were conducted to investigate potential sources of heterogeneity and assess the impact of removing low quality studies from the pooled analyses. Where possible, subgroup analyses were performed to assess the influence of the following factors on the overall RR estimate: study design (randomized versus observational; induction versus maintenance), patient population (CD versus UC versus IBD), combination therapy regimen (combination therapy versus monotherapy) and ADA assay type (drug sensitive versus drug tolerant).
2.9. Quality of the evidence
The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach was used to assess the overall certainty of the evidence. Results from RCTs were initially considered high-quality, but potentially downgraded due to risk of bias; indirectness of evidence; unexplained heterogeneity; publication bias or sparse data [27]. Observational data were initially considered low quality. Outcomes with less than 35 events were reduced by two GRADE levels; outcomes with less than 300 events were reduced by one GRADE level.
3. Results
3.1. Search results
The search identified 11881 records, from which 3368 duplicates were removed. Of the remaining 8513 records, 7994 were deemed ineligible based on title and abstract. Full-text review was required for 519 records, and 398 records were excluded. Most excluded studies did not report on ADA formation or had no control group. A total of 68 studies met the inclusion criteria (Figure 1). The included studies are described in Supplementary Table 1. ADA formation rates in each study are shown in Supplementary Table 2. Table 1 summarizes the main results and provides an overall assessment of the certainty of the evidence.
Figure 1:
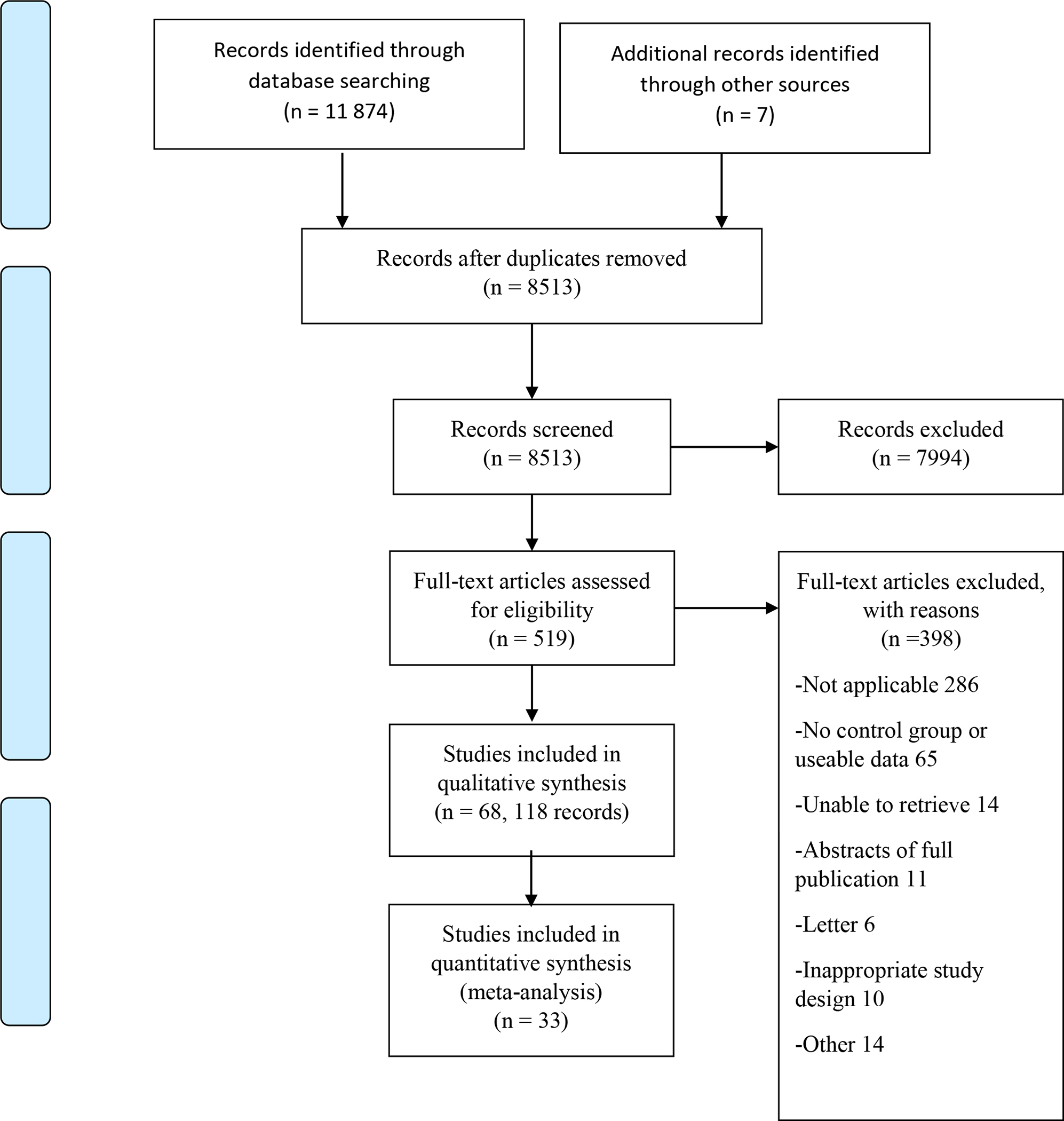
PRISMA Flow Diagram
Table 1:
Summary of findings
| Outcome | Studies (N) | Participants (N) | Risk of Bias | Inconsistency | Indirectness | Imprecision | Reporting bias | Pooled RR (95% CI, p) | Quality |
|---|---|---|---|---|---|---|---|---|---|
| Comparison: Infliximab combination therapy vs. infliximab monotherapy | |||||||||
| ADA formation (all studies) | 13 | 1825 | High | Low | No indirectness | 405 events | None | 0.52 (0.44, 0.62; p<0.001) | ⊕⊕⊕⊕ High |
| ADA formation (randomized to monotherapy or combination therapy) | 3 | 413 | Low | No | No indirectness | 40 events | None | 0.13 (0.05, 0.33; p<0.001) | ⊕⊕⊕⊝ Moderate1 |
| ADA formation (observational data) | 10 | 1412 | High | No | No indirectness | 365 events | None | 0.59 (0.49, 0.71; p<0.001) | ⊕⊕⊕⊕ High |
| ADA formation (induction treatment) | 3 | 352 | High | No | No indirectness | 197 events | None | 0.57 (0.47, 0.70; p<0.001) | ⊕⊕⊕⊝ Moderate1 |
| ADA formation (maintenance treatment) | 10 | 1473 | High | Moderate | No indirectness | 208 events | None | 0.47 (0.35, 0.63; p<0.001) | ⊕⊕⊕⊝ Moderate1 |
| ADA formation (CD patients) | 10 | 1471 | High | Low | No indirectness | 378 events | None | 0.52 (0.44, 0.62; p<0.001) | ⊕⊕⊕⊕ High |
| ADA formation (UC patients) | 1 | 68 | Low | Not applicable | Not applicable | 8 events | None | 0.12 (0.02, 0.92; p=0.04) | ⊕⊕⊝⊝ Low2 |
| ADA formation (IBD patients) | 2 | 286 | High | No | No indirectness | 19 events | None | 0.83 (0.34, 2.03; p=0.68) | ⊕⊕⊝⊝ Low2 |
| ADA formation (Thiopurines only) | 4 | 491 | High | Moderate | No indirectness | 108 events | None | 0.50 (0.37, 0.67; p<0.001) | ⊕⊕⊕⊝ Moderate1 |
| ADA formation (MTX only) | 2 | 235 | High | Moderate | No indirectness | 81 events | None | 0.51 (0.36. 0.72; p<0.001) | ⊕⊕⊕⊝ Moderate1 |
| ADA formation (Corticosteroids only) | 2 | 477 | Low | Low | No indirectness | 89 events | None | 0.80 (0.53, 1.22; p=0.30) | ⊕⊕⊕⊝ Moderate1 |
| ADA formation (Drug sensitive assays) | 11 | 1561 | High | Low | No indirectness | 342 events | None | 0.49 (0.41, 0.60; p<0.001) | ⊕⊕⊕⊕ High |
| ADA formation (Drug tolerant assays) | 2 | 264 | High | High | No indirectness | 63 events | None | 0.67 (0.44, 1.04; p=0.07) | ⊕⊕⊝⊝ Low3 |
| Comparison: Infliximab ADA positive vs ADA undetectable | |||||||||
| Clinical response | 7 | 1127 | High | No | No indirectness | 573 events | None | 0.75 (0.61, 0.91; p=0.004) | ⊕⊕⊕⊕ High |
| Infusion reactions | 5 | 1242 | Low | Moderate | No indirectness | 230 events | None | 2.36 (1.85, 3.01; p<0.001) | ⊕⊕⊕⊝ Moderate1 |
| Comparison: Adalimumab combination therapy vs. adalimumab monotherapy | |||||||||
| ADA formation (all data) | 5 | 698 | Low | No | No indirectness | 38 events | None | 0.34 (0.16, 0.75; p=0.007) | ⊕⊕⊕⊝ Moderate1 |
| ADA formation (maintenance treatment) | 4 | 539 | Low | No | No indirectness | 38 events | None | 0.31 (0.14, 0.69; p=0.004) | ⊕⊕⊕⊝ Moderate1 |
| Comparison: Golimumab combination therapy vs. golimumab monotherapy | |||||||||
| ADA formation | 1 | 1103 | Low | Not applicable | Not applicable | 32 events | None | 0.29 (0.10, 0.83; p=0.02) | ⊕⊕⊕⊝ Moderate |
| Comparison: Golimumab ADA positive vs ADA undetectable | |||||||||
| Clinical response (week 6) | 1 | 720 | Low | Not applicable | Not applicable | 374 events | None | 1.26 (0.91, 1.75; p=0.17) | ⊕⊕⊕⊕ High |
| Clinical response (week 54) | 1 | 263 | Low | Not applicable | Not applicable | 146 events | None | 0.51 (0.16, 1.65; p=0.26) | ⊕⊕⊕⊝ Moderate1 |
| Clinical remission (week 6) | 1 | 720 | Low | Not applicable | Not applicable | 135 events | None | 1.35 (0.62, 2.92; p=0.45) | ⊕⊕⊕⊝ Moderate1 |
| Clinical remission (week 54) | 1 | 263 | Low | Not applicable | Not applicable | 77 events | None | 0.48 (0.08, 2.98; p=0.43) | ⊕⊕⊕⊝ Moderate1 |
| Mucosal healing (week 6) | 1 | 720 | Low | Not applicable | Not applicable | 316 events | None | 1.26 (0.84, 1.89; p=0.26) | ⊕⊕⊕⊕ High |
| Mucosal healing (week 54) | 1 | 263 | Low | Not applicable | Not applicable | 127 events | None | 0.59 (0.18, 1.90; p=0.37) | ⊕⊕⊕⊝ Moderate1 |
| Comparison: Certolizumab pegol combination therapy vs. certolizumab pegol monotherapy | |||||||||
| ADA formation (all data) | 2 | 1139 | Low | Low | No indirectness | 43 events | None | 0.30 (0.14, 0.67; p=0.003) | ⊕⊕⊕⊝ Moderate1 |
| Comparison: Ustekinumab combination therapy vs. ustekinumab monotherapy | |||||||||
| ADA formation (all data) | 2 | 917 | Low | Low | No indirectness | 50 events | None | 0.59 (0.30, 1.18; p<0.13) | ⊕⊕⊕⊝ Moderate1 |
| Comparison: Natalizumab combination therapy vs. natalizumab monotherapy | |||||||||
| ADA formation (all data) | 3 | 763 | Low | No | No indirectness | 70 events | None | 0.17 (0.08, 0.38; p<0.001) | ⊕⊕⊕⊝ Moderate1 |
Downgraded 1 level due to sparse data
Downgraded 2 levels due to sparse data
Downgraded 2 levels due to sparse data & high heterogeneity
ADA: anti-drug antibodies; IBD: inflammatory bowel disease; CD: Crohn’s disease; UC: ulcerative colitis; MTX: methotrexate.
