

Abstract
Background
Patients with colorectal cancer who undergo surgery face many postoperative problems. These problems include the risk of relapse, side effects, and long-term complications.
Objective
This study sought to design and develop a remote monitoring system as a technological solution for the postdischarge care of these patients.
Methods
This research was conducted in 3 main steps: system feature extraction, system design, and evaluation. After feature extraction from a systematic review, the necessary features were defined by 18 clinical experts in Iran. In the next step, the architecture of the system was designed based on the requirements; the software and hardware parts of the system were embedded in the architecture, then the software system components were drawn using the unified modeling language diagrams, and the details of software system implementation were identified. Regarding the hardware design, different accessible hardware modules were evaluated, and suitable ones were selected. Finally, the usability of the system was evaluated by demonstrating it over a Skype virtual meeting session and using Nilsen’s usability principles.
Results
A total of 21 mandatory features in 5 main categories, including patient information registration, periodic monitoring of health parameters, education, reminders, and assessments, were defined and validated for the system. The software was developed using an ASP.Net core backend, a Microsoft SQL Server database, and an Ionic frontend alongside the Angular framework, to build an Android app. The user roles of the system included 3 roles: physicians, patients, and the system administrator. The hardware was designed to contain an Esp8266 as the Internet of Things module, an MLX90614 infrared temperature sensor, and the Maxim Integrated MAX30101 sensor for sensing the heartbeat. The hardware was designed in the shape of a wristband device using SolidWorks 2020 and printed using a 3D printer. The firmware of the hardware was developed in Arduino with the capability of firmware over the air. In evaluating the software system from the perspective of usability, the system received an average score of 3.8 out of 5 from 4 evaluators.
Conclusions
Sensor-based telemonitoring systems for patients with colorectal cancer after surgery are possible solutions that can make the process automatic for patients and caregivers. The apps for remote colorectal patient monitoring could be designed to be useful; however, more research regarding the developed system’s implementation in clinic settings and hospitals is required to understand the probable barriers and limitations.
Keywords: eHealth, telemedicine, colorectal cancer, cancer survivor, IoT, mHealth, patient monitoring, remote monitoring, postdischarge care, cancer, patient care, cancer care, postoperative complications
Introduction
Cancer is one of the leading causes of death worldwide. According to reported statistics by the World Health Organization in 2021, this disease was the cause of nearly 10 million deaths worldwide [1].
Among the types of cancer, colorectal cancer (CRC) has the highest incidence of new gastrointestinal cancers globally. CRC includes the colon and rectal cancers [2]. New CRC cases are 19.7 per 100,000 people globally and 12.9 in Iran [3]. In a review conducted in 2019, CRC was reported to be one of the most common cancers among Iranian men and women in the whole review investigation period (2004-2009) [4]. In 2020, CRC accounted for 10% (1.9 million cases) of global cancer incidence and 9.4% (0.9 million deaths) of cancer deaths. CRC is the third-most deadly cancer in both genders worldwide. The international number of new CRC cases, based on population growth, aging projection, and human development, is predicted to reach 3.2 million in 2040 [5].
Strategies of treatment for CRC vary according to the stage and type of cancer. Some treatment procedures include endoscopy for macroscopic intramucosal carcinoma, surgical lymph node dissection, laparoscopic surgery, palliative chemotherapy, radiotherapy, extensive surgery, and local ablative therapies for metastases [5,6].
In the meantime, CRC surgery is associated with many different complications that affect the efficacy of the surgery and patients’ overall health and survival [6]. The most frequent postoperative surgical complications after colorectal resections are surgical site infection, anastomotic leakage, intra-abdominal abscess, ileus, and bleeding. These complications have different influences on the outcomes and have to be diagnosed accurately. Monitoring and standardization of postoperative care to minimize these complications are essential [7].
Most of these complications usually occur in the first week [8] to the first month [9] after surgery. Therefore, these patients need continuous care during this period. Due to the lack of specialized personnel and their high workload [10], on the one hand, and the high costs of health care for patients with cancer [11], on the other, the importance of technology-based intervention to monitor the condition of surgical patients after discharge is increasing.
In addition, the 5 most common factors in admitting patients with cancer to the intensive care unit include sepsis, respiratory failure, heart failure, cardiopulmonary resuscitation, and surgical complications [12]. Monitoring the patients could help early detection of these complications. Moreover, patient monitoring can give the physician a clear vision of the discharged patient’s health status. If patients are not monitored and followed after discharge, different events may occur, including emergency conditions, unplanned readmission to the intensive care unit, unplanned resurgery, or specific complications such as infection [13].
