

Abstract
Purpose of review:
Liquid biopsies have emerged as a non-invasive alternative to tissue biopsy with potential applications during all stages of pediatric oncology care. The purpose of this review is to provide a survey of pediatric cell-free DNA (cfDNA) studies, illustrate their potential applications in pediatric oncology, and to discuss technological challenges and approaches to overcome these hurdles.
Recent findings:
Recent literature has demonstrated liquid biopsies’ ability to inform treatment selection at diagnosis, monitor clonal evolution during treatment, sensitively detect minimum residual disease following local control and provide sensitive post-therapy surveillance. Advantages include reduced procedural anesthesia, molecular profiling unbiased by tissue heterogeneity, and ability to track clonal evolution. Challenges to wider implementation in pediatric oncology, however, include blood volume restrictions and relatively low mutational burden in childhood cancers. Multi-omic approaches address challenges presented by low-mutational burden and novel bioinformatic analyses allow a single assay to yield increasing amounts of information, reducing blood volume requirements.
Summary:
Liquid biopsies hold tremendous promise in pediatric oncology, enabling non-invasive serial surveillance with adaptive care. Already integrated into adult care, recent advances in technologies and bioinformatics have improved applicability to the pediatric cancer landscape.
Keywords: Liquid biopsy, cfDNA, biomarkers, circulating DNA
Introduction
First identified in 1948, cell-free DNA (cfDNA) has become a promising circulating biomarker in oncology [1,2]. Developments in liquid biopsy, the capture of cfDNA, circulating proteins and circulating tumor cells (CTCs), have led to adoption of technologies across stages of patient management including screening and diagnosis, molecular prognostication, tracking treatment response, detection of minimal residual disease (MRD), monitoring clonal evolution, and post-therapy surveillance [3–7]. The U.S Food and Drug Administration approved the first digital drop polymerase chain reaction (ddPCR) liquid biopsy tests in 2016, and two next generation sequencing (NGS) liquid biopsy panels in 2020 as companion diagnostics for associated targeted therapies [8–10]. As of the time of publication, no liquid biopsy tests have been FDA approved in pediatrics.
Liquid biopsies are of particular interest for pediatric oncology since they are non-invasive, avoiding procedural sedation and enabling serial sampling. Furthermore, liquid biopsies mitigate diagnostic challenges of tumor heterogeneity and accessibility by capturing genetic material shed throughout the body. This promise, however, comes with unique challenges that have limited wider implementation in pediatrics. Pediatric and adult cancers have differing genomic properties; pediatric cancers have low mutational burden [11–14] with few recurrent hotspots [15**–20]. Adult cancers feature more point mutations (single nucleotide variants (SNV)) and insertion/deletion errors (indels), while pediatric cancers are characterized by chromosomal structural variations including copy number alterations (CNA), translocations, and fusion genes [12,14,15**,21–23]. This review highlights studies that illustrate the potential applications of cfDNA in pediatric cancers. We discuss technological challenges and emerging approaches to overcome these hurdles.
cfDNA Overview
cfDNA are ~120–220bp long fragments [24] of double-stranded DNA found in plasma, cerebral spinal fluid (CSF), saliva, pleural fluid, ascites, stool, aqueous humor, and urine [25–28]. cfDNA molecules are released from healthy and malignant cells through apoptosis, necrosis, and secretion, then cleared from circulation with a half-life of several minutes to 2.5 hours [29,30]. cfDNA’s rapid clearance and dynamic changes make it an ideal biomarker for “real-time” analyses compared to classic biomarkers like alpha-fetoprotein (AFP) [31].
cfDNA originating from tumors (circulating tumor DNA; ctDNA) are shorter than normal cfDNA (~90–150bp) [32–34*]. The portion of overall cfDNA comprised of ctDNA varies with cancer type, tumor location, tumor burden, and metastases. In low-burden and early disease, ctDNA fraction is minute [35,36]. The detection of ctDNA therefore requires ultrasensitive methods that detect somatic variations. Thus, a broad understanding of the available technologies and evaluation of these considerations is necessary when selecting an approach for analyzing cfDNA.
Technologies
PCR
Polymerase chain reactions (PCR) specifically amplify targeted cfDNA templates. To improve sensitivity and amplify a minute quantity of ctDNA, ddPCR technology subdivides PCR reactions into numerous nano-liter droplets, and can detect variant allele fractions (VAF) as low as 0.001% [7,37]. Although ddPCR attains high sensitivities, it has limitations. First, it requires a priori knowledge of disease- or patient-specific mutations [37], thereby missing any de novo mutations. Similarly, genome-wide surveys of translocations, indels, and CNA are limited given the focused nature of the assay.
NGS
NGS methods do not require prior knowledge of mutations, but have worse limits of detection than ddPCR and increased cost. The primary parameters affecting cost are breadth and depth of sequencing. Breadth is the proportion of the genome that is sequenced. NGS breadth varies from a panel of genes of interest (e.g., CAPPseq [38]), to regions of the genome (e.g., whole exome sequencing (WES)), to the entire genome (whole genome sequencing (WGS)). This gives NGS the capacity to detect both recurrent hotspot mutations and previously unknown or uncommon variants.
Depth refers to the average number of times a base pair is sequenced. Shallow WGS (e.g., 0.1–2x ultra-low pass WGS (ULP-WGS)) accurately detects CNAs [39] at low cost but has poor sensitivity for specific somatic variants. As depth increases, SNVs, indels, and translocations may be identified. However, since assay cost increases, deep-sequencing panels typically restrict breadth, focusing on smaller genomic regions and missing abnormalities outside of those regions.
Methylation, Fragmentomics, and Transcriptomics
While previous methods identify genetic variations to characterize ctDNA, recent techniques leverage other ctDNA signatures. Pediatric cancer’s low mutational burden may be better suited to alternative markers or combinatorial approaches. Methylation, for example, is a promising pediatric marker since epigenetic dysregulation is a recurrent characteristic of childhood cancers [40]. The circulating methylome can be measured in targeted cfMeDIP-seq [41] or ddMethyLight assays [42] as well as genome-wide approaches [43]. Methylation fingerprints may also define cfDNA tissues of origin [44,45]. Emerging bioinformatic techniques, such as fragmentomics and transcriptomics, leverage non-random differences in cfDNA fragments and sequence coverage for in silico enrichment of ctDNA [33,34*,46], and infer transcriptome profiles based on chromatin availability and nucleosome footprints [47–51**].
Clinical Applications of Liquid Biopsies
The diversity of assays available to profile cfDNA is matched by the range of potential applications for these tools in the clinic (Fig. 1).
Figure 1. Clinical applications of liquid biopsy in pediatric oncology.
