

Abstract
In the United States, concentrations of criteria air pollutants have declined in recent decades. Questions remain regarding whether improvements in air quality are equitably distributed across subpopulations. We assessed spatial variability and temporal trends in concentrations of particulate matter with an aerodynamic diameter ≤2.5 μm (PM2.5) and ozone (O3) across North Carolina from 2002–2016, and associations with community characteristics. Estimated daily PM2.5 and O3 concentrations at 2010 Census tracts were obtained from the Fused Air Quality Surface Using Downscaling archive and averaged to create tract-level annual PM2.5 and O3 estimates. We calculated tract-level measures of: racial isolation of non-Hispanic Black individuals, educational isolation of non–college educated individuals, the neighborhood deprivation index (NDI), and percentage of the population in urban areas. We fitted hierarchical Bayesian space-time models to estimate baseline concentrations of and time trends in PM2.5 and O3 for each tract, accounting for spatial between-tract correlation. Concentrations of PM2.5 and O3 declined by 6.4 μg/m3 and 13.5 ppb, respectively. Tracts with lower educational isolation and higher urbanicity had higher PM2.5 and more pronounced declines in PM2.5. Racial isolation was associated with higher PM2.5 but not with the rate of decline in PM2.5. Despite declines in pollutant concentrations, over time, disparities in exposure increased for racially and educationally isolated communities.
Keywords: air pollution, disparities, environmental justice, ozone, PM2.5, segregation
Abbreviations
- CrI
credible interval
- EI
educational isolation
- EPA
Environmental Protection Agency
- NHB
non-Hispanic Black
- NDI
Neighborhood Deprivation Index
- O3
ozone
- PM2.5
particulate matter with an aerodynamic diameter ≤2.5 μm
- RI
racial isolation
- SES
socioeconomic status
- WAIC
Watanabe-Akaike information criterion
An extensive literature has demonstrated that exposure to ambient air pollution is harmful to health (1). Exposures to ozone (O3) and particulate matter with an aerodynamic diameter ≤2.5 μm (PM2.5) are linked with adverse health outcomes, including mortality (2–4), cardiovascular (5, 6) and respiratory disease (7, 8), hospital admissions (9, 10), and adverse pregnancy outcomes (11–13), among others. However, exposure to air pollutants and health impacts at a given level of exposure are not necessarily uniform across all communities and subpopulations.
In the United States, racial/ethnic minorities and low–socioeconomic status (SES) communities may be disproportionately exposed to specific air pollutants (14, 15). Studies have demonstrated that ambient PM2.5 concentrations tend to be higher in communities with higher proportions of non-Hispanic Black (NHB) or Hispanic residents, higher poverty levels, and greater degrees of racial segregation and urbanicity (16–18); these community characteristics are also linked with health outcomes (19–21). A 2019 study showed a decline in PM2.5 exposure in the United States between 2005 and 2015 but found that pollution inequity, or the difference between the environmental health damage caused by a racial/ethnic group and the damage that group experiences, remained high for NHB and Hispanic persons (22). In addition to differential exposures, some populations may be more susceptible to health effects associated with air pollution. A recent study observed a more pronounced mortality risk associated with PM2.5 exposure among racial/ethnic minorities and low-income individuals (23).
Overall concentrations of criteria air pollutants in the United States have declined in recent decades. The US Environmental Protection Agency (EPA) estimated that daily 8-hour maximum O3 concentrations declined by 22% between 1990 and 2017, while 24-hour average PM2.5 concentrations declined by 40% between 2000 and 2017 (24). Despite these improvements, 120 million Americans resided in areas with PM2.5 or O3 concentrations above the level specified by the National Ambient Air Quality Standards (NAAQS) in 2021 (25, 26). Furthermore, while the increased health risks at concentrations in excess of the NAAQS are well-established (25), there is a growing body of evidence that air pollution is detrimental to health even at lower concentrations (23, 27). Associations between PM2.5 and O3 exposure and health outcomes, specifically all-cause, cardiovascular-, and respiratory-related hospitalizations (27) and mortality (23), persist at concentrations below the NAAQS.
Despite national/overall improvements in air quality, it is unclear how consistently the air quality is improving across communities/populations, where the greatest improvements are, and thus who benefits. It is also unclear whether the magnitude/pace of the decline is similar across communities, or whether some populations are experiencing a slower decline in pollution and, therefore, an attenuated risk reduction. Disparities in air pollution exposure may in fact widen if air quality is improving more rapidly in areas that already have lower levels. These issues raise questions of environmental (in)justice, which is a complex concept with multiple definitions involving exposures, outcomes, and processes related to the experience of different subpopulations (28).
To address these questions, we first described levels and temporal trends in PM2.5 and O3 concentrations across North Carolina over 15 years (2002–2016). We then evaluated whether baseline levels and temporal trends in PM2.5 and O3 concentrations related to community-level characteristics, including measures of racial isolation (RI), educational isolation (EI), neighborhood deprivation, and urbanicity. Measures of RI, EI, neighborhood deprivation, and urbanicity were selected because previous work has demonstrated associations between: 1) urbanicity, SES, and air pollutants, specifically O3 and PM2.5 (29, 30); and 2) RI and PM2.5, even after controlling for urbanicity (16). As a recently developed measure, less is known about relationships between EI, air pollution, and health, but educational attainment is often used as a proxy for SES that is also associated with health outcomes (30–32). Overall—across all metrics—we hypothesized that communities with higher air pollutant concentrations (of either air pollutant) were more likely to have larger declines in pollutant concentrations, because such communities have more “room for improvement.”
METHODS
Data
Air pollution data.
Estimated concentrations of PM2.5 and O3 in North Carolina were obtained for 2002–2016 from the publicly available EPA Fused Air Quality Surface Using Downscaling (“downscaler”) data. The downscaler utilizes a hierarchical Bayesian space-time modeling framework that combines gridded output from the Community Multiscale Air Quality model with monitoring data from the National Air Monitoring Station and State and Local Air Monitoring Station networks to produce daily point-level concentration estimates at the 2010 Census-tract centroids across the United States (33–35). Archived daily downscaler surfaces are available from the US EPA. Detailed descriptions of the downscaler modeling technique and performance are provided elsewhere (34). Downscaler output includes estimates of 24-hour average PM2.5 and 8-hour maximum O3 concentrations at census-tract centroids for each day in the study period (2002–2016). We averaged daily values to generate an annual average PM2.5 and 6-month (April–September) average O3 concentration estimates for each tract. Six-month averages of O3 were calculated for April–September because this warm season is when O3 concentrations tend to be highest, and when the most O3 monitors are typically operational.
Racial isolation of non-Hispanic Black individuals.
Massey and Denton (36) identified 5 dimensions of racial residential segregation, namely, evenness/dissimilarity, exposure/isolation, concentration, centralization, and clustering. Later, it was determined that clustering, centralization, and concentration were also measures of evenness, thus simplifying the conceptual framework to evenness and exposure/isolation (37, 38). Additionally, a review of segregation and health noted that studies had conceptualized segregation in one of 2 ways (39): 1) a formal measure of geographical segregation of racial groups with indices reflecting either exposure/isolation, evenness, concentration, centralization, or clustering (36); and 2) a proxy measure (e.g., Black racial composition, % NHB). Prior assessments of segregation and health have found it conceptually problematic to conflate formal vs. proxy measures. Thus, we chose to employ a formal measure of RI because of the importance of isolation as one of the 5 domains of racial residential segregation long defined in the literature, and the domain that may be most closely related to adverse and disparate outcomes for racially, economically, and educationally minoritized populations (19, 40).