Telemedicine services have become a powerful solution for providing health services. Studies show the impact of telemedicine services on time savings, patient transportation, and cost savings. The use of these technologies can satisfy patients and health care providers and facilitate their affairs [14]. Since it has been estimated that patients tend to use mobile apps in the postsurgery period [15], it is possible to create a platform to facilitate communication between the patient and the care team using mobile technologies [16], especially smartphones. Health care providers make decisions based on laboratory tests, reports, and self-reported data and according to the patient’s symptoms [17]. So, mobile apps have been developed to monitor patients’ postdischarge and recovery duration [17,18].
In this regard, similar previous studies were accomplished for remote care, self-management, and telemonitoring of patients with cancer after surgery by applying telephone calls, messaging systems, web portals, and mobile apps [19-21].
Also, more specific studies have been carried out for postoperative telemonitoring, education, and self-care in CRC [22-25]. For example, Keng et al [26] developed an integrated discharge monitoring system based on a mobile app to support patients at home after colorectal surgery. Their study included 106 participants, and 93 of them used the designed apps. Another study by Miller et al [22] developed a remote monitoring application to support and improve the care of patients with CRC for the first 30 postoperative days. Their study included 9 clinicians and 10 patients in phase 1 of their study, which was conducted to identify the views of patients and clinicians regarding the remote monitoring app. Phase 2, which included 15 clinicians and 8 patients, was conducted to evaluate the views and usability of a paper-based version of the app. Sun et al [23], in a pilot study, developed a wireless outcomes monitoring program for major abdominal cancer surgery. The study evaluated their system on 20 patients. In a recent study by Salmani et al [25], a smartphone-based app for the self-management of patients with CRC was developed. In another former study, Kim et al [24] developed and assessed a mobile web-based educational program for patients with CRC undergoing enhanced recovery after surgery. In their study, 59 colorectal patients were assigned to the treatment group that received mobile health intervention, and 59 patients were assigned to the conventional care group.
Despite the research conducted on remote monitoring apps for CRC survivors, there has still been a research gap in the development of a system for telemonitoring patients with CRC after surgery equipped with sensors that can collect the data on time and give the patients suitable messages based on the situation. These multiuser mobile-based monitoring systems could provide the ability to collect, analyze, and give proper feedback to both patients and health care providers simultaneously.
Due to the issues raised and the lack of electronic systems for remote monitoring of patients with CRC in Iran, there is a need to develop such a monitoring system. Therefore, the study’s purpose is to design and evaluate a remote monitoring system for patients with CRC undergoing surgery.
Methods
Ethics Approval
The clinician experts evaluated the proposed software system for proof of concept; no patient data were used in this study. The Research Ethics Committees of the School of Public Health and Allied Medical Sciences, Tehran University of Medical Sciences approved the current research ethics with the approval ID IR.TUMS.SPH.REC.1399.270.
System Development
In the first step, the requirements of such a system were gathered from the literature and the opinions of experts. This step is explained in detail in our previous research [27]. After this step, a system architecture containing software and hardware was designed to fulfill the requirements. The software and hardware were developed based on the available technologies and tools.
Software Design
To design the software, use case diagrams are designed and evaluated for this system. After this step, the suitable tools to create the software systems were chosen, and the software was created. The REST (representational state transfer) architecture was used to develop the web service, and the PWA (progressive web application) approach was used to enable the software to run offline using cached data.
Due to the diversity of users’ devices (Android [Google Inc]–based and iOS [Apple Inc]–based phones) for developing client-side software, the Ionic software development kit on the Angular framework was used to develop a mobile hybrid app. After the client-side programming (in Visual Studio Code v1.52 [Microsoft]), the outputs were generated as PWA and Android-based software. The output of the Java code was generated and then compiled by the Android Studio 4.1.1 Integrated Development Environment (IDE).
Hardware Design
Due to the need for hardware customization, hardware was designed and created. The hardware is designed to be a wristband with the capability of sensing the heartbeat and body temperature. For this purpose, photoplethysmography (PPG) sensors, temperature sensors, Internet of Things (IoT) modules, batteries, and display modules were selected among the available options. To select the appropriate PPG sensor, due to the elimination of ambient noise and higher accuracy requirements, MAX30101, a ready-made module, was selected. Next, an IoT module, the Wemos D1 mini development board (based on the ESP8266mod), was selected based on its appropriate capabilities and price. An MLX90614 infrared thermometer is used as the temperature sensor. Other components, such as the battery and the display, were chosen in the next step. After selecting the hardware modules, the hardware prototype circuit was created on a breadboard. The firmware was developed in Arduino and then finalized by designing and printing the circuit on a printed circuit board. A wristband enclosure for the board is designed in SolidWorks 2019 software (SolidWorks Corp) and printed using a 3D printer.
