

Abstract
Objective:
Utilizing a multi-level meta-analytic approach, this review is the first to systematically quantify the efficacy of reading interventions for school-aged children with ADHD, and identify potential factors that may increase the success of reading-related interventions for these children.
Method:
18 studies (15 peer-reviewed articles, 3 dissertations) published from 1986 to 2020 (N=564) were meta-analyzed.
Results:
Findings revealed reading interventions are highly effective for improving reading skills based on both study-developed/curriculum-based measures (g=1.91) and standardized/norm-referenced achievement tests (g=1.11) in high-quality studies of children with rigorously-diagnosed ADHD. Reading interventions that include at least 30 hours of intervention targeting decoding/phonemic awareness meet all benchmarks to be considered a Level 1 (Well-Established) Evidence-Based Practice with Strong Research Support for children with ADHD based on clinical and special education criteria.
Conclusions:
Our findings collectively indicate that reading interventions should be the first-line treatment for reading difficulties among at-risk readers with ADHD.
Keywords: ADHD, Reading Intervention, Meta-analysis
ADHD is a neurodevelopmental disorder that affects 5% of school-aged children (Polanczyk et al., 2014) and is associated with clinically significant impairments in the family, peer, and academic domains (Kofler et al., 2017) at an annual U.S. cost of illness of over $100 billion (Zhao et al., 2019). Academic impairment is one of the foremost reasons for assessment and intervention for individuals with ADHD. An estimated 33% to 80% of children with ADHD demonstrate academic and learning difficulties (DuPaul & Langberg, 2015; Mayes & Calhoun, 2006) that frequently persist into adolescence and adulthood (Ek et al., 2011; Miranda et al., 2014). Reading difficulties are especially prominent in ADHD (for review, see Frazier et al., 2007), with 25–40% of children with ADHD presenting with a co-occurring diagnosis of reading disability (DuPaul et al., 2013; August & Garfinkel, 1990; Semrud-Clikeman et al., 1992). Notably, reading difficulties are apparent even in children with ADHD who do not meet formal criteria for reading disability (Ghelani et al., 2004). This is highly concerning given that studies have repeatedly demonstrated that early ADHD-related reading difficulties predict a host of negative outcomes, including later behavioral and conduct problems (Fergusson & Lynskey, 1997; Bennett et al., 2003), continued reading difficulties into adolescence (McGee et al., 2002), increased rates of high school dropout (McGee et al. 2002), and later job instability (Maughan et al., 1985). Given the prevalence of reading underachievement in ADHD and associated negative outcomes (Loe & Feldman, 2007), it is imperative to evaluate the efficacy of reading interventions for at-risk readers with ADHD, as well as potential factors that may increase the success of reading-related interventions for these children.
ADHD and Reading Interventions
Presently, empirically supported treatments for ADHD primarily consist of psychostimulant medication and behavioral interventions (Evans et al., 2018; Pelham et al., 2022; Raggi & Chronis, 2006). These interventions demonstrate robust effects for decreasing ADHD symptoms (Swanson et al., 1995; Fabiano et al., 2015; cf. Sonuga-Barke et al., 2013). In contrast, these first-line interventions demonstrate minimal to no benefits for academic achievement broadly or reading achievement specifically (Majewicz-Hefley & Carlson, 2007; Rapport et al., 1994; Kortekaas-Rijlaarsdam et al., 2019; Boland et al., 2020; MTA Cooperative Group; 1999; Fabiano et al., 2015; van der Oord et al., 2008). This replicated finding may be surprising given that the prevailing clinical model of ADHD (American Psychological Association, 2013) considers reading/academic underachievement to be a functional outcome of core ADHD symptoms (see Rapport et al., 2000). However, these findings indicate clearly that alternate approaches are needed to remediate these children’s reading difficulties (Tannock et al., 2018; Tamm et al., 2017).
To that end, interventions that directly target reading skills reflect a highly promising option for at-risk readers with ADHD, given decades of replicated evidence for the efficacy of reading interventions within the developmental and educational literatures (e.g., Al Otaiba & Fuchs, 2002; Ron Nelson et al., 2003; Tran et al., 2011). Reading interventions provide direct and explicit instruction on core reading skills (for review, see National Reading Panel, 2000). A primary goal of reading is to glean meaning and draw inferences from written text – a skill referred to as reading comprehension (Sideridis et al., 2006). According to the influential ‘simple view of reading,’ children’s reading comprehension can be fully explained by two interrelated components (for review see Lonigan et al., 2018): decoding (i.e., converting written symbols to speech sounds to form words) and language comprehension (i.e., comprehension of language when not presented as text, such as oral language; Gough & Tunmer, 1986). Given children with ADHD experience deficits across all components of the simple view of reading (Friedman et al., 2017; Korrel et al., 2017; Miller et al., 2013, 2014), it can be hypothesized that reading interventions specifically targeting component(s) of the simple view of reading will lead to better reading outcomes. Indeed, within the developmental/educational literatures reading interventions that target ‘simple view’ component(s) have been found to produce robust downstream effects on reading comprehension (National Reading Panel, 2000). Moreover, such benefits have been found for children across socioeconomic status (Bus et al., 1995) and intellectual abilities (Hill, 2016), though reading interventions that intervene at younger ages generally result in larger benefits (Goodwin & Ahn, 2013; Hall & Burns, 2018) – at least for at-risk readers without ADHD.
Nevertheless, by nature of their neurodevelopmental diagnosis, children with ADHD are at an increased risk for attentional, behavioral, and neurocognitive difficulties that may impact learning – i.e., it is likely that reading problems in ADHD are due, at least in part, to interfering behaviors or alternate underlying causes rather than solely the skill-based deficits targeted by extant reading interventions (e.g., Aduen et al., 2018; Kofler et al., 2018). As such, (a) at-risk readers with ADHD may be less responsive to reading interventions than their non-ADHD peers (Ron Nelson et al., 2003; Rabiner et al., 2004), to the extent that reading difficulties are caused/maintained by different underlying mechanisms for children with ADHD than they are for children without ADHD; and (b) the effectiveness of the core components of these interventions may vary for children with and without ADHD. Indeed, the ADHD reading intervention literature is characterized by high levels of variability in outcomes, with some studies reporting that reading interventions are highly effective (e.g., g = 2.14; Lane et al., 2001), while other studies report minimal (e.g., g = 0.15–0.23; Gum, 2003) and even iatrogenic (e.g., g= −0.86; Hendricks, 2020) treatment outcomes.
This heterogeneity may reflect the wide range of methodologies and interventions studied. For example, intervention dosage—though a nonsignificant predictor of reading intervention efficacy in studies not recruiting based on ADHD status (Hall & Burns, 2018; Okkinga et al., 2018)—may affect reading intervention outcomes for children with ADHD (e.g., Miller et al., 2013). The hypothesized benefits of higher intervention dosage for children with ADHD may occur because children with ADHD are off-task during academic instruction about 25% of the time (Kofler et al., 2008), and demonstrate more frequent moment-to-moment shifts between attentive and inattentive behavior (Rapport et al., 2009; Kofler et al., 2008). In that context, it stands to reason that they may need to spend more time in treatment to obtain the same results as their more attentive peers.
Similarly, it has been hypothesized that adding ADHD treatment (e.g., behavioral management, psychostimulant medication) to reading interventions should produce greater improvements in reading by reducing the interfering effects of ADHD behaviors on learning (Williamson et al., 2014; Bental & Tirosh, 2008). However, the available evidence suggests that combining psychostimulant medication and/or behavioral management training with reading interventions yields no incremental benefits on reading outcomes relative to reading intervention alone (e.g., Denton et al., 2020; Tannock et al., 2018; Tamm et al., 2017; Strong Hilsmier et al., 2016).
ADHD reading intervention studies also differ markedly in terms of how they assess efficacy (e.g., standardized achievement tests versus study-developed/curriculum-based measures of reading); which component(s) of reading they target (e.g., phonetic decoding versus reading comprehension); the presence and quality of their control group(s); as well as the rigor of their ADHD diagnostic method (e.g., single-informant/method versus gold-standard multi-informant/method) – all of which have been shown to affect estimates of ADHD-related impairments and/or response to intervention in prior meta-analyses (e.g., Kofler et al., 2008; Alderson et al., 2007). A meta-analysis is clearly needed to determine the extent to which reading interventions work for at-risk readers with ADHD, as well as examine intervention-specific, methodological, and child factors that may maximize the efficacy of reading interventions for this population.
Prior Meta-Analyses
To our knowledge, no prior meta-analyses have examined reading interventions for school-aged children with ADHD specifically. However, two recent meta-analyses reported on reading interventions for struggling readers with emotional and/or behavioral disorders more generally (Benner et al., 2010; Roberts et al., 2020). Both studies found large improvements in word reading and reading comprehension (g=0.90–1.02) but did not directly assess the extent to which these effects held specifically for children with ADHD. Interestingly, while Benner et al. (2010) did not test moderators of treatment outcome, Roberts et al. (2020) found that combining reading intervention with behavioral supports produced significantly smaller improvements in reading (i.e., g=0.26 versus g=1.29), whereas study quality and design, participant grade, and intervention group size did not moderate treatment effects. From these findings, Roberts et al. (2020) concluded that adding behavioral interventions to reading treatment was unsupported. Taken together, both the Benner et al. (2010) and Roberts et al. (2020) meta-analyses supported the use of reading interventions for children with emotional and/or behavioral disorders broadly, but neither review specifically examined the efficacy of reading interventions for children with ADHD.
A partial exception to this critique is a recent meta-analysis of primarily single case design studies by Stewart & Austin (2020), who examined the efficacy of reading interventions that target higher-level reading skills such as comprehension, vocabulary, and fluency for older children with ADHD in grades 4 to 12. The authors found moderate treatment gains across 16 ADHD reading intervention studies (single-subject Tau-U = 0.33–1.19; between group g = 0.41–2.63). However, while Stewart & Austin’s (2020) study represents an important initial step, the conclusions that can be drawn from this study appear limited due to their restricted sample size (65 total participants across 16 included studies) and exclusion of studies targeting key lower-order reading skills (e.g., decoding; Foorman et al., 2016). Similarly, Stewart and Austin’s (2020) conclusion that reading interventions do not meet criteria as an evidence-based practice for children with ADHD warrants scrutiny due to their restrictive inclusion criteria, which resulted in the exclusion of all three randomized control trials (RCT) published during their specified dates of review. In addition, the authors excluded studies that included children younger than 4th grade, which may significantly limit conclusions that can be drawn given (a) evidence from non-ADHD samples that earlier reading intervention is likely to produce more robust improvements (Goodwin & Ahn, 2013; Hall & Burns, 2018), and that (b) the majority of research on reading interventions for children with ADHD has been conducted with samples that include children both younger and older than 4th grade (e.g., Tamm et al., 2017; Tannock et al., 2018).
Current Study
Taken together, reading problems are highly prevalent in children with ADHD (Daucourt et al., 2020; Willcutt et al., 2010), and untreated ADHD-related reading difficulties portend adverse near- and long-term behavioral (Fergusson & Lynskey, 1997; Bennett et al., 2003), academic (McGee et al., 2002), and occupational difficulties (Maughan et al., 1985). However, evidence-based treatments targeting ADHD behavioral symptoms generally do not produce downstream improvements in reading skills as noted above, and the evidence for reading-specific interventions for this high-risk population is surprisingly mixed.
The current meta-analysis systematically examined both peer-reviewed and unpublished literature to (a) quantify the extent to which reading interventions are effective for at-risk readers with ADHD; (b) investigate participant, study quality and design, and intervention characteristics associated with maximum improvement in reading skills for children with ADHD; and (c) evaluate the extent to which reading interventions can be classified as an evidence-based treatment for children with ADHD based on both clinical (Evans et al., 2018) and special education (Cook et al., 2015) standards.
