

Abstract
Background.
Social determinants of health are relevant to cardiovascular outcomes but have had limited examination in atrial fibrillation (AF).
Objectives.
The purpose of this study was to examine the association of annual household income and cardiovascular outcomes in individuals with AF.
Methods.
We analyzed administrative claims for individuals with AF from 2009–2015 captured by a health claims database. We categorized estimates of annual household income as <$40,000; $40–59,999; $60–74,999; $75–99,999; and ≥$100,000. Covariates included demographics, education, cardiovascular disease risk factors, comorbid conditions, and anticoagulation. We examined event rates by income category and in multivariable-adjusted models in reference to the highest income category (≥$100,000).
Results.
Our analysis included 336,736 individuals (age 72.7±11.9 years; 44.5% women; 82.6% white, 8.4% black, 7.0% Hispanic, and 2.1% Asian) with AF followed for median (25th, 75th percentile) of 1.5 (0.6, 3.0) years. We observed an inverse association between income and heart failure and myocardial infarction (MI) with evidence of progressive risk across decreased income categories. Individuals with household income <$40,000 had the greatest risk for heart failure (hazard ratio [HR] 1.17; 95% confidence interval [CI], 1.05, 1.30) and MI (HR 1.18; 95% CI 0.98, 1.41) compared to those with income ≥$100,000.
Conclusions.
We identified an association between lower household income and adverse outcomes in a large cohort of individuals with AF. Our findings support consideration of income in the evaluation of cardiovascular risk in individuals with AF.
Keywords: atrial fibrillation, income, cardiovascular outcomes, social determinant of health, health claims
INTRODUCTION
Atrial fibrillation (AF) is a common, highly morbid cardiac arrhythmia that is associated with multiple cardiovascular and non-cardiovascular complications. AF results in significant social and medical burdens, and accounts for $6 billion in annual U.S. healthcare spending.1 Care for AF is complex and requires adequate social resources and health literacy to monitor for symptoms, navigate and adhere to complicated medication regimens (such as anticoagulation), and coordinate primary and specialty care services.2
Social determinants of health are relevant to AF given their potential to affect treatment and associated outcomes. To date the foremost focus of social determinants in AF has been on race. Studies have underscored racial differences in treatment, awareness of the condition, and risk for adverse outcomes.3,4 In a community-based study, income has likewise been related to increased risk of developing AF.5 Median neighborhood income has also been positively associated with access to direct oral anticoagulants (as opposed to warfarin).6 Additional social determinants of health, such as neighborhood-and community-level factors and health care access, likewise have relevance to health outcomes,7 and may mediate associations between income and health outcomes in AF. Examination of the interaction of race and income in AF remains limited and may demonstrate how interrelated social factors contribute towards adverse outcomes and thereby direct treatment efforts.
We investigated the association of household income and cardiovascular outcomes in individuals with AF. We utilized a database of deidentified, aggregated commercial and Medicare Advantage health claims, thereby enabling us to conduct our analysis in a large, socially diverse cohort with enhanced generalizability. Our primary hypothesis was that lower income would be associated with increased risks of heart failure, myocardial infarction, and stroke in this large cohort of individuals with AF. Our secondary hypothesis was that lower income would be a stronger risk factor for adverse outcomes in racial and ethnic minorities compared to white referents.
METHODS
Cohort selection
We obtained data from Optum© Clinformatics® Data Mart (Eden Prairie, MN, www.optum.com), a large U.S. database comprised of inpatient, outpatient, emergency department, pharmacy, and laboratory health claims. Data are de-identified and informed consent is thereby waived. Medical claims include International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis and procedure codes; Current Procedural Terminology, Version 4 (CPT-4) procedure codes; Healthcare Common Procedure Coding System procedure codes; and site of service codes. The database includes commercial and Medicare Advantage enrollees and is geographically diverse across the U.S. and similar to the insured population.8 Analysis was conducted at Emory University with the approval of the Institutional Review Board. Patients or the public were not involved in the design, or conduct, or reporting, or dissemination of our research.
We selected individuals having a diagnosis of AF during the period of January 1, 2009 to September 30, 2015. AF was defined by the presence of at least 1 inpatient or 2 outpatient claims for AF (ICD-9-CM 427.31 or 427.32 in any diagnostic position). We required 2 outpatient claims in order to minimize the impact of rule-out diagnoses and improve the specificity of our definition of AF; this restriction is not applied to inpatient claims, which have greater specificity for the diagnosis of AF. This approach has been validated elsewhere.9 Outpatient AF diagnostic codes were temporally separated by a minimum of 1 week to a maximum of 1 year. Date of diagnosis (first in-patient claim or second out-patient claim) was defined as the date of study entry for time-dependent analyses. We used the second outpatient claim of AF to preclude the immortal time bias inherent to initiating analysis at the first date of AF diagnosis. We identified 727,935 individuals with a diagnosis of AF.
Household Income
Household income was derived by AmeriLINK Consumer Marketing Database which provides estimates of annual household income. Income data are collected by monthly survey from a representative cross section of the U.S. population of >30,000 households and are informed by 130 variables that encompass ZIP+4 (a highly specific geographic locator), Internal Revenue Service data, address-level home value, aggregated credit, and short-term loans. Derived estimates of household income are validated by comparison to self-reported income collected by household surveys.10 The claims database divides household income into 6 categories: <$40,000, $40–49,999, $50–59,999, $60–74,999, $75–99,999, and ≥$100,000. For this analysis, we categorized income as <$40,000; $40–59,999; $60–74,999; $75–99,999; and ≥$100,000. We combined the $40–49,9999 and $50–59,999 categories due to the limited numbers cohort participants in these two categories of estimated annual household income.
