

Abstract
Background:
The coronavirus disease 2019 (COVID-19) pandemic has caused unprecedented disruptions to the lives of families. This study aimed to investigate the impact of pandemic-associated stress on food parenting practices including interactions surrounding snacks, and child diet.
Methods:
Parents (N = 318) of 2-12-year old children completed a cross-sectional online survey assessing current COVID-19-specific stress, pre-COVID-19 stress, financial stress (e.g. food insecurity), food parenting practices, and child snack intake frequency. Structural Equation Modeling was used to model simultaneous paths of relationships and test direct and indirect effects.
Results:
Stress, including financial hardship, was higher compared with before the crisis. The majority of children had regular mealtimes and irregular snack times. Higher COVID-19-specific stress was associated with more non-nutritive use of food and snacks (e.g. emotional and instrumental feeding), but also more structure and positive interactions (e.g. eating with or engaging with child around mealtimes). Higher COVID-19-specific stress was also associated with greater child intake frequency of sweet and savory snacks, with some evidence for mediation by snack parenting practices.
Conclusion:
Our findings indicate that stress associated with the COVID-19 pandemic may be linked to child snack intake with potential impacts on child obesity risk, and suggest several modifiable points of intervention within the family context.
Keywords: COVID-19, stress, parents, feeding, diet
1. Introduction
The coronavirus disease 2019 (COVID-19) pandemic has caused unprecedented changes to the lives of families in the US and around the globe (Liu, Bao, Huang, Shi, & Lu, 2020; Wang, Zhang, Zhao, Zhang, & Jiang, 2020). As the pandemic began to grow, mandatory lockdowns with consequent closure of non-essential businesses, kindergartens and schools, and cancellation of out-of-home leisure time activities and social gatherings (Fegert, Vitiello, Plener, & Clemens, 2020) forced the majority of children and parents to stay at home for a prolonged time. Further, due to isolation and contact restriction, parents were deprived of many available support systems (e.g. from family members, friends, school or other institutions) and resources (e.g. daycare, public libraries) (Fegert et al., 2020). Instead, parents, often mothers (Minello, 2020), were required to juggle work (from home), childcare, and home schooling by themselves (Di Giorgio, Di Riso, Mioni, & Cellini, 2020; Fegert et al., 2020). An article in the New York Times fittingly pondered the question of whether or not parents can have a child and a job in the COVID-19 economy (Perelman, 2020).
The annual Stress in America poll (American Psychological Association, 2020) demonstrated an increase in reported stress from the previous year with parents reporting higher stress compared with adults without children. Thus, parents are experiencing particularly marked pressures during the pandemic (Neubauer, Schmidt, Kramer, & Schmiedek, 2020), due not only to pandemic-related uncertainties, but also to disruption of habits (Aymerich-Franch, 2020) and daily routines of work and life, including schooling schedules (Flesia, Fietta, Colicino, Segatto, & Monaro, 2020; Ruiz-Roso et al., 2020). Despite increased stress, quarantine (e.g. “shelter-in-place”) and isolation (e.g. social distancing) directives have a second, potentially positive consequence – families spend more time together. Families are more likely to eat meals together at home with family meals being described as “part of the new normal” (Wilkins, 2020). This increases opportunities for parent-child interactions involving food.
‘Food parenting’ practices, i.e. the ways that parents feed their children, are associated with child eating behaviors, dietary intake and weight (Ventura & Birch, 2008). Vaughn et al.’s (2016) content map of food parenting practices distinguishes three constructs: i) coercive control, such as using food to control negative emotions of the child or applying rigid limits, ii) structure, such as having routines (e.g. regarding schedule or family members being present) or monitoring child intake, and iii) autonomy support or promotion, such as educating the child about nutrition or involving the child in food planning, shopping or preparation. While coercive control is hypothesized to be associated with less desirable child outcomes, structure and autonomy support are hypothesized to have beneficial outcomes.
Recently, a specific focus on snack parenting practices has emerged. Snacking is highly prevalent among children (Larson & Story, 2013) and contributed up to 28% of daily energy intake in US preschoolers before the pandemic (Rudy et al., 2018). Snack foods most commonly consumed by US children (2-18 years) are often high in energy-density and highly processed, including desserts/sweet and salty foods (Piernas & Popkin, 2010). To investigate the character and correlates of snack-specific parenting practices, targeted questionnaires have been developed (Corsini, Wilson, Kettler, & Danthiir, 2010; Gevers, Kremers, de Vries, & van Assema, 2018), with the Parenting around SNAcking Questionnaire (P-SNAQ) (Davison et al., 2018) intentionally based on the content map of food parenting practices.
Compared to parents’ food parenting practices during mealtimes, Davison et al. (2015) reported that parents frequently had a permissive approach to children’s snacking, such as being less likely to have specific rules or limits around snacks, showing low involvement in snack regulation or context, and engaging in emotion-based provision of snacks. Snack choices are less likely to be determined beforehand (i.e. more likely to be chosen in the moment), than main meals, which are more often pre-planned (Damen, Luning, Fogliano, & Steenbekkers, 2019). Complementing this picture, Fisher et al. (2015) showed that parents are flexible about the snack food quality and commonly place higher importance on behavioral management than provision of nutrition. With children of all ages spending more time at home due to the COVID-19 pandemic, snack parenting practices may therefore assume a more prominent role in parent-child food interactions, and have a particularly strong potential to impact children’s diets both positively and negatively.
Previous research shows that different types of stress, such as parenting stress (Gouveia, Canavarro, & Moreira, 2019), maternal psychological stress (Mitchell, Brennan, Hayes, & Miles, 2009; Rodgers et al., 2014; Swyden et al., 2017) and economic/financial stress or food insecurity (Bauer et al., 2015; Feinberg, Kavanagh, Young, & Prudent, 2008; Gross, Mendelsohn, Fierman, Racine, & Messito, 2012), can impact parents’ food parenting practices. Parents who report more stress appear to be at risk of using coercive practices that are less responsive to children’s hunger and satiety cues (Hurley, Black, Papas, & Caulfield, 2008). Stressed parents may also be more likely to use food or snacks as coping strategies to manage children’s behavior or emotions. However, to date, no study has investigated relationships between stress in parents, and snack parenting practices. Similarly, no study has examined the association of parents’ stress with food parenting practices that are generally perceived as positive (i.e. structure, autonomy support or promotion). In the current situation, another pressing question emerges: how might stress caused by the COVID-19 pandemic and associated lockdown impact the food parenting practices described above (i.e. coercive, structure-related, autonomy supportive, snack specific)?
Further, it is important to test whether stress-induced changes to snack parenting might have downstream effects on child snack intake. During the COVID-19 pandemic changes in child appetite (e.g. reduced appetite) (Orgilés, Morales, Delveccio, Mazzeschi, & Espada, 2020), emotional/stress eating (Wilkins, 2020) and more frequent snacking has been reported, including increased intake of healthy (e.g. fruit and vegetable) but especially fried, sweet and snack foods (Pietrobelli et al., 2020; Ruiz-Roso et al., 2020). These changes in dietary habits, especially changes that last for sustained periods of time and increase intake of higher caloric, highly palatable snack foods, could increase children and adolescents’ risk of obesity (Larson & Story, 2013). No studies have yet investigated whether general food parenting practices or snack-related practices – behaviors which may be modifiable and thus potential intervention targets – might mediate effects of pandemic-associated disruption on children’s intake during the pandemic.
The current study had three aims. The first was to briefly characterize current stress (COVID-19 specific and financial stress) experienced by parents due to the pandemic, as well as parents’ food parenting practices (i.e. positive mealtime practices, general feeding practices and snack parenting practices) during the COVID-19 pandemic. The second was to investigate relationships between parents’ COVID-19-specific stress and measures of food parenting practices. The third was to test whether effects of parents’ COVID-19-specific stress on frequency of children’s snack food intake could be partially explained by snack parenting practices. We hypothesized that the pandemic would increase parent stress levels and that parents would report high levels of food interactions with their children, that parents’ pandemic-associated stress would be related to food parenting practices, and that snack parenting would partly mediate effects of pandemic-associated stress on child snack intake.
