

Abstract
Objectives
To review available health and nutrition claims for infant formula products in multiple countries and to evaluate the validity of the evidence used for substantiation of claims.
Design
International cross sectional survey.
Setting
Public facing and healthcare professional facing company owned or company managed formula industry websites providing information about products marketed for healthy infants delivered at full term in 15 countries: Australia, Canada, Germany, India, Italy, Japan, Nigeria, Norway, Pakistan, Russia, Saudi Arabia, South Africa, Spain, the United Kingdom, and the United States in 2020-22.
Main outcome measures
Number and type of claims made for each product and ingredient. References cited were reviewed and risk of bias was assessed for registered clinical trials using the Cochrane risk of bias tool, and for systematic reviews using the Risk Of Bias in Systematic reviews tool.
Results
757 infant formula products were identified, each with a median of two claims (range from 1 (Australia) to 4 (US)), and 31 types of claims across all products. Of 608 products with ≥1 claims, the most common claim types were “helps/supports development of brain and/or eyes and/or nervous system” (323 (53%) products, 13 ingredients), “strengthens/supports a healthy immune system” (239 (39%) products, 12 ingredients), and “helps/supports growth and development” (224 (37%) products, 20 ingredients). 41 groups of ingredients were associated with ≥1claims, but many claims were made without reference to a specific ingredient (307 (50%) products). The most common groups of ingredients cited in claims were long chain polyunsaturated fatty acids (278 (46%) products, 9 different claims); prebiotics, probiotics, or synbiotics (225 (37%) products, 19 claims); and hydrolysed protein (120 (20%) products, 9 claims). 161/608 (26%) products with ≥1 claims provided a scientific reference to support the claim—266 unique references were cited for 24 different claim types for 161 products. The reference types most frequently cited were clinical trials (50%, 134/266) and reviews (20%, 52/266). 28% (38/134) of referenced clinical trials were registered, 14% (19/134) prospectively. 58 claims referred to 32 registered clinical trials, of which 51 claims (27 trials) related to a randomised comparison. 46 of 51 claims (90%) referenced registered clinical trial outcomes at high risk of bias, and all cited systematic reviews and pooled analyses, carried a high risk of bias.
Conclusions
Most infant formula products had at least one health and nutrition claim. Multiple ingredients were claimed to achieve similar health or nutrition effects, multiple claims were made for the same ingredient type, most products did not provide scientific references to support claims, and referenced claims were not supported by robust clinical trial evidence.
Introduction
Human breast milk is the optimal source of infant nutrition.1 Consistent evidence supports multiple short term and long term health risks to both children and mothers when substitutes such as infant formula are used.2 3 4 5 Decisions about infant feeding can be influenced by a range of medical, socio-political, and psychological factors; however, the marketing of infant formula is an important factor that can undermine breastfeeding.6 7 Recent multinational research by the World Health Organization and United Nations International Children’s Emergency Fund (Unicef) highlighted how “pervasive, personalised and powerful” the marketing of infant formula can be, with personal data on digital platforms being used to refine strategies.8 9 Industry spends billions per annum promoting breast milk substitutes, and multiple, often emotive, techniques are used to promote products.8
Health and nutrition claims about infant formula are controversial because they can enhance the perceived benefits of formula over breastfeeding and thereby undermine breastfeeding.10 Suboptimal breastfeeding is estimated to result in about 600 000 child deaths from pneumonia and diarrhoea and 100 000 maternal deaths from ovarian or breast cancer each year.11 Furthermore, doubt exists about the veracity of common claims. In a convenience sample of countries, we identified the claims about health and nutrition visible on public facing websites of infant formula companies. Additionally, we assessed the evidence cited in support of these claims.
Methods
Study design and settings
This cross sectional study involved data collection from a convenience sample of 15 countries: Australia, Canada, Germany, India, Italy, Japan, Nigeria, Norway, Pakistan, Russia, Saudi Arabia, South Africa, Spain, the United Kingdom, and the United States. We selected these countries through purposive sampling to identify high income and low and middle income countries where a collaborator was willing and able to participate in data collection. A predefined protocol was developed for data extraction, which took place between April 2020 and July 2022 (see supplementary figure 1).
Health and nutrition claims search
We identified health and nutrition claims on official public facing and healthcare professional facing company owned or company managed formula industry websites when available, that provide information on their products. Local search engines, such as Google or country specific equivalents, were used to identify infant formula products marketed locally. After identification of the products, we searched for corresponding healthcare professional facing websites. The browsing cache was cleared to ensure no previous behavioural patterns would affect the search results, and the search in each country was conducted in the country’s official language. In countries with multiple languages, searches were performed in the main official languages. Predefined search terms were used (see supplementary figure 1), with the search results limited to the first 20 pages returned for each country. To ensure the websites were specific to each country, only those ending in the appropriate country code top level domain were included—for example, the suffix .au for Australia. To ensure accurate future retrieval, all included websites were captured and stored in the internet archive (https://archive.org/web) at the time of access. To ensure the sample of infant formula products was complete, additional sources, such as national guidelines and lists of infant formula products provided by local regulators or health authorities were reviewed when available. Full datasets from each participating country are available at https://osf.io/pbd9y/.
Inclusion criteria
We defined infant formula as any formula suitable for infants aged 12 months or younger that serves as a breast milk substitute. Products subdivided by age or stage of development were treated as separate products because country specific regulation of claims can vary according to infants’ age and indication for using the product. We also included food for special medical purposes, such as extensively hydrolysed or amino acid formula, as these are often used for feeding healthy infants delivered at full term.12 13 We excluded formulas for inborn errors of metabolism such as galactosaemia, formulas specified for preterm or low birthweight infants, milks for toddlers, and supplements such as breast milk fortifiers.