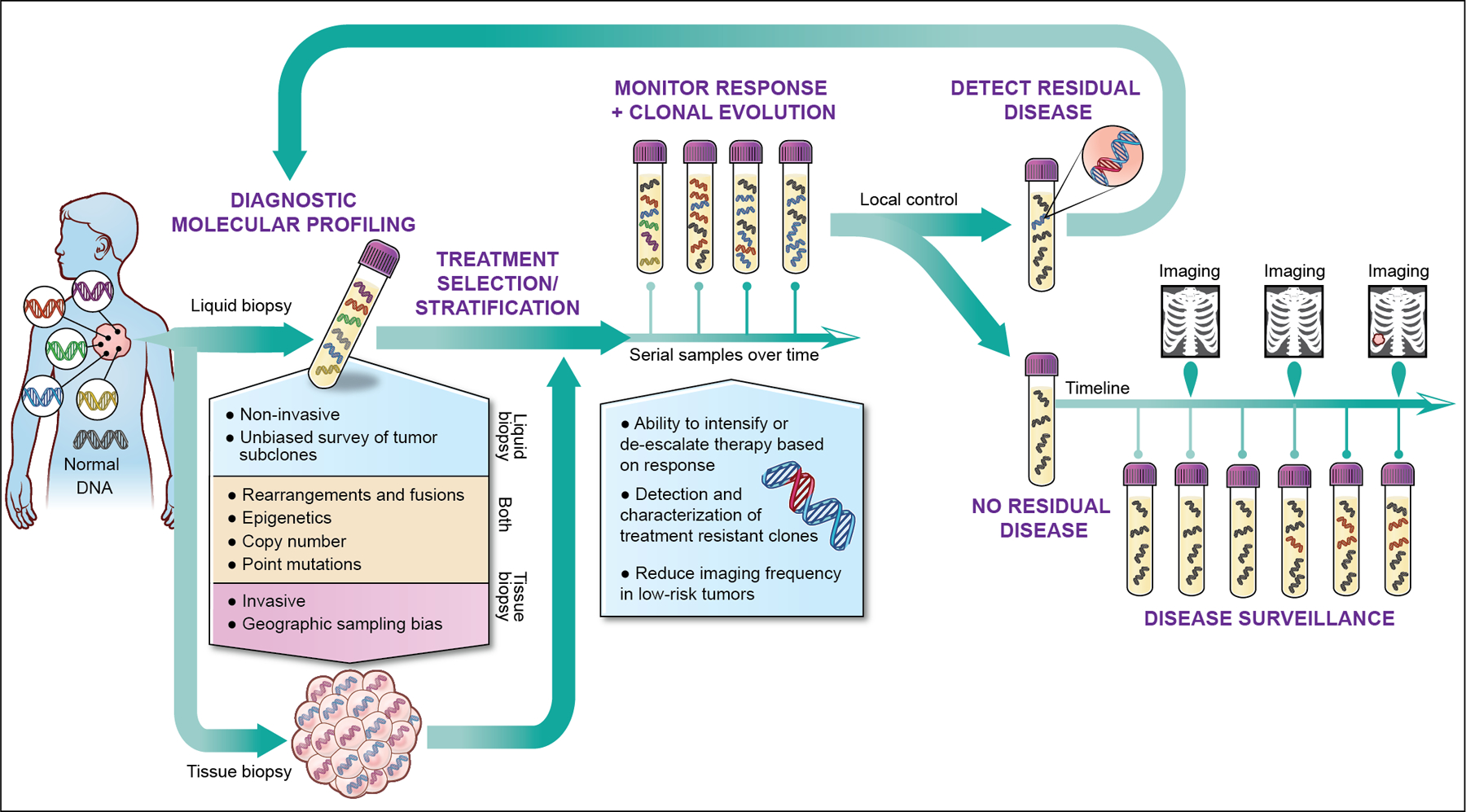
Liquid biopsies capture genetic material shed throughout the body, enabling non-invasive molecular profiling without the confounding variable of tumor heterogeneity. Liquid biopsies can therefore inform care and treatment selection at diagnosis, monitor clonal evolution during treatment, sensitively detect minimum residual disease following local control and provide sensitive post-therapy surveillance. Multiple studies have demonstrated that liquid biopsies have the potential to detect relapsed disease before radiographically evident.
Molecular Profiling and Treatment Selection
Sequencing from multiple regions of the same tumor reveals significant intratumor genetic heterogeneity [52,53]. Up to 69% of detected somatic mutations are absent from other regions of the same tumor [52], leading to potential sampling biases during biopsy. Liquid biopsy of cfDNA captures genetic materials released from multiple tissue regions and separate disease foci, mitigating sampling biases. Current adult clinical trials employ cfDNA for risk stratification and treatment selection [7,54].
Liquid biopsy could similarly be used to inform management of pediatric cancers, guiding treatment intensification and de-escalation. Intra- and interlesional heterogeneity of MYCN and ALK, for example, is well described in neuroblastoma [55,56]. Accurate assessment of MYCN, ALK, and segmental chromosome alterations (SCA), has prognostic implications [57–59] and is incorporated into treatment selection. Intermediate-risk neuroblastoma patients without MYCN amplification or specific SCA maintain excellent outcomes with treatment reduction [60]; therefore, genomic misclassification would lead to inappropriate de-escalation of treatment. Multiple studies demonstrate sensitive and tissue concordant molecular characterization of these genes and SCA in neuroblastoma using liquid biopsies [61–65]. The promise of liquid biopsy for risk stratification is further illustrated in pediatric sarcomas. In Ewing sarcoma (EWS) and osteosarcoma, the presence of detectable ctDNA alone predicts inferior outcomes. Furthermore, 8q gain in osteosarcoma cfDNA portended poorer 3-year event-free survival (EFS) (60% vs 80.9%) [66], and EWS high-risk co-mutations of STAG and TP53 [67] are detectable in cfDNA [68].
Implementation of liquid biopsy for genomic characterization of Wilms tumor could reconcile international treatment paradigms. European consortium paradigms recommend neoadjuvant chemotherapy without tissue diagnosis due to the prevalence of favorable disease and risk of metastatic seeding with biopsy or surgery. In contrast, North American algorithms recommend upfront nephrectomy for biology-guided therapy. In small studies, TP53 mutations were detectable in 100% of pre-nephrectomy urine cfDNA [69] and tumor-confirmed mutations were identified in plasma [70]. cfDNA profiles of poor prognosis TP53 mutations [71,72] and 1p/16q alterations [70], therefore, could guide therapy without risking seeding tumor.
Treatment Response and Clonal Evolution
While mortality from primary pediatric cancers has decreased, intensification of treatments has led to increased treatment-related morbidity [73]. Clinical trials, therefore, have examined response-adapted protocols that reduce long-term morbidities in hematologic malignancies [74–76]. In pediatric solid tumors, response-adapted therapy is hindered by lack of serial biopsies; response markers are limited to imaging [77] and necrosis estimates on post-neoadjuvant resections [78]. Liquid biopsies offer non-invasive, serial monitoring to assess tumor burden, clonal evolution, and epigenetic changes.
In a small osteosarcoma cohort, patients with >80% necrosis in resections had undetectable ctDNA following initiation of neoadjuvant therapy. Patients with less than 70% necrosis, however, had persistence of ctDNA throughout therapy [64]. Although larger validation studies are needed, these data suggest that ctDNA may predict prognostic post-neoadjuvent percent necrosis in osteosarcoma [78]. Similarly, dynamic changes in ctDNA have been shown to correlate with tumor burden in Wilms tumor [79], hepatoblastoma [80], retinoblastoma [81–83], EWS [51**,77,84] and neuroblastoma [61,62]. Additionally, circulating epigenetic signatures approximate tumor burden and response. Data suggest that regional differences in coverage over DNase I hypersensitive sites (DHSs), a surrogate for chromatin status and epigenetic signatures [49,51**], infer tissue type and can estimate tumor burden [51**]. Applebaum et al. measured epigenetic signatures using 5-hydroxymethylcytosine (5-hmC) to predict disease burden and response in metastatic neuroblastoma. 5hmC deposition on MYCN predicted relapse and end of induction total 5-hmC levels are prognostic. In two patients with no clinical evidence of disease, 5hmC profiling predicted subsequent relapse [85*].
Finally, serial cfDNA can monitor clonal evolution and identify therapy-resistant subclones. A landmark study in lung cancer reported that cfDNA is more sensitive than tissue biopsy for detection of acquired resistance to erlotinib through EGFRT790M mutations [86]. In pediatrics, cfDNA temporally resolved heterogeneity in progressive neuroblastoma with a mean of 22 new SNV between diagnostic and subsequent samples, including 17 commonly acquired relapse-specific mutations [61]. Similarly, Barris et al identified TP53 mutations in relapsed osteosarcoma plasma not identified in initial tumor or germline [87]. In medulloblastoma, dynamic changes in CSF cfDNA methylation mirror tissue changes during treatment and progression [43].
