

Abstract
Several studies have demonstrated the effect of an organization’s culture and climate on the delivery of services to clients and the success of clinical outcomes. Workers’ perceptions are integral components of organizational social context, and in order to create a positive organizational culture and climate, managers and frontline staff need to have a shared understanding of the social context. The existing literature does not adequately address that discrepancies in perceptions of culture and climate between frontline staff and managers impact the implementation of policies and services. The purpose of this study is to compare the workgroup-level culture and climate of a single, large child and family social services organization, based on the reported experiences of front-line workers and senior managers. The results showed that, as a group, senior managers rated the organization as having a culture that was much more proficient and much less rigid and a climate that was more engaged and more functional than the average frontline workgroup. The discrepancies between the perceptions of upper management and workgroup-level staff indicate the need for interventions that can improve communication and cohesiveness between these two groups.
Keywords: Organizational culture, Organizational climate, Hillside Family of Agencies, HFA
Introduction
The large gap between viewpoints of quality clinical services in children’s mental health is well documented (Brekke, Ell, & Palinkas, 2007; Garland et al., 2010; Raghavan, Inoue, Ettner, & Hamilton, 2010; Zima et al., 2005). Many of the efforts to implement effective treatments have focused narrowly on the training of clinicians, but conceptual models have focused on how effective practices can be implemented in routine care (Patterson & Dulmus, 2012). These models have repeatedly emphasized the importance of the organizational social contexts in which these practices will be deployed (Aarons, Hurlburt, & Horwitz, 2011; Damschroder et al., 2009; Greenhalgh, Robert, Macfarlane, Bate, & Kyriakidou, 2004). In fact, simply implementing evidence-based treatments with fidelity does not always lead to improved clinical outcomes (Weisz et al., 2012), which suggests that concurrent improvements in the context of care may need to be prioritized. This paper describes the critical role that organizational social context (and in particular, organizational culture and climate) plays in service delivery, the effect that organizational leaders have in shaping and improving organizational culture and climate, and the importance of leaders and staff members sharing an understanding of the relative strengths and weaknesses of a given organization’s culture and climate. This paper then reports a study that tests the level of concordance between organizational leaders’ and staff members’ assessments of organizational culture and climate in a large children’s social service system.
The Role of Organizational Social Context in Service Delivery
Human service organizations create a social context for the services they provide. Organizational culture and climate are two aspects of context that are particularly important.
Organizational culture
Organizational culture, or the beliefs, values and norms inherent in an organization’s fundamental operations, serves to guide employees in their actions and responses to the surrounding environment (Ahmed, 1998; Shadur, Kienzle & Rodwell, 1999; Aarons & Sawitzky, 2006; Hemmelgarn, Glisson & James, 2006). Culture functions to support organizational survival amidst the influence of both external and internal forces, such as national and local policy, as well as employee values and assumptions (Brightman & Sayeed, 1990). Culture is a powerful, covert force that unifies the organization by giving members a common language (Kane-Urrabazo, 2006; McGrath & Tobias, 2008). It is also dynamic, created by the interactions among individuals in the organization and shaped by leadership behavior based on structures, routines, rules, and norms (Kane-Urrabazo, 2006; Conceicao & Altman, 2011; Harrington, 2011), and leadership decisions regarding internal operations and strategic planning (Giberson et al., 2009; Patterson, 2011).
Organizational climate
Organizational climate refers to the practices and procedures that define perceptions of the environment (Ahmed, 1998). It captures the qualities of the work environment and explains how the individual employees experience the environment (Glisson & Green, 2010). As such, employees’ emotional responses to various characteristics of the work environment influence climate. While it is an individual experience, coworkers often share climate through socialization and climate becomes a collective perception of formal and informal organizational policies, practices and procedures (Glisson & James, 2002; Shadur, Kienzle & Rodwell, 1999). Climate helps to set the tone of the organization, and further, it can work to either facilitate or impair employee involvement (Glisson & James, 2002). Although visible at the surface-level, organizational climate is a gauge of the more deeply-entrenched organizational culture (Shadur, Kienzle & Rodwell, 1999).
Implications and outcomes related to culture and climate
Organizational culture and climate have considerable implications for both employees and the clients they serve. Research has identified organizational culture and climate as significant predictors of employee commitment and satisfaction (Hemmelgarn, Glisson & James, 2006), and of employees’ intention to leave an organization (Shim, 2010). As such, employees associated with more constructive cultures had more positive work attitudes, perceived the services they provided to be of higher quality and were less likely to quit their jobs (Glisson & James, 2002). Similarly, amongst children’s services, positive climates have been associated with outcomes of improved psychosocial functioning and the receipt of more comprehensive services, increased continuity in services received, and increased caseworker responsiveness and availability (Glisson, & Green, 2010).