System Usability Evaluation
After creating the system, to perform usability evaluation, explanations of the system were provided to 4 experts (this number corresponds to the number of evaluators (3 to 5 people) proposed by Nielsen [28]) in a virtual session through Skype software (Skype Technologies, a division of Microsoft). By providing the username and password to log in to the system, they were asked to evaluate the system’s usability by completing an online questionnaire. This questionnaire was designed based on Nielsen’s 10 principles [29]. Finally, 4 experts evaluated the system.
Results
System Development
The set of eHealth system capabilities related to patients with CRC and survivors obtained from the categorization of requirements is given in Textbox 1.
The set of eHealth system capabilities related to colorectal cancer patients and survivors.
Patient information registration
Registration of patient social and demographic information
Registration of the details of diagnosis and preoperative treatments
Registration of surgical specifications and postoperative treatments
Periodic monitoring of health parameters
Weight monitoring
Side effects monitoring
Education
Cancer information
Common issues and problems for colorectal cancer patients and survivors
Information about medication
Information about chemotherapy
Nutrition information
Information about rehabilitation
Information about the treatment process
Informing about postdischarge care
Information on pain management
Information on emergency management
Reminders
Reminders of hospital referrals
Reminder for drug use
Patient-tailored information
Assessments
Quality of life assessment
Nutrition status assessment
Physician-patient relationship assessment
According to the expected capabilities of the system, the general architecture of the system consists of 3 software parts: client-side application, web service, and database. A hardware part containing a smart wristband has also been embedded in the architecture (Figure S1 in Multimedia Appendix 1).
Software Design
The Microsoft Visual Studio 2019 IDE and Microsoft SQL Server 2019 were used to develop server-side software (back end) and database, respectively. The web services were implemented with the ASP.NET Core framework (Microsoft).
The Visual Studio Code v1.51.1 IDE was used to develop the client-side software (front end). As a mobile hybrid app, Ionic software development kit and Angular framework were used for software development.
The output of the Android-based app was created (Figure 1). The system data items were designed to be flexible so that the specialist could add the required data item to the system if not by default. The client-side app includes 3 panels for survivors, clinicians, and admin, as shown in Figure 2.
Figure 1.
The “Behyar” Android app.
Figure 2.

Behyar app. (A) A page in the survivor panel for entering the side effect. The drop-down shown on top is for selecting the side effect. The slider shown with a fire icon is for choosing the intensity of that side effect, and the last input is for selecting the date and time of occurrence. (B) A page in the clinician panel to monitor the side effects of the survivor. The figure shows the intensity of appetite loss on multiple dates. (C) A page in the Admin panel for managing clinicians in the system. The page shows the information of 2 clinicians and a form for adding a new clinician to the system.
Hardware Design
The hardware block diagram of the designed device is shown in Figure 3.
Figure 3.
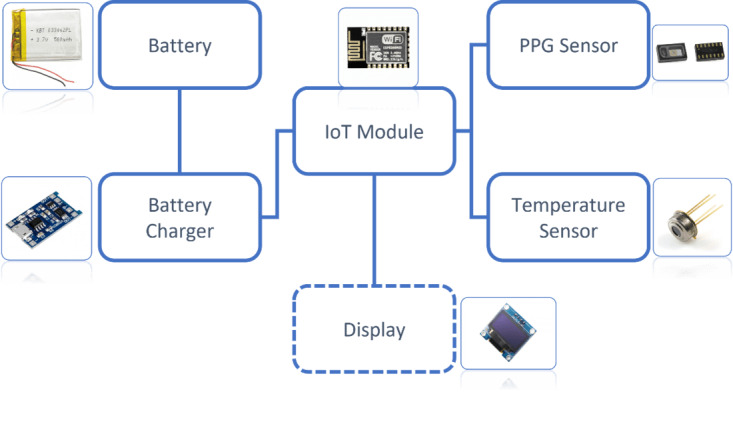
Hardware block diagram of the wristband. PPG: photoplethysmography.
The MAX30101 PPG signal obtained from the wrist is shown in Figure 4A. The red, blue, and green colors show the PPG signals from RED, IR, and GREED LEDs, respectively. For smoothing the signal obtained from the MAX30101 module, the fast Fourier transform technique was used. The frequencies greater than 4 Hz and less than 0.5 Hz were filtered (Figure 4B).
Figure 4.
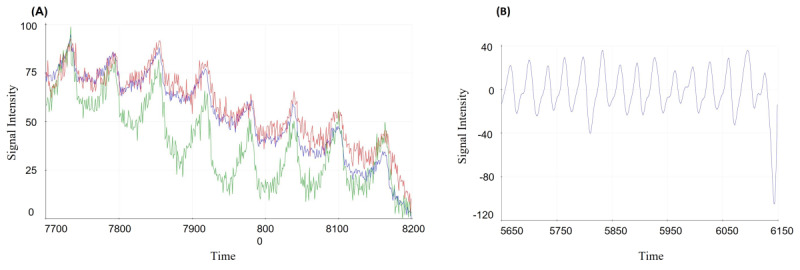
Photoplethysmography (PPG) signal retrieved from the MAX30101 PPG sensor. (A) Raw PPG signal from the wrist. (B) PPG signal after applying a filter.
