

Abstract
Background
Incontinence of stool and flatus are frequent complications of childbirth. We examined the prevalence and possible causes of these adverse outcomes in a large cohort of women.
Methods
We studied 949 pregnant women who gave birth in 5 hospitals in 1995/96 in the province of Quebec. These women, participants in a randomized controlled trial of prenatal perineal massage, completed a self-administered questionnaire 3 months after giving birth.
Results
Three months after delivery 29 women (3.1%) reported incontinence of stool, and 242 (25.5%) had involuntary escape of flatus. Incontinence of stool was more frequent among women who delivered vaginally and had third- or fourth-degree perineal tears than among those who delivered vaginally and had no anal sphincter tears (7.8% v. 2.9%). Forceps delivery (adjusted risk ratio [RR] 1.45, 95% confidence interval [CI] 1.01–2.08) and anal sphincter tears (adjusted RR 2.09, 95% CI 1.40–3.13) were independent risk factors for incontinence of flatus or stool or both. Anal sphincter injury was strongly and independently associated with first vaginal birth (RR 39.2, 95% CI 5.4–282.5), median episiotomy (adjusted RR 9.6, 95% CI 3.2–28.5), forceps delivery (adjusted RR 12.3, 95% CI 3.0–50.4) and vacuum-assisted delivery (adjusted RR 7.4, 95% CI 1.9–28.5) but not with birth weight (adjusted RR for birth weight 4000 g or more: 1.4, 95% CI 0.6–3.0) or length of the second stage of labour (adjusted RR for second stage 1.5 hours or longer compared with less than 0.5 hours: 1.2, 95% CI 0.5–2.7).
Interpretation
Anal incontinence is associated with forceps delivery and anal sphincter laceration. Anal sphincter laceration is strongly predicted by first vaginal birth, median episiotomy, and forceps or vacuum delivery but not by birth weight or length of the second stage of labour.
Anal incontinence after childbirth is more common than was previously believed.1 The reported frequency of incontinence of stool in primiparous women ranges from 2% to 6%,2,3,4,5,6 and incontinence of either stool or flatus from 13% to 25%.2,4,5,7,8 After severe perineal laceration the rate of anal incontinence climbs to 17% to 62%.1,7,9,10,11,12
However, risk factors for anal incontinence in women giving birth have not received adequate attention.13,14 Incomplete anal control, although not life-threatening, may be caused by obstetric management and treated effectively. The objectives of this study were to describe the prevalence and severity of postpartum anal incontinence and to identify maternal and obstetric risk factors for this adverse outcome.
Methods
Information for this study was collected during a randomized controlled trial of perineal massage in the third trimester of pregnancy, approved by the ethics committees of the participating hospitals.15,16 The study population consisted of pregnant women with or without a previous vaginal birth scheduled to give birth in 5 hospitals in the province of Quebec. Women in the experimental group were to massage the perineum daily from 34 to 35 weeks' gestation until delivery; women in the control group were not to massage. The frequency of massage was classified into thirds according to the proportion of eligible days on which it was done.
All 1198 women recruited into the trial between March and December 1995 completed a baseline questionnaire on sociodemographic and obstetric characteristics. Detailed data on the occurrence and severity of perineal lacerations and episiotomy were recorded immediately after birth by the attending physician or house staff. The perineum was considered intact if there was no laceration or an unsutured first-degree tear. For study purposes first-degree lacerations involved sutured injury to the perineal or vaginal skin but not the underlying muscle; second-degree lacerations involved, in addition, fascia and muscles of the perineal body. A third-degree tear was defined as partial or complete laceration of the external anal sphincter, and a fourth-degree tear as complete rupture of the external anal sphincter with laceration of the anorectal mucosa. Other information about labour and delivery was abstracted from the medical record. We obtained the delivery record for previous deliveries to determine the type of delivery and perineal outcomes.
