

Abstract
Early psychosocial adversities exist at many levels, including caregiving-related, extrafamilial, and sociodemographic, which despite their high interrelatedness may have unique impacts on development. In this paper, we focus on caregiving-related early adversities (crEAs) and parse the heterogeneity of crEAs via data reduction techniques that identify experiential cooccurrences. Using network science, we characterized crEA cooccurrences to represent the comorbidity of crEA experiences across a sample of school-age children (n = 258; 6–12 years old) with a history of crEAs. crEA dimensions (variable level) and crEA subtypes (subject level) were identified using parallel factor analysis/principal component analysis and graph-based Louvain community detection. Bagging enhancement with cross-validation provided estimates of robustness. These data-driven dimensions/subtypes showed evidence of stability, transcended traditional sociolegally defined groups, were more homogenous than sociolegally defined groups, and reduced statistical correlations with sociodemographic factors. Finally, random forests showed both unique and common predictive importance of the crEA dimensions/subtypes for childhood mental health symptoms and academic skills. These data-driven outcomes provide additional tools and recommendations for crEA data reduction to inform precision medicine efforts in this area.
Keywords: caregiving related early adversities, heterogeneity, prediction, subtyping
Childhood adversities are the leading preventable environmental risk factors in cognitive and mental health development (Benjet et al., 2010; Clark et al., 2010; Kessler et al., 2010; McLaughlin et al., 2012; Wade et al., 2019). There are many sources/types of adversities (e.g., Aber, 2013; Cicchetti et al., 2000) – at the family, socioeconomic, and community levels – which despite interacting and often cooccurring, may have unique impacts on development. Here, we focus on caregiving-related early adversities (crEAs), which include adverse experiences that directly undermine the parent-child relationship, including caregiver-involved maltreatment and separations from caregivers. In contrast to other childhood adversities, crEAs represent interruptions, separations, and/or dysfunctions in the parent-child transactional system (Cicchetti & Rizley, 1981; Sameroff & Chandler, 1975) and can disrupt the developmental processes that play a foundational role in emotional and cognitive health (discussed in Cicchetti & Toth, 2005; Tottenham, 2020). Yet, there is heterogeneity within crEAs that may predict unique outcomes. (e.g., Manly et al., 2001; McLaughlin et al., 2014; Trickett & McBride-Chang, 1995). Here, we aimed to parse the heterogeneity of crEAs by identifying stable patterns of cooccurrence in a heterogeneous sample highly enriched for crEA exposure.
Experiential heterogeneity is a significant and long-recognized challenge in the literature on childhood adversity (Cicchetti & Rizley, 1981; see Smith & Pollak, 2021). One common approach for reducing this heterogeneity is to identify patterns of experiential cooccurrences. At the variable level, studies of community samples that use factor analysis (FA) often identify a household dysfunction type factor (Green et al., 2010; Scott et al., 2013), but findings can differ for other factors. These differences may reflect study-specific definitions of adversity and/or assessment methods, demographic characteristics, and/or unstable factor structures. At the individual level (i.e., subtypes) latent class/profile analysis (LCA) has most often been used and has identified (i) multiple-item subtypes (commonly involving indices of household dysfunction), (ii) the presence/absence of sex abuse being a defining subtype feature, and (iii) emotional maltreatment and/or neglect being common across subtypes (Berzenski & Yates, 2011; Brown et al., 2019; Hazen et al., 2009; Pears et al., 2008; Petrenko et al., 2012; Warmingham et al., 2019). Dimensions/subtypes of cooccurrence serve the function of identifying crEAs homogeneity based on which experiences are likely to cooccur for a given child. The goal of this type of heterogeneity reduction is different from process-oriented approaches that aim to identify homogeneity based on distinct “kinds” (e.g., psychological/physical; threat/deprivation; abuse/neglect; predictability; fragmentation) with the aim of revealing pathways through which various experiences operate (Baram et al., 2012; Belsky et al., 2012; Herzog et al., 2020; Infurna et al., 2016; Ivy et al., 2008; Sheridan & McLaughlin, 2014). Thus, consideration of both parameterized crEA cooccurrences and of parameterized “kinds” may improve investigations of crEA effects by contextualizing crEAs in their naturally occurring state (i.e., which crEAs are likely to occur together for a child) and identifying the mechanisms through which crEAs predict outcomes, respectively.
Here, we took advantage of new advances in statistical approaches to focus specifically on cooccurrences of adversities that exist within the context of the caregiver-child relationship. To better characterize the heterogeneity of crEA exposure and associated polyvictimization (Finkelhor et al., 2007; Ney et al., 1994), children included in this sample were broadly sampled for crEAs, and included children with a history of foster care (non-familial, domestic), kinship care (domestic), foster care (abroad), previous institutional care (abroad), and/or caregiving disruptions followed by reunion with biological parents. These groups may commonly be understood as belonging to separate experiential categories, defined by socio-legal boundaries (SLgroups), yet they all share the experience of significant disruptions to the parent-child relationship. Without a formal examination of cooccurrences across SLgroups, we are left asking whether findings from on SLgroup (e.g., institutional care) could generalize to another (e.g., domestic foster care). Experiential cooccurrences have not been examined across these groups; here, we bring these groups together in a single investigation because by doing so, we may uncover experiential crEA dimensions and subtypes that transcend SLgroups and provide new insight into the properties of crEAs that transcend these socio-legal boundaries.
An important limitation of using SLgroups (or other investigator-defined groups) in research is they may not recognize within-population differences (e.g., the prevalence of one type of crEAs may vary within one population), and at the same time, they may not recognize between-population similarities (e.g., domestic foster care experiences may share features with institutional care abroad experiences). Such approaches may also fail to adequately represent the full set of crEAs a child experienced (Smith & Pollak, 2021). For example, children who have experienced institutional care have also experienced multiple other crEAs, including (a) abandonment/parental separation, (b) emotional neglect, (c) physical neglect, and/or (d) supervisory neglect (among other possible adversities) (Groark & McCall, 2011; Groark et al., 2011; Gunnar et al., 2000; van IJzendoorn et al., 2020). Here, we apply data-driven approaches to both the reported and coded information about all possible crEA experiences encountered, regardless of SLgroup, and subject these crEAs to empirically based tools to define homogenous crEA subtypes.
Examining crEAs at the level of SLgroups (or other investigator-defined groups) also increases the risk of introducing sociodemographic confounds (i.e., socioeconomic status [SES], race (Lacey et al., In Press; Maguire-Jack et al., 2020)) that might be mechanistically distinct from crEAs. Using network science, we characterized the cooccurrence of crEA experiences across a highly heterogeneous sample to represent the comorbidity of crEA experiences (Finkelhor et al., 2007; Ney et al., 1994) in both dimensional and subtype form. While doing so, we also aimed to weaken the link with sociodemographics (e.g., SES; race). Univariate approaches are not designed for this task because: (i) there is a tradeoff between model simplicity and adequate representation of variance in the data, (ii) sociodemographics are typically embedded into a given SLgroup (note: regressing these variables “out” is insufficient and does not really remove their effect), (iii) SES is itself highly dimensional, (iv) there is heightened potential for statistical inflation due to high comorbidity between variables (although see counterresponse in McLaughlin et al., 2021; Smith & Pollak, 2021), and (v) it is unknown whether the regressed-out variable is the actual agentic variable.
Network science can identify stable dimensions/subtypes of crEA cooccurrence that transcend traditional socio-legal nosologies (Cohodes et al., 2021; Fair et al., 2012; Insel & Cuthbert, 2015; Karalunas et al., 2014; Sheridan et al., 2020) and address the challenge of confounding sociodemographics (Kim & Drake, 2018). Dimensional approaches posit that dimensions (e.g., psychological/physical; threat/deprivation; abuse/neglect; predictability/unpredictability; fragmentation) have specific developmental effects on distinct neural circuits (McLaughlin et al., 2021). Dimensions operate by creating continua of variables, unlike subtyping which creates groups of individuals; thus subtyping is a step necessary for making predictions and tailoring treatments/support for the individual (Pears et al., 2008). The utility and explanatory power of dimensions (variable level) are enhanced via creation of homogenous subtypes (subject level) (Feczko & Fair, 2020; Feczko et al., 2019), which can be used in conjunction with dimensions for predictive modeling (Chabernaud et al., 2012; Nikolaidis, DeRosa, et al., 2021; Nikolaidis, Paksarian, et al., 2021; Tang et al., 2020).
Our Aim 1 was to characterize the dimensionality of crEA cooccurrence (variable level) in a broad range of SLgroups at greatest risk for significant and heterogeneous crEA experiences. Towards this end, we used FA to identify the crEAs dimensional structure (and confirmed it with separate PCA). In addition, to ensure that factors were robust to within-sample heterogeneity, we incorporated bootstrap resampling (“bagging”-enhancement with cross-validation). Bootstrap resampling assesses variability in the variable loadings for each dimension, providing an estimate of which variables reliably contribute to each component/factor and thus increasing the stability of crEA dimensions. Aim 2 was to find subtypes of crEA cooccurrence (individual level) that are independent from SES and also show reduced subgroup heterogeneity compared to SLgroups.Towards this end, we used graph-based Louvain community detection (Blondel et al., 2008) to identify homogeneous subtypes based on similar crEA profiles. This network analytic approach can discover groups of individuals that have experienced similar crEA exposures regardless of SLgroup. Louvain community detection uses an iterative modularity-optimizing procedure to identify homogenous groups of individuals, and subtypes are data-driven rather than based on a priori assumptions. We then tested whether associations between the observed dimensions/subtypes and specific outcomes (mental health, academic skills) were strengthened by the use of these data-driven approaches. The window of crEA exposure for this sample occurred anytime between birth and middle childhood, and the outcomes were measured during the school-age period (ages 6–12 years). Finally, Aim 3 was to compare prediction of mental health and academic skills outcomes using crEA dimensions and subtype information. To accomplish this, we conducted a conditional random forest analysis predicting measures of mental health and academic skills. We applied this approach using different subsets of predictor variables and assessed the relative predictive accuracy of these models as well as the ranked variable importance of each of the models in predicting mental health and academic skills.
Method
Participants
258 children (6–12 years old) were part of a larger, ongoing longitudinal neuroimaging study on crEA (see Supplemental Material for details on recruitment). Children with a history of significant crEA exposure (n = 184) were recruited from SLgroups that were expected to be enriched for crEAs (i.e., maltreatment and/or disruptions in caregiving) (see Table 1 and Supplementary Table 2). Additionally, a comparison group (n = 74) was included who had no reported crEA exposure. Exclusion criteria included autism or severe intellectual disability that precluded study participation and significant neonatal complications. The sample was racially/ethnically diverse (35% European-American/White, 30% African-American/Black, 15% > 1 race, 10% Asian-American, 1% Native American, 10% “other”; 29% Hispanic/Latinx). Median yearly household income was $95,000 (range: $10,000–$800,000) for the crEA-exposed sample and $75,000 (range: $10,000–$780,000) for the nonexposed comparison sample. Mean parental education was 16 (crEAs) and 16.25 years (comparisons), indicating that the average parent had completed a 4-year college degree. Primary caregivers who were interviewed and completed questionnaires included biological parents (16%), adoptive parents (80%), or other formal caregivers (2%) for the crEA-exposed youth, and biological parents (100%) for the comparison group.
Table 1.