Using 2010 US Census data on the percentage of tract population self-identifying as NHB, we use a local spatial measure of RI to quantify geographic separation of NHB from other racial groups (41). The RI index is calculated based on the racial composition (e.g., % NHB) of tracts neighboring a given index tract i. We defined “neighbor” by adjacency, such that neighbors are tracts sharing a border or vertex with index tract i. The RI index ranges from 0 to 1 and represents a weighted average proportion of NHB in the local environment. For example, individuals in a neighborhood environment (i.e., index tract and neighboring tracts) that is predominantly non-NHB will have an RI value close to 0. In contrast, individuals living in a neighborhood environment that is nearly all NHB will have an RI value that is close to 1. The RI index was computed for all tracts within the study area with non-zero population in the neighborhood environment of the index tract. Based on previous work (16), we hypothesized that higher RI communities may have higher PM2.5 concentrations but not necessarily higher O3 concentrations.
Educational isolation of non–college educated individuals.
Using 2010 US Census data on the percentage of tract population aged 25 years or older with a college degree, we use a local, spatial measure of EI to quantify the geographic separation of non–college educated individuals from college educated individuals. This index is calculated in the same way as RI, and results in a weighted average proportion of non–college educated individuals in the local environment. The EI index ranges from 0 to 1: Individuals living in a neighborhood environment that is predominantly of college educated individuals will have an EI value close to 0. In contrast, individuals living in a neighborhood environment that is nearly all non–college educated individuals will have an EI value that is close to 1. EI was computed for all tracts within the study area with non-zero population in the neighborhood environment of the index tract. We hypothesized that higher EI communities may have lower PM2.5 and O3 concentrations, in part because EI may be higher in areas with less industry and lower population density (the correlation between EI and urbanicity is −0.46), in addition to census tracts in central parts of urban areas (32). The correlation between EI and RI in the United States is around 0.21 (32), and in North Carolina, it is 0.23.
The construction of the spatial measures of neighborhood-level RI (41) and EI (32) are described in detail elsewhere and summarized in Web Appendixes 1 and 2 (available at https://doi.org/10.1093/aje/kwac059), respectively.
Neighborhood deprivation.
Tract-level data from the 2010 Census were utilized to calculate a previously developed Neighborhood Deprivation Index (NDI) (42). The NDI was calculated using the first factor loadings from a principal components analysis of the following census variables: percentage of households in poverty, percentage of female-headed households with dependents, percentage with annual household income below $30,000, percentage of households on public assistance, percentage of male persons in management/professional occupation, percentage living in crowded housing, percentage unemployed, and percentage without a high-school education. Larger NDI values indicate more severe deprivation. NDI is typically used in urban settings; it is unclear how relevant it is for statewide analyses like those presented here. Nevertheless, because a measure of socioeconomic status is used so commonly in disparities analyses, we included NDI in our analysis.
Urbanicity.
Urbanicity was estimated based on the tract-level percentage of the population residing in urban settings that is available as a continuous variable (range: 0%–100%) in the 2010 Census data. An urban area comprises a densely settled core of census tracts and/or census blocks that meet minimum population density requirements, along with adjacent territory containing nonresidential urban land uses as well as territory with low population density included to link outlying densely settled territory with the densely settled core. Specifically, to qualify as urban, the territory identified must encompass at least 2,500 people, at least 1,500 of whom reside outside institutional group quarters. “Rural” encompasses all population, housing, and territory not included within an urban area (43).
Statistical analysis
To evaluate whether and how air pollution concentrations were changing over the study period, we plotted tract-level annual average PM2.5 and annual 6-month (April–September) average O3 concentrations over time and mapped PM2.5 and O3 concentrations at the beginning (2002), midpoint (2009), and end (2016) of the study period. We refer to 2002 levels as “baseline” conditions for the purposes of this study.
To estimate overall (i.e., statewide) and tract-specific baseline air pollutant concentrations as well as statewide and tract-specific temporal trends in air pollutant concentrations, we fitted a model that estimates separate but spatially correlated linear time trends for each census tract. This model is a modification of that proposed by Bernardinelli et al. (44) and takes the form:
 |
(1) |
where  is the annual average PM2.5 (or O3) concentration in census tract i in year t;
is the annual average PM2.5 (or O3) concentration in census tract i in year t;  represents the statewide intercept;
represents the statewide intercept;  is a census tract–level random effect that allows for differences in baseline concentrations;
is a census tract–level random effect that allows for differences in baseline concentrations;  represents the statewide temporal trend in air pollution over the study period;
represents the statewide temporal trend in air pollution over the study period;  is a tract-level random effect that represents the tract-specific differential temporal trend; and
is a tract-level random effect that represents the tract-specific differential temporal trend; and  . Thus, each census tract i has its own linear time trend, with a spatially varying intercept,
. Thus, each census tract i has its own linear time trend, with a spatially varying intercept,  , and a spatially varying slope,
, and a spatially varying slope,  .
.
Each set of random effects  and
and  are modeled using independent conditional autoregressive prior distributions proposed by Leroux et al. (45), allowing for the possibility of spatial correlation between these spatially-varying parameters. Specifically, one of these random effect parameters is assumed a priori to be normally distributed, conditional on the parameters from all other tracts, and centered at the weighted average of neighboring values such that
are modeled using independent conditional autoregressive prior distributions proposed by Leroux et al. (45), allowing for the possibility of spatial correlation between these spatially-varying parameters. Specifically, one of these random effect parameters is assumed a priori to be normally distributed, conditional on the parameters from all other tracts, and centered at the weighted average of neighboring values such that
 |
where  (i.e., a vector of random effects with the ith entry removed), and
(i.e., a vector of random effects with the ith entry removed), and  is equal to
is equal to  if tracts i and j are neighbors (i.e., share a border or vertex) and 0 otherwise. The
if tracts i and j are neighbors (i.e., share a border or vertex) and 0 otherwise. The  parameters are defined in a similar way, using
parameters are defined in a similar way, using  and
and  , and thus not shown. This flexible specification allows for several spatial patterns during modeling. For example, a small random effect variance,
, and thus not shown. This flexible specification allows for several spatial patterns during modeling. For example, a small random effect variance,  , indicates that there is less variability in that set of parameters with many values near zero, and that a single statewide intercept or slope may adequately describe variability in the air pollution concentrations. In the case of a larger
, indicates that there is less variability in that set of parameters with many values near zero, and that a single statewide intercept or slope may adequately describe variability in the air pollution concentrations. In the case of a larger  value,
value,  , the spatial dependence parameter, indicates whether the variability is closer to independence (
, the spatial dependence parameter, indicates whether the variability is closer to independence ( near zero) or spatially correlated (
near zero) or spatially correlated ( near 1). To ensure that we do not influence these choices before seeing the data, we specify weakly informative prior distributions for the model parameters to allow the data to drive the inference rather than our prior beliefs. Specifically:
near 1). To ensure that we do not influence these choices before seeing the data, we specify weakly informative prior distributions for the model parameters to allow the data to drive the inference rather than our prior beliefs. Specifically:
 |
 |
 |
To explore whether and how air pollution levels and temporal trends in pollutant concentrations are related to tract-level characteristics, we extended equation 1 to include a vector of variables for urbanicity, RI of NHB, EI of non–college educated individuals, and NDI that are specific to census tract i ( ) such that
) such that
 |
(2) |
Equation 2 allows us to evaluate how baseline levels of air pollution relate to tract-level RI, EI, NDI, and urbanicity, and whether the variability in the intercepts can be explained by these tract-level covariates. The term for interaction between these covariates and time allows us to assess whether and how tract-level characteristics relate to temporal trends in air pollution, and whether the variability in the slopes can be explained by these covariates. To evaluate whether the covariates included in equation 2 have explained any variability, we can compare the  and
and  from equations 1 and 2 and more formally compare the model fits using the Watanabe-Akaike information criterion (WAIC). Smaller WAIC values indicate an improved balance of model fit and complexity among a group of competing models fit to the same data set (46). The same prior distributions from the previous model were used in this analysis, with the newly added regression parameters specified as
from equations 1 and 2 and more formally compare the model fits using the Watanabe-Akaike information criterion (WAIC). Smaller WAIC values indicate an improved balance of model fit and complexity among a group of competing models fit to the same data set (46). The same prior distributions from the previous model were used in this analysis, with the newly added regression parameters specified as 
Models were fitted separately for PM2.5 and O3. For each pollutant, we fitted models with random slopes and random intercepts as well as models with random intercepts only. The WAIC was used to select the most appropriate model specification (i.e., with or without random slopes) (46). For each model, 50,000 posterior samples were collected from the joint posterior distribution after a burn-in period of 10,000 iterations using the car.linear function in CARBayesST (47) or the S.CARmultilevel function in CARBayes (48) for models with and without random slopes, respectively. We thinned the collected samples by a factor of 5 in order to reduce posterior autocorrelation, resulting in 10,000 posterior samples for inference. Visual inspection of individual parameter trace plots and calculation of the Geweke diagnostic (49) suggested no obvious signs of nonconvergence of the models. Statistical analyses were performed using R, version 3.5 (50).