Three months post partum a questionnaire was mailed to each participant regarding the frequency (never, less than once a week, 1 to 6 times a week, daily or more than once a day) of involuntary loss of stool or passage of flatus.
For the analysis of risk factors, anal incontinence was treated as dichotomous (none v. any). Maternal, obstetric and newborn candidate variables for the adjusted models were those proposed in the medical literature or those with a univariate risk ratio (RR) less than 0.8 or greater than 1.25. We obtained univariate RRs and their 95% confidence intervals (CIs) separately for incontinence of stool and incontinence of flatus. We carried out multivariate analysis to explore the relative importance of various predictors using the combined outcome “incontinence of stool or flatus” to provide more stable estimates, since the number of women with each outcome was too small to permit adjustment for multiple predictors. Candidate variables for the multivariate model were those with an RR less than 0.8 or greater than 1.25 on univariate analysis of either incontinence of stool or incontinence of flatus. Periurethral tears and urinary incontinence were associated with anal incontinence but were excluded from the model, which was restricted to factors potentially causing anal incontinence. In the multivariate analyses, to avoid adjusting for a factor intermediate in the causal pathway, we included type of delivery and episiotomy in one model, and degree of perineal injury in a separate model.
In multivariate analyses of risk factors for common occurrences, such as postpartum anal incontinence, odds ratios from logistic regression analyses overestimate relative risk. To avoid this, we estimated adjusted RRs using a log–binomial model (generalized linear model with a log link and the binomial distribution for the error term).17 The response variable in this model is the log of the prevalence, and prevalence ratios are obtained by exponentiating the parameter estimates.
Results
Questionnaires were returned by 949 (79.2%) of the 1198 women. These women constituted the study population, which has been described in a previous publication.16