Sample information
| Demographics | Clinical and academic achievement test scores | ||||||
|---|---|---|---|---|---|---|---|
| Age Mean (years) | Age range (years) | Sex | CBCL total (T Scores) | WASI FSIQ | WIAT reading | WIAT number | |
| Full crEA sample | M = 9.05 | 6:12 | N = 184 | M = 55.83 | M = 97.91 | M = 41.77 | M = 38.65 |
| SD = 1.99 | 97F/85M | SD = 13.23 | SD = 13.50 | SD = 30.89 | SD = 27.52 | ||
| DA | M = 8.72 | 6:12 | N = 88 | M = 59.85 | M = 94.48 | M = 37.05 | M = 34.16 |
| SD = 1.75 | 40F/48M | SD = 13.0 | SD = 12.20 | SD = 29.59 | SD = 26.47 | ||
| DC | M = 9.06 | 6:12 | N = 36 | M = 52.33 | M = 97.66 | M = 41.30 | M = 40.31 |
| SD = 2.33 | 22F/14M | SD = 12.55 | SD = 13.49 | SD = 29.10 | SD = 26.74 | ||
| PI | M = 9.51 | 6:12 | N = 51 | M = 51.55 | M = 102.74 | M = 48.47 | M = 44.31 |
| SD = 2.06 | 31F/20M | SD = 12.70 | SD = 13.60 | SD = 33.47 | SD = 28.24 | ||
| IFC | M = 9.86 | 7:12 | N = 7 | M = 55.14 | M = 104.14 | M = 50.43 | M = 42.43 |
| SD = 1.86 | 4F/3M | SD = 12.55 | SD = 17.09 | SD = 29.84 | SD = 21.82 | ||
Note. We summarize the relevant demographic, clinical, and cognitive characteristics of the current sample. Rows describe these characteristics in the full sample and across each of the individual SLgroups. The sample was comprised of a roughly even split across the sexes, with most children between 6–12 years of age. CBCL = Child Behavioral Checklist; DA = domestic adoption; DC = disrupted caregiving; FSIQ = full scale intelligence quotient; IFC = International Foster Care; PI = previously institutionalized; SLgroups = sociolegally defined groups; WASI = Wechlser abbreviated scale intelligence; WIAT = Wechsler individual achievement.
Materials
Caregiving-related early adversities
crEAs were assessed through semistructured interviews and a questionnaire (see Supplementary Table 1 for description of crEAs used in this paper). The Maternal Interview for Childhood Maltreatment (MICM; Cicchetti et al., 2003) assesses the lifetime presence of maltreatment subtypes through an interview with the parent. For the purpose of this paper’s focus on crEAs, we only included endorsements if they involved a primary caregiver. The term “parent” in this paper refers to any adult who was the primary caregiver of the child. crEAs were coded from parents’ narratives using the manualized Maltreatment Classification System (Cicchetti & Toth, 1993). The MICM provides information on subtype, timing, relationship to child, occurrence of separations and placements, and severity of incidents. Note, in this paper, emotional abuse (acts of commission) and emotional neglect (acts of omission) were coded separately (rather than the MICM’s combined score for emotional maltreatment). The Traumatic Events Screening Inventory (TESI; Ford et al., 2002) is a 24-item parent-completed questionnaire that measures lifetime occurrence of exposure to trauma. We also added two items relating to children living with a caregiver with severe mental illness or problematic alcohol/drug use. The TESI also assesses developmental timing and relationship of child to perpetrator (when relevant). Only events related to the caregiver (i.e., crEAs) were used in the current paper. Additionally, parents were interviewed about their children’s caregiving placement histories with an in-house calendar-style instrument that provided information about number and timing of caregiving placements. Interviews were administered by trained master’s students in Clinical Psychology, with supervision by C.H. For the purpose of the current study, we used the dichotomous variables (presence/absence) of crEAs (see Figure 1 for variables included, Supplementary Table 1 for descriptions of crEAs, and Supplementary Table 2 for frequency of crEAs). Variables labeled “TESI/MICM” are crEAs endorsed either through the TESI and/or MICM. Note that crEAs were coded as such regardless of parental agency or intent.
Figure 1.
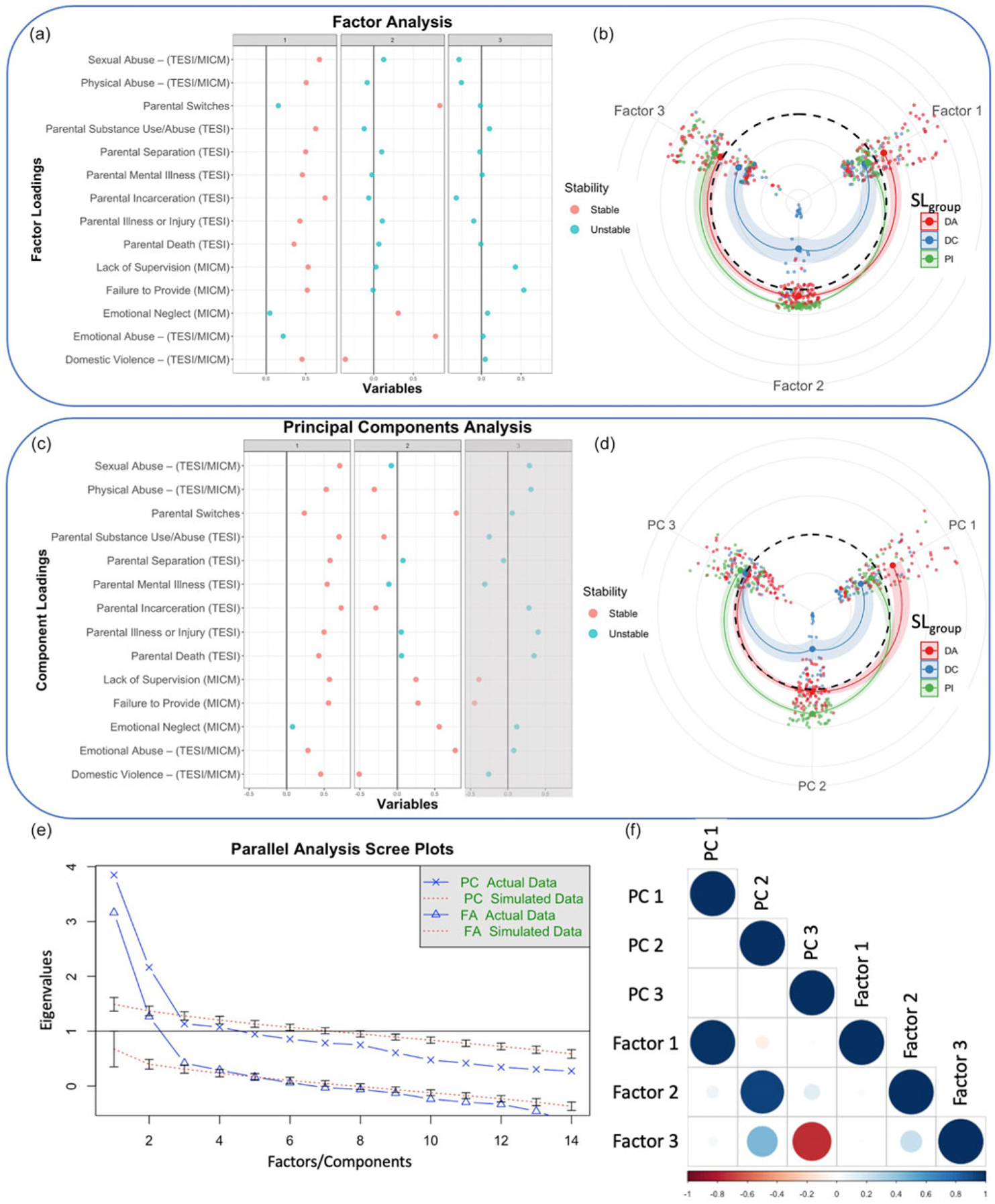
Full sample FA and PCA: (a) Factor analysis (FA). Caregiver-related early adversities (crEA) variables are shown on the y-axis, and variable loadings are shown across the first four principal factors on the x-axis. Note that the scree plot in E indicated that the first four were all significant. We labeled variables as unstable (blue) if the 95% confidence interval of the loading distribution across 1000 bootstraps included zero. We labeled variables as stable (red) when they did not. (b) Individual participant loadings on each of the FAs grouped by SLgroup (DA = domestic adoption; DC = disrupted caregiving; PI = previous institutional care) (note: IFC was not included here due to small sample size. Dashed circle represents the sample average score. (c) Principal component analysis (PCA). Variable loadings of the first four components. Note that the scree plot in E indicated that the first two factors were significant. (d) Individual participant loadings on each of the FAs grouped by SLgroup. Dashed circle represents sample average score. (e) Parallel analysis scree plot showing only the first two PCs have greater eigenvalues than the null distribution while the FA eigenvalues are greater than null for the first four factors. (f) Correlation matrix between the first four PCs and FAs. We see a very high correspondence (Pearson’s r = .899; r = .905) between the first two FA/PCs, respectively and moderate correlation between FA and PCs 3. Factor One: Additive Exposure. Factor Two: Emotional Maltreatment (without Domestic Violence) Factor Three: Physical/Supervisory Neglect. Sexual Abuse, Physical Abuse, and Emotional Abuse were all coded as either experiencing or witnessing through either TESI or MICM. Domestic Violence was coded as either experience or threat through either TESI or MICM. MICM = Maternal Interview of Childhood Maltreatment; TESI = Traumatic Events Screening Inventory.
Demographics and income
Parents provided information about their child’s race and ethnicity, education of current primary caregiver, and current household income. Children were also administered two subtests (vocabulary and matrix reasoning) of the Wechsler Abbreviated Scale of Intelligence (Wechsler, 1999) to obtain estimated IQ for demographic purposes only.
Child outcomes
To index the overall extent of mental health symptoms, the Total Score from the parent-completed Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001) was used. Children’s academic achievement was assessed with the Wechsler Individual Achievement Test (WIAT-III; Vaughan-Jensen et al., 2011). Outcome scores used (CBCL and WIAT-III) were age-standardized before analysis.
Procedure
Families visited the laboratory where parents completed questionnaires and interviews about their child, while children were administered task assessments and participated in MRI scanning in separate rooms. Based on scanner availability, some children completed task assessments before scanning, while others completed task assessments afterward.
Multivariate models of crEA heterogeneity
Aim 1.
To identify dimensions of crEA cooccurrence, we applied a bagging-enhanced FA and principal components analysis (PCA) approach with 10,000 bootstrap resampled models aggregated. Bagging allowed us to address problems of sample variance in multivariate models and thereby improve their stability (Breiman, 1996; Nikolaidis et al., 2020). Through aggregating factor loadings across multiple models, the most important and robust crEAs within each factor can be determined, improving interpretability of our models. To choose the number of significant factors to assess in our study we used parallel analysis, a permutation testing method for FA and PCA (Horn, 1965). We used individual items from the MICM and TESI to calculate the FA and PCA. When items were highly redundant, we counted either endorsement. Physical abuse, sexual abuse, domestic violence, and emotional abuse were coded in this way.
Aim 2.
To examine whether homogenous crEA cooccurrence subtypes could be created, we applied Louvain community detection using the Phenograph package in R to the patterns of crEA exposure across all participants. LCA is an established probabilistic clustering method developed over 70 years ago (Vermunt & Magidson, 2004). LCA has been known to be sensitive to group differences but can be problematic when data are more variable (Green, 2014). LCA is a top-down approach that makes assumptions of the distribution of the data and the existence of latent (unobserved) classes in the data, for which each individual is given a probability of assignment. More recently, many researchers have become interested in the use of Louvain community detection as a graph-based algorithm for discovering clusters of individuals. We have previously established a pipeline for creating highly reproducible clusters through Louvain community detection (Nikolaidis, DeRosa, et al., 2021; Nikolaidis, Paksarian, et al., 2021), and in the current work, we have employed this reliability optimized pipeline to bear on the issue of subtypes in crEAs. Additional details on Louvain community detection are provided in the Supplemental Materials.