2. Methods
2.1. Study procedure and sample
An online survey was created via Qualtrics to investigate the impact of the COVID-19 crisis on familial health behaviors including eating behavior, TV/screen time, physical activity, and sleep. Survey data collection was from May 26, 2020 to June 29, 2020. The survey included 484 questions and took an estimated 60 minutes for participants to complete. Participants were recruited via Amazon’s Mechanical Turk (MTurk) and social media. MTurk's demographic filters (based on consistent self-reported answers over time) were used to target individuals of 18 years or more. Parents of 2-12 year-olds were asked additional questions relating to their parenthood and child health behaviors. Instructions were to complete only one survey per family, and parents who had more than one child in the study age range were instructed to complete questions for their youngest child. Residents of New Jersey, Delaware, District of Columbia, and Illinois were initially targeted, as those states in the US were under lockdown orders on the date the survey was distributed. After the initial survey distribution, the survey was extended to include residents of California, Maine, Michigan, Nebraska, New Mexico, New York, Oregon, Pennsylvania, Tennessee, and Washington, states with regional lockdowns. MTurk users with poor survey completion metrics (less than 1000+ approved completed surveys or a user-approval rating below 85%) were excluded. MTurk participants were compensated $6 for the completion of the survey. For social media recruitment, research personnel shared the survey link to their personal social media accounts. Participants recruited through social media were entered into a gift card lottery, where three participants were randomly selected to receive a $20 Amazon gift card. A consent statement was provided to all participants at the beginning of the survey: “Your completion of this survey will serve as your consent to be in this research study.” All methods were approved by the Johns Hopkins University Institutional Review Board. In total, 579 participants commenced the survey (MTurk = 76%, social media = 24%). Out of the 579, n = 467 completed the survey in its entirety, with an additional n = 123 completing up to 75% and a further n = 109 completing up to 50%. Of the 579 participants, 325 reported being a parent of children aged 2-12 years old. Seven cases were excluded since children were younger than 2 years of age, leaving a total of 318 parents.
2.2. Measures
Participants reported demographic and socio-economic information including parent and child age and sex, parent employment status, education level, annual household income, relationship status, living arrangements, and race/ethnicity. Additionally, participants provided brief COVID-19-specific information including whether their own or their partner’s work was considered ‘essential’, if they had tested positive for COVID-19, and what effect the pandemic had on regular childcare.
Stress.
Information about financial, general and COVID-19-specific stress was also obtained. First, financial questions assessed participants’ current and pre-COVID-19 financial situation (responses: ‘cannot make ends meet’ to ‘comfortable, with extra’), food insecurity (2-item screener by Hager et al., 2010) and receipt of public assistance (e.g. food support/stamps). Second, parents indicated how stressed they were in general right now, as well as before the pandemic (e.g. “In general, how would you rate your level of stress before the COVID-19 crisis?”). Responses were scored between 0-10, with higher scores indicating more stress. Third, parents responded to 16 COVID-19-specific stress items (see Appendix, e.g. “How stressed are you about the following in relation to the COVID-19 crisis? - Losing my job, I will get COVID-19, My child will fall behind in school”). Response options ranged from 1 = “not at all” to 5 = “extremely”. All items were averaged and the overall mean COVID-19 stress score was used in analysis (Cronbach’s alpha = 0.91).
Food parenting practices:
A combination of study-specific and validated instruments was used. A first set of questions aimed to capture variability in routines and positive behaviors tied to specific eating occasions, or meals. First, parents were asked about the current regularity of the child’s eating routine (e.g. “Does your child have a regular time to eat dinner?”). Next, parents responded to questions about five positive practices for each type of eating occasion (breakfast, lunch, dinner, snacks) with items based on subscales of the Comprehensive Feeding Practices Questionnaire (CFPQ) (Musher-Eizenman & Holub, 2007). Practices which included a) parent makes a variety of healthy foods available (α = 0.83), b) child helps prepare foods (α = 0.84), c) parent or partner/spouse eats together with child (α = 0.69), d) parent engages with child during meal (e.g. teaching about nutrition/healthy eating, educating child for instance by weighing food) (α = 0.88), and e) parent models healthy eating by eating healthy foods at meals themselves (α = 0.83). Response options ranged from 1 = never, 2 = occasionally, 3 = sometimes, 4 = often, to 5 = always. Scores for each of the five practices were averaged across the four meal occasions, and higher scores indicated more positive mealtime practices.
Next, general feeding practices were assessed using the following subscales of validated questionnaires: emotional feeding (5 items, e.g. “I give my child something to eat if s/he is feeling bored”, α = 0.93) and instrumental feeding (4 items, e.g. “I reward my child with something to eat when s/he is well behaved”, α = 0.79) from the Parent Feeding Style Questionnaire (PFSQ) (Wardle, Sanderson, Guthrie, Rapoport, & Plomin, 2002), monitoring (4 items, e.g. “How much do you keep track of the high-fat foods that your child eats?”, α = 0.92) from the CFPQ, structured meal timing (3 items, e.g. “I decide the times when my child eats his/her meals”, α = 0.61), structured meal setting (3 items, e.g. “I insist my child eats meals at the table ”, α = 0.75) and family meal setting (1 item, “My child eats the same meals as the rest of the family”) from the Feeding Practices and Structure Questionnaire (FPSQ) (Jansen, Williams, Mallan, Nicholson, & Daniels, 2016). The response options for all items were 1 = never, 2 = rarely, 3 = sometimes, 4 = often, and 5 = always.
Snack parenting practices were assessed with four subscales from the Parenting around SNAcking Questionnaire (P-SNAQ) (Davison et al., 2018): a) emotion-based snack feeding (5 items, e.g. “I give my child a snack to improve her mood”, α = 0.90; note: 1 item about giving snack to make child feel less distressed was added), b) restriction of snacks (3 items, e.g. “I hide snacks from my child”, α = 0.75), c) snack planning and routines (3 items, e.g. “I give my child snacks at about the same time each day”, α = 0.78), and d) snack rules and limits (4 items, e.g. “I tell my child when she can have a snack”, α = 0.86). Response options ranged from 1 = really not like me, 2 = sort of not like me, 3 = sort of like me, to 4 = really like me.
Child diet.
Parents answered questions about child diet adapted from previously used food frequency questionnaires (Neuhouser, Lilley, Lund, & Johnson, 2009; NIH National Cancer Institute). For the current analysis, parent-reported child intake frequencies of sweet snacks (a) chocolate or candies [abbreviated going forward to ‘chocolate’], (b) cookies, cakes, pies, brownies [‘cookies’], (c) doughnuts, Danishes, muffins [‘doughnuts’], (d) ice cream and frozen desserts [‘ice cream’], and savory snacks ((a) regular chips, (b) low-fat chips, (c) other salty snacks) were used. Response options were adapted to assess the frequency of intake over the past seven days, with options ranging from never to multiple times per day. Responses to the food items were recoded to reflect the frequency of consumption per week (Gregório et al., 2017).
2.3. Data Analysis
Descriptive statistics and bivariate correlations among study variables were examined using SPSS 26 (IBM Corp., Armonk, New York). All remaining analyses examining relationships were conducted using maximum likelihood estimation with bias-corrected bootstrapping with 1000 re-samples in Mplus v.6.12 (Muthén & Muthén, 1998-2017).
First, simultaneous relationships between overall COVID-19-specific stress and food parenting measures were examined, while controlling for pre-COVID-19 stress level, child age, gender and socioeconomic disadvantage. For this purpose, we created a socioeconomic disadvantage index by summing four dichotomized indicators of relative disadvantage to generate a continuous variable (range 0-4) with higher scores reflecting more disadvantage (i) lower household income (< $50,000 = 1, ≥ $50,000 = 0), ii) lower education (2-year college degree or less = 1, 4-year college or graduate degree = 0), iii) food insecurity (yes = 1, no = 0), iv) receipt of public assistance (yes = 1, no = 0).