When a claim was repeated between public facing and healthcare professional facing websites, it was counted as one claim for the specific product. We defined a claim as text that “states, suggests or implies that a food or component of the food has, or may have, an effect on the human body.”14
We included all health and nutrition claims but excluded those limited to the nutritive value of the product (termed nutrient content claims in the UK and nutrition claims in the European Union) where there was no reference to a potentially beneficial effect on physiology, growth, development, function, or health.10 Examples of excluded nutrient content claims include “good source of vitamin D” or “source of calcium.” The classification of health and nutrition claims varies between legislatures—we included claims that linked the product or an ingredient of the product with a potentially beneficial effect on the normal functioning, growth and development, or health of consumers.14
All health and nutrition claims found on products’ websites or packaging were recorded along with any cited scientific references (see supplementary table 1) and translated into English. Two researchers (KYC and LP) independently screened recorded claims and used a thematic content analysis approach to group the claim types.15 Any disparity was resolved by discussion and further involvement of additional research team members (RJB and DM).
Ingredients explicitly stated in the claim were recorded. We then categorised claims by the different ingredients to which they were linked. Even when products shared the same brand name, we counted them separately across countries because the claims for each product often differed across countries. If a claim was presented on the same product potentially distributed in different countries, we counted it as a unique claim in each respective country because at present no valid source exists to reliably confirm that two infant formulas carrying the same name are identical across different countries. Images of infant formula products were stored when available.
Evaluation of cited scientific evidence
To determine scientific substantiation of the health and nutrition claims, we collated any references provided by the formula companies. These were identified on the infant formula product or websites available to the public and healthcare professionals. We summarised the type of evidence cited. For cited registered clinical trials or systematic reviews of clinical trials we collated basic descriptive details, including funding source and conflicts of interest. We also undertook risk of bias assessment for any relevant outcome cited in the claim. We used the revised Cochrane risk of bias tool (RoB 2) for registered clinical trials16 and the Risk Of Bias In Systematic reviews (ROBIS) tool to assess risk of bias in systematic reviews and pooled analyses.17
Statistical analysis
Descriptive statistics were calculated, with continuous variables summarised as median (interquartile range) and categorical variables as frequency (percentage). A spider network was used to describe associations between claims and ingredients from the infant formula products identified in our search. These networks were generated using Python, with the libraries numpy, pandas, and matplotlib. For the main analysis we predefined inclusion of ingredients and claims with a frequency of at least 10.
Patient and public involvement
Although no patients or members of the public were directly involved in this project, we did speak to mothers with and without experience of infant formula use about the study. We also asked a member of the public to read the manuscript.
Results
Investigators in 15 of the 20 countries that agreed to participate successfully completed data collection. Of the remaining five countries, collaborators were unable to perform an extensive search and detailed data extraction when the study was conducted. In total, we identified 757 infant formula products and 1884 health and nutrition claims that could be categorised into 31 claim types (see supplementary table 1). The median number of claims for each product was 2 (interquartile range 1-4) and this was similar for products designated as infant formula (0-6 months and 0-12 months), follow-on formula (6-12 months), and food for special medical purposes. The frequency of claims varied across countries (see supplementary table 1). The most common claim types were “helps/supports development of brain and/or eyes and/or nervous system” (323 (53%) products, 13 ingredients), “strengthens/supports a healthy immune system” (239 (39%) products, 12 ingredients), “helps/supports growth and development” (224 (37%) products, 20 ingredients), “easy to digest” (182 (30%) products, 14 ingredients), and “dietary management of allergy including cow’s milk allergy (CMA)” (96 (16%) products, 4 ingredients) (table 1; also see supplementary figures 2-4).
Table 1.
Most common claims (number of products with relevant claims ≥10) made for different categories of infant formula: for infant formula (0-6 and 0-12 months), follow-on formula (6-12 months), and food for special medical purposes (FSMP)
| Claim | No (%) of products with relevant claim (n=608 products with ≥1 claim) | No of claims with ingredient cited | Quotes as examples of claims | No (%) with ≥1 claim | ||
|---|---|---|---|---|---|---|
| Infant formula (n=222) | Follow-on formula (n=95) | FSMP (n=291) | ||||
| Helps/supports development of brain and/or eyes and/or nervous system | 323 (53) | 172 | Omega-3 DHA like that found in Enfamil has been clinically shown to: improve attention span, problem solving, and visual development | 137 (62) | 62 (65) | 116 (40) |
| Strengthens/supports a healthy immune system | 239 (39) | 143 | Studies have shown positive effects of nucleotides for the infants’ immune function and in periods with rapid growth like in the newborn period | 88 (40) | 53 (56) | 70 (24) |
| Helps/supports growth and development | 224 (37) | 88 | Arachidonic acid: Components contained in breast milk helps growth and development | 82 (37) | 40 (42) | 75 (26) |
| Easy to digest | 182 (30) | 82 | Amino acids means that this will be easily digestible, and is good for infants with stomach - and digestive - conditions | 75 (34) | 16 (17) | 87 (30) |
| Dietary management of allergy including cow’s milk allergy (CMA) | 96 (16) | 35 | Helps more babies overcome cow’s milk allergy and return to consuming regular milk proteins in as fast as 6 months of feeding | 1 (0) | 0 (0) | 71 (24) |
| Stimulates growth of healthy intestinal bacteria | 91 (15) | 50 | Whey proteins, lactose and nucleotides to support the growth of useful gut bacteria | 40 (18) | 15 (16) | 36 (12) |
| Strengthens and develops bones | 77 (13) | 45 | Supports the normal development of bones and teeth with vitamin D (according to the law) | 33 (15) | 30 (32) | 14 (5) |
| Promotes softer/improves stool consistency | 71 (12) | 36 | Contains a blend of 2 dietary fibres, GOS [galacto-oligosaccharides] and polydextrose, shown to soften stools | 33 (15) | 10 (11) | 28 (10) |
| Reduces risk of allergy development | 63 (10) | 30 | It is clinically demonstrated to help reduce future allergy challenges at 3 years | 17 (7) | 5 (5) | 34 (12) |
| Dietary management of colic | 55 (9) | 21 | It is formulated to aid digestive malabsorption with an enriched level of sn-2 palmitate to help ease constipation (soften stools) and a reduced level of lactose to help ease colic | 6 (3) | 3 (3) | 37 (13) |
| Dietary management of regurgitation | 54 (9) | 41 | Contains rice starch that becomes thicker in your baby’s stomach is clinically proven to reduce frequent spit up | 0 (0) | 0 (0) | 38 (13) |
| Improves absorption and/or digestion | 35 (6) | 20 | Improved absorption and digestion due to the presence of: An easy to digest fat blend including MCT/LCT [medium chain triglycerides/light chain triglycerides] | 11 (5) | 5 (5) | 19 (7) |
| Dietary management of constipation | 20 (3) | 8 | NAN Sensilac is an infant formula based on cow’s milk, especially developed for children with sensitive stomachs and those with a tendency to constipation | 5 (2) | 1 (1) | 11 (4) |
Associations between health and nutrition claims and specific ingredients
A total of 41 ingredients described in conjunction with health claims were identified, and claims referred to one ingredient or more 1724 times. The median number of different claims for each ingredient was 3 (interquartile range 1-6), and the median number of different ingredients with the same claim type attributed was 4 (interquartile range 2-7). Figure 1 shows the network plot of all relationships between the claims and ingredients with a frequency of ≥10 (see supplementary figures 3 and 4 for plots of countries surveyed in 2020 and 2022). In total, 473 (27%) claims were not linked to a specific ingredient (table 2 and supplementary figures 3 and 4). The most frequently identified claim type linked to a particular ingredient was “helps/supports development of brain and/or eye and/or nervous system,” which was linked to long chain polyunsaturated fatty acids (259/1724 (15%) claims).