RESULTS
Descriptive statistics
There were 2,163 census tracts in the study area. Average concentrations of PM2.5 and O3 in 2002, the start of the study period, were 13.5 μg/m3 and 56.6 ppb, respectively. To visualize how air pollution concentrations changed in North Carolina over the 15-year study period, we plotted tract-level annual average PM2.5 (Figure 1A) and 6-month average O3 concentrations (Figure 1B). Both PM2.5 and O3 levels decreased between 2002 and 2016, although the decline was not monotonic for either pollutant. For both PM2.5 and O3, there were no tracts in which concentrations increased between the beginning and end of the study period. Within-tract declines in concentrations, measured as percent change between the beginning and end of the study period, ranged from 20.8% to 45.1% for PM2.5 and 19.4% to 32.7% for O3.
Figure 1.
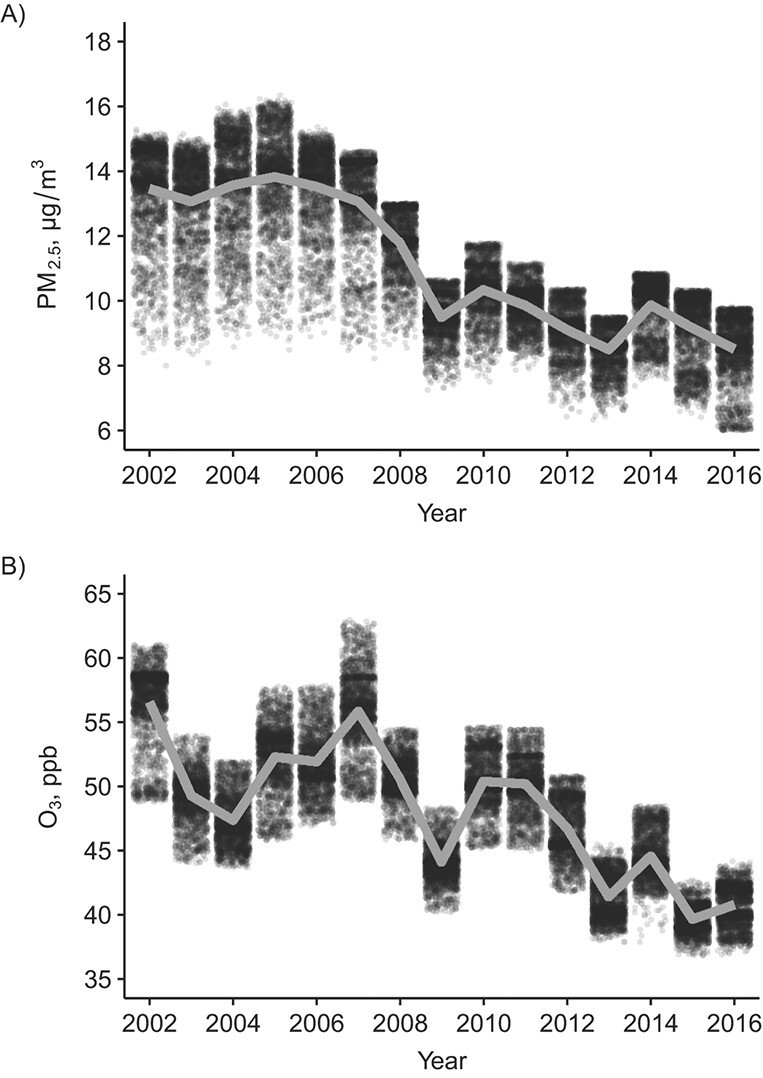
Downscaler-estimated air pollution concentrations, North Carolina, 2002–2016. A) Tract-specific annual average concentrations of particulate matter with an aerodynamic diameter ≤2.5 μm (PM2.5), μg/m3; B) tract-specific annual average concentrations of ozone (O3), ppb.
We also mapped tract-level PM2.5 and O3 concentrations at the beginning, midpoint, and end of the study period (Web Figures 1–2, respectively), as well as community-level covariates, namely RI, EI, NDI, and urbanicity (Web Figures 3–6, respectively). Descriptive statistics of community-level covariates (e.g., mean, standard deviation, range) are provided in Web Table 1. Correlations between each community-level characteristic ranged from −0.46 (urbanicity and EI) to 0.58 (EI and NDI) (Web Table 2).
Model selection
For both PM2.5 and O3, we fitted models (null and with adjustments) with random slopes and random intercepts as well as models with random intercepts only (WAIC values are provided in Web Table 3). Based on the WAIC results, we present adjusted PM2.5 models with random intercepts and slopes, and adjusted O3 models with random intercepts only. Variance inflation factors (VIFs) in the adjusted models, which included all 4 community characteristics (RI, EI, NDI, and urbanicity), ranged from a minimum of 1.45 (RI) to a maximum of 2.10 (EI) in the PM2.5 and O3 models. VIFs in excess of 5 are generally a cause for concern (51, 52), and some researchers have argued for use of a more conservative threshold of 2.5 (53).
Statistical analysis
Particulate matter with an aerodynamic diameter ≤2.5 μm.
We estimated tract-level baseline PM2.5 concentrations and temporal trends in PM2.5 concentrations after adjustment for RI, EI, NDI, and urbanicity and including a term for interaction between these characteristics and year, as described in equation 2. The tract-specific intercepts ( ) from the adjusted model are shown in Figure 2A (these values also represent the fitted concentrations from 2009, the midpoint of the study period). The fitted, statewide average PM2.5 concentration was 11.2 μg/m3 in 2009, and the statewide slope (α) was −6.37 μg/m3. The highest PM2.5 concentrations (yellow) were observed in central and south-central North Carolina, particularly in and extending outward from Charlotte (Mecklenburg County), North Carolina. Lower PM2.5 concentrations (dark blue) were observed in tracts in far western and eastern parts of the state, representing the Appalachian Mountains and Coastal Plain region, respectively.