Outcome ascertainment
We identified incident cardiovascular events that occurred within the enrollment period after the date of AF diagnosis. The outcomes of interest were obtained from inpatient claims and included heart failure,11 myocardial infarction,12, 13 and ischemic stroke.14 Each outcome was defined using the primary discharge diagnosis in an inpatient claim as follows: heart failure was defined by the presence of ICD-9-CM codes 402.x1, 404.x1, 404.x3, and 428; myocardial infarction was defined by the presence of ICD-9-CM discharge diagnosis code of 410.xx; ischemic stroke was defined by the presence of ICD-9-CM codes 434.xx and 436.xx. Supplementary Table 1 provides a comprehensive list of ICD codes used to identify the outcomes of heart failure, myocardial infarction and stroke.
Covariates
Age, sex, and race are included in the claims data. The database collects race and ethnicity from public records (e.g., driver’s license) and by imputation with commercially available software (E-Tech, Ethnic Techologies, South Hackensack, New Jersey) that employs validated algorithms incorporating racial and ethnic neighborhood composition as ascertained by the U.S. Census, residential zip code, and first and last name.15 Race and ethnicity were subsequently categorized as white, black, Asian, or Hispanic. Education level was derived from Census data at the ZIP+4 level and categorized as less than high school diploma, high school diploma, less than bachelor degree, bachelor degree or higher, or unknown. For this analysis we categorized education as less than high school diploma and high school diploma; less than bachelor degree; or bachelor degree or higher. Additional clinical covariates were selected from prior analyses of AF with recognized contributions to the outcomes studied here and relevance to AF.16 These covariates included hypertension, diabetes, prior coronary heart disease, prior heart failure, prior stroke, chronic obstructive pulmonary disease, and chronic kidney disease. All covariates were defined by ICD-9-CM codes in inpatient and outpatient claims prior to or at the time of AF diagnosis, as listed in Supplementary Table 1.
Oral Anticoagulation
We identified oral anticoagulants including warfarin, dabigatran, rivaroxaban, and apixaban prescribed within 3 months prior to 6 months after the date of AF diagnosis. Data were obtained from outpatient pharmaceutical claims, which provide the National Drug Code, the prescription fill date, and the number of days supplied.
Statistical Analysis
We summarized the distributions of continuous and categorical variables. Our primary analysis was the association of income with incident heart failure, myocardial infarction, and ischemic stroke in individuals with AF. Date of AF diagnosis was defined as time 0 and time of study entry for each individual included in our cohort. We calculated the rates of incident events during follow-up through database disenrollment or September 30, 2015, whichever came first. We then examined associations of income with myocardial infarction, heart failure, and ischemic stroke in multivariable-adjusted Cox proportional hazards models that compared risk by income category using income ≥$100,000 as the referent. For each outcome assessed we excluded the respective prevalent disease. We then examined for interactions by race and income as well as for income and education. All analyses were adjusted initially for age, sex, and race (model 1); then for age, sex, race, education, hypertension, diabetes, ischemic stroke, coronary heart disease, and heart failure (model 2); and then adjusted for all covariates including age, sex, race, education, hypertension, diabetes, ischemic stroke, coronary heart disease, heart failure, chronic obstructive pulmonary disease, and chronic kidney disease as well as oral anticoagulant use (model 3). We stratified individuals by race and ethnicity to assess for differences in risk by income level to investigate differences by race and ethnicity strata.
We verified the assumption of proportional hazards with Schoenfeld residuals. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC). Given the potential for residual confounding in our analysis, we conducted a bias analysis using the methods articulated by VanderWeele and Ding.17 Specifically, we calculated the E-value for the hazard ratios obtained comparing the lowest to the highest income category for those endpoints in which we found associations. The E-value can be interpreted as the minimum strength of association that an unmeasured confounder would need to have with both the exposure and the outcome, after adjusting for the measured covariates, to explain away an observed association.17
RESULTS
After excluding individuals with <180 days of enrollment before a diagnosis of AF (n=312,958), and those missing income (n=66,822), race or ethnicity (n=11,130), or education (n=289), there were 336,736 individuals included in the analysis (mean age 72.7±11.9 years; 44.5% women), as summarized in Table 1.
Table 1.
Characteristics of AF cohort, 2009–2015.
| Entire cohort | <$40K | $40–59K | $60–74K | $75–99K | $100K | |
|---|---|---|---|---|---|---|
| No. of Individuals Demographics | 336,736 | 129,845 | 62,833 | 34,685 | 41,246 | 68,127 |
| Age, years [mean (SD)] | 72.7 (11.9) | 77.2 (9.3) | 73.5 (11.1) | 71.4 (11.8) | 69.6 (12.3) | 66 (12.8) |
| Women | 149,865 (44.5) | 73,896 (56.9) | 26,426 (42.1) | 13,421 (38.7) | 14,963 (36.3) | 21,159 (31.1) |
| Race | ||||||
| White | 277,964 (82.6) | 101,939 (78.5) | 51,418 (81.8) | 28,913 (83.4) | 35,210 (85.4) | 60,484 (88.8) |