Detection of Minimum Residual Disease and Post Therapy Surveillance
cfDNA’s short half-life [29,30] and representation of spatial heterogeneity [88] make it an ideal biomarker to detect post-operative minimum residual disease (MRD) and early recurrence. In adults, post-operative persistence of ctDNA portends a >80% risk of relapse in colorectal cancers [89] and urothelial carcinomas [90]. These findings suggest that ctDNA positivity post-neoadjuvent therapy or surgery could inform clinical decisions regarding follow-up frequency and need for adjuvant or radiation therapy. Indeed, the addition of immunotherapy to urothelial carcinoma patients with post-operative ctDNA improved disease-free survival and overall survival [90]. Furthermore, application of cfDNA for MRD may enable earlier relapse detection. In lung cancer, recurrence of detectable ctDNA identified relapse a median of 5.2 months earlier than imaging [91]; in colon and breast cancer, cfDNA outperforms biochemical biomarkers CEA and CA 15–3 for early, sensitive detection of recurrence [92,93].
To date, there have been no large MRD pediatric studies using cfDNA; however, case series demonstrate feasibility. Hayashi et al, used tumor-informed EWS-ETS ddPCR to detect fusion genes in plasma from three EWS patients. Two patients had persistent post-operative ctDNA and clinically relapsed. The only ctDNA negative patient remained in remission [84]. In osteosarcoma, three of seven patients followed with targeted NGS liquid biopsy relapsed, all of whom had recurrence of detectable ctDNA prior to radiographic relapse [87]. Circulating mutant Rb1 becomes undetectable following enucleation of intraocular retinoblastoma [94,95] but was again detectable in regionally recurrent or metastatic relapsed disease [83]. Finally, previously detectable circulating CTNNB1 in hepatoblastoma becomes undetectable following total resection with no histological or radiographic evidence of residual disease [80].
Challenges and Future Directions
Rapid technological advances coupled with exciting preliminary studies in pediatric histologies portend an important future for cfDNA in pediatric oncology, however several important considerations must be considered in this population.
Blood draw limitations
An assay’s limit of detection is constrained by the number of unique sequencing reads generated. Each milliliter of blood has approximately 1,000 genome equivalents (GE) [96] and sequencing to a depth greater than unique GE results in duplicated reads with no improvement in limits of detection [97**]. Theoretically, this presents a barrier in pediatrics due to weight-based limits in blood draw volume. Kahana-Edwin et al., however, highlight that the percentage of total blood volume collected during weight-based draws in pediatrics is consistent with adults. Furthermore, even early-stage pediatric cancers often represent a larger tumor burden relative to patient size than adult counterparts. Taken together, pediatric assays should capture a proportional or higher ratio of ctDNA:cfDNA due to relative tumor burden in similarly staged diseases [98]. Indeed, pediatric studies in neuroblastoma [65,99], EWS [66] and hepatoblastoma [80] have demonstrated the feasibility of sensitive detection from less than 1mL of plasma, and studies of unilateral intraocular retinoblastoma, characterized by exceptionally small tumor volumes, detect ctDNA in plasma [83,100].
Clonal hematopoiesis of indeterminate potential
An emerging challenge in liquid biopsies is false positives due to somatic mutations present in peripheral blood but not in tumor, termed clonal hematopoiesis of indeterminate potential (CHIP) [101]. A common phenomenon associated with aging, CHIP is the presence of a mutant clone in the blood without evidence of dysplasia, neoplasm or cytopenia [102]. CHIP are attributed to survival advantages in certain mutations acquired during normal hematopoietic stem cell (HSC) divisions [103]. Studies of serial samples banked 10 years apart suggest that CHIP rarely undergo continued expansion [104] and have minimal risk of transforming into hematologic malignancy [105,106].
CHIP are classically defined as having a VAF of ≥2% [102–105,107], however, this threshold is based on previous limits of detection using WES [105]. Recent studies using error suppression algorithms suggest that CHIP accumulation likely begins in fetal development. 18.2% of sequenced cord blood samples harbor low frequency (VAF 0.002–0.006) somatic mutations [108] and, during normal hematopoiesis, individuals gain one mutation in HSCs per decade [103,109]. It is hypothesized, however, that these mutations do not confer survival advantages in youth [110] and, consequently, VAF of CHIP typically remains <0.5% until age 50 [107,111]. The VAF of CHIP in pediatrics, therefore, remains undetectable by many liquid biopsy assays [7,39]. As technologies continue to push limits of detection in an effort to identify early-stage cancer, low-VAF CHIP may become a relevant source of false-positives in pediatric oncology. Multi-omic or combinatorial imaging-cfDNA assays may mitigate this.
CHIP frequency increases in adults who received chemotherapy [105,112,113] and radiation therapy [105,113]. These CHIP are enriched for TP53 mutations [113], the most common somatically mutated gene in pediatric cancer [13], presenting a potential source of false positives in post-therapy surveillance and MRD detection. The only study examining CHIP in pediatric cancer survivors, however, showed no increases using a 14-gene NGS panel [110]. Larger, longitudinal studies including broader panels or WGS with error suppression are necessary for validation.
Low mutational burden
With early-stage disease, increasing the number of targeted mutations improves probability of detection [5]. Pediatric cancers, however, have approximately one-fourteenth of the mutation burden of adult cancers [13], with as few as one SNV per exome [12], limiting targeted panels’ utility in early-stage detection.
One strategy to improve probability of detection is to expand assayed targets by integrating “multi-omic” features including CNA [32,34*,51**], fragmentation profiles [32–34*,46,51**], protein [114–116] and epigenetics [51**]. CNA are the most common alteration in pediatric solid tumors [13,15**,22] and may be inferred from off-target reads of targeted panels [117] or detected using ULP-WGS [34*,39,81]. The utility of cfDNA CNA as a biomarker has been shown in neuroblastoma [61,62,65], retinoblastoma [81,82], and EWS [64], and the sensitivity of these assays can be boosted with fragmentomics [32–34*,46]. Our group reported that CNA combined with fragment size analysis not only detects malignancy, but can accurately distinguish benign from malignant tumors in neurofibromatosis type 1 (NF1) [34*]. For small tumors, combinatorial assays with cfDNA and protein have doubled sensitivity in Stage I/II pancreatic cancers and lesions measuring <1.5cm [115]. Furthermore, pediatric cancers have a high incidence of mutations in epigenetic regulators [13,15**,118]. Integrating epigenetic and genetic signatures enabled accurate classification of sarcoma types [51**]. Finally, combinatorial approaches may not be multi-omic but multi-modality. Using a pan-cancer liquid biopsy for surveillance, Lennon et al. increased their positive predictive value by 45% after integrating imaging features [119].
Conclusions
Liquid biopsies have emerged as a non-invasive alternative to tissue biopsy. Despite the potential to allow serial molecular profiling while reducing invasive procedures and anesthesia events, implementation in pediatrics has been limited and liquid biopsy remains only a research tool. This is partly due to challenges presented by relatively low mutational burden. Multi-omic strategies show promise for sensitive detection of low mutational burden disease, but are expensive and require more blood for parallel assays. Exciting recent studies demonstrate that bioinformatic processing of 12x-35x WGS enables characterization of copy number analysis, small indels, fusions, chromatin accessibility, and detailed fragmentomics from a single assay (Fig. 2) [51**,97**]. These novel approaches offer tremendous promise for childhood cancer by detecting the most common pediatric alterations in childhood cancers, incorporating multi-omic input, and reducing required blood and cost.
Figure 2. Moderate depth WGS improve detection by enabling multi-omic integration from a single assay.