3.2. Risk of bias assessment
The risk of bias assessments are reported in Supplementary Tables 3 and 4. The RCTs scored low or unclear risk of bias for most domains. One study was rated as high risk of bias with respect to attrition bias, and seven studies were rated as high risk of bias with respect to blinding. For the observational studies, one study was deemed to be at high risk of bias (NOS *score 6), and 13 studies were deemed to be at low risk of bias (*range 7–9).
3.3. Infliximab
The search identified 26 eligible studies for infliximab, 5 of which were RCTs and 21 were observational. Thirteen studies allowed us to evaluate combination therapy to monotherapy. Eleven studies allowed us to evaluate ADA-positive to ADA-negative or ADA-undetectable patients. Seventeen studies included patients with CD, six studies included patients with UC, and two studies included IBD patients (Supplementary Table 1).
3.3.1. ADA formation
Thirteen studies allowed us to evaluate ADA formation rates among patients treated with infliximab monotherapy versus combination therapy with an immunomodulator (supplementary table 1). Follow-up ranged between 12 weeks and 36 months (median). ADA development occurred in 15.8% (136/863) of patients on combination therapy compared to 28.0% (269/962) of patients on monotherapy. The pooled RR was 0.52 (95% CI 0.44, 0.62, 13 studies, p<0.001; GRADE high; Figure 2.1.1) with low heterogeneity (I2=40%, p=0.07).
Figure 2:
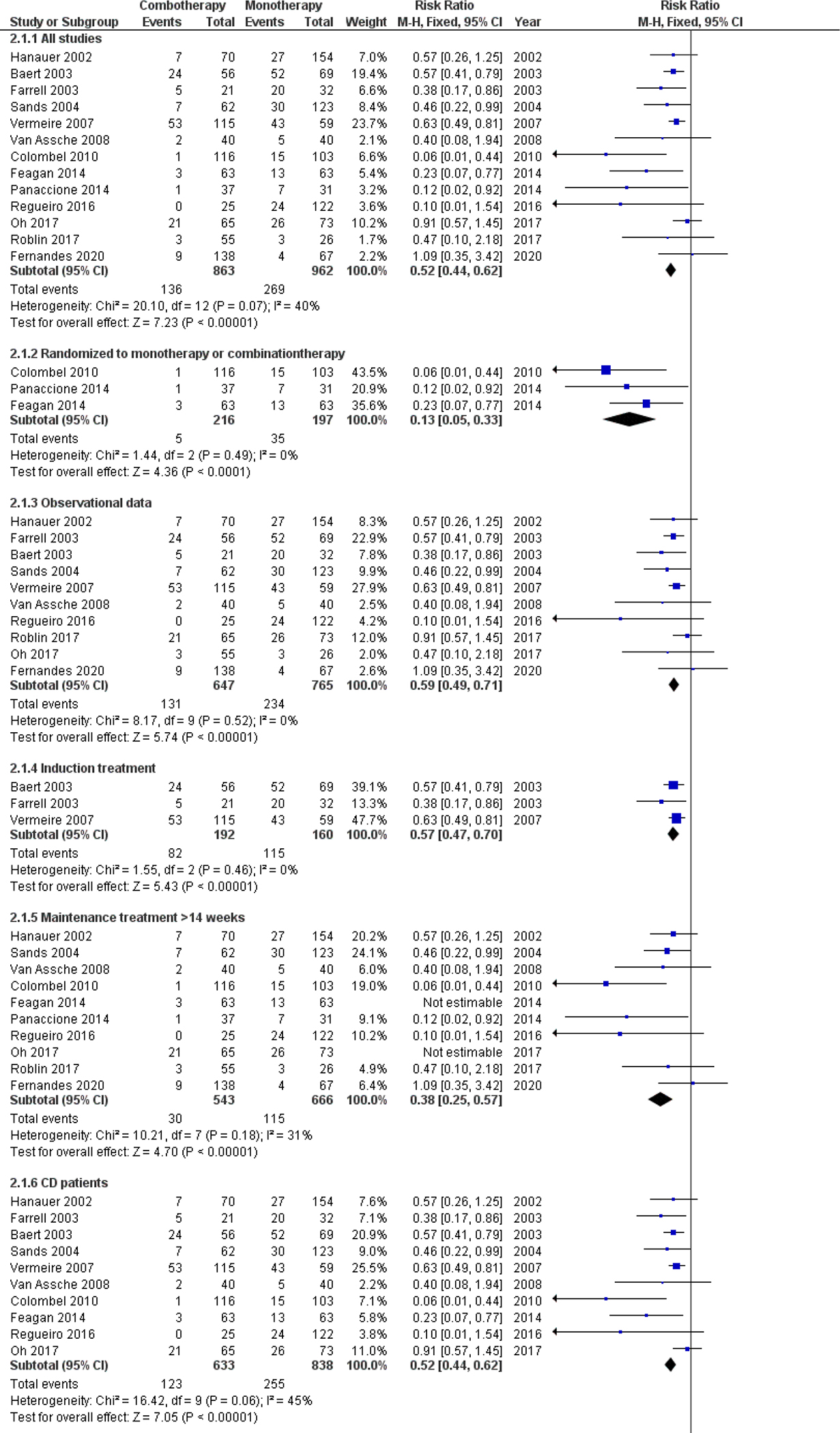
ADA formation in infliximab combo- versus monotherapy.
IBD: inflammatory bowel disease; CD: Crohn’s disease; UC: ulcerative colitis; MTX: methotrexate.
The pooled RR for RCT studies was 0.13 (95% CI 0.05, 0.33, 3 studies, p<0.001, GRADE moderate; Figure 2.1.2) with no heterogeneity detected (I2= 0%, p=0.49). The pooled RR for observational studies was 0.59 (95% CI 0.49, 0.71, 10 studies, p<0.001, GRADE high; Figure 2.1.3). The RR estimates continued to demonstrate a statistically significant effect in favour of combination therapy when data were pooled based on study design (induction versus maintenance [Figures 2.1.4 and 2.1.5] and CD versus UC [Figures 2.1.6 and 2.1.7], with between-study heterogeneity remaining low. The RR estimate did not show a statistically significant effect in the mixed population (Figure 2.1.8).
ADA formation resulting from infliximab combination therapy with azathioprine was evaluated in four studies. The pooled RR was 0.50 (95% CI 0.37, 0.67, p<0.001, GRADE moderate; Figure 2.1.9). The between study heterogeneity was moderate (I2=74%). When removing the study by Vermeire et al. (a study on episodic infliximab treatment) from the analysis, the pooled RR was 0.15 (95% CI 0.05, 0.41; p<0.001, GRADE moderate; Supplementary Figure 1).
Two studies compared the presence of ADA formation among patients treated with infliximab monotherapy relative to infliximab in combination with methotrexate (Figure 2.1.10) with a pooled RR of 0.51 (95% CI 0.36, 0.72, p<0.001; GRADE moderate). The between-study heterogeneity was moderate (I2=61%).
Two studies explored the effect of combined infliximab and corticosteroid therapy on ADA formation, without the use of concomitant immunomodulators (Figure 2.1.11). Sixteen percent (32/200) of patients on combination therapy developed ADAs, compared to 21% (57/277) of patients on monotherapy. This effect was not statistically significant (RR 0.80, 95% CI 0.53, 1.22, p=0.30; GRADE moderate), and the between-study heterogeneity was low (I2 = 33%).
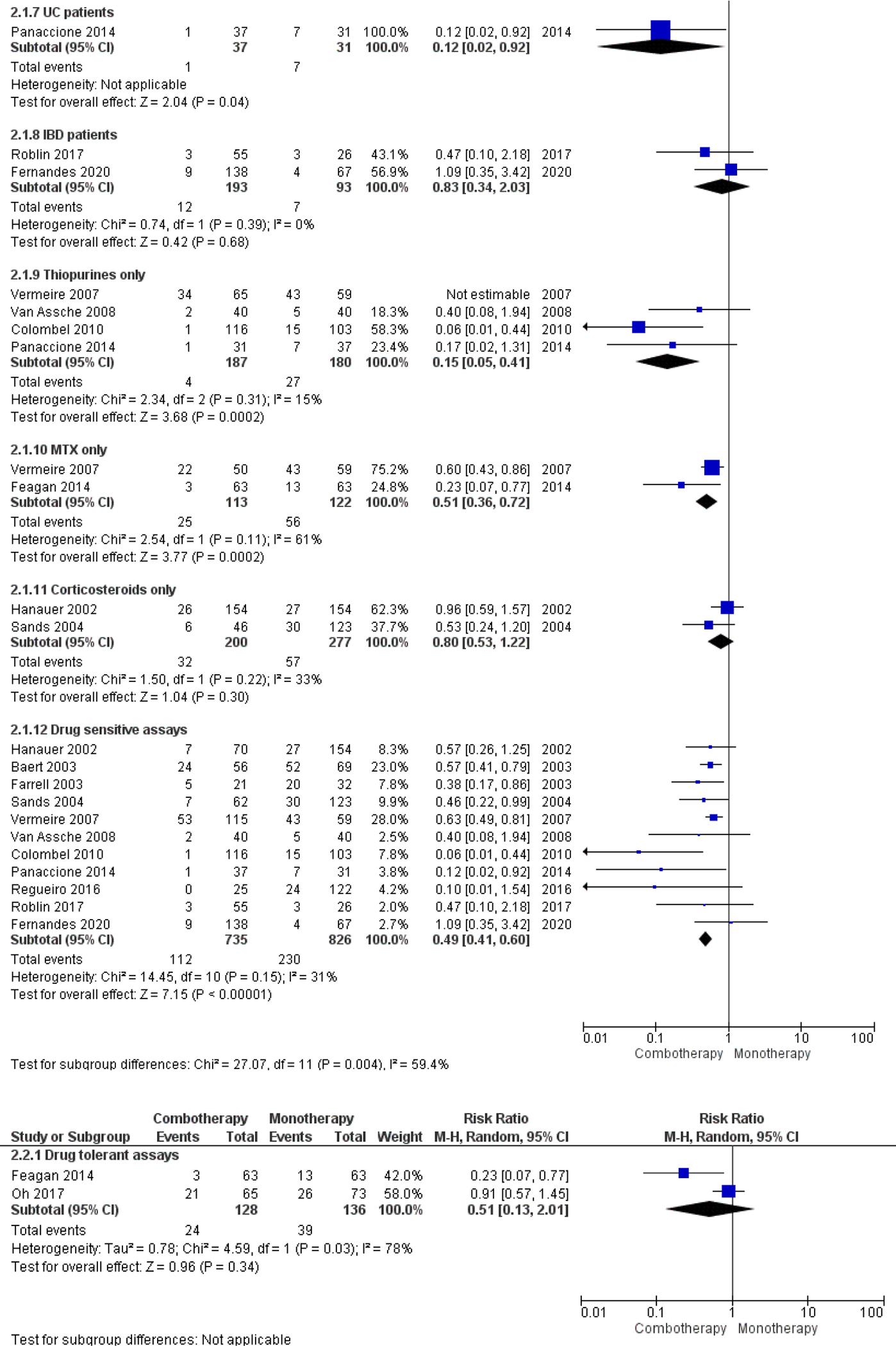
The pooled RR for studies that used a drug sensitive assay was 0.49 (95% CI 0.41, 0.60, 11 studies, p<0.001; GRADE high), and the between study heterogeneity was low (I2 = 31%) (Figure 2.1.12). For two studies that used a drug tolerant assay, ADA development occurred in 19% (24/128) of patients receiving combination therapy versus 29% (39/136) of patients receiving monotherapy. The pooled RR was 0.51 (95% CI 0.13–2.01; p=0.34 GRADE low) and the between-study heterogeneity was high (I2 = 78%) (Figure 2.2). When removing Oh et al. (a prospective observational study) from the analysis, the RR was 0.23 (95% CI 0.07, 0.77; p=0.02, GRADE low; Supplementary Figure 2).