Additionally, children have had more positive long-term outcomes in systems with more engaged organizational climates, beyond the impact of location and multiple variables such as a child’s age, gender, race, family income, and level of harm resulting from maltreatment (Glisson & Green, 2010). In contrast, less than ideal organizational climates have been associated with reduced caseworker capacity to help clients through increased job-related stress and contributed to high turnover rates and depersonalized relationships with clients (Glisson & Green, 2010); such characteristics have been found to negatively affect service quality and outcomes (Glisson, Dukes & Green, 2006). A developing literature is investigating culture and climate’s impact on whether or not empirically supported treatments (ESTs) will be adopted in practice (Patterson & Dulmus, 2012; Patterson, Dulmus, & Maguin, 2012) and whether there are organizational profiles that are better EST implementers (Patterson, in-press).
The Role of Organizational Leaders in Shaping Organizational Culture and Climate
Leadership is one of the many factors examined in a growing body of literature surrounding children’s mental health services (Novins, Green, Legha & Aarons, 2013). It has been described from two perspectives: transactional leadership – emphasizing the exchanges between leader and subordinates – and, transformational leadership - fostering a climate of innovation and growth (Bass, 1990; Avolio, Bass & Jung, 1999). In addition, transformational leadership has been identified as a mediating factor between leaders’ sense of belonging with the organization (i.e. organizational identification) and that of staff (Schuh, Zhange, Egold, Graf, Pandey & van Dick, 2011); as well as providing a buffering effect between staffs’ emotional exhaustion and their intention to leave an organization (Green, Miller & Aarons, 2013). Furthermore, although both types of leadership have been associated with attitudes toward the adoption of evidence-based practices (Aarons, 2006), transformational leadership has particular implications for the implementation of evidence-based practices given its influence in creating a climate of innovation (Aarons & Sommerfeld, 2012).
As an integral component of organizations, leaders have the potential to influence the work environment in significant ways. Through such considerations as a focus on staff development, empowerment and role clarity, leaders have the ability to impact both organizational and staffing outcomes (Chen & Silverthorne, 2005; Mendes & Stander, 2011). As such, organizational leaders (i.e. senior managers) have the task of fostering cultures and climates that sustain growth and enable development at all levels of the organization. They are challenged to ensure employees are consistent in their interpretation and evaluation of expectations in order to avoid any confusion related to miscommunicating the organization’s overall goals and mission (Ahmed, 1998). The presence of discrepancies between formally declared priorities and frontline realities, especially under competing employment demands, affects consistency (Zohar & Luria, 2010).
More differentiated organizations, that is, organizations with more departments and services, require more integration (Damanpour, 1991). Fragmentation of the culture results from departmentalization or specialization and the inconsistency of messages between the organizational culture and the departmental subcultures. A struggle between the organizational culture and its subcultures is likely to occur when messages conflict between senior management and front-line workers. Senior managers are responsible for assuring that the communication from and between the various facets of the organization (e.g. policies, staff) are consistent with its avowed mission, beliefs, and values, as well as aligning disparate individual beliefs and values with those of the organization (Ross, 2008).
Consistency Between Leaders’ and Staff Members’ Ratings of Culture and Climate
Although management may be responsible for aligning individuals and departments with the mainstream environment of the organization, evidence suggests that they may not be consistent or accurate in their evaluation of the organizational culture and climate. Differences in beliefs between major stakeholders can create gaps in an organization. Brightman and Sayeed (1990) evaluated differences between members of the management team and the senior team of a utility firm. While the senior team noted the need for increased socialization among employees for the organization to accomplish its mission, the management team acknowledged the need for increased task support and task innovation. Although the senior and management team members had similar social styles, they were dissimilar in personality styles and values (Brightman & Sayeed, 1990).
In addition to differences in perception of climate and culture between levels of management, researchers have identified differences between management and front-line workers. Martin, Jones, and Callan (2005) explored contrasts in front-line worker’s perception within two organizations (a large, state public sector organization and a hospital) that were undergoing considerable change and restructuring. Significant differences existed between upper-level (e.g. senior policy officers and unit managers) and lower-level (e.g. non-clinical staff) employees, within the researchers’ hierarchical categorization. Upper-level employees reported greater leader vision, change self-efficacy, and organizational commitment than lower-level employees, as well as higher levels of supervisor support and more positive perceptions about the extent to which leaders exhibited a vision for the organization.
In their study of primary health care organizations, Carlfjord, Andersson, Nilsen, Bendtsen, and Lindberg (2010) found that managers scored organizational climate dimensions higher than clinical staff members. Additionally, managers perceived employees as more committed to the organization and rated overall attitudes toward new ideas more positively than the staff had reported. Compared to staff, managers were generally less aware of conflicts and perceived the climate to be more positive.
Multiple studies that assessed climate and patient care in hospital environments (Hansen, Williams & Singer, 2011; Hartmann et al., 2008; Rosen et al., 2010; Singer et al., 2009) found that senior management routinely rated the hospital climate higher than frontline staff. However, frontline staff perceptions were more closely associated with patient readmission and compromised patient safety than senior management perceptions. Frontline staff members were more accurate than senior management in identifying weaknesses in safety climate associated with worse patient outcomes. Consistently, staff with direct contact with patients had the most exposure to potential safety issues and resultantly had significantly higher levels of problematic response compared to senior managers, whose work is removed from the direct patient care environment (Hartmann et al., 2008). As senior managers are less often exposed to frontline work, they may be less informed about safety performance than frontline workers whose actions directly affect patients; this is true regardless of health care systems or settings (Rosen et al., 2010).