| Black | 28,286 (8.4) | 15,262 (11.8) | 5,532 (8.8) | 2,617 (7.6) | 2,414 (5.9) | 2,461 (3.6) |
| Asian | 6,976 (2.1) | 1,954 (1.5) | 1,155 (1.8) | 780 (2.3) | 1,015 (2.5) | 2,072 (3) |
| Hispanic | 23,510 (7.0) | 10,690 (8.2) | 4,728 (7.5) | 2,375 (6.9) | 2,607 (6.3) | 3,110 (4.6) |
| Education | ||||||
| < High School | 103,579 (30.8) | 61,581 (47.4) | 20,952 (33.4) | 8,894 (25.6) | 7,648 (18.5) | 4,504 (6.6) |
| < Bachelor’s degree | 188,007 (55.8) | 64,051 (49.3) | 37,173 (59.2) | 22,184 (64) | 27,102 (65.7) | 37,497 (55.0) |
| ≥ Bachelor’s Degree | 45,150 (13.4) | 4,213 (3.2) | 4,708 (7.5) | 3,607 (10.4) | 6,496 (15.8) | 26,126 (38.4) |
| Comorbidities | ||||||
| CHA2DS2-VASc [mean (SD)] | 4.1 (2.0) | 4.7 (1.8) | 4.2 (1.9) | 3.8 (2.0) | 3.6 (2.0) | 3.0 (2.0) |
| Hypertension | 275,630 (82.8) | 113,145 (87.9) | 52,605 (84.6) | 28,262 (82.5) | 32,538 (80.0) | 49,080 (73.3) |
| Diabetes | 176,929 (34.9) | 75,342 (38.6) | 34,336 (36.9) | 18,176 (35.4) | 20,502 (33.0) | 28,573 (27.1) |
| Prior CHD | 148,841 (44.2) | 62,204 (47.9) | 29,159 (46.4) | 15,446 (44.5) | 17,346 (42.1) | 24,686 (36.2) |
| Prior HF | 110,242 (32.7) | 50,549 (38.9) | 21,176 (33.7) | 10,746 (31) | 11,773 (28.5) | 15,998 (23.5) |
| Prior stroke | 88,607 (26.3) | 39,746 (30.6) | 17,273 (27.5) | 8,717 (25.1) | 9,763 (23.7) | 13,108 (19.2) |
| COPD | 116,482 (34.6) | 52,986 (40.8) | 22,572 (35.9) | 11,416 (32.9) | 12,573 (30.5) | 16,935 (24.9) |
| CKD | 70,388 (20.9) | 33,176 (25.6) | 13,862 (22.1) | 6,867 (19.8) | 7,326 (17.8) | 9,157 (13.4) |
| Oral Anticoagulant Use | 86,702 (25.8) | 31,182 (24.0) | 16,210 (25.8) | 9,274 (26.8) | 11,277 (27.3) | 18,759 (27.5) |
Values correspond to N (percentage) unless otherwise stated. CHD, coronary heart disease; HF, heart failure; COPD, chronic obstructive pulmonary disease; CKD, chronic kidney disease. CHA2DS2-VASc: congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke/transient ischemic attack, vascular disease, age 65–75 years, and sex category. SD: standard deviation
The majority were white race (82.6%) with 28,286 (8.4%) black, 23,510 (7.0%) Hispanic, and 6,976 (2.1%) Asian. A greater proportion of black (54%) and Hispanic (45%) individuals belonged to the lowest income category compared to whites (37%) or Asians (28%). Education was likewise distributed by income, with a greater proportion of individuals with lower education belonging to lower income categories. In contrast, 58% of individuals with a bachelor degree or higher were in the highest income category.
During a median (25th, 75th percentile) follow-up of 1.5 (0.6, 3.0) years there were 4,736 cases of heart failure; 1,444 cases of myocardial infarction; and 3,435 cases of stroke. Table 2 summarizes the incidence rates for each of the outcomes by income category. With increasing income category, event rates decreased with respect to myocardial infarction, heart failure, and stroke.
Table 2.
Age-, sex-, race-standardized incidence rates and 95% confidence intervals (per 1000 person-years) of cardiovascular disease (heart failure, myocardial infarction, ischemic stroke), by income
| Event | <$40K | $40–59K | Income $60–74K | $75–99K | ≥$100K |
|---|---|---|---|---|---|
| Heart failure* | 5.4 (4.2, 6.6) | 4.1 (3.5, 4.6) | 3.4 (2.7, 4.0) | 3.1 (2.7, 3.6) | 3.0 (2.4, 3.5) |
| Myocardial infarction† | 2.1 (1.6, 2.7) | 1.9 (1.5, 2.4) | 1.4 (0.9, 1.9) | 1.4 (1.0, 1.7) | 1.6 (1.0, 1.5) |
| Stroke‡ | 3.2 (2.2, 4.2) | 2.5 (2.0, 3.0) | 2.3 (1.9, 2.7) | 2.1 (1.8, 2.4) | 2.3 (2.0, 2.6) |
Prevalent heart failure was excluded from Model 3 when calculating incident heart failure
Prevalent coronary heart disease was excluded from Model 3 when calculating incident myocardial infarction
Prevalent ischemic stroke was excluded from Model 3 when calculating incident ischemic stroke
Table 3 summarizes the hazard ratios with p-values for the trend of the associations of income with each of the cardiovascular outcomes, while Figure 1 presents them graphically.
Table 3.
Hazard ratios and 95% confidence intervals of cardiovascular outcomes by income category and adjusted for covariates in cohort with AF
| Income | ||||||
|---|---|---|---|---|---|---|
| <$40K | $40–59K | $60–74K | $75–99K | ≥$100K | p-value for trend | |
| Heart Failure* | ||||||
| Model 1 | 1.41 (1.28, 1.55) | 1.30 (1.17, 1.44) | 1.22 (1.08, 1.38) | 1.18 (1.05, 1.33) | 1 (ref) | <0.0001 |
| Model 2 | 1.19 (1.07, 1.32) | 1.14 (1.02, 1.28) | 1.11 (0.98, 1.26) | 1.10 (0.97, 1.24) | 1 (ref) | 0.03 |
| Model 3 | 1.17 (1.05, 1.30) | 1.13 (1.01, 1.26) | 1.10 (0.97, 1.25) | 1.09 (0.97, 1.23) | 1 (ref) | 0.05 |
| Myocardial Infarction† | ||||||
| Model 1 | 1.35 (1.14, 1.60) | 1.28 (1.07, 1.54) | 1.18 (0.95, 1.46) | 1.10 (0.89, 1.36) | 1 (ref) | 0.005 |
| Model 2 | 1.18 (0.98, 1.42) | 1.16 (0.96, 1.41) | 1.09 (0.87, 1.36) | 1.05 (0.85, 1.30) | 1 (ref) | 0.42 |
| Model 3 | 1.18 (0.98, 1.41) | 1.15 (0.95, 1.40) | 1.09 (0.87, 1.36) | 1.05 (0.84, 1.30) | 1 (ref) | 0.46 |
| Ischemic stroke‡ | ||||||
| Model 1 | 1.06 (0.95, 1.18) | 0.97 (0.86, 1.1) | 0.99 (0.86, 1.14) | 1.00 (0.87, 1.15) | 1 (ref) | 0.36 |
| Model 2 | 0.98 (0.87, 1.11) | 0.92 (0.81, 1.04) | 0.95 (0.82, 1.09) | 0.97 (0.84, 1.11) | 1 (ref) | 0.62 |
| Model 3 | 0.99 (0.88, 1.12) | 0.92 (0.81, 1.05) | 0.95 (0.82, 1.1) | 0.97 (0.84, 1.12) | 1 (ref) | 0.61 |
Prevalent heart failure was excluded from Model 3 when calculating incident heart failure
Prevalent coronary heart disease was excluded from Model 3 when calculating incident myocardial infarction
Prevalent ischemic stroke was excluded from Model 3 when calculating incident ischemic stroke
Model 1 adjusted for baseline age, sex, and race.