) from the adjusted model are shown in Figure 2A (these values also represent the fitted concentrations from 2009, the midpoint of the study period). The fitted, statewide average PM2.5 concentration was 11.2 μg/m3 in 2009, and the statewide slope (α) was −6.37 μg/m3. The highest PM2.5 concentrations (yellow) were observed in central and south-central North Carolina, particularly in and extending outward from Charlotte (Mecklenburg County), North Carolina. Lower PM2.5 concentrations (dark blue) were observed in tracts in far western and eastern parts of the state, representing the Appalachian Mountains and Coastal Plain region, respectively.
Figure 2.
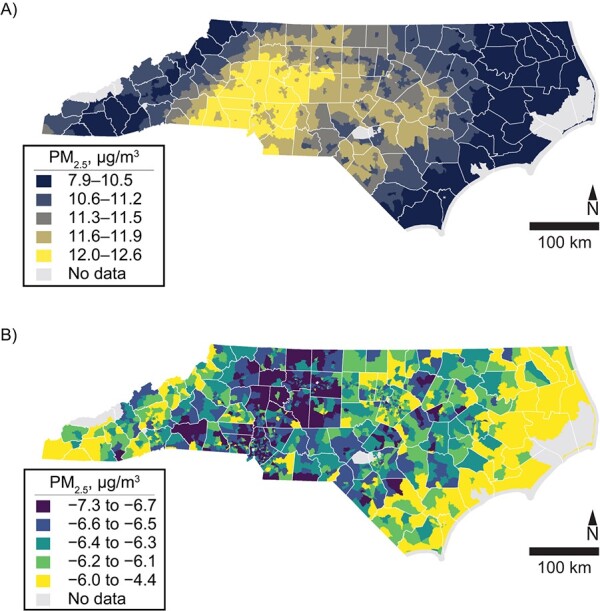
Particulate matter with an aerodynamic diameter ≤2.5 μm (PM2.5) concentrations, North Carolina, 2002–2016. A) Tract-specific variations in average PM2.5 concentration; B) tract-specific variations in change in PM2.5 concentration.
Modeled temporal trends in PM2.5, specifically the tract-specific slopes ( ) in the adjusted model, are shown in Figure 2B. Tracts with smaller-than-average declines in PM2.5 concentrations are shown in yellow, while tracts with larger-than-average declines in PM2.5 are shown in in dark blue. Tracts with larger declines in PM2.5 tend to be concentrated in central North Carolina, particularly western-central North Carolina. This coincides to some extent, but not completely, with the areas that had the highest baseline levels of PM2.5.
) in the adjusted model, are shown in Figure 2B. Tracts with smaller-than-average declines in PM2.5 concentrations are shown in yellow, while tracts with larger-than-average declines in PM2.5 are shown in in dark blue. Tracts with larger declines in PM2.5 tend to be concentrated in central North Carolina, particularly western-central North Carolina. This coincides to some extent, but not completely, with the areas that had the highest baseline levels of PM2.5.
Associations between the tract-level variables and PM2.5 concentrations (baseline levels and change over time) are reported in Table 1. A 1-standard-deviation increase in RI (0.17) was associated with a 0.11 μg/m3 (95% credible interval (CrI): 0.06, 0.15) increase in PM2.5 at baseline. A 1-standard-deviation increase in the percent of population in urban settings (30.1%) was associated with a 0.21 μg/m3 (95% CrI: 0.17, 0.26) increase in PM2.5 concentration at baseline. In contrast, 1-standard-deviation increase in EI (0.15) was associated with a 0.10 μg/m3 (95% CrI: 0.04, 0.15) decrease in PM2.5 concentration at baseline. This combination of results is sensible in that RI tends to be highest in urban areas, and EI tends to be higher in rural areas (e.g., Web Figures 3 and 4).
Table 1.
Associations Between Tract-Level Social and Demographic Variables and Baseline Levels and Time Trends in PM2.5 Concentrations, North Carolina, 2002–2016a
| Variable b | Main Effect | Interaction With Time | ||
|---|---|---|---|---|
| Posterior Median | 95% CrI | Posterior Median | 95% CrI | |
| RI of non-Hispanic Black individuals | 0.11 | 0.061, 0.15 | −0.015 | −0.064, 0.034 |
| EI of non–college educated individuals | −0.10c | −0.15, −0.044 | −0.067c | −0.13, −0.0085 |
| Percentage of population in urban settings | 0.21c | 0.17, 0.26 | −0.12c | −0.17, −0.074 |
| NDI | −0.011 | −0.039, 0.017 | −0.0031 | −0.029, 0.024 |
Abbreviations: CrI, credible interval; EI, educational isolation; NDI, Neighborhood Deprivation Index; PM2.5, particulate matter with an aerodynamic diameter of ≤2.5 μm; RI, racial isolation.
a Models adjusted for all community-level characteristics (i.e., RI, EI, urbanicity, and NDI); separate models were not fitted for each community-level characteristic. Values are shown to 2 significant digits.
b Correlations between demographic variables ranged from −0.46 (between EI and urbanicity) to 0.58 (between EI and NDI); ranges of variable values and correlations between all variables are provided in Web Tables 1–2.
c Coefficients for which the 95% CrI does not include zero.
Terms for interaction with year were statistically significant and negative for both urbanicity and EI, although the significance on EI was marginal. Interaction terms can be interpreted as location-specific slopes. For example, communities (census tracts) with higher urbanicity values have smaller (more negative) slopes than communities with lower urbanicity values. That is, the decline in PM2.5 over time is steeper in more-urban areas than in less-urban areas. Similarly, communities with higher EI values have more-negative slopes than communities with lower EI values, such that the decline in PM2.5 over time is steeper in more educationally isolated communities than in less educationally isolated communities.
For example, an “average” tract would have a baseline PM2.5 concentration of 13.5 μg/m3 and a change in PM2.5 over the study period of −6.4 μg/m3. A tract that is 2 standard deviations above the average in terms of urbanicity, holding other variables constant, would have a baseline PM2.5 concentration of 13.9 μg/m3 and a change in PM2.5 over the study period of −6.7 μg/m3. That is, for a tract with higher urbanicity, the baseline PM2.5 concentration is higher, but the decline in PM2.5 is also steeper. In contrast, a tract that is 2 standard deviations above the average in terms of RI, holding other variables constant, would have a baseline PM2.5 concentration of 13.7 μg/m3 (higher than average) and a change in PM2.5 over the study period of −6.4 μg/m3 (same as the average).
These findings indicate that there are existing disparities in PM2.5 exposure with respect to RI, EI, and urbanicity, with more-urban and higher-RI tracts having higher baseline PM2.5 exposures, and higher-EI tracts having lower baseline PM2.5 exposures. Time trends in PM2.5 concentrations differed by urbanicity and EI only. In contrast to more-urban communities, which have high PM2.5 levels that are improving more markedly over time, high-RI communities have high PM2.5 levels that do not show such an improvement.
Posterior median estimates of  , reported in Web Table 4, declined from the null model (1.93) to the adjusted model (1.58), suggesting that some of the variability in baseline PM2.5 values is explained by the covariates in the adjusting model. The posterior median estimate of
, reported in Web Table 4, declined from the null model (1.93) to the adjusted model (1.58), suggesting that some of the variability in baseline PM2.5 values is explained by the covariates in the adjusting model. The posterior median estimate of  also declined between the null (0.72) and adjusting (0.69) model.
also declined between the null (0.72) and adjusting (0.69) model.