At 3 months after delivery incontinence of stool occurred in 3.1% (29/948) of the women, at least once daily in 0.3% (3/948) (Table 1). Incontinence of stool was present in 1.8% (2/114) of the women who underwent cesarean section, 2.9% (23/783) of those who gave birth vaginally without recognized anal sphincter damage, and 7.8% (4/51) of those who gave birth vaginally with recognized anal sphincter damage. Among the women who gave birth vaginally, the univariate RR for incontinence of stool in those with anal sphincter damage compared with those without recognized sphincter damage was 2.8 (95% CI 0.8–9.6) (Table 2). On univariate analysis macrosomia (birth weight 4000 g or more), episiotomy (median in all cases), anal sphincter tears and prepregnancy urinary incontinence were predictive of incontinence of stool (RR > 1.25), but other factors examined, including instrumental delivery, were not (Table 2).
Table 1
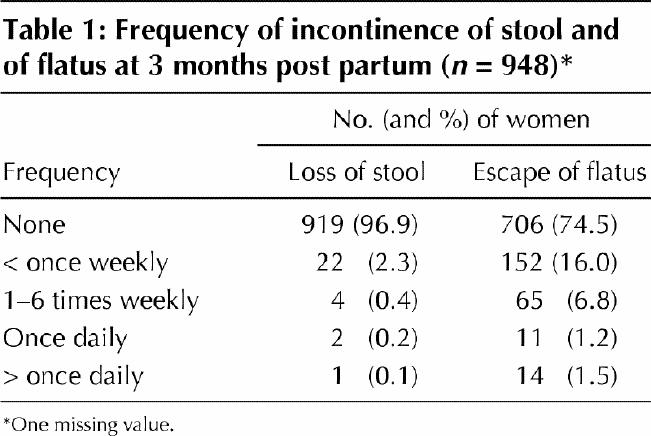
Table 2
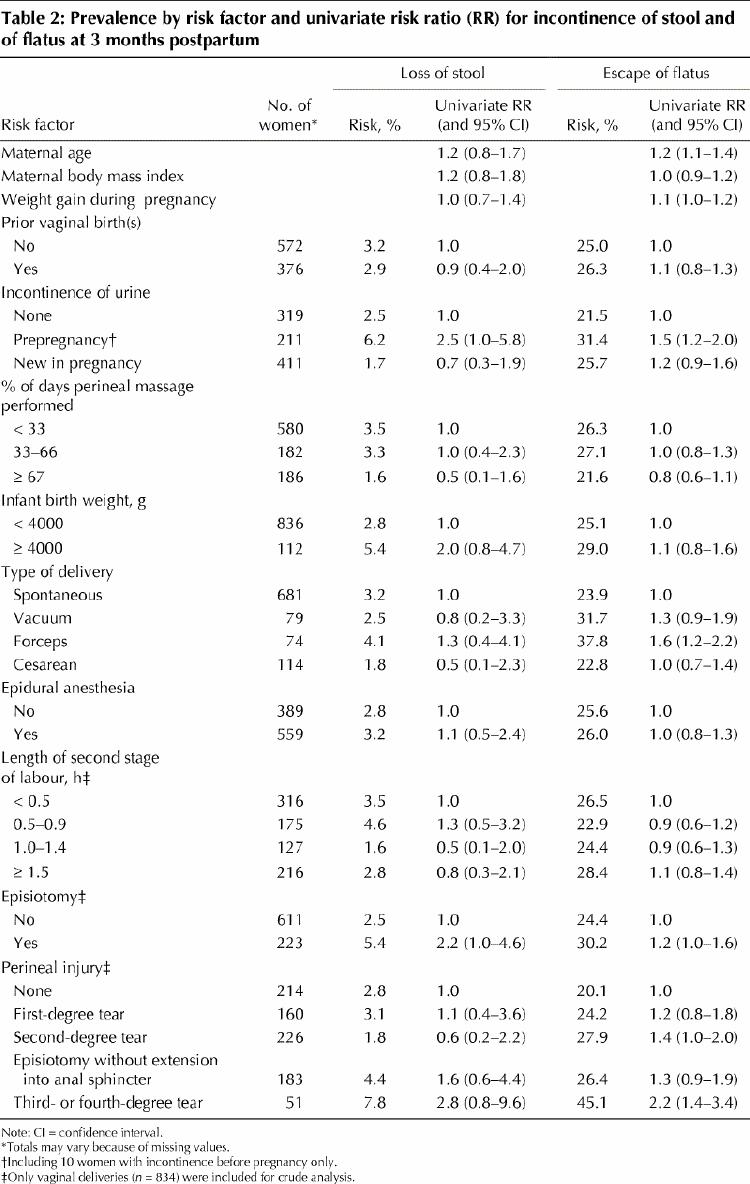
Among the women with forceps-assisted delivery, none of the 51 with an intact anal sphincter had incontinence of stool, as compared with 3 (13.0%) of the 23 with sphincter lacerations (p < 0.03, Fisher's exact test). Even after we excluded the data for the 51 women in whom an anal sphincter tear was recognized, fecal incontinence tended to be commoner among women with a median episiotomy (4.4% [8/183]) than among those who gave birth vaginally with a first- or second-degree laceration (2.3% [9/386]) (univariate RR 1.9, 95% CI 0.7–4.8). The latter had a risk of fecal incontinence similar to that of women with an intact perineum (2.8% [6/214]) (univariate RR 0.8, 95% CI 0.3–2.3). It was not possible to control simultaneously for multiple predictors in the analysis of incontinence of stool owing to the small number of women affected.
Involuntary escape of flatus was reported by 25.5% (242/948) of the women; in 2.6% (25/948) this occurred at least once daily (Table 1). The proportion of women affected was similar whether delivery was cesarean (22.8% [26/114]) or vaginal (25.9% [216/834]) (univariate RR 0.9, 95% CI 0.6–1.3). On univariate analysis operative vaginal delivery (compared with spontaneous delivery), anal sphincter tears and urinary incontinence before becoming pregnant were the only factors associated with incontinence of flatus (RR > 1.25) (Table 2). Women with incontinence of stool were more likely than those continent of stool to also have involuntary escape of flatus (65.5% [19/29] v. 24.3% [223/918]) (univariate RR 2.7, 95% CI 2.0–3.6). Neither natural hair colour nor the presence of stretch marks predicted incontinence of stool or of flatus (data not shown).