Model 2 adjusted for baseline age, sex, race, education, hypertension, diabetes, and prevalent ischemic stroke, prevalent coronary heart disease, and prevalent heart failure.
Model 3 adjusted for baseline age, sex, race, education, hypertension, diabetes, prevalent ischemic stroke, prevalent coronary heart disease, prevalent heart failure, chronic obstructive pulmonary disease, chronic kidney disease, and oral anticoagulant use.
Figures 1A, 1B, 1C. Hazard ratios with 95% confidence intervals of incident heart failure, myocardial infarction, and ischemic stroke by income category and adjusted for covariates in cohort with AF.
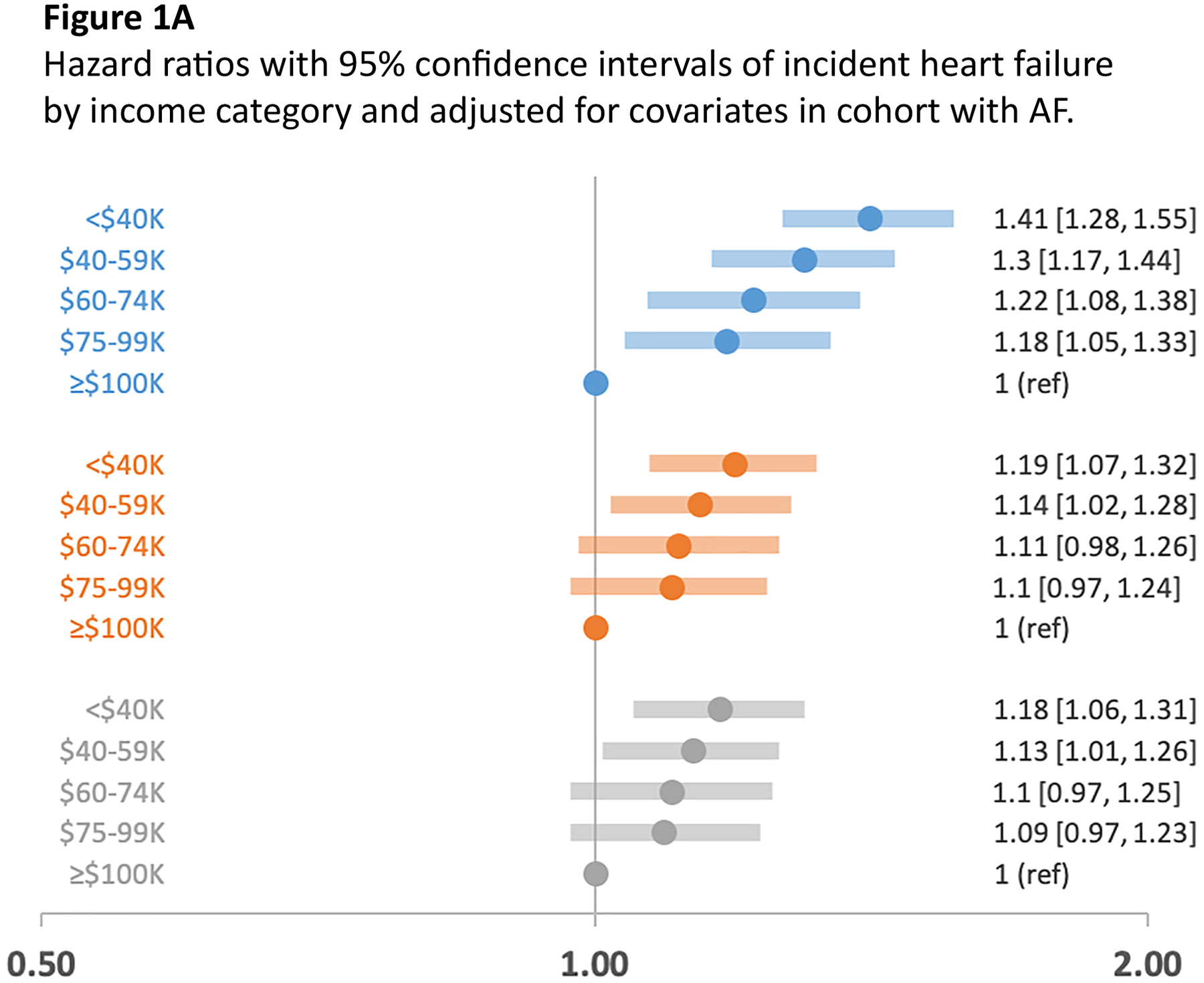
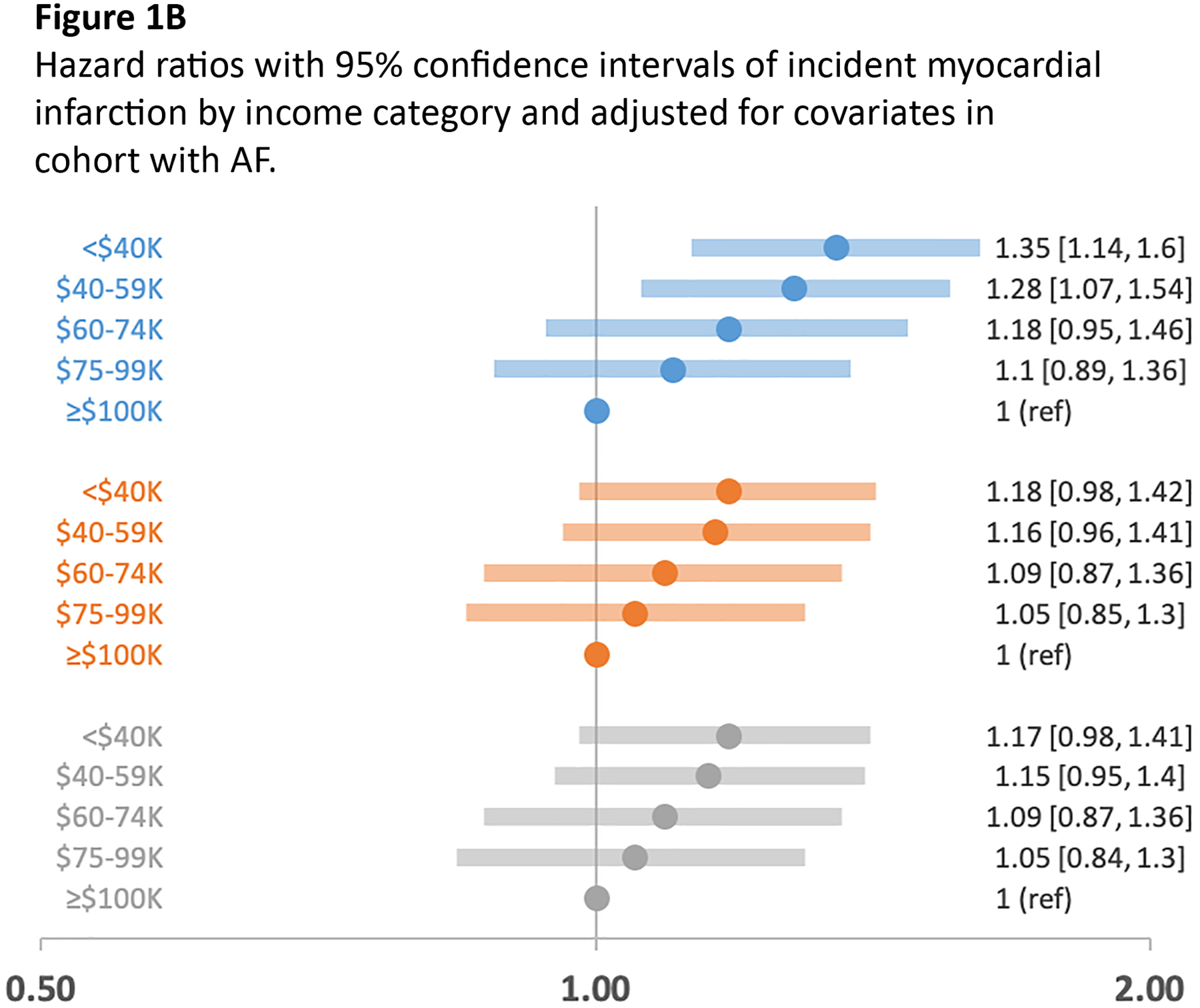
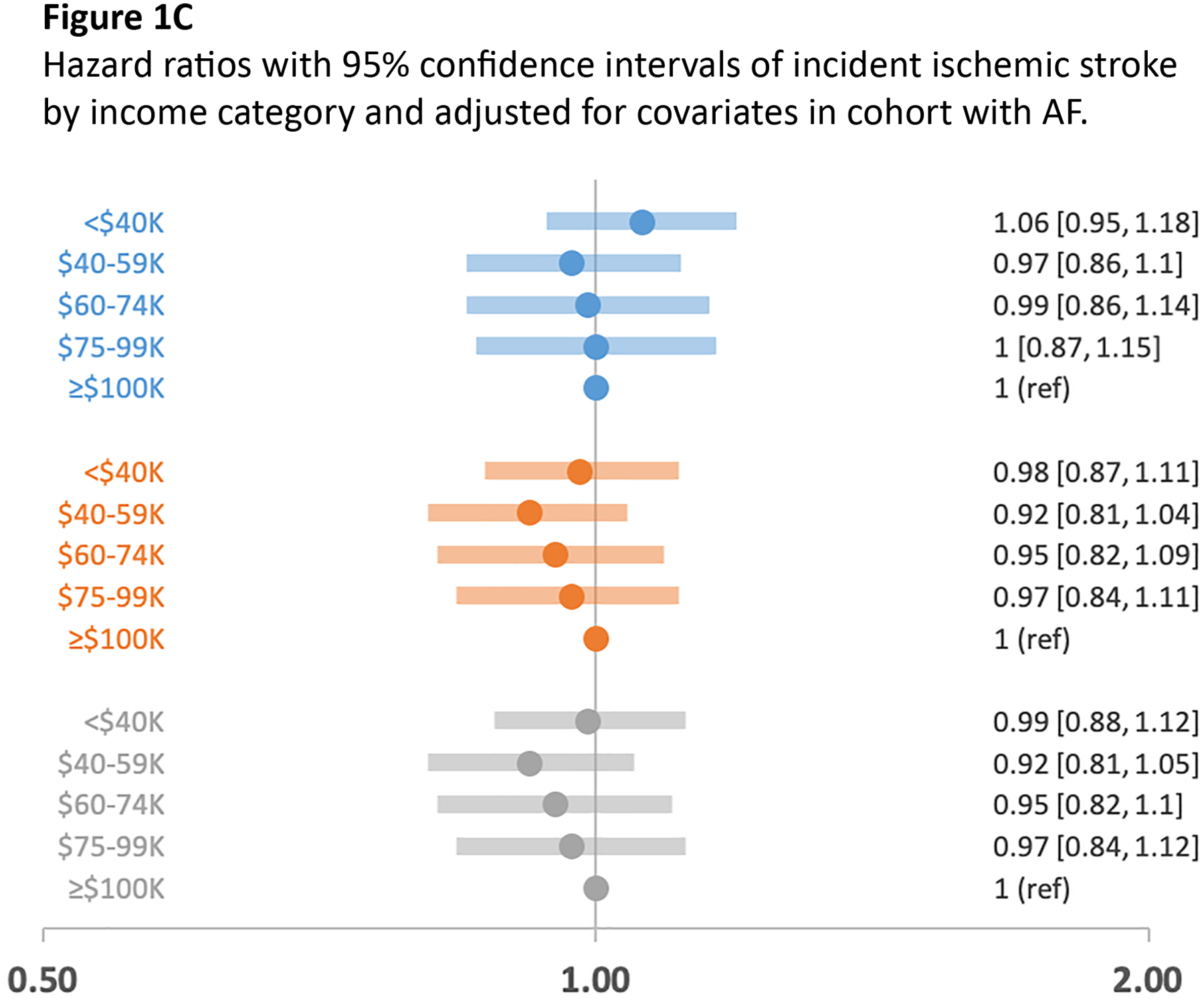
Figures 1A, 1B, and 1C are forest plots of multivariable-adjusted hazard ratios with 95% confidence intervals of incident cardiovascular outcomes heart failure, myocardial infarction, and ischemic stroke by income category. Incident event rates were calculated and related to income in multivariable-adjusted Cox proportional hazard models that compared risk by income category with income >$100,000 as referent. Model 1, adjusted for age, sex, and race; Model 2, adjusted for age, sex, race, education, hypertension, diabetes, prevalent coronary heart disease, and prevalent heart failure; Model 3, adjusted for age, sex, race, education, hypertension, diabetes, prevalent coronary heart disease, prevalent heart failure, chronic obstructive coronary disease, chronic kidney disease, and oral anticoagulant use. Figure 1A, heart failure by income category; Figure 1B, myocardial infarction by income category; Figure 1C, ischemic stroke by income category adjusted for the 3 models.
We observed a graded, inverse association between income and the risks for heart failure and myocardial infarction. Individuals in the lowest income category had the greatest risk for heart failure with a hazard ratio (HR) of 1.17 (95% confidence interval [CI], 1.05, 1.30) and myocardial infarction with a HR of 1.18 (95% CI 0.98, 1.41) relative to the highest income category. The association between income and heart failure remained significant in the lowest income category after multivariable adjustment with the clinical covariates, oral anticoagulant use, and education. We did not observe an association between income and ischemic stroke.