Based upon the attentional, behavioral, and neurocognitive difficulties associated with ADHD that impact reading skill acquisition and performance (Kofler et al., 2019; Rucklidge & Tannock, 2002), we hypothesized that extant reading interventions would be effective for children with ADHD, but at a smaller magnitude than seen in children without ADHD. To our knowledge, no previous review has examined moderators of reading intervention efficacy for children with ADHD. However, based on prior work demonstrating minimal/no direct benefits of psychostimulant medication and behavioral treatment on academic outcomes (e.g., van der Oord et al., 2008), we hypothesized that adding ADHD treatment to reading intervention would not provide additive benefits relative to reading intervention alone. Finally, based on the influential ‘simple view of reading’ model (e.g., Lonigan et al., 2018) we hypothesized that interventions targeting decoding and/or language comprehension skills would be associated with greater reading improvements than interventions targeting other aspects of reading.
2. Method
2.0. Transparency and openness
We report how we determined our sample size, all data inclusion/exclusion criteria, all manipulations, and all measures in the study (Simmons et al., 2012). The meta-analysis was not preregistered; we transparently report our a priori plan and minor changes made after accessing the data below. Data were analyzed using the R statistical program “Metafor” package (Rstudio Team, 2020; Viechtbauer, 2010). Study data can be found in Tables 1 and 2.
Table 1.
Participant characteristics
| Study First-Author | N | MEAN AGE (YEARS) /GRADE | % MALE | % MED | IQ | % HIGH SES | % WHITE | % SLD-RD | % ESE | Self-Contained (Y/N) |
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| Clarfield (2005) | 3 | 0 | 1.0 | 0.67 | - | - | 1.0 | - | 0.67 | N |
| Crabtree (2010) | 2 | 2 | 1 | - | - | - | 1 | 1 | 1 | N |
| Denton 1 (2020) | 72 | 1 | 0.67 | 0 | 86.2 | 0.22 | 0.18 | - | 0.36 | N |
| Denton 2 (2020) | 63 | 1 | 0.47 | 1 | 86.7 | 0.27 | 0.23 | - | 0.42 | N |
| Gum (2003) | 8 | 2 | 0.88 | 0.38 | - | - | - | 0.38 | 1 | N |
| Hedin et al. (2011) | 2 | 1 | 1.0 | 1.0 | - | - | - | - | - | N |
| Hendricks 1 (2020) | 4 | 1 | - | - | - | - | - | - | - | N |
| Hendricks 2 (2020) | 7 | 1 | - | - | - | - | - | - | - | N |
| Johnson (2012) | 2 | 2 | 1 | 1 | - | - | 1 | 0 | 1 | N |
| Lane (2001) | 7 | 0 | 0.71 | - | 87.9 | - | 0.57 | - | 0 | N |
| Luckey (2009) | 135 | 1 | - | - | - | - | - | 0 | - | N |
| Raffaele Mendez (2016) | 2 | 0 | 1.0 | - | - | - | 1.0 | - | 0 | N |
| Richardson (1987) | 42 | - | - | 1 | - | - | - | 1 | 0 | N |
| Rogevich (2008) | 15 | 2 | 1 | - | 92.4 | 0 | 0.47 | - | 1 | Y |
| Saddler (2017) | 2 | 1 | 1 | 0.5 | - | - | 0 | - | 1 | Y |
| Shimabukuro (1996) | 3 | 2 | 1 | - | - | - | - | 1 | 1 | Y |
| Strong Hilsmier (2016) | 2 | 1 | 0.5 | - | - | - | - | - | 1 | Y |
| Tamm 1 (2017) | 66 | 1 | 0.47 | 1 | 86.7 | 0.27 | 0.23 | - | 0.42 | N |
| Tamm 2 (2017) | 73 | 1 | 0.67 | 0 | 86.2 | 0.22 | 0.18 | - | 0.36 | N |
| Tannock 1 (2018) | 17 | 0 | 0.83 | 1 | 92.9 | - | - | 1 | 0 | N |
| Tannock 2 (2018) | 10 | 0 | 0.92 | 1 | 90.1 | - | - | 1 | 0 | N |
| Tannock 3 (2018) | 11 | 1 | 0.7 | 0 | 87.1 | - | - | 1 | 0 | N |
| Tannock 4 (2018) | 13 | 0 | 0.64 | 0 | 97.2 | - | - | 1 | 0 | N |
| Walcott (2014) | 3 | 0 | 1 | - | - | - | 0.67 | - | 0 | N |
Note: “-“= not reported; Mean age (years)/grade: 0 = mean age of ≤8.5 years or grades K-2; 1 = mean age of 8.6–11.0 years or grades 3–5 or; 2 = mean age 11+ years or grades 6+; %Male = Percentage of the sample male; %Med = Percentage of the sample taking psychostimulant medication; IQ = standard scores from standardized/norm-referenced IQ tests; SES = socioeconomic status; %White = Percentage of the sample white; %SLD-RD = Percentage of the sample diagnosed with a DSM-V specific learning disorder in reading; %ESE = Percentage of the sample receiving exceptional student education services; Self-Contained (Y/N) = whether students in the sample are placed in a self-contained classroom
Table 2.
Study characteristics
| Study First-Author | Mean Effect (g) | Intervention Target | Treatment Outcome | Treatment Match Outcome (Y/N/Both) | Measure | Diagnostic Rigor (0/1/2) | Read Plus Behavior (Y/N/ Both) | Treatment Format | RCT (Y/N) | Control Group (Y/N) | Treatment Dosage (Min) | Treatment Duration (Weeks) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Clarfield (2005) | 2.03 | Decoding | Decoding | Y | Standardized | 0 | No | Individual | N | N | 800 | 6–9 |
| Crabtree (2010) | 1.55 | Comp | Comp | Y | CBM | 1 | No | Group | N | N | 157.5 | - |
| Denton (2020) | 0.36 | Multi | Both | Y | Standardized | 2 | Both | Group | Y | Y | 2,475 | 16 |
| Gum (2003) | −0.08 | Comp | Both | Both | Standardized | 0 | No | Individual | N | N | 701 | 9–12 |
| Hedin (2011) | 2.19 | Comp | Comp | Y | CBM | 1 | No | Individual | N | N | 420 | 14 |
| Hendricks (2020) | 0.53 | Comp | Both | Both | Standardized | 0 | No | Group | N | N | 700 | 14–15 |
| Johnson (2012) | 2.54 | Comp | Comp | Y | CBM | 1 | No | Group | N | N | 195 | - |
| Lane (2001) | 1.82 | Decoding | Decoding | Y | Standardized | 0 | No | Group | N | N | 900 | 10 |
| Luckey (2009) | 0.80 | Decoding | Decoding | Y | Standardized | 1 | No | Individual | N | N | 6,000 | 12–20 |
| Raffaele Mendez (2016) | 0.67 | Decoding | Both | Both | Standardized | 0 | No | Group | N | N | 2,240 | 16 |
| Richardson (1986) | 0.69 | Decoding | Comp | N | Standardized | 0 | No | Group | N | N | - | - |
| Rogevich (2008) | 2.74 | Comp | Comp | Y | CBM | 1 | No | Group | N | Y | 225 | 1–2 |
| Saddler (2017) | −0.10 | Comp | Comp | Y | CBM | 1 | No | Group | N | N | 210 | 3–4 |
| Shimabukuro (1996) | 2.61 | Comp | Comp | Y | CBM | 1 | No | Group | N | N | 362.5 | 10 |
| Strong Hilsmier (2016) | 0.22 | Decoding | Both | Both | Standardized | 1 | Both | Individual | N | N | 960 | 12 |
| Tamm (2017) | 1.12 | Multi | Both | Y | Standardized | 1 | Both | Group | Y | Y | 2,880 | 16 |
| Tannock (2018) | 0.36 | Decoding | Both | Both | Standardized | 2 | No | Group | Y | Y | 2,100 | 10 |
| Walcott (2014) | 3.18 | Decoding | Decoding | Y | Standardized | 0 | No | Group | N | N | 320 | 4 |
Note: “-“ = not reported; g = hedge’s g; g = 0.2 is a small effect; g = 0.5 is a medium effect; g = 0.8 or greater is a large effect; Comp = comprehension; Multi = multiple reading skills (e.g., decoding + reading comprehension); Treatment Match Outcome (Y/N/Both) = whether target of intervention matched assessed treatment outcome; Standardized = standardized/norm-referenced assessment; CBM = study-developed/curriculum-based measures; Diagnostic Rigor = higher values reflect greater diagnostic rigor; 0 = single informant/questionnaire; 1 = referral/prior diagnoses; 2 = gold standard diagnostic practice; Read Plus Behavior (Y/N) = reading intervention with adjunctive behavioral intervention; RCT (Y/N) = whether intervention study was a RCT; Treatment Format = whether treatment delivered in an individual or small group/combined setting; Control Group (Y/N) = whether study had a control group; Treatment Dosage (Min) = average total minutes of treatment; Treatment Duration (Weeks) = average number of weeks to complete treatment.
2.1. Literature searches
Study selection was conducted following the Preferred Items for Systematic Reviews and Meta-analysis guidelines (PRISMA; Moher et al., 2015; see Figure 1). Multiple search methods were applied to include all relevant literature, not just published articles (McAuley et al., 2000; Rosenthal, 1994). First, comprehensive literature searches of both peer-reviewed studies as well as unpublished dissertations and theses were conducted using PsycINFO, ERIC, and ProQuest Dissertations and Theses. Search terms included permutations of the ADHD diagnostic label (ADHD, attention, hyperactiv*, inattent*, hyperkinesis, impulsivity, minimal brain dysfunction, minimal brain damage, MBD), reading intervention, reading treat*, RTI, response to intervention, and reading instruction. An asterisk after a root word directs search engines to include any derivative of the word that is followed by the asterisk. To avoid missing studies due to database misclassification, no search delimiters were selected. Searches were conducted by the first, second, and third authors (ESMC, JAS, EDH). All included studies were reviewed by at least two of these authors, and disagreements were resolved via discussion after all three authors reviewed the study (100% consensus). After the initial searches, emails were sent to authors of both peer-reviewed studies and unpublished dissertations that examined reading interventions among children with ADHD or elevated ADHD symptoms but did not report sufficient data for effect size calculation (3 of 8 authors did not respond, 4 authors responded and indicated that data were no longer accessible, and 1 author provided the requested data). Studies were additionally identified via (a) referral by experts on academic interventions for children with ADHD as well as (b) from articles cited in prior meta-analyses or systematic reviews on reading interventions for children with ADHD and/or emotional behavioral concerns. Collectively, these procedures generated an initial database of 3,312 items including chapters, peer-reviewed articles, dissertations, and theses written since 1937. All search processes and study recruitment were terminated on June 21, 2021 (Figure 1).
Fig. 1.