Fig 1.
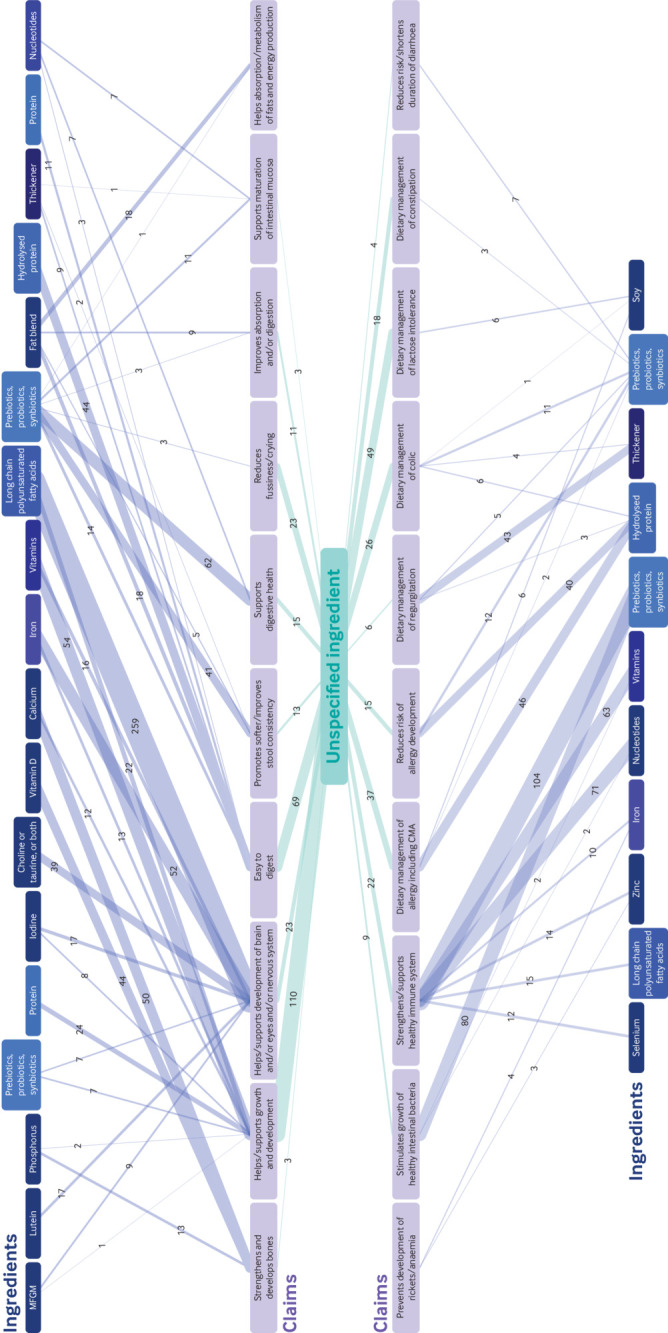
Network plot of claims associated with ingredients with a frequency of ≥10. Green midpoint box represents health claims associated with a non-specified ingredient. Blue labels represent type of ingredient; different shades represent unique ingredients associated with different claims. Purple labels represent health and nutrition claims. Thickness of lines represents frequency of health claims associated with an ingredient. CMA=cow’s milk allergy; MFGM=milk fat globule membrane
Table 2.
Most common ingredients (number of separate claims cited for ingredient ≥100) used for substantiation of claims in different categories of infant formula: infant formula (0-6 and 0-12 months), follow-on formula (6-12 months), and food for special medical purposes (FSMP)
| Ingredient | No (%) of products with ingredient/total of 608 products with ≥1 claim (%) | No of separate claims cited for relevant ingredient | Quotes as examples of claims | No (%) with ≥1 claim related to ingredient | ||
|---|---|---|---|---|---|---|
| Infant formula (n=222) | Follow-on formula (n=95) | FSMP (n=291) | ||||
| Not specified | 307 (50) | 473 | - | 80 (36) | 22 (23) | 128 (44) |
| Long chain polyunsaturated fatty acids | 278 (46) | 322 | With the addition of long chain omega 3 and omega 6 fatty acids, the proteins have been replaced with amino acids, assisting with the healthy brain and eye development of children | 76 (34) | 49 (52) | 78 (27) |
| Prebiotics, probiotics, synbiotics | 225 (37) | 389 | This specific blend of prebiotics has been shown to encourage the growth and activity of beneficial bacteria in the infant gut, as well as improve stool frequency and consistency | 84 (38) | 28 (29) | 62 (21) |
| Hydrolysed protein | 120 (20) | 152 | Contains a unique combination of starch and 100 whey, partially hydrolysed protein for the dietary management of reflux and regurgitation | 12 (5) | 2 (2) | 75 (26) |
| Vitamins | 116 (19) | 193 | Vitamins A, C &D to help support the normal function of baby’s immune system . . . | 33 (15) | 36 (38) | 26 (9) |
Multiple ingredients were associated with the same type of health and nutrition claim—for example, “strengthens/supports a healthy immune system” is linked to prebiotics, probiotics, or synbiotics (104/1724 (6%) claims) as well as other vitamins, excluding vitamin D (63/1724 (4%) claims). In some cases, it was unclear which specific ingredient formed the basis of a claim when multiple ingredients were listed for one claim—for example, “Contains ingredients that support: Immune function with nucleotides and vitamin A, C, E, selenium and zinc; digestive health with easy to digest whey proteins, lactose and nucleotides to support the growth of useful gut bacteria; Strong bones with calcium, phosphorus, magnesium and vitamin D.”