The prototype of the circuit was developed with modules on the breadboard (Figure S2A in Multimedia Appendix 1), the firmware code was written in the Arduino IDE, and the firmware was uploaded to the Wemos D1 mini development board. The soldering of parts was performed on a printed circuit board (Figure S2B in Multimedia Appendix 1). The assembled hardware is shown in Figure S2C in Multimedia Appendix 1. The hardware’s firmware was developed to have the capability of being upgraded remotely (FOTA: Firmware Over-The-Air).
The enclosure was designed to fit the dimensions of the circuit shown in Figure S3A in Multimedia Appendix 1. After the 3D design of the frame, the 3D prototype of the enclosure was printed. Finally, the wristband was created, as shown in Figure S3B in Multimedia Appendix 1.
The Arduino IDE was used for hardware programming. Altium Designer 2020 (Altium Limited) and SolidWorks 2019 were used for designing the printed circuit board and the frame, respectively.
System Usability Evaluation
The 4 male experts finally evaluated the current software of the system in terms of usability based on Nielsen’s 10 principles. The experts included cancer surgeons, radiation oncologists, and blood and cancer subspecialists with a mean age of 45 years and an average of 12 years of clinical experience. According to the results presented in Table 1, this system generally gained an average score of 3.8 out of 5 in terms of usability.
Table 1.
Result of system usability evaluation based on Nielsen’s 10 principles.
| Items | Score 1 | Score 2 | Score 3 | Score 4 | Score 5 | Average score |
| Visibility of system status (very confusing to very clear) | 0 | 0 | 1 | 1 | 2 | 4.25 |
| Match between the system and the real world (irrational to very logical) | 0 | 1 | 2 | 1 | 0 | 3 |
| User control and freedom (this is not possible to this is very convenient) | 0 | 0 | 0 | 4 | 0 | 4 |
| Consistency and standards (vague to clear) | 0 | 0 | 1 | 3 | 0 | 3.75 |
| Error prevention (never to always) | 0 | 0 | 0 | 4 | 0 | 4 |
| Recognition rather than recall (from inappropriate to appropriate) | 0 | 1 | 0 | 0 | 3 | 4.25 |
| Flexibility and efficiency of use (very inappropriate to very appropriate) | 0 | 1 | 1 | 1 | 1 | 3.5 |
| Aesthetic and minimalist design (very inappropriate to very appropriate) | 0 | 0 | 1 | 1 | 2 | 4.25 |
| Recognize, diagnose, and recover from errors (never to always) | 0 | 1 | 0 | 2 | 1 | 3.75 |
| Help and documentation (inadequate to appropriate) | 0 | 1 | 1 | 2 | 0 | 3.25 |
Discussion
Principal Findings
In this study, the system for remote monitoring of patients undergoing surgery due to CRC was designed according to the identified priorities. The architecture was considered front end and back end separately for modular designing and creating multiple program versions to run on different platforms [30].
Based on the overall architecture of the system, suitable tools were applied to create the system. ASP.NET Core 3.1 was used because of its open-source, multiplatform capability, and flexibility in development. Security and access levels were defined based on the roles defined in the system and access tokens on the web service.
Client-side software was designed to be hybrid to run on different platforms. PWA and Android software have been used in various fields of health care [31-33]. Secure Sockets Layer protocol was installed on the webserver for communication security. Since the core of the current system’s software is designed as a web service, it is possible to integrate it with other software systems.
Off-the-shelf commercial wristbands with the ability to measure heart rate along with body temperature were not found in the Iranian market at a reasonable price. Thus, the wristband device is designed. The detection of the heartbeat was enabled on the hardware device by PPG technology. PPG technology is a noninvasive technology for measuring various indicators such as heart rate [34] and blood pressure [35]. It is used by a ready-made module (MAX30101) to eliminate noise and reach the signal with higher accuracy.
The findings show that green light has a better PPG signal than red and infrared light due to its greater penetration power in the wrist tissue. This is also mentioned by Fortino and Giampà [35]. The filter (fast Fourier transform algorithm) was used to remove noise, improving signal quality.
It is noteworthy that the price of the sensor selected to measure body temperature following the COVID-19 pandemic and the high demand for this sensor to measure body temperature were about 15 times the price increase, making it difficult to provide.