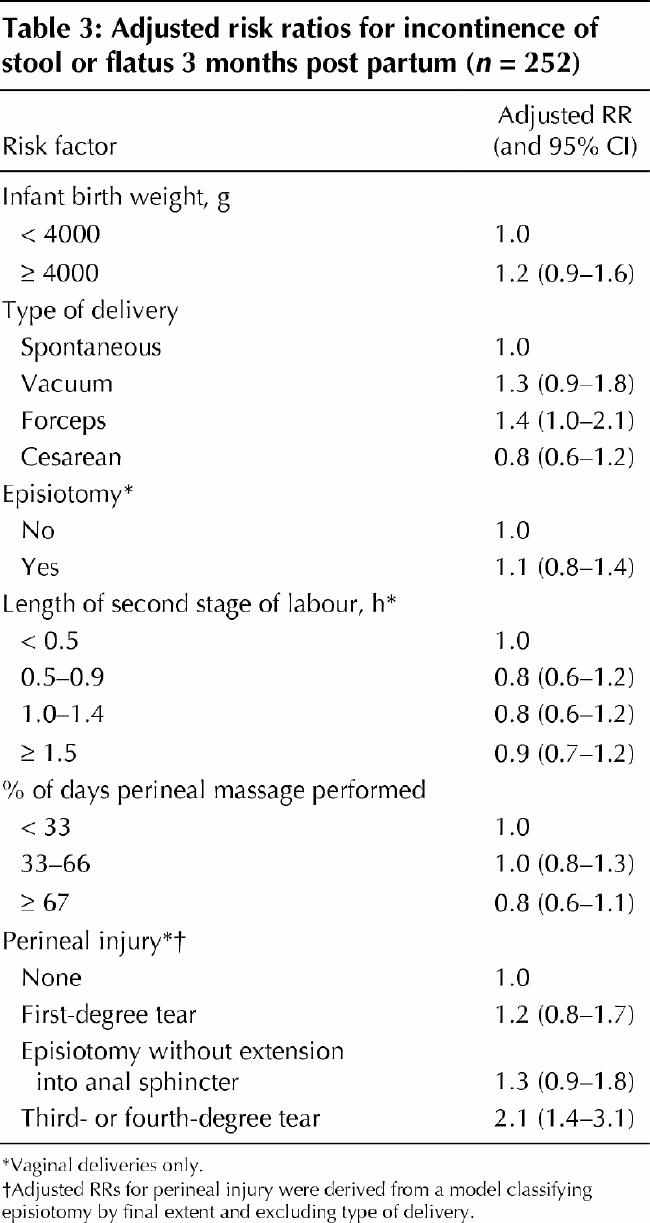
Overall, 252 women had incontinence of either flatus or stool. Multivariate analysis of predictors of postpartum anal incontinence (i.e., incontinence of either flatus or stool) showed a significant independent association with forceps (compared with spontaneous) delivery but not with vacuum extraction, episiotomy or cesarean section (Table 3). Maternal age, body mass index, parity and epidural anesthesia were not included in the adjusted model since they were not associated with anal incontinence on univariate analysis. When we replaced episiotomy and type of delivery by degree of perineal injury in the multivariate model, incontinence of flatus or stool was predicted by anal sphincter laceration but not by lesser degrees of perineal trauma (Table 3).