Specific ingredients were also linked to multiple claims—for example, long chain polyunsaturated fatty acids were associated with “helps/supports development of brain and/or eye and/or nervous system” (259/1724 (15%) claims), “helps/supports growth and development” (22/1724 (1%) claims), “strengthens/supports a healthy immune system” (15/1724 (1%) claims), “easy to digest” (3/1724 (0.2%) claims), and “support digestive health” (1/1724 (0.1%) claim).
Scientific substantiation of health and nutrition claims
Across all countries, 161 out of 608 (26%) products with one claim or more provided a reference to substantiate a given claim. Overall, 161 products cited a total of 266 unique scientific references in support of 17 of the 31 different claims (fig 2). Of the 266 unique references, the most abundant reference types were clinical trials (134 (50%)), review articles (52 (20%)), and other original peer reviewed citations, including cohort, animal, and cross sectional studies (38 (14%)). Table 3 illustrates the type of scientific evidence behind the 10 most common health and nutrition claims. Other references included non-peer reviewed citations (24 (9%)), including opinion pieces (11 (4%)); reports, guidelines, or regulations (10 (4%)); and systematic reviews with meta-analyses or other types of pooled analyses (8 (3%)) (see supplementary table 6).
Fig 2.

Outline of main number of products, claims, ingredients, and references cited
Table 3.
Scientific substantiation of 10 most common infant formula health and nutrition claims, excluding reference duplicates (266 unique references)
| Type of claim | Total No of claims with references cited | No/total No (%) of references | ||||||
|---|---|---|---|---|---|---|---|---|
| Registered clinical trials | Non-registered clinical trials | Reviews* | Meta-analyses, pooled analyses, systematic reviews | Other peer reviewed citation† | Reports, guidelines, regulations | Opinion pieces, abstracts, posters, other‡ | ||
| All claims | 560 | 38/266 (14) | 96/266 (36) | 52/266 (20) | 8/266 (3) | 38/266 (14) | 10/266 (4) | 24/266 (9) |
| Helps/supports development of brain and/or eyes and/or nervous system | 136 | 3/38 (8) | 22/96 (23) | 10/52 (19) | 3/8 (38) | 4/38 (11) | 5/10 (50) | 6/24 (25) |
| Strengthens/supports a healthy immune system | 94 | 7/38 (18) | 15/96 (16) | 23/52 (44) | 1/8 (13) | 6/38 (16) | 1/10 (10) | 6/24 (25) |
| Stimulates growth of healthy intestinal bacteria | 56 | 8/38 (21) | 9/96 (9) | 8/52 (15) | 0/8 (0) | 4/38 (11) | 0/10 (0) | 2/24 (8) |
| Dietary management of allergy including cow’s milk allergy (CMA) | 49 | 6/38 (16) | 19/96 (20) | 5/52 (10) | 0/8 (0) | 4/38 (11) | 2/10 (20) | 2/24 (8) |
| Helps/supports growth and development | 36 | 9/38 (24) | 11/96 (11) | 2/52 (4) | 1/8 (13) | 2/38 (5) | 1/11 (9) | 2/24 (8) |
| Reduces risk of allergy development | 36 | 6/38 (16) | 6/96 (6) | 6/52 (12) | 2/8 (25) | 3/38 (8) | 0/11 (0) | 3/24 (13) |
| Easy to digest | 27 | 1/38 (3) | 5/96 (5) | 1/52 (2) | 2/8 (25) | 3/38 (8) | 0/11 (0) | 3/24 (13) |
| Promotes softer/improves stool consistency | 24 | 4/38 (11) | 7/96 (7) | 3/52 (6) | 0/8 (0) | 3/38 (8) | 0/11 (0) | 0/24 (0) |
| Dietary management of colic | 15 | 1/38 (3) | 8/96 (8) | 0/52 (0) | 0/8 (0) | 1/38 (3) | 0/11 (0) | 1/24 (4) |
| Strengthens and develops bones | 7 | 2/38 (5) | 0/96 (0) | 1/52 (2) | 0/8 (0) | 0/38 (0) | 0/11 (0) | 3/24 (13) |
Including textbook chapters.
Including cohort studies, animal studies, and cross sectional studies.
Including opinion pieces, conference abstracts or poster presentations, market research, websites, and nutrition content labels.
Risk of bias assessment of clinical trials and systematic reviews
In total, 58 claims referenced 38 publications arising from 32 registered clinical trials, of which 51 claims (27 trials) related to a randomised comparison. Most (28/32, 88%) registered trials had formula industry funding and/or formula industry affiliated authors, and just four trials (supporting eight claims) had no nutrition industry funding or relevant author conflicts of interest. Risk of bias was not assessed for seven of these claims because the citation was related to a non-randomised trial, an observational analysis of a trial population, or no relevant claim outcome being reported in the cited trial (see supplementary table 7). Forty six of 51 (90%) claims referenced registered clinical trial outcomes that carried a high risk of bias (fig 3). Risk of bias arose from deviations from intervention and missing outcome data. It was also notable that claims were usually not related to the primary outcome of the registered trial, and in three cases the claim was not supported by the study findings. Nine claims (across six claim types) cited eight systematic reviews or pooled analyses.18 19 20 21 22 One of the claims did not have a direct link with the evidence synthesis in the referenced systematic review of studies of human breast milk long chain polyunsaturated fatty acid concentrations.22 All seven other systematic reviews or pooled analyses cited in support of the claims carried a high risk of bias (see supplementary table 8). Five of seven systematic reviews or pooled analyses were funded by formula industry, whereas six out of seven had at least one industry affiliated author. None of them had a prespecified protocol in the public domain, and none of them described using a risk of bias assessment to evaluate included trials.