Aim 3.
Finally, to investigate the relative importance of crEA exposure to later outcomes, we applied random forests to predict CBCL Total Score and WIAT Reading and WIAT Numbers. We used crEA dimensions, crEA subtypes, individual crEAs, and SES variables as predictors. Random forest assesses out-of-sample prediction accuracy – this means that the prediction of each tree is based solely on the participants not used to create the decision tree. Therefore, on average, by aggregating across all trees, random forest assesses the out-of-sample prediction accuracy. To compare the informativeness of our predictions against an appropriate “null,” we shuffled our predictor and target variables 1000× and repeated the prediction for each of our target variables.
Results
Aim 1. Identifying dimensions of crEAs across SL groups
FA revealed three dimensions of crEA exposure (Figure 1a), which held significantly more variance than would be expected due to chance (Figure 1e). The factor loadings shown in Figure 1a reveal a largely additive exposure factor, representing exposure to a majority of the crEAs (Factor 1: Additive Exposure), with a notable exception of emotional abuse, emotional neglect, and parental switches. Instead, the second factor selectively loaded onto these three crEAs (Factor 2: Emotional Maltreatment without Domestic Violence). High positive scores on Factor 2 reflected higher likelihood of exposure to emotional maltreatment, and more negative scores reflected higher likelihood of exposure to domestic violence. Notably, Factors 1 and 2 were uncorrelated (Figure 1f), suggesting orthogonality of the two experiential dimensions. Factor 3 (Physical/Supervisory Neglect) showed large positive loadings on failure to provide and lack of supervision, although the bagging enhancement indicated that this factor was not stable. The pattern of factor loadings was largely reproduced in a parallel PCA (Figure 1b). Notably, the first two principal components, which were determined to be significant based on the Parallel Analysis (Figure 1e), were nearly identical to the first two factor loadings (PC1-FA1 Pearson correlation = 0.899; PC2-FA2 Pearson Correlation = 0.905) (Figure 1f), suggesting that these crEA dimensions were robust across different dimensional approaches. The factors/components showed some discrimination between SLgroups and also showed distribution across SLgroups. For example, in Figure 1b and d note that the domestic adoption group scored on average highest in the first factor/component, but also showed the highest within-group heterogeneity (spread of individual participant loadings).
Aim 2. Creating homogeneous subtypes using specific crEA exposures
In addition to identifying crEA dimensions, we created crEA subtypes. Subtyping individuals by crEAs is important because it facilitates prediction at the individual level. That is, we may find that one previously institutionalized child has more in common, in terms of crEAs, with a child who experienced domestic adoption than she/he does with another previously institutionalized child. Louvain community detection was used to find subtypes of archetypal “exposure profiles” that explained the heterogeneity in crEAs. The LCD solution had a modularity Q score of 0.51, reflecting the considerable heterogeneity of the crEA data. Figure 2a shows a correlation matrix of crEA profiles with the rows and columns ordered according to agglomerative hierarchical clustering. Columns are colored according to the initial SLgroups, while the rows are colored according to resulting crEA profile clusters from Louvain community detection. These clustering approaches highlight the experiential heterogeneity between individuals within the same SLgroup. For example, Figure 2a shows that the crEA Subtype 1 (orange) was composed of individuals from each SLgroup, a point made more explicit by Figure 2c. Figure 2b shows the distribution of crEAs across the subtypes and SLgroups (colored in the top two rows). Figure 2c shows the subtype heterogeneity across SLgroups, which were well-distributed across the five crEA subtypes. We calculated intersubject crEA profile correlations to assess if crEA subtypes resulted in improved group homogeneity, and Figure 2d shows that the SLgroups had significantly higher heterogeneity (p < .05) and lower inter-subject crEA profile correlation than the crEA subtypes. Figure 3a shows how each of the 5 subtypes loaded onto each of the three (dimensionalized) factors. Notably, we see that the three factors were more easily able to distinguish between crEA subtypes than SLgroups (comparing Figure 3a to Figure 1b and d). The clearer separation of subtypes in Figure 3a relative to the overlap of SLgroups within each factor in Figure 1b and d indicates the enhanced homogeneity of the crEA subtypes over the SLgroups, thus highlighting the large heterogeneity of SLgroups.
Figure 2.
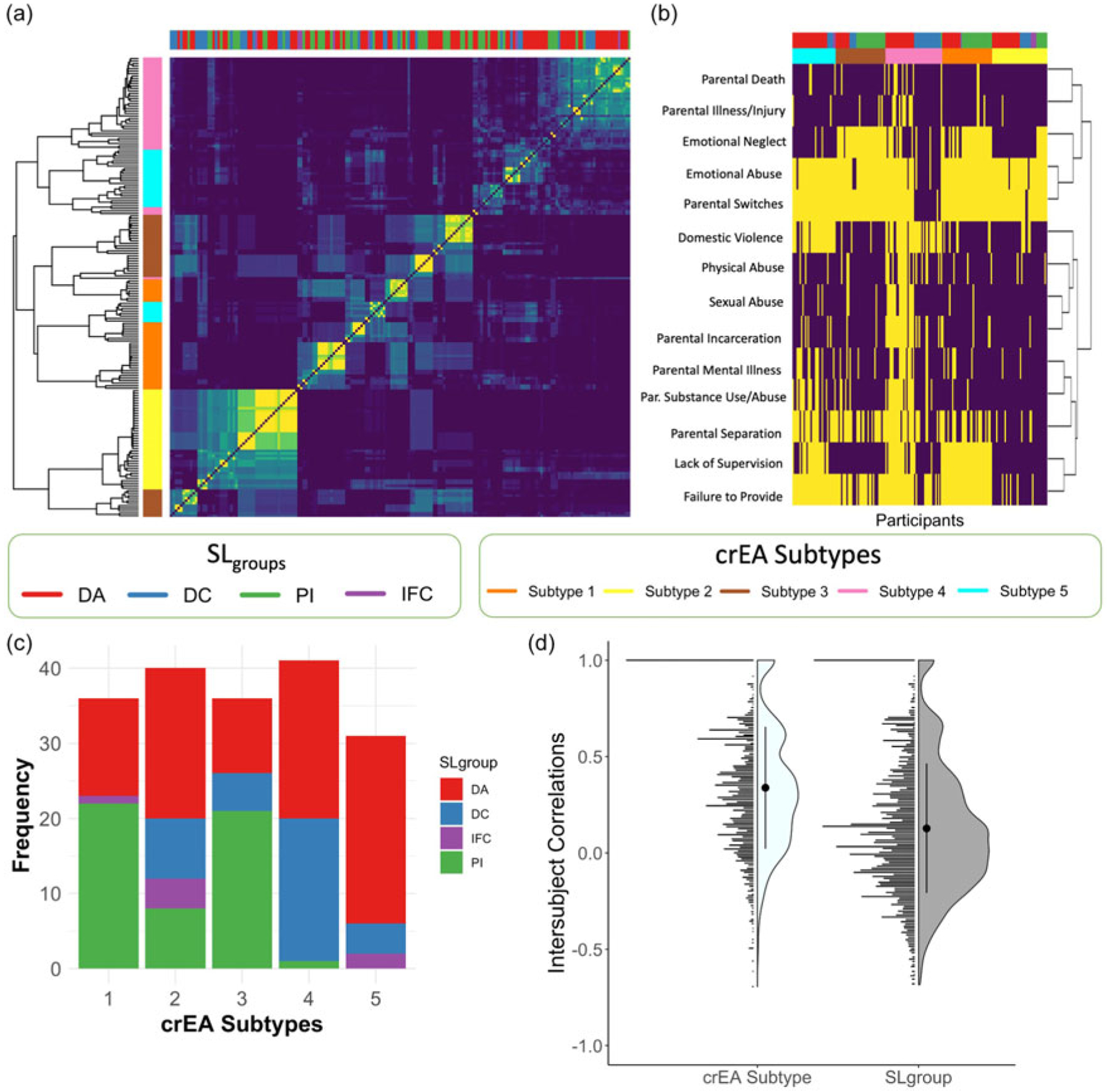
Subtyping. (a) Louvain community detection is used to find clusters of participants with similar exposure profiles to caregiver-related early adversities (crEAs). We show a correlation matrix across all participants. Yellow indicates two participants are highly similar in crEA exposure profiles. Cell(i,j) corresponds to the similarity in exposure profile between participant i and participant j. The topmost row color codes participants by their socio-legal groups SL(groups) (DA: red, DC: green, PI: blue, IFC: purple), while column to the left of that color codes participants by their exposure profile cluster (Cluster 1: purple, Cluster 2: light blue; Cluster 3: brown; Cluster 4: yellow). Rows and columns are organized by hierarchical agglomerative clustering. Notably we see that all crEA profile clusters are made up of individuals from multiple SLgroups, demonstrating heterogeneity of adversities in each exposure environment. (b) Hierarchical clustering was applied to show how crEAs cluster together and how these crEAs clusters are distributed across the individual participants, across the crEAs profile clusters, and SLgroups. The Y-axis shows all crEAs, and the X-axis shows the crEAs scores (yellow=presence, purple=absence) for each individual participant. The topmost row color codes participants by their SLgroups, while the row underneath color codes participants by their crEA exposure profile cluster. Yellow indicates subjects are endorsed for a particular crEA. (c) We show how the four SLgroups are distributed across the four crEA profile clusters. (d) We show the intersubject correlations in crEA exposure profiles across the four SLgroups and crEA profile clusters. Sexual abuse, physical abuse, and emotional abuse were all coded as either experiencing or witnessing through either TESI or MICM. Domestic Violence was coded as either actual or threat through either TESI or MICM. MICM = Maternal Interview of Childhood Maltreatment; TESI = Traumatic Events Screening Inventory.
Figure 3.