Interactions for race/ethnicity and income and for income and education were not statistically significant in multivariable-adjusted models. The results of analyses stratified by race and ethnicity are presented in Supplementary tables 2A through 2D. Our bias assessment identified an E-value of 2.17 (CI, lower limit, 1.88) for the association between extreme income categories and heart failure in Model 1, and an E-value of 2.04 (CI, lower limit, 1.54) for the association between extreme income categories and myocardial infarction in Model 1. We concluded from these calculations that potential unmeasured confounders, such as neighborhood SES or racial segregation, have weaker associations with the endpoints of interest and therefore are unlikely to be responsible for the observed associations.18, 19
Discussion
In a large, geographically diverse health claims database, we observed associations between annual income and increased risk of heart failure and myocardial infarction in individuals with incident AF. Specifically, we observed progressively increased risk for these adverse cardiovascular outcomes, such that individuals with income categorized as <$40,000/year had the greatest risk. The association of lower household income and the increased risk of heart failure remained significant even after multivariable adjustment. These findings were observed over a relatively limited follow-up duration (median 1.5 years).
There was no association between income and risk of ischemic stroke in the cohort as a whole. Lack of an association may be due to the relatively limited follow-up duration in this study and/or the similar prevalence of anticoagulant prescriptions across income categories.
Prior study of income in relation to AF and cardiovascular disease