Table 3
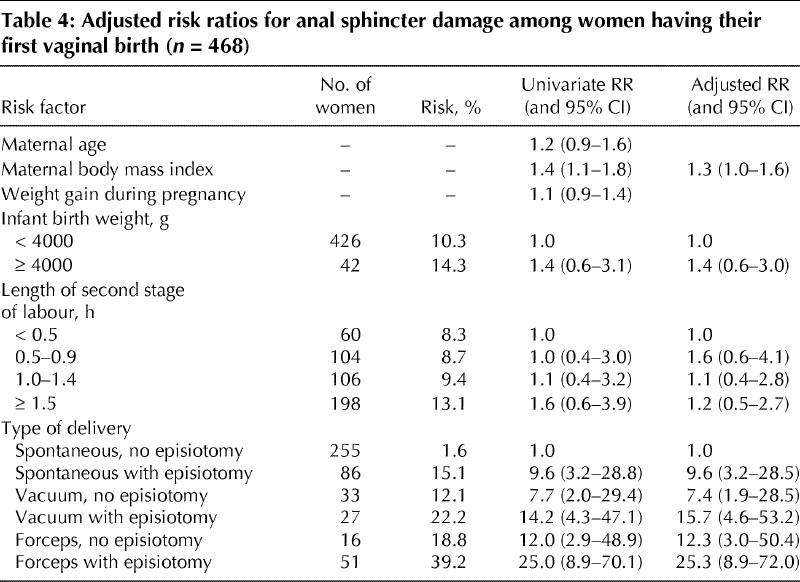
Anal sphincter tears were most strongly predicted by lack of previous vaginal birth: 10.7% (50/468) of women having a first vaginal birth had an anal sphincter tear, as compared with 0.3% (1/367) of women with a previous vaginal birth (RR 39.2, 95% CI 5.4–282.5). None of the 47 women with anal sphincter tears at a previous birth had an anal sphincter tear at the current birth. Median episiotomy and vacuum or forceps delivery were highly significant independent predictors of anal sphincter tears at first vaginal delivery (Table 4). Since there were significant interactions between median episiotomy and vacuum and forceps delivery, the relative risk of tears with each combination of interventions is presented in Table 4. In multivariate analysis the association between macrosomia and anal sphincter damage was not statistically significant (Table 4). The results did not change when this analysis was repeated with birth weight in quintiles: the adjusted RR of anal sphincter injury for the heaviest quintile (greater than 3820 g) compared with the lightest (less than 3050 g) was 1.32 (95% CI 0.55–3.18). The apparent increase in anal sphincter injury with duration of the second stage of labour on univariate analysis disappeared after adjustment for the confounding effects of episiotomy and operative delivery (Table 4). No association was found on univariate analysis between anal sphincter injury and perineal massage, stretch marks or epidural anesthesia.
Table 4
Interpretation
At 3 months post partum 3.1% of the women in our study were incontinent of stool, and 25.5% were incontinent of flatus. Similar levels of incontinence have been reported by other investigators.18,19 Although fecal incontinence has a more devastating effect on quality of life than does incontinence of flatus, the 2.6% of women with daily loss of flatus have an awkward and embarrassing problem. Lack of control over flatus is a common and persistent problem,7,20 so it is important to prevent.
Anal sphincter injury was associated with an increased rate of incontinence of feces (7.8%) and of flatus (45%), consistent with earlier findings.1,4,7,9,10,11 Forceps delivery also increased the risk of anal incontinence. Signorello and colleagues4 found a higher rate of incontinence of stool among women who had had an episiotomy than among those with spontaneous lacerations, even after excluding anal sphincter tears; we found a relative risk of 1.9, which was not statistically significant. Further study of this issue with a larger sample is warranted: if there is a true increase in risk with episiotomy, it would be clinically important enough to alter obstetric management.
Anal incontinence was associated with urinary incontinence. Although anal sphincter defects are usually identifiable in postpartum anal incontinence, this does not explain the association with urinary incontinence. Research using endoanal sonography in conjunction with MRI scanning may elucidate the anatomic damage to the mechanisms of continence.