Next we investigated inter-relationships between COVID-19 stress level, snack parenting, and child snacking. Specifically, we tested relationships between the four snack parenting practices (i.e. emotion-based snack feeding, restriction of snacks, snack planning and routines and snack rules and limits), and children’s intake frequency for the seven sweet and savory snack types. To this end, the model described in the previous paragraph was adjusted in two ways: i) all parent-child mealtime practices except for the four snack parenting practices were removed, and ii) the model was expanded to include the following seven types of snack food: 1) chocolate, 2) cookies, 3) doughnuts, 4) ice cream, 5) regular chips, 6) low-fat chips, and 7) other salty snacks. These relationships were also adjusted for the four covariates, as well as overall COVID-19 stress. Mediation analysis (i.e. testing of indirect effects) was only performed when snack parenting practices (mediators) were significantly associated with both the independent variable (overall COVID-19 stress) and either of the outcome variables (child intake frequency of sweet and savory snacks), controlling for the independent variable. The approach described by Preacher and Hayes (2008) was used to test the four mediators (i.e. snack parenting practices) simultaneously if more than one was associated with the outcome variable in the previous step (see Figure 1). Model fit was evaluated using the following indices: Root Mean-Square Error of Approximation (RMSEA < 0.08), Comparative Fit Index (CFI > 0.90), and Tucker-Lewis Index (TLI > 0.90) (Hu & Bentler, 1999). The statistical significance of the i) specific indirect effects, ii) total indirect effects (combination of all specific indirect effects) and iii) direct effects (independent variable on outcome, controlling for mediators) was determined using bias-corrected bootstrapped 95% confidence intervals (MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002; Mackinnon, Lockwood, & Williams, 2004).
Figure 1:
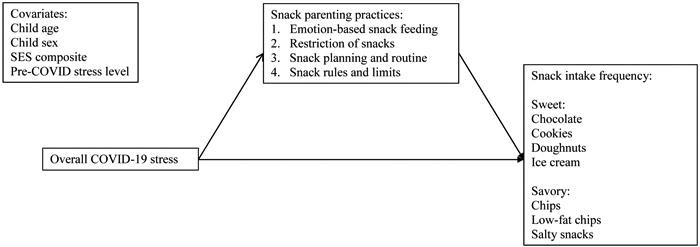
Conceptual mediation model including overall COVID-19 stress, four snack parenting practices and child sweet and savory snack intake frequency. Covariates are regressed on the mediators and the outcome variables.
3. Results
3.1. Stress
Table 1 shows sample characteristics. A substantial proportion of participants indicated that financial strain had increased in comparison with before the COVID-19 crisis. For instance, while 44.0% of parents reported that their money situation did not change compared with before the COVID-19 crisis and 16.4% indicated that it ‘improved’, 31.1% said it ‘worsened’ and 8.5% reported that it ‘significantly worsened’. Prior to the pandemic, 8 (2.5%) families indicated that they could not make ends meet which now increased to 23 (7.2%); similarly, 33 (10.4%) indicated that they previously had to “cut back”, while this had now increased to 78 (24.5%). This shift in categories (in addition to ‘Enough but no extra’: previously 155 [48.7%], now 133 [41.8%]; ‘Comfortable, with extra’: previously 122 [38.4%], now 84 [26.4%]) was significant (χ2 = 151.32, df = 9, p < 0.001). Likewise, food insecurity and receipt of public assistance significantly increased in comparison to before the COVID crisis: 76 (24.4% yes now) vs. 70 (22.5% yes pre-COVID; χ2 = 66.94, df = 1, p < 0.001) and 62 (19.6% yes now) vs. 44 (13.9% yes pre-COVID; χ2 = 186.40, df = 1, p < 0.001) respectively.
Table 1:
Sample characteristics for parents and their children (N = 318)
| n or M | % or SD | Range | |
|---|---|---|---|
| Child age (years) | 6.7 | 3.1 | 2-12.9 |
| Preschool-aged (<6 years) | 149 | 46.9 | |
| School-aged (≥6 years) | 169 | 53.1 | |
| Child sex (female)# | 153 | 48.1 | |
| Parent age | 37.7 | 6.6 | 24-66 |
| Parent sex (female) | 206 | 64.8 | |
| Relationship status | |||
| Partnered/married | 280 | 88.1 | |
| Single | 19 | 6.0 | |
| Divorced/separated | 19 | 6.0 | |
| Living arrangements during pandemic | |||
| Living with partner/spouse and children | 280 | 88.1 | |
| Living with children, no partner/spouse | 38 | 11.9 | |
| Number of children currently in household | 2.1 | 1.1 | 1-9 |
| Ethnicity# | |||
| Hispanic, Latinx or Spanish origin | 27 | 8.5 | |
| Race | |||
| White | 246 | 77.4 | |
| Asian | 23 | 7.2 | |
| Black or African American | 18 | 5.7 | |
| Hispanic/Latinx | 10 | 3.1 | |
| Native American/Alaska Native | 5 | 1.6 | |
| More than 1 race or other | 16 | 4.9 | |
| Household income (<$50,000)# | 74 | 23.6 | |
| Education level | |||
| No or partial college | 17 | 36.8 | |
| 4-year college degree | 125 | 39.3 | |
| Graduate degree | 76 | 23.9 | |
| Employment status | |||
| Full-time employment | 204 | 64.2 | |
| Homemaker (full-time parent) | 50 | 15.7 | |
| Part-time employment | 35 | 11.0 | |
| Self-employed | 13 | 4.1 | |
| Unemployed and seeking work | 11 | 3.5 | |
| Student | 4 | 1.3 | |
| Retired | 1 | 0.3 | |
| Essential worker role (yes) | |||
| Self | 100 | 31.4 | |
| Partner | 114 | 40.7 | |
| Positive COVID-19 test | 2 | 0.6 | |
| Effect on regular childcare | |||
| Self or partner/spouse had to change work schedule to care for child(ren) | 122 | 38.4 | |
| No child in childcare | 114 | 35.8 | |
| Regular childcare was not affected | 51 | 16.0 | |
| Difficulty arranging for childcare | 21 | 6.6 | |
| Pay less for childcare | 8 | 2.5 | |
| Pay more for childcare | 2 | 0.6 | |
Only six participants indicated different living arrangements prior to the COVID-19 pandemic
Prefer not to answer: child gender – 2 (0.6%), ethnicity – 2 (0.6%) and 1 (0.3%) didn’t know, income – 5 (1.6%).
Parents reported a significant increase in their general stress level (t = −7.74, p <0.001), from an average of 3.93 (SD = 2.25, range 0-9.5) pre-COVID-19 to an average of 4.97 (SD = 2.69, range 0-10) now. Specifically, 11.9% reported no change, 19.5% reported a lower stress level now while the majority, 68.6%, reported a higher stress level now compared to pre-COVID-19. For the overall COVID-19-specific stress score, a mean of 2.69 (SD = 0.90) was recorded with a possible range from 1-5. As expected, both the pre-COVID-19 and current stress levels were significantly positively correlated with the overall COVID-19 stress score (r = .34 and r = .59 respectively, both p <0.001).
3.2. Food parenting practices during the COVID-19 pandemic
Despite pandemic-related disruption, most parents reported that children had a regular breakfast (n = 236, 78.4%), lunch (n = 235, 75.6%) and/or dinner (n = 246, 77.7%) time, with few variations between pre-school and school-aged children. In contrast, only 84 (28.6%) children had a regular snack time, reflecting 48 (34.5%) pre-school and 36 (22.6%) school-aged children. Additionally, 8.8% of parents reported that they ate meals together three or more times a day with all or most of their family members living in their household before the crisis. This number increased to 14.5% (χ2 = 228.96, df = 4, p < 0.001) during the crisis.
Table 2 shows means, standard deviations, and child age-related differences in parents’ positive mealtime practices, general feeding practices, and snack parenting practices. On average, means for the positive mealtime practices and structure-related practices (i.e. autonomy support) were higher than the means of emotional and instrumental feeding or the snack parenting practices. Out of the 15 practices, 10 differed between pre-school and school-aged children. School-aged children were more likely than pre-school-aged children to help prepare foods. Parents or their partner of pre-school-aged children were more likely to eat meals with their children, compared with parents of school-aged children. Parents of pre-school-aged children also reported higher endorsement of all snack parenting and general feeding practices compared to parents of school-aged children, with the exception of emotional feeding and family meal setting.