The examination of income and AF has had limited study with one community-based study identifying a graded, inverse, dose-response association between total family income and risk of incident AF.6 In contrast, the association of income with cardiovascular outcomes and mortality has been well established. Total family income has been inversely associated with cardiovascular disease and cardiovascular death in multiple studies and was deemed a “neglected” metric for cardiovascular disease.20, 21, 22 An analysis of the National Longitudinal Mortality Study identified a strong association between income and mortality that was most pronounced at incomes below $22,500.23 Income has further relevance to longevity. Robust data indicate a strong linear association between income and length of life in US adults.24 The aforementioned studies indicate the relevance of income to health outcomes including cardiovascular disease and mortality. Our study now contributes further data on the importance of income, specifically toward the associations of income and health outcomes directly relevant to the increasing number of people with AF.
Rationale for the association of income and health outcomes
Multiple potential pathways have been proposed to relate income and health. The socioecological theory asserts that health is shaped by multiple factors: social, family, and community networks; living and working conditions; and broad social, economic, cultural, and environmental conditions and policies.25 Low income as determined by socioeconomic status has been associated in general with diminished access to preventative care,26 specialty care,27 and poorer clinical outcomes.28 Low socioeconomic status yields decreased access to prescription medications,29 and may contribute toward competing priorities for using health services, medications, and diverse other needs. Low income may complicate adherence to medications or appointments, as individuals struggle to choose between material necessities and medical care. Furthermore, limited health literacy is more prevalent in lower income individuals, and likewise may add to the heterogenous contributions of social determinants on complicated chronic disease such as AF.2 This study demonstrates an important association between income and cardiovascular disease in AF and we recognize that further research is needed to understand the complex pathways by which patients with low income and AF develop adverse outcomes.