Giving birth vaginally for the first time predicts anal sphincter injury:21 the RR of 39.2 in our study is striking. The central role of median episiotomy and operative delivery, especially forceps delivery, in causing anal sphincter damage in these women has been demonstrated previously.15,22,23,24 Performing median episiotomy at the time of operative delivery adds markedly to the risk of sphincter laceration. Avoiding episiotomy and using mediolateral episiotomy if necessary would decrease the risk of anal sphincter damage.25
We found no association between epidural anesthesia and anal incontinence or sphincter injury. Donnelly and associates2 reported that anal sphincter injury (defined as symptoms or abnormal laboratory results) was related to epidural anesthesia and length of the second stage of labour. However, when we took episiotomy and operative delivery into account, neither the length of the second stage of labour nor the baby's birth weight were significantly associated with anal incontinence or sphincter laceration.
Our findings are important in understanding how best to manage the second stage of labour. Because of the reported association of pelvic floor damage with a long second stage and a large baby, obstetricians may be inclined to shorten the second stage by means of episiotomy and assisted delivery. Our results show that these very interventions may cause anal sphincter damage. When we controlled for these factors in the analysis, a long second stage of labour and large baby were not significantly associated with anal sphincter laceration or anal incontinence. Further investigation is needed to determine the role of active compared with passive management (early compared with late pushing) in the second stage of labour to prevent pelvic floor damage.
Footnotes
This article has been peer reviewed.
Acknowledgements: This study was supported by the Medical Research Council of Canada, the Fonds de la recherche en santé du Québec and Organon Canada. Dr. Marcoux holds a National Health Research Scholarship from Health Canada.
Competing interests: None declared.
Correspondence to: Dr. Erica Eason, Box 803, 501 Smyth Rd., Ottawa ON K1H 8L6; fax 613 739-6266; eeason@ohri.ca [Reprints will not be available.]
References
- 1.Crawford LA, Quint EH, Pearl ML, DeLancey JO. Incontinence following rupture of the anal sphincter during delivery. Obstet Gynecol 1993;82:527-31. [PubMed]
- 2.Donnelly V, Fynes M, Campbell D, Johnson H, O'Connell PR, O'Herlihy C. Obstetric events leading to anal sphincter damage. Obstet Gynecol 1998;92:955-61. [DOI] [PubMed]
- 3.Meyer S, Schreyer A, de Grandi P, Hohlfeld P. The effects of birth on urinary continence mechanisms and other pelvic-floor characteristics. Obstet Gynecol 1998;92:613-8. [DOI] [PubMed]
- 4.Signorello LB, Harlow BL, Chekos AK, Repke JT. Midline episiotomy and anal incontinence: retrospective cohort study. BMJ 2000;320:86-90. [DOI] [PMC free article] [PubMed]
- 5.Zetterstrom J, Lopez A, Anzen B, Norman M, Holmstrom B, Mellgren A. Anal sphincter tears at vaginal delivery: risk factors and clinical outcome of primary repair. Obstet Gynecol 1999;94:21-8. [PubMed]
- 6.MacArthur C, Bick DE, Keighley MRB. Faecal incontinence after childbirth. Br J Obstet Gynaecol 1997;104:46-50. [DOI] [PubMed]