Table 2:
Means and standard deviations for food parenting practices (positive mealtime practices, general feeding practices, snack parenting practices) for the total sample and separated for pre-school and school-aged children
| Total sample (N=318) |
Pre-schoolers (n=149) |
School-aged children (n=169) |
p- value* |
||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | ||
| Positive mealtime practices | |||||||
| Variety of healthy food available | 4.03 | 0.73 | 4.05 | 0.63 | 4.01 | 0.81 | 0.667 |
| Child helps prepare food | 2.45 | 0.99 | 2.21 | 1.02 | 2.67 | 0.92 | <0.001 |
| Parent or partner/spouse eats with child | 3.23 | 0.77 | 3.34 | 0.78 | 3.13 | 0.76 | 0.019 |
| Parent engages with child around mealtime (e.g. teach about nutrition) | 2.55 | 1.04 | 2.56 | 0.99 | 2.54 | 1.08 | 0.903 |
| Parent models healthy eating | 3.25 | 0.91 | 3.26 | 0.89 | 3.23 | 0.93 | 0.774 |
| General feeding practices | |||||||
| PFSQ emotional feedinga | 2.04 | 0.94 | 2.10 | 0.97 | 1.98 | 0.91 | 0.249 |
| PFSQ instrumental feeding | 2.12 | 0.83 | 2.25 | 0.80 | 2.00 | 0.85 | 0.007 |
| CFPQ monitoringb | 3.60 | 1.10 | 3.86 | 0.95 | 3.38 | 1.17 | <0.001 |
| FPSQ structured meal settingc | 3.81 | 0.92 | 3.92 | 0.84 | 3.72 | 0.97 | 0.044 |
| FPSQ structured meal timing | 3.38 | 0.82 | 3.55 | 0.79 | 3.24 | 0.81 | 0.001 |
| FPSQ family meal setting | 3.80 | 0.99 | 3.76 | 1.02 | 3.83 | 0.97 | 0.497 |
| Snack parenting practices (P-SNAQ)d | |||||||
| Emotion-based snack feeding | 2.22 | 0.85 | 2.34 | 0.86 | 2.11 | 0.84 | 0.017 |
| Restriction of snacks | 2.12 | 0.92 | 2.38 | 0.90 | 1.89 | 0.88 | <0.001 |
| Snack planning and routines | 2.19 | 0.85 | 2.35 | 0.84 | 2.06 | 0.84 | 0.003 |
| Snack rules and limits | 2.74 | 0.85 | 2.88 | 0.79 | 2.63 | 0.89 | 0.008 |
One-way ANOVA results are presented. Results remained the same when group differences were examined with Mann-Whitney U-tests because some scales showed a tendency for non-normality.
Parental Feeding Style Questionnaire (PFSQ), 1= ‘never’ to 5= ‘always’ (Wardle et al., 2002)
Comprehensive Feeding Practices Questionnaire (CFPQ), 1= ‘never’ to 5= ‘always’ (Musher-Eizenman & Holub, 2007)
Feeding Practices and Structure Questionnaire (FPSQ), 1= ‘never’ to 5= ‘always’ (Jansen et al., 2016)
Parenting around SNAcking Questionnaire (P-SNAQ), 1= ‘really not like me’ to 4= ‘Really like me’ (Davison et al., 2018)
3.3. Relationships between overall COVID-19 stress and all food parenting practices measures during the pandemic
Table 3 shows the relationships between overall COVID-19 stress and all measures of food parenting practices. Overall COVID-19 stress was positively associated with the parent or partner eating with the child and engaging with child around mealtimes, emotional and instrumental feeding, and all snack parenting practices, while stress was negatively associated with making a variety of healthy foods available. COVID-19 stress was not associated with monitoring child intake, the three structure-related feeding practices, children helping prepare foods, or parents modeling healthy eating.
Table 3:
Associations between overall COVID-19 stress and food parenting practices
| Overall COVID-19 stress score | |||
|---|---|---|---|
| β | 95%CI | p-value | |
| Positive mealtime practices | |||
| Variety of healthy food available | −0.17 | −.24, −.04 | 0.008 |
| Child helps prepare food | 0.07 | −.05, .20 | 0.256 |
| Parent or partner/spouse eats with child | 0.15 | .02, .24 | 0.022 |
| Parent engages with child around mealtime (e.g. teach about nutrition) | 0.21 | .10, .39 | 0.001 |
| Parent models healthy eating | 0.05 | −.09, .19 | 0.460 |
| General feeding practices | |||
| PFSQ emotional feedinga | 0.20 | .08, .33 | 0.001 |
| PFSQ instrumental feeding | 0.28 | .15, .36 | <0.001 |
| CFPQ monitoringb | 0.06 | −.07, .22 | 0.324 |
| FPSQ structured meal settingc | 0.02 | −.11, .15 | 0.772 |
| FPSQ structured meal timing | 0.06 | −.05, .16 | 0.273 |
| FPSQ family meal setting | 0.05 | −.09, .19 | 0.480 |
| Snack parenting practices (P-SNAQ)d | |||
| Emotion-based snack feeding | 0.17 | .04, .28 | 0.011 |
| Restriction of snacks | 0.13 | .02, .25 | 0.025 |
| Snack planning and routines | 0.20 | .08, .29 | <0.001 |
| Snack rules and limits | 0.16 | .04, .26 | 0.007 |
Simultaneously examined and adjusted for child age, pre-COVID-19 stress level, SES
Model fit: χ2 (df) = 7.40 (6), p = 0.286, RMSEA = .03 (.00-.08), CFI = 1.00 and TLI = .98
Parental Feeding Style Questionnaire (PFSQ), 1= ‘never’ to 5= ‘always’ (Wardle et al., 2002)
Comprehensive Feeding Practices Questionnaire (CFPQ), 1= ‘never’ to 5= ‘always’ (Musher-Eizenman & Holub, 2007)
Feeding Practices and Structure Questionnaire (FPSQ), 1= ‘never’ to 5= ‘always’ (Jansen et al., 2016)
Parenting around SNAcking Questionnaire (P-SNAQ), 1= ‘really not like me’ to 4= ‘Really like me’ (Davison et al., 2018)
3.4. Relationships between overall COVID-19 stress, snack parenting practices and child sweet and savory snack intake frequency during the pandemic
Relationships between snack parenting practices and child sweet and savory snack intake frequencies were examined next. Results are presented in Table 4. Emotion-based snack feeding was positively associated with children’s intake frequency of ice cream, regular chips, low-fat chips and other salty snacks. Restriction of snacks and snack planning & routines were both positively associated with intake frequency of low-fat chips. Snack rules & limits, in contrast, was negatively associated with intake frequency of cookies and low-fat chips.