Fig 3.
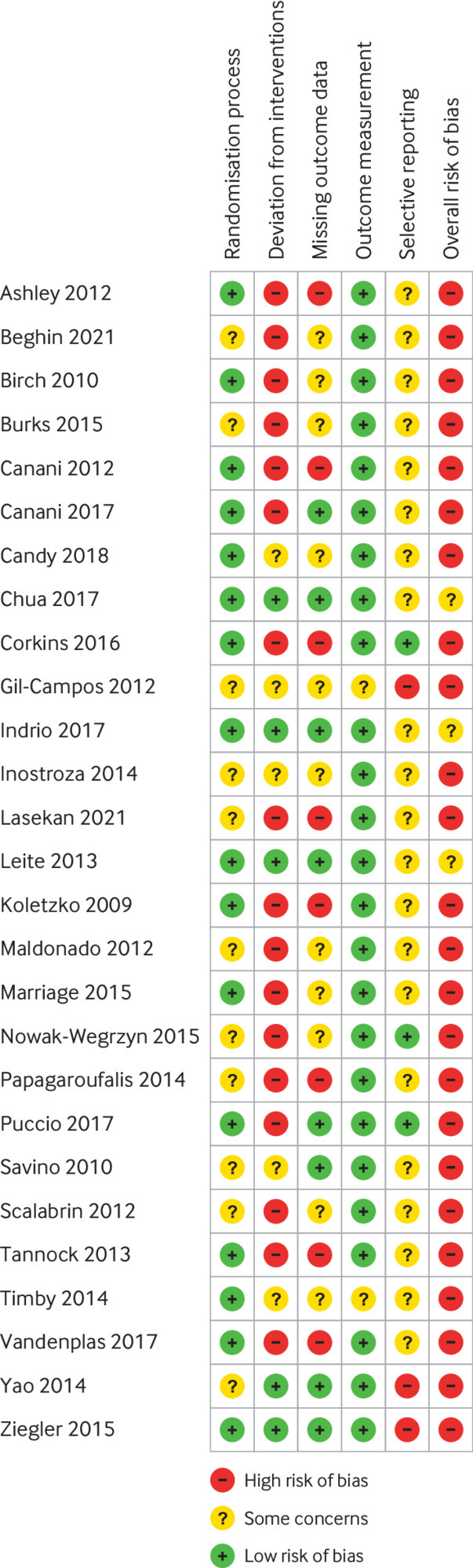
Risk of bias assessment of clinical trials
Discussion
In this cross sectional survey, we found multiple different claims for similar ingredients across competing infant formula products, and we found multiple ingredients with the same category of claim attributed to them. The scientific evidence used to substantiate claims carried a high risk of bias.
Our finding that health and nutrition claims for infant formula are common is supported by previous work.15 These claims appear on infant formula products and promotional materials despite national regulations and international guidance prohibiting them. Claims were commonly found on infant formula packaging and promotional websites, across countries with both high and low levels of compliance with the current international legal instrument, the International Code for Marketing Breast milk Substitutes.23 This could suggest that the global regulatory and public health communities, governments, and public policy civil servants are failing to effectively limit the use of claims in marketing of breast milk substitutes, as seen in other related sectors.24 This can both undermine breastfeeding and increase costs for families,25 as high prices for infant formula have detrimental effects on families residing in low and middle income countries.11 26 27 28 The frequencies of claims about health and nutrition were similar in low and middle income and in high income countries. Some variation in claims was observed between countries (see supplementary table 1); however, detailed analysis of reasons for variation in claims by country is beyond the scope of this study.
Claims linking long chain polyunsaturated fatty acids to the development of brain, eyes, and nervous system were the most common. This causal link is reported despite recent evidence failing to substantiate the association.29 30 Other common claims, such as for prebiotics, probiotics, and synbiotics and for strengthening and supporting a healthy immune system also do not have strong substantiation in the scientific literature.31 It is worth noting that claims were frequently made in the absence of a link to a specific ingredient. When a link to an ingredient was present, evidence was often inadequate, with many claims not supported by appropriate referencing of published, peer reviewed scientific literature. Two thirds of products with at least one claim did not provide a reference to any evidence, and, when registered clinical trials were cited, they had a high level of conflict of interest and industry funding and carried a high risk of bias. Lack of independence or transparency and high risk of bias and selective outcome reporting have been identified as features of formula trials as a whole.32 This lack of scientific underpinning for claims contrasts with consumer facing statements such as “widely studied” or “supported by over 40 years of research,” which implied scientific support.8 This can be misleading for parents and healthcare workers alike, subsequently affecting their recommendations. Parallels can be drawn with pharmaceutical companies, which have been criticised for drug advertising in medical journals, influencing readers’ understanding, and resulting in some “mythical associations” between medical conditions and branded drugs.33 34 35 Overall, private sector activities impacting public health, either positively or negatively, and the enabling political economic systems and norms are referred to as commercial determinants of health.36 Unethical marketing strategies and political activities, including misinformation, lobbying, and donations are well documented features of the current interplay between corporations and public wellbeing.36
Notably, for many ingredients the risks and benefits of addition to infant formula have not been well substantiated. Human breast milk consists of thousands of biologically active components,37 which are highly variable within and between mothers and can be modified by maternal and environmental factors,38 potentially impacting infant health outcomes. The presence of a particular biologically active ingredient does not, however, mean that it is crucial for infant development. Addition of individual ingredients with known biological activity to infant formula should be better supported by robust scientific evidence regarding long term benefits and safety.39 40
Strengths and limitations of this study
This study synthesised evidence from a range of countries, with different regulatory environments and population infant feeding practices, and formally documented the relationship between health and nutrition claims and ingredients cited in infant formula. The relationship between health and nutrition claims and ingredients across different environments was recorded—these relationships could not have been effectively shown without undertaking this study internationally, as the claims made for specific ingredients vary by region. Information was collected in a harmonised fashion, following a predetermined protocol and after preliminary training. The risk of bias assessment for clinical trials and systematic reviews used for substantiation of claims was performed using standardised recommended tools. Finally, outcomes of the primary analysis were confirmed in the sensitivity analysis from the additional countries, representing different geographical regions.