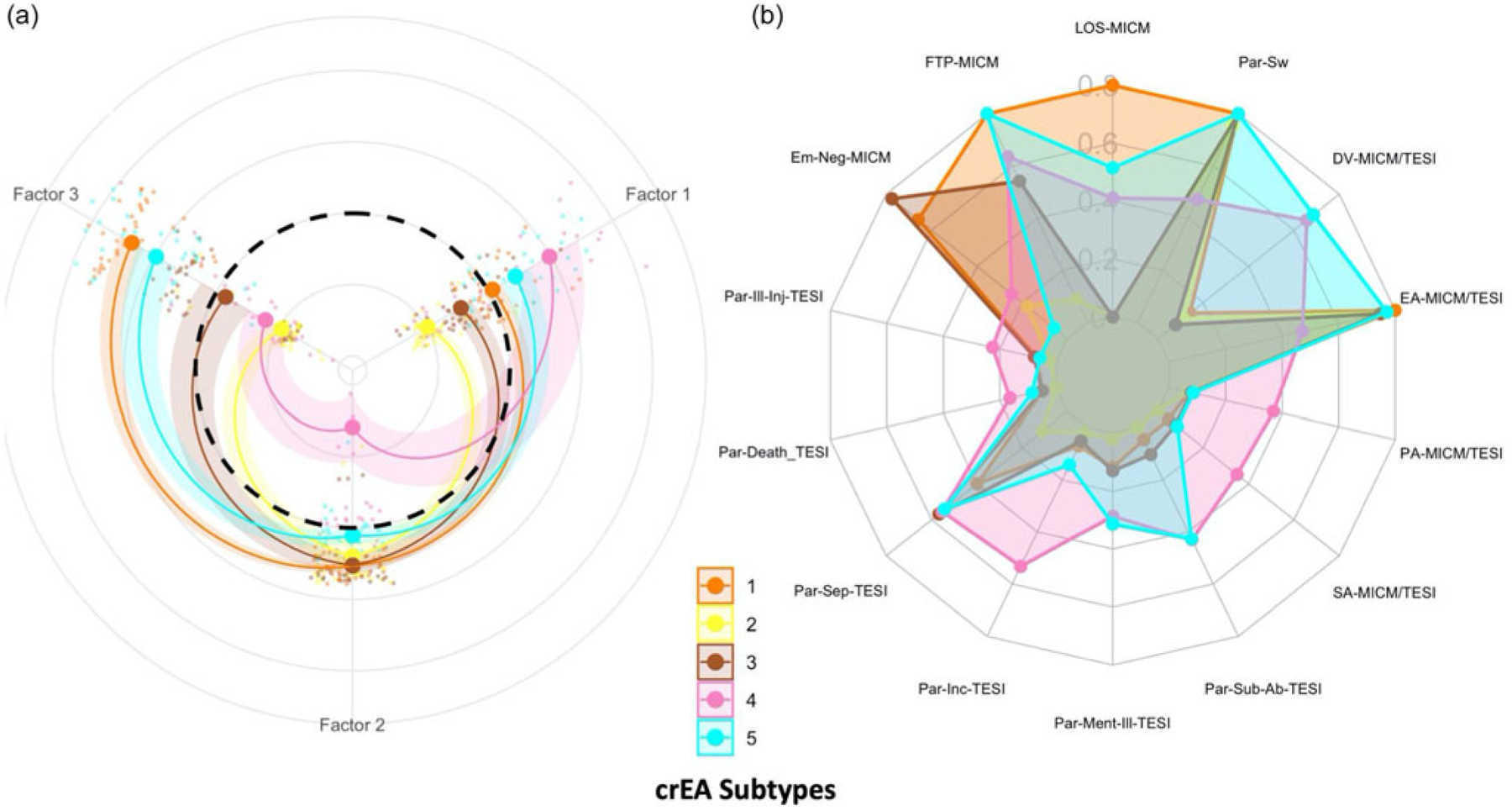
crEA subtypes. (a) Factor 1: Additive Exposure; Factor 2: Emotional Maltreatment without Domestic Violence; Factor 3: Physical/Supervisory Neglect. Subtype 1 showed highest scores on Factor 3. Subtypes 2 and 3 showed low scores on Factor 3 and Factor 1 but higher than average scores on Factor 2. Subtype 4 had the highest scores on Factor 1 and lowest on Factor 2, suggesting high exposures to domestic violence. Subtype 5 showed second highest scores in the Factor 1 and Factor 3. The dashed circle indicates the sample average for each factor score. (b) We show how the five crEA subtypes loaded onto each of the individual crEA exposures. MICM = Maternal Interview on Child Maltreatment; TESI = Traumatic Events Screening Inventory. LOS-MICM = Lack of Supervision (MICM); Par-Sw = Parental Switches; DV-MICM/TESI = Domestic Violence – Threat or Actual (MICM/TESI); EA-MICM/TESI = Emotional Abuse (MICM/TESI); PA-MICM/TESI = Physical Abuse – Threat or Actual (MICM/TESI); SA-MICM/TESI = Experiencing and/or Witnessing Sexual Abuse (TESI); Par-Sub-Ab-TESI = Parental Substance Use/Abuse (TESI); Par-Ment-Ill-TESI = Parental Mental Illness (TESI); Par-Inc-TESI = Parental Incarceration (TESI); Par-Sep-TESI = Parental Separation (TESI); Par-Death-TESI = Parental Death (TESI); Par-Ill-Inj-TESI = Parental Illness or Injury (TESI); Em-Neg-MICM = Emotional Neglect (MICM); FTP-MICM = Failure to Provide (MICM). Sexual abuse, physical abuse, and emotional abuse were all coded as either experiencing or witnessing through either TESI or MICM. Domestic Violence was coded as either actual or threat through either TESI or MICM.
crEA subtyping not only identified greater experiential homogeneity, but it also avoided third variable confounds of noninterest. In other words, Table 2 shows that SLgroups were significantly associated with non-crEA variables (e.g., current parental income and education, race) that are known to have substantial impact on children’s development, but may exert distinct impacts from crEAs on child outcome. These sociodemographic variables were more strongly linked to SLgroup than crEA subtype, and at the same time, the majority of crEAs tested (10 out of 14) were more strongly linked to crEA subtype than to the SLgroups.
Table 2.
Group comparisons
| SLgroups | crEA subtypes | Effect | ||
|---|---|---|---|---|
| Demographics | Household income | F = 31.34; p < .0001; eta = 0.35 | F = 4.87; p < .05; eta = 0.027 | SLgroups |
| Years of education primary caregiver | F = 15.62; p < .0001; eta = 0.21 | F = 4.767; p < .03; eta = 0.026 | SLgroups | |
| Sex | X-sq = 4.84; p > .05; eta = 0.049 | X-sq = 6.23; p > .05; eta = 0.062 | crEA subtypes | |
| Race | X-sq = 110.56; p < .0001; eta = 0.43 | X-sq = 56.91; p < .001; eta = 0.32 | SLgroups | |
| Caregiver early adversity (crEAs) | Lack of supervision (MICM) | X-sq = 24.36; p < .0001; eta = 0.19 | X-sq = 111.12; p < .0001; eta = 0.43 | crEA subtypes |
| Failure to provide (MICM) | X-sq = 18.43; p < .0005; eta = 0.15 | X-sq = 91.54; p < .0001; eta = 0.40 | crEA subtypes | |
| Emotional neglect (MICM) | X-sq = 87.27; p < .0001; eta = 0.39 | X-sq = 86.29; p < .0001; eta = 0.39 | == | |
| Parental illness or injury (TESI) | X-sq = 4.27; p > .05; eta = 0.043 | X-sq = 14.77; p < .01; eta = 0.13 | crEA subtypes | |
| Parental death (TESI) | X-sq = 4.49; p > .05; eta = 0.047 | X-sq = 11.36; p < .05; eta = 0.10 | crEA subtypes | |
| Parental separation (TESI) | X-sq = 4.23; p > .05; eta = 0.043 | X-sq = 35.74; p < .0001; eta = 0.25 | crEA subtypes | |
| Parental incarceration (TESI) | X-sq = 8.75; p < .05; eta = 0.083 | X-sq = 61.2; p < .0001; eta = 0.33 | crEA subtypes | |
| Parental mental illness (TESI) | X-sq = 18.46; p < .0005; eta = 0.15 | X-sq = 16.05; p < .005; eta = 0.14 | SLgroups | |
| Parental substance use/Abuse (TESI) | X-sq = 31.68; p < .0001; eta = 0.23 | X-sq = 50.99; p < .0001; eta = 0.30 | crEA subtypes | |
| Sexual abuse (MICM/TESI) | X-sq = 22.35; p < .05; eta = 0.18 | X-sq = 36.65; p < .0001; eta = 0.25 | crEA subtypes | |
| Physical abuse (MICM/TESI) | X-sq = 6.71; p > .05; eta = 0.066 | X-sq = 32.82; p < .0001; eta = 0.23 | crEA subtypes | |
| Emotional abuse (MICM/TESI) | X-sq = 81.30; p < .0001; eta = 0.38 | X-sq = 45.44; p < .0001; eta = 0.28 | SLgroups | |
| Domestic violence (MICM/TESI) | X-sq = 38.49; p < .0001; eta = 0.26 | X-sq = 92.30; p < .0001; eta = 0.40 | crEA subtypes | |
| Parental switches | X-sq = 92.25; p < .0001; eta = 0.40 | X-sq = 63.09; p < .0001; eta = 0.34 | SLgroups | |
| Factors | Additive exposure | F = 10.30; p < .0001; eta = 0.15 | F = 29.92; p < .0001; eta = 0.14 | SLgroups |
| Emotional maltreatment w/o DV | F = 76.95; p < .0001; eta = 0.56 | F = 30.46; p < .0001; eta = 0.14 | SLgroups | |
| Physical/supervisory neglect | F = 6.023; p < .001; eta = 0.091 | F = 1.43; p > .05; eta = 0.008 | SLgroups | |
Note. Summary of key demographic variables, caregiver-related early adversities (crEAs), and factor scores across all sociolegally defined groups (SLgroups) and data-driven crEA subtypes. Compared to crEA subtypes, SLgroups were more strongly linked to key SES related variables: Household Income, Years of Education for Primary Caregiver, while showing smaller effect sizes on 10/14 individual crEAs. MICM: sexual abuse, physical abuse, and emotional abuse were all coded as either experiencing or witnessing through either TESI or MICM. Domestic violence was coded as either actual or threat through either TESI or MICM. Maternal Interview on Child Maltreatment; TESI: Traumatic Events Screening Inventory.
Aim 3. Predicting childhood outcomes: Comparing methods
We compared the empirically derived crEA dimensions and crEA subtypes in their power to predict mental health symptoms (CBCL Total Score) and academic performance (WIAT Reading & Numbers) relative to SLgroups, individual crEAs, current household income, and caregiver education (Figure 3). We were able to predict out-of-sample outcomes with an R-squared of 33.2%, 24.9%, and 25.8% in predictions of CBCL Total Score, WIAT Reading, and Numbers, respectively (Figure 3). Prediction accuracy for these outcomes was all significantly higher than what would have been expected due to chance.
The variable importance plots clearly show that overall, dimensions were the most predictive of all outcomes. Factor 1: Additive Exposure was the most important in predicting scores across most outcomes, while Factor 2: Emotional Maltreatment without Domestic Violence and Factor 3: Physical/Supervisory Neglect varied in their relative importance depending on the outcome of interest. Note that household income by itself was also a reliable predictor of academic outcomes, independent of the crEA factors.
Figure 4 shows that the subtypes, while predicting CBCL, did not perform as well as the factors (i.e., dimensions). However, because subtypes are a necessary variable to complement dimensions in that they operate at the child level (rather than the variable level), we then assessed the predictive value of each subtype separately. Figure 5a compares their performance in predicting outcomes (i.e., variable importance) relative to SLgroups. crEA subtypes alone underperformed SLgroups in predicting outcomes (most likely because SLgroups are highly confounded with SES, which was a strong predictor). However, when crEA subtypes were tested with the addition of SES, prediction of outcomes was greatly improved (subsequently outperforming SLgroups). Whereas variable importance data tell us how accurately each variable predicts outcomes, Figure 5b presents the actual outcome scores per subtype. Relative to the comparison group (Comps) included for reference, crEA subtypes showed elevated scores on the CBCL and lower scores on the WIAT Numbers and WIAT Reading. We then compared each subtype to each other using random forests, which showed unique patterns of prediction (i.e., variable importances) across crEA subtypes, such that individual subtypes showed unique predictions depending on outcome of interest (Figure 5c).
Figure 4.