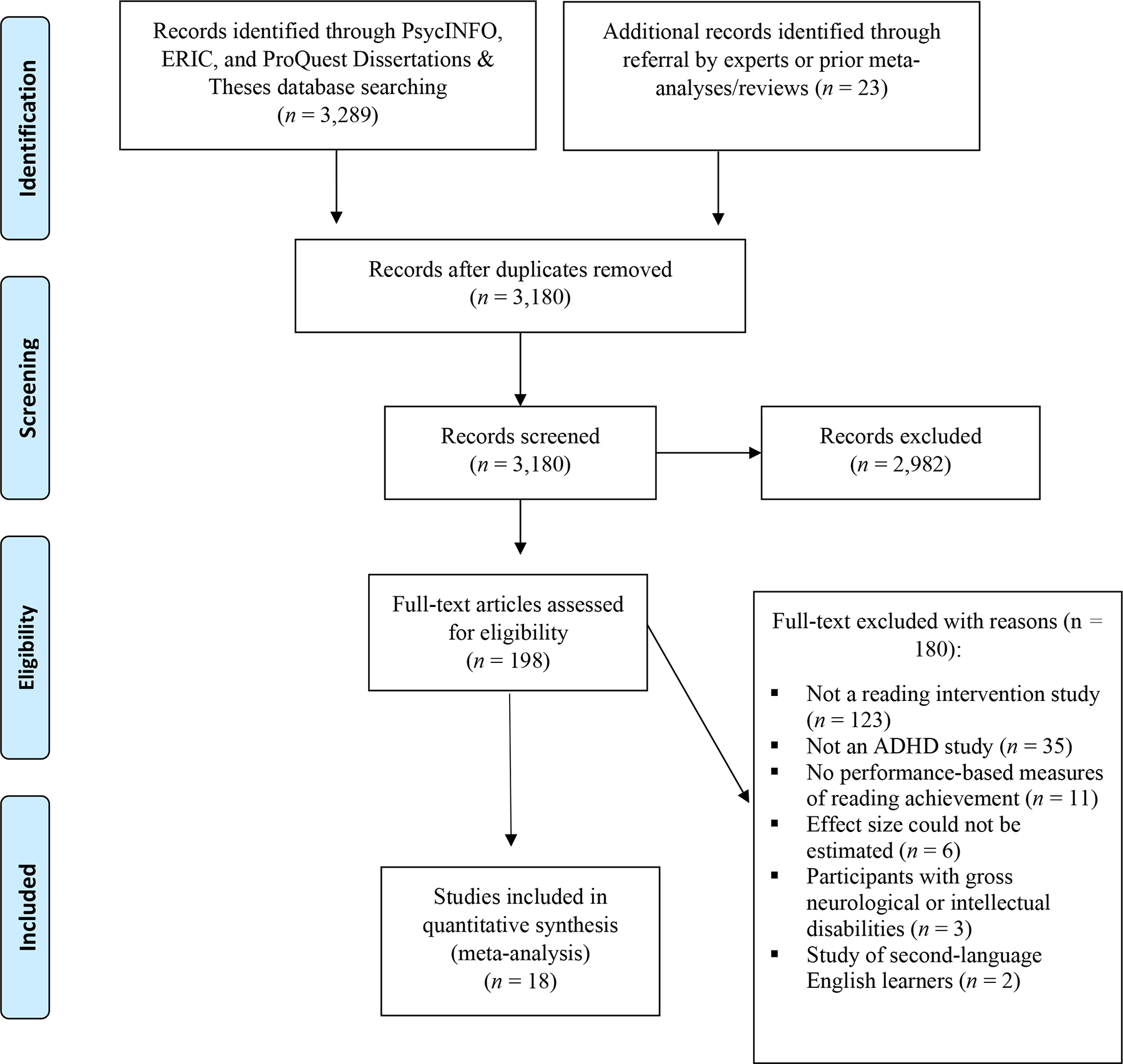
PRISMA flow diagram of included studies.
2.2. Inclusion Criteria
Inclusion and exclusion criteria are described below with the number of studies omitted for each criterion in parentheses. The initial exclusion process included removing duplicates (132) and items that were not empirical studies (e.g., book chapters, letters to the editor, policy briefs, manuals; 787). Among the remaining studies, several studies failed to meet multiple inclusion criteria; the counts below indicate first failed criteria identified. The following served as inclusion criteria for the review: Studies (a) conducted in English (7) that included (b) an intervention targeting a reading skill (2,056) for children and/or adolescents with a diagnosis of ADHD or related labels (e.g., attention problems, hyperactive) and co-occurring reading difficulties (302) that (c) used performance-based measures of reading achievement (11) from which (d) effect sizes could be estimated based on reported data or test statistics or could be obtained from the study author (6). Exclusion criteria included: (a) participants with gross neurological, sensory, or motor impairment, history of a seizure disorder, psychosis, or intellectual disability (3); (b) studies of second-language English learners (2); and (c) single case study designs (6). Single-case study designs were excluded because single-case effect sizes are incompatible with effect sizes derived from between-group studies (Rindskopf et al., 2012), and because they have been summarized recently by Stewart & Austin (2020).
A total of 18 studies (15 peer-reviewed studies, 3 dissertations) published from 1986 to 2020 met all study criteria and were included in one or more sets of analyses.1 Nine of these 18 studies reported data for two or more independent subsamples (defined as ADHD samples with non-overlapping participants), resulting in k = 24 independent samples reporting on N = 564 participants. Several studies reported multiple outcome variables, resulting in a total of 57 pre-post intervention effect sizes (1–5 effect sizes per independent sample).
2.3. Coding of moderators
All potential moderator variables were coded by the first and second authors according to the characteristics reported in Tables 1 and 2. Each study was coded on several domains (defined below), including subject characteristics, study design and treatment characteristics, and outcome measures. Continuous variables were used whenever possible (Hedges & Pigott, 2004). Fifty percent of studies were double-coded by the first and second authors for reliability, which was excellent (r = .997); discrepancies were resolved collaboratively.
2.3.1. Study and sample characteristics
Study characteristics were defined as follows: continuous demographic variables included publication year and the percentage of each sample who were (a) taking psychostimulant medication for ADHD and (b) receiving exceptional student education (ESE) services based on each study’s chosen indicator. Most studies defined ESE status in terms of whether children had a pre-existing Individualized Education Plan (IEP), received additional help from a paraprofessional, or were diagnosed with reading disability. In addition, a subset of studies included children placed in a self-contained classroom, which was coded as an additional dichotomous variable given that this reflects a more restrictive educational placement that may reflect more severe learning and/or behavioral difficulties (Fuchs & Fuchs, 2006).
A publication year of 2020 was assigned for studies where unpublished data were provided by authors. For child age/grade, a continuous measure was not feasible due to inconsistent reporting across studies. As such, an ordinal variable was created by splitting studies into 3 approximately equal groups (0 = Grades K-2 or mean age of ≤8.5 years; 1 = Grades 3–5 or mean age of 8.6–11.0; 2 = Grades 6+ or mean age 11+ years). We also initially coded child IQ (reported in only k = 12 of 24 samples), SES (k = 5 of 24 samples), race/ethnicity (k = 11 of 24 samples), and co-occurring reading disability status (k = 12 of 24 samples) but these factors could not be examined as potential moderators due to limited reporting across studies/samples.
Diagnostic method was coded ordinally as an index of study quality based on the recommendations for gold standard diagnosis of ADHD in prior meta-analytic reviews (e.g., Alderson et al., 2007; Kofler et al., 2008, 2016; Lipszyc & Schachar, 2010), with higher values reflecting more rigorous diagnostic procedures: 0 = referral or prior diagnosis only; 1 = single informant rating scale and/or interview; 2 = multiple informants and settings (multiple informant report based on standardized/norm-referenced questionnaires and/or clinical interviews). We also initially coded additional indices of study rigor including (a) use of a randomized control trial design, (b) inclusion of any control group, and (c) inclusion of a gold-standard active, credible control group (all 0=No; 1=Yes). However, these variables were found to be multicollinear with diagnostic method (and each other) and were therefore excluded (i.e., studies using gold standard ADHD diagnostic practices also tended to include active, credible control groups and RCT methods; r>.90, p<.001). Diagnostic method was retained over these alternate indices of study quality because our primary aim was to quantify reading intervention outcomes unique to children with ADHD, and less rigorous diagnostic practices have been shown to produce ‘ADHD’ groups that contain a large percentage of children without ADHD (e.g., Alderson et al., 2007; Sciutto et al., 2007). Nonetheless, given this multicollinearity, we focus our interpretation of this moderator on both diagnostic and methodological quality in the Discussion.
2.3.2. Intervention and outcome characteristics
Intervention dosage was coded as a continuous variable based on the mean (or midpoint for studies only reporting a range) number of minutes of intervention. Two variables were coded to assess the potential incremental benefits of adding ADHD treatment to reading interventions: (a) Intervention type was coded as 0 = “reading intervention only” vs. 1 = “reading intervention + behavioral treatment”; and (b) the percentage of the sample who received psychostimulant medication during treatment as described above.
All other intervention characteristics were coded dichotomously/dummy coded: Intervention target (Decoding/Phonemic Awareness, Multicomponent, or Reading Comprehension) was dummy coded as a set of k-1 variables with Decoding/Phonemic Awareness as the reference variable. Studies were coded as Multicomponent if they targeted multiple reading skills (e.g., decoding + reading comprehension). Intervention outcome was coded as 0 = “simple view of reading component skills” (i.e., decoding skills) vs. 1 = “reading comprehension”. Intervention target and outcome were coded based on the simple view of reading model as described above (Lonigan et al., 2018). We had intended to also include language comprehension here, but none of the included studies directly targeted non-print-based understanding of language. We also created a dichotomous variable to code whether the treatment target matched the treatment outcome (0=No; 1=Yes) given the expectation that ‘near transfer’ gains on skills directly taught in the intervention would be greater than ‘far transfer’ gains on skills not explicitly taught in the intervention (e.g., Simons et al., 2016).
Finally, we coded whether each study assessed intervention effects using standardized measures of reading achievement (coded as 0) or curriculum-based measures of reading skills (coded as 1). We expected that curriculum-based measures would be associated with larger effect sizes given that they are study-created to match the intervention content, whereas standard scores from norm-referenced tests would be associated with smaller effect sizes given that they were not developed to assess change and may be particularly insensitive to detecting intervention effects for children with neurodevelopmental disorders (see Farmer et al., 2020). We had intended to also code whether studies reported outcomes based on item response theory-based growth scale values or person ability scores (which are based on the same norming samples as standard scores but were developed explicitly to assess response to intervention; Farmer et al., 2020; Kaufman & Kaufman, 2014), but no studies used this preferred metric.
Delivery format (individual = 0 vs. group or combined group+individual = 1) was also coded initially, but was multicollinear with exceptional student education (ESE) status (i.e., studies with higher proportions of children with ESE status tended to deliver the intervention individually, presumably due to the more impaired nature of the sample; r=.80, p<.001). ESE status was retained given prior evidence that ESE status may be associated with smaller academic gains (Bussing et al., 2012).
2.4. Computation of effect sizes
Means, SDs, and sample sizes for each group were used to compute Hedges’ g effect sizes using the R statistical program “Metafor” package (Rstudio Team, 2020; Viechtbauer, 2010). For one study (Richardson, 1986), means and SDs were unavailable and thus effect sizes were estimated using the reported sample size and p-value (Alderson et al., 2007). Hedges’ g effect sizes are Cohen’s d effect sizes corrected for study sample size due to the upward bias in effect size magnitude of small N studies (2013). An effect size of 0.20 is considered small, 0.50 is medium, and 0.80 is large (Cohen, 2013). A random effects model was chosen due to the wide variance in reading outcomes and intervention types. The random effects model weights each effect size by its inverse variance weight (1/SE2) to correct for study-level sampling error as recommended (Hunter & Schmidt, 2004; Lipsey & Wilson, 2001).
2.4.1. Missingness
For all studies, Hedges’ g values were either computed given the data presented within the article (k = 51) or were provided directly from the article author (k = 6). For 2 studies, estimates of variance were not reported, but were instead estimated using multiple imputation as laid out by van Buuren (2018) so that these effect sizes could be used for subsequent analyses. Multiple imputation was done using the “MICE” package in R (van Buuren & Groothuis-Oudshoorn, 2011), which has been effectively used to account for missing data in other meta-analytic projects (e.g., Jolani et al., 2012). Missingness was also an issue for several moderators within this project, and as such multiple imputation using the same process and package was used to impute missing values on a sample-by-sample basis. To limit bias from multiple imputation, a 50% cutoff of missingness was used to determine which variables were eligible for multiple imputation as recommended (Mishra & Khare, 2014; Lee & Huber, 2011; Lee & Carlin, 2012). As such, variables with missingness of 50% of independent samples or greater were excluded from use as noted above (i.e., IQ, SES, ethnicity, and percentage of the sample with co-occurring reading disability); all other potential moderators were reported in at least 94% of independent samples and therefore missingness was handled via multiple imputation as described above.