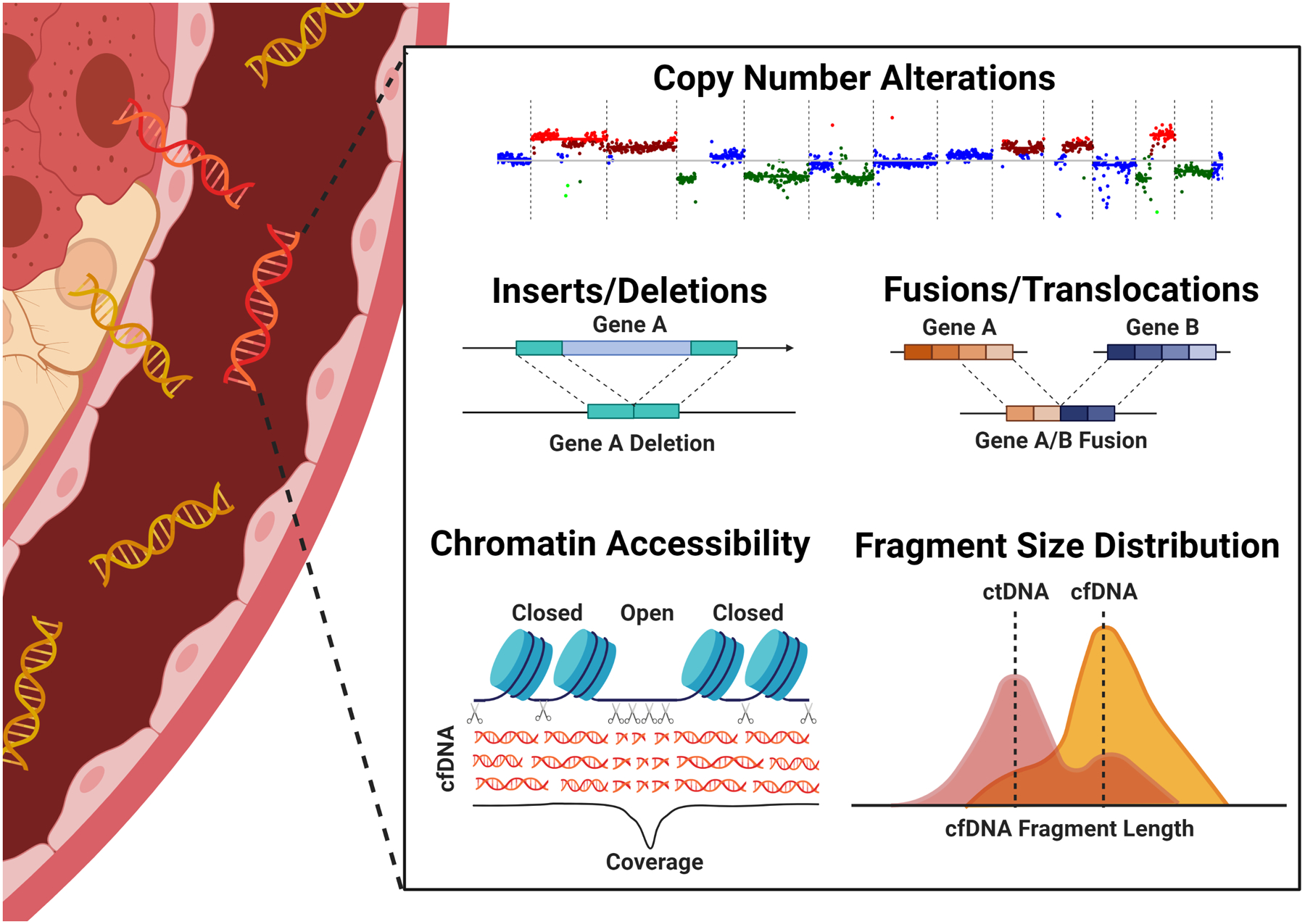
Recent studies have demonstrated that, with advanced bioinformatic analysis, WGS to depths of 12–35x is sufficient for detection of copy number alterations, indels, translocations and fusions, assessment of chromatin accessibility and fragmentomics [51**,97**]. In addition to detecting the most common genomic alterations in childhood cancer, therefore, integration of these output also infers epigenetic and transcriptomic signatures. Combinatorial approaches, previously requiring multiple assays, enhance detection of early stage cancers. Created with BioRender.com.
Key points:
Liquid biopsies non-invasively capture cfDNA and circulating biomarkers shed from cancerous and healthy cells.
Liquid biopsies enable accurate molecular diagnostics and prognostication, tracking treatment response, detection of MRD, monitoring clonal evolution, and post-therapy surveillance.
Multi-omic liquid biopsies hold promise for the overcoming the low-mutational burden challenge in pediatric cancers.
Acknowledgements:
NIH Medical Arts created Figure 1. Images from BioRender were used to create Figure 2.
Financial support and sponsorship
None.
Abbreviations:
- 5-hmC
5-Hydroxymethylcytosine
- AFP
alpha-fetoprotein
- CSF
cerebral spinal fluid
- cfDNA
cell-free DNA
- CHIP
clonal hematopoiesis of indeterminate significance (CHIP)
- CTC
circulating tumor cells
- CNA
copy number alterations
- ctDNA
circulating tumor DNA
- ddPCR
digital drop polymerase chain reaction
- DHSs
DNase I hypersensitive site
- EWS
Ewing sarcoma
- GE
genome equivalents
- HSCs
hematopoietic stem cells
- indel
insertion and deletion error
- MRD
minimum residual disease
- NGS
next generation sequencing
- NF1
neurofibromatosis type 1
- PCR
polymerase chain reaction
- SCA
segmental chromosome alterations
- SNV
single nucleotide variant
- ULP-WGS
ultra low pass whole genome sequencing
- WES
whole exome sequencing
- WGS
whole genome sequencing
- VAF
variant allele frequency
Footnotes
Conflicts of interest
There are no conflicts of interest.
References
- 1.Mandel P, Metais P. [Nuclear Acids In Human Blood Plasma]. C R Seances Soc Biol Fil. 1948. February;142(3–4):241–3. [PubMed] [Google Scholar]
- 2.Stroun M, Anker P, Lyautey J, Lederrey C, Maurice PA. Isolation and characterization of DNA from the plasma of cancer patients. Eur J Cancer Clin Oncol. 1987;23(6):707–12. [DOI] [PubMed] [Google Scholar]
- 3.Abbou SD, Shulman DS, DuBois SG, Crompton BD. Assessment of circulating tumor DNA in pediatric solid tumors: The promise of liquid biopsies. Pediatr Blood Cancer. 2019;66(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Andersson D, Fagman H, Dalin MG, Ståhlberg A. Circulating cell-free tumor DNA analysis in pediatric cancers. Mol Aspects Med. 2020;72(August 2019):100819. [DOI] [PubMed] [Google Scholar]
- 5.Wan J Liquid biopsies come of age: towards implementation of circulating tumour DNA. Nat Rev Cancer. 2017;17:223–38. [DOI] [PubMed] [Google Scholar]
- 6.Merker JD, Oxnard GR, Compton C, Diehn M, Hurley P, Lazar AJ, et al. Circulating Tumor DNA Analysis in Patients With Cancer: American Society of Clinical Oncology and College of American Pathologists Joint Review. J Clin Oncol Off J Am Soc Clin Oncol. 2018. June;36(16):1631–41. [DOI] [PubMed] [Google Scholar]
- 7.Corcoran RB, Chabner BA. Application of Cell-free DNA Analysis to Cancer Treatment. N Engl J Med. 2018. November;379(18):1754–65. [DOI] [PubMed] [Google Scholar]
- 8.U.S. Food and Drug Administration. cobas EGFR Mutation Test v2 [Internet]. fda.gov. 2016. [cited 2021 Aug 28]. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/cobas-egfr-mutation-test-v2
- 9.U.S. Food and Drug Administration. FDA Approves First Liquid Biopsy Next-Generation Sequencing Companion Diagnostic Test [Internet]. fda.gov. 2020. [cited 2021 Aug 28]. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-first-liquid-biopsy-next-generation-sequencing-companion-diagnostic-test
- 10.U.S. Food and Drug Administration. FDA approves liquid biopsy NGS companion diagnostic test for multiple cancers and biomarkers [Internet]. fda.gov. 2020. [cited 2021 Aug 28]. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-liquid-biopsy-ngs-companion-diagnostic-test-multiple-cancers-and-biomarkers
- 11.Vogelstein B, Papadopoulos N, Velculescu VE, Zhou S, Diaz LA, Kinzler KW. Cancer Genome Landscapes. Science (80-). 2013. March;339(6127):1546–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lawrence MS, Stojanov P, Polak P, Kryukov GV, Cibulskis K, Sivachenko A, et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nat 2013 4997457. 2013. June 16;499(7457):214–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gröbner SN, Worst BC, Weischenfeldt J, Buchhalter I, Kleinheinz K, Rudneva VA, et al. The landscape of genomic alterations across childhood cancers. Nature. 2018. March 15;555(7696):321–7. [DOI] [PubMed] [Google Scholar]
- 14.Campbell BB, Light N, Fabrizio D, Zatzman M, Fuligni F, de Borja R, et al. Comprehensive Analysis of Hypermutation in Human Cancer. Cell. 2017. November;171(5):1042–1056.e10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- **15.Newman S, Nakitandwe J, Kesserwan CA, Azzato EM, Wheeler DA, Rusch M, et al. Genomes for Kids: The scope of pathogenic mutations in pediatric cancer revealed by comprehensive DNA and RNA sequencing. Cancer Discov. 2021;candisc.1631.2020. [DOI] [PMC free article] [PubMed] [Google Scholar]; This study use a multi-omic approach (WGS, WES, RNAseq) to examine tumor and germline from pediatric cancers. The authors demonstrated that, in tissue, combinatorial approaches are necessary to identify the full range of genomic variants in childhood cancer.