Study Purpose
The purpose of this study is to compare the workgroup-level culture and climate of a single, large child and family social services organization, based on the reported experiences of front-line workers and senior managers. To the best of our knowledge, no similar research has been conducted in the mental health field. Understanding the level of concordance between front-line workers and senior managers’ viewpoints of the working environment will benefit any efforts to improve organizational cultures and climates.
Method
Setting
The setting for this study was the Hillside Family of Agencies (HFA), the largest child and family human service agency in Western and Central New York State (NYS). HFA has helped children and their families for more than 170 years, and currently employs more than 2,400 staff within four affiliate organizations. HFA provides services to clients across 30 New York counties and in Prince George’s County, Maryland and two affiliate organizations provide support services. Affiliates of this $140+ million network provide services to children from birth to age 26 in more than 12,000 families each year. HFA provides services in six major categories, including child welfare, mental health, juvenile justice, education, youth development, and developmental disabilities/mental health. HFA holds NYS licenses with the Office of Children and Family Services, the Office of Mental Health, the Office for People with Developmental Disabilities, and the Department of Health and the State Education Department and is accredited by the Council on Accreditation. Since 2007, HFA has focused on a strategic intent to become a leading agency in translating research into effective practice solutions. HFA continues to grow, demonstrating strong financial performance with an annual average increase of 9% in consolidated revenue.
Study Sample
The participants in this study consisted of 1,273 “frontline” employees (i.e., employees with direct service contact with the children and families this agency served) and 26 senior managers and top agency executives (i.e., employees with no direct contact with children and families with the sole responsibility of senior management of the organization).
Frontline workers
Frontline workers were employed in a total of 55 different programs across the four direct service affiliates. A senior HFA manager defined the 55 frontline programs according to the program’s service function and supervisory structure. Several programs with fewer than five workers were excluded because they did not meet measurement scoring criteria. All frontline workers in a program were supervised by the same supervisor and were housed in the same location and each program provided a single type of service (e.g., residential, outpatient, day treatment, etc.). Across HFA, two types of programs predominated: community based (n = 17, 31%) and residential (n = 18, 33%). The remaining program types included day treatment (n = 5, 9%), foster care and residential-based schools (n = 4, 7% for each), medical (n = 3, 5%), service integration (n = 2, 4%), and adoption and outpatient (n = 1, 2% for each). Programs were not divided equally across the four affiliates. Affiliate A had six programs, affiliate B had three programs, affiliate C had two programs and affiliate D had 44 programs, including 13 community-based and 15 residential programs. The participation rate for this study was 82%, yielding a total sample of 1,273 participants from a total of 1,552 child and family service providers.
The number of frontline participants per program ranged from 5 to 84 (Median = 15, M = 23, SD = 18). About 13% of the sample worked at affiliate A; about 8% worked at affiliate B; about 5% worked at affiliate C; and 74% worked at affiliate D. Approximately 42% of respondents worked in residential programs; 23% worked in community-based programs; 12% worked in day treatment programs; and 11% worked in residential-based school programs. The remaining respondents worked in four, much smaller services. Aggregate data on the demographic characteristics of the population of HFA frontline employees were not obtained from HFA Human Relations. Thus the extent to which participating employees differed from all study-eligible employees could not be determined.
Sample demographics
Table 1 presents the demographic characteristics of the frontline workers and the senior managers. Front-line workers and senior managers differed significantly on educational level (χ2[4, 1222] = 10.56, p = .032) and major (χ2[5, 1105] = 14.12, p = .015). As shown in Table 1, compared to front-line workers a larger percentage of senior managers held a Masters (46.2% versus 27.2%) and smaller percentages held an Associates or only a high school diploma (7.7% versus 17.0% and 0.0% versus 16.6%, respectively). With respect to major and compared to front-line workers, a larger percentage of senior managers had a social work major (42.3% versus 17.6%) and smaller percentages had an education major or a psychology major (7.7% versus 22.8% and 3.8% versus 15.6%, respectively). In addition, we consider it very likely that senior managers were significantly older and had worked in their present position for more years; however, the way the data were collected did not permit those computations.
Table 1.
Demographic Characteristics of Front-line Workers and Senior Managers
| Characteristic | Front-line Workers (n = 1273) |
Senior Managers (n = 26) |
|---|---|---|
| Education* | ||
| High School graduate | 17.0% | 7.7% |
| Associates | 16.6% | 0.0% |
| Bachelors | 38.0% | 42.3% |
| Masters | 27.2% | 46.2% |
| Doctoral | 1.2% | 3.8% |
| Major* | ||
| Education | 22.8% | 2 7.7% |
| Social work | 17.6% | 11 42.3% |
| Nursing | 4.4% | 2 7.7% |
| Medicine | 0.4% | 0 0.0% |
| Psychology | 15.6% | 1 3.8% |
| Other | 39.3% | 10 38.5% |
| Ethnicity NS | ||
| White | 75.2% | 92.3% |
| Black | 15.8% | 3.8% |
| Other/Multiple | 9.0% | 3.8% |
| Female NS | 58.8% | 61.5% |
| Age: | Range: 19–73 Mean: 35.4 SD: 11.0 |
Range: 35–62 Mean: 50.0 SD: ND |
| Years of Experience | Range: 0–50 Mean: 9.6 SD: 8.5 |
Range: ND Mean: ND SD: ND |
| Years in Present Job | Range: 0–36 Mean: 5.0 SD: 5.6 |
Range: 0–30 Mean: 15.3 SD: ND |
Notes. ND: Data not collected/statistic not computed.
p < .05.