2.4.1. Publication bias: the file drawer problem
To assess for publication bias, three separate analyses were conducted. First, results were visualized using a funnel plot. Next, Egger’s (1997) test was computed for detection of publication bias. Finally, the fail-safe N was computed (Rosenthal, 1979). The fail-safe N represents the number of studies with null effects that would have to be included in the analysis to significantly reduce the obtained effect size enough that its corresponding p-value becomes non-significant.
2.4.2. Moderator analyses
Potential moderators were examined via the R package “Metafor” (Rstudio Team, 2020; Viechtbauer, 2010). Several studies produced multiple effect sizes, and thus a three-level (multi-level) modeling approach was selected to account for nesting of effect sizes as recommended (Assink & Wibbelink, 2016). The three-level model separates the proportion of variance attributable to the study, sample, and individual level for each effect size. The three-level model was selected over traditional meta-regression, as (a) the former allows for the inclusion of multiple effect sizes from a single study while controlling for dependency between effect sizes and (b) importantly avoids the artificial decrease in heterogeneity that occurs when averaging effect sizes within studies (Cheung, 2014; Hox, 2010).
3. Results
3.1. Overview
Publication bias was assessed, followed by heterogeneity tests and then tests of moderators when warranted. Next, ‘best case’ estimates were computed based on the results of the moderator meta-regression (Lipsey & Wilson, 2001). Finally, the included studies were scrutinized using established criteria to determine whether reading interventions could be considered evidence-based practice for at-risk readers with ADHD (Evans et al., 2018; Cook et al., 2015).
3.2. Publication bias
Visual inspection of the stem-and-leaf histogram of obtained effect sizes (Table 3) indicated clear differences between studies based on outcome test selection (i.e., standardized/norm-referenced academic achievement tests versus study-developed/curriculum-based academic skill measures). Overall, however, the funnel plot indicated a fairly symmetrical distribution of effect sizes across studies indicating no evidence of publication bias. Similarly, neither the Egger’s test (z = 1.94, p>.05) nor the fail-safe N = 2,418 provided significant evidence of publication bias.
Table 3.
Histogram of Hedges’ g Effect Sizes
| Stem | Effect Size | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| 4 | 4.60 | |||||||||
| … | ||||||||||
| 2 | 2.03 | 2.14 | 2.19 | 2.54 | 2.61 | 2.74 | ||||
| … | ||||||||||
| 1 | 1.24 | 1.50 | 1.55 | 1.76 | 1.79 | |||||
| 0.9 | 0.97 | 0.98 | ||||||||
| 0.8 | 0.80 | 0.83 | ||||||||
| 0.7 | 0.70 | 0.78 | ||||||||
| 0.6 | 0.61 | 0.69 | ||||||||
| 0.5 | 0.51 | 0.52 | 0.53 | 0.58 | ||||||
| 0.4 | 0.40 | 0.42 | 0.43 | 0.44 | 0.45 | 0.46 | 0.47 | |||
| 0.3 | 0.32 | 0.33 | 0.34 | 0.34 | 0.36 | 0.38 | 0.38 | 0.39 | ||
| 0.2 | 0.21 | 0.23 | 0.23 | 0.23 | 0.24 | 0.25 | 0.28 | |||
| 0.1 | 0.11 | 0.15 | 0.15 | 0.16 | ||||||
| 0 | ||||||||||
| −0 | −0.02 | −0.03 | −0.10 | |||||||
| −0.1 | ||||||||||
| −0.2 | −0.27 | |||||||||
| −0.3 | ||||||||||
| −0.4 | −0.43 | −0.47 | ||||||||
| −0.5 | ||||||||||
| −0.6 | −0.61 | |||||||||
| −0.7 | ||||||||||
| −0.8 | −0.86 | |||||||||
| −0.9 | ||||||||||
Note. Histogram of effect sizes across studies. The left column reflects the ones and tenths digits, and the right columns reflect each obtained effect size. Each entry indicates one unique effect size. Bold font represents curriculum-based measures and un-bolded font represents standardized measures. Italic font indicates that the treatment targeted decoding skills. Positive values indicate positive treatment gains.
3.3.1. Tier I: Overall (moderator independent) estimate of reading intervention efficacy
Reading interventions produced overall large magnitude benefits for children with ADHD (g = 0.96, 95% CI [0.56, 1.36]). However, the overall test of heterogeneity was significant (Q[56]=152.46, p <.0001), with a large proportion of this variability (40.9%) attributable to between-study differences. This heterogeneity indicated that the overall effect size was likely not the best estimate of reading intervention efficacy for children with ADHD and supported the examination of potential moderators.
3.3.2. Tier II: Study, treatment, and demographic moderators of between-study differences
Outcome test selection.
Outcome test selection (i.e., standardized/norm-referenced tests vs. study-developed/curriculum-based measures) was tested first as a potential moderator because visual inspection of the data indicated clear differences in effect sizes based on this study characteristic as noted above (Table 2). As expected, test selection was a significant moderator (p = .001), with curriculum-based measures (g = 1.91, 95% CI [0.92, 2.89]) associated with significantly larger effect sizes than norm-referenced achievement tests (g = 0.66, 95% CI [0.37, 0.95]).
The overall test of heterogeneity was not significant for studies that used curriculum-based measures (k = 7; n = 30; Q[6] = 7.87, p = 0.25), indicating that g = 1.91 is the best estimate for reading improvements as assessed by study-created/curriculum based measures of the specific skills trained during the interventions (i.e., additional moderator analyses for these studies were not warranted). In contrast, significant heterogeneity remained among studies using standardized/norm-referenced outcome tests (k = 50; n = 538; Q[49] = 123.04, p < .0001), suggesting that g = 0.66 is likely not the best estimate of reading intervention efficacy for these outcomes and supporting the examination of additional moderators to provide a more accurate estimate of the extent to which the skills gained from reading interventions produce ‘downstream’ improvements on reading achievement.
Moderators of reading intervention efficacy as assessed by standardized/norm-referenced outcome tests.
As shown in Table 4, results of the 3-level meta-regression where all moderators were entered into a single regression indicated that better diagnostic methods (and better study methodology given the multicollinearity described above; p<.001), inclusion of students in self-contained classrooms (p=.006), and higher intervention dosage (i.e., more minutes; p=.003) were each associated with significantly smaller estimates of reading intervention efficacy. In contrast, interventions that targeted decoding/phonemic awareness yielded significantly larger benefits relative to interventions that targeted reading comprehension (decoding vs. reading comprehension: p<.01), whereas training additional skills beyond decoding failed to produce incremental benefits relative to just training decoding skills (decoding vs. multicomponent: p=.50, ns).
Table 4.
Overall effects and Moderators of Effects
| k | Hedges’ g | 95% CI | |
|---|---|---|---|
|
| |||
| Overall Hedges’ g effect size | 57 | 0.96 | 0.56 to 1.36 |
| CBM measures | 7 | 1.91 | 0.92 to 2.89 |
| Standardized measures | |||
| Overall (moderator independent) effect | 50 | 0.66 | 0.37 to 0.95 |
| Moderated (best case) estimate | 50 | 1.11 | -- |
| B-weights | 95% CI | ||
| Moderated Hedges’ g effect sizes for Standardized Outcome Tests | |||
| Intercept | 3.54 | ||
| Sample Characteristics | |||
| Age | −0.09 | −0.72 to 0.53 | |
| Medication status (%) | 0.03 | −0.41 to 0.47 | |
| ESE status (%) | −0.30 | −1.32 to 0.71 | |
| Self-contained classroom (N/Y) | −2.03 | −3.43 to −0.63** | |
| Study Characteristics | |||
| Diagnostic Rigor | −0.89 | −1.15 to −0.62*** | |
| Intervention Target (Dummy Coded) | |||
| Reading Comprehension vs. Decoding | −1.26 | −2.20 to −0.32* | |
| Multicomponent vs. Decoding | 0.15 | −0.29 to 0.58 | |
| Outcome Characteristics | |||
| Treatment outcome | 0.13 | −0.13 to 0.39 | |
| Treatment target matches treatment outcome (N/Y) | 0.29 | −0.12 to 0.69 | |
| Intervention Characteristics | |||
| Added Behavioral Treatment (N/Y) | 0.16 | −0.33 to 0.65 | |
| Treatment Duration (minutes) | −0.35 | −0.57 to −0.13** | |
Note. Effect sizes are considered significantly different from 0.0 (statistically significant at p < .05) if their 95% confidence interval does not include 0.0. The best-case estimate reflects expected benefits of reading treatments with 30+ intervention hours targeting decoding skills for children with rigorously diagnosed ADHD placed in regular education classrooms.
k = number of included studies
p<.01
p<.001
No other significant moderators were found, suggesting that reading intervention benefits for at-risk readers with ADHD do not vary according to child age/grade (range 6–18 years/1st-12th grade; p=.77), assessed reading skill outcome (p=.31), or whether the skill(s) targeted by the treatment matched the skill(s) assessed by the outcome test (p=.16). In addition, adding ADHD treatment failed to produce incremental gains in reading as evidenced by the nonsignificant effects for both medication (p=.88) and behavioral treatment (p=.50). After accounting for all tested moderators, no significant variance remained to be explained at the study, sample, and individual level (p=.07).
3.3.3. Tier III: Best Case Estimation
Next, ‘best case’ estimates (Lipsey & Wilson, 2001) were calculated based on the Tier II moderator results. For studies using curriculum-based outcome tests, there was no significant heterogeneity, indicating that the very large effect size of g = 1.91 is the best estimate for improvements in the specific reading skills directly trained by these interventions. For studies using standardized/norm-referenced outcome tests, the best case estimate was obtained by solving the Tier II meta-regression equation using values for each significant moderator corresponding to empirically-supported best practice (e.g., Kofler et al., 2008). The best case metric is value neutral – it does not imply whether lower or higher values are desirable – and facilitates conclusions concerning overall improvements on standardized tests of reading skills for children with ADHD (Lipsey & Wilson, 2001).
As described above, the current findings indicate that reading intervention efficacy varies according to diagnostic rigor/study quality, intervention target, minutes of intervention, and whether participants were placed in a self-contained classroom. For diagnostic rigor, we selected the value corresponding to gold-standard/multi-informant methods given that this reflects higher study quality and confidence that children in the ADHD group in fact have ADHD (e.g., Sciutto et al., 2007). For intervention target, we selected studies targeting decoding/phonemic awareness rather than reading comprehension given that the former is associated with better outcomes and reflects a recommended treatment target based on the influential ‘simple view of reading’ model (e.g., Lonigan et al., 2018). For intervention duration, we selected the mean for this variable across included studies (1,800 minutes/30 hours). For classroom type, we selected the value corresponding to general education classroom placement given that most children with ADHD receive services in general education classrooms (Fuchs & Fuchs, 2006).
Solving the regression equation using these values and their corresponding B-weights (Table 4) indicates that, on average, reading interventions are likely to produce large magnitude improvements on standardized/norm-referenced tests of reading achievement for groups of children with rigorously diagnosed ADHD in regular education classrooms who receive at least 30 hours of reading intervention that targets decoding/phonemic awareness skills (g = 1.11).