- 16.Kaseb AO, Sánchez NS, Sen S, Kelley RK, Tan B, Bocobo AG, et al. Molecular Profiling of Hepatocellular Carcinoma Using Circulating Cell-Free DNA. Clin Cancer Res. 2019. October;25(20):6107 LP–6118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sacher AG, Paweletz C, Dahlberg SE, Alden RS, O’Connell A, Feeney N, et al. Prospective Validation of Rapid Plasma Genotyping for the Detection of EGFR and KRAS Mutations in Advanced Lung Cancer. JAMA Oncol. 2016. August;2(8):1014–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jenkins S, Yang JC-H, Ramalingam SS, Yu K, Patel S, Weston S, et al. Plasma ctDNA Analysis for Detection of the EGFR T790M Mutation in Patients with Advanced Non-Small Cell Lung Cancer. J Thorac Oncol Off Publ Int Assoc Study Lung Cancer. 2017. July;12(7):1061–70. [DOI] [PubMed] [Google Scholar]
- 19.Sanmamed MF, Fernández-Landázuri S, Rodríguez C, Zárate R, Lozano MD, Zubiri L, et al. Quantitative Cell-Free Circulating BRAFV600E Mutation Analysis by Use of Droplet Digital PCR in the Follow-up of Patients with Melanoma Being Treated with BRAF Inhibitors. Clin Chem. 2015. January;61(1):297–304. [DOI] [PubMed] [Google Scholar]
- 20.Schmiegel W, Scott RJ, Dooley S, Lewis W, Meldrum CJ, Pockney P, et al. Blood-based detection of RAS mutations to guide anti-EGFR therapy in colorectal cancer patients: concordance of results from circulating tumor DNA and tissue-based RAS testing. Mol Oncol. 2017. February;11(2):208–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kandoth C, McLellan MD, Vandin F, Ye K, Niu B, Lu C, et al. Mutational landscape and significance across 12 major cancer types. Nature. 2013. October;502(7471):333–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ma X, Liu Y, Liu Y, Alexandrov LB, Edmonson MN, Gawad C, et al. Pan-cancer genome and transcriptome analyses of 1,699 paediatric leukaemias and solid tumours. Nat 2018 5557696. 2018. February 28;555(7696):371–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sweet-Cordero EA, Biegel JA. The genomic landscape of pediatric cancers: Implications for diagnosis and treatment. Science (80-). 2019. March;363(6432):1170–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Alcaide M, Cheung M, Hillman J, Rassekh SR, Deyell RJ, Batist G, et al. Evaluating the quantity, quality and size distribution of cell-free DNA by multiplex droplet digital PCR. Sci Rep. 2020. December;10(1):12564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Siravegna G, Marsoni S, Siena S, Bardelli A. Integrating liquid biopsies into the management of cancer. Nat Rev Clin Oncol. 2017. September;14(9):531–48. [DOI] [PubMed] [Google Scholar]
- 26.Husain H, Melnikova VO, Kosco K, Woodward B, More S, Pingle SC, et al. Monitoring Daily Dynamics of Early Tumor Response to Targeted Therapy by Detecting Circulating Tumor DNA in Urine. Clin Cancer Res. 2017. August;23(16):4716–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wang Y, Springer S, Mulvey CL, Silliman N, Schaefer J, Sausen M, et al. Detection of somatic mutations and HPV in the saliva and plasma of patients with head and neck squamous cell carcinomas. Sci Transl Med. 2015. June;7(293):293ra104–293ra104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.De Mattos-Arruda L, Mayor R, Ng CKY, Weigelt B, Martínez-Ricarte F, Torrejon D, et al. Cerebrospinal fluid-derived circulating tumour DNA better represents the genomic alterations of brain tumours than plasma. Nat Commun. 2015. December;6(1):8839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Yao W, Mei C, Nan X, Hui L. Evaluation and comparison of in vitro degradation kinetics of DNA in serum, urine and saliva: A qualitative study. Gene. 2016. September 15;590(1):142–8. [DOI] [PubMed] [Google Scholar]
- 30.Lo YMD, Zhang J, Leung TN, Lau TK, Chang AMZ, Hjelm NM. Rapid Clearance of Fetal DNA from Maternal Plasma. Am J Hum Genet. 1999. January;64(1):218–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Shim JH, Han S, Lee YJ, Lee SG, Kim KM, Lim YS, et al. Half-life of serum alpha-fetoprotein: An early prognostic index of recurrence and survival after hepatic resection for hepatocellular carcinoma. Ann Surg. 2013. April;257(4):708–17. [DOI] [PubMed] [Google Scholar]
- 32.Mouliere F, Mair R, Chandrananda D, Marass F, Smith CG, Su J, et al. Detection of cell‐free DNA fragmentation and copy number alterations in cerebrospinal fluid from glioma patients. EMBO Mol Med. 2018. December 6;10(12). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mouliere F, Chandrananda D, Piskorz AMA, Moore EEK, Morris J, Ahlborn LBL, et al. Enhanced detection of circulating tumor DNA by fragment size analysis. Sci Transl Med. 2018. November 7;10(466):eaat4921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *34.Szymanski JJ, Sundby RT, Jones PA, Srihari D, Earland N, Harris PK, et al. Cell-free DNA ultra-low-pass whole genome sequencing to distinguish malignant peripheral nerve sheath tumor (MPNST) from its benign precursor lesion: A cross-sectional study. PLOS Med. 2021;18(8):e1003734. [DOI] [PMC free article] [PubMed] [Google Scholar]; This is the first study use cfDNA to identify malignancy in a cancer predisposition syndrome. Copy number analysis with fragmentomics distinguished benign from malignant tumors and cfDNA profiles recapitulated characteristic tissue genomic alterations.