Our study has several limitations. Firstly, data were extracted by multiple researchers, and this could have led to differences in extraction approaches between sites. We (LP, KYC, DM) mitigated this by training and closely supervising researchers to limit any variations in searches, data extraction, and coding. However, it was not feasible to completely exclude the possibility of inconsistencies in data collection or missing products. Secondly, researchers conducted their search and data extraction in the local language before translating data to English for analysis, which could have introduced minor discrepancies. Thirdly, data are not fully representative of the global situation, as we were only able to access high quality data for 15 countries. The selected countries do, however, represent different geographical regions and therefore provide a global overview of infant formula health and nutrition claims. Fourthly, some products might have been missed during the search, which could result in selection bias. All collaborators adopted a comprehensive search strategy, thereby limiting the number of products potentially being missed and ensuring that the data represents what a consumer would be able to come across in a search. Fifthly, as the products were found through online searches, national guidelines, and local regulators or health authority websites, some of the infant formula physically available instore may not have been available or covered online. Sixthly, lack of back translation, whereby the completed translation is translated back into the original language and differences are compared and reconciled, is a potential limitation. Finally, products with the same or similar brand name across different countries were counted as separate products because composition might differ across markets. This could artificially inflate the number of associations between the same claim and the same ingredient. This limitation should not have an effect on the key findings, such as the number of claims for each product, ingredients being associated with multiple different claims and vice versa, and lack of scientific substantiation for claims.
Comparison with other studies
The need for more evidence to support marketing claims found on infant formulas has been highlighted previously.41 This study comprehensively assesses infant formula claims internationally and links claims and ingredients across multiple jurisdictions. Although previous attempts at examining health and nutrition claims of infant formula were limited to a single country, a lack of scientific evidence to support claims was also found.15 42 We have added to this by further investigating claims found on healthcare professional websites for all countries included, by formally linking claims and ingredients and assessing risk of bias in registered clinical trials and systematic reviews. We identified a high level of redundancy in relationships between claims and ingredients, and little scientific substantiation of claims. Exposure to formula marketing strategies has recently been assessed internationally by the WHO, and it is clear that most parents are exposed to formula marketing during pregnancy or the postnatal period and are often misled by claims.8 43
We have previously suggested that health and nutrition claims for products regarded as breast milk substitutes should not be permitted. These products are so important for the infants who need them, and any true advances in breast milk substitute composition should be made available to all infants receiving relevant products. These advances should be standard in all formula products and not be limited to certain infant formulas as appealing factors for marketing purposes.10 This new information about the extent and complexity of health and nutrition claims for products comprising breast milk substitutes underlines a lack of scientific evidence available to support these claims and their important role as vehicles for marketing. Given the known adverse effects of breast milk substitutes,3 these findings strengthen our previous call for a ban on health and nutrition claims for breast milk substitutes.10
Conclusions
Despite previous attempts to change the landscape of infant formula marketing undertaken by multiple reputable organisations, including but not limited to, the First Steps Nutrition Trust,44 International Baby Foods Action Network, WHO, and Unicef,8 9 progress in regulating infant formula claims is slow. Although advances have been made in implementing mandatory compositional and information requirements for infant formula, transparency is still lacking about health and nutrition claims linked to infant formula. We have identified a high prevalence of claims on infant formula products in multiple countries that seem to have little or no scientific substantiation. These findings support calls for a revised regulatory framework for breast milk substitutes to better protect consumers and avoid the harms associated with aggressive marketing of such products.
What is already known on this topic
Health and nutrition claims on infant formula products are controversial, banned in some jurisdictions, and may undermine breastfeeding
Data on the prevalence of claims and their scientific substantiation are limited
What this study adds
In an international survey of 15 countries, most products carried at least one claim, a wide range of different claims was made for similar ingredients, and multiple classes of ingredients were used as a basis for similar claims
Three quarters of products with at least one claim did not provide a reference to the evidence in support of the claim
When claims cited scientific evidence, 14% of citations were registered clinical trials and 90% of those carried a high risk of bias
Acknowledgments
We acknowledge the work of our international collaborators during the data extraction process: Shuyi Zhang, associate researcher in child health, Capital Institute of Paediatrics, Beijing, China, and Amadou Faal, scientific officer, Medical Research Council Gambia at London School of Hygiene and Tropical Medicine.
Web extra.
Extra material supplied by authors
Supplementary information: Additional figures 1-4, tables 1-8, and references
Contributors: KYC and LP contributed equally to this work as first co-authors. DM and RJB contributed equally to this work as senior co-authors. DM and RJB conceived the study. DM, KYC, and LP designed the study, with advice and input from RJB. DM, KYC, and LP developed and piloted the study protocol and data extraction. KYC, LP, EP, MB, RC, PC, EC-M, SDE, ED, PH, YK, MRS, LPS, ST, MW, QY, IA, LA-D, MAK, CM, RO, JG, BEY, BB, MG, MEL, and SZ completed data extraction for respective countries. SA, BH, KYC, LP, DM, and RJB assessed the scientific substantiation of all health and nutrition claims. JZ conceptualised and implemented data visualisation. KYC, LP, DM, and RJB wrote the first draft of the manuscript. All authors critically reviewed and revised the manuscript and approved the final manuscript. DM acts as guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This study received no external funding.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: no support from any organisation for the submitted work. Outside of the submitted work: JG and LPS benefit from unrestricted research grants from Danone Nutricia Research to Leipzig University for research into human milk composition within the Ulm Birth Cohort Studies. This work is not related to the present publication. RJB declares consultancy payment from Cochrane, Wiley and the British Society for Allergy and Clinical Immunology for editorial work, and payment for expert witness work in cases involving food anaphylaxis and a disputed infant formula health claim. BEY owns Feed Baby Love, which provides educational resources to parents and providers regarding infant feeding.