3.3.2. ADA concentration
Four infliximab studies reported ADA concentrations. We did not combine quantitative data for analysis due to the heterogeneous units of measurement used to define ADA concentrations and heterogeneity in statistical reporting.
For the Baert et al. study, the median ADA concentration was higher in patients receiving monotherapy relative to combination therapy [9]. The median concentration of ADAs to infliximab was 13.8 μg/ml (95% CI 7.9–16.2) among patients with luminal disease receiving monotherapy therapy, compared to 1.3 μg/ml (95% CI 0.6–3.2) among patients with luminal disease receiving combination therapy. In patients with fistulizing disease receiving monotherapy, the median concentration of ADAs to IFX was 21.4 μg/ml (95% CI 13.2–24.5) compared to 1.5 μg/ml (95% CI 0.4–8.8) among patients with fistulizing disease receiving combination therapy.
In a study by Farrell et al., ADA concentrations were lower in patients pretreated with hydrocortisone compared to placebo (median 2.9 versus 11.1 μg/ml at week 8 and 1.6 versus 3.4 μg/ml at week 16) [16].
Among 96 patients who developed ADA to infliximab, Vermeire et al. reported 27 (28%), 30 (31%) and 39 (41%) patients with ADA concentrations of below 8, above 8 or above 20 μg/ml respectively [28].
Using a drug tolerant assay, Oh et al. showed a lower median ADA concentration of 8.064 AU/mL (IQR 6.929–9.908) in patients in remission compared to 11.209 AU/mL (IQR 8.008–118.835) in patients with active disease [29].
3.3.3. Serum drug concentrations
Five infliximab studies compared serum drug concentrations among ADA-positive and ADA-negative patients. We did not combine data for analysis due the heterogeneous cut-off values used to define ADA-positive and ADA-negative patients. A post-hoc analysis of the ACT-1 and ACT-2 trials showed that patients with ADA formation had a higher likelihood of low drug serum concentrations (p<0.001) [30, 31]. Seow et al. showed that of 66/108 patients with undetectable drum serum concentrations, 44 (66.7%) were ADA-positive and 22 (33.3%) were ADA negative [32]. Vermeire et al. showed lower median concentrations of 7.55 μg/mL (IQR2.65–13.73) after 1 infusion of infliximab in patients who later became ADA-positive, compared with median drug serum concentrations of 11.15 μg/mL [IQR 5.98–18.98] in patients who remained ADA-negative [28]. Oh et al. reported median trough levels of 0.141 μg/mL (IQR 0.002–0.869) in ADA-positive patients versus median trough levels of 1.415 μg/mL (IQR 0.570–2.495) in ADA-negative patients, using a drug tolerant assay [29]. Van Stappen et al. reported an inverse correlation between ADA concentration, as measured with a drug ‘tolerant’ assay, and infliximab trough concentrations in a posthoc analysis of the TAXIT trial [33]. Patients in the highest quadrant of ADA concentrations had lower trough concentrations when compared to the two lowest quadrants and ADA-negative patients (p<0.001). Median trough concentrations were lower in ADA-positive patients when using a drug tolerant and a drug sensitive assay (0.0, IQR 0.0–0.0 μg/ml) compared with ADA-negative patients (1.8, IQR 1.4–2.4 μg/ml) (p<0.001) and patients who were ADA-positive with a drug tolerant assay only (1.7, IQR 0.7–2.3, p<0.001). There was no difference in trough concentration between ADA-negative patients and patients who were ADA-positive with a drug tolerant assay only (p=1.0). Indicating that low concentration ADA that are undetectable at trough using a drug ‘sensitive’ assay may be pharmacologically less relevant.
3.3.4. Clinical outcomes
A lower overall clinical response to infliximab rate was observed in ADA-positive compared with ADA-undetectable patients (RR 0.75, 95% CI 0.61, 0.91, p=0.004, 7 studies, GRADE high; Figure 3). The heterogeneity was low for this comparison (I2= 0%, p=0.51).
Figure 3:
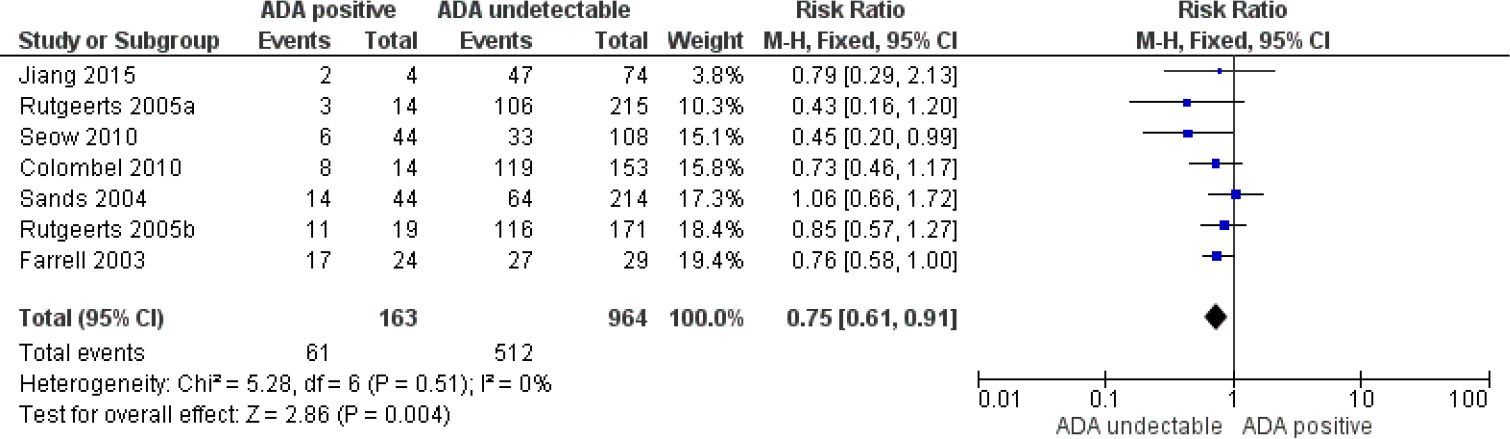
Clinical response to infliximab in patients with positive versus undetectable ADA.
3.3.5. Endoscopic outcomes
Two infliximab studies reported on endoscopic outcomes in relation to ADA status. Data were not pooled due to high heterogeneity. Seow et al. showed no difference in endoscopic improvement between ADA-positive and ADA-undetectable patients (25% vs 35%; p=0.61). However, detectable infliximab serum drug concentrations were associated with endoscopic improvement (76% vs 28%; P<0.001) [32]. Reguiero et al. observed a higher endoscopic recurrence rate after ileocecal resection in ADA positive (64.7%, 11/17) vs ADA negative (46.7%, 7/15) or ADA inconclusive (30.1%, 22/73) patients [34].
3.3.6. Biochemical outcomes
No infliximab studies reported on the relationship between biochemical disease activity and ADA formation.
3.3.7. Adverse events
Infliximab infusion reactions occurred in 65/175 (37.1%) of ADA-positive patients versus 165/1067 (15.5%) ADA-undetectable patients (RR 2.36, 95% CI 1.85, 3.01, p<0.001, 5 studies, GRADE moderate; Figure 4). Moderate heterogeneity was detected (I2= 59%, p=0.04).
Figure 4:
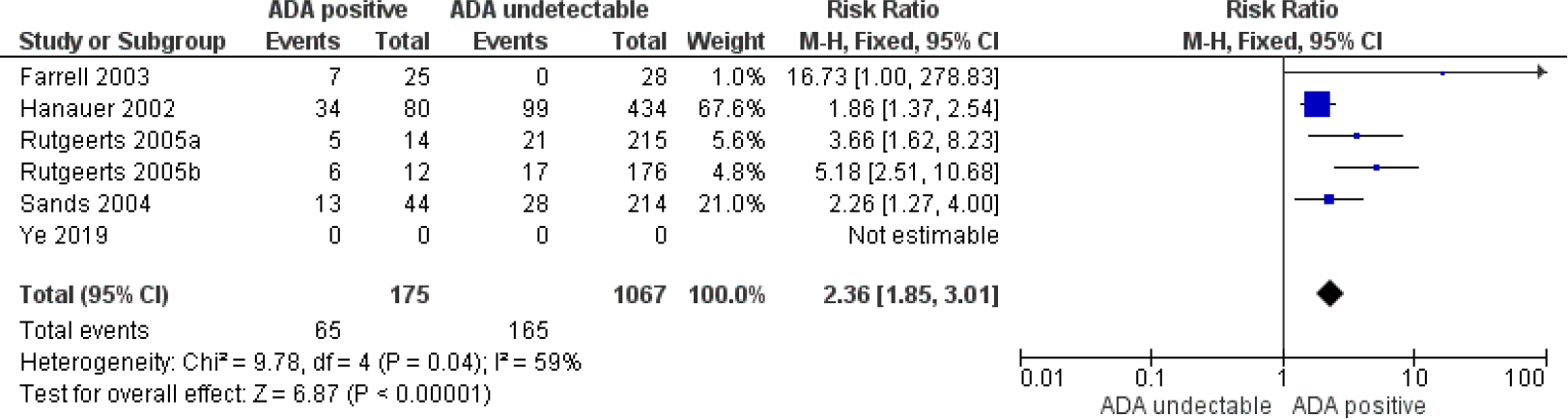
Infusions reactions in infliximab treated patients with positive versus undetectable ADA.