- 35.Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, et al. Circulating mutant DNA to assess tumor dynamics. Nat Med. 2008. September;14(9):985–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bettegowda C, Sausen M, Leary RJ, Kinde I, Wang Y, Agrawal N, et al. Detection of Circulating Tumor DNA in Early- and Late-Stage Human Malignancies. Sci Transl Med. 2014. February;6(224):224ra24–224ra24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kockerols CCB, Valk PJM, Levin M-D, Pallisgaard N, Cornelissen JJ, Westerweel PE. Digital PCR for BCR-ABL1 Quantification in CML: Current Applications in Clinical Practice. HemaSphere. 2020. December;4(6):e496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Newman AM, Bratman SV, To J, Wynne JF, Eclov NCW, Modlin LA, et al. An ultrasensitive method for quantitating circulating tumor DNA with broad patient coverage. Nat Med. 2014. May;20(5):548–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Adalsteinsson VAV, Ha G, Freeman SS, Choudhury AD, Stover DG, Parsons HA, et al. Scalable whole-exome sequencing of cell-free DNA reveals high concordance with metastatic tumors. Nat Commun. 2017. December 6;8(1):1324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Filbin M, Monje M. Developmental origins and emerging therapeutic opportunities for childhood cancer. Nat Med. 2019. March 6;25(3):367–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Shen SY, Singhania R, Fehringer G, Chakravarthy A, Roehrl MHA, Chadwick D, et al. Sensitive tumour detection and classification using plasma cell-free DNA methylomes. Nature. 2018. November 14;563(7732):579–83. [DOI] [PubMed] [Google Scholar]
- 42.Cho N-Y, Park J-W, Wen X, Shin Y-J, Kang J-K, Song S-H, et al. Blood-Based Detection of Colorectal Cancer Using Cancer-Specific DNA Methylation Markers. Diagnostics 2021, Vol 11, Page 51. 2020. December 31;11(1):51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Li J, Zhao S, Lee M, Yin Y, Li J, Zhou Y, et al. Reliable tumor detection by whole-genome methylation sequencing of cell-free DNA in cerebrospinal fluid of pediatric medulloblastoma. Sci Adv. 2020. October 1;6(42):5427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sun K, Jiang P, Chan KCA, Wong J, Cheng YKY, Liang RHS, et al. Plasma DNA tissue mapping by genome-wide methylation sequencing for noninvasive prenatal, cancer, and transplantation assessments. Proc Natl Acad Sci. 2015. October 6;112(40):E5503–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Gai W, Zhou Z, Agbor-Enoh S, Fan X, Lian S, Jiang P, et al. Applications of genetic-epigenetic tissue mapping for plasma dna in prenatal testing, transplantation and oncology. Elife. 2021. March 1;10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Cristiano S, Leal A, Phallen J, Fiksel J, Adleff V, Bruhm DC, et al. Genome-wide cell-free DNA fragmentation in patients with cancer. Nature. 2019. June 29;570(7761):385–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Lo YMD, Han DSC, Jiang P, Chiu RWK. Epigenetics, fragmentomics, and topology of cell-free DNA in liquid biopsies. Science (80-). 2021. April 9;372(6538). [DOI] [PubMed] [Google Scholar]
- 48.Jiang P, Sun K, Tong Y, Cheng S, Cheng T, Heung M. Preferred end coordinates and somatic variants as signatures of circulating tumor DNA associated with hepatocellular carcinoma. Proc Natl Acad Sci U S A. 2018. November 13;115(46):E10925–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Sun K, Jiang P, Cheng S, Cheng T, Wong J, Wong V. Orientation-aware plasma cell-free DNA fragmentation analysis in open chromatin regions informs tissue of origin. Genome Res. 2019. March 1;29(3):418–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ivanov M, Baranova A, Butler T, Spellman P, Mileyko V. Non-random fragmentation patterns in circulating cell-free DNA reflect epigenetic regulation. BMC Genomics. 2015. June 18;16(8):S1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- **51.Peneder P, Stütz AM, Surdez D, Krumbholz M, Semper S, Chicard M, et al. Multimodal analysis of cell-free DNA whole-genome sequencing for pediatric cancers with low mutational burden. Nat Commun. 2021. December 28;12(1):3230. [DOI] [PMC free article] [PubMed] [Google Scholar]; In this study, the authors demonstrate that modest-depth WGS is sufficient to describe cancer-specific chromatin signatures using the novel LIQUORICE alogirthm. Advanced fragmentomic analyses are introduced for classification of low mutation burden cancers. Finally, the authors use ingetgrated genetic/epigenetic analysis to sensitively detect and distinguish between various pediatric sarcomas.
- 52.Gerlinger M, Rowan A, Horswell S, Larkin J, Endesfelder D, Gronroos E. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med. 2012. March 8;366(10):883–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Swanton C Intratumor heterogeneity: evolution through space and time. Cancer Res. 2012. October 1;72(19):4875–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Tie J, Chapman M. Circulating tumour DNA (ctDNA) analysis informing adjuvant chemotherapy in Stage II Colon Cancer [Internet]. Australian New Zealand Clinical Trials Registry. [cited 2021 Sep 8]. Available from: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12615000381583
- 55.Bellini A, Bernard V, Leroy Q, Frio TR, Pierron G, Combaret V, et al. Deep Sequencing Reveals Occurrence of Subclonal ALK Mutations in Neuroblastoma at Diagnosis. Clin Cancer Res. 2015. November 1;21(21):4913–21. [DOI] [PubMed] [Google Scholar]
- 56.Theissen J, Boensch M, Spitz R, Betts D, Stegmaier S, Christiansen H, et al. Heterogeneity of the MYCN Oncogene in Neuroblastoma. Clin Cancer Res. 2009. March 15;15(6):2085–90. [DOI] [PubMed] [Google Scholar]
- 57.Janoueix-Lerosey I, Schleiermacher G, Michels E, Mosseri V, Ribeiro A, Lequin D, et al. Overall Genomic Pattern Is a Predictor of Outcome in Neuroblastoma. J Clin Oncol. 2009. March 1;27(7):1026–33. [DOI] [PubMed] [Google Scholar]
- 58.Schleiermacher G, Mosseri V, London WB, Maris JM, Brodeur GM, Attiyeh E, et al. Segmental chromosomal alterations have prognostic impact in neuroblastoma: a report from the INRG project. Br J Cancer 2012 1078. 2012. September 13;107(8):1418–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Ambros PF, Ambros IM, Brodeur GM, Haber M, Khan J, Nakagawara A, et al. International consensus for neuroblastoma molecular diagnostics: report from the International Neuroblastoma Risk Group (INRG) Biology Committee. Br J Cancer. 2009. May 28;100(9):1471–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Twist C, London WB, Naranjo A, Schmidt M Lou, Adkins ES, Mattei P, et al. Maintaining outstanding outcomes using response- and biology-based therapy for intermediate-risk neuroblastoma: A report from the Children’s Oncology Group study ANBL0531. 10.1200/jco20143215_suppl10006. 2014. May 20;32(15_suppl):10006–10006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Chicard M, Colmet-Daage L, Clement N, Danzon A, Bohec M, Bernard V, et al. Whole-Exome Sequencing of Cell-Free DNA Reveals Temporo-spatial Heterogeneity and Identifies Treatment-Resistant Clones in Neuroblastoma. Clin Cancer Res. 2018. February 15;24(4):939–49. [DOI] [PubMed] [Google Scholar]