The use of IoT technologies to design system hardware was considered in this study. The whole system could be considered a Medical Internet of Things system. Medical Internet of Things refers to IoT applications in medicine [36]. The 4 IoT core modules were selected and evaluated for suitability. However, the modules that can communicate via General Packet Radio Services require minimal user intervention (there is no need for a pairing process). Due to the requirements of the electronic components for proper operation, especially in conditions with a weak signal antenna, these modules were not used. The ESP8266MOD module with Wi-Fi capability was selected. This module is suitable for connecting sensors and sending sensor data to the central server [37]. Other modules have also been used in studies. For example, in the study of Onubeze [38], the nRF51822 with the MAX30100 module was used to design a wireless heart rate monitor. IoT-based hardware can measure temperature and the PPG signal. This hardware can also be used to measure blood pressure and blood oxygen saturation [39]. If monitoring physical activity is a priority in other diseases, this feature can be added to the wristband by adding accelerometer and pedometer sensors. An intelligently integrated model of the health care system for cancer care is presented in the Onasanya and Elshakankiri study [40]. This model provides 4 layers of cancer care, hospital, data, and service layer, which are designed hardware that can be used in the cancer care layer.
In this study, the wristband enclosure was designed in SolidWorks software and printed using a 3D printer. Due to the high speed of preparation, 3D printing is recommended as a suitable method for making the prototype.
In this study, web software technologies and mobile apps were used. In similar studies, Mayer et al [41], Cheong et al [42], Keng et al [26], and Miller et al [22] used mobile and web applications were used. In the Maxwell-Smith et al [43] study, there is no reference to the technology applied in the system software.
Concerning the hardware presented in this study, the ability to measure heart rate and body temperature was considered. In the study of Miller et al [22], the health professionals for future apps proposed applying wearable outcome measures for detecting increased heart rate and temperature as the key measures that would be helpful in clinical assessments and remote monitoring of CRC surgery.
In other studies related to the monitoring of patients with cancer, for example, Maxwell-Smith et al [43] and Jonker et al [21] applied a commercially available wearable activity monitor (Fitbit) to monitor physical activity, and in another study by Cheong et al [42], hardware was used to monitor physical activity and heart rate. In Sun et al’s [23] study, commercially available wristband pedometers were used to capture data on daily steps for functional recovery monitoring after major abdominal cancer surgery.
In general, based on the advantages expressed in most studies [21,23,44], novel approaches and technology-based solutions to postoperative assessment based on subjective and objective measures and timely intervention in the surgical oncology setting are beneficial. This could improve long-term outcomes and facilitate providing health services. So the development and evaluation of these systems for various cancer surgeries are recommended.
Strength and Limitations
The system designed in this research was the first monitoring system designed for CRC survivors in Iran, which could be assumed as the strength of this research.
A major limitation of this study was the initial evaluation of the software’s usability. The evaluation of the proposed system should be performed in multiple aspects with the involvement of more experts and patients. Due to the resource limitations in this study, we decided to limit the study’s scope in the initial usability evaluation. Another limitation is the availability of hardware sensors and modules in the Iranian market, which limits the choice of sensors in the hardware design.
Conclusions
The results showed that the use of a mobile health app could be used to monitor CRC patients. By including features such as the possibility of changing information items by the expert, the system can be provided with the necessary flexibility in different conditions. Additionally, creating hardware for monitoring vital signs along with system software in terms of creating customization capabilities can help obtain quantitative and qualitative data from patients and survivors to possibly provide better care. From the specialists’ perspective, user interface evaluation of monitoring systems for surgical patients with CRC can achieve an acceptable score. To better understand the usefulness of such systems, in addition to evaluating the user interface, continuous surveys of the system’s effects on indicators such as patients’ quality of life, improving their complications, their nutritional status, and their satisfaction with using the system should be considered.
Acknowledgments
This work was supported by the Tehran University of Medical Sciences (Grant number 26299).
Abbreviations
- CRC
colorectal cancer
- IDE
Integrated Development Environment
- IoT
Internet of Things
- PPG
photoplethysmography
- PWA
progressive web application
The system architecture and hardware.
Data Availability
The data sets generated and analyzed during this study are available from the corresponding author upon reasonable request.
Footnotes
Authors' Contributions: MS, SRNK, and SMA contributed to the study conception and design. Material preparation and analysis were performed by SMA. System evaluation was done by KR, RG, FM, and AJ. The first draft of the manuscript was written by SMA. TB contributed to organizing and writing the final version of the manuscript, and NM was the advisor of the project. SRNK and MS supervised the project, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Conflicts of Interest: None declared.
References
- 1.Cancer. World Health Organization. [2023-01-20]. https://www.who.int/news-room/fact-sheets/detail/cancer .