One study reported significantly higher median ADA titers in patients with infusion reactions compared to those without (20.1 vs 3.2 μg/ml) [9]. Concentrations of 8 μg/ml or higher predicted a higher risk of infusion reactions (RR 2.40; 95% CI 1.65, 3.66; P<0.001). A single study by Ye et al. reported that 2/2 patients that had an infusion reaction at week 30 were ADA positive. In total, 19/220 infusion reactions were reported but ADA formation was not reported in these cases [35].
3.3.8. Antibody assays
In four infliximab studies, a drug-tolerant assay was used for the assessment of ADA formation. In these studies, the reported ADA formation rates were 47/138 (34.1%), 16/126 (12.7%), 21/122 (17.2%) and 13/42 (31%), respectively.
3.4. Adalimumab
The search identified 10 RCTs of adalimumab treatment that met the eligibility criteria. Seven studies reported data on combination therapy. One study randomized patients to receive adalimumab in combination with immunomodulators or as monotherapy. No studies compared ADA-positive to ADA-negative patients. The majority of studies included patients with CD and two studies included patients with UC (Supplementary Table 1).
3.4.1. ADA formation
ADA formation occurred in 2.2% (6/273) of patients receiving adalimumab combination therapy compared to 7.5% (32/425) of patients treated with monotherapy. The pooled RR was 0.31 (95% CI 0.14, 0.69, 5 studies, p=0.004, GRADE moderate; Figure 5.1.1). No heterogeneity was detected (I2 = 0%, P=0.82). The RR estimate continued to demonstrate a statistically significant protective effect in favour of combination therapy when data were pooled based on study design (maintenance treatment; Figure 5.1.2). Data on the influence of methotrexate, thiopurines or corticosteroids were unavailable.
Figure 5:
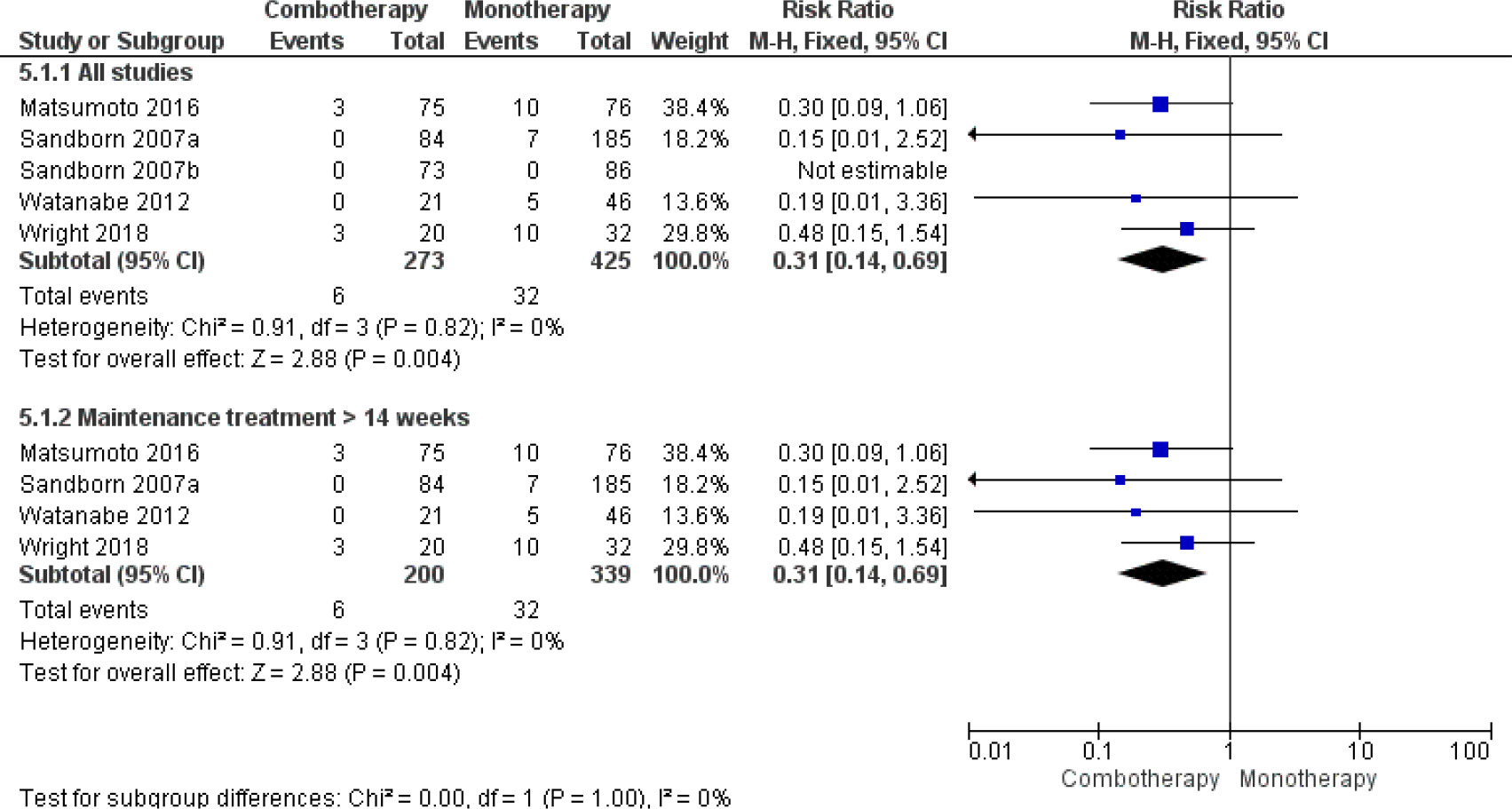
ADA formation in adalimumab combo- versus monotherapy.
3.4.2. Other outcomes
Data on the impact of ADA formation on clinical, biochemical and endoscopic outcomes or serum drug concentrations and adverse events were not available.
3.5. Infliximab and adalimumab
One study by Roblin et al. showed increased incidence of ADA development and undetectable drug concentrations in the monotherapy group after switching TNF antagonist therapy (i.e. from infliximab to adalimumab or from adalimumab to infliximab) because of clinical failure and immunogenicity [36]. Starting the subsequent biologic with combination therapy significantly reduced ADA development and the incidence of undetectable drug concentrations (adalimumab and azathioprine: Hazard ratio [HR] 0.12; 95% CI 0.03, 0.40; p<0.001; infliximab and azathioprine: HR 0.16 95%; CI 0.06, 0.37; p<0.001). This effect was consistent only for infliximab and not for adalimumab when ADA were measured using a drug tolerant assay (adalimumab and azathioprine: HR 0.61; 95% CI 0.30, 1.24; p=0.17; and infliximab and azathioprine: HR 0.18; 95% CI 0.08, 0.41).
3.6. Golimumab
The search yielded three RCTs of golimumab treatment that met the eligibility criteria. None of the studies randomized patients to monotherapy or combination therapy. No studies compared ADA-positive to ADA-negative patients. All three studies analyzed UC patients (Supplementary Table 1).
3.6.1. ADA formation
Sandborn et al. reported data on the protective effect of combination therapy on ADA formation [37, 38]. ADA formation occurred in 1.1% (4/362) of patients on combination therapy compared to 3.8% (28/741) of patients on monotherapy. The calculated RR was 0.29 (95% CI 0.10, 0.83; p=0.02; GRADE moderate) (Supplementary Figure 3). A post-hoc analysis of PURSUIT-SC, PURSUIT-M and PURSUIT-IV showed much higher ADA detection when using a drug tolerant assay (21.8% versus 2.8%). ADA rates were higher in patients in the PURSUIT-M study who were randomized to placebo after induction treatment (31.6% versus 20.2%). ADA rates were lower in patients receiving immunomodulators (11.8% versus 26.9%; p<0.001) and ADA rates were lower in patients receiving golimumab monotherapy doses of 100mg versus 50mg (22.4% versus 37.1%; p-value unavailable). Additionally, ADA-positive patients with a drug-tolerant assay had lower ADA titers as opposed to ADA-positive patients with a drug-sensitive assay. Trough serum golimumab concentrations were lower in ADA-positive patients 0.51 vs 0.85 μg/mL [50 mg q4w]; 0.85 vs 1.60 μg/mL [100 mg q4w]).
3.6.2. Other outcomes
A post-hoc analysis of Sandborn et al. reported clinical and endoscopic outcomes in relation to ADA status at weeks 6 and 54 and no significant associations were found [39]. However, in the post-hoc analysis by Adedokun et al., clinical response rates were lower at week 54 in ADA-positive versus ADA-negative patients when using a drug-tolerant assay (38.1% versus 52.8%; p=0.047). ADA-formation did not have an impact on injection site reactions. Other data on the effect of ADA formation on biochemical outcomes or adverse events were not available.
3.7. Certolizumab pegol
The search yielded six RCTs that evaluated treatment with certolizumab pegol that met the eligibility criteria. None of the studies randomized patients to monotherapy or combination therapy. Two studies compared ADA-positive to ADA-negative patients. All studies analyzed CD patients (Supplementary Table 1).
3.7.1. ADA formation
Three certolizumab pegol studies provided data on the effect of combination therapy on ADA formation, of which two could be compared. ADA formation occurred in 3.3% (7/213) of patients on combination therapy compared to 10.9% (36/331) of patients on monotherapy (RR 0.30, 95% CI 0.14, 0.67; 2 studies; p=0.003, GRADE moderate; Figure 6). Heterogeneity was low (I2 = 0%, p=0.43). In all studies, patients received scheduled maintenance treatment for more than 14 weeks. In the PRECiSE 3 study, an extension of PRECiSE 1 and PRECiSE 2, ADA formation occurred in 14.6% (31/213) of patients on combination therapy compared to 27% (103/382) of patients who received monotherapy (RR 0.54; 95% CI 0.37, 0.78; p<0.001). Data on the effect of methotrexate, thiopurines or corticosteroids on ADA formation were unavailable. In the PRECiSE 2 trial it was shown that immunogenicity rates were higher in patients receiving induction treatment who were then assigned to placebo when compared to patients receiving maintenance treatment (18% versus 8%). This was mainly reflected by patients receiving monotherapy (24% ADA positive).
Figure 6:

ADA formation in certolizumab pegol combo- versus monotherapy.
3.7.2. Serum drug concentrations
An integrated analysis of 5-year follow-up of the PRECiSE trial showed a lower range of mean drug serum concentrations in ADA-positive versus ADA-negative patients (0.88–15.25 vs 8.33–29.89 μg/ml) and no influence of ADA-formation on adverse events [40].
3.7.3. Clinical outcomes
Schreiber et al. reported that of the 17 patients with positive tests for ADA against certolizumab pegol, 12 (71%) had a response through week 26, compared with 62% (121/196) of patients with negative antibody tests [41]. In a 7-year analysis of the PRECiSE 3 trial, Sandborn et al. found no difference in clinical disease activity between persistently ADA-positive and ADA-undetectable patients [42].
3.7.4. Biochemical outcomes
Sandborn et al. demonstrated that median CRP and fecal calprotectin concentrations were higher (p<0.05 at some visits) and plasma CZP concentrations were significantly lower (p<0.0001 at all visits) in patients with persistent ADAs when compared to the ADA negative group [42].
3.7.5. Other outcomes
Data on the influence of ADA formation on endoscopic outcomes and antibody assays were not available.