Table 4:
Associations between snack parenting practicesa and child sweet and savory intake frequencies, adjusting for overall COVID-19 stress and other covariates
| Emotion-based snack feeding | Restriction of snacks | Snack planning and routines | Snack rules and limits | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | 95%CI | p-value | β | 95%CI | p-value | β | 95%CI | p-value | β | 95%CI | p-value | |
| Sweet snacks | ||||||||||||
| Chocolate or any other types of candy (examples: M&Ms, candy bars, jelly bellies, dummies, and lifesavers). | 0.10 | −0.11, 1.64 | 0.086 | 0.16 | −0.11, 2.30 | 0.075 | 0.05 | −0.61, 1.29 | 0.486 | −0.07 | −1.48, 0.38 | 0.244 |
| Cookies, cake, pie, or brownies. | 0.06 | −0.30, 0.78 | 0.384 | 0.11 | −0.27, 1.07 | 0.244 | 0.04 | −0.35, 0.65 | 0.558 | −0.15 | −1.11, −0.04 | 0.036 |
| Doughnuts, sweet rolls, Danish, muffins, pan dulce, or pop-tarts. | 0.05 | −0.16, 0.70 | 0.218 | 0.05 | −0.51, 1.00 | 0.523 | 0.11 | −0.14, 1.30 | 0.116 | −0.10 | −1.08, 0.01 | 0.056 |
| Ice cream or other frozen desserts. | 0.13 | 0.15, 0.92 | 0.006 | −0.03 | −0.55, 0.29 | 0.547 | 0.05 | −0.28, 0.72 | 0.391 | 0.01 | −0.38, 0.45 | 0.874 |
| Savory snacks | ||||||||||||
| Regular potato chips, tortilla chips, corn chips and puffs (such as all flavors of Ruffles, Lays, Pringles, Doritos, Fritos, Cheetos) | 0.11 | 0.13, 1.23 | 0.015 | 0.05 | −0.45, 1.02 | 0.449 | 0.07 | −0.38, 1.22 | 0.303 | −0.09 | −1.23, 0.08 | 0.087 |
| Low-fat or non-fat potato chips, tortilla chips, and corn chips (such as Baked Lays, Reduced-fat Doritos, Fat-free Pringles) | 0.08 | 0.02, 0.89 | 0.039 | 0.17 | 0.20, 1.50 | 0.011 | 0.15 | 0.29, 1.40 | 0.003 | −0.10 | −1.03, −0.04 | 0.036 |
| Other salty snacks (like cheese nibs, Chex mix, goldfish crackers, Ritz | 0.10 | 0.06, 1.16 | 0.031 | 0.040 | −0.48, 0.93 | 0.535 | 0.09 | −0.25, 1.35 | 0.174 | −0.09 | −1.16, 0.11 | 0.104 |
Adjusted for child age, pre-COVID-19 stress level, SES and overall COVID-19 stress
Model fit: χ2 (df) = 7.40 (6), p = 0.286, RMSEA (90%CI) = .03 (.00-.08), CFI = 1.00 and TLI = .98
Parenting around SNAcking Questionnaire (P-SNAQ), 1= ‘really not like me’ to 4= ‘Really like me’ (Davison et al., 2018)
Table 5 gives results from tests of direct effects, specific indirect effects, and total indirect effects within the mediation models. The relationship between doughnuts and snack rules & limits was included given p = 0.056. Overall COVID-19 stress was directly positively associated with intake of all seven sweet and savory snack food types. Two snack parenting practices showed a partial mediation effect (i.e. significant indirect effect). Higher COVID-19-specific stress was associated with more emotion-based snack feeding, which was in turn related to more frequent ice cream intake by the children. Higher COVID-19-specific stress was also associated with using more snack planning and being more likely to have a snack routine, which in turn was related to more frequent low-fat chips intake.
Table 5:
Direct and indirect effects of overall COVID-19 stress on child sweet and savory snack intake frequencies through snack parenting practicesa (N = 318)
| Meditation model | Effect | β | 95%CI | p-value | % variance explainedb |
|---|---|---|---|---|---|
| Chocolate | Direct | 0.12 | 0.00, 1.75 | 0.050 | 9.5 |
| Cookies | Direct | 0.17 | 0.26, 1.02 | 0.001 | 8.2 |
| Snack rules | Indirect | −0.02 | −0.05, 0.00 | 0.086 | |
| Doughnuts | Direct | 0.17 | 0.37, 1.29 | <0.001 | 12.2 |
| Snack rules | Indirect | −0.02 | −0.04, 0.00 | 0.110 | |
| Ice cream | Direct | 0.13 | 0.08, 0.89 | 0.019 | 10.0 |
| Emotion-based snack feeding | Indirect | 0.02 | 0.00, 0.04 | 0.050 | |
| Chips | Direct | 0.21 | 0.55, 1.99 | 0.001 | 13.5 |
| Emotion-based snack feeding | Indirect | 0.02 | −0.00, 0.04 | 0.073 | |
| Low-fat chips | Direct | 0.25 | 0.51, 2.07 | 0.001 | 20.4 |
| Emotion-based snack feeding | Indirect | 0.01 | −0.00, 0.03 | 0.087 | |
| Restriction of snacks | Indirect | 0.02 | −0.00, 0.04 | 0.066 | |
| Snack planning | Indirect | 0.03 | 0.01, 0.05 | 0.009 | |
| Snack rules | Indirect | −0.02 | −0.03, 0.00 | 0.106 | |
| Total indirect | 0.05 | 0.01, 0.09 | 0.018 | ||
| Salty snacks | Direct | 0.25 | 0.69, 2.14 | <0.001 | 9.5 |
| Emotion-based snack | Indirect | 0.02 | −0.00, 0.03 | 0.088 |
Parenting around SNAcking Questionnaire (P-SNAQ), 1= ‘really not like me’ to 4= ‘Really like me’ (Davison et al., 2018)
Based on overall COVID-19 stress, mediators and covariates (child age, pre-COVID-19 stress level, SES)
4. Discussion
This study aimed to examine parents’ stress levels in response to the COVID-19 pandemic and test if COVID-19-specific stress was associated with multiple food parenting practices (positive mealtime practices, general feeding practices, snack parenting practices) used by parents with their 2-12-year-old children. We additionally examined whether snack parenting practices (emotion-based snack feeding, restriction of snacks, snack planning and routines, and snack rules and limits) could partially explain relationships between COVID-19-specific stress and children’s sweet and savory snack food intake frequency during the pandemic. Our results suggest that parents experienced increased levels of general and pandemic-related stress, and that parents’ overall COVID-19-specific stress was associated with greater use of non-nutritive feeding behaviors but also with greater efforts to plan and create routines around meals or snacks, and with positive interactions during eating occasions. We additionally found that children’s intake of sweet and savory snacks was associated with snack parenting practices, as well as directly related to the level of parent’s COVID-19 stress.
Our observations relating to stress replicate those of others. Specifically, families in the current sample reported increased general stress compared with before the COVID-19 pandemic (see also Orgilés et al., 2020). Current stress due to COVID-19-specific circumstances was also evident in parents, and captured here by our composite COVID-19 stress measure.
As anticipated, high rates of eating meals together as a family were observed, potentially as a result of increased parental presence in the home due to remote working and childcare responsibilities – 38.4% of our sample reported that they or their partner had to change their work schedule to care for the child themselves. Since family meals have been associated with beneficial effects on child diet (albeit inconsistently, Fink, Racine, Mueffelmann, Dean, & Herman-Smith, 2014), this highlights a possible positive impact of pandemic-associated lockdown. However, it should be noted that while this change may have positive effects for some families, it can also act as a stressor. For example, if children cannot participate in lunches and snack time at school or childcare, these mealtimes now have to be “covered” at home, increasing food costs and time demands on parents.
Notably, the majority of families (>75%) ensured that children had regular breakfast, lunch and/or dinner times, while less regularity was seen for snacks, potentially implying that parents provided snacks at random times or following certain cues (e.g. to manage emotions or as reward for behavior). Ensuring to have regular meals is in line with the ‘structured days hypothesis’ (Brazendale et al., 2017) and recommendations emphasized during the COVID-19 pandemic to establish and keep a routine and structure to children’s days as far as possible (Romero, López-Romero, Domínguez-Álvarez, Villar, & Gómez-Fraguela, 2020; UNICEF, 2020). Along the same lines, mean scores for the structure-related food parenting practices, but also parental modeling of healthy eating, were higher than the coercive practices, with monitoring levels being comparable to previous samples of US parents (Musher-Eizenman, de Lauzon-Guillain, Holub, Leporc, & Charles, 2009). Structure-related practices were unrelated to COVID-19 stress. Together our findings suggest that parents frequently use structure within the meal environment, and these positive practices may be less influenced by COVID-19-related stress compared to other food parenting practices, despite severe disruptions to general schedules and shifts in daily routines during the pandemic.
Differences between pre-school and school-aged children were seen for several food parenting measures. School-aged children were more likely to help prepare foods at mealtimes, likely reflecting their greater autonomy and skills in comparison with pre-school-aged children. As younger children require more guidance, parents of the pre-school-aged group were more likely to eat with their child, provide more structure around meals in general and snacks specifically, and restrict snacks. Additionally, parents in the current study reported higher scores of instrumental feeding and emotion-based snack feeding with this age group, which may reflect the increased risk of behavioral problems observed in preschool children during the pandemic (Romero 2020). Further, use of snacks to reward and soothe was more prevalent in this age group (Blaine 2015). Previous studies have similarly shown less frequent use of restrictive feeding practices (Gray, Janicke, Wistedt, & Dumont-Driscoll, 2010) and use of rewards (Haszard, Williams, Dawson, Skidmore, & Taylor, 2013) for older children.