Measures
Organizational social context
The Organizational Social Context Measurement Model (OSC) is a measurement system guided by a model of social context; it consists of both organizational (structure and culture) and individual (work attitudes and behavior) level constructs. These constructs include individual and shared perceptions (climate), which are believed to mediate the organization’s impact on the individual (Glisson, 2002; Glisson et al., 2008). The OSC measurement tool contains 105 items that form four domains, 16 first order factors and 7 second order factors, which have been confirmed in a national sample of 100 mental health service organizations with approximately 1,200 clinicians. The self-administered Likert scale survey takes approximately 20 minutes to complete and is presented on a scannable bubble sheet booklet.
The OSC is a measure of a program’s culture and climate as reported by its workers; thus, scores are computed for the program as a whole and not for its individual workers. The scores reported are T scores, whose computation is based on Glisson et al.’s (2008) sample of agencies. The three factors that comprise an organization’s culture are: Proficiency (α = .94), Rigidity (α = .81), and Resistance (α = .81) (Glisson et al., 2008). Proficient cultures will place the health and well-being of clients first and workers will work to meet the unique needs of individual clients using the most recent available knowledge (e.g., “Members of my organizational unit are expected to be responsive to the needs of each client” and “Members of my organizational unit are expected to have up-to-date knowledge”). Rigid cultures allow workers a small amount of discretion and flexibility in their activities, with the majority of controls from strict bureaucratic rules and regulations (e.g., “I have to ask a supervisor or coordinator before I do almost anything” and “The same steps must be followed in processing every piece of work”). Resistant cultures are described as workers showing little interest in changes or new ways of providing services. Workers in Resistant cultures will suppress any openings to change (e.g., “Members of my organizational unit are expected to not make waves” and “Members of my organizational unit are expected to be critical”). The reliability values for the front-line sample were .89, .73 and .73 for Proficiency, Rigidity, and Resistance, respectively.
The factors for organizational climate are Engagement (α = .78), Functionality (α = .90), and Stress (α = .94) (Glisson et al., 2008). In Engaged climates, workers perceive that they can accomplish worthwhile activities and stay personally involved in their work while remaining concerned about their clients (e.g., “I feel I treat some of the clients I serve as impersonal objects,” “I have accomplished many worthwhile things in this job”). Workers in Functional climates receive support from their coworkers and have a well-defined understanding of how they fit into the organizational work unit (e.g., “This agency provides numerous opportunities to advance if you work for it” and “My job responsibilities are clearly defined”). Stressful climates are ones where workers are emotionally exhausted and overwhelmed as the result of their work; they feel that they are unable to accomplish the necessary tasks at hand (e.g., “I feel like I am at the end of my rope” and “The amount of work I have to do keeps me from doing a good job”). The reliability values for the front-line sample were .80, .90 and .92 for Engagement, Functionality, and Stress, respectively.
Demographic data for front-line workers were taken from the demographic questions that are part of the OSC survey booklet. Demographic data for the senior managers were taken from agency records.
Data Collection Procedure
Upon IRB approval, the OSC survey was administered to participants in paper and pencil format. Data collection occurred in groups, without the presence of agency supervisory or administrative personnel who did not also have direct service responsibilities. Each group was read instructions assuring subjects that their responses were anonymous and data would only be reported back to the organization in aggregated form. Participating employees received no compensation for participation. Completed surveys were collected, checked for completeness, and securely shipped to Dr. Glisson’s research center in Tennessee for scoring.
Results
The plot in Figure 1 compares and locates the senior manager scale scores in relation to the scale scores for the 55 workgroups. The plotted scores are T scores. The score mean and standard deviation and score range for workgroups and the senior manager scale score are plotted for each of the OCC scales. As shown in Figure 1, the workgroup scores for each scale are spread over a substantial range, with smallest at about 26 points, for Proficiency and Rigidity, and the largest at about 41 points, for Resistance and Functionality. Compared to the workgroup means, the senior manager group scores are consistently more positive, i.e., more proficient, less rigid, etc. Placed in an effect size metric, senior managers perceived their organization as more proficient and less resistant by an effect size of about 2.5 SDs (standard deviations) for both scales, compared with the average workgroup. Senior managers also perceived the organization as more engaged and more functional, by an effect size of about 1.4 and 1.2 SDs, respectively, compared to the average workgroup. Senior managers were similar to the average frontline workgroup only in the level of perceived resistance and stress.
Figure 1.