3.3.4. Tier V: Critical Evaluation of the Extent to Which Reading Interventions Meet Established Criteria for Evidence-Based Practice for Children with ADHD
Finally, we evaluated each study based on its intervention targets and the established criteria for evidence-based practice in (a) Clinical Psychology and (b) Special Education. In the clinical psychology literature, the Chambless & Hollon (1998) criteria are used to determine degree of evidence-base (Evans et al., 2018). Based on these criteria, of the 18 studies examined in this review only three reading interventions (Denton et al., 2020; Tamm et al., 2017; Tannock et al., 2018) met all 5 of the Methods criteria, were randomized controlled trials, were collectively conducted by at least two independent investigatory teams in independent settings (Denton/Tamm, Tannnock), and all demonstrated greater effects as compared to already well-established treatments for ADHD. Consistent with our best case findings above, all three trials targeted decoding skills and included at least 30 hours of intervention. Thus, based on the Chambless criteria, decoding interventions to improve reading outcomes meet all criteria to be considered a Level 1: Well-Established Treatment for school-aged, at-risk readers with ADHD.
In the special education literature, the well-established Council for Exceptional Children Evidence-based Practices in Special Education two-step criteria for evidence-based practice is used (CEC EBP; Cook et al., 2015). Based on these criteria, the same three studies (Denton et al., 2020; Tannock et al., 2018; Tamm et al., 2017) were the only interventions that met the necessary Step 1 quality indicators (QIs) for all assessed areas including Context and Setting, Participants, Intervention Agents, Description of Practice, Implementation Fidelity, Internal Validity, Outcome Measures/Dependent Variables, and Data Analysis. In Step 2, these studies also collectively satisfied all 3 evidence-based practice criteria, including (a) at least 2 methodologically sound randomized controlled trials with positive effects, with (b) minimum 60 total participants across studies, and (c) no negative effects. As noted above, all three trials (Denton et al., 2020; Tannock et al., 2018; Tamm et al., 2017) targeted decoding and consisted of at least 30 hours of intervention. As such, based on CEC EBP criteria, decoding interventions to improve reading outcomes meet all criteria to be considered an Evidence-Based Practice with Strong Research Support for school-aged, at-risk readers children with ADHD.
Discussion
The present study was the first to systematically quantify the benefits of reading interventions for at-risk readers with ADHD and co-occurring reading difficulties. Utilizing a multilevel meta-analytic approach (Assink & Wibbelink, 2016), we obtained a large overall effect size of g = 0.96. However, significant heterogeneity was detected, such that study-developed/curriculum-based measures (g = 1.91) yielded larger treatment effects than studies that utilized standardized outcome measures, rigorous ADHD diagnostic standards, and interventions that consisted of at least 30 hours of reading intervention that targets decoding/phonemic awareness (g = 1.11). In contrast to our hypothesis, the overall effect of reading interventions for children with ADHD was generally greater than the overall effect found for reading interventions in studies that did not specifically recruit for children with ADHD (e.g., g = 0.21–0.95; Swanson, 1999; Gersten et al., 2020; Hall & Burns, 2018; Scammacca, 2007, 2015), and instead more comparable to the large magnitude benefits of reading interventions previously reported in meta-analyses of children with behavioral/emotional difficulties more generally (g = 0.90–1.02; Benner et al., 2010; Roberts et al., 2020). These results excitingly suggest that children with ADHD may benefit as much, or potentially even more, from extant reading interventions as their non-ADHD peers despite the well-known neurocognitive and behavioral risks associated with the disorder. Furthermore, critical evaluation of the included studies based on established criteria from influential professional societies indicates that decoding interventions meet all established criteria to be considered well-established, evidence-based practices based on both clinical and special education criteria (Cook et al., 2015; Evans et al., 2018). Collectively, our findings suggest the provision of at least 30 hours of targeted decoding/phonemic awareness intervention can be highly effective for treating ADHD-related reading difficulties.
In terms of factors that affect the efficacy of reading interventions for children with ADHD, aligned with prior meta-analytic evidence (e.g., Scammacca et al., 2015; Swanson, 1999) our best case estimates indicated that study-developed/curriculum-based measures (g=1.91) produced larger estimates of reading intervention efficacy than standardized/norm-referenced tests (g=1.11). Our current view is that the true magnitude of reading intervention benefits for children with ADHD likely lies somewhere in between these two estimates. That is, the curriculum-based estimate is likely inflated by the use of study-created (often psychometrically unvalidated) measures that may be too similar to the training content to accurately assess the transfer of training gains to reading skills more generally (e.g., Simons et al., 2016). In turn, the standardized test estimate is likely deflated because norm-referenced test scores are relatively insensitive to change – particularly for children with neurodevelopmental disorders such as ADHD who do not make gains at the same rate as the neurotypical children who comprise the test standardization sample (e.g., Farmer et al., 2020). In contrast, person-ability scores (e.g., growth scale values; Kaufman & Kaufman, 2014) are based on the same normative sample used to construct standard scores, but are developed using item response theory specifically to assess response to intervention. Unfortunately, none of the included studies used this preferred metric, despite frequent calls for increased scrutiny regarding the reliability, validity, and sensitivity of standardized/norm-referenced measures for assessing reading intervention gains (National Reading Panel, 2000; Paris & Stahl, 2005). We strongly recommend that future studies report and analyze the preferred growth scale/person-ability scores when assessing change over time/response to intervention.
Whereas studies using curriculum-based measures produced highly consistent results (6 of 7 effect sizes fell between g=1.5 and 2.7), studies using standardized tests differed widely in terms of the reading intervention efficacy (Table 3). The current meta-analysis identified several participant, treatment, and study characteristics that accounted for this between-study variability. First, higher quality studies that used gold-standard, multi-informant assessment procedures and randomization/active control conditions produced significantly smaller effect sizes than studies using less rigorous diagnostic/control methods. These results are consistent with prior ADHD meta-analyses showing that higher study quality and diagnostic rigor are typically associated with smaller effects (Kofler et al., 2008; Alderson et al., 2007), and also consistent with the intervention literature more broadly (e.g., Simons et al., 2016). Previous meta-analyses have hypothesized that the larger effect sizes associated with less rigorous ADHD diagnostic procedures likely reflect the inadvertent inclusion of children without ADHD in the ‘ADHD’ groups in these studies (Kofler et al., 2008). However, this explanation seems unlikely in the current study given that our overall effect suggests reading interventions tend to be more effective for children with ADHD than children without ADHD. A more likely explanation reflects the multicollinearity between diagnostic rigor and study quality identified in our preliminary analyses. That is, it is well known that effect sizes are inflated in studies with designs that are unable to control for expectancies, maturation, and other threats to validity, and as such it is unsurprising that smaller effects are obtained when these confounds are removed.
Next, we found that interventions targeting decoding/phonemic awareness yielded significantly larger benefits than interventions directly targeting reading comprehension, whereas training additional skills beyond decoding fail to produce incremental benefits relative to training decoding skills only. This pattern of results was consistent regardless of whether the skill targeted in treatment matched the skill assessed by the outcome test, and was consistent with meta-analytic evidence for school-aged children broadly indicating that adding reading comprehension instruction does not produce incremental benefits relative to interventions that specifically target foundational reading skills (e.g., decoding/phonological awareness; Denton et al., 2022). Collectively, our results suggest that interventions targeting phonemic decoding are likely to produce larger reading gains for at-risk readers with ADHD than interventions targeting reading comprehension, irrespective of whether the treatment goal is to improve decoding or reading comprehension skills. These findings are consistent with predictions from the influential ‘simple view of reading’ model (e.g., Lonigan et al., 2018), which posits that children’s reading comprehension skills can be entirely explained by their decoding and language comprehension skills. Notably, however, no intervention in the current study directly targeted language comprehension (i.e., non-print-based understanding of language). Future study on reading interventions that target both components of the simple view of reading may lead to treatments that provide optimal reading outcomes for children with ADHD.
Unexpectedly, higher treatment dosages were associated with significantly smaller treatment effects. Interestingly, this counterintuitive association has also been found in prior studies, and has been hypothesized to be a product of higher quality studies delivering larger dosages of instruction (e.g., Hall et al., 2017; Scammacca et al., 2015; Tran et al., 2011; Wanzek et al., 2010). However, this hypothesis was not supported in the current meta-analysis because the negative effect of higher treatment dosage was significant over and above the effect of diagnostic rigor/study quality. Instead, we hypothesize that higher intervention dosage may be a marker for the inclusion of more severely reading disabled children (Daniel et al., 2021; Vaughn et al., 2003). Unfortunately, however, we were unable to analyze reading disability status or baseline reading level as moderators due to insufficient reporting across included studies, as noted above. With that said, it is important to note that the reading interventions included in the present review can be considered highly intensive, with treatments including on average 30 hours of intervention (range = 3.5–100 hours) within the average span of 10–11 weeks (range = 1–20 weeks). It will be important for future work to specifically assess optimal treatment duration (which may be dependent on comorbidities or other prognostic indicators) for at-risk readers with ADHD and whether more vs. less intensive treatments are needed.
Finally, adding ADHD-specific behavioral treatment or medication to reading interventions failed to provide incremental reading benefits for children with ADHD. These results differed from Roberts et al. (2020), who found that adding behavioral supports to reading interventions produced significantly smaller improvements in reading for children with emotional/behavioral disorders broadly. In contrast, our findings are firmly aligned with the breadth of research demonstrating that reductions in the hypothesized core domains of ADHD (i.e., inattention, hyperactivity-impulsivity) via behavioral management or psychostimulant medication do not lead to, or at best provide minimal, downstream effects on academic achievement (Rapport et al., 2000; van der Oord et al., 2008). Of course, most if not all reading interventions likely include some behavioral components (e.g., redirecting attention back to the training materials, reinforcing reading skill practice). In that context, these findings suggest that adding ADHD-specific treatments to target interfering behaviors does not provide adjunctive benefits on reading outcomes for children with ADHD (Froehlich et al., 2018) over and above the typical behavioral management strategies used when working with children. Importantly, however, none of the included studies directly targeted the academic enablers or skills (e.g., organization, task engagement, and study skills) that support academic functioning for children with ADHD (DuPaul et al., 2004; Evans et al., 2016; Gallagher & Abikoff, 2014). Future reading intervention research may benefit from evaluating the potential additive effects of contingency/behavior modification plans that provide immediate corrective feedback, individualized attention, and frequent reinforcement of these academic enablers during reading intervention given their association with better academic achievement broadly (DuPaul et al., 2004; Evans et al., 2016; Gallagher & Abikoff, 2014).
Limitations
The results of this meta-analysis demonstrate that reading interventions produce robust improvements in reading skills for at-risk readers with ADHD. Strengths of our study include the use of three-level meta-analytic modeling to deal with dependencies across effect sizes (Assink & Wibbelink, 2016), use of best case estimation, as well as critical evaluation of included studies relative to established clinical and special education evidence-based practice criteria. The present study was also the first to examine participant, study, and treatment moderators of reading intervention effects for children with ADHD. Despite these methodological refinements, the following limitations must be considered when interpreting results. First, due to inconsistent reporting across included studies, we were unable to examine several potentially relevant moderators, including SES, race/ethnicity, IQ, and the extent to which reading interventions produce similar gains for children with ADHD with and without a diagnosed reading disability. Children with comorbid ADHD and reading disability may present with a unique set of neurocognitive, affective, and behavioral profiles compared to children with either diagnosis alone (Dupaul et al., 2013; Ek et al., 2011; Miranda et al., 2014). As such, it will be important to examine whether these children experience significantly different responses to reading intervention than children with ADHD who have less severe reading difficulties. With that said, meta-analyses of reading interventions for struggling readers more broadly indicate that demographic factors including SES and IQ are not significant predictors of reading intervention outcomes (Bus et al., 1995; Stuebing et al., 2009; Swanson,1999; Wanzek et al., 2016). Nevertheless, continued investigation of child, family, and social-community factors (Chan et al., 2022) that promote optimal reading outcomes will be important for determining ‘what works for whom in what context.’