- 62.Chicard M, Boyault S, Colmet Daage L, Richer W, Gentien D, Pierron G, et al. Genomic Copy Number Profiling Using Circulating Free Tumor DNA Highlights Heterogeneity in Neuroblastoma. Clin Cancer Res. 2016. November 15;22(22):5564–73. [DOI] [PubMed] [Google Scholar]
- 63.Lodrini M, Sprüssel A, Astrahantseff K, Tiburtius D, Konschak R, Lode HN, et al. Using droplet digital PCR to analyze MYCN and ALK copy number in plasma from patients with neuroblastoma. Oncotarget. 2017. October 17;8(49):85234–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Klega K, Imamovic-Tuco A, Ha G, Clapp AN, Meyer S, Ward A, et al. Detection of Somatic Structural Variants Enables Quantification and Characterization of Circulating Tumor DNA in Children With Solid Tumors. JCO Precis Oncol. 2018. November;2018(2):1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Kahana-Edwin S, Cain LE, McCowage G, Darmanian A, Wright D, Mullins A, et al. Neuroblastoma Molecular Risk-Stratification of DNA Copy Number and ALK Genotyping via Cell-Free Circulating Tumor DNA Profiling. Cancers (Basel). 2021. July 5;13(13):3365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Shulman DS, Klega K, Imamovic-Tuco A, Clapp A, Nag A, Thorner AR, et al. Detection of circulating tumour DNA is associated with inferior outcomes in Ewing sarcoma and osteosarcoma: a report from the Children’s Oncology Group. Br J Cancer. 2018. August 21;119(5):615–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Tirode F, Surdez D, Ma X, Parker M, Deley MC Le, Bahrami A, et al. Genomic landscape of Ewing sarcoma defines an aggressive subtype with co-association of STAG2 and TP53 mutations. Cancer Discov. 2014. November 1;4(11):1342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Shukla NN, Patel JA, Magnan H, Zehir A, You D, Tang J, et al. Plasma DNA-Based Molecular Diagnosis, Prognostication, and Monitoring of Patients With EWSR1 Fusion-Positive Sarcomas. JCO Precis Oncol. 2017. November;1(1):1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Treger TD, Chagtai T, Butcher R, Cresswell GD, Al-Saadi R, Brok J, et al. Somatic TP53 Mutations Are Detectable in Circulating Tumor DNA from Children with Anaplastic Wilms Tumors. Transl Oncol. 2018. December 1;11(6):1301–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Dix DB, Seibel NL, Chi Y-Y, Khanna G, Gratias E, Anderson JR, et al. Treatment of Stage IV Favorable Histology Wilms Tumor With Lung Metastases: A Report From the Children’s Oncology Group AREN0533 Study. J Clin Oncol. 2018. June 1;36(16):1564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Ooms AHAG, Gadd S, Gerhard DS, Smith MA, Guidry Auvil JM, Meerzaman D, et al. Significance of TP53 mutation in Wilms tumors with diffuse anaplasia: A report from the Children’s Oncology Group. Clin Cancer Res. 2016. November 15;22(22):5582–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Maschietto M, Williams RD, Chagtai T, Popov SD, Sebire NJ, Vujanic G, et al. TP53 mutational status is a potential marker for risk stratification in Wilms tumour with diffuse anaplasia. PLoS One. 2014. October 14;9(10). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Armstrong GT, Liu Q, Yasui Y, Neglia JP, Leisenring W, Robison LL, et al. Late mortality among 5-year survivors of childhood cancer: a summary from the Childhood Cancer Survivor Study. J Clin Oncol. 2009. May 10;27(14):2328–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.van Dongen JJ, Seriu T, Panzer-Grümayer ER, Biondi A, Pongers-Willemse MJ, Corral L, et al. Prognostic value of minimal residual disease in acute lymphoblastic leukaemia in childhood. Lancet (London, England). 1998. November 28;352(9142):1731–8. [DOI] [PubMed] [Google Scholar]
- 75.Kelly KM, Cole PD, Pei Q, Bush R, Roberts KB, Hodgson DC, et al. Response‐adapted therapy for the treatment of children with newly diagnosed high risk Hodgkin lymphoma (AHOD0831): a report from the Children’s Oncology Group. Br J Haematol. 2019. October 10;187(1):39–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Oeffinger KC, Stratton KL, Hudson MM, Leisenring WM, Henderson TO, Howell RM, et al. Impact of Risk-Adapted Therapy for Pediatric Hodgkin Lymphoma on Risk of Long-Term Morbidity: A Report From the Childhood Cancer Survivor Study. J Clin Oncol. 2021. July 10;39(20):2266–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Krumbholz M, Hellberg J, Steif B, Bäuerle T, Gillmann C, Fritscher T, et al. Genomic EWSR1 Fusion Sequence as Highly Sensitive and Dynamic Plasma Tumor Marker in Ewing Sarcoma. Clin Cancer Res. 2016. September 1;22(17):4356–65. [DOI] [PubMed] [Google Scholar]
- 78.Meyers PA, Schwartz CL, Krailo M, Kleinerman ES, Betcher D, Bernstein ML, et al. Osteosarcoma: A Randomized, Prospective Trial of the Addition of Ifosfamide and/or Muramyl Tripeptide to Cisplatin, Doxorubicin, and High-Dose Methotrexate. J Clin Oncol. 2005. March 20;23(9):2004–11. [DOI] [PubMed] [Google Scholar]
- 79.Miguez ACK, Barros BD de F, de Souza JES, da Costa CML, Cunha IW, Barbosa PNVP, et al. Assessment of somatic mutations in urine and plasma of Wilms tumor patients. Cancer Med. 2020. August 1;9(16):5948–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Kahana-Edwin S, McCowage G, Cain L, Saletta F, Yuksel A, Graf N, et al. Exploration of CTNNB1 ctDNA as a putative biomarker for hepatoblastoma. Pediatr Blood Cancer. 2020. November 1;67(11):e28594. [DOI] [PubMed] [Google Scholar]
- 81.Polski A, Xu L, Prabakar RK, Kim JW, Shah R, Jubran R, et al. Cell-Free DNA Tumor Fraction in the Aqueous Humor Is Associated With Therapeutic Response in Retinoblastoma Patients. Transl Vis Sci Technol. 2020. September 1;9(10):30–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Berry JL, Xu L, Murphree AL, Krishnan S, Stachelek K, Zolfaghari E, et al. Potential of Aqueous Humor as a Surrogate Tumor Biopsy for Retinoblastoma. JAMA Ophthalmol. 2017. November 1;135(11):1221–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Abramson DH, Mandelker D, Francis JH, Dunkel IJ, Brannon AR, Benayed R, et al. Retrospective Evaluation of Somatic Alterations in Cell-Free DNA from Blood in Retinoblastoma. Ophthalmol Sci. 2021. March 1;1(1):100015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Hayashi M, Chu D, Meyer CF, Llosa NJ, McCarty G, Morris CD, et al. Highly Personalized Detection of Minimal Ewing Sarcoma Disease Burden from Plasma Tumor DNA. Cancer. 2016. October 1;122(19):3015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *85.Applebaum MA, Barr EK, Karpus J, West-Szymanski DC, Oliva M, Sokol EA, et al. 5-Hydroxymethylcytosine Profiles in Circulating Cell-Free DNA Associate with Disease Burden in Children with Neuroblastoma. Clin Cancer Res. 2020. March 15;26(6):1309–17. [DOI] [PMC free article] [PubMed] [Google Scholar]; This study demonstrates that epigenetic signatures in cfDNA are a viable marker for risk stratification and prognostication in pediatric cancers. The authors approximate tumor burden and predict risk of relapse in neuroblastoma.