The lead author affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Dissemination to participants and related patient and public communities: The findings of this study will be disseminated to regulators, industry clinical trials departments, and charities that support and advise parents and other carers of young children in making decisions about feeding. The outcomes will be widely shared with the general public through both academic (eg, medical journals, national and international conferences, professional societies) and public (eg, press releases, mass media communications, and informing public health experts and policy makers) channels.
Provenance and peer review: Not commissioned; externally peer reviewed.
Ethics statements
Ethical approval
Not required. All information used for the analyses was already in the public domain, with the exception of the clinical trial protocols and statistical analysis plans, which were kindly provided by some trialists and trial sponsors at our request, to confirm methods used in the relevant trials.
Data availability statement
Technical appendix, statistical code, and dataset available from the corresponding author on reasonable request.
References
- 1. Lessen R, Kavanagh K. Position of the academy of nutrition and dietetics: promoting and supporting breastfeeding. J Acad Nutr Diet 2015;115:444-9. 10.1016/j.jand.2014.12.014 [DOI] [PubMed] [Google Scholar]
- 2. Rollins NC, Bhandari N, Hajeebhoy N, et al. Lancet Breastfeeding Series Group . Why invest, and what it will take to improve breastfeeding practices? Lancet 2016;387:491-504. 10.1016/S0140-6736(15)01044-2 [DOI] [PubMed] [Google Scholar]
- 3. Victora CG, Bahl R, Barros AJD, et al. Lancet Breastfeeding Series Group . Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet 2016;387:475-90. 10.1016/S0140-6736(15)01024-7 [DOI] [PubMed] [Google Scholar]
- 4. Allen J, Hector D. Benefits of breastfeeding. N S W Public Health Bull 2005;16:42-6. 10.1071/NB05011 [DOI] [PubMed] [Google Scholar]
- 5. Gartner LM, Morton J, Lawrence RA, et al. American Academy of Pediatrics Section on Breastfeeding . Breastfeeding and the use of human milk. Pediatrics 2005;115:496-506. 10.1542/peds.2004-2491 [DOI] [PubMed] [Google Scholar]
- 6. Kong SKF, Lee DTF. Factors influencing decision to breastfeed. J Adv Nurs 2004;46:369-79. 10.1111/j.1365-2648.2004.03003.x [DOI] [PubMed] [Google Scholar]
- 7. Radzyminski S, Callister LC. Mother’s Beliefs, Attitudes, and Decision Making Related to Infant Feeding Choices. J Perinat Educ 2016;25:18-28. 10.1891/1058-1243.25.1.18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.World Health Organization. How the Marketing of Formula Milk Influences our Decisions on Infant Feeding. 2022 [cited 2022 Aug 25]. https://www.who.int/publications/i/item/9789240044609
- 9.World Health Organization. Marketing of breast milk substitutes: national implementation of the international code, status report 2020. 2020.
- 10. Munblit D, Crawley H, Hyde R, Boyle RJ. Health and nutrition claims for infant formula are poorly substantiated and potentially harmful. BMJ 2020;369:m875. 10.1136/bmj.m875 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Walters DD, Phan LTH, Mathisen R. The cost of not breastfeeding: global results from a new tool. Health Policy Plan 2019;34:407-17. 10.1093/heapol/czz050 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Mehta S, Allen HI, Campbell DE, Arntsen KF, Simpson MR, Boyle RJ. Trends in use of specialized formula for managing cow’s milk allergy in young children. Clin Exp Allergy 2022;52:839-47. 10.1111/cea.14180 [DOI] [PubMed] [Google Scholar]
- 13. Strzalkowski AJ, Järvinen KM, Schmidt B, Young BE. Protein and carbohydrate content of infant formula purchased in the United States. Clin Exp Allergy 2022;52:1291-301. 10.1111/cea.14232 [DOI] [PubMed] [Google Scholar]
- 14.European Commission. Health Claims. https://ec.europa.eu.
- 15. Berry NJ, Gribble KD. Health and nutrition content claims on websites advertising infant formula available in Australia: A content analysis. Matern Child Nutr 2017;13:e12383. 10.1111/mcn.12383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019;366:l4898. 10.1136/bmj.l4898 [DOI] [PubMed] [Google Scholar]
- 17. Whiting P, Savović J, Higgins JPT, et al. ROBIS group . ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol 2016;69:225-34. 10.1016/j.jclinepi.2015.06.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Morale SE, Hoffman DR, Castañeda YS, Wheaton DH, Burns RA, Birch EE. Duration of long-chain polyunsaturated fatty acids availability in the diet and visual acuity. Early Hum Dev 2005;81:197-203. 10.1016/j.earlhumdev.2004.09.008 [DOI] [PubMed] [Google Scholar]
- 19. Czerkies LA, Kineman BD, Cohen SS, Reichert H, Carvalho RS. A Pooled Analysis of Growth and Tolerance of Infants Exclusively Fed Partially Hydrolyzed Whey or Intact Protein-Based Infant Formulas. Int J Pediatr 2018;2018:4969576. 10.1155/2018/4969576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Alexander DD, Cabana MD. Partially hydrolyzed 100% whey protein infant formula and reduced risk of atopic dermatitis: a meta-analysis. J Pediatr Gastroenterol Nutr 2010;50:422-30. 10.1097/MPG.0b013e3181cea52b [DOI] [PubMed] [Google Scholar]
- 21. Alexander DD, Yan J, Bylsma LC, et al. Growth of infants consuming whey-predominant term infant formulas with a protein content of 1.8 g/100 kcal: a multicenter pooled analysis of individual participant data. Am J Clin Nutr 2016;104:1083-92. 10.3945/ajcn.116.130633 [DOI] [PubMed] [Google Scholar]