Finally, several planned moderators were excluded due to multicollinearity that confounded/qualified our interpretation of other moderators (e.g., diagnostic method/study quality; ESE status/individual vs. group treatment format). Studies examining each of these factors alone and in combination are needed to disentangle the effects of these factors on reading outcomes for children with ADHD. Moreover, standardized/norm-referenced tests are important for documenting disability but also possess several undesirable characteristics that limit their ability to detect change – particularly for children with neurodevelopmental populations such as ADHD as discussed above (for review, please see Farmer et al., 2020). In contrast, the content of study-created/curriculum-based measures is often psychometrically unvalidated and potentially ‘too close’ in content to the training curriculum, limiting conclusions that can be drawn regarding transfer of the trained skills to children’s reading skills in general. Therefore, we encourage researchers to analyze and report person-ability scores/growth scale values that are developed based on item response theory specifically for assessing change and increasingly provided by standardized academic test publishers (e.g., Kaufman & Kaufman, 2014).
Clinical Implications.
Based on the results of the present study, decoding interventions meet the most rigorous criteria to be considered well-established, evidence-based treatments with strong research support for reading difficulties in children with ADHD based on established benchmarks in both clinical psychology and special education (Evans et al., 2018; Cook et al., 2015). Decoding interventions should therefore be the first-line treatment for reading difficulties among at-risk readers with ADHD. In particular, our results revealed that reading interventions that provide at least 30 hours of intensive instruction in phonemic decoding are likely to produce large magnitude improvements in reading for children with ADHD despite the affective, behavioral, and neurocognitive risks associated with the disorder. In contrast, prior meta-analytic evidence indicates clearly that extant evidence-based ADHD treatments produce minimal to no improvements in reading or other academic domains (Boland et al., 2020; van der Oord et al., 2008), and the current findings suggest that adding ADHD treatment to reading intervention is not likely to produce incremental benefits on reading outcomes. Together, the current review presents systematic and robust evidence for decoding interventions as a highly effective, evidence-based intervention for the pervasive reading difficulties associated with ADHD.
Footnotes
Declarations of interest: none
Seven of the 16 studies included in Stewart & Austin (2020) were included in the present meta-analysis, whereas the other 9 studies included in Stewart & Austin (2020) were excluded from the current review due to focusing on second-language English learners (1), single-case design studies (6), or not directly targeting reading skills (i.e., spelling, effects of color on reading; 2).
Contributor Information
Elizabeth S.M. Chan, Florida State University
Jeffrey A. Shero, Florida State University
Eric D. Hand, Florida State University
Alissa M. Cole, Florida State University
Fatou Gaye, Florida State University
Jamie A. Spiegel, Florida International University
Michael J. Kofler, Florida State University
References
- Aduen PA, Day TN, Kofler MJ, Harmon SL, Wells EL, & Sarver DE (2018). Social problems in ADHD: Is it a skills acquisition or performance problem?. Journal of psychopathology and behavioral assessment, 40(3), 440–451. 10.1007/s10862-018-9649-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alderson RM, Rapport MD, & Kofler MJ (2007). Attention-deficit/hyperactivity disorder and behavioral inhibition: a meta-analytic review of the stop-signal paradigm. Journal of abnormal child psychology, 35(5), 745–758. 10.1007/s10802-007-9131-6 [DOI] [PubMed] [Google Scholar]
- Al Otaiba S, & Fuchs D (2002). Characteristics of children who are unresponsive to early literacy intervention: A review of the literature. Remedial and Special Education, 23(5), 300–316. 10.1177/07419325020230050501 [DOI] [Google Scholar]
- Assink M, & Wibbelink CJ (2016). Fitting three-level meta-analytic models in R: A step-by-step tutorial. The Quantitative Methods for Psychology,12(3), 154–174. [Google Scholar]
- August GJ, & Garfinkel BD (1990). Comorbidity of ADHD and reading disability among clinic-referred children. Journal of abnormal child psychology, 18(1), 29–45. 10.1007/BF00919454 [DOI] [PubMed] [Google Scholar]
- Benner GJ, Nelson JR, Ralston NC, & Mooney P (2010). A meta-analysis of the effects of reading instruction on the reading skills of students with or at risk of behavioral disorders. Behavioral Disorders, 35(2), 86–102. 10.1177/019874291003500202 [DOI] [Google Scholar]
- Bennett KJ, Brown KS, Boyle M, Racine Y, & Offord D (2003). Does low reading achievement at school entry cause conduct problems?. Social Science & Medicine, 56(12), 2443–2448. 10.1016/S0277-9536(02)00247-2 [DOI] [PubMed] [Google Scholar]
- Bental B, & Tirosh E (2008). The effects of methylphenidate on word decoding accuracy in boys with attention-deficit/hyperactivity disorder. Journal of Clinical Psychopharmacology, 28(1), 89–92. 10.1097/jcp.0b013e3181603f0e [DOI] [PubMed] [Google Scholar]
- Boland H, DiSalvo M, Fried R, Woodworth KY, Wilens T, Faraone SV, & Biederman J (2020). A literature review and meta-analysis on the effects of ADHD medications on functional outcomes. Journal of psychiatric research, 123, 21–30. 10.1016/j.jpsychires.2020.01.006 [DOI] [PubMed] [Google Scholar]
- Bus AG, Van Ijzendoorn MH, & Pellegrini AD (1995). Joint book reading makes for success in learning to read: A meta-analysis on intergenerational transmission of literacy. Review of Educational Research, 65(1), 1–21. 10.3102/00346543065001001 [DOI] [Google Scholar]
- Bussing R, Porter P, Zima BT, Mason D, Garvan C, & Reid R (2012). Academic outcome trajectories of students with ADHD: Does exceptional education status matter?. Journal of Emotional and Behavioral Disorders, 20(3), 131–143. 10.1177/1063426610388180 [DOI] [Google Scholar]
- Chambless DL, & Hollon SD (1998). Defining empirically supported therapies. Journal of consulting and clinical psychology, 66(1), 7. 10.1037/0022-006X.66.1.7 [DOI] [PubMed] [Google Scholar]
- Chan ES, Groves NB, Marsh CL, Miller CE, Richmond KP, & Kofler MJ (2022). Are There Resilient Children with ADHD?. Journal of Attention Disorders, 26(5), 643–655. 10.1177/10870547211025629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheung MWL (2014). Modeling dependent effect sizes with three-level meta-analyses: A structural equation modeling approach. Psychological Methods, 19(2), 211. 10.1037/a0032968 [DOI] [PubMed] [Google Scholar]
- *Clarfield J, & Stoner G (2005). The effects of computerized reading instruction on the academic performance of students identified with ADHD. School Psychology Review, 34(2), 246–254. 10.1080/02796015.2005.12086286 [DOI] [Google Scholar]
- Cohen J (2013). Statistical power analysis for the behavioral sciences. Routledge. [Google Scholar]
- Cook BG, Buysse V, Klingner J, Landrum TJ, McWilliam RA, Tankersley M, & Test DW (2015). CEC’s standards for classifying the evidence base of practices in special education. Remedial and Special Education, 36(4), 220–234. 10.1177/0741932514557271 [DOI] [Google Scholar]
- *Crabtree T, Alber-Morgan SR, & Konrad M (2010). The effects of self-monitoring of story elements on the reading comprehension of high school seniors with learning disabilities. Education and Treatment of Children, 3(2), 187–203. [Google Scholar]
- Daniel J, Vaughn S, Roberts G, & Grills A (2022). The importance of baseline word reading skills in examining student response to a multicomponent reading intervention. Journal of learning disabilities, 55(4), 259–271. 10.1177/00222194211010349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daucourt MC, Erbeli F, Little CW, Haughbrook R, & Hart SA (2020). A meta-analytical review of the genetic and environmental correlations between reading and ADHD symptoms and reading and math. Scientific Studies of Reading, 24(1), 23–56. 10.1080/10888438.2019.1631827 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Denton CA, Hall C, Cho E, Cannon G, Scammacca N, & Wanzek J (2022). A meta-analysis of the effects of foundational skills and multicomponent reading interventions on reading comprehension for primary-grade students. Learning and Individual Differences, 93, 102062. 10.1016/j.lindif.2021.102062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Denton CA, Tamm L, Schatschneider C, & Epstein JN (2020). The effects of ADHD treatment and reading intervention on the fluency and comprehension of children with ADHD and word reading difficulties: A randomized clinical trial. Scientific Studies of Reading, 24(1), 72–89. 10.1080/10888438.2019.1640704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DuPaul GJ, Gormley MJ, & Laracy SD (2013). Comorbidity of LD and ADHD: Implications of DSM-5 for assessment and treatment. Journal of learning disabilities, 46(1), 43–51. 10.1080/10888438.2019.1640704 [DOI] [PubMed] [Google Scholar]
- DuPaul GJ, & Langberg JM (2015). Educational impairments in children with ADHD.