- 86.Remon J, Caramella C, Jovelet C, Lacroix L, Lawson A, Smalley S, et al. Osimertinib benefit in EGFR-mutant NSCLC patients with T790M-mutation detected by circulating tumour DNA. Ann Oncol Off J Eur Soc Med Oncol. 2017;28(4):784–90. [DOI] [PubMed] [Google Scholar]
- 87.Barris DM, Weiner SB, Dubin RA, Fremed M, Zhang X, Piperdi S, et al. Detection of circulating tumor DNA in patients with osteosarcoma. Oncotarget. 2018. February 27;9(16):12695–704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Pereira B, Chen CT, Goyal L, Walmsley C, Pinto CJ, Baiev I, et al. Cell-free DNA captures tumor heterogeneity and driver alterations in rapid autopsies with pre-treated metastatic cancer. Nat Commun. 2021. December 27;12(1):3199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Henriksen TVV, Tarazona N, Frydendahl A, Reinert T, Carbonell-Asins JA, Sharma S, et al. Serial circulating tumor DNA analysis to assess recurrence risk, benefit of adjuvant therapy, growth rate and early relapse detection in stage III colorectal cancer patients. J Clin Oncol. 2021. May 20;39(15_suppl):3540–3540. [Google Scholar]
- 90.Powles T, Assaf ZJ, Davarpanah N, Banchereau R, Szabados BE, Yuen KC, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021. July 15;595(7867):432–7. [DOI] [PubMed] [Google Scholar]
- 91.Chaudhuri AA, Chabon JJ, Lovejoy AF, Newman AM, Stehr H, Azad TD, et al. Early Detection of Molecular Residual Disease in Localized Lung Cancer by Circulating Tumor DNA Profiling. Cancer Discov. 2017;7(12):1394–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Tie J, Cohen JD, Wang Y, Li L, Christie M, Simons K, et al. Serial circulating tumour DNA analysis during multimodality treatment of locally advanced rectal cancer: A prospective biomarker study. Gut. 2019. April 1;68(4):663–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Dawson S-J, Tsui DWY, Murtaza M, Biggs H, Rueda OM, Chin S-F, et al. Analysis of Circulating Tumor DNA to Monitor Metastatic Breast Cancer. N Engl J Med. 2013. March 28;368(13):1199–209. [DOI] [PubMed] [Google Scholar]
- 94.Abramson DH. Retinoblastoma: Saving life with vision. Annu Rev Med. 2014;65:171–84. [DOI] [PubMed] [Google Scholar]
- 95.Abramson DH, Fabius AWM, Issa R, Francis JH, Marr BP, Dunkel IJ, et al. Advanced Unilateral Retinoblastoma: The Impact of Ophthalmic Artery Chemosurgery on Enucleation Rate and Patient Survival at MSKCC. PLoS One. 2015. December 1;10(12):e0145436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Devonshire AS, Whale AS, Gutteridge A, Jones G, Cowen S, Foy CA, et al. Towards standardisation of cell-free DNA measurement in plasma: controls for extraction efficiency, fragment size bias and quantification. Anal Bioanal Chem. 2014. October;406(26):6499–512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- **97.Zviran A, Schulman RC, Shah M, Hill STK, Deochand S, Khamnei CC, et al. Genome-wide cell-free DNA mutational integration enables ultra-sensitive cancer monitoring. Nat Med 2020 267. 2020. June 1;26(7):1114–24. [DOI] [PMC free article] [PubMed] [Google Scholar]; This study describes how the current paradigm of deep sequencing of cfDNA with targeted panels is limited in low-disease-burden settings by low tumor fraction with few unqiue genomic equivlanets. They demonostrate that modest depth (35x) WGS improves sensitivity by increasting breadth to integrate the cumulative signals of multiple genomic features and alterations.
- 98.Kahana-Edwin S, Cain LE, Karpelowsky J. Roadmap to Liquid Biopsy Biobanking from Pediatric Cancers–Challenges and Opportunities. Biopreserv Biobank. 2021. April 1;19(2):124–9. [DOI] [PubMed] [Google Scholar]
- 99.Trigg RM, Shaw JA, Turner SD. Opportunities and challenges of circulating biomarkers in neuroblastoma. Open Biol. 2019. May 1;9(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Kothari P, Marass F, Yang JL, Stewart CM, Stephens D, Patel J, et al. Cell‐free DNA profiling in retinoblastoma patients with advanced intraocular disease: An MSKCC experience. Cancer Med. 2020. September 1;9(17):6093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Hu Y, Ulrich BC, Supplee J, Kuang Y, Lizotte PH, Feeney NB, et al. False-Positive Plasma Genotyping Due to Clonal Hematopoiesis. Clin Cancer Res. 2018. September 15;24(18):4437–43. [DOI] [PubMed] [Google Scholar]
- 102.Steensma DP, Bejar R, Jaiswal S, Lindsley RC, Sekeres MA, Hasserjian RP, et al. Clonal hematopoiesis of indeterminate potential and its distinction from myelodysplastic syndromes. Blood. 2015. July 2;126(1):9–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Silver AJ, Bick AG, Savona MR. Germline risk of clonal haematopoiesis. Vol. 22, Nature Reviews Genetics. Nature Research; 2021. p. 603–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Young AL, Tong RS, Birmann BM, Druley TE. Clonal hematopoiesis and risk of acute myeloid leukemia. Haematologica. 2019;104(12):2410–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Bhattacharya R, Bick AG. Clonal Hematopoiesis of Indeterminate Potential: an Expanding Genetic Cause of Cardiovascular Disease. Curr Atheroscler Reports 2021 2311. 2021. September 1;23(11):1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Xie M, Lu C, Wang J, McLellan MD, Johnson KJ, Wendl MC, et al. Age-related mutations associated with clonal hematopoietic expansion and malignancies. Nat Med. 2014. December 19;20(12):1472–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Bick AG, Weinstock JS, Nandakumar SK, Fulco CP, Bao EL, Zekavat SM, et al. Inherited causes of clonal haematopoiesis in 97,691 whole genomes. Nat 2020 5867831. 2020. October 14;586(7831):763–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Wong WH, Tong S, Druley TE. Error-Corrected Sequencing of Cord Bloods Identifies Pediatric AML-Associated Clonal Hematopoiesis. Blood. 2017. December 7;130(Supplement 1):2687–2687. [Google Scholar]
- 109.Welch JS, Ley TJ, Link DC, Miller CA, Larson DE, Koboldt DC, et al. The origin and evolution of mutations in Acute Myeloid Leukemia. Cell. 2012. July 20;150(2):264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Collord G, Park N, Podestà M, Dagnino M, Cilloni D, Jones D, et al. Clonal haematopoiesis is not prevalent in survivors of childhood cancer. Br J Haematol. 2018. May 1;181(4):537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Laurie CACC, Laurie CACC, Rice K, Doheny KF, Zelnick LR, McHugh CP, et al. Detectable clonal mosaicism from birth to old age and its relationship to cancer. Nat Genet. 2012. June 6;44(6):642–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Olszewski AJ, Chorzalska AD, Kim AS, Quesenberry PJ, Lopresti ML, Fenton MA, et al. Clonal haematopoiesis of indeterminate potential among cancer survivors exposed to myelotoxic chemotherapy. Br J Haematol. 2019. August 1;186(3):e31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Bolton KL, Ptashkin RN, Gao T, Braunstein L, Devlin SM, Kelly D, et al. Cancer therapy shapes the fitness landscape of clonal hematopoiesis. Nat Genet. 2020;52(11):1219–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Chen G, Chen J, Liu H, Chen S, Zhang Y, Li P, et al. Comprehensive Identification and Characterization of Human Secretome Based on Integrative Proteomic and Transcriptomic Data. Front Cell Dev Biol. 2019. November 21;7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Cohen JD, Javed AA, Thoburn C, Wong F, Tie J, Gibbs P, et al. Combined circulating tumor DNA and protein biomarker-based liquid biopsy for the earlier detection of pancreatic cancers. Proc Natl Acad Sci. 2017. September 19;114(38):10202–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Cohen JD, Li L, Wang Y, Thoburn C, Afsari B, Danilova L, et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science (80-). 2018. February 23;359(6378):926–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Yao R, Yu T, Qing Y, Wang J, Shen Y. Evaluation of copy number variant detection from panel-based next-generation sequencing data. Mol Genet Genomic Med. 2019. January;7(1):e00513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Huether R, Dong L, Chen X, Wu G, Parker M, Wei L, et al. The landscape of somatic mutations in epigenetic regulators across 1000 pediatric cancer genomes. Nat Commun. 2014. April 8;5:3630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Lennon AM, Buchanan AH, Kinde I, Warren A, Honushefsky A, Cohain AT, et al. Feasibility of blood testing combined with PET-CT to screen for cancer and guide intervention. Science (80-). 2020. July 3;369(6499). [DOI] [PMC free article] [PubMed] [Google Scholar]