- 7.Sultan AH, Kamm MA, Hudson CN, Thomas JM, Bartram CI. Anal sphincter disruption during vaginal delivery. N Engl J Med 1993;329:1905-11. [DOI] [PubMed]
- 8.Fynes M, Donnelly V, Behan M, O'Connell PR, O'Herlihy C. Effect of second vaginal delivery on anorectal physiology and faecal continence: a prospective study. Lancet 1999;354(9183):983-6. [DOI] [PubMed]
- 9.Bek KM, Laurberg S. Risks of anal incontinence from subsequent vaginal delivery after a complete obstetric anal sphincter tear. Br J Obstet Gynaecol 1992; 99:724-6. [DOI] [PubMed]
- 10.Haadem K, Ohrlander S, Lingman G. Long-term ailments due to anal sphincter rupture caused by delivery — a hidden problem. Eur J Obstet Gynecol Reprod Biol 1988;27(1):27-32. [DOI] [PubMed]
- 11.Mellerup SS, Bondesen H, Istre O, Vilmann P. Perineal rupture following vaginal delivery. Long-term consequences. Acta Obstet Gynecol Scand 1988;67 (4):315-8. [PubMed]
- 12.Haadem K, Dahlstrom JA, Lingman G. Anal sphincter function after delivery: a prospective study in women with sphincter rupture and controls. Eur J Obstet Gynecol Reprod Biol 1990;35(1):7-13. [DOI] [PubMed]
- 13.Sultan AH, Kamm MA. Faecal incontinence after childbirth. Br J Obstet Gynaecol 1997;104:979-82. [DOI] [PubMed]
- 14.Thorp JM Jr, Norton PA, Wall LL, Kuller JA, Eucker B, Wells E. Urinary incontinence in pregnancy and the puerperium: a prospective study. Am J Obstet Gynecol 1999;181:266-73. [DOI] [PubMed]
- 15.Labrecque M, Eason E, Marcoux S, Lemieux F, Pinault JJ, Feldman P, et al. Randomized controlled trial of prevention of perineal trauma by perineal massage during pregnancy. Am J Obstet Gynecol 1999;180:593-600. [DOI] [PubMed]
- 16.Labrecque M, Eason E, Marcoux S. Randomized trial of perineal massage during pregnancy: perineal symptoms three months after delivery. Am J Obstet Gynecol 2000;182:76-80. [DOI] [PubMed]
- 17.Skov T, Deddens J, Petersen MR, Endahl L. Prevalence proportion ratios: estimation and hypothesis testing. Int J Epidemiol 1998;27:91-5. [DOI] [PubMed]
- 18.Sleep J, Grant A. West Berkshire perineal management trial: three year follow up. BMJ 1987;295:749-51. [DOI] [PMC free article] [PubMed]
- 19.Wilson PD, Herbison RM, Herbison GP. Obstetric practice and the prevalence of urinary incontinence three months after delivery. Br J Obstet Gynaecol 1996;103:154-61. [DOI] [PubMed]
- 20.Farrell S, Allen VM, Baskett TF. Anal incontinence in primiparas. J Soc Obstet Gynaecol Can 2001;23:321-6. [DOI] [PubMed]
- 21.Peleg D, Kennedy CM, Merrill D, Zlatnik FJ. Risk of repetition of a severe perineal laceration. Obstet Gynecol 1999;93(6):1021-4. [DOI] [PubMed]
- 22.Labrecque M, Baillargeon L, Dallaire M, Tremblay A, Pinault JJ, Gingras S. Association between median episiotomy and severe perineal lacerations in primiparous women. CMAJ 1997;156:797-802. Available: www.cma.ca/cmaj/vol-156/issue-6/0797.htm [PMC free article] [PubMed]
- 23.Klein MC, Gauthier RJ, Jorgensen SH, Robbins JM, Kaczorowski J, Johnson B, et al. Does episiotomy prevent perineal trauma and pelvic floor relaxation? [article] Online J Curr Clin Trials 1992;Jul 1(doc 10)[6019 words]. [DOI] [PubMed]
- 24.Coats PM, Chan KK, Wilkins M, Beard RJ. A comparison between midline and mediolateral episiotomies. Br J Obstet Gynaecol 1980;87:408-12. [DOI] [PubMed]
- 25.Eason EL, Labrecque M, Well G, Feldman P. Preventing perineal trauma during childbirth: a systematic review. Obstet Gynecol 2000;95:464-71. [DOI] [PubMed]