- 22. Brenna JT, Varamini B, Jensen RG, Diersen-Schade DA, Boettcher JA, Arterburn LM. Docosahexaenoic and arachidonic acid concentrations in human breast milk worldwide. Am J Clin Nutr 2007;85:1457-64. 10.1093/ajcn/85.6.1457 [DOI] [PubMed] [Google Scholar]
- 23. World Health Organization . International Code of Marketing of Breast-Milk Substitutes. WHO, 1981. [Google Scholar]
- 24. Caraher M, Perry I. Sugar, salt, and the limits of self regulation in the food industry. BMJ 2017;357:j1709. 10.1136/bmj.j1709 [DOI] [PubMed] [Google Scholar]
- 25.Neuberger Z. WIC Food Package Should Be Based on Science: Foods with New Functional Ingredients Should Be Provided Only If They Deliver Health or Nutritional Benefits. 2010. https://www.cbpp.org/research/wic-food-package-should-be-based-on-science
- 26. Howard C, Howard F, Lawrence R, Andresen E, DeBlieck E, Weitzman M. Office prenatal formula advertising and its effect on breast-feeding patterns. Obstet Gynecol 2000;95:296-303. [DOI] [PubMed] [Google Scholar]
- 27. Sobel HL, Iellamo AD, Raya RR, Padilla AA, Sta Ana FS, 3rd, Nyunt-U S. The economic burden of infant formula on families with young children in the Philippines. J Hum Lact 2012;28:174-80. 10.1177/0890334412436719 [DOI] [PubMed] [Google Scholar]
- 28. Rothstein JD, Winch PJ, Pachas J, et al. Vulnerable families and costly formula: a qualitative exploration of infant formula purchasing among peri-urban Peruvian households. Int Breastfeed J 2021;16:11. 10.1186/s13006-021-00356-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Verfuerden ML, Dib S, Jerrim J, Fewtrell M, Gilbert RE. Effect of long-chain polyunsaturated fatty acids in infant formula on long-term cognitive function in childhood: A systematic review and meta-analysis of randomised controlled trials. PLoS One 2020;15:e0241800. 10.1371/journal.pone.0241800 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Verfürden ML, Gilbert R, Lucas A, Jerrim J, Fewtrell M. Effect of nutritionally modified infant formula on academic performance: linkage of seven dormant randomised controlled trials to national education data. BMJ 2021;375:e065805. 10.1136/bmj-2021-065805 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Cuello-Garcia CA, Brożek JL, Fiocchi A, et al. Probiotics for the prevention of allergy: A systematic review and meta-analysis of randomized controlled trials. J Allergy Clin Immunol 2015;136:952-61. 10.1016/j.jaci.2015.04.031 [DOI] [PubMed] [Google Scholar]
- 32. Helfer B, Leonardi-Bee J, Mundell A, et al. Conduct and reporting of formula milk trials: systematic review. BMJ 2021;375:n2202. 10.1136/bmj.n2202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Gamirova A, Berbenyuk A, Levina D, et al. Food Proteins in Human Breast Milk and Probability of IgE-Mediated Allergic Reaction in Children During Breastfeeding: A Systematic Review. J Allergy Clin Immunol Pract 2022;10:1312-1324.e8. 10.1016/j.jaip.2022.01.028 [DOI] [PubMed] [Google Scholar]
- 34. O’Reilly D, Dorodnykh D, Avdeenko NV, et al. Perspective: The Role of Human Breast-Milk Extracellular Vesicles in Child Health and Disease. Adv Nutr 2021;12:59-70. 10.1093/advances/nmaa094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Scott T, Stanford N, Thompson DR. Killing me softly: myth in pharmaceutical advertising. BMJ 2004;329:1484-7. 10.1136/bmj.329.7480.1484 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.World Health Organization. Commercial Determinants of Health. 2022 [cited 2022 Aug 25]. https://www.who.int/health-topics/commercial-determinants-of-health#tab=tab_1
- 37. Boix-Amorós A, Collado MC, Van’t Land B, et al. Reviewing the evidence on breast milk composition and immunological outcomes. Nutr Rev 2019;nuz019. 10.1093/nutrit/nuz019 [DOI] [PubMed] [Google Scholar]
- 38. Samuel TM, Zhou Q, Giuffrida F, Munblit D, Verhasselt V, Thakkar SK. Nutritional and Non-nutritional Composition of Human Milk Is Modulated by Maternal, Infant, and Methodological Factors. Front Nutr 2020;7:576133. 10.3389/fnut.2020.576133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Kaneko KJ, Fasano J, Choudhuri S. Bioactive ingredients in infant formula: The value for a robust interdisciplinary discussion on safety assessment paradigm. J Pediatr 2020;216:250-1. 10.1016/j.jpeds.2019.08.035 [DOI] [PubMed] [Google Scholar]
- 40. Abrams SA, Daniels SR. Protecting Vulnerable Infants by Ensuring Safe Infant Formula Use. J Pediatr 2019;211:201-6. 10.1016/j.jpeds.2019.04.032 [DOI] [PubMed] [Google Scholar]
- 41. Hughes HK, Landa MM, Sharfstein JM. Marketing Claims for Infant Formula: The Need for Evidence. JAMA Pediatr 2017;171:105-6. 10.1001/jamapediatrics.2016.3837 [DOI] [PubMed] [Google Scholar]
- 42.First Steps Nutrition Trust. Claims made for infant formula, ingredients and formulations. 2020. https://static1.squarespace.com/static/59f75004f09ca48694070f3b/t/5eba3eac6a3b687667d9891e/1589264046551/Claims_made_for_infant_formula_and_ingredients_May2020_final.pdf
- 43. Parry K, Taylor E, Hall-Dardess P, Walker M, Labbok M. Understanding women’s interpretations of infant formula advertising. Birth 2013;40:115-24. 10.1111/birt.12044 [DOI] [PubMed] [Google Scholar]
- 44.Brown A, Jones S, Evans E. Marketing of infant milk in the UK: what do parents see and believe? 2020 [cited 2022 Aug 25]. https://static1.squarespace.com/static/59f75004f09ca48694070f3b/t/6053645514d0f3072adec94e/1616077909798/Marketing_of_infant_milk_in_the_UK-what_do_parents_see_and_believe_finala.pdf
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary information: Additional figures 1-4, tables 1-8, and references
Data Availability Statement
Technical appendix, statistical code, and dataset available from the corresponding author on reasonable request.