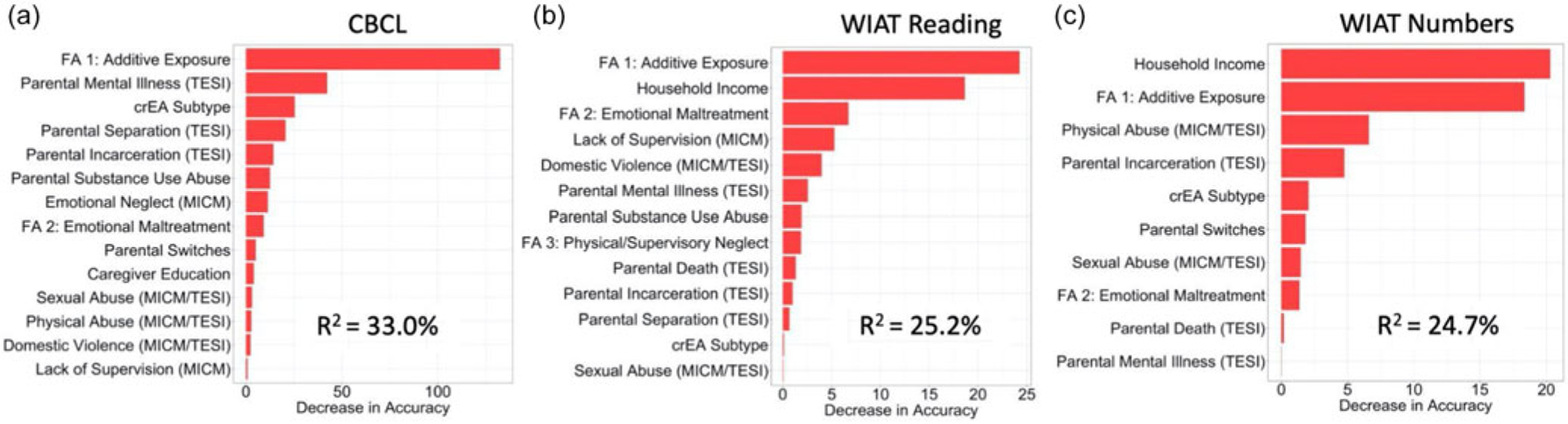
The individual crEAs and FA scores were used to predict three key outcomes (CBCL Total Score, WIAT Reading percentile, and WIAT Numbers percentile) in the sample using Random Forest. Each plot shows the ranking of variable importance in making the prediction in out-of-bag data. Note: Caregiver Education and Household Income reflect current values. Sexual abuse, physical abuse, and emotional abuse were all coded as either experiencing or witnessing through either TESI or MICM. Domestic Violence was coded as either actual or threat through either TESI or MICM.
Figure 5.
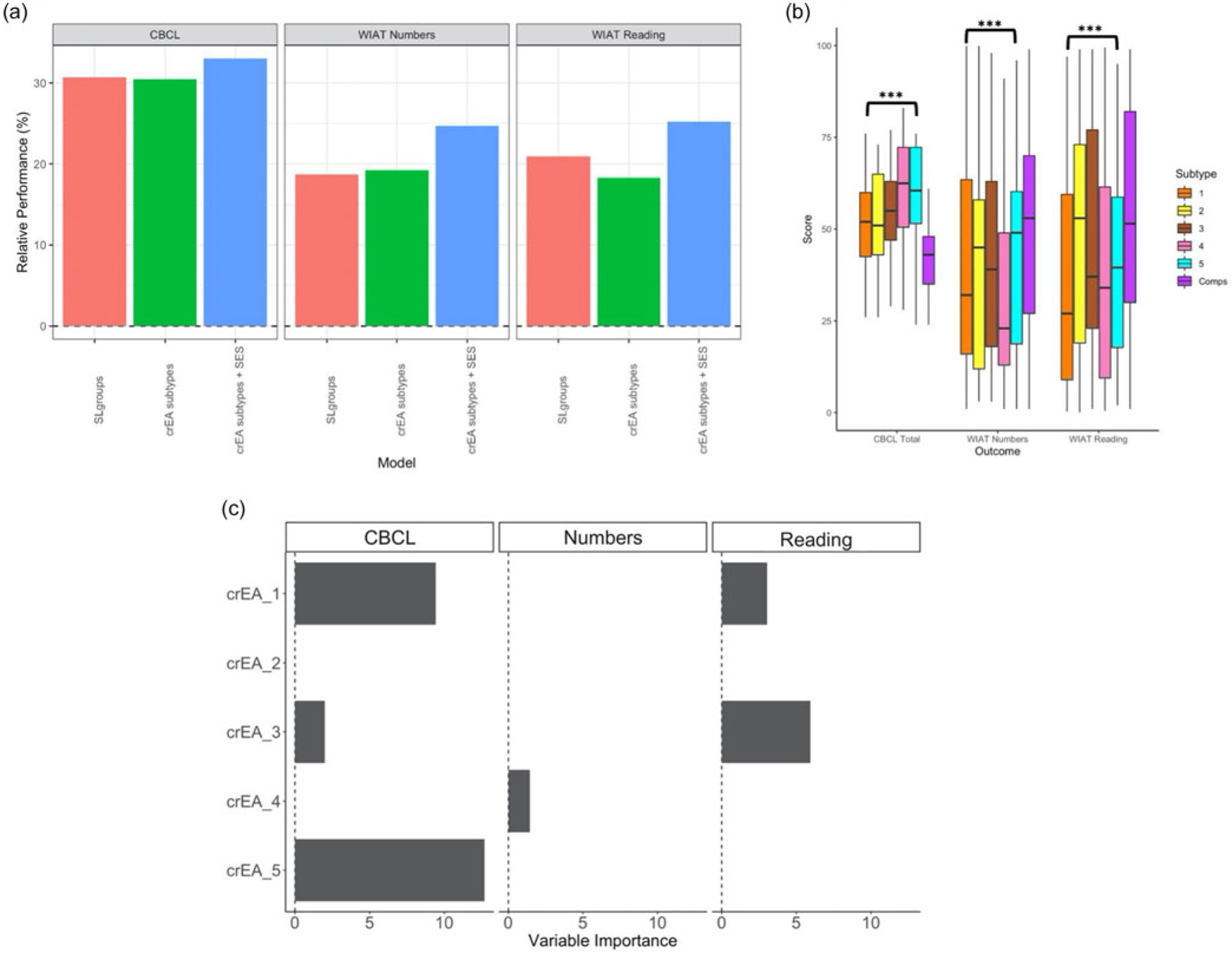
(a) We show the performance of SLgroups and crEA subtypes with and without adding in SES variables (Current Household Income, Parental Years of Education) in predicting CBCL, WIAT Numbers and WIAT Reading. (b) Distributions of crEA subtypes relative to a comparison group without crEA exposure across the three outcomes variables. ANOVA comparing comparison group to all crEA subtypes p < .0001 (***). (c) Variable importance values for each of the individual crEA subtypes in RF predictions with current SES. CBCL = Child Behavior Checklist; WIAT = Wechsler Individual Achievement.
Discussion
Aim 1. crEA dimensions show stability and cross sociolegally defined boundaries
Examining cooccurrences of crEAs through dimension reduction is an important first step towards understanding the natural patterns of crEA cooccurrence, especially in understudied and heterogeneous samples which may not be fully reflected in other studies. Three crEA cooccurrence dimensions were empirically derived. Even though aspects of the current study differed from the extant literature – by sampling from a broad range of SLgroups and exclusively focusing on caregiving-related adversities rather than a broader range of early adversities – we still found that the main dimensions of crEAs share similarities with previously established dimensional approaches. For example, Factor 1: Additive Exposure closely resembles the maladaptive family functioning identified in other samples (Green et al., 2010; Scott et al., 2013) and conceptually aligns with cumulative risk models (e.g., Sameroff & Chandler, 1975). Factor 2: Emotional Maltreatment without Domestic Violence also resembles the “emotional abuse and emotional neglect” maltreatment subtype identified by Matsumoto et al. (2020) in a recent meta-analysis. When comparing our work to previous results, it is important to note two things. First, the current sample may have included a broader range of SLgroups than what might have been used in other studies. This was an intentional decision that would allow for identifying dimensions that could transcend multiple and seemingly disparate SLgroups. Second, the dimensional and subtyping approaches used here exclusively focused on crEAs, whereas early adversity is often studied through a broader lens (e.g., other studies might include metrics of extrafamilial and/or sociodemographic adversities).
These three empirically derived dimensions revealed which events were more likely to occur together. Factor 3: Physical/Supervisory Neglect was the least stable, suggesting it was not as robust to sampling variability. Factor 1: Additive Exposure was largely an additive crEA exposure factor in that it contained all crEA items (except for those in Factor 2: Emotional Maltreatment without Domestic Violence – see Figure 1), as higher scores indicated a greater number of distinct crEA exposure types. Thus, the identification of Factor 1 supports the idea that grouping individuals by a single exposure do not accurately represent the range of crEAs experienced by a child. The loadings in this factor were robust within sample, as well as being consistent with other samples (Green et al., 2010; Scott et al., 2013). The robustness of this factor reflects the unfortunate reality that polyvictimization may be more common than singular exposures (e.g., Wolfe, 2018). Looking beyond the additive exposure factor, we found that some crEAs did not aggregate into the additive exposure factor. Namely, emotional abuse, emotional neglect, and caregiver switching (coded from interviews) loaded instead onto Factor 2: Emotional Maltreatment without Domestic Violence, perhaps reflecting the threats to attachment-related representations common across these items (Hornor, 2012; Spinazzola et al., 2014; Tonmyr et al., 2011). Unlike Factor 1, where one crEA exposure was more likely to cooccur with another crEA exposure, Factor 2 (which was uncorrelated with Factor 1) suggests that for some individuals, emotional maltreatment may be likely to occur in the absence of crEAs that load onto Factor 1.
Emotional maltreatment, despite being one of the most prevalent forms of child maltreatment (Pears et al., 2008), is often the most hidden form of maltreatment (Barnet et al., 2005; Hart & Brassard, 1987) and is considered by some to be the “core” issue in childhood trauma (Hart & Brassard, 1987). We deviated from the MICM coding by splitting emotional maltreatment into emotional abuse and emotional neglect for greater precision; nonetheless, Factor 2 supports the MICM’s combination of emotional neglect and emotional abuse. To be clear, our coding system included separation from a primary caregiver – regardless of the parental intent or agency (e.g., abandonment, death, or incarceration) or developmental timing as an incident of “emotional abuse,” which is often not coded as a form of emotional abuse. Our decision is consistent with the approach of coding the experience rather than parental intent/agency (Cicchetti et al., 2003), motivated by the importance of considering the even from the child’s perspective (Smith & Pollak, 2021). Thus, our definition of emotional abuse, while describing a caregiving-related adversity, does not necessarily mean the abuse is perpetrated by the caregiver. Separation from/abandonment by parents might be the most emotionally traumatic event in a child’s life (even if it is deemed necessary for the child’s well-being), yet it is unlikely to be reported by adoptive parents or court records as one of the many traumas experienced by a child (especially if the child experienced other forms of maltreatment)1. Note for example, that the frequency of “Separation from parent” as measured by parental questionnaire (i.e., TESI) was lower than “Parental Switches” frequency, which was coded from interviews with parents, although these measured the same type of event. From the young child’s perspective, the separation/removal would be a major threat to emotional well-being, consistent with the MICM’s code for emotional maltreatment. Note that emotional neglect did not load with physical/supervisory neglect (i.e., failure to provide and supervisory neglect) consistent with previous reports (Lambert et al., 2017); this lack of association provides empirical motivation to caution against treating neglect generically but instead recognizing that emotional neglect may have different phenomenological properties than physical/supervisory neglect. Bagging enhancement showed that Factor 2 was robust, and indeed, Factor 2 in this sample is highly consistent with a recent meta-analysis of the self-reported childhood maltreatment literature that also identified emotional maltreatment as a unique dimension of cooccurrence (Matsumoto et al., 2020). Taken together, these findings motivate continued inquiry into the merits of a caregiving-related emotional maltreatment dimension.