- 2.Benson AB, Venook AP, Al-Hawary MM, Arain MA, Chen Y, Ciombor KK, Cohen S, Cooper HS, Deming D, Farkas L, Garrido-Laguna I, Grem JL, Gunn A, Hecht JR, Hoffe S, Hubbard J, Hunt S, Johung KL, Kirilcuk N, Krishnamurthi S, Messersmith WA, Meyerhardt J, Miller ED, Mulcahy MF, Nurkin S, Overman MJ, Parikh A, Patel H, Pedersen K, Saltz L, Schneider C, Shibata D, Skibber JM, Sofocleous CT, Stoffel EM, Stotsky-Himelfarb E, Willett CG, Gregory KM, Gurski LA. Colon cancer, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19(3):329–359. doi: 10.6004/jnccn.2021.0012.jnccnGLS1903 [DOI] [PubMed] [Google Scholar]
- 3.Estimated age-standardized incidence rates (world) in 2018, all cancers, both sexes, all ages. International Agency for Research on Cancer. 2018. [2023-01-20]. https://tinyurl.com/mrxsppp4 .
- 4.Danaei M, Haghdoost A, Momeni M. An epidemiological review of common cancers in Iran; a review article. Iran J Blood Cancer. 2019;11(3):77–84. [Google Scholar]
- 5.Xi Y, Xu P. Global colorectal cancer burden in 2020 and projections to 2040. Transl Oncol. 2021;14(10):101174. doi: 10.1016/j.tranon.2021.101174. https://linkinghub.elsevier.com/retrieve/pii/S1936-5233(21)00166-2 .S1936-5233(21)00166-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pak H, Maghsoudi LH, Soltanian A, Gholami F. Surgical complications in colorectal cancer patients. Ann Med Surg. 2020;55:13–18. doi: 10.1016/j.amsu.2020.04.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kirchhoff P, Clavien PA, Hahnloser D. Complications in colorectal surgery: risk factors and preventive strategies. Patient Saf Surg. 2010 Mar 25;4(1):5. doi: 10.1186/1754-9493-4-5. https://pssjournal.biomedcentral.com/articles/10.1186/1754-9493-4-5 .1754-9493-4-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cleeland CS, Wang XS, Shi Q, Mendoza TR, Wright SL, Berry MD, Malveaux D, Shah PK, Gning I, Hofstetter WL, Putnam JB, Vaporciyan AA. Automated symptom alerts reduce postoperative symptom severity after cancer surgery: a randomized controlled clinical trial. J Clin Oncol. 2011 Mar 10;29(8):994–1000. doi: 10.1200/JCO.2010.29.8315. https://europepmc.org/abstract/MED/21282546 .JCO.2010.29.8315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kazaure HS, Roman SA, Sosa JA. Association of postdischarge complications with reoperation and mortality in general surgery. Arch Surg. 2012 Dec;147(11):1000–7. doi: 10.1001/2013.jamasurg.114.1392155 [DOI] [PubMed] [Google Scholar]
- 10.Huang JH, Su TY, Raknim P, Lan KC. Implementation of a wireless sensor network for heart rate monitoring in a senior center. Telemed J E Health. 2015;21(6):493–498. doi: 10.1089/tmj.2014.0081. [DOI] [PubMed] [Google Scholar]
- 11.Financial burden of cancer care. National Cancer Institute Cancer Trends Progress Report. 2021. [2023-01-20]. https://progressreport.cancer.gov/after/economic_burden .
- 12.Hawari FI, Nazer LH, Addassi A, Rimawi D, Jamal K. Predictors of ICU admission in patients with cancer and the related characteristics and outcomes: a 5-year registry-based study. Crit Care Med. 2016 Mar;44(3):548–53. doi: 10.1097/CCM.0000000000001429. [DOI] [PubMed] [Google Scholar]
- 13.Huizinga E. Early recognition of the deteriorating surgical patient using HealthPatch MD, a wireless and wearable vital signs monitor–an early clinical feasibility study [Master's thesis] University of Twente. 2017. [2023-01-20]. https://essay.utwente.nl/72821/
- 14.Gunter RL, Chouinard S, Fernandes-Taylor S, Wiseman JT, Clarkson S, Bennett K, Greenberg CC, Kent K Craig. Current use of telemedicine for post-discharge surgical care: a systematic review. J Am Coll Surg. 2016;222(5):915–927. doi: 10.1016/j.jamcollsurg.2016.01.062. https://europepmc.org/abstract/MED/27016900 .S1072-7515(16)00147-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Abelson JS, Symer M, Peters A, Charlson M, Yeo H. Mobile health apps and recovery after surgery: what are patients willing to do? Am J Surg. 2017;214(4):616–622. doi: 10.1016/j.amjsurg.2017.06.009.S0002-9610(17)30230-1 [DOI] [PubMed] [Google Scholar]