Relevance of social determinants to clinical care and practice
Recognizing that social determinants are associated with health outcomes, there has been increased focus on their incorporation into routine clinical care. The National Academy of Medicine has recommended inclusion of social and behavioral determinants in electronic health records due to the “substantial empirical evidence of the contribution of social and behavioral factors to function status and the onset, progression, and effective treatment of disease.”30 Our analysis indicates the substantive contribution of income towards adversity and its prominent role as a social determinant of health. Our study is unable to distinguish the multiple mechanisms and pathways that may relate income and adverse cardiovascular outcomes; however, our findings underscore the importance of further studies to examine the practical implications of utilizing income in routine clinical assessment with the goal of identifying and effectively intervening on high-risk patient populations. Collecting and utilizing income data as one component of a risk stratification tool that incorporates a suite of social determinants of health in the clinical setting may be of interest to clinicians seeking to identify and intervene on vulnerable patients, health systems attempting to improve the outcomes of populations, and health plans seeking to provide high value, cost conscious care.
Strengths and limitations
Our analysis had several strengths, most particularly the availability of nationwide health claims data from over 300,000 individuals diagnosed with AF. The generalizability of our analysis to insured persons with AF is strengthened by the utilization of a database that is geographically diverse and racially representative as well as inclusive of enrollees of both private and Medicare advantage plans.
We would also like to summarize the important limitations of our study. First, inclusion in this cohort required that individuals have health insurance, thereby allowing health claims data to be captured. Consequently, the exclusion of a highly vulnerable patient population may underestimate the effect of income on adverse cardiovascular outcomes in individuals with AF and may not be generalizable to the uninsured population. Second, utilizing claims data selects for individuals with AF who are more often in need of medical care, thereby limiting the generalizability to individuals with AF who do not seek care and do not generate health claims. Third, requiring two outpatient claims for AF was intended to increase specificity of the diagnostic algorithm but excluding individuals with only 1 outpatient claim may have selected for individuals with more symptomatic AF, again limiting the generalizability of our results to patients with asymptomatic paroxysmal AF. Fourth, we relied exclusively on health claims for ascertainment of AF, covariates, and the cardiovascular outcomes; we are not able to correlate administrative claims with clinical data by individual review of health records. Fifth, several variables including income, race, and education were derived using varied algorithms, thereby subject to misrepresentation. Sixth, we expect that there is residual confounding by omission of informative, socially relevant variables (neighborhood-level determinants, treatment adherence, health literacy) that may be part of a causal pathway to relate income and adverse clinical outcomes associated with AF. However, our assessment for uncontrolled confounding suggested that only a strong unmeasured confounder (E-value >2) would be able to explain the observed associations. Seventh, our follow-up time for this study was limited to a median of 1.5 years. We expect that a longer study interval would have yielded more events to include in the analysis. The limited follow-up time also allows for the potential of reverse causation. Eighth, our analyses do not account for the effect of AF treatment during the observation period. However, we included prescription of oral anticoagulation for stroke prevention as a fundamental metric of routine clinical care for AF. Finally, we recognize our categorization of income as limited. The measurement of income is complex and may be adjusted for family size, the addition of noncash benefits such as food stamps or Medicare, or broadened to include wealth and assets that are separate from income.25
Conclusion
In conclusion, in a retrospective analysis of a large U.S. health care utilization database, we observed a significant association between income and risk of cardiovascular outcomes relevant to AF, specifically heart failure and myocardial infarction. Our results are consistent with prior evidence that underscores the relevance of income to increased risk for cardiovascular and health outcomes. Further study must now address how to incorporate data regarding income into the treatment of patients with AF to improve cardiovascular outcomes and mitigate adverse outcomes in vulnerable patient populations.
Supplementary Material
3. Key Questions:
1. What is already known about this subject?
Income is strongly associated with cardiovascular disease risk and mortality. There has been limited knowledge of the association between income and adverse cardiovascular outcomes in individuals with atrial fibrillation.
2. What does this study add?
This study identified significant associations between household income and risks for myocardial infarction and heart failure in individuals with prevalent atrial fibrillation. Individuals in the lowest income quartile had 1.3- to 1.4-fold greater risk for myocardial infarction and heart failure relative to the highest income quartile. These results support prior evidence demonstrating the relevance of social resources to health outcomes.
3. How might this impact on clinical practice?
Household income is a social determinant of health that mediates access to care and health outcomes. Incorporating social factors in health systems and the provision of care provide opportunities to promote equity, address disparities, and improve outcomes in vulnerable patient populations.
Funding:
Research reported in this publication was supported by the NHLBI/NIH award number R01HL122200 and R01HL143010. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This work was supported by Grant 2015084 from the Doris Duke Charitable Foundation, New York, NY, and by American Heart Association grant 16EIA26410001.
Footnotes
Disclosures:
Dr. Lindsay Bengtson is an employee of Optum©. There are no other author disclosures.