Leveraging best-practices in robust multivariate analysis to assess crEA cooccurrences, dimension reduction methods (FA, PCA) demonstrated that patterns of crEA cooccurrence not only replicated some aspects of previously established models but are also robust within our heterogenous sample. There was correspondence between the FA and PCA results, and the bagging enhancement provided confidence about the factor structure in the present sample. It is worth noting that variability in sampling of crEAs across studies may lead to differential crEA dimensions, but similarly broadly enriched samples for crEAs are more likely to yield similar results. We found that crEA dimensions (i.e., factors) both differed within a given SLgroup and transcended SLgroup borders, indicating that a given SLgroup is not homogeneous. Moreover, this transcendence indicates that seemingly distinct SLgroups may have common experience profiles that can inform our understanding of how to generalize findings from one crEA population to another. Indeed, homogeneity analysis of the crEA subtypes showed that there was greater cross-SLgroup than within-SLgroup similarity (i.e., a child with a history of domestic adoption could have more in common (in terms of crEAs) with a child previously institutionalized abroad than he/she might with another who experienced domestic adoption).
Aim 2. crEA subtyping shows increased homogeneity and reduced conflation with sociodemographics
Subtyping is an old and essential approach in medicine. Like dimensions, subtypes try to reduce experiential heterogeneity (Shorter & Tyrer, 2003; Wardenaar & de Jonge, 2013), but operate at the level of the individual rather than the variable. When describing dimensionality in a heterogeneous sample, subtyping provides valuable additional information on the organization of the sample. While dimensionality type analyses (FA/PCA) summarize the main patterns of the sample as a whole, subtyping allows for a breakdown of the data to examine more detailed patterns among subgroups. We found that the SLgroups were distributed across the crEA subtypes (i.e., crEA subtypes transcended SLgroups). The crEA subtypes demonstrated improved homogeneity over SLgroups, and they corresponded very well to the crEA dimensions (Figures 2 and 3a). These findings imply that the replicability of crEAs results will be improved by using crEA subtypes rather than SLgroups. These results also indicate that it is possible to translate back and forth between empirically defined dimensions and empirically derived subtypes, depending on the research question at hand (Chabernaud et al., 2012; Tang et al., 2020). Overall, the results of the data-driven community detection used in this study corresponded with many of the subtypes identified with other methods (e.g., logistic regression, latent class analysis) (Brown et al., 2019; Hazen et al., 2009; Pears et al., 2008; Petrenko et al., 2012; Warmingham et al., 2019). In future work, researchers may look to benchmark different methodological approaches and address the strengths and weaknesses of discrete (Louvain, k-means) versus probabilistic (latent class analysis, Gaussian mixture models).
We also found that data-derived subtypes of crEAs were less dependent on SES compared to SLgroups (Table 2), implying this data-driven approach is optimal when examining links between crEAs and outcomes because it avoids potentially misinterpreting crEAs’ effects that are actually SES effects. Diving deeper into these results through conditional random forest makes these implications clearer. Figure 5a shows that the performance of the crEA subtypes and the traditional SLgroups did not greatly differ. However, the SLgroups were highly correlated with sociodemographics (parental income, education, race) (Table 2). In contrast, data-driven subtypes largely reduced or even circumvented these confounds (while at the same time were more sensitive to crEAs than the SLgroups). Indeed, Figure 4 shows that household income had independent effects from crEA dimensions on mental health and academic outcomes, and Figure 5a shows that model prediction of the crEA subtypes with the addition of a separate SES variable outperformed SLgroups (which themselves were highly conflated with SES). This finding suggests that data-driven subtyping may be better suited to parse the specific impact of crEAs (without sociodemographic confounds). These results show that it is possible to examine crEAs separately from sociodemographic factors and offer an approach that circumvents the pitfalls associated with traditional statistical methods of “regressing out” variables.
Aim 3. crEA dimensions and subtypes robustly predict outcomes
Conditional random forests assessed the statistical predictive value of the data-driven dimensions and subtypes (Note: the statistical “prediction” here does not imply deterministic forecasting of the impact of crEAs on future outcomes). This approach (relative to traditional regression) is robust to high-dimensional data, nonlinear associations, and extreme values, and it allows for crEA cooccurrence. We found that CBCL total score was most strongly predicted by parental mental illness, crEA subtype, and Factor 1 score (Additive Exposure), suggesting that each of these are highly informative of mental health symptoms in this sample. On the other hand, WIAT performance for both reading and numbers was strongly predicted by household income as well as Factor 1, demonstrating the importance of accounting for SES when discussing outcomes, and suggesting that models using SLgroups may be conflating effects of crEAs with those of SES. We found that it was more informative to predict CBCL and WIAT outcomes by using data-derived groups that are independent from SES, and then using SES separately rather than using SLgroups which are associated with SES. This allows for more segregation between crEAs and SES in the conditional random forest model and enables better performance.
Variable importance, which indexes a variable’s predictive worth for a given outcome (conditional on other variables present), is calculated across thousands of models. These models provided strong evidence for both crEA-specific and crEA-general associations with mental health symptoms (CBCL) and academic outcomes (WIAT Reading, WIAT Numbers). Relative to a non-crEA comparison group (Figure 5b), the data-driven crEA subtypes were associated with a greater risk for CBCL symptoms (with each subtype showing greater risk – “crEA-general”), consistent with results identified with latent profile analysis indicating that a subtype with the greatest polyvictimization had greater mental health risk (Pears et al., 2008). Academic achievement on the other hand showed more subtype specificity – “crEA-specific” – for example, Subtypes 1 and 3 being most informative for predicting reading and Subtype 4 being most informative for math. However, Figure 5c (which excludes the comparison group and examines only within the crEA sample) shows a deeper level of specificity. That is, we see crEA-general effects relative to a nonexposed group, but within the sample exposed to crEAs, we see crEA-specific effects, both of which are informative. For example, Subtypes 1, 3, and 5 were better at predicting CBCL symptoms relative to the other crEA subtypes, whereas Subtypes 1 and 3 were better at predicting reading relative to the other crEA subtypes. These comparisons suggest that while all children who experience crEAs may be at higher risk for mental health and academic difficulties, it is important to be aware that domain-specific risks may be especially elevated for some subtypes (even if all subtypes are at elevated risk). For example, Subtype 4, which was largely dominated by high scores on Factor 1, showed higher risk on CBCL and WIAT numbers compared to the other subtypes. This pattern of results indicates that in addition to specific experience-outcome associations, there may be final common pathways (i.e., developmental equifinality) (Cicchetti & Blender, 2004; Cicchetti & Rogosch, 1996; Hanson et al., 2015) for CBCL scores. There are “common denominator” experiences shared across many crEA kinds (e.g., injury to trust-related process) that may give rise to a common pathway for the development of mental health difficulties (Tottenham, 2020). That is, we should expect some developmental domains to show crEA-specific effects and other domains to show crEA-general effects within the same child.
Data-driven dimensions performed even better than the subtypes in predicting CBCL scores and academic achievement (Figure 4). This is perhaps not surprising since dimensions provide scores that more closely track an individual’s experience than categorical variables, and discretization inherent to subtyping may discard meaningful within-subtype variance. Nonetheless, subtypes are important for identifying groups, and past work suggests that hybrid approaches employing both dimensions and subtypes add even greater predictive value than either in isolation (Chabernaud et al., 2012). Dimensions also outperformed individual crEA exposures. Factor 1: Additive Exposure predicted all three outcomes tested here, consistent with evidence that polyvictimization is associated with poorer outcomes (even relative to repeated instances of the same kind) (Finkelhor et al., 2007), and the large variable importance scores suggest robustness/replicability (in an out-of-sample fashion) of this crEA-general effect. In contrast, Factor 2: Emotional Maltreatment without Domestic Violence was a better predictor of reading skills than math skills. We note that Factors 1 and 3 (which included physical/supervisory forms of neglect) and Factor 2 (which included emotional neglect) predicted different outcomes, further supporting the separation of physical/supervisory from emotional neglect (i.e., combining physical/supervisory with emotional neglect introduces heterogeneity rather than reducing it).
Are these crEA endorsements reliable and valid? We cannot indicate how reliable parental reporting of crEAs was in this study. This is unfortunately the nature of crEAs assessments, which will always have the challenge of both omissions and commissions in reporting. Formal court, medical, or child protective services (CPS) records are sometimes believed to be the most reliable and valid measures. However, as Sierau et al. (2017) have summarized, CPS records are biased towards more “readily observable [crEAs] that call for urgent action (e.g., severe physical abuse or neglect),” but they are less sensitive to more “invisible” crEAs like emotional maltreatment. Consequently, reliance on CPS reports increases the risk of omitting certain crEAs (Trickett et al., 2009). Reliance on parent reports likewise has merits and weaknesses. Parent reports may be valuable sources of crEA exposures that are missed by reliance on records; however, parents may also be unable or unwilling to provide veridical information. Note in the current sample of children with crEAs exposure, most of the reporting parents were not the biological parent. While this parent may have been less reluctant to report crEAs experienced by their child, they may also be less privy than biological parents to all crEAs experienced by their child.
The current study made decisions about how best to define crEAs. As is the case with all research on childhood adversities, the entire process of documenting maltreatment is fraught with decisions and inevitable bias – whether it is coming from the investigator, the official records, the case workers, the parents, and/or the children (Fluke et al., 1999; Kim et al., 2017) – or the means through which experiences were coded/collected (e.g., what is/is not recorded in court documents, what is/is not reported by a biological versus adoptive parent). For example, a child who experienced physical neglect and subsequent placement in foster care may be described as experiencing “physical neglect” by court records, adoptive parents, and/or the investigator. However, this child also experienced separation from a primary attachment figure, which itself can be emotionally traumatic (Bowlby, 1977; Bowlby et al., 1956) (note – separation from parents is often omitted as an adverse study variable despite the tremendous impact of this event on development).
In the current paper, we used two different types of parent report, questionnaire format (e.g., TESI) and semistructured parent interview (MICM) that was later coded for crEAs using the MCS. The MCS is a reliable and valid coding system (Manly, 2005; Manly et al., 2013) that differentiates between maltreatment subtypes by providing mutually exclusive subtype criteria and anchor examples. By doing so, the MCS codes generate crEA endorsements that may or may not match the parent’s crEAs endorsement (i.e., the objective coding does not rely on parental definitions, whereas a questionnaire might). In a direct comparison, Sierau et al. (2017) showed that parental interview (via MICM) corresponds with CPS records between a fair to substantial range.
Additional limitations
There are limitations that are worth discussing as they play a role in the interpretation of the current work. First, beyond the window of birth-to-middle childhood, we did not consider the timing of the crEA experiences in developing our subtyping or multivariate FA, which limits the specificity of the phenotypic profiles created here. It is well established that timing of these events plays an important role in their impact on later psychiatric, cognitive, and academic outcomes (Cowell et al., 2015; Manly et al., 2001; Schalinski et al., 2016). Furthermore, we also did not consider the severity of each of these outcomes, although most crEAs were severe in our sample (not reported). Following our work here, it will be important for future work to consider integrating the chronicity and severity of crEA occurrence into multivariate subtypes and factor scores. With the current results, future work can also examine crEA exposure from an experience profile subtyping perspective, which may be useful for deriving homogeneous groups of participants.
Conclusions
The links between caregiving-related adversity and child outcomes are highly complex, and no single approach will sufficiently capture this complexity. Here, we provide some additional guidance to research that aims to investigate the heterogeneity inherent in the cooccurrence of early adversities that directly interfere with the parent-child relationship. Results indicate that despite substantial heterogeneity, greater homogeneity can be achieved via data-driven dimensionalizing and subtyping. These approaches applied to the current broad sample of children (from seemingly disparate SLgroups) provided evidence that the dimensions and subtypes were internally stable, transcended traditional sociolegally defined groups, and reduced statistical correlations with sociodemographic factors. They also showed predictive value for childhood outcomes in a both crEA-specific and crEA-general fashion, depending on behavioral domain and comparison groups. Assessments of cooccurrences provide one means of representing experiential complexity and do so by describing the context in which crEAs occur. Given the high-dimensional space within which crEAs exist, cooccurrence variables might be considered for use in parallel with other dimensions.