- 16.Pareek P, Vishnoi JR, Kombathula SH, Vyas RK, Misra S. Teleoncology: the youngest pillar of oncology. JCO Glob Oncol. 2020 Oct;6:1455–1460. doi: 10.1200/GO.20.00295. https://europepmc.org/abstract/MED/32997540 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Semple JL, Armstrong KA. Mobile applications for postoperative monitoring after discharge. CMAJ. 2017;189(1):E22–E24. doi: 10.1503/cmaj.160195. http://www.cmaj.ca/cgi/pmidlookup?view=long&pmid=27920015 .cmaj.160195 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Semple JL, Sharpe S, Murnaghan ML, Theodoropoulos J, Metcalfe KA. Using a mobile app for monitoring post-operative quality of recovery of patients at home: a feasibility study. JMIR mHealth uHealth. 2015;3(1):e18. doi: 10.2196/mhealth.3929. https://mhealth.jmir.org/2015/1/e18/ v3i1e18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Young JM, Butow PN, Walsh J, Durcinoska I, Dobbins TA, Rodwell L, Harrison JD, White K, Gilmore A, Hodge B, Hicks H, Smith S, O'Connor G, Byrne CM, Meagher AP, Jancewicz S, Sutherland A, Ctercteko G, Pathma-Nathan N, Curtin A, Townend D, Abraham NS, Longfield G, Rangiah D, Young CJ, Eyers A, Lee P, Fisher D, Solomon MJ. Multicenter randomized trial of centralized nurse-led telephone-based care coordination to improve outcomes after surgical resection for colorectal cancer: the CONNECT intervention. J Clin Oncol. 2013 Oct 01;31(28):3585–91. doi: 10.1200/JCO.2012.48.1036.JCO.2012.48.1036 [DOI] [PubMed] [Google Scholar]
- 20.Panda N, Solsky I, Huang EJ, Lipsitz S, Pradarelli JC, Delisle M, Cusack JC, Gadd MA, Lubitz CC, Mullen JT, Qadan M, Smith BL, Specht M, Stephen AE, Tanabe KK, Gawande AA, Onnela J, Haynes AB. Using smartphones to capture novel recovery metrics after cancer surgery. JAMA Surg. 2020;155(2):123–129. doi: 10.1001/jamasurg.2019.4702. https://europepmc.org/abstract/MED/31657854 .2753807 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jonker LT, Lahr MMH, Oonk MHM, de Bock GH, van Leeuwen BL. Post-discharge telemonitoring of physical activity, vital signs, and patient-reported symptoms in older patients undergoing cancer surgery. Ann Surg Oncol. 2021;28(11):6512–6522. doi: 10.1245/s10434-021-09707-3. https://europepmc.org/abstract/MED/33641013 .10.1245/s10434-021-09707-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Miller M, Roxburgh CS, McCann L, Connaghan J, Van-Wyk H, McSorley S, Maguire R. Development of a remote monitoring application to improve care and support patients in the first 30 days following colorectal cancer surgery. Semin Oncol Nurs. 2020;36(6):151086. doi: 10.1016/j.soncn.2020.151086. https://strathprints.strath.ac.uk/74924/ S0749-2081(20)30101-7 [DOI] [PubMed] [Google Scholar]
- 23.Sun V, Dumitra S, Ruel N, Lee B, Melstrom L, Melstrom K, Woo Y, Sentovich S, Singh G, Fong Y. Wireless monitoring program of patient-centered outcomes and recovery before and after major abdominal cancer surgery. JAMA Surg. 2017;152(9):852–859. doi: 10.1001/jamasurg.2017.1519. https://europepmc.org/abstract/MED/28593266 .2629732 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kim BY, Park KJ, Ryoo SB. Effects of a mobile educational program for colorectal cancer patients undergoing the enhanced recovery after surgery. Open Nurs J. 2018;12(1):142–154. doi: 10.2174/1874434601812010142. https://europepmc.org/abstract/MED/30197720 .TONURSJ-12-142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Salmani H, Nahvijou A, Sheikhtaheri A. Smartphone-based application for self-management of patients with colorectal cancer: development and usability evaluation. Support Care Cancer. 2022 May;30(4):3249–3258. doi: 10.1007/s00520-021-06754-0.10.1007/s00520-021-06754-0 [DOI] [PubMed] [Google Scholar]
- 26.Keng CJS, Goriawala A, Rashid S, Goldstein R, Schmocker S, Easson A, Kennedy E. Home to stay: an integrated monitoring system using a mobile app to support patients at home following colorectal surgery. J Patient Exp. 2020;7(6):1241–1246. doi: 10.1177/2374373520904194. https://journals.sagepub.com/doi/10.1177/2374373520904194?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_2374373520904194 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ayyoubzadeh SM, Shirkhoda M, Rostam Niakan Kalhori S, Mohammadzadeh N, Zakerabasali S. A smartphone remote monitoring app to follow up colorectal cancer survivors: requirement analysis. JMIR Cancer. 2022;8(1):e18083. doi: 10.2196/18083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Nielsen J. How to conduct a heuristic evaluation. Nielsen Norman Group. [2023-01-20]. https://www.nngroup.com/articles/how-to-conduct-a-heuristic-evaluation/
- 29.Nielsen J. 10 usability heuristics for user interface design. Nielsen Norman Group. 2020. [2023-01-20]. https://www.nngroup.com/articles/ten-usability-heuristics/
- 30.Divide or join: the frontend backend dilemma. Open Sense Labs. 2019. Sep 27, [2023-01-25]. https://opensenselabs.com/blog/articles/frontend-backend .
