

Abstract
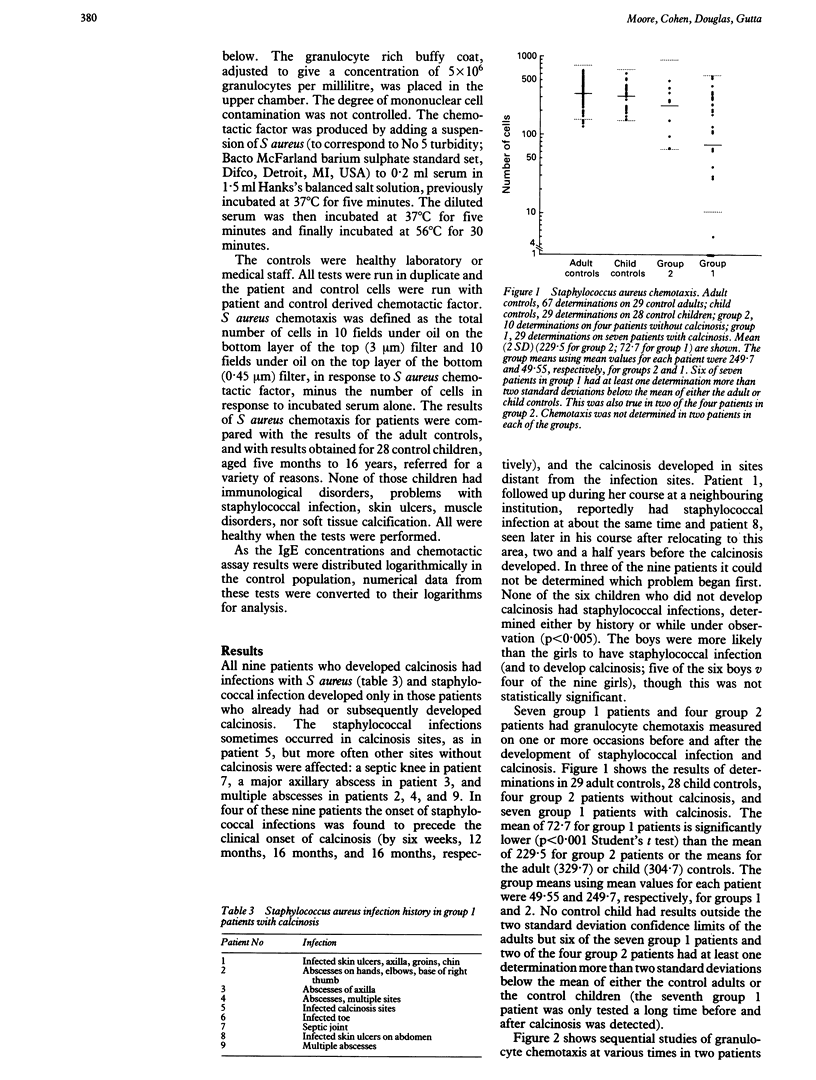