References
- 1.Benjamin EJ, Virani SS, Callaway CW, et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation. 2018;137:e67–e492. [DOI] [PubMed] [Google Scholar]
- 2.Magnani JW, Mujahid MS, Aronow HD, et al. Health Literacy and Cardiovascular Disease: Fundamental Relevance to Primary and Secondary Prevention: A Scientific Statement From the American Heart Association. Circulation. 2018;138:e48–e74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Magnani JW, Norby FL, Agarwal SK, et al. Racial Differences in Atrial Fibrillation-Related Cardiovascular Disease and Mortality: The Atherosclerosis Risk in Communities (ARIC) Study. JAMA Cardiol. 2016;1:433–441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Essien UR, Holmes DN, Jackson LR, et al. Association of Race/Ethnicity With Oral Anticoagulant Use in Patients With Atrial Fibrillation: Findings From the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation II. JAMA Cardiol. 2018;3:1174–1182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Misialek JR, Rose KM, Everson-Rose SA, et al. Socioeconomic status and the incidence of atrial fibrillation in whites and blacks: the Atherosclerosis Risk in Communities (ARIC) study. J Am Heart Assoc. 2014;3:e001159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sholzberg M, Gomes T, Juurlink DN, et al. The Influence of Socioeconomic Status on Selection of Anticoagulation for Atrial Fibrillation. PLoS ONE. 2016;11:e0149142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Havranek EP, Mujahid MS, Barr DA, et al. Social Determinants of Risk and Outcomes for Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2015;132:873–898. [DOI] [PubMed] [Google Scholar]
- 8.Wallace PJ, Shah ND, Dennen T, et al. Optum Labs: building a novel node in the learning health care system. Health Aff (Millwood). 2014;33:1187–1194. [DOI] [PubMed] [Google Scholar]
- 9.Incidence and prevalence of atrial fibrillation and associated mortality among Medicare beneficiaries, 1993–2007. - PubMed - NCBI [Internet]. [cited 2019 Dec 5];Available from: https://www.ncbi.nlm.nih.gov/pubmed/22235070 [DOI] [PMC free article] [PubMed]
- 10.KDM Group. AmeriLINK Income Products [Internet]. 2014; Available from: https://www.kbmg.com/products/amerilink/. Accessed 6 Aug 2019.
- 11.Saczynski JS, Andrade SE, Harrold LR, et al. Mini-Sentinel Systematic Evaluation of Health Outcome of Interest Definitions for Studies Using Administrative and Claims Data. Pharmacoepidemiol Drug Saf [Internet]. 2012. [cited 2018 Aug 18];21 Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3808171/ [Google Scholar]
- 12.Kiyota Y, Schneeweiss S, Glynn RJ, et al. Accuracy of Medicare claims-based diagnosis of acute myocardial infarction: estimating positive predictive value on the basis of review of hospital records. Am Heart J. 2004;148:99–104. [DOI] [PubMed] [Google Scholar]
- 13.Wahl PM, Rodgers K, Schneeweiss S, et al. Validation of claims-based diagnostic and procedure codes for cardiovascular and gastrointestinal serious adverse events in a commercially-insured population. Pharmacoepidemiol Drug Saf. 2010;19:596–603. [DOI] [PubMed] [Google Scholar]
- 14.Andrade SE, Harrold LR, Tjia J, et al. A systematic review of validated methods for identifying cerebrovascular accident or transient ischemic attack using administrative data. Pharmacoepidemiol Drug Saf. 2012;21 Suppl 1:100–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.DeFrank JT, Bowling JM, Rimer BK, et al. Triangulating differential nonresponse by race in a telephone survey. Prev Chronic Dis. 2007;4:A60. [PMC free article] [PubMed] [Google Scholar]
- 16.Huxley RR, Lopez FL, Folsom AR, et al. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2011;123:1501–1508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.VanderWeele TJ, Ding P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Annals of Internal Medicine. 2017;167:268. [DOI] [PubMed] [Google Scholar]
- 18.Akwo EA, Kabagambe EK, Harrell FE, et al. Neighborhood Deprivation Predicts Heart Failure Risk in a Low-Income Population of Blacks and Whites in the Southeastern United States. Circ Cardiovasc Qual Outcomes. 2018;11:e004052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kershaw KN, Osypuk TL, Do DP, et al. Neighborhood-Level Racial/Ethnic Residential Segregation and Incident Cardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis. Circulation. 2015;131:141–148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kaplan GA, Keil JE. Socioeconomic factors and cardiovascular disease: a review of the literature. Circulation. 1993;88:1973–1998. [DOI] [PubMed] [Google Scholar]
- 21.Lemstra M, Rogers M, Moraros J. Income and heart disease: Neglected risk factor. Can Fam Physician. 2015;61:698–704. [PMC free article] [PubMed] [Google Scholar]
- 22.Khaing W, Vallibhakara SA, Attia J, McEvoy M, Thakkinstian A. Effects of education and income on cardiovascular outcomes: A systematic review and meta-analysis. Eur J Prev Cardiolog. 2017;24:1032–1042. [DOI] [PubMed] [Google Scholar]
- 23.Backlund E, Sorlie PD, Johnson NJ. A comparison of the relationships of education and income with mortality: the national longitudinal mortality study. Social Science & Medicine. 1999;49:1373–1384. [DOI] [PubMed] [Google Scholar]
- 24.Chetty R, Stepner M, Abraham S, et al. The Association Between Income and Life Expectancy in the United States, 2001–2014. JAMA. 2016;315:1750–1766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McLeroy KR, Bibeau D, Steckler A, et al. An ecological perspective on health promotion programs. Health Educ Q. 1988;15:351–377. [DOI] [PubMed] [Google Scholar]
- 26.Katz SJ, Hofer TP. Socioeconomic disparities in preventive care persist despite universal coverage. Breast and cervical cancer screening in Ontario and the United States. JAMA. 1994;272:530–534. [PubMed] [Google Scholar]
- 27.Alter DA, Iron K, Austin PC, et al. SESAMI Study Group. Socioeconomic status, service patterns, and perceptions of care among survivors of acute myocardial infarction in Canada. JAMA. 2004;291:1100–1107. [DOI] [PubMed] [Google Scholar]
- 28.Clark AM, DesMeules M, Luo W, et al. Socioeconomic status and cardiovascular disease: risks and implications for care. Nat Rev Cardiol. 2009;6:712–722. [DOI] [PubMed] [Google Scholar]
- 29.Hyun KK, Brieger D, Woodward M, et al. The effect of socioeconomic disadvantage on prescription of guideline-recommended medications for patients with acute coronary syndrome: systematic review and meta-analysis. Int J Equity Health. 2017;16:162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Committee on the Recommended Social and Behavioral Domains and Measures for Electronic Health Records, Board on Population Health and Public Health Practice, Institute of Medicine. Capturing Social and Behavioral Domains and Measures in Electronic Health Records: Phase 2 [Internet]. Washington (DC): National Academies Press (US); 2015. [cited 2019 Nov]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK268995/ [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.