The positive associations we observed between overall COVID-19-associated stress and emotional and instrumental feeding and restricting snacks are in line with previously demonstrated relationships between “regular stress” and coercive food parenting practices. In our sample, parents reporting high levels of COVID-19-specific stress relied more on practices that were less responsive to their children’s hunger and satiety cues and may be more dependent on the current situation (e.g. conflict resolution). El-Behadli and colleagues (2015) posit that stress effectively interferes with parents’ ability to provide appropriate parenting or feeding. This may also explain why parents reporting higher levels of COVID-19 stress were less likely to provide a variety of healthy foods at meals. Alternatively, parents experiencing higher levels of COVID-19 stress may be more likely to use coercive as well as structure-related food parenting practices to compensate for other areas of their lives where they feel a loss of control or predictability, which has been shown to play a significant role in the experience of perceived stress in the current crisis (Flesia et al., 2020). This may explain why higher COVID-19 stress scores were associated with more snack planning & routine, and snack rules & limits. Due to the disruption of daily life captured by our measure of COVID-19 stress, parents reporting higher stress levels may also have been required to engage more in such food parenting practices, as well as to eat more frequently with the child and engage more frequently with children around mealtime (e.g. teaching about nutrition, cooking/planning meals). Indeed, when comparing the group who had to (and was able to) change their work schedule to care for their child with the 5 other response options listed in Table 1, the former group reported higher stress levels but also engaging with the child around meals more (data not shown). In contrast, before the crisis, these tasks may have been fulfilled by teachers or out-of-home caretakers who provided a structured meal routine, potentially including breakfasts, lunches and snacks. In some cases this obligation may have been a source of pandemic-associated stress for parents, driving the cross-sectional relationships we saw here.
Our analyses of relationships between snack parenting practices and child snack intake frequencies revealed that emotion-based snack feeding was positively associated with children’s intake frequency of ice cream, regular chips, low-fat chips and other salty snacks after adjustment for covariates and simultaneous modeling. While this cross-sectional analysis cannot establish a causal relationship, our results confirm that parents give their children a variety of snack foods to improve their mood and suggest that emotion-based snack feeding may result in a net increase in intake of those foods. In contrast, those parents that reported higher scores on snack rules & limits reported lower child snack intake frequencies. This effect was significant for cookies and low-fat chips, and approached significance for doughnuts and regular chips (p = 0.056 and 0.087), and is consistent with evidence suggesting that structure and monitoring has positive effects on children’s intake (Davison et al., 2018). Finally, snack planning and routine as well as restriction were positively associated with low-fat chip intake frequency. These relationships may reflect parents’ efforts to create a healthy profile of child intake by planning healthier snacks for their child and restricting high-fat foods in favor of lower fat versions. Notably, no previous studies have related snack parenting practices measured with the P-SNAQ to child food intake.
Our conceptual model hypothesized a sequential chain of direct and indirect effects from parental COVID-19 stress and snack parenting on child intake frequency. Findings suggested that the level of COVID-19 stress experienced within families was directly positively associated with child snack intake frequencies of all sweet and savory foods. Interestingly, no relationship between stress and child fruit intake was seen (data not shown), implying that these direct associations may be specific to sweet and savory snack foods, the most common snack foods in the US (Piernas & Popkin, 2010). Two relationships were partially mediated by snack parenting practices. Higher COVID-19 stress was associated with more emotion-based snack feeding, which in turn was related to more frequent child ice cream intake. Higher COVID-19 stress was also associated with using more snack planning and routine, which in turn was related to more frequent low-fat chips intake by the child. Parents’ perceptions and behaviors around low-fat chips should be further investigated in future studies. However, the current result may reflect a phenomenon such that parents experiencing stress associated with pandemic-induced increases in childcare obligations – for example, dealing with children at home while simultaneously working at home – are obliged to exercise more control of snacks, and these parents offer snack options perceived as healthier, in this case low-fat chips. Taken together, our results suggest that parents experiencing high levels of COVID-19 stress implement different snack parenting practices; they use snacks to manage children’s emotions, and they (newly) create a snack schedule and set up a routine. Di Giorgio and colleagues (2020) argue that children need structured and pre-planned days to help them adapt to the new circumstances created by the pandemic. Further, parents have reported COVID-19 pandemic confinement induced boredom in children along with other symptoms such as difficulty concentrating, irritability, restlessness, loneliness, and nervousness (Orgilés et al., 2020). Parents may therefore set snack schedules and routines partly in response to increased boredom and related behavior in children.
On the whole, COVID-19 stress and parental snack practices explained a relatively small amount of variance in intake frequency. Unmeasured factors may contribute to children’s snacking in times of COVID-19, and potentially mediate the effect of stress. One such factor may be the child’s own stress level and related emotional symptoms. Child boredom and stress were shown to increase due to COVID-19 confinement (Ruiz-Roso et al., 2020), as well as difficulties with following daily routines, self-control and self-regulation in 2-5-year-olds (Di Giorgio et al., 2020). Similarly, children’s craving for ‘hyperpalatable comfort foods’ (Gallo, Gallo, Young, Moritz, & Akison, 2020) and emotional eating behaviors may increase within a stressful home environment and thus lead to higher intake of these foods. Consistent with this, maternal and child eating behaviors, besides parental feeding, have previously been suggested as potential pathways linking stress and child nutrition/obesity (El-Behadli et al., 2015). Confinement could lead to frequent snacking and irregular eating behaviors in adolescents due to stress or boredom (Ruiz-Roso et al., 2020) or simply offer more opportunities to snack while being at home (Gallo et al., 2020). Regrettably, Pietrobelli et al. (2020) and an article in the New York Times (Creswell, 2020) reported that homes during lockdown appear to be stocked with ultra-processed and caloric dense foods, hence this obesogenic home food environment may be contributing to overeating and weight gain in children.
Our findings of direct effects of COVID-19-specific stress on child intake are in contrast to some other results reporting effects of general stress. Berge et al. (2018) focused on chronic stress and did not find a significant association with parents serving more desserts to their 5-7-year-olds. Webb (2018) examined the relationship between family stress when children were 3 years of age and found no direct or indirect (via parent-child relationship) associations with consumption of sugary snacks at 5 years. Our results may be different due to the immediate, acute nature of COVID-19 related stress, which may of course turn into chronic stress for some families. Our findings could also be driven by factors unique to the pandemic. For example, our COVID-19 stress measure likely captured the stress associated with removal of many non-food related sources of entertainment in family life, making parents more likely to stock less healthy food in the house for the whole family (increasing availability and accessibility of those foods to children) (Adams, Caccavale, Smith, & Bean, 2020), and more likely to use food as a fun activitiy or ‘treat’ for children – a phenomenon that may not have been captured in our measure of emotion-based snack feeding.
Our results have practical implications. For example, we have shown that COVID-19 stress experienced within the family has direct and indirect associations with higher child snack intake frequency, while others have linked parenting distress assessed during the pandemic with other negative child outcomes (e.g. conduct disorder) (Romero et al. (2020). Increased stress experienced in families during the pandemic is, therefore, of concern for children’s mental as well as physical health and requires intervention. Our results suggest that recommendations for reducing negative quarantine impacts should include evidence-based information to help reduce stress or interrupt the path by which stress leads to non-optimal feeding practices. Others have proposed wide dissemination of stress management programs for parents and children (Domínguez-Álvarez, López-Romero, Isdahl-Troye, Gómez-Fraguela, & Romero, 2020) and implementation of special (psychological) support programs for families, especially targeted to sustain working parents and fostering positive child management (e.g. care and schooling) (Di Giorgio et al., 2020). Recommendations regarding the most suitable food parenting practices in times of a crisis could be added to the UNICEF Coronavirus (COVID-19) parenting tips (Cluver et al., 2020; UNICEF, 2020).
Further research is necessary to quantify the impact of the COVID-19 pandemic on children and their families. It is not clear if the changes reported here and in other research will persist or reverse when lockdowns are removed and children return to school or childcare. Research based on chronic stress suggests that parents might adapt their feeding practices to the ‘new normal’ in response to ongoing stressors or threats (Berge et al., 2018), instead of implementing quick-fixes (e.g. easier meal options) in response to acute stress. The long term impact of COVID-19 on parental feeding practices is yet to be determined, and will likely depend heavily on the duration of the pandemic itself. Research will also need to determine long- as well as short-term effects not only on eating and dietary habits but on body weight, which could additionally be influenced by other behaviors such as sleep, physical activity and screen time.