Ozone.
As with PM2.5, we estimated baseline O3 concentrations and temporal trends in O3 concentrations after adjustment for RI, EI, NDI, and urbanicity, and including a term for interaction between these characteristics and year (as described by equation 2). The tract-specific intercepts ( ) from the adjusted model are shown in Figure 3 (these values also represent the fitted concentrations from 2009, the midpoint of the study period). Tract-specific slopes are not presented in Figure 3 because, for O3, the model selected based on WAIC included only random intercepts; however, a map of tract-specific slopes from the O3 model with random slopes and intercepts is provided in the Web Figure 7. The statewide average O3 concentration was 48.1 ppb in 2009, and the statewide slope (α) was −13.5 ppb (over the entire study period). Similar to PM2.5, the highest O3 concentrations were observed in south-central North Carolina, in and extending outward from Charlotte (Mecklenburg County), North Carolina. The lowest O3 concentrations were observed in the coastal plains, particularly the southeastern part of the state.
) from the adjusted model are shown in Figure 3 (these values also represent the fitted concentrations from 2009, the midpoint of the study period). Tract-specific slopes are not presented in Figure 3 because, for O3, the model selected based on WAIC included only random intercepts; however, a map of tract-specific slopes from the O3 model with random slopes and intercepts is provided in the Web Figure 7. The statewide average O3 concentration was 48.1 ppb in 2009, and the statewide slope (α) was −13.5 ppb (over the entire study period). Similar to PM2.5, the highest O3 concentrations were observed in south-central North Carolina, in and extending outward from Charlotte (Mecklenburg County), North Carolina. The lowest O3 concentrations were observed in the coastal plains, particularly the southeastern part of the state.
Figure 3.
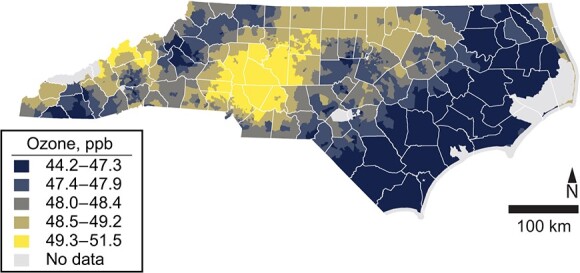
Tract-specific variations in average ozone (O3) concentrations, North Carolina, 2002–2016.
Associations between the tract-level variables and O3 concentrations (baseline levels and change over time) are reported in Table 2. Urbanicity and NDI were associated with baseline O3 concentrations. A 1-standard-deviation increase (30.1%) in the percent of population in urban settings was associated with a 0.38 ppb (95% CrI: 0.30, 0.47) increase in O3 concentration. A 1-standard-deviation increase in NDI (2.1) was associated with a 0.061 ppb (95% CrI: 0.11, 0.017) decrease in O3 concentration.
Table 2.
Associations Between Tract-Level Social and Demographic Variables and Baseline Levels and Time Trends in Ozone Concentrations, North Carolina, 2002–2016a
| Variable b | Main Effect | Interaction With Time | ||
|---|---|---|---|---|
| Posterior Median | 95% CrI | Posterior Median | 95% CrI | |
| RI of non-Hispanic Black individuals | −0.065 | −0.15, 0.019 | −0.63c | −0.78, −0.47 |
| EI of non–college educated individuals | 0.023 | −0.077, 0.12 | 0.54c | 0.35, 0.73 |
| Percentage of population in urban settings | 0.38c | 0.30, 0.47 | 0.084 | −0.079, 0.25 |
| NDI | −0.061c | −0.11, −0.017 | 0.078 | −0.0080, 0.17 |
Abbreviations: CrI, credible interval; EI, educational isolation; NDI, Neighborhood Deprivation Index; RI, racial isolation.
a Models adjusted for all community-level characteristics (i.e., RI, EI, urbanicity, and NDI); separate models were not fitted for each community-level characteristic. Values are shown to 2 significant digits.
b Correlations between demographic variables ranged from −0.46 (between EI and urbanicity) to 0.58 (between EI and NDI); ranges of variable values and correlations between all variables are provided in Web Tables 1–2.
c Coefficients for which the 95% CrI does not include zero.
Additionally, terms for interaction with year were statistically significant for RI and EI but had differing signs, indicating that the change in O3 concentration over time is modified by the degree of RI and EI. Specifically, communities (census tracts) with higher RI have smaller (more negative) slopes than locations with lower RI. This indicates that the decline in O3 over time is steeper in more racially isolated communities than in less racially isolated communities. In contrast, communities with higher EI values have larger (less negative) slopes than communities with lower EI values, such that the decline in O3 over time is shallower in more educationally isolated communities than in less educationally isolated communities.
As an example, for O3, an “average” tract would have a baseline O3 concentration of 56.6 ppb and a change in O3 over the study period of −13.5 ppb. A tract that is 2 standard deviations above the average in terms of urbanicity, holding other variables constant, would have a baseline O3 concentration of 57.4 ppb but the same change in O3 over the study period (−13.5 ppb). A tract that is 2 standard deviations above the average in terms of EI, holding other variables constant, would have a baseline O3 concentration of 56.6 ppb (same as the average) and a change in O3 over the study period of −12.4 ppb (below-average improvement). These exposure differences and changes in exposure differences over time may seem small, but they apply to a large number of people, and differences in the rates of change over time suggest that there is potential for disparities to worsen, or develop.
These findings suggest that there are existing disparities in O3 exposure with respect to urbanicity and NDI, with more-urban and lower-NDI tracts having higher baseline O3 exposures. In contrast, O3 concentrations at baseline did not differ by RI or EI, but trends over time did. Specifically, declines in O3 concentrations over time were steeper in high-RI tracts compared with low-RI tracts, and shallower in high-EI tracts compared with low-EI tracts. Should these trends of differential rates of decline in O3 concentration by community-level EI and RI continue (or accelerate), disparities in O3 exposure by EI and RI may emerge.
Posterior median estimates of  declined from the null model (5.99) to the adjusted model (5.37) (Web Table 4), indicating that some variability in baseline O3 concentrations was explained by the covariates.
declined from the null model (5.99) to the adjusted model (5.37) (Web Table 4), indicating that some variability in baseline O3 concentrations was explained by the covariates.
DISCUSSION
Although average levels of PM2.5 and O3 have declined over the past 2 decades in the United States (24), it is unclear where improvements in air quality are concentrated and what populations are benefiting most from improvements. Moreover, an overall improvement in air quality could, in fact, mask widening disparities based on geographic, social, or demographic factors. Here, we describe baseline levels and temporal trends in PM2.5 and O3 concentrations in the state of North Carolina during 2002–2016. We evaluated whether baseline concentrations and temporal trends related to tract-level community characteristics, including measures of racial and educational isolation, deprivation, and urbanicity.
Areas with higher baseline PM2.5 concentrations have more “room for improvement” compared with areas that had lower baseline PM2.5 concentrations, making it intuitive for higher-exposure areas to have more marked declines (improvement) in PM2.5 compared with lower-exposure areas. In fact, we observed this with urban tracts, which had both higher baseline PM2.5 values and more pronounced declines in PM2.5 over time. That is, over the study period, disparities in PM2.5 exposure were reduced in more-urban compared with less-urban areas. In contrast, a different relationship was observed for RI. More racially isolated tracts also had higher than average baseline PM2.5 concentrations, but unlike urban tracts, high-RI tracts did not exhibit more marked declines in PM2.5 over time. This finding suggests a disparity in who benefits from declines in PM2.5 concentrations and associated improvements in air quality. In fact, it suggests that areas with higher RI may actually experience an increase in PM2.5 exposure disparity over time, despite an overall decline in PM2.5 levels. Some tracts, such as more educationally isolated tracts, had lower baseline PM2.5 values, but also more pronounced declines in PM2.5 over the study period, compared with less educationally isolated tracts. Thus, areas with low EI may also experience an increase in PM2.5 exposure disparity over time (compared with areas with high EI).