3.8. Vedolizumab
The search yielded nine RCTs that met eligibility criteria. No eligible observational studies were identified. None of the studies randomized patients to vedolizumab with or without an immunomodulator. None of the studies compared ADA-positive to ADA-negative patients. Four studies analyzed CD patients and five studies analyzed UC patients (Supplementary Table 1).
3.8.1. ADA formation
ADA formation occurred in 8.4% of patients treated with vedolizumab. Numerical data on ADA formation in patients treated with monotherapy or concomitant immunomodulator therapy were unavailable. Feagan et al. reported that concomitant immunomodulator therapy was associated with decreased immunogenicity [43]. No other data were available regarding the influence of combination therapy on antibody formation to vedolizumab.
3.8.2. Infusion reactions
Three studies reported on infusion reactions in patients treated with vedolizumab. The number of infusion reactions was very low, however most patients with an infusion reaction were ADA-positive. Wyant et al. reported no relationship between immunogenicity and safety in an long-term safety analysis of the GEMINI studies [44].
3.8.3. Other outcomes
Feagan et al. studied ADA formation against MLN02 (a predecessor compound of vedolizumab which had a modified amino acid sequence and was expressed in a different system) at dosages of 0.5 mg/kg and 2.0 mg/kg, and showed that ADAs were more frequently detected at lower dosages [45]. Additionally, it was reported that patients with clinically significant ADA titers had lower remission rates. Sandborn et al. showed that ADA to subcutaneous or intravenous vedolizumab resulted in lower drug exposure and reduced efficacy, although the number of ADA-positive patients was very low. It was also observed that patients receiving vedolizumab induction treatment who were then randomized to placebo had higher ADA rates (30%). Other relevant data on the influence of ADA formation on clinical, biochemical and endoscopic outcomes or serum drug concentrations and adverse events were not available [46].
3.9. Ustekinumab
The search yielded four RCTs that met the eligibility criteria. No eligible observational studies were identified. None of the studies randomized patients to ustekinumab in combination with immunomodulators or ustekinumab monotherapy. One study compared ADA-positive to ADA-negative patients. All studies analyzed CD patients (Supplementary Table 1).
3.9.1. ADA formation
ADA development occurred in 3.7% (10/273) of patients on combination therapy compared to 6.2% (40/644) of patients treated with monotherapy (RR 0.59; 95% CI 0.30, 1.12; 2 studies; p=0.13; GRADE moderate; Supplementary Figure). Low heterogeneity was detected (I2= 30%, p=0.23).
3.9.2. Other outcomes
In a post-hoc analysis of UNIFI, Adedokun et al. reported lower serum ustekinumab concentrations in ADA-positive versus ADA-negative patients at week 24 (0.31 μg/ml; IQR 0.11–2.14, vs 2.76 μg/ml; IQR 1.87–4.18). They also showed that there was no relationship between ADA status and clinical efficacy. Furthermore they reported no difference in endoscopic response between ADA positive and negative patients and no relationship between ADA positivity and injection site reactions or anaphylactic reactions [47, 48]. Other data on the influence of antibody formation on clinical, biochemical and endoscopic outcomes or serum drug concentrations and adverse events were not available.
3.10. Natalizumab
The search yielded six RCTs and one prospective study that met the eligibility criteria. None of the studies randomized patients to natalizumab in combination with immunomodulators or natalizumab monotherapy. None of the studies compared ADA positive to ADA negative patients. All studies analyzed CD patients (Supplementary Table 1).
3.10.1. ADA formation
ADA development occurred in 2.6% (10/389) of patients treated with combination therapy compared to 16.0% (60/374) of patients assigned to monotherapy (RR 0.20; 95% CI 0.11, 0.39; 2 studies, p<0.001; GRADE moderate; Supplementary Figure 5). No heterogeneity was detected (I2 = 0%, P = 0.48). Only one study assessed maintenance treatment (>14 weeks), thus no subgroup analysis could be performed. Data on the effect of methotrexate, thiopurines or corticosteroids on ADA formation were unavailable.
3.10.2. Other outcomes
Data on the influence of ADA formation on clinical, biochemical and endoscopic outcomes or serum drug concentrations and adverse events were not available. None of the studies used drug tolerant assays.
3.11. Etrolizumab
The search yielded two RCTs that met the eligibility criteria. No eligible observational studies were identified. None of the studies randomized patients to etrolizumab in combination with immunomodulators or etrolizumab monotherapy. None of the studies compared ADA-positive to ADA-negative patients. Both studies analyzed UC patients (Supplementary Table 1).
3.11.1. ADA formation
ADAs were measured in 119 patients. Reported ADA formation rates were 4.9% (4/81) (Vermeire et al.) and 5.3% (2/38) (Rutgeerts et al.). ADAs were detected with a drug tolerant assay in both studies. None of the studies reported on the effect of combination therapy on antibody formation. Other data on the influence of ADA formation on clinical, biochemical and endoscopic outcomes or serum drug concentrations and adverse events were not available.
4. Discussion
The results of this systematic review and meta-analysis showed that ADA formation to biologic agents was reduced in patients treated with combination therapy compared to patients treated with monotherapy. Combination therapy has been the preferred strategy for patients starting infliximab treatment, however our findings are consistent with the notion that starting combination therapy with immunomodulators may also be an effective strategy for reducing ADA formation in patients treated with adalimumab, golimumab, certolizumab pegol, and natalizumab. Although comparative evidence is lacking, it is likely that combination therapy reduces ADA formation for other approved biologics agents (i.e., ustekinumab, etrolizumab and vedolizumab). For instance, Feagan et al. noted lower immunogenicity in patients treated with vedolizumab in combination with an immunomodulator, yet quantitative data are lacking [43]. ADA formation with ustekinumab was lower in patients treated with combination therapy compared to monotherapy (4% vs 6%), however this difference was not statistically significant, which may be a consequence of the low number of patients developing ADA.
ADA formation has a negative impact on clinical, biochemical, and endoscopic outcomes. For example, ADA formation to infliximab has usually been associated with lower clinical response rates and Vande Casteele et al. demonstrated higher concentrations of CRP in ADA positive patients [49]. Nonetheless, Seow et al. found that ADA positivity had no influence on endoscopic outcomes in patients treated with infliximab [32]. Sandborn et al. found higher median CRP and fecal calprotectin concentrations in patients persistently positive for ADA to certolizumab pegol, however this was not reflected in clinical outcomes [42]. Based on the available evidence, no robust conclusions can be drawn regarding the effect of ADA formation on biochemical and endoscopic treatment outcomes. Importantly, none of these studies were powered to assess the influence of ADA formation on these outcomes. Additionally, it is relevant to note that ADA positive patients may have sufficient serum drug concentrations during the majority of the treatment interval, especially for drugs that are more frequently administered (e.g. adalimumab). Lastly, patients who are in remission and develop ADAs are unlikely to immediately lose response due to pharmacodynamic carryover.
Several studies reported on ADA formation and infusion reactions to infliximab or vedolizumab [9, 16, 31, 45, 46, 50, 51]. ADA formation was associated with an increased risk for infusion reactions with infliximab (RR 2.36; 95% CI 1.85, 2.81), however the data regarding vedolizumab were insufficient for meta-analysis.
Rates of ADA formation differed substantially amongst biologics, and across different studies of the same agent. The highest reported incidence of ADA formation in patients receiving scheduled infliximab, adalimumab or golimumab monotherapy was 40.7% (44/108), 16.7% (1/6) and 37.1%, respectively. For scheduled certolizumab pegol and vedolizumab treatment, the highest reported incidence of ADA formation was 24.2% (30/124) and 10.8% (4/37), respectively. Lower rates were reported in patients receiving scheduled natalizumab, ustekinumab and etrolizumab monotherapy (4.1% [5/123], 11.1% [2/18], 4.6% [23/505] and 4.9% [4/81], respectively), despite the use of drug tolerant assays for the newer molecules (ustekinumab and etrolizumab). Higher proportions of ADAs were seen in the older studies where patients were treated episodically, or only received induction treatment with one to three infusions (i.e. phase 2 studies). For instance, the highest reported incidence of ADA formation for episodic infliximab was 60.8% (76/125) [9]. Additionally, ADA rates were higher for episodic vedolizumab, certolizumab pegol and golimumab treatment [14, 45, 52–54]. For the other biologics, the impact of episodic treatment is unknown. Another reason for differences in immunogenicity could be differences in structure of the agent (i.e. infliximab is a chimeric monoclonal antibody). Although the described differences in ADA rates should be interpreted cautiously because of differences between assays it is likely that immunogenicity is of less concern with newer biologics especially given that these agents have been assessed, in the most part, using highly sensitive drug-tolerant assays.
There were several aspects that we could not assess in this review. Only a few studies used drug tolerant assays and a meta-analysis of studies comparing different assays could therefore not be made. However, immunogenicity rates for infliximab, vedolizumab and golimumab are higher when measuring with a drug tolerant assay [14, 33, 53, 55]. Furthermore, we were unable to assess the impact of drug dose on immunogenicity due to lack of sufficient data. Thus it is important to note that higher drug concentrations in patients treated with higher doses may have masked the detection of ADA. Despite those limitations, there are data suggesting that higher doses of infliximab and golimumab result in less immunogenicity [14, 15]. It has been shown that ADA formation results in low serum drug concentrations due to accelerated clearance, which is the main reason for treatment failure due to ADA formation, together with drug neutralization [56, 57]. Some of the included studies showed lower serum drug concentrations in ADA-positive patients, but we could not perform a meta-analysis due to scarce data and data heterogeneity. We could also not account for the impact of route of administration, which may also be a factor influencing immunogenicity. For instance, there is evidence that subcutaneous infliximab is less immunogenic than intravenous infliximab [58]. Furthermore, we did not assess the difference between neutralizing versus non-neutralizing and transient vs. sustained antibodies, since most studies did not distinguish between the two. Transient ADAs are probably clinically less relevant and sustained ADAs are more likely to result in treatment failure [59, 60]. Additionally, we did not evaluate the risk of developing ADAs when rechallenging with the same biologic agent or when switching to a second biologic. For instance, it has been shown that the risk of ADA formation is higher when switching to a second TNF antagonist [61, 62]. It has also been shown that re-treatment with the same TNF antagonist after stopping maintenance treatment (‘drug holiday’) is associated with a higher risk of adverse events such as infusion reactions and ADA development, which is also seen with episodic treatment [9, 63, 64]. We did also not assess risk of immunogenicity when switching from originator to biosimilar biologicals since this was not within the scope of this review. Nevertheless, is has been shown in previous studies that switching to a biosimilar is safe, effective and not associated with increased immunogenicity [65, 66]. Lastly, there is also some evidence that genetic factors play a role in immunogenicity [67]. Thus, these results should be interpreted with caution and in the context of important aforementioned data gaps. The incidence of ADA for different biologics is likely higher than reported, since most studies used drug sensitive assays. Additionally, there are several important factors impacting ADA formation that could not be properly assessed in this review. However, this does not negate the fact that ADA formation is associated with poorer treatment outcomes and that combination therapy with an immunomodulator results in less immunogenicity, which is mainly of importance for agents with considerable immunogenic potential. Given the fact that immunogenicity is much lower for the newest agents (e.g. anti-integrins and ustekinumab), the benefit of combination therapy for prevention of ADA formation is probably trivial in these agents.