- DuPaul GJ, Volpe RJ, Jitendra AK, Lutz JG, Lorah KS, & Gruber R (2004). Elementary school students with AD/HD: Predictors of academic achievement. Journal of School Psychology, 42(4), 285–301. 10.1016/j.jsp.2004.05.001 [DOI] [Google Scholar]
- Egger M, Smith GD, Schneider M, & Minder C (1997). Bias in meta-analysis detected by a simple, graphical test. Bmj, 315(7109), 629–634. 10.1136/bmj.315.7109.629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ek U, Westerlund J, Holmberg K, & Fernell E (2011). Academic performance of adolescents with ADHD and other behavioural and learning problems—a population-based longitudinal study. Acta Paediatrica, 100(3), 402–406. 10.1111/j.1651-2227.2010.02048.x [DOI] [PubMed] [Google Scholar]
- Evans SW, Langberg JM, Schultz BK, Vaughn A, Altaye M, Marshall SA, & Zoromski AK (2016). Evaluation of a school-based treatment program for young adolescents with ADHD. Journal of consulting and clinical psychology, 84(1), 15. 10.1037/ccp0000057 [DOI] [PubMed] [Google Scholar]
- Evans SW, Owens JS, Wymbs BT, & Ray AR (2018). Evidence-based psychosocial treatments for children and adolescents with attention deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 47(2), 157–198. 10.1080/15374416.2013.850700 [DOI] [PubMed] [Google Scholar]
- Fabiano GA, Schatz NK, Aloe AM, Chacko A, & Chronis-Tuscano A (2015). A systematic review of meta-analyses of psychosocial treatment for attention-deficit/hyperactivity disorder. Clinical child and family psychology review, 18(1), 77–97. 10.1007/s10567-015-0178-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farmer CA, Kaat AJ, Thurm A, Anselm I, ... & Miller JS (2020). Person ability scores as an alternative to norm-referenced scores as outcome measures in studies of neurodevelopmental disorders. American Journal on Intellectual and Developmental Disabilities, 125(6), 475–480. 10.1352/1944-7558-125.6.475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fergusson DM, Lynskey MT, & Horwood LJ (1997). Attentional difficulties in middle childhood and psychosocial outcomes in young adulthood. Journal of Child Psychology and Psychiatry, 38(6), 633–644. 10.1111/j.1469-7610.1997.tb01690.x [DOI] [PubMed] [Google Scholar]
- Foorman B, Beyler N, Borradaile K, Coyne M, Denton CA, Dimino J, ... & Wissel S (2016). Foundational Skills to Support Reading for Understanding in Kindergarten through 3rd Grade. Educator’s Practice Guide. NCEE 2016–4008. What Works Clearinghouse. [Google Scholar]
- Frazier TW, Youngstrom EA, Glutting JJ, & Watkins MW (2007). ADHD and achievement: Meta-analysis of the child, adolescent, and adult literatures and a concomitant study with college students. Journal of learning disabilities, 40(1), 49–65. 10.1177/00222194070400010401 [DOI] [PubMed] [Google Scholar]
- Friedman LM, Rapport MD, Raiker JS, Orban SA, & Eckrich SJ (2017). Reading comprehension in boys with ADHD: the mediating roles of working memory and orthographic conversion. Journal of Abnormal Child Psychology, 45(2), 273–287. [DOI] [PubMed] [Google Scholar]
- Froehlich TE, Fogler J, Barbaresi WJ, Elsayed NA, Evans SW, & Chan E (2018). Using ADHD medications to treat coexisting ADHD and reading disorders: a systematic review. Clinical Pharmacology & Therapeutics, 104(4), 619–637. 10.1002/cpt.1192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuchs D, & Fuchs LS (2006). Introduction to response to intervention: What, why, and how valid is it?. Reading research quarterly, 41(1), 93–99. [Google Scholar]
- Gallagher R, Abikoff HB, & Spira EG (2014). Organizational skills training for children with ADHD: An empirically supported treatment. Guilford Publications. [Google Scholar]
- Gersten R, Haymond K, Newman-Gonchar R, Dimino J, & Jayanthi M (2020). Meta-analysis of the impact of reading interventions for students in the primary grades. Journal of Research on Educational Effectiveness, 13(2), 401–427. 10.1080/19345747.2019.1689591 [DOI] [Google Scholar]
- Ghelani K, Sidhu R, Jain U, & Tannock R (2004). Reading comprehension and reading related abilities in adolescents with reading disabilities and attention-deficit/hyperactivity disorder. Dyslexia, 10(4), 364–384. 10.1002/dys.285 [DOI] [PubMed] [Google Scholar]
- Goodwin AP, & Ahn S (2013). A meta-analysis of morphological interventions in English: Effects on literacy outcomes for school-age children. Scientific Studies of Reading, 17(4), 257–285. 10.1080/10888438.2012.689791 [DOI] [Google Scholar]
- Gough PB, & Tunmer WE (1986). Decoding, reading, and reading disability. Remedial and Special Education, 7, 6–10. [Google Scholar]
- *Gum LI (2003). Collateral effects of computer-assisted reading instruction on the classroom behaviors of learners with emotional and/or behavioral disorders. Tennessee Technological University. [Google Scholar]
- Hall MS, & Burns MK (2018). Meta-analysis of targeted small-group reading interventions. Journal of School Psychology, 66, 54–66. 10.1016/j.jsp.2017.11.002 [DOI] [PubMed] [Google Scholar]
- Hedges LV (1981). Distribution theory for Glass’s estimator of effect size and related estimators. Journal of Educational Statistics, 6(2), 107–128. 10.3102/10769986006002107 [DOI] [Google Scholar]
- Hedges LV, & Pigott TD (2004). The power of statistical tests for moderators in meta-analysis. Psychological methods, 9(4), 426. 10.1037/1082-989X.9.4.426 [DOI] [PubMed] [Google Scholar]
- *Hedin LR, Mason LH, & Gaffney JS (2011). Comprehension strategy instruction for two students with attention-related disabilities. Preventing School Failure, 55(3), 148–157. 10.1080/1045988X.2010.499393 [DOI] [Google Scholar]
- *Hendricks EL (2019). Predicting Poor Readers’ Response to a Multi-Component Reading Comprehension Intervention. Vanderbilt University. [Google Scholar]
- Hill DR (2016). Phonics based reading interventions for students with intellectual disability: A systematic literature review. Journal of Education and Training Studies, 4(5), 205–214. [Google Scholar]
- Hox JJ (2010). Multilevel analysis: techniques and applications. Routledge. [Google Scholar]
- Hunter JE, & Schmidt FL (2004). Methods of meta-analysis: Correcting error and bias in research findings. Sage. [Google Scholar]
- *Johnson JW, Reid R, & Mason LH (2012). Improving the reading recall of high school students with ADHD. Remedial and Special Education, 33(4), 258–268. 10.1177/0741932511403502 [DOI] [Google Scholar]
- Jolani S (2012). Dual imputation strategies for analyzing incomplete data. Utrecht University. [Google Scholar]
- Kaufman AS, Kaufman NL (2014). Technical & interpretive manual: Kaufman Test of Educational Achievement (3rd ed.). Bloomington, MN: NCS Pearson. [Google Scholar]
- Kofler MJ, Irwin LN, Soto EF, Groves NB, Harmon SL, & Sarver DE (2019). Executive functioning heterogeneity in pediatric ADHD. Journal of abnormal child psychology, 47(2), 273–286. 10.1007/s10802-018-0438-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kofler MJ, Raiker JS, Sarver DE, Wells EL, & Soto EF (2016). Is hyperactivity ubiquitous in ADHD or dependent on environmental demands? Evidence from meta-analysis. Clinical psychology review, 46, 12–24. 10.1016/j.cpr.2016.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kofler MJ, Rapport MD, & Matt Alderson R (2008). Quantifying ADHD classroom inattentiveness, its moderators, and variability: a meta-analytic review. Journal of child psychology and psychiatry, 49(1), 59–69. 10.1111/j.1469-7610.2007.01809.x [DOI] [PubMed] [Google Scholar]
- Kofler MJ, Sarver DE, Harmon SL, Moltisanti A, Aduen PA, Soto EF, & Ferretti N (2018). Working memory and organizational skills problems in ADHD. Journal of child psychology and psychiatry, 59(1), 57–67. 10.1111/jcpp.12773 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kofler MJ, Sarver DE, Spiegel JA, Day TN, Harmon SL, & Wells EL (2017). Heterogeneity in ADHD: Neurocognitive predictors of peer, family, and academic functioning. Child neuropsychology, 23(6), 733–759. 10.1080/09297049.2016.1205010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Korrel H, Mueller KL, Silk T, Anderson V, & Sciberras E (2017). Research review: Language problems in children with ADHD - a systematic meta-analytic review. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 58, 640–654. [DOI] [PubMed] [Google Scholar]
- Kortekaas-Rijlaarsdam AF, Luman M, Sonuga-Barke E, & Oosterlaan J (2019). Does methylphenidate improve academic performance? A systematic review and meta-analysis. European child & adolescent psychiatry, 28(2), 155–164. 10.1007/s00787-018-1106-3 [DOI] [PubMed] [Google Scholar]
- *Lane KL, O’Shaughnessy TE, Lambros KM, Gresham F, & Beebe-Frankenberger M (2001). The efficacy of phonological awareness training with first-grade students who have behavior problems and reading difficulties. Journal of Emotional and Behavioral Disorders, 9, 219–231. 10.1177/106342660100900402 [DOI] [Google Scholar]
- Lee KJ, & Carlin JB (2012). Recovery of information from multiple imputation: a simulation study. Emerging themes in epidemiology, 9(1), 1–10. 10.1186/1742-7622-9-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee JH, & Huber J (2011, September). Multiple imputation with large proportions of missing data: How much is too much?. In United Kingdom Stata Users’ Group Meetings 2011 (No. 23). Stata Users Group. [Google Scholar]
- Lipsey MW, & Wilson DB (2001). Practical meta-analysis (Vol. 49). Sage Publications. [Google Scholar]
- Lipszyc J, & Schachar R (2010). Inhibitory control and psychopathology: a meta-analysis of studies using the stop signal task. Journal of the International Neuropsychological Society, 16(6), 1064–1076. 10.1017/S1355617710000895 [DOI] [PubMed] [Google Scholar]
- Loe IM, & Feldman HM (2007). Academic and educational outcomes of children with ADHD. Journal of pediatric psychology, 32(6), 643–654. 10.1093/jpepsy/jsl054 [DOI] [PubMed] [Google Scholar]
- Lonigan CJ, Burgess SR, & Schatschneider C (2018). Examining the simple view of reading with elementary school children: Still simple after all these years. Remedial and Special Education, 39(5), 260–273. 10.1177/0741932518764833 [DOI] [Google Scholar]
- *Luckey AJ (2009). Cognitive and academic gains as a result of cognitive training. Arizona State University. [Google Scholar]
- Majewicz-Hefley A, & Carlson JS (2007). A meta-analysis of combined treatments for children diagnosed with ADHD. Journal of Attention Disorders, 10(3), 239–250. 10.1177/1087054706289934 [DOI] [PubMed] [Google Scholar]
- Maughan B, Gray G, & Rutter M (1985). Reading retardation and antisocial behaviour: A follow-up into employment. Journal of Child Psychology and Psychiatry, 26(5), 741–758. 10.1111/j.1469-7610.1985.tb00588.x [DOI] [PubMed] [Google Scholar]
- Mayes SD, & Calhoun SL (2006). Frequency of reading, math, and writing disabilities in children with clinical disorders. Learning and Individual Differences, 16(2), 145–157. 10.1016/j.lindif.2005.07.004 [DOI] [Google Scholar]
- McAuley L, Pham B, Tugwell P, & Moher D (2000). Does the inclusion of grey literature influence estimates of intervention effectiveness reported in meta-analyses?. The Lancet, 356(9237), 1228–1231. 10.1016/S0140-6736(00)02786-0 [DOI] [PubMed] [Google Scholar]
- McGee R, Prior M, Williams S, Smart D, & Sanson A (2002). The long-term significance of teacher-rated hyperactivity and reading ability in childhood: Findings from two longitudinal studies. Journal of Child Psychology and Psychiatry, 43(8), 1004–1017. 10.1111/1469-7610.00228 [DOI] [PubMed] [Google Scholar]
- Miller AC, Fuchs D, Fuchs LS, Compton DL, Kearns D, Zhang W, Yen L, Patton S, & Kirchner D (2014). Behavioral attention: a longitudinal study of whether and how it influences the development of word reading and reading comprehension among at-risk readers. Journal of Research on Educational Effectiveness, 7, 232–249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller AC, Keenan JM, Betjemann RS, Willcutt EG, Pennington BF, & Olson RK (2013). Reading comprehension in children with ADHD: Cognitive underpinnings of the centrality deficit. Journal of abnormal child psychology, 41(3), 473–483. 10.1007/s10802-012-9686-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miranda A, Berenguer C, Colomer C, & Roselló R (2014). Influence of the symptoms of Attention Deficit Hyperactivity Disorder (ADHD) and comorbid disorders on functioning in adulthood. Psicothema, 26(4), 471–476. [DOI] [PubMed] [Google Scholar]
- Mishra S, & Khare D (2014). On comparative performance of multiple imputation methods for moderate to large proportions of missing data in clinical trials: a simulation study. Journal of Medical Statistics and Informatics, 2(1), 9. 10.7243/2053-7662-2-9 [DOI] [Google Scholar]