Supplementary Material
Acknowledgements.
Michelle VanTieghem is now at Virta Health, San Francisco, CA; Nicolas Camacho is now at Duke University, Durham, NC; Tricia Choy is now at the University of California, Riverside, CA; Ian J. Douglas is now at the University of Texas, Austin, TX.
Funding statement.
This work was supported by the National Institute of Mental Health of the National Institutes of Health (5RO1MH091864). AN is also supported by NIMH R21MH118556-01 and a Young Investigator award from the Brain and Behavior Research foundation. MPM is also supported by an endowment from Phyllis Green and Randolph Cowen. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Supplementary material. The supplementary material for this article can be found at https://doi.org/10.1017/S0954579421001668
Conflicts of interest. We have no known conflicts of interest to disclose.
This is not to deny that, in many instances, separations must occur for the child’s welfare. It is to recognize that the separation itself might be an additional necessary, although emotionally painful, experience for the child.
References
- Aber JL (2013). Family and community level effects. In Nelson CA (Ed.), Threats to optimal development: Integrating biological, psychological, and social risk factors: The Minnesota symposia on child psychology (vol. 27, pp. 229). Psychology Press. [Google Scholar]
- Achenbach TM, & Rescorla LA Eds (2001). Manual for the Aseba school-age forms & profiles. University of Vermont, Research Center for Children, Youth, & Families. [Google Scholar]
- Baram TZ, Davis EP, Obenaus A, Sandman CA, Small SL, Solodkin A … Stern H (2012). Fragmentation and unpredictability of early-life experience in mental disorders. American Journal of Psychiatry, 169(9), 907–915. 10.1176/appi.ajp.2012.11091347 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnet O, Miller-Perrin CL, & Perrin RD (2005). Child psychological maltreatment. In Barnett O, Miller-Perrin CL, & Perrin RD (Eds.), Family violence across the lifespan: An introduction (2nd edn., pp. 151–178). Sage Publications. [Google Scholar]
- Belsky J, Schlomer GL, & Ellis BJ (2012). Beyond cumulative risk: Distinguishing harshness and unpredictability as determinants of parenting and early life history strategy. Developmental Psychology, 48(3), 662. 10.1037/a0024454 [DOI] [PubMed] [Google Scholar]
- Benjet C, Borges G, & Medina-Mora ME (2010). Chronic childhood adversity and onset of psychopathology during three life stages: Childhood, adolescence and adulthood. Journal of Psychiatric Research, 44(11), 732–740. 10.1016/j.jpsychires.2010.01.004 [DOI] [PubMed] [Google Scholar]
- Berzenski SR, & Yates TM (2011). Classes and consequences of multiple maltreatment: A person-centered analysis. Child Maltreatment, 16(4), 250–261. 10.1177/1077559511428353 [DOI] [PubMed] [Google Scholar]
- Blondel VD, Guillaume J-L, Lambiotte R, & Lefebvre E (2008). Fast unfolding of communities in large networks. Journal of Statistical Mechanics: Theory and Experiment, 2008(10), P10008. [Google Scholar]
- Bowlby J (1977). The making and breaking of affectional bonds: Ii. Some Principles of psychotherapy: The fiftieth Maudsley Lecture (expanded version). British Journal of Psychiatry, 130(5), 421–431. 10.1192/bjp.130.5.421 [DOI] [PubMed] [Google Scholar]
- Bowlby J, Ainsworth M, Boston M, & Rosenbluth D (1956). The effects of mother-child separation: A follow-up study. British Journal of Medical Psychology, 29(3–4), 211–247. 10.1111/j.2044-8341.1956.tb00915.x [DOI] [PubMed] [Google Scholar]
- Breiman L (1996). Bagging predictors. Machine Learning, 24(2), 123–140. [Google Scholar]
- Brown SM, Rienks S, McCrae JS, & Watamura SE (2019). The cooccurrence of adverse childhood experiences among children investigated for child maltreatment: A latent class analysis. Child Abuse and Neglect, 87, 18–27. 10.1016/j.chiabu.2017.11.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chabernaud C, Mennes M, Kelly C, Nooner K, Di Martino A, Castellanos FX … Milham MP (2012). Dimensional brain-behavior relationships in children with attention-deficit/hyperactivity disorder. Biological Psychiatry, 71(5), 434–442. 10.1016/j.biopsych.2011.08.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicchetti D, & Blender JA (2004). A multiple-levels-of-analysis approach to the study of developmental processes in maltreated children. Procedings of the National Academy of Sciences of the United States of America, 101(50), 17325–17326. 10.1073/pnas.0408033101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicchetti D, & Rizley R (1981). Developmental perspectives on the etiology, intergenerational transmission, and sequelae of child maltreatment. New Directions for Child and Adolescent Development, 1981(11), 31–55. 10.1002/cd.23219811104 [DOI] [Google Scholar]
- Cicchetti D, & Rogosch FA (1996). Equifinality and multifinality in developmental psychopathology. Development and Psychopathology, 8(4), 597–600. 10.1017/S0954579400007318 [DOI] [Google Scholar]
- Cicchetti D, & Toth SL (1993). Advances in applied developmental psychology: Child abuse, child development and social policy (pp. 7–73). Ablex Publishing Corp. [Google Scholar]
- Cicchetti D, & Toth SL (2005). Child maltreatment. Annual Review of Clinical Psychology, 1, 409–438. 10.1146/annurev.clinpsy.1.102803.144029 [DOI] [PubMed] [Google Scholar]
- Cicchetti D, Toth SL, & Manly JT (2003). Maternal Maltreatment Classification Interview, Unpublished manuscript, Mt. Hope Family Center, Rochester, NY.. [Google Scholar]
- Cicchetti D, Toth SL, & Maughan A (2000). An ecological-transactional model of child maltreatment. In Sameroff AJ, Lewis M, & Miller SM (Eds.), Handbook of developmental psychopathology. Kluwer Academic Publishers, 10.1007/978-1-4615-4163-9_37 [DOI] [Google Scholar]
- Clark C, Caldwell T, Power C, & Stansfeld SA (2010). Does the influence of childhood adversity on psychopathology persist across the lifecourse? A 45-year prospective epidemiologic study. Annals of Epidemiology, 20(5), 385–394. 10.1016/j.annepidem.2010.02.008 [DOI] [PubMed] [Google Scholar]
- Cohodes EM, Kitt ER, Baskin-Sommers A, & Gee DG (2021). Influences of early-life stress on frontolimbic circuitry: Harnessing a dimensional approach to elucidate the effects of heterogeneity in stress exposure. Developmental Psychobiology, 63, 153–172. 10.1002/dev.21969 [DOI] [PubMed] [Google Scholar]
- Cowell RA, Cicchetti D, Rogosch FA, & Toth SL (2015). Childhood maltreatment and its effect on neurocognitive functioning: Timing and chronicity matter. Development and Psychopathology, 27(2), 521–533. 10.1017/S0954579415000139 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fair DA, Nigg JT, Iyer S, Bathula D, Mills KL, Dosenbach NU … Milham MP (2012). Distinct neural signatures detected for adhd subtypes after controlling for micro-movements in resting state functional connectivity MRI data. Frontiers in Systems Neuroscience, 6, 80. 10.3389/fnsys.2012.00080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feczko E, & Fair DA (2020). Methods and challenges for assessing heterogeneity. Biological Psychiatry, 88(1), 9–17. 10.1016/j.biopsych.2020.02.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feczko E, Miranda-Dominguez O, Marr M, Graham AM, Nigg JT, & Fair DA (2019). The heterogeneity problem: Approaches to identify psychiatric subtypes. Trends in Cognitive Sciences, 23(7), 584–601. 10.1016/j.tics.2019.03.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finkelhor D, Ormrod RK, & Turner HA (2007). Poly-victimization: A neglected component in child victimization. Child Abuse and Neglect, 31(1), 7–26. 10.1016/j.chiabu.2006.06.008 [DOI] [PubMed] [Google Scholar]
- Fluke JD, Yuan YY, & Edwards M (1999). Recurrence of maltreatment: An application of the national child abuse and neglect data system (Ncands). Child Abuse and Neglect, 23(7), 633–650. 10.1016/s0145-2134(99)00039-3 [DOI] [PubMed] [Google Scholar]
- Ford JD, Racusin R, Rogers K, Ellis C, Schiffman J, Ribbe D … Edwards J (2002). Traumatic Events Screening Inventory for Children (TESI-C) version 8.4. National Center for PTSD and Dartmouth Child Psychiatry Research Group, Dartmouth VT. [Google Scholar]
- Green JG, McLaughlin KA, Berglund PA, Gruber MJ, Sampson NA, Zaslavsky AM … Kessler RC (2010). Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: Associations with first onset of Dsm-Iv disorders. Archives of General Psychiatry, 67(2), 113–123. 10.1001/archgenpsychiatry.2009.186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green MJ (2014). Latent class analysis was accurate but sensitive in data simulations. Journal of Clinical Epidemiology, 67(10), 1157–1162. 10.1016/j.jclinepi.2014.05.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Groark CJ, & McCall RB (2011). Improving institutions: Can we? Should we? How? International Journal of Child & Family Welfare, 14(2), 64–72. [Google Scholar]
- Groark CJ, McCall RB, Fish L, & Team, W. C. I. E. (2011). Characteristics of environments, caregivers, and children in three central american orphanages. Infant Mental Health Journal, 32(2), 232–250. 10.1002/imhj.20292 [DOI] [PubMed] [Google Scholar]
- Gunnar MR, Bruce J, & Grotevant HD (2000). International adoption of institutionally reared children: Research and policy. Development and Psychopathology, 12(4), 677–693. 10.1017/s0954579400004077 [DOI] [PubMed] [Google Scholar]
- Hanson JL, Nacewicz BM, Sutterer MJ, Cayo AA, Schaefer SM, Rudolph KD … Davidson RJ (2015). Behavioral problems after early life stress: Contributions of the hippocampus and amygdala. Biological Psychiatry, 77(4), 314–323. 10.1016/j.biopsych.2014.04.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hart SN, & Brassard MR (1987). A major threat to children’s mental health: Psychological maltreatment. American Psychologist, 42(2), 160–165. 10.1037//0003-066x.42.2.160 [DOI] [PubMed] [Google Scholar]
- Hazen AL, Connelly CD, Roesch SC, Hough RL, & Landsverk JA (2009). Child maltreatment profiles and adjustment problems in high-risk adolescents. Journal of Interpersonal Violence, 24(2), 361–378. 10.1177/0886260508316476 [DOI] [PubMed] [Google Scholar]
- Herzog JI, Thome J, Demirakca T, Koppe G, Ende G, Lis S … Steil R (2020). Influence of severity of type and timing of retrospectively reported childhood maltreatment on female amygdala and hippocampal volume. Scientific Reports, 10(1), 1–10. 10.1038/s41598-020-57490-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horn JL (1965). A rationale and test for the number of factors in factor analysis. Psychometrika, 30, 179–185. 10.1007/BF02289447 [DOI] [PubMed] [Google Scholar]
- Hornor G (2012). Emotional maltreatment. Journal of Pediatric Health Care, 26(6), 436–442. 10.1016/j.pedhc.2011.05.004 [DOI] [PubMed] [Google Scholar]
- Infurna MR, Reichl C, Parzer P, Schimmenti A, Bifulco A, & Kaess M (2016). Associations between depression and specific childhood experiences of abuse and neglect: A meta-analysis. Journal of Affective Disorders, 190, 47–55. 10.1016/j.jad.2015.09.006 [DOI] [PubMed] [Google Scholar]
- Insel TR, & Cuthbert BN (2015). Medicine. Brain disorders? Precisely. Science, 348(6234), 499–500, 10.1126/science.aab2358, [DOI] [PubMed] [Google Scholar]