Our study had strengths and limitations. Data was collected later in the initial lockdown phase which allowed for assessment of variables of interest in relation to pandemic-related stressors that may not have been immediately present, such as unemployment, financial hardship, contracting the virus. Measures of financial strain indicated substantial variation within our sample, supporting generalizability of our results to populations ranging in socioeconomic status. Our sample size allowed application of structural equation modeling. However, data were cross-sectional and based on parental self-report and therefore may be biased by subjective recollection about change compared with pre-COVID-19. Reliance on an online survey method did not allow for verification of data (e.g. respondents actually caring for children in the target age group), and indirectly added ‘having internet access’ to the eligibility criteria. Although financial hardship was present, our sample was weighted towards wealthier, more educated families (mostly college graduates), and the majority of respondents were white. Our findings may be less applicable to racial and ethnic minorities of low SES families living in different geographic regions. Finally, we did not ask families detailed questions about their current as well as pre-COVID-19 childcare arrangements or children’s school attendance. Therefore, we were not able to determine the specific impact of changes in school attendance, for instance, to families’ meal routines. However, 24.5% of our sample reported eating meals together a little more, and 9.7% much more, compared to before the COVID-19 crisis, while 7.6% said that they ate meals together a little/much less.
Limitations notwithstanding, our results suggest that during the first wave of the COVID-19 pandemic, parents experienced increased levels of stress, and this stress was associated with the way they interacted with their children around food. Specifically, parents reporting higher pandemic-associated stress reported more use of food to manage their children’s emotions (coercive) but also more efforts to plan and create routines around meals or snacks (structure), and more positive interactions in terms of eating and engaging with their children around mealtime (autonomy support). Children’s intake of sweet and savory snacks was higher when parents reported greater pandemic-associated stress, and was associated with snack parenting practices. Support and guidance for parents is therefore warranted, to protect children’s nutritional health during the pandemic.
Supplementary Material
Acknowledgments
Funding: This project was funded by Dalio Philanthropies, with additional support from NIH grants R01DK113286, R01DK117623 and UG3OD023313.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of competing interest: None.
Ethical statement
A consent statement was provided to all participants at the beginning of the survey: “Your completion of this survey will serve as your consent to be in this research study.” All methods were approved by the Johns Hopkins University Institutional Review Board (REF NO. CIR00056262).
References
- Adams EL, Caccavale LJ, Smith D, & Bean MK (2020). Food Insecurity, the Home Food Environment, and Parent Feeding Practices in the Era of COVID-19. Obesity, 28(11), 2056–2063. doi: 10.1002/oby.22996 [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychological Association. (2020). Stress in America™ 2020. Stress in the Time of COVID-19, Volume One. Retrieved from https://www.apa.org/news/press/releases/stress/2020/report [Google Scholar]
- Aymerich-Franch L (2020). COVID-19 lockdown: impact on psychological well-being and relationship to habit and routine modifications. PsyArXiv. May 14. doi: 10.31234/osf.io/9vm7r. [DOI] [Google Scholar]
- Bauer KW, MacLehose R, Loth KA, Fisher JO, Larson NI, & Neumark-Sztainer D (2015). Eating- and weight-related parenting of adolescents in the context of food insecurity. J Acad Nutr Diet, 115(9), 1408–1416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berge JM, Tate A, Trofholz A, Fertig A, Crow S, Neumark-Sztainer D, & Miner M (2018). Examining within- and across-day relationships between transient and chronic stress and parent food-related parenting practices in a racially/ethnically diverse and immigrant population : Stress types and food-related parenting practices. Int J Behav Nutr Phys Act, 15(1), 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brazendale K, Beets MW, Weaver RG, Pate RR, Turner-McGrievy GM, Kaczynski AT, … von Hippel PT (2017). Understanding differences between summer vs. school obesogenic behaviors of children: the structured days hypothesis. Int J Behav Nutr Phys Act, 14(1), 100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cluver L, Lachman JM, Sherr L, Wessels I, Krug E, Rakotomalala S, … McDonald K (2020). Parenting in a time of COVID-19. The Lancet, 395(10231), e64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corsini N, Wilson C, Kettler L, & Danthiir V (2010). Development and preliminary validation of the Toddler Snack Food Feeding Questionnaire. Appetite, 54(3), 570–578. [DOI] [PubMed] [Google Scholar]
- Creswell J (2020, April 9, 2020). 'I just need the comfort’: Processed foods make a pandemic comeback. Retrieved from https://www.nytimes.com/2020/04/07/business/coronavirus-processed-foods.html [Google Scholar]
- Damen FWM, Luning PA, Fogliano V, & Steenbekkers BLPA (2019). What influences mothers’ snack choices for their children aged 2–7? Food Quality and Preference, 74, 10–20. [Google Scholar]
- Davison KK, Blake CE, Blaine RE, Younginer NA, Orloski A, Hamtil HA, … Fisher JO (2015). Parenting around child snacking: development of a theoretically-guided, empirically informed conceptual model. Int J Behav Nutr Phys Act, 12, 109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davison KK, Blake CE, Kachurak A, Lumeng JC, Coffman DL, Miller AL, … Fisher JO (2018). Development and preliminary validation of the Parenting around SNAcking Questionnaire (P-SNAQ). Appetite, 125, 323–332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Di Giorgio E, Di Riso D, Mioni G, & Cellini N (2020). The interplay between mothers’ and children behavioral and psychological factors during COVID-19: An Italian study. PsyArXiv. April 30. doi: 10.31234/osf.io/dqk7h. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Domínguez-Álvarez B, López-Romero L, Isdahl-Troye A, Gómez-Fraguela JA, & Romero E (2020). Children Coping, Contextual Risk and their Interplay during the COVID-19 Pandemic: a Spanish Case. PsyArXiv. June 29. doi: 10.31234/osf.io/bt6kr. [DOI] [PMC free article] [PubMed] [Google Scholar]
- El-Behadli AF, Sharp C, Hughes SO, Obasi EM, & Nicklas TA (2015). Maternal depression, stress and feeding styles: towards a framework for theory and research in child obesity. Br J Nutr, 113 Suppl, S55–71. [DOI] [PubMed] [Google Scholar]
- Fegert JM, Vitiello B, Plener PL, & Clemens V (2020). Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: a narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc Psychiatry Ment Health, 14, 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feinberg E, Kavanagh PL, Young RL, & Prudent N (2008). Food insecurity and compensatory feeding practices among urban black families. Pediatrics, 122(4), e854–860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fink SK, Racine EF, Mueffelmann RE, Dean MN, & Herman-Smith R (2014). Family Meals and Diet Quality Among Children and Adolescents in North Carolina. Journal of Nutrition Education and Behavior, 46(5), 418–422. [DOI] [PubMed] [Google Scholar]
- Fisher JO, Wright G, Herman AN, Malhotra K, Serrano EL, Foster GD, & Whitaker RC (2015). "Snacks are not food". Low-income, urban mothers' perceptions of feeding snacks to their preschool-aged children. Appetite, 84, 61–67. [DOI] [PubMed] [Google Scholar]
- Flesia L, Fietta V, Colicino E, Segatto B, & Monaro M (2020). Stable psychological traits predict perceived stress related to the COVID-19 outbreak. PsyArXiv. April 24. doi: 10.31234/osf.io/yb2h8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gallo LA, Gallo TF, Young SL, Moritz KM, & Akison LK (2020). The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students. Nutrients, 12(6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gevers DWM, Kremers SPJ, de Vries NK, & van Assema P (2018). The Comprehensive Snack Parenting Questionnaire (CSPQ): Development and Test-Retest Reliability. Int J Environ Res Public Health, 15(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gouveia MJ, Canavarro MC, & Moreira H (2019). How can mindful parenting be related to emotional eating and overeating in childhood and adolescence? The mediating role of parenting stress and parental child-feeding practices. Appetite, 138, 102–114. [DOI] [PubMed] [Google Scholar]