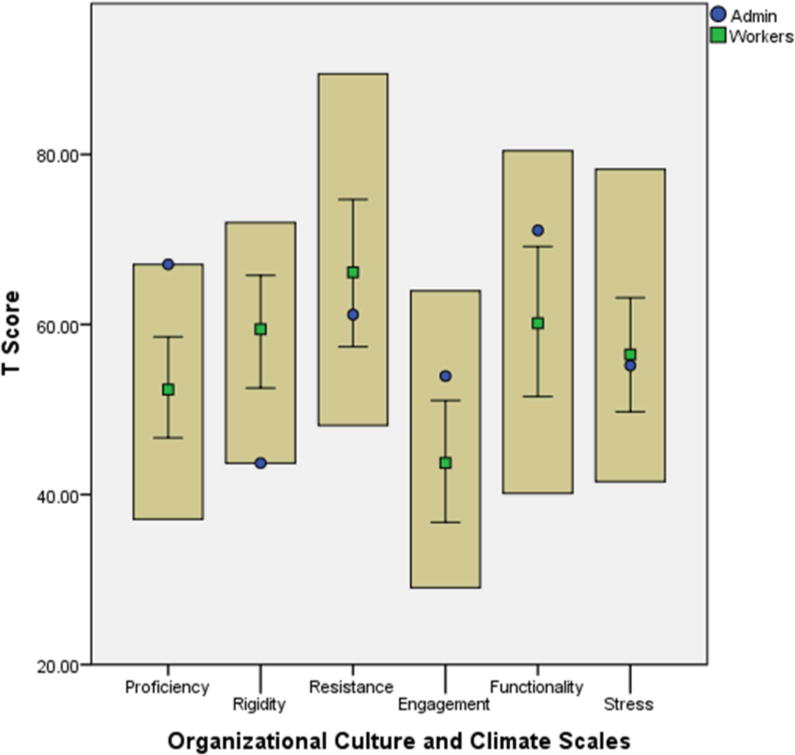
Culture and Climate Scale Scores of the Senior Manager Group Plotted Against the Mean, Standard Deviation and Range of Culture and Climate Scale Scores of the Front-line Workers Workgroups
Glisson et al., (2008) described a profile for the ideal culture as having a Proficiency score 2 standard deviations (SDs: 20 T-score points) above the Rigidity and Resistance scale scores and a profile for the ideal climate as having Engagement and Functionality scores 2 SDs above the Stress score. As a review of Table 2 shows, neither the senior manager group nor average workgroup profiles show an ideal culture profile or an ideal climate profile. In fact, none of the workgroups have either an ideal culture profile or an ideal climate profile.
Table 2.
Culture and Climate Scale Scores for Administration Group (N = 1) and Mean, Standard Deviation and Range of Scale Scores for Workgroups (N = 55)
| Group | Proficiency | Rigidity | Resistance | Engagement | Functionality | Stress |
|---|---|---|---|---|---|---|
| Senior Management | ||||||
| Score | 67.07 | 43.70 | 61.16 | 53.94 | 71.07 | 55.18 |
| Workgroups | ||||||
| Mean | 52.35 | 59.45 | 66.14 | 43.72 | 60.15 | 56.47 |
| SD | 5.66 | 6.34 | 8.71 | 7.11 | 8.79 | 6.76 |
| Median | 53.25 | 59.20 | 66.52 | 43.94 | 59.46 | 56.29 |
| Minimum | 37.10 | 45.66 | 48.14 | 29.05 | 40.14 | 41.53 |
| Maximum | 63.48 | 71.98 | 89.47 | 63.95 | 80.44 | 78.26 |
| Range | 26.38 | 26.32 | 41.33 | 34.90 | 40.30 | 36.73 |
| ES1 | 2.60 | −2.48 | −0.57 | 1.44 | 1.24 | 0.19 |
Note.
ES (Effect Size) computed relative to workgroup mean.
Discussion
The purpose of the present study was to compare frontline workers’ and senior managers’ experience of the workgroup level organizational culture and climate in a single, large child and family social services organization. The results showed that, as a group, senior managers rated the organization as having a culture that was much more proficient and much less rigid and a climate that was more engaged and more functional than the average frontline workgroup. Senior managers were similar to the average workgroup only on the levels of resistance and stress. Our discussion focuses on the importance of an upper management and direct care staff sharing an understanding of the organizational context, the need for interventions that can improve organizational context and leadership, limitations of the current study, and directions for future research.
The Importance of a Shared Understanding of Organizational Culture and Climate
In order to build an ideal culture and climate in which all levels of an organization share similar perspectives, its leaders should be sensitive to the environment and aware of their influence on others around them (Ahmed, 1998; Patterson, Dulmus, & Maguin, 2013; Rentsch, 1990). While many leaders acknowledge the significance of culture, few realize their roles and responsibilities in its development (Kane-Urrabazo, 2006). Through effectively managing crucial organizational factors, such as strengthening supervisory and practice supports that diminish employees’ emotional exhaustion, senior managers can positively influence the development of an ideal working environment (Brooks, Patterson, & McKiernan, 2012). However, such management strategies for organizational change and the creation of a positive organizational culture and climate need to be based on understanding employees’ individual perceptions about the organizational environment (Shim, 2010).