Different patterns were observed for O3 compared with PM2.5. We did not observe that “high exposure” areas had more pronounced declines (improvement) in O3 concentrations compared with “low exposure” areas. Specifically, more-urban and less-deprived areas had higher baseline O3 levels but declines in O3 were similar across urbanicity and deprivation values. RI and EI were not associated with baseline O3 concentrations but did exhibit interactions with time. Specifically, high-RI tracts exhibited steeper declines in O3 concentrations over the study period, while high-EI tracts had shallower declines in O3 levels. That is, there was more improvement in O3 concentrations in high-RI tracts compared with low-RI tracts over the study period, and less improvement in O3 concentrations in high-EI tracts compared with low-EI tracts. This suggests that, over time, disparities in O3 exposure may be widening for high-EI vs. low-EI areas, despite an overall time trend of improving O3 concentrations.
We observed differences in patterning of PM2.5 and O3 exposure according to sociodemographic characteristics, which is interesting but not necessarily unexpected. Previous work has also observed differences in PM2.5 and O3 exposure patterns by racial isolation and urbanicity (16) but did not consider how exposures are changing over time. The differences in spatial and/or sociodemographic patterning of these pollutants may relate to the sources of these pollutants and/or their behavior and formation in the atmosphere. PM2.5 is a primary pollutant that is often emitted as a by-product of combustion (e.g., in automobile engines, industrial processes), while O3, a secondary pollutant, is formed in light-catalyzed reactions between precursor pollutants, namely nitrogen oxides and volatile organic compounds (54). Ozone concentrations are typically higher where there is a mixture of precursor pollutants in the atmosphere, which may have anthropogenic or biogenic sources (e.g., vegetation such as trees), some of which may be more common in suburban or rural locations as compared with urban areas (55). Moreover, there are documented patterns of siting hazardous waste sites, polluting industrial facilities, and other undesirable activities or contaminated land-use types disproportionately in communities with lower SES and a higher proportion of racial/ethnic minorities (56). Thus, type and density of emission sources of PM2.5 and O3 precursors, and resulting ambient concentrations, may differ depending on community-level characteristics such as RI, EI, NDI, and urbanicity, among others.
This study has several limitations. The models used here assume a linear trend in air pollution concentrations over time. This is an oversimplification of the temporal trend in pollutant concentrations, but there is a clear decline in concentration of both pollutants between the beginning and end of the study period (e.g., Figure 1). Air pollutant concentrations were obtained from the Fused Air Quality Surface Using Downscaling (“downscaler”) data archive and represent predictions from a statistical model as opposed to observed (monitored) concentrations. These predictions enabled us to conduct this study because: 1) air pollution concentrations were available across the study area, creating a continuous spatial surface for fitting spatial models; and 2) estimates of ambient air pollution concentrations were available across census tracts with differing levels of the sociodemographic covariates of interest. This second point is particularly salient since air pollutant monitors are more often located in urban areas (57). Some evidence also suggests that racial/ethnic minorities may reside closer to pollution sources and farther from monitoring locations (58). Thus, there may be greater uncertainty in downscaler-derived ambient concentration estimates for specific types of communities (e.g., less urban). In forthcoming research, we examine whether uncertainty characterizing the downscaler-estimated concentrations differed by community characteristics such as SES, urbanicity, and RI, among others. Briefly, we observe some disparities in uncertainty of downscaler-derived PM2.5 and O3 that relate to community characteristics such as SES and RI.
We selected to adjust for RI, EI, NDI, and urbanicity because these characteristics may be relevant to health outcomes, and there is evidence that some of them are correlated with pollution levels as well. RI and urbanicity are associated with air pollution levels, specifically PM2.5 (16), as well as health outcomes (59). EI is a newly developed measure of isolation that may be associated with health and developmental outcomes (32). Associations between NDI and health have been observed, even after controlling for air pollution exposure (60). However, there are multiple approaches to assessing neighborhood conditions, including segregation and SES, and no one measure is perfect. Here, we chose to calculate EI comparing college educated with non–college educated groups because there are large and growing gaps in health outcomes between college and non–college educated individuals, and although there is considerable local variability, the majority of the US population has at least a high-school degree (61, 62). We chose to calculate RI with respect to NHB because of the existing literature that examines segregation of Black persons, elevated environmental exposures, and health outcomes (16, 63); a long, particular history of social, political, and economic forces conspiring to specifically segregate NHB from the majority White population (64); and, proportionally, NHB represent the largest racial/ethnic minority group in North Carolina (65). Potentially important avenues for future research include examining relationships between air pollution and: 1) EI calculated for those with vs. without a high-school degree (instead of college degree); 2) RI calculated for other racial/ethnic groups, such as Hispanic persons; and 3) alternative metrics or additional metrics of segregation, racial composition, and socioeconomic status.
Despite limitations, this study has important strengths. It is a statewide analysis of air pollution trends over a period of 15 years. The simulated air pollution data used to evaluate trends in PM2.5 and O3 concentrations over time provide excellent temporal and spatial coverage and have been used in previous studies of air pollution exposure and health (12, 66). This work provides information on, geographically, where PM2.5 and O3 levels are highest and lowest, and where PM2.5 and O3 levels are declining more vs. less rapidly. Moreover, this research identifies the sociodemographic populations in North Carolina with higher vs. lower ambient air pollution exposures, and identifies populations for which ambient air pollution exposures are declining more vs. less rapidly. North Carolina is home to Warren County, considered by many to be the birthplace of the US environmental justice movement in the 1980s (67, 68). It is located in the American South, which is unique among regions in the United States in that there are high-RI communities in both urban and rural areas; in much of the rest of the United States, NHB individuals reside predominantly in urban and suburban communities (32). Compared with the United States overall, North Carolina has a higher than average percentage of the population identifying as NHB (22.2% vs 13.4%) and also has a higher poverty rate (13.6% vs. 11.4%), although both of these variables exhibit considerable heterogeneity across the state (65). However, a key contribution of this work is the approach and framework it provides for examining whether disparities are widening or narrowing over time, and which types of communities have higher air pollution levels and/or more rapidly declining air pollution levels. Importantly, we show that despite overall PM2.5 declines across North Carolina during the study period, areas with high EI and urbanicity exhibited greater declines, while areas with high RI showed lesser declines. These findings suggest that communities are not all benefiting equally from air quality improvements, and that disparities in exposure may be widening for specific populations.
Supplementary Material
ACKNOWLEDGMENTS
Author affiliations: Global Health Institute, School of Medicine, Duke University, Durham, North Carolina, United States (Mercedes A. Bravo); Children’s Environmental Health Initiative, University of Notre Dame, South Bend, Indiana, United States (Mercedes A. Bravo, Man Chong Leong, Marie Lynn Miranda); Department of Biostatistics, School of Public Health, Yale University, New Haven, Connecticut, United States (Joshua L. Warren); Department of Biostatistics, University of Florida, Gainesville, Florida, United States (Man Chong Leong); Department of Environmental Health Sciences, School of Public Health, Yale University, New Haven, Connecticut, United States (Nicole C. Deziel); Department of Sociology, Rice University, Houston, Texas, United States (Rachel T. Kimbro); School of the Environment, Yale University, New Haven, Connecticut, United States (Michelle L. Bell); and Department of Applied and Computational Mathematics and Statistics, University of Notre Dame, South Bend, Indiana, United States (Marie Lynn Miranda).