Reduced ADA formation in patients treated with infliximab in combination with an immunomodulator has also been shown in several uncontrolled or retrospective studies [10, 11, 68, 69]. Another systematic review, studying the immunogenicity of TNF antagonists in autoimmune inflammatory diseases found similar results [70]. However, most of the studies in this review were not conducted in patients with IBD. ADA formation was also associated with inferior treatment outcomes. Nevertheless, in other cohort studies it has been shown that immunogenicity increases drug clearance, resulting in lower serum drug concentrations that are, in turn, associated with poorer treatment outcomes for various biologic agents [10, 11].
Despite the available evidence, several knowledge gaps remain. For instance, not much is known on how ADA titers are associated with serum drug concentrations and what ADA titers result in sub-therapeutic serum drug concentrations (i.e. patients could have sub-therapeutic drug concentrations due to ADA formation which is not detected by drug sensitive assays). To evaluate this question, studies with drug tolerant assays should be conducted. Drug sensitive assays only show ADAs when serum drug concentrations are low or undetectable and thus an inverse correlation between both continuous measures is a self-fulfilling prophecy. Detecting ADAs earlier on, before serum drug concentrations become sub-therapeutic, could be of clinical value and should be evaluated in future studies. In this review, we identified some studies that used a drug tolerant assay. However, the studies did not evaluate this issue. A retrospective study showed that a cut-off in ADA lower than 282 ng/mL was valuable for decision making for interval shortening and dose doubling in infliximab [71]. Controlled prospective studies for different biologics are needed to further assess this phenomenon. These questions also highlight the importance of harmonizing ADA detection methods. Usage of uniform assays and standards would result in more comparable data for meta-analysis and would ultimately lead to improved clinical utility. Additionally, small retrospective cohort studies have suggested that adding an immunomodulator in monotherapy patients who develop ADAs may reverse ADA formation [17, 18]. However, no prospective controlled studies have been conducted.
With respect to combination therapy, the optimal doses of immunomodulators that suffice for prevention of ADA formation are unknown. To our knowledge only one study has addressed this issue [72]. Roblin et al. showed that lower doses of azathioprine worked equally well for ADA prevention with infliximab. More studies on this topic should be conducted in the future. However, it has been shown that lower doses of methotrexate suffice for prevention of immunogenicity in rheumatic diseases [73].
This study has several strengths. To our knowledge this is the first comprehensive systematic review and meta-analysis studying immunogenicity and comparing monotherapy with combination therapy in IBD patients. An extensive literature search was conducted and all available biologics for treatment of IBD were evaluated. In doing so, we highlighted several knowledge gaps that need to be addressed in the future. This review also has some limitations. Firstly, the search was conducted in April 2020. New data may have become available in the meantime, especially regarding newer agents. Given the scale of this project it was not possible to finish the manuscript within one year after the search. Therefore, this review should be updated in the future when more data regarding the newer agents has become available. Furthermore, ADA formation was not the primary outcome in any of the studies. As a result, many studies reported on ADA formation in a smaller subset of patients with available blood samples and not in the entire cohort which could potentially lead to over or underestimation of ADA rates. Additionally, factors such as the amount of blood samples taken, the time-points for measuring, assay types, and treatment duration were not always comparable across studies. Moreover, in the older studies with infliximab, patients were treated episodically, resulting in higher immunogenicity rates which is not applicable to the scheduled treatment regimens used today. Such heterogeneity has likely influenced the results of the meta-analysis. Nevertheless, we believe that most evidence was sufficient to draw reliable conclusions regarding ADA formation and combination therapy with immunomodulators.
In conclusion, our analyses showed that combination therapy reduced ADA formation for most biologics for which data were available. The protective effect of combination therapy on ADA formation may be greater for those biologics with higher immunogenic potential and thus the risks associated with combination therapy may not outweigh the potential benefits for newer, less immunogenic agents. Combination therapy for a subsequent biologic agent should be considered when switching from a biologic agent in a sensitized patient because of persistent loss of response and presence of ADA. Future studies should focus on harmonizing ADA assays, determining clinically relevant concentration cut-offs for ADA and optimal dosing of immunomodulators to prevent ADA formation.
Supplementary Material
Key findings:
Differences in analytical methods to detect anti-drug antibodies (ADA) hamper comparison of true ADA rates across biologics in IBD.
Use of combination therapy with immunomodulators appeared to reduce ADA positivity for most biologics.
For infliximab, ADA were associated with reduced drug efficacy and increased adverse events. This could not be assessed for other agents due to lack of data.
Future studies should focus on harmonizing ADA assays, determining clinically relevant concentration cut-offs for ADA and optimal dosing of immunomodulators to prevent ADA formation.
Acknowledgements:
We would like to thank John MacDonald [Alimentiv Inc, London, Ontario, Canada] for his assistance in the writing process.
Disclosures:
SB: has served as speaker for Abbvie, Merck, Sharp & Dome, Takeda, Jansen Cilag, Pfizer and Tillotts.
CEP: is an employee of Robarts Clinical Trials, Inc.
JFB: has served as speaker for Abbvie, Merck, Sharp & Dome, Takeda and Tillots.
ML: has served as speaker and/or principal investigator for: Abbvie, Celgene, Covidien, Dr. Falk, Ferring Pharmaceuticals, Gilead, GlaxoSmithKline, Janssen-Cilag, Merck Sharp & Dohme, Pfizer, Protagonist therapeutics, Receptos, Takeda, Tillotts, Tramedico. He has received research grants from AbbVie, Merck Sharp & Dohme, Achmea healthcare and ZonMW.
BGF: has received grant/research support from Millennium Pharmaceuticals, Merck, Tillotts Pharma AG, AbbVie, Novartis Pharmaceuticals, Centocor Inc., Elan/Biogen, UCB Pharma, Bristol-Myers Squibb, Genentech, ActoGenix, and Wyeth Pharmaceuticals Inc.; consulting fees from Millennium Pharmaceuticals, Merck, Centocor Inc., Elan/Biogen, Janssen-Ortho, Teva Pharmaceuticals, Bristol-Myers Squibb, Celgene, UCB Pharma, AbbVie, Astra Zeneca, Serono, Genentech, Tillotts Pharma AG, Unity Pharmaceuticals, Albireo Pharma, Given Imaging Inc., Salix Pharmaceuticals, Novonordisk, GSK, Actogenix, Prometheus Therapeutics and Diagnostics, Athersys, Axcan, Gilead, Pfizer, Shire, Wyeth, Zealand Pharma, Zyngenia, GiCare Pharma Inc., and Sigmoid Pharma; and speaker bureaux fees from UCB, AbbVie, and J&J/Janssen.
WJS: has received research grants from Abbvie, Abivax, Arena Pharmaceuticals, Boehringer Ingelheim, Celgene, Genentech, Gilead Sciences, Glaxo Smith Kline, Janssen, Lilly, Pfizer, Prometheus Biosciences, Seres Therapeutics, Shire, Takeda, Theravance Biopharma; consulting fees from Abbvie, Abivax, Admirx, Alfasigma, Alimentiv (previously Robarts Clinical Trials, owned by Alimentiv Health Trust), Alivio Therapeutics, Allakos, Amgen, Applied Molecular Transport, Arena Pharmaceuticals, Bausch Health (Salix), Beigene, Bellatrix Pharmaceuticals, Boehringer Ingelheim, Boston Pharmaceuticals, Bristol Meyers Squibb, Celgene, Celltrion, Cellularity, Cosmo Pharmaceuticals, Escalier Biosciences, Equillium, Forbion, Genentech/Roche, Gilead Sciences, Glenmark Pharmaceuticals, Gossamer Bio, Immunic (Vital Therapies), Index Pharmaceuticals, Intact Therapeutics, Janssen, Kyverna Therapeutics, Landos Biopharma, Lilly, Oppilan Pharma, Otsuka, Pandion Therapeutics, Pfizer, Progenity, Prometheus Biosciences, Prometheus Laboratories, Protagonists Therapeutics, Provention Bio, Reistone Biopharma, Seres Therapeutics, Shanghai Pharma Biotherapeutics, Shire, Shoreline Biosciences, Sublimity Therapeutics, Surrozen, Takeda, Theravance Biopharma, Thetis Pharmaceuticals, Tillotts Pharma, UCB, Vendata Biosciences, Ventyx Biosciences, Vimalan Biosciences, Vivelix Pharmaceuticals, Vivreon Biosciences, Zealand Pharma; stock or stock options from Allakos, BeiGene, Gossamer Bio, Oppilan Pharma, Prometheus Biosciences, Prometheus Laboratories Progenity, Shoreline Biosciences, Ventyx Biosciences, Vimalan Biosciences, Vivreon Biosciences; and employee at Shoreline Biosciences. Spouse: Iveric Bio - consultant, stock options; Progenity - stock; Oppilan Pharma - consultant, stock options; Prometheus Biosciences - employee, stock, stock options; Prometheus Laboratories – stock, stock options, consultant; Ventyx Biosciences – stock, stock options; Vimalan Biosciences – stock, stock options.
VJ: Has received scientific advisory board fees from Janssen, Takeda, Pfizer, Sandoz, Abbvie and Merck; and speaker bureaux fees from Takeda, Ferring, Janssen, Pfizer and Shire.
GDH: has served as advisor for Abbvie, Ablynx, Allergan, Amakem, Amgen, AM Pharma, Arena Pharmaceuticals, AstraZeneca, Avaxia, Biogen, Bristol Meiers Squibb, Boerhinger Ingelheim, Celgene/Receptos, Celltrion, Cosmo, Covidien/Medtronics, Ferring, DrFALK Pharma, Eli Lilly, Engene, Galapagos, Genentech/Roche, Gilead, Glaxo Smith Kline, Hospira/Pfizer, Immunic, Johnson and Johnson, Lycera, Medimetrics, Millenium/Takeda, Mitsubishi Pharma, Merck Sharp Dome, Mundipharma, Nextbiotics, Novonordisk, Otsuka, Pfizer/Hospira, Photopill, Prometheus laboratories/Nestle, Progenity, Protagonist, Robarts Clinical Trials, Salix, Samsung Bioepis, Sandoz, Seres/Nestle, Setpoint, Shire, Teva, Tigenix, Tillotts, Topivert, Versant and Vifor; received speaker fees from Abbvie, Biogen, Ferring, Johnson and Johnson, Merck Sharp Dome, Mundipharma, Norgine, Pfizer, Samsung Bioepis, Shire, Millenium/Takeda, Tillotts and Vifor.
NVC: received research grants and personal fees from R-Biopharm, Takeda and UCB; and personal fees from Alimentiv, Inc. (formerly Robarts Clinical Trials, Inc.), Celltrion and Prometheus.
Grant support:
NVC holds a Research Scholar Award from the American Gastroenterological Association. WJS and NVC are supported in part by the NIDDK-funded San Diego Digestive Diseases Research Center (P30 DK120515).
Footnotes
Declarations
Writing assistance: No funding was received for writing assistance.
Availability of data and material:
All data will be made available.