Internal consistency of policies and practices can support congruence between communication and practice within an organization (Kane-Urrabazo, 2006) and can improve service effectiveness (Ross, 2008). Similarly, greater consensus among individual members leads to better-defined climate as an organizational property (Zohar & Luria, 2010). A strong organizational climate indicates the transparency of policies and procedures and guidelines for action. In an ideal working climate, there is less room for interpretation, resulting in clearer supervisory practices that promote strong group climates (Patterson et al., 2013). The more the members interact among themselves and with their leader, the more likely they are to come up with consensual appraisals and consequently, foster a stronger climate (Zohar & Luria, 2010).
The Need for Interventions that Can Improve the Organizational Context of Care Delivery
The discrepancies between the perceptions of upper management and workgroup-level staff indicate the need for interventions that can improve communication between these two groups. Glisson and colleagues’ (Glisson et al., 2010) Availability, Responsiveness, and Continuity (ARC) organizational implementation strategy works to improve organizational social context in part by instituting participatory decision making and facilitating communication between different levels of the organization. Further, work is underway to develop and test models of leadership training specific to the implementation of EST (Aarons, Horowitz, Dlugosz, & Ehrhart, 2012). These types of interventions hold promise for increasing leaders’ awareness of issues related to organizational culture and climate that may serve as barriers to implementation and quality service delivery; however, there is clearly room for innovative approaches.
Limitations
The single most important limitation of this study is the data were obtained from a single, albeit large, child and family services agency. Within the limits of possibly nonrandom voluntary participation by agency service providers and the exclusion of a few programs that did not meet OSC scoring requirements for program size, this study is an analysis of the agency as a population. We cannot establish whether this agency is representative of all agencies, or even of other agencies at a similar size level. More importantly, we cannot establish whether these results are a good proxy for the results that would be obtained from a sample of agencies. In addition, the OSC instrument was developed for use with frontline workers and not senior managers.
Directions for Future Research
As with any new area of study, more investigation and information are necessary. As mentioned earlier, the social work field continues the move toward widespread EST implementation. Treatment efficacy studies should consider measuring the perceptions of the treatment adopter as well as those in upper management (Patterson et al., 2013). Similar to Glisson and colleagues’ attempts with their ARC strategy, one cannot assume that ESTs can be smoothly integrated into practice once trickled down from the decision makers. Although frontline workers and management might share the common perception of the overall mission of the organization, these two groups could differ in their perceptions of how the organization goes about accomplishing this mission. A shared perception of the mission and specific clinical intervention could significantly improve the process of EST implementation which might ultimately impact client outcomes.
Contributor Information
David A. Patterson, Silver Wolf (Adelv unegv Waya), Brown School, Washington University in St. Louis, St. Louis, Missouri, USA.
Catherine Dulmus, Buffalo Center for Social Research, University at Buffalo, Buffalo, New York, USA.
Eugene Maguin, Buffalo Center for Social Research, University at Buffalo, Buffalo, New York, USA.
John Keesler, Buffalo Center for Social Research, University at Buffalo, Buffalo, New York, USA.
Byron Powell, Brown School, Washington University in St. Louis, St. Louis, Missouri, USA.
References
- Aarons GA. Transformational and transactional leadership: Association with attitudes toward evidence-based practice. Psychiatric Services. 2006;57(8):1162–1169. doi: 10.1176/appi.ps.57.8.1162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aarons GA, Horowitz JD, Dlugosz LR, Ehrhart MG. The role of organizational processes in dissemination and implementation research. In: Brownson RC, Colditz GA, Proctor EK, editors. Dissemination and implementation research in health: Translating science to practice. New York: Oxford University Press; 2012. pp. 128–153. [Google Scholar]
- Aarons GA, Hurlburt M, Horwitz SM. Advancing a conceptual model of evidence-based practice implementation in public service sectors. Administration and Policy in Mental Health and Mental Health Services Research. 2011;38:4–23. doi: 10.1007/s10488-010-0327-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aarons G, Sawitzky A. Organizational climate partially mediates the effect of culture on work attitudes and staff turnover in mental health services. Administration and Policy in Mental Health and Mental Health Services Research. 2006;33:289–301. doi: 10.1007/s10488-006-0039-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aarons GA, Sommerfeld DH. Leadership, innovation climate and attitudes toward evidence-based practice during a statewide implementation. Journal of the American Academy of Child and Adolescent Psychiatry. 2012;51(4):423–431. doi: 10.1016/j.jaac.2012.01.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahmed PK. Culture and climate for innovation. European Journal of Innovation Management. 1998;1:30–43. [Google Scholar]