- Gray WN, Janicke DM, Wistedt KM, & Dumont-Driscoll MC (2010). Factors associated with parental use of restrictive feeding practices to control their children's food intake. Appetite, 55(2), 332–337. doi: 10.1016/j.appet.2010.07.005 [DOI] [PubMed] [Google Scholar]
- Gregório MJ, Rodrigues AM, Eusébio M, Sousa RD, Dias S, André B, … Canhão H (2017). Dietary Patterns Characterized by High Meat Consumption Are Associated with Other Unhealthy Life Styles and Depression Symptoms. Front Nutr, 4, 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gross RS, Mendelsohn AL, Fierman AH, Racine AD, & Messito MJ (2012). Food insecurity and obesogenic maternal infant feeding styles and practices in low-income families. Pediatrics, 130(2), 254–261. [DOI] [PubMed] [Google Scholar]
- Hager ER, Quigg AM, Black MM, Coleman SM, Heeren T, Rose-Jacobs R, … Frank DA (2010). Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics, 126(1), e26–32. [DOI] [PubMed] [Google Scholar]
- Haszard JJ, Williams SM, Dawson AM, Skidmore PM, & Taylor RW (2013). Factor analysis of the Comprehensive Feeding Practices Questionnaire in a large sample of children. Appetite, 62, 110–118. doi: 10.1016/j.appet.2012.11.017 [DOI] [PubMed] [Google Scholar]
- Hu L. t., & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equ Modeling, 6(1), 1–55. [Google Scholar]
- Hurley KM, Black MM, Papas MA, & Caulfield LE (2008). Maternal symptoms of stress, depression, and anxiety are related to nonresponsive feeding styles in a statewide sample of WIC participants. J Nutr, 138(4), 799–805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jansen E, Williams KE, Mallan KM, Nicholson JM, & Daniels LA (2016). The Feeding Practices and Structure Questionnaire (FPSQ-28): A parsimonious version validated for longitudinal use from 2 to 5 years. Appetite, 100, 172–180. [DOI] [PubMed] [Google Scholar]
- Larson N, & Story M (2013). A review of snacking patterns among children and adolescents: what are the implications of snacking for weight status? Child Obes, 9(2), 104–115. [DOI] [PubMed] [Google Scholar]
- Liu JJ, Bao Y, Huang X, Shi J, & Lu L (2020). Mental health considerations for children quarantined because of COVID-19. Lancet Child Adolesc Health, 4(5), 347–349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, & Sheets V (2002). A comparison of methods to test mediation and other intervening variable effects. Psychol Methods, 7(1), 83–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackinnon DP, Lockwood CM, & Williams J (2004). Confidence Limits for the Indirect Effect: Distribution of the Product and Resampling Methods. Multivariate Behav Res, 39(1), 99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minello A (2020). The pandemic and the female academic. Nature. [DOI] [PubMed] [Google Scholar]
- Mitchell S, Brennan L, Hayes L, & Miles CL (2009). Maternal psychosocial predictors of controlling parental feeding styles and practices. Appetite, 53(3), 384–389. [DOI] [PubMed] [Google Scholar]
- Musher-Eizenman DR, de Lauzon-Guillain B, Holub SC, Leporc E, & Charles MA (2009). Child and parent characteristics related to parental feeding practices. A cross-cultural examination in the US and France. Appetite, 52(1), 89–95. doi: 10.1016/j.appet.2008.08.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Musher-Eizenman DR, & Holub S (2007). Comprehensive Feeding Practices Questionnaire: validation of a new measure of parental feeding practices. J Pediatr Psychol, 32(8), 960–972. [DOI] [PubMed] [Google Scholar]
- Muthén L, & Muthén B (1998-2017). Mplus user’s guide, eight edition. Los Angeles, CA: Muthen & Muthen. [Google Scholar]
- Neubauer A, Schmidt A, Kramer A, & Schmiedek F (2020). A Little Autonomy Support Goes a Long Way: Daily Autonomy-Supportive Parenting, Child Well-Being, Parental Need Fulfillment, and Change in Child, Family, and Parent Adjustment Across the Adaptation to the COVID-19 Pandemic. PsyArXiv. May 30. doi: 10.31234/osf.io/t4asz. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neuhouser ML, Lilley S, Lund A, & Johnson DB (2009). Development and validation of a beverage and snack questionnaire for use in evaluation of school nutrition policies. J Am Diet Assoc, 109(9), 1587–1592. [DOI] [PubMed] [Google Scholar]
- NIH National Cancer Institute. (24 July, 2020). Dietary Screener Questionnaires (DSQ) in the NHANES 2009-10: DSQ. Retrieved from https://epi.grants.cancer.gov/nhanes/dietscreen/questionnaires.html#paper
- Orgilés M, Morales A, Delveccio E, Mazzeschi C, & Espada JP (2020). Immediate Psychological Effects of COVID-19 Quarantine in Youth from Italy and Spain. PsyArXiv. April 21. 10.31234/osf.io/5bpfz. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perelman D (2020, July 8, 2020). In the Covid-19 Economy, You Can Have a Kid or a Job. You Can’t Have Both. Retrieved from https://www.nytimes.com/2020/07/02/business/covid-economy-parents-kids-career-homeschooling.html [Google Scholar]
- Piernas C, & Popkin BM (2010). Trends in snacking among U.S. children. Health Aff (Millwood), 29(3), 398–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pietrobelli A, Pecoraro L, Ferruzzi A, Heo M, Faith M, Zoller T, … Heymsfield SB (2020). Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity, 28(8), 1382–1385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preacher KJ, & Hayes AF (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891. [DOI] [PubMed] [Google Scholar]
- Rodgers RF, Paxton SJ, McLean SA, Campbell KJ, Wertheim EH, Skouteris H, & Gibbons K (2014). Maternal negative affect is associated with emotional feeding practices and emotional eating in young children. Appetite, 80, 242–247. [DOI] [PubMed] [Google Scholar]
- Romero E, López-Romero L, Domínguez-Álvarez B, Villar P, & Gómez-Fraguela JA (2020). Testing the effects of COVID-19 confinement in Spanish children: The role of parents’ distress, emotional problems and specific parenting. PsyArXiv. June 24. doi: 10.31234/osf.io/spxtw. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rudy E, Bauer KW, Hughes SO, O'Connor TM, Vollrath K, Davey A, … Fisher JO (2018). Interrelationships of child appetite, weight and snacking among Hispanic preschoolers. Pediatr Obes, 13(1), 38–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruiz-Roso MB, de Carvalho Padilha P, Mantilla-Escalante DC, Ulloa N, Brun P, Acevedo-Correa D, … Dávalos A (2020). Covid-19 Confinement and Changes of Adolescent's Dietary Trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients, 12(6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swyden K, Sisson SB, Morris AS, Lora K, Weedn AE, Copeland KA, & DeGrace B (2017). Association Between Maternal Stress, Work Status, Concern About Child Weight, and Restrictive Feeding Practices in Preschool Children. Matern Child Health J, 21(6), 1349–1357. [DOI] [PubMed] [Google Scholar]
- UNICEF. (2020). Coronavirus (COVID-19) parenting tips: Expert tips to help you deal with COVID-19 parenting challenges. Retrieved from https://www.unicef.org/coronavirus/covid-19-parenting-tips
- Vaughn AE, Ward DS, Fisher JO, Faith MS, Hughes SO, Kremers SP, … Power TG (2016). Fundamental constructs in food parenting practices: a content map to guide future research. Nutr Rev, 74(2), 98–117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ventura AK, & Birch LL (2008). Does parenting affect children's eating and weight status? Int J Behav Nutr Phys Act, 5, 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang G, Zhang Y, Zhao J, Zhang J, & Jiang F (2020). Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet, 395(10228), 945–947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wardle J, Sanderson S, Guthrie CA, Rapoport L, & Plomin R (2002). Parental feeding style and the inter-generational transmission of obesity risk. Obes Res, 10(6), 453–462. [DOI] [PubMed] [Google Scholar]
- Webb HJ, Zimmer-Gembeck MJ, Scuffham PA, Scott R, & Barber B (2018). Family stress predicts poorer dietary quality in children: Examining the role of the parent–child relationship. Infant and Child Development, 27(4), e2088. [Google Scholar]
- Wilkins JL (2020). Challenges and Opportunities Created by the COVID-19 Pandemic. Journal of Nutrition Education and Behavior. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.