References
- 1.van der Valk ME, Mangen MJ, Leenders M, Dijkstra G, van Bodegraven AA, Fidder HH, et al. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-TNFalpha therapy: results from the COIN study. Gut. 2014;63(1):72–9. [DOI] [PubMed] [Google Scholar]
- 2.Bots SJA, Hoekman DR, Benninga MA, Ponsioen CY, D’Haens GR, Lowenberg M. Patterns of anti-TNF use and associated treatment outcomes in inflammatory bowel disease patients: results from an analysis of Dutch health insurance claims data. The Netherlands journal of medicine. 2017;75(10):432–42. [PubMed] [Google Scholar]
- 3.Plevy SE, Landers CJ, Prehn J, Carramanzana NM, Deem RL, Shealy D, et al. A role for TNF-alpha and mucosal T helper-1 cytokines in the pathogenesis of Crohn’s disease. Journal of immunology (Baltimore, Md : 1950). 1997;159(12):6276–82. [PubMed] [Google Scholar]
- 4.Masuda H, Iwai S, Tanaka T, Hayakawa S. Expression of IL-8, TNF-alpha and IFN-gamma m-RNA in ulcerative colitis, particularly in patients with inactive phase. Journal of clinical & laboratory immunology. 1995;46(3):111–23. [PubMed] [Google Scholar]
- 5.Benson JM, Peritt D, Scallon BJ, Heavner GA, Shealy DJ, Giles-Komar JM, et al. Discovery and mechanism of ustekinumab: a human monoclonal antibody targeting interleukin-12 and interleukin-23 for treatment of immune-mediated disorders. mAbs. 2011;3(6):535–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hamann A, Andrew DP, Jablonski-Westrich D, Holzmann B, Butcher EC. Role of alpha 4-integrins in lymphocyte homing to mucosal tissues in vivo. Journal of immunology (Baltimore, Md : 1950) 1994;152(7):3282–93. [PubMed] [Google Scholar]
- 7.Soler D, Chapman T, Yang LL, Wyant T, Egan R, Fedyk ER. The binding specificity and selective antagonism of vedolizumab, an anti-alpha4beta7 integrin therapeutic antibody in development for inflammatory bowel diseases. The Journal of pharmacology and experimental therapeutics. 2009;330(3):864–75. [DOI] [PubMed] [Google Scholar]
- 8.Rutgeerts PJ, Fedorak RN, Hommes DW, Sturm A, Baumgart DC, Bressler B, et al. A randomised phase I study of etrolizumab (rhuMAb beta7) in moderate to severe ulcerative colitis. Gut. 2013;62(8):1122–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Baert F, Noman M, Vermeire S, Van Assche G, G DH, Carbonez A, et al. Influence of immunogenicity on the long-term efficacy of infliximab in Crohn’s disease. N Engl J Med. 2003;348(7):601–8. [DOI] [PubMed] [Google Scholar]
- 10.Karmiris K, Paintaud G, Noman M, Magdelaine-Beuzelin C, Ferrante M, Degenne D, et al. Influence of trough serum levels and immunogenicity on long-term outcome of adalimumab therapy in Crohn’s disease. Gastroenterology. 2009;137(5):1628–40. [DOI] [PubMed] [Google Scholar]
- 11.O’Meara S, Nanda KS, Moss AC. Antibodies to infliximab and risk of infusion reactions in patients with inflammatory bowel disease: a systematic review and meta-analysis. Inflammatory bowel diseases. 2014;20(1):1–6. [DOI] [PubMed] [Google Scholar]
- 12.Colombel JF, Sandborn WJ, Reinisch W, Mantzaris GJ, Kornbluth A, Rachmilewitz D, et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. N Engl J Med. 2010;362(15):1383–95. [DOI] [PubMed] [Google Scholar]
- 13.Panaccione R, Ghosh S, Middleton S, Marquez JR, Scott BB, Flint L, et al. Combination therapy with infliximab and azathioprine is superior to monotherapy with either agent in ulcerative colitis. Gastroenterology. 2014;146(2):392–400.e3. [DOI] [PubMed] [Google Scholar]
- 14.Adedokun OJ, Gunn GR, Leu JH, Gargano C, Xu Z, Sandborn WJ, et al. Immunogenicity of Golimumab and its Clinical Relevance in Patients With Ulcerative Colitis. Inflammatory bowel diseases. 2019;25(9):1532–40. [DOI] [PubMed] [Google Scholar]
- 15.Hanauer SB, Wagner CL, Bala M, Mayer L, Travers S, Diamond RH, et al. Incidence and importance of antibody responses to infliximab after maintenance or episodic treatment in Crohn’s disease. Clinical Gastroenterology & Hepatology. 2004;2:542–53. [DOI] [PubMed] [Google Scholar]
- 16.Farrell RJ, Alsahli M, Jeen YT, Falchuk KR, Peppercorn MA, Michetti P. Intravenous hydrocortisone premedication reduces antibodies to infliximab in Crohn’s disease: a randomized controlled trial. Gastroenterology. 2003;124(4):917–24. [DOI] [PubMed] [Google Scholar]
- 17.Ben-Horin S, Waterman M, Kopylov U, Yavzori M, Picard O, Fudim E, et al. Addition of an immunomodulator to infliximab therapy eliminates antidrug antibodies in serum and restores clinical response of patients with inflammatory bowel disease. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2013;11(4):444–7. [DOI] [PubMed] [Google Scholar]
- 18.Strik AS, van den Brink GR, Ponsioen C, Mathot R, Lowenberg M, D’Haens GR. Suppression of anti-drug antibodies to infliximab or adalimumab with the addition of an immunomodulator in patients with inflammatory bowel disease. Alimentary pharmacology & therapeutics. 2017;45(8):1128–34. [DOI] [PubMed] [Google Scholar]
- 19.Hart MH, de Vrieze H, Wouters D, Wolbink GJ, Killestein J, de Groot ER, et al. Differential effect of drug interference in immunogenicity assays. Journal of immunological methods. 2011;372(1–2):196–203. [DOI] [PubMed] [Google Scholar]
- 20.Steenholdt C, Ainsworth MA, Tovey M, Klausen TW, Thomsen OO, Brynskov J, et al. Comparison of techniques for monitoring infliximab and antibodies against infliximab in Crohn’s disease. Therapeutic Drug Monitoring. 2013;35(4):530–8. [DOI] [PubMed] [Google Scholar]
- 21.Higgins JPTTJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.1 (updated September 2020). Cochrane, 2020. Available from www.training.cochrane.org/handbook. [Google Scholar]
- 22.Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006–12. [DOI] [PubMed] [Google Scholar]
- 23.Bots S, Vande Casteele N, Brandse JF, Lowenberg M, Feagan BG, Sandborn WJ, et al. Antibody development against biologic agents used for the treatment of inflammatory bowel disease and antibody prevention with immunosuppressives. Cochrane Database of Systematic Reviews. 2016(5). [Google Scholar]
- 24.Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj. 2011;343:d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M. The Newcastle-Ottawa Scale (NOS) for assessing the quality of non randomised studies in meta-analyses 2017. [Available from: www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
- 26.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj. 2003;327(7414):557–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. Bmj. 2008;336(7650):924–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Vermeire S, Noman M, Van Assche G, Baert F, D’Haens G, Rutgeerts P. Effectiveness of concomitant immunosuppressive therapy in suppressing the formation of antibodies to infliximab in Crohn’s disease. Gut. 2007;56(9):1226–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Oh EH, Ko DH, Seo H, Chang K, Kim GU, Song EM, et al. Clinical correlations of infliximab trough levels and antibodies to infliximab in South Korean patients with Crohn’s disease. World journal of gastroenterology. 2017;23(8):1489–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Adedokun OJ, Sandborn WJ, Feagan BG, Rutgeerts P, Xu Z, Marano CW, et al. Association between serum concentration of infliximab and efficacy in adult patients with ulcerative colitis. Gastroenterology. 2014;147(6):1296–307 e5. [DOI] [PubMed] [Google Scholar]
- 31.Rutgeerts P, Sandborn WJ, Feagan BG, Reinisch W, Olson A, Johanns J, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353(23):2462–76. [DOI] [PubMed] [Google Scholar]
- 32.Seow CH, Newman A, Irwin SP, Steinhart AH, Silverberg MS, Greenberg GR. Trough serum infliximab: a predictive factor of clinical outcome for infliximab treatment in acute ulcerative colitis. Gut. 2010;59(1):49–54. [DOI] [PubMed] [Google Scholar]
- 33.Van Stappen T, Vande Casteele N, Van Assche G, Ferrante M, Vermeire S, Gils A. Clinical relevance of detecting anti-infliximab antibodies with a drug-tolerant assay: post hoc analysis of the TAXIT trial. Gut. 2018;67(5):818–26. [DOI] [PubMed] [Google Scholar]
- 34.Regueiro M, Feagan BG, Zou B, Johanns J, Blank MA, Chevrier M, et al. Infliximab Reduces Endoscopic, but Not Clinical, Recurrence of Crohn’s Disease After Ileocolonic Resection. Gastroenterology. 2016;150(7):1568–78. [DOI] [PubMed] [Google Scholar]
- 35.Ye BD, Pesegova M, Alexeeva O, Osipenko M, Lahat A, Dorofeyev A, et al. Efficacy and safety of biosimilar CT-P13 compared with originator infliximab in patients with active Crohn’s disease: an international, randomised, double-blind, phase 3 non-inferiority study. Lancet. 2019;393(10182):1699–707. [DOI] [PubMed] [Google Scholar]
- 36.Roblin X, Williet N, Boschetti G, Phelip JM, Del Tedesco E, Berger AE, et al. Addition of azathioprine to the switch of anti-TNF in patients with IBD in clinical relapse with undetectable anti-TNF trough levels and antidrug antibodies: a prospective randomised trial. Gut. 2020;69(7):1206–12. [DOI] [PubMed] [Google Scholar]
- 37.Sandborn WJ, Feagan BG, Marano C, Zhang H, Strauss R, Johanns J, et al. Subcutaneous golimumab maintains clinical response in patients with moderate-to-severe ulcerative colitis. Gastroenterology. 2014;146(1):96–109.e1. [DOI] [PubMed] [Google Scholar]
- 38.Sandborn WJ, Feagan BG, Marano C, Zhang H, Strauss R, Johanns J, et al. Subcutaneous golimumab induces clinical response and remission in patients with moderate-to-severe ulcerative colitis. Gastroenterology. 2014;146(1):85–95; quiz e14–5. [DOI] [PubMed] [Google Scholar]