- Avolio BJ, Bass BM, Jung DI. Re-examining the components of transformational and transactional leadership using the Multifactor Leadership Questionnaire. Journal of Occupational and Organizational Psychology. 1999;72:441–462. [Google Scholar]
- Bass BM. From transactional to transformational leadership: Learning to share the vision. Organizational Dynamics. 1990;18:19–31. [Google Scholar]
- Brekke JS, Ell K, Palinkas LA. Translational science at the National Institute of Mental Health: Can social work take its rightful place? Research on Social Work Practice. 2007;17(1):123–133. doi: 10.1177/1049731506293693. [DOI] [Google Scholar]
- Brooks CT, Patterson DA, McKiernan PM. Group supervision attitudes: Organizational strategies to adopting evidence-based practices. The Qualitative Report. 2012;17(1):191–199. [PMC free article] [PubMed] [Google Scholar]
- Brightman HJ, Sayeed L. The pervasiveness of senior management’s view of the cultural gaps within a division. Group and Organization Studies. 1990;15:266–278. [Google Scholar]
- Carlfjord S, Andersson A, Nilsen P, Bendtsen P, Lindberg M. The importance of organizational climate and implementation strategy at the introduction of a new working tool in primary health care. Journal of Evaluation in Clinical Practice. 2010;16:1326–1332. doi: 10.1111/j.1365-2753.2009.01336.x. [DOI] [PubMed] [Google Scholar]
- Chen JC, Silverthorne C. Leadership effectiveness, leadership style, and employee readiness. Leadership and Organization Development Journal. 2005;26:280–288. [Google Scholar]
- Conceicao SCO, Altman BA. Training and development process and organizational culture change. Organization Development Journal. 2011;29:33–43. [Google Scholar]
- Damanpour F. Organizational innovation: A meta-analysis of effects of determinants and moderators. The Academy of Management Journal. 1991;34(3):555–590. [Google Scholar]
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implementation Science. 2009;4(50) doi: 10.1186/1748-5908-4-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garland AF, Brookman-Frazee L, Hurlburt MS, Accurso EC, Zoffness RJ, Haine-Schlagel R, Ganger W. Mental health care for children with disruptive behavior problems: A view inside therapists’ offices. Psychiatric Services. 2010;61(8):788–795. doi: 10.1176/appi.ps.61.8.788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giberson TR, Resick CJ, Dickson MW, Mitchelson JK, Randall KR, Clark MA. Leadership and organizational culture: Linking CEO characteristics to cultural values. Journal of Business Psychology. 2009;24:123–137. [Google Scholar]
- Gillard A, Witt PA, Watts CE. An examination of staff-level stakeholders and organizational culture at a camp for youth with HIV/AIDS. Journal of Park and Recreation Administration. 2010;28:61–78. [Google Scholar]
- Glisson C, Dukes D, Green P. The effects of the ARC organizational intervention on caseworker turnover, climate, and culture in children’s service systems. Child Abuse & Neglect. 2006;30:855–880. doi: 10.1016/j.chiabu.2005.12.010. [DOI] [PubMed] [Google Scholar]
- Glisson C, Green P. Organizational climate, services, and outcomes in child welfare systems. Child Abuse and Neglect. 2010;35:582–591. doi: 10.1016/j.chiabu.2011.04.009. [DOI] [PubMed] [Google Scholar]
- Glisson C, James lR. The cross-level effects of culture and climate in human service teams. Journal of Organizational Behavior. 2002;23:767–794. [Google Scholar]
- Glisson C, Landsverk J, Schoenwald S, Kelleher K, Hoagwood KE, Mayberg S, Green P. Assessing the organizational social context (OSC) of mental health Services: Implications for research and practice. Administration and Policy in Mental Health and Mental Health Services Research. 2008;35:98–113. doi: 10.1007/s10488-007-0148-5. [DOI] [PubMed] [Google Scholar]
- Glisson C, Schoenwald S, Hemmelgarn A, Green P, Dukes D, Armstrong KS, Chapman JE. Randomized trial of MST and ARC in a two-level evidence-based treatment implementation strategy. Journal of Consulting and Clinical Psychology. 2010;78(4):537–550. doi: 10.1037/a0019160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green AE, Miller EA, Aarons GA. Transformational leadership moderates the relationship between emotional exhaustion and turnover intention among community mental health providers. Community Mental Health Journal. 2013;49:373–379. doi: 10.1007/s10597-011-9463-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: Systematic review and recommendations. The Milbank Quarterly. 2004;82(4):581–629. doi: 10.1111/j.0887-378X.2004.00325.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hansen LO, Williams MV, Singer SJ. Perceptions of hospital safety climate and incidence of readmission. Health Services Research. 2011;46:596–616. doi: 10.1111/j.1475-6773.2010.01204.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrington A. Affecting the environment. Occupational Health. 2011;63(2):1–4. [Google Scholar]
- Hartmann CW, Rosen AK, Meterko M, Shokeen P, Zhao S, Singer S, Falwell A, Gaba DM. An overview of patient safety climate in the VA. Health Services Research. 2008;43:1263–1284. doi: 10.1111/j.1475-6773.2008.00839.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hemmelgarn AL, Glisson C, James LR. Organizational culture and climate: Implications for services and interventions research. Clinical Psychology: Science and Practice. 2006;13:73–89. [Google Scholar]