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, ... & Stewart LA (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic reviews, 4(1), 1–9. 10.1186/2046-4053-4-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- MTA Cooperative Group. (1999). A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Archives of general psychiatry, 56(12), 1073–1086. 10.1001/archpsyc.56.12.1073 [DOI] [PubMed] [Google Scholar]
- National Reading Panel (US), National Institute of Child Health, Human Development (US), National Reading Excellence Initiative, National Institute for Literacy (US), & United States Department of Health. (2000). Report of the National Reading Panel: Teaching children to read: An evidence-based assessment of the scientific research literature on reading and its implications for reading instruction: Reports of the subgroups. National Institute of Child Health and Human Development, National Institutes of Health. [Google Scholar]
- Okkinga M, van Steensel R, van Gelderen AJ, van Schooten E, Sleegers PJ, & Arends LR (2018). Effectiveness of reading-strategy interventions in whole classrooms: A meta-analysis. 10.1007/s10648-018-9445-7 [DOI] [Google Scholar]
- Paris SG, & Stahl SA (Eds.). (2005). Children’s reading comprehension and assessment. Routledge. [Google Scholar]
- Pelham WE, Altszuler AR, Merrill BM, Raiker JS, Macphee FL, Ramos M, ... & Waxmonsky JG (2022). The effect of stimulant medication on the learning of academic curricula in children with ADHD: A randomized crossover study. Journal of consulting and clinical psychology, 90(5), 367–380. 10.1037/ccp0000725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Polanczyk GV, Willcutt EG, Salum GA, Kieling C, & Rohde LA (2014). ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. International Journal of Epidemiology, 43(2), 434–442. 10.1093/ije/dyt261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rabiner DL, & Malone PS; Conduct Problems Prevention Research Group. (2004). The impact of tutoring on early reading achievement for children with and without attention problems. Journal of Abnormal Child Psychology, 32(3), 273–284. 10.1023/B:JACP.0000026141.20174.17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raggi VL, & Chronis AM (2006). Interventions to address the academic impairment of children and adolescents with ADHD. Clinical child and family psychology review, 9(2), 85–111. 10.1007/s10567-006-0006-0 [DOI] [PubMed] [Google Scholar]
- *Raffaele Mendez LM, Pelzmann CA, & Frank MJ (2016). Engaging struggling early readers to promote reading success: A pilot study of reading by design. Reading & Writing Quarterly, 32(3), 273–297. 10.1080/10573569.2014.986592 [DOI] [Google Scholar]
- Rapport MD, Chung KM, Shore G, Denney CB, & Isaacs P (2000). Upgrading the science and technology of assessment and diagnosis: Laboratory and clinic-based assessment of children with ADHD. Journal of clinical child psychology, 29(4), 555–568. [DOI] [PubMed] [Google Scholar]
- Rapport MD, Denney C, Paul GJ, & Gardner MJ (1994). Attention deficit disorder and methylphenidate: normalization rates, clinical effectiveness, and response prediction in 76 children. Journal of the American Academy of Child & Adolescent Psychiatry, 33(6), 882–893. 10.1097/00004583-199407000-00015 [DOI] [PubMed] [Google Scholar]
- Rapport MD, Kofler MJ, Alderson RM, Timko T, & DuPaul GJ (2009). Variability of attention processes in ADHD: Observations from the classroom. Journal of Attention Disorders, 12, 563–573. 10.1177/1087054708322990 [DOI] [PubMed] [Google Scholar]
- *Richardson E, Kupietz S, & Maitinsky S (1987). What is the role of academic intervention in the treatment of hyperactive children with reading disorders?. Journal of Children in Contemporary Society, 19(1–2), 153–167. 10.1300/J274v19n01_13 [DOI] [Google Scholar]
- Rindskopf D, Shadish W, & Hedges LV (2012). A simple effect size estimator for single case designs using WinBUGS. Online Submission
- Roberts GJ, Cho E, Garwood JD, Goble GH, Robertson T, & Hodges A (2020). Reading interventions for students with reading and behavioral difficulties: A meta-analysis and evaluation of co-occurring difficulties. Educational Psychology Review, 32(1), 17–47. 10.1007/s10648-019-09485-1 [DOI] [Google Scholar]
- *Rogevich M., & Perin D (2008). Effects on science summarization of a reading comprehension int-ervention for adolescents with behavior and attention disorders. Exceptional Children, 74(2), 135–154. 10.1177/001440290807400201 [DOI] [Google Scholar]
- Ron Nelson J, Benner GJ, & Gonzalez J (2003). Learner characteristics that influence the treatment effectiveness of early literacy interventions: A meta-analytic review. Learning Disabilities Research & Practice, 18(4), 255–267. 10.1111/1540-5826.00080 [DOI] [Google Scholar]
- Rosenthal R (1994). Science and ethics in conducting, analyzing, and reporting psychological research. Psychological Science, 5(3), 127–134. 10.1111/j.1467-9280.1994.tb00646.x [DOI] [PubMed] [Google Scholar]
- Rosenthal R (1979). The file drawer problem and tolerance for null results. Psychological bulletin, 86(3), 638. 10.1037/0033-2909.86.3.638 [DOI] [Google Scholar]
- RStudio T (2020). RStudio: integrated development for R. Rstudio Team, PBC, Boston, MA: URL http://www.rstudio.com. [Google Scholar]
- Rucklidge JJ, & Tannock R (2002). Neuropsychological profiles of adolescents with ADHD: Effects of reading difficulties and gender. Journal of child psychology & psychiatry, 43(8), 988–1003. 10.1111/1469-7610.00227 [DOI] [PubMed] [Google Scholar]
- *Saddler B, Asaro-Saddler K, Moeyaert M, & Ellis-Robinson T (2017). Effects of a summarizing strategy on written summaries of children with emotional and behavioral disorders. Remedial and Special Education, 38(2), 87–97. 10.1177/0741932516669051 [DOI] [Google Scholar]
- Sciutto MJ, & Eisenberg M (2007). Evaluating the evidence for and against the overdiagnosis of ADHD. Journal of attention disorders, 11(2), 106–113. 10.1177/1087054707300094 [DOI] [PubMed] [Google Scholar]
- Scammacca NK, Roberts G, Vaughn S, & Stuebing KK (2015). A meta-analysis of interventions for struggling readers in grades 4–12: 1980–2011. Journal of Learning Disabilities, 48(4), 369–390. 10.1177/0022219413504995 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scammacca N, Roberts G, Vaughn S, Edmonds M, Wexler J, Reutebuch CK, & Torgesen JK (2007). Interventions for adolescent struggling readers: A meta-analysis with implications for practice. Center on Instruction. [Google Scholar]
- Semrud-Clikeman M, Biederman J, Sprich-Buckminster S, Lehman BK, Faraone S, & Norman D (1992). Comorbidity between ADDH and learning disability: A review and report in a clinically referred sample. Journal of the American Academy of Child & Adolescent Psychiatry, 31(3), 439–448. 10.1097/00004583-199205000-00009 [DOI] [PubMed] [Google Scholar]
- *Shimabukuro SM (1996). The effects of self-monitoring of academic performance on students with learning disabilities and ADD/ADHD. University of Hawai’i at Manoa. [Google Scholar]
- Sideridis GD, Mouzaki A, Simos P, & Protopapas A (2006). Classification of students with reading comprehension difficulties: The roles of motivation, affect, and psychopathology. Learning disability quarterly, 29(3), 159–180. 10.2307/30035505 [DOI] [Google Scholar]
- Simons DJ, Boot WR, Charness N, Gathercole SE, …Stine-Morrow EA (2016). Do “brain-training” programs work?. Psychological Science in the Public Interest, 17(3), 103–186. 10.1177/1529100616661983 [DOI] [PubMed] [Google Scholar]
- Simmons FR, Willis C, & Adams AM (2012). Different components of working memory have different relationships with different mathematical skills. Journal of Experimental Child Psychology, 111(2), 139–155. 10.1016/j.jecp.2011.08.011 [DOI] [PubMed] [Google Scholar]
- *Strong Hilsmier A, Wehby JH, & Falk KB (2016). Reading fluency interventions for middle school students with academic and behavioral disabilities. Reading Improvement, 53(2), 53–64. [Google Scholar]
- Sonuga-Barke EJ, Brandeis D, Cortese S, Daley D, Ferrin M, Holtmann M, ... & European ADHD Guidelines Group. (2013). Nonpharmacological interventions for ADHD: Systematic review and meta-analyses of randomized controlled trials of dietary and psychological treatments. American Journal of Psychiatry, 170(3), 275–289. 10.1176/appi.ajp.2012.12070991 [DOI] [PubMed] [Google Scholar]
- Stewart AA, & Austin CR (2020). Reading interventions for students with or at risk of ADHD: A systematic review. Remedial and Special Education, 41(6), 352–367. 10.1177/0741932519849660 [DOI] [Google Scholar]
- Stuebing KK, Barth AE, Molfese PJ, Weiss B, & Fletcher JM (2009). IQ is not strongly related to response to reading instruction: A meta-analytic interpretation. Exceptional children, 76(1), 31–51. 10.1177/001440290907600102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swanson HL (1999). Reading research for students with LD: A meta-analysis of intervention outcomes. Journal of learning disabilities, 32(6), 504–532. 10.1177/002221949903200605 [DOI] [PubMed] [Google Scholar]
- Swanson JM, McBurnett K, Christian DL, & Wigal T (1995). Stimulant medications and the treatment of children with ADHD. Advances in clinical child psychology, 265–322. 10.1007/978-1-4757-9044-3_7 [DOI] [Google Scholar]
- *Tamm L, Denton CA, Epstein JN, Schatschneider C, Taylor H, Arnold LE, ... & Vaughn A (2017). Comparing treatments for children with ADHD and word reading difficulties: A randomized clinical trial. Journal of consulting and clinical psychology, 85(5), 434. 10.1037/ccp0000170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Tannock R, Frijters JC, Martinussen R, White EJ, Ickowicz A, Benson NJ, & Lovett MW (2018). Combined modality intervention for ADHD with comorbid reading disorders: A proof of concept study. Journal of learning disabilities, 51(1), 55–72. 10.1177/0022219416678409 [DOI] [PubMed] [Google Scholar]
- Tran L, Sanchez T, Arellano B, & Lee Swanson H (2011). A meta-analysis of the RTI literature for children at risk for reading disabilities. Journal of learning disabilities, 44(3), 283–295. 10.1177/0022219410378447 [DOI] [PubMed] [Google Scholar]
- Van Buuren S (2018). Flexible imputation of missing data. CRC press. [Google Scholar]
- Van Buuren S, & Groothuis-Oudshoorn K (2011). mice: Multivariate imputation by chained equations in R. Journal of statistical software, 45(3), 1–67. 10.18637/jss.v045.i03 [DOI] [Google Scholar]
- Van der Oord S, Prins PJ, Oosterlaan J, & Emmelkamp PM (2008). Efficacy of methylphenidate, psychosocial treatments and their combination in school-aged children with ADHD: a meta-analysis. Clinical psychology review, 28(5), 783–800. 10.1016/j.cpr.2007.10.007 [DOI] [PubMed] [Google Scholar]
- Vaughn S, Linan-Thompson S, Kouzekanani K, Pedrotty Bryant D, Dickson S, & Blozis SA (2003). Reading instruction grouping for students with reading difficulties. Remedial and Special Education, 24(5), 301–315. 10.1177/07419325030240050501 [DOI] [Google Scholar]
- Viechtbauer W (2010). Conducting meta-analyses in R with the metafor package. Journal of statistical software, 36(3), 1–48. [Google Scholar]
- *Walcott CM, Marett K, & Hessel AB (2014). Effectiveness of a computer-assisted intervention for young children with attention and reading problems. Journal of Applied School Psychology, 30(2), 83–106. 10.1080/15377903.2013.874389 [DOI] [Google Scholar]
- Wanzek J, Wexler J, Vaughn S, & Ciullo S (2010). Reading interventions for struggling readers in the upper elementary grades: A synthesis of 20 years of research. Reading and writing, 23(8), 889–912. 10.1007/s11145-009-9179-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wanzek J, Vaughn S, Scammacca N, Gatlin B, Walker MA, & Capin P (2016). Meta-analyses of the effects of tier 2 type reading interventions in grades K-3. Educational psychology review, 28(3), 551–576. 10.1007/s10648-015-9321-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willcutt EG, Betjemann RS, McGrath LM, Chhabildas NA, Olson RK, DeFries JC, & Pennington BF(2010). Etiology and neuropsychology of comorbidity between RD and ADHD: The case for multiple deficit models. Cortex, 46(10), 1345–1361. 10.1016/j.cortex.2010.06.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williamson D, Murray DW, Damaraju CV, Ascher S, & Starr HL (2014). Methylphenidate in children with ADHD with or without learning disability. Journal of attention disorders, 18(2), 95–104. 10.1177/1087054712443411 [DOI] [PubMed] [Google Scholar]
- Zhao X, Page TF, Altszuler AR, Pelham III WE, Kipp H, … Pelham WE Jr (2019). Family burden of raising a child with ADHD. Journal of Abnormal Child Psychology, 47(8), 1327–1338. 10.1007/s10802-019-00518-5 [DOI] [PubMed] [Google Scholar]