- Ivy AS, Brunson KL, Sandman C, & Baram TZ (2008). Dysfunctional nurturing behavior in rat dams with limited access to nesting material: A clinically relevant model for early-life stress. Neuroscience, 154(3), 1132–1142. 10.1016/j.neuroscience.2008.04.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karalunas SL, Fair D, Musser ED, Aykes K, Iyer SP, & Nigg JT (2014). Subtyping attention-deficit/hyperactivity disorder using temperament dimensions: Toward biologically based nosologic criteria. JAMA Psychiatry, 71(9), 1015–1024. 10.1001/jamapsychiatry.2014.763 [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- Kessler RC, McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM … Williams DR (2010). Childhood adversities and adult psychopathology in the who world mental health surveys. British Journal of Psychiatry, 197(5), 378–385. 10.1192/bjp.bp.110.080499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim H, & Drake B (2018). Child maltreatment risk as a function of poverty and race/ethnicity in the USA. International Journal of Epidemiology, 47(3), 780–787. 10.1093/ije/dyx280 [DOI] [PubMed] [Google Scholar]
- Kim K, Mennen FE, & Trickett PK (2017). Patterns and correlates of cooccurrence among multiple types of child maltreatment. Child and Family Social Work, 22(1), 492–502. 10.1111/cfs.12268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lacey RE, Howe LD, Kelly-Irving M, Bartley M, & Kelly Y (In Press). The Clustering of Adverse Childhood Experiences in the Avon Longitudinal Study of Parents and Children: Are Gender and Poverty Important? Journal of Interpersonal Violence. 10.1177/0886260520935096 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lambert HK, King KM, Monahan KC, & McLaughlin KA (2017). Differential associations of threat and deprivation with emotion regulation and cognitive control in adolescence. Development and Psychopathology, 29(3), 929–940. 10.1017/S0954579416000584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maguire-Jack K, Lanier P, & Lombardi B (2020). Investigating racial differences in clusters of adverse childhood experiences. American Journal of Orthopsychiatry, 90(1), 106–114. 10.1037/ort0000405 [DOI] [PubMed] [Google Scholar]
- Manly JT (2005). Advances in research definitions of child maltreatment. Child Abuse and Neglect, 29(5), 425–439. 10.1016/j.chiabu.2005.04.001 [DOI] [PubMed] [Google Scholar]
- Manly JT, Kim JE, Rogosch FA, & Cicchetti D (2001). Dimensions of child maltreatment and children’s adjustment: Contributions of developmental timing and subtype. Development and Psychopathology, 13(4), 759–782. 10.1017/S0954579401004023 [DOI] [PubMed] [Google Scholar]
- Manly JT, Oshri A, Lynch M, Herzog M, & Wortel S (2013). Child neglect and the development of externalizing behavior problems: Associations with maternal drug dependence and neighborhood crime. Child Maltreatment, 18(1), 17–29. 10.1177/1077559512464119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matsumoto M, Piersiak H, Letterie M, & Humphreys K (2020). Population-based estimates of associations between child maltreatment type: A meta-analysis. PsyArXiv, 10.31234/osf.io/cv5qw, [DOI] [PubMed] [Google Scholar]
- McLaughlin KA, Greif Green J, Gruber MJ, Sampson NA, Zaslavsky AM, & Kessler RC (2012). Childhood adversities and first onset of psychiatric disorders in a national sample of US adolescents. Archives of General Psychiatry, 69(11), 1151–1160. 10.1001/archgenpsychiatry.2011.2277 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Sheridan M, Humphreys KL, Belsky J, & Ellis BJ (2021). The value of dimensional models of early experience: Thinking clearly about concepts and categories. Perspectives on Psychological Science, 16(6), 1463–1472. 10.1177/1745691621992346 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Sheridan MA, & Lambert HK (2014). Childhood adversity and neural development: Deprivation and threat as distinct dimensions of early experience. Neuroscience and Biobehavioral Reviews, 47, 578–591. 10.1016/j.neubiorev.2014.10.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ney PG, Fung T, & Wickett AR (1994). The worst combinations of child abuse and neglect. Child Abuse and Neglect, 18(9), 705–714. 10.1016/0145-2134(94)00037-9 [DOI] [PubMed] [Google Scholar]
- Nikolaidis A, DeRosa J, Kass M, Droney I, Alexander L, Di Martino A … Paksarian D (2021). Heterogeneity in Covid-19 pandemic-induced lifestyle stressors and predicts future mental health in adults and children in the US and UK. medRxiv, 10.1101/2021.08.10.21261860, [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nikolaidis A, Paksarian D, Alexander L, Derosa J, Dunn J, Nielson DM … Merikangas KR (2021). The Coronavirus Health and Impact Survey (CRISIS) reveals reproducible correlates of pandemic-related mood states across the atlantic. Scientific Reports, 11(1), 8139. 10.1038/s41598-021-87270-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nikolaidis A, Solon Heinsfeld A, Xu T, Bellec P, Vogelstein J, & Milham M (2020). Bagging improves reproducibility of functional parcellation of the human brain. Neuroimage, 214, 116678. 10.1016/j.neuroimage.2020.116678 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pears KC, Kim HK, & Fisher PA (2008). Psychosocial and cognitive functioning of children with specific profiles of maltreatment. Child Abuse and Neglect, 32(10), 958–971, 10.1016/j.chiabu.2007.12.009, [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petrenko CL, Friend A, Garrido EF, Taussig HN, & Culhane SE (2012). Does subtype matter? Assessing the effects of maltreatment on functioning in preadolescent youth in out-of-home care. Child Abuse and Neglect, 36(9), 633–644, 10.1016/j.chiabu.2012.07.001, [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sameroff AJ, & Chandler MJ (1975). Reproductive risk and the continuum of caretaking casualty. Review of Child Development Research, 4, 187–244. [Google Scholar]
- Schalinski I, Teicher MH, Nischk D, Hinderer E, Muller O, & Rockstroh B (2016). Type and timing of adverse childhood experiences differentially affect severity of PTSD, dissociative and depressive symptoms in adult inpatients. BMC Psychiatry, 16, 295. 10.1186/s12888-016-1004-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scott BG, Burke NJ, Weems CF, Hellman JL, & Carrión VG (2013). The interrelation of adverse childhood experiences within an at-risk pediatric sample. Journal of Child & Adolescent Trauma, 6(3), 217–229. [Google Scholar]
- Sheridan MA, & McLaughlin KA (2014). Dimensions of early experience and neural development: Deprivation and threat. Trends in Cognitive Sciences, 18(11), 580–585. 10.1016/j.tics.2014.09.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheridan MA, Shi F, Miller AB, Salhi C, & McLaughlin KA (2020). Network structure reveals clusters of associations between childhood adversities and development outcomes. Developmental Science, 23(5), e12934. 10.1111/desc.12934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shorter E, & Tyrer P (2003). Separation of anxiety and depressive disorders: Blind alley in psychopharmacology and classification of disease. British Medical Journal, 327(7407), 158–160. 10.1136/bmj.327.7407.158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sierau S, Brand T, Manly JT, Schlesier-Michel A, Klein AM, Andreas A … White LO (2017). A multisource approach to assessing child maltreatment from records, caregivers, and children. Child Maltreatment, 22(1), 45–57. 10.1177/1077559516675724 [DOI] [PubMed] [Google Scholar]
- Smith KE, & Pollak SD (2021). Rethinking concepts and categories for understanding the neurodevelopmental effects of childhood adversity. Perspectives on Psychological Science, 16(1), 67–93. 10.1177/1745691620920725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spinazzola J, Hodgdon H, Liang L-J, Ford JD, Layne CM, Pynoos R … Kisiel C (2014). Unseen wounds: The contribution of psychological maltreatment to child and adolescent mental health and risk outcomes. Psychological Trauma: Theory, Research, Practice, and Policy, 6(S1), S18. 10.1037/a0037766 [DOI] [Google Scholar]
- Tang S, Sun N, Floris DL, Zhang X, Di Martino A, & Yeo BTT (2020). Reconciling dimensional and categorical models of autism heterogeneity: A brain connectomics and behavioral study. Biological Psychiatry, 87(12), 1071–1082. 10.1016/j.biopsych.2019.11.009 [DOI] [PubMed] [Google Scholar]
- Tonmyr L, Draca J, Crain J, & Macmillan HL (2011). Measurement of emotional/psychological child maltreatment: A review. Child Abuse and Neglect, 35(10), 767–782. 10.1016/j.chiabu.2011.04.011 [DOI] [PubMed] [Google Scholar]
- Tottenham N (2020). Neural meaning making, prediction, and prefrontal–subcortical development following early adverse caregiving. Development and Psychopathology, 32(5), 1563–1578. 10.1017/S0954579420001169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trickett PK, & McBride-Chang C (1995). The developmental impact of different forms of child abuse and neglect. Developmental Review, 15(3), 311–337. 10.1006/drev.1995.1012 [DOI] [Google Scholar]
- Trickett PK, Mennen FE, Kim K, & Sang J (2009). Emotional abuse in a sample of multiply maltreated, urban young adolescents: Issues of definition and identification. Child Abuse and Neglect, 33(1), 27–35. 10.1016/j.chiabu.2008.12.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van IJzendoorn MH, Bakermans-Kranenburg MJ, Duschinsky R, Fox NA, Goldman PS, Gunnar MR … Skinner GC (2020). Institutionalisation and deinstitutionalisation of children 1: A systematic and integrative review of evidence regarding effects on development. The Lancet Psychiatry, 7(8), 703–720. 10.1016/S2215-0366(19)30399-2 [DOI] [PubMed] [Google Scholar]
- Vaughan-Jensen J, Adame C, McLean L, & Gámez B (2011). Test review:D. Wechsler Wechsler Individual Achievement Test. San Antonio, TX: Pearson, 2009. Journal of Psychoeducational Assessment, 29(3), 286–291, 10.1177/0734282910385645, [DOI] [Google Scholar]
- Vermunt JK, & Magidson J (2004). Latent class analysis. The Sage Encyclopedia of Social Sciences Research Methods, 2, 549–553. [Google Scholar]
- Wade M, Fox NA, Zeanah CH, & Nelson CA 3rd (2019). Long-term effects of institutional rearing, foster care, and brain activity on memory and executive functioning. Proceedings of the National Academy of Sciences of the United States of America, 116(5), 1808–1813. 10.1073/pnas.1809145116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wardenaar KJ, & de Jonge P (2013). Diagnostic heterogeneity in psychiatry: Towards an empirical solution. BMC Medicine, 11, 201. 10.1186/1741-7015-11-201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warmingham JM, Handley ED, Rogosch FA, Manly JT, & Cicchetti D (2019). Identifying maltreatment subgroups with patterns of maltreatment subtype and chronicity: A latent class analysis approach. Child Abuse and Neglect, 87, 28–39. 10.1016/j.chiabu.2018.08.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wechsler D (1999). The Wechsler abbreviated scale of intelligence. The Psychological Corporation. [Google Scholar]
- Wolfe DA (2018). Why polyvictimization matters. Journal of Interpersonal Violence, 33(5), 832–837. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.