- Kane-Urrabazo C. Management’s role in shaping organizational culture. Journal of Nursing Management. 2006;14:188–194. doi: 10.1111/j.1365-2934.2006.00590.x. [DOI] [PubMed] [Google Scholar]
- Martin AJ, Jones ES, Callan VJ. Status differences in employee adjustment during organizational change. Journal of Managerial Psychology. 2005;21:145–162. [Google Scholar]
- McGrath D, Tobia S. Organizational culture as a hidden resource. New Directions for Community Colleges. 2008;144:41–53. [Google Scholar]
- Mendes F, Stander MW. Positive organization: The role of leader behavior in work engagement and retention. SA Journal of Industrial Psychology. 2011;37(1) Art. #900, 13 pages. [Google Scholar]
- Novins DK, Green AE, Legha RK, Aarons GA. Dissemination and implementation of evidence-based practices for child and adolescent mental health: A systematic review. Journal of the American Academy of Child and Adolescent Psychiatry. 2013;52(10):1009–1025. doi: 10.1016/j.jaac.2013.07.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson DA. Organizational resource investments: Do funding policies impact client outcomes? Counselor. 2011;12:40–44. [Google Scholar]
- Patterson DA. What are the ideal characteristics of empirically supported treatment adopters? Journal of Evidence-Based Social Work (In-press) [Google Scholar]
- Patterson DA, Dulmus CN. Organizational barriers to adopting an alcohol screening and brief intervention in community-based mental health organizations. Best Practices in Mental Health: An International Journal. 2012;8(1):16–28. [PMC free article] [PubMed] [Google Scholar]
- Patterson DA, Dulmus CN, Maguin E. Empirically supported treatment’s impact on organizational culture and climate. Research on Social Work Practice. 2012;22(6):665–671. doi: 10.1177/1049731512448934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson DA, Dulmus CN, Maguin E. Is Openness to Using Empirically Supported Treatments Related to Organizational Culture and Climate? Journal of Social Service Research. 2013;39:562–571. doi: 10.1080/01488376.2013.804023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson DA, Dulmus CN, Maguin E, Cristalli ME. Factors influencing worker morale: Evaluating provider demographics, workplace environment and using ESTs. Research on Social Work Practice. 2013;23(3):302–308. [Google Scholar]
- Patterson DA, Maguin E, Dulmus CN, Nisbet BC. Individual worker level attitudes toward empirically supported treatments. Research on Social Work Practice. 2013;23(1):95–99. doi: 10.1177/1049731512463442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phillips-Morrow G, Burris-Kitchen D, Der-Karabetian A. Assessing campus climate of cultural diversity: A focus on Focus Groups. College Student Journal. 2000;34:589–606. [Google Scholar]
- Raghavan R, Inoue M, Ettner SL, Hamilton BH. A preliminary analysis of the receipt of mental health services consistent with national standards among children in the child welfare system. American Journal of Public Health. 2010;100(4):742–749. doi: 10.2105/AJPH.2008.151472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rentsch JR. Climate and culture: Interaction and qualitative differences in organizational meaning. Journal of Applied Psychology. 1990;75:668–681. [Google Scholar]
- Rosen AK, Singer S, Zhao S, Shokeen P, Meterko M, Gaba D. Hospital safety climate and safety outcomes: Is there a relationship in the VA? Medical Care Research and Review. 2010;67:590–608. doi: 10.1177/1077558709356703. [DOI] [PubMed] [Google Scholar]
- Ross AL. Transformation education: A vehicle for structuring group care organizations to increase service quality and effectiveness. Residential Treatment for Children and Youth. 2008;24:131–157. [Google Scholar]
- Schuh SC, Zhange X, Egold NW, Graf MM, Pandey D, van Dick R. Leader and follower organizational identification: The mediating role of leader behavior and implications for follower OCB. Journal of Occupational and Organizational Psychology. 2011;85:421–432. [Google Scholar]
- Shadur MA, Kienzle R, Rodwell JJ. The relationship between organizational climate and employee perceptions of involvement. Group & Organization Management. 1999;24:479–503. [Google Scholar]
- Shim M. Factors influencing child welfare employee’s turnover: Focusing on organizational culture and climate. Children and Youth Services Review. 2010;32:847–856. [Google Scholar]
- Singer S, Lin S, Falwell A, Gaba D, Baker L. Relationship of safety climate and safety performance in hospitals. Health Services Research. 2009;44:399–421. doi: 10.1111/j.1475-6773.2008.00918.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weisz JR, Chorpita BF, Palinkas LA, Schoenwald SK, Miranda J, Bearman SK, Daleiden EL, et al. Testing standard and modular designs for psychotherapy treating depression, anxiety, and conduct problems in youth: A randomized effectiveness trial. Archives of General Psychiatry. 2012;69(3):274–282. doi: 10.1001/archgenpsychiatry.2011.147. [DOI] [PubMed] [Google Scholar]
- Zima BT, Hurlburt MS, Knapp P, Ladd H, Tang L, Duan N, Wallace P, et al. Quality of publicly-funded outpatient specialty mental health care for common childhood psychiatric disorders in California. Journal of the American Academy of Child and Adolescent Psychiatry. 2005;44(2):130–144. doi: 10.1097/00004583-200502000-00005. [DOI] [PubMed] [Google Scholar]
- Zohar D, Luria G. Group leaders as gatekeepers: Testing safety climate variations across levels of analysis. Applied Psychology: An International Review. 2010;59:647–673. [Google Scholar]