- 39.Adedokun OJ, Xu Z, Marano CW, Strauss R, Zhang H, Johanns J, et al. Pharmacokinetics and Exposure-response Relationship of Golimumab in Patients with Moderately-to-Severely Active Ulcerative Colitis: Results from Phase 2/3 PURSUIT Induction and Maintenance Studies. Journal of Crohn’s & colitis. 2017;11(1):35–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Sandborn W, Dubinsky M, Kosutic G, Parker G, Spearman M, Hasan I, et al. Incidence of anti-drug antibodies in crohn’s disease patients during 5 years of certolizumab pegol therapy. Inflammatory bowel diseases. 2016;22:S41. [Google Scholar]
- 41.Sandborn WJ, Feagan BG, Stoinov S, Honiball PJ, Rutgeerts P, Mason D, et al. Certolizumab pegol for the treatment of Crohn’s disease. N Engl J Med. 2007;357(3):228–38. [DOI] [PubMed] [Google Scholar]
- 42.Sandborn WJ, Wolf DC, Kosutic G, Parker G, Schreiber S, Lee SD, et al. Effects of Transient and Persistent Anti-drug Antibodies to Certolizumab Pegol: Longitudinal Data from a 7-Year Study in Crohn’s Disease. Inflammatory bowel diseases. 2017;23(7):1047–56. [DOI] [PubMed] [Google Scholar]
- 43.Feagan BG, Rutgeerts P, Sands BE, Hanauer S, Colombel JF, Sandborn WJ, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369(8):699–710. [DOI] [PubMed] [Google Scholar]
- 44.Wyant T, Yang L, Lirio R, Rosario M. Long-term immunogenicity of vedolizumab in ulcerative colitis and Crohn’s disease (GEMINI Programme). Journal of Crohn’s and Colitis. 2019;13 (Supplement 1):S331. [Google Scholar]
- 45.Feagan BG, Greenberg GR, Wild G, Fedorak RN, Pare P, McDonald JW, et al. Treatment of active Crohn’s disease with MLN0002, a humanized antibody to the alpha4beta7 integrin. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2008;6(12):1370–7. [DOI] [PubMed] [Google Scholar]
- 46.Parikh A, Leach T, Wyant T, Scholz C, Sankoh S, Mould DR, et al. Vedolizumab for the treatment of active ulcerative colitis: a randomized controlled phase 2 dose-ranging study. Inflammatory bowel diseases. 2012;18(8):1470–9. [DOI] [PubMed] [Google Scholar]
- 47.Adedokun OJ, Xu Z, Marano C, O’Brien C, Szapary P, Zhang H, et al. Ustekinumab Pharmacokinetics and Exposure Response in a Phase 3 Randomized Trial of Patients With Ulcerative Colitis: Ustekinumab PK and exposure-response in UC. Clinical Gastroenterology & Hepatology. 2019;06:06. [DOI] [PubMed] [Google Scholar]
- 48.Sands BE, Sandborn WJ, Panaccione R, O’Brien CD, Zhang H, Johanns J, et al. Ustekinumab as induction and maintenance therapy for ulcerative colitis. New England Journal of Medicine. 2019;381(13):1201–14. [DOI] [PubMed] [Google Scholar]
- 49.Vande Casteele N, Ferrante M, Van Assche G, Ballet V, Compernolle G, Van Steen K, et al. Trough concentrations of infliximab guide dosing for patients with inflammatory bowel disease. Gastroenterology. 2015;148(7):1320–9 e3. [DOI] [PubMed] [Google Scholar]
- 50.Hanauer SB, Feagan BG, Lichtenstein GR, Mayer LF, Schreiber S, Colombel JF, et al. Maintenance infliximab for Crohn’s disease: the ACCENT I randomised trial. Lancet. 2002;359(9317):1541–9. [DOI] [PubMed] [Google Scholar]
- 51.Sands BE, Anderson FH, Bernstein CN, Chey WY, Feagan BG, Fedorak RN, et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N Engl J Med. 2004;350(9):876–85. [DOI] [PubMed] [Google Scholar]
- 52.Feagan BG, Greenberg GR, Wild G, Fedorak RN, Pare P, McDonald JW, et al. Treatment of ulcerative colitis with a humanized antibody to the alpha4beta7 integrin. N Engl J Med. 2005;352(24):2499–507. [DOI] [PubMed] [Google Scholar]
- 53.Sandborn WJ, Baert F, Danese S, Krznaric Z, Kobayashi T, Yao X, et al. Efficacy and Safety of Vedolizumab Subcutaneous Formulation in a Randomized Trial of Patients With Ulcerative Colitis. Gastroenterology. 2020;158(3):562–72.e12. [DOI] [PubMed] [Google Scholar]
- 54.Schreiber S, Khaliq-Kareemi M, Lawrance IC, Thomsen OO, Hanauer SB, McColm J, et al. Maintenance therapy with certolizumab pegol for Crohn’s disease. N Engl J Med. 2007;357(3):239–50. [DOI] [PubMed] [Google Scholar]
- 55.Steenholdt C, Bendtzen K, Brynskov J, Thomsen OO, Ainsworth MA. Clinical implications of measuring drug and anti-drug antibodies by different assays when optimizing infliximab treatment failure in Crohn’s disease: post hoc analysis of a randomized controlled trial. The American journal of gastroenterology. 2014;109(7):1055–64. [DOI] [PubMed] [Google Scholar]
- 56.Brandse JF, Mould D, Smeekes O, Ashruf Y, Kuin S, Strik A, et al. A Real-life Population Pharmacokinetic Study Reveals Factors Associated with Clearance and Immunogenicity of Infliximab in Inflammatory Bowel Disease. Inflammatory bowel diseases. 2017;23(4):650–60. [DOI] [PubMed] [Google Scholar]
- 57.Papamichael K, Chachu KA, Vajravelu RK, Vaughn BP, Ni J, Osterman MT, et al. Improved Long-term Outcomes of Patients With Inflammatory Bowel Disease Receiving Proactive Compared With Reactive Monitoring of Serum Concentrations of Infliximab. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2017;15(10):1580–8.e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Schreiber SLJ, Dudkowiak R, Gawdis Lahat A., Wojnarska BPA, Horynski M, Farkas K, Kierkus J, Kowalski M, Ben-Horin SYBD, Lee SJ, Kim SH, Kim MR, Kim HN, W. R. Noninferiority of novel subcutaneous infliximab (ct-p13) to intravenous infliximab (ct-p13) in patients with active crohn’s disease and ulcerative colitis: week 30 results from a multicentre, randomised controlled pivotal trial. Unit Eur Gastroenterol J.7(10):1412. [Google Scholar]
- 59.Ungar B, Chowers Y, Yavzori M, Picard O, Fudim E, Har-Noy O, et al. The temporal evolution of antidrug antibodies in patients with inflammatory bowel disease treated with infliximab. Gut. 2014;63(8):1258–64. [DOI] [PubMed] [Google Scholar]
- 60.Roblin X, Marotte H, Leclerc M, Del Tedesco E, Phelip JM, Peyrin-Biroulet L, et al. Combination of C-reactive protein, infliximab trough levels, and stable but not transient antibodies to infliximab are associated with loss of response to infliximab in inflammatory bowel disease. Journal of Crohn’s & colitis. 2015;9(7):525–31. [DOI] [PubMed] [Google Scholar]
- 61.Roblin X, Verot C, Paul S, Duru G, Williet N, Boschetti G, et al. Is the Pharmacokinetic Profile of a First Anti-TNF Predictive of the Clinical Outcome and Pharmacokinetics of a Second Anti-TNF? Inflammatory bowel diseases. 2018. [DOI] [PubMed] [Google Scholar]
- 62.Bartelds GM, Wijbrandts CA, Nurmohamed MT, Stapel S, Lems WF, Aarden L, et al. Anti-infliximab and anti-adalimumab antibodies in relation to response to adalimumab in infliximab switchers and anti-tumour necrosis factor naive patients: a cohort study. Annals of the rheumatic diseases. 2010;69(5):817–21. [DOI] [PubMed] [Google Scholar]
- 63.Casanova MJ, Chaparro M, Garcia-Sanchez V, Nantes O, Leo E, Rojas-Feria M, et al. Evolution After Anti-TNF Discontinuation in Patients With Inflammatory Bowel Disease: A Multicenter Long-Term Follow-Up Study. The American journal of gastroenterology. 2017;112(1):120–31. [DOI] [PubMed] [Google Scholar]
- 64.Torres J, Boyapati RK, Kennedy NA, Louis E, Colombel JF, Satsangi J. Systematic Review of Effects of Withdrawal of Immunomodulators or Biologic Agents From Patients With Inflammatory Bowel Disease. Gastroenterology. 2015;149(7):1716–30. [DOI] [PubMed] [Google Scholar]
- 65.García Beloso N, Altabás González I, Samartín Ucha M, Gayoso Rey M, De Castro Parga ML, Salgado Barreira Á, et al. Switching between reference adalimumab and biosimilars in chronic immune-mediated inflammatory disease: a systematic literature review. Br J Clin Pharmacol. 2021. [DOI] [PubMed] [Google Scholar]
- 66.Albshesh A, Ben-Horin S. CT-P13: a review on a biosimilar to infliximab in the treatment of inflammatory bowel disease. Expert Opin Biol Ther. 2019;19(10):971–8. [DOI] [PubMed] [Google Scholar]
- 67.Sazonovs A, Kennedy NA, Moutsianas L, Heap GA, Rice DL, Reppell M, et al. HLA-DQA1*05 Carriage Associated With Development of Anti-Drug Antibodies to Infliximab and Adalimumab in Patients With Crohn’s Disease. Gastroenterology. 2020;158(1):189–99. [DOI] [PubMed] [Google Scholar]
- 68.Steenholdt C, Svenson M, Bendtzen K, Thomsen OO, Brynskov J, Ainsworth MA. Severe infusion reactions to infliximab: aetiology, immunogenicity and risk factors in patients with inflammatory bowel disease. Alimentary pharmacology & therapeutics. 2011;34(1):51–8. [DOI] [PubMed] [Google Scholar]
- 69.West R, Woude C, Hansen B, Felt-Bersma R, Tilburg A, Drapers J, et al. Clinical and endosonographic effect of ciprofloxacin on the treatment of perianal fistulae in Crohn’s disease with infliximab: a double-blind placebo-controlled study. Alimentary pharmacology & therapeutics [Internet]. 2004; 20(11–12):[1329–36 pp.]. Available from: http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/054/CN-00514054/frame.html. [DOI] [PubMed] [Google Scholar]
- 70.Pecoraro V, De Santis E, Melegari A, Trenti T. The impact of immunogenicity of TNFalpha inhibitors in autoimmune inflammatory disease. A systematic review and meta-analysis. Autoimmunity reviews. 2017;16(6):564–75. [DOI] [PubMed] [Google Scholar]
- 71.Dreesen E, Van Stappen T, Ballet V, Peeters M, Compernolle G, Tops S, et al. Anti-infliximab antibody concentrations can guide treatment intensification in patients with Crohn’s disease who lose clinical response. Alimentary pharmacology & therapeutics. 2018;47(3):346–55. [DOI] [PubMed] [Google Scholar]
- 72.Roblin X, Boschetti G, Williet N, Nancey S, Marotte H, Berger A, et al. Azathioprine dose reduction in inflammatory bowel disease patients on combination therapy: an open-label, prospective and randomised clinical trial. Alimentary pharmacology & therapeutics. 2017;46(2):142–9. [DOI] [PubMed] [Google Scholar]
- 73.Schaeverbeke T, Truchetet ME, Kostine M, Barnetche T, Bannwarth B, Richez C. Immunogenicity of biologic agents in rheumatoid arthritis patients: lessons for clinical practice. Rheumatology (Oxford). 2016;55(2):210–20. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
All data will be made available.