This work was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health (award numbers R00MD011304 (PI: M.A.B.) and R01MD012769 (PI: M.L.B.)) and the National Institute of Environmental Health Sciences (award number R01ES028819 (PI: M.L.M.)). M.A.B.’s research is also supported by the Whitehead Scholars program at the Duke University School of Medicine.
Air pollution and Census data are publicly available. Indices are constructed from publicly available Census data and are available upon request from the corresponding author.
We gratefully acknowledge the work of Claire Osgood for data management expertise and Joshua Too for graphics preparation.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This publication was developed under Assistance Agreement no. RD835871 (PI: M.L.B.) awarded by the US Environmental Protection Agency to Yale University. It has not been formally reviewed by EPA. The views expressed in this document are solely those of M.L.B. and do not necessarily reflect those of the Agency. EPA does not endorse any products or commercial services mentioned in this publication.
Conflict of interest: none declared.
REFERENCES
- 1. World Health Organization . Review of Evidence on Health Aspects of Air Pollution. Geneva, Switzerland: WHO European Centre for Environment and Health; 2013. [Google Scholar]
- 2. Bell ML, McDermott A, Zeger SL, et al. Ozone and short-term mortality in 95 US urban communities, 1987-2000. JAMA. 2004;292(19):2372–2378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Crouse DL, Peters PA, Hystad P, et al. Ambient PM2.5, O3, and NO2 exposures and associations with mortality over 16 years of follow-up in the Canadian Census Health and Environment Cohort (CanCHEC). Environ Health Perspect. 2015;123(11):1180–1186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Krall JR, Anderson GB, Dominici F, et al. Short-term exposure to particulate matter constituents and mortality in a national study of U.S. urban communities. Environ Health Perspect. 2013;121(10):1148–1153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kaufman JD, Adar SD, Barr RG, et al. Association between air pollution and coronary artery calcification within six metropolitan areas in the USA (the Multi-Ethnic Study of Atherosclerosis and Air Pollution): a longitudinal cohort study. Lancet. 2016;388(10045):696–704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Kaufman JD, Elkind MSV, Bhatnagar A, et al. Guidance to reduce the cardiovascular burden of ambient air pollutants: a policy statement from the American Heart Association. Circulation. 2020;142(23):e432–e447. [DOI] [PubMed] [Google Scholar]
- 7. Wang M, Sampson PD, Sheppard L, et al. Long-term exposure to ambient ozone and progression of subclinical arterial disease: the Multi-Ethnic Study of Atherosclerosis and Air Pollution. Environ Health Perspect. 2019;127(5):057001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Kirwa K, Eckert CM, Vedal S, et al. Ambient air pollution and risk of respiratory infection among adults: evidence from the Multiethnic Study of Atherosclerosis (MESA). BMJ Open Respir Res. 2021;8(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Dominici F, Peng RD, Bell ML, et al. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA. 2006;295(10):1127–1134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Bravo MA, Ebisu K, Dominici F, et al. Airborne fine particles and risk of hospital admissions for understudied populations: effects by urbanicity and short-term cumulative exposures in 708 US communities. Environ Health Perspect. 2017;125(4):594–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Chang HH, Reich BJ, Miranda ML. Time-to-event analysis of fine particle air pollution and preterm birth: results from North Carolina, 2001–2005. Am J Epidemiol. 2012;175(2):91–98. [DOI] [PubMed] [Google Scholar]
- 12. Gray SC, Edwards SE, Schultz BD, et al. Assessing the impact of race, social factors and air pollution on birth outcomes: a population-based study. Environ Health. 2014;13(1):4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Pereira G, Evans KA, Rich DQ, et al. Fine particulates, preterm birth, and membrane rupture in Rochester. NY Epidemiology. 2016;27(1):66–73. [DOI] [PubMed] [Google Scholar]
- 14. Miranda ML, Edwards SE, Keating MH, et al. Making the environmental justice grade: the relative burden of air pollution exposure in the United States. Int J Environ Res Public Health. 2011;8(6):1755–1771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Bell ML, Ebisu K. Environmental inequality in exposures to airborne particulate matter components in the United States. Environ Health Perspect. 2012;120(12):1699–1704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Bravo MA, Anthopolos R, Bell ML, et al. Racial isolation and exposure to airborne particulate matter and ozone in understudied US populations: environmental justice applications of downscaled numerical model output. Environ Int. 2016;92–93:247–255. [DOI] [PubMed] [Google Scholar]
- 17. Morello-Frosch R, Lopez R. The riskscape and the colorline: examining the role of segregation in environmental health disparities. Envivonmental Research. 2006;102(2):181–196. [DOI] [PubMed] [Google Scholar]
- 18. Mikati I, Benson AF, Luben TJ, et al. Disparities in distribution of particulate matter emission sources by race and poverty status. Am J Public Health. 2018;108(4):480–485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Acevedo-Garcia D, Lochner KA, Osypuk TL, et al. Future directions in residential segregation and health research: a multilevel approach. Am J Public Health. 2003;93(2):215–221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Massey D. Segregation and stratification: a biosocial perspective. Du Bois Rev. 2004;1(1):7–25. [Google Scholar]
- 21. Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav. 2010;51(1_suppl):S28–S40. [DOI] [PubMed] [Google Scholar]
- 22. Tessum CW, Apte JS, Goodkind AL, et al. Inequity in consumption of goods and services adds to racial–ethnic disparities in air pollution exposure. Proc Natl Acad Sci. 2019;116(3):6001–6006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Di Q, Wang Y, Zanobetti A, et al. Air pollution and mortality in the Medicare population. N Engl J Med. 2017;376(26):2513–2522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. US Environmental Protection Agency . Our Nation's Air. Washington, DC: US Environmental Protection Agency; 2020. [Google Scholar]
- 25. US Environmental Protection Agency . Reviewing National Ambient Air Quality Standards (NAAQS): scientific and technical information. 2021; https://www.epa.gov/naaqs. Accessed March 19, 2021.
- 26. US Environmental Protection Agency . The Green Book. 8-hour ozone (2015) nonattainment area summary 2021; https://www3.epa.gov/airquality/greenbook/jnsum.html. Accessed March 8, 2021.