- 31.Yuliawan D, Widyandana D, Nur Hidayah R. Utilization of Nursing Education Progressive Web Application (NEPWA) media in an education and health promotion course using Gagne’s model of instructional design on nursing students: quantitative research and development study. JMIR Nurs. 2020;3(1):e19780. doi: 10.2196/19780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wu HC, Chang CJ, Lin CC, Tsai MC, Chang CC, Tseng MH. Developing screening services for colorectal cancer on Android smartphones. Telemed J E Health. 2014;20(8):687–695. doi: 10.1089/tmj.2013.0288. https://europepmc.org/abstract/MED/24848873 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wibowo A, Hartanto CA, Wirawan PW. Android skin cancer detection and classification based on MobileNet v2 model. Int J Adv Intell Inform. 2020;6(2):135–148. doi: 10.26555/ijain.v6i2.492. [DOI] [Google Scholar]
- 34.Temko A. Accurate heart rate monitoring during physical exercises using PPG. IEEE Trans Biomed Eng. 2017;64(9):2016–2024. doi: 10.1109/tbme.2017.2676243. [DOI] [PubMed] [Google Scholar]
- 35.Fortino G, Giampà V. PPG-based methods for non invasive and continuous blood pressure measurement: an overview and development issues in body sensor networks. IEEE International Workshop on Medical Measurement and Applications (MEMEA); 2010; Canada. 2010. [DOI] [Google Scholar]
- 36.What is medical IoT? Arm: Glossary medical IoT. [2023-01-20]. https://www.arm.com/glossary/medical-iot .
- 37.Patnaik Patnaikuni DR. A comparative study of Arduino, Raspberry Pi and ESP8266 as IoT development board. Int J Adv Res Comput Sci. 2017;8(5):2350–2352. [Google Scholar]
- 38.Onubeze A. Developing a wireless heart-rate monitor with MAX30100 and nRF51822. Helsinki Metropolia University of Applied Sciences. 2016. [2023-01-20]. https://core.ac.uk/download/pdf/80990741.pdf .
- 39.Wan J, Zou Y, Li Y, Wang J. Reflective type blood oxygen saturation detection system based on MAX30100. International Conference on Security, Pattern Analysis, and Cybernetics (SPAC); 2017; Shenzhen, China. IEEE; 2017. [Google Scholar]
- 40.Onasanya A, Elshakankiri M. Smart integrated IoT healthcare system for cancer care. Wireless Netw. 2019;27(6):4297–4312. doi: 10.1007/s11276-018-01932-1. [DOI] [Google Scholar]
- 41.Mayer DK, Landucci G, Awoyinka L, Atwood AK, Carmack CL, Demark-Wahnefried W, McTavish F, Gustafson DH. SurvivorCHESS to increase physical activity in colon cancer survivors: can we get them moving? J Cancer Surviv. 2018;12(1):82–94. doi: 10.1007/s11764-017-0647-7. https://europepmc.org/abstract/MED/28994035 .10.1007/s11764-017-0647-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Cheong IY, An SY, Cha WC, Rha MY, Kim ST, Chang DK, Hwang JH. Efficacy of mobile health care application and wearable device in improvement of physical performance in colorectal cancer patients undergoing chemotherapy. Clin Colorectal Cancer. 2018;17(2):e353–e362. doi: 10.1016/j.clcc.2018.02.002.S1533-0028(17)30545-5 [DOI] [PubMed] [Google Scholar]
- 43.Maxwell-Smith C, Cohen PA, Platell C, Tan P, Levitt M, Salama P, Makin GB, Tan J, Salfinger S, Kader Ali Mohan GR, Kane RT, Hince D, Jiménez-Castuera R, Hardcastle SJ. Wearable activity technology and action-planning (WATAAP) to promote physical activity in cancer survivors: randomised controlled trial protocol. Int J Clin Health Psychol. 2018;18(2):124–132. doi: 10.1016/j.ijchp.2018.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Eustache J. A mobile phone app improves patient-physician communication and reduces emergency department visits after colorectal surgery. Dis Colon Rectum. 2021;66(1):130–137. doi: 10.1097/dcr.0000000000002187. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The system architecture and hardware.
Data Availability Statement
The data sets generated and analyzed during this study are available from the corresponding author upon reasonable request.