- 27. Makar M, Antonelli J, Di Q, et al. Estimating the causal effect of fine particulate matter levels on death and hospitalization: are levels below the safety standards harmful? Epidemiology. 2017;28(5):627–634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. US Environmental Protection Agency . EPA Annual Environmental Justice Progress Report FY 2018. Washington, DC: US Environmental Protection Agency; 2018. [Google Scholar]
- 29. Strosnider H, Kennedy C, Monti M, et al. Rural and urban differences in air quality, 2008–2012, and community drinking water quality, 2010–2015—United States. MMWR Surveill Summ. 2017;66(13):1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Hajat A, Diez-Roux AV, Adar SD, et al. Air pollution and individual and neighborhood socioeconomic status: evidence from the Multi-Ethnic Study of Atherosclerosis (MESA). Environ Health Perspect. 2013;121(11-12):1325–1333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Lawrence EM, Zajacova A. The relationship between education and health: reducing disparities through a contextual approach. Annual Rev Public Health. 2018;39(1):273–289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Bravo MA, Leong MC, Gelfand AE, et al. Assessing disparity using measures of racial and educational isolation. Int J Environ Res Public Health. 2021;18(17): 9384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Berrocal VJ, Gelfand AE, Holland DM. A bivariate space-time downscaler under space and time misalignment. Ann Appl Stat. 2010;4(4):1942–1975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Berrocal VJ, Gelfand AE, Holland DM. Space-time data fusion under error in computer model output: an application to modeling air quality. Biometrics. 2012;68(3):837–848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Berrocal VJ, Gelfand AE, Holland DM. A spatio-temporal downscaler for output from numerical models. J Agric Biol Environ Stat. 2010;15(176–197). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Massey DS, Denton NA. The dimensions of residential segregation. Soc Forces. 1988;67(2):281–315. [Google Scholar]
- 37. Reardon SF, O’Sullivan D. Measures of spatial segregation. Sociol Methodol. 2004;34(1):121–162. [Google Scholar]
- 38. Johnston R, Poulsen M, Forrest J. Ethnic and racial segregation in U.S. metropolitan areas, 1980–2000: the dimensions of segregation revisited. Urban Affairs Review. 2007;42(4):479–504. [Google Scholar]
- 39. White K, Borrell LN. Racial/ethnic residential segregation: framing the context of health risk and health disparities. Health Place. 2011;17(2):438–448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Shihadeh ES, Flynn N. Segregation and crime: the effect of black social isolation on the rates of black urban violence. 1996;74(4):1325–1352. [Google Scholar]
- 41. Anthopolos R, James SA, Gelfand AE, et al. A spatial measure of neighborhood level racial isolation applied to low birthweight, preterm birth, and birthweight in North Carolina. Spat Spatiotemporal Epidemiol. 2011;2(4):235–246. [DOI] [PubMed] [Google Scholar]
- 42. Messer LC, Laraia BA, Kaufman JS, et al. The development of a standardized neighborhood deprivation index. J Urban Health. 2006;83(6):1041–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. US Census Bureau . 2010 Census Urban and Rural Classification and Urban Area Criteria. 2010; https://www.census.gov/programs-surveys/geography/guidance/geo-areas/urban-rural/2010-urban-rural.html. Accessed September 14, 2021.
- 44. Bernardinelli L, Clayton D, Pascutto C, et al. Bayesian analysis of space-time variation in disease risk. Stat Med. 1995;14(21-22):2433–2443. [DOI] [PubMed] [Google Scholar]
- 45. Leroux BG, Lei X, Breslow N. Estimation of disease rates in small areas: a new mixed model for spatial dependence. In: Statistical Models in Epidemiology, the Environment, and Clinical Trials. New York, NY: Springer-Verlag; 2000:179–191. [Google Scholar]
- 46. Watanabe S. Asymptotic equivalence of Bayes cross validation and widely applicable information criterion in singular learning theory. J Mach Learn Res. 2010;11:3571–3594. [Google Scholar]
- 47. Lee D, Rushowrth A, Napier G. Spatio-temporal areal unit modeling in R with conditional autoregressive priors using the CARBayesST package. J Stat Softw. 2018;84(9). [Google Scholar]
- 48. Lee D. CARBayes: an R package for Bayesian spatial modeling with conditional autoregressive priors. J Stat Softw. 2013;55(13). [Google Scholar]
- 49. Geweke J. Evaluating the accuracy of sampling-based approaches to the calculation of posterior moments. In: Bernardo JM, Berger JO, Dawid AP, Smith AFM, eds. Bayesian Statistics. Oxford, UK: Oxford University Press; 1992:169–193. [Google Scholar]
- 50. R Core Team . A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2019. [Google Scholar]
- 51. James G, Witten D, Hastie T, et al. An Introduction to Statistical Learning: Wtih Applications in R. New York, NY: Springer; 2017. [Google Scholar]
- 52. Menard R. An introduction to logistic regression diagnostics. In: Lewis-Beck MS, ed. Applied Logistic Regression Analysis. 2nd ed. Thousand Oaks, CA: SAGE Publications; 2001. [Google Scholar]
- 53. Johnson RE, Jones K, Manley D. Confounding and collinearity in regression analysis: a cautionary tale and an alternative procedure, illustrated by studies of British voting behaviour. Qual Quant. 2018;52(4):1957–1976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Seinfeld JH, Pandis SN. Chapter 6: Chemistry of the troposphere. In: Atmospheric Chemistry and Physics: From Air Pollution to Climate Change. 3rd ed. New York, NY: John Wiley & Sons Inc.; 2016:175–264. [Google Scholar]
- 55. Bergin MS, West JJ, Keating TJ, et al. Regional atmospheric pollution and transboundary air quality management. Annu Rev Environ Resour. 2005;30(1):1–37. [Google Scholar]
- 56. Mohai P, Saha R. Which came first, people or pollution? Assessing the disparate siting and post-siting demographic change hypotheses of environmental injustice. Environ Res Lett. 2015;10(11). [Google Scholar]
- 57. Bravo MA, Fuentes M, Zhang Y, et al. Comparison of exposure estimation methods for air pollutants: ambient monitoring data and regional air quality simulation. Environ Res. 2012;116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Stuart AL, Mudhasakul S, Sriwantanapongse W. The social distribution of neighborhood pollution and monitoring protection. J Air Waste MA. 2009;59(5):591–602. [DOI] [PubMed] [Google Scholar]
- 59. Bravo MA, Anthopolos R, Kimbro RT, et al. Residential racial isolation and spatial patterning of type 2 diabetes mellitus in Durham, North Carolina. Am J Epidemiol. 2018;187(7):1467–1476. [DOI] [PubMed] [Google Scholar]
- 60. Vinikoor-Imler LC, Gray SC, Edwards SE, et al. The effects of exposure to particulate matter and neighbourhood deprivation on gestational hypertension. Paediatr Perinat Epidemiol. 2012;26(2):91–100. [DOI] [PubMed] [Google Scholar]
- 61. US Census Bureau . More working women than men have college degrees, Census Bureau reports. 2011; https://www.census.gov/newsroom/releases/archives/education/cb11-72.html. Accessed September 10, 2021.
- 62. Case A, Deaton A. Life expectancy in adulthood is falling for those without a BA degree, but as educational gaps have widened, racial gaps have narrowed. Proc Natl Acad Sci. 2021;118(11). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Bailey ZD, Krieger N, Agénor M, et al. Structural racism and health inequities in the USA: evidence and interventions. Lancet. 2017;389(10077):1453–1463. [DOI] [PubMed] [Google Scholar]
- 64. Rothstein R. The Color of Law: a Forgotten History of How Our Government Segregated America. New York, NY: Liveright Publishing Corporation; 2017. [Google Scholar]
- 65. US Census Bureau . 2010 Decennial Census. Washington DC: US Census Bureau; 2010. [Google Scholar]
- 66. Gray SC, Edwards SE, Miranda ML. Race, socioeconomic status, and air pollution exposure in North Carolina. Environ Res. 2013;126:152–158. [DOI] [PubMed] [Google Scholar]
- 67. McGurty EM. Warren County, NC, and the emergence of the environmental justice movement: unlikely coalitions and shared meanings in local collective action. Soc Natur Resour. 2000;13(4):373–387. [Google Scholar]
- 68. Mohai P, Pellow D, Roberts JT. Environmental justice. Annu Rev Env Resour. 2009;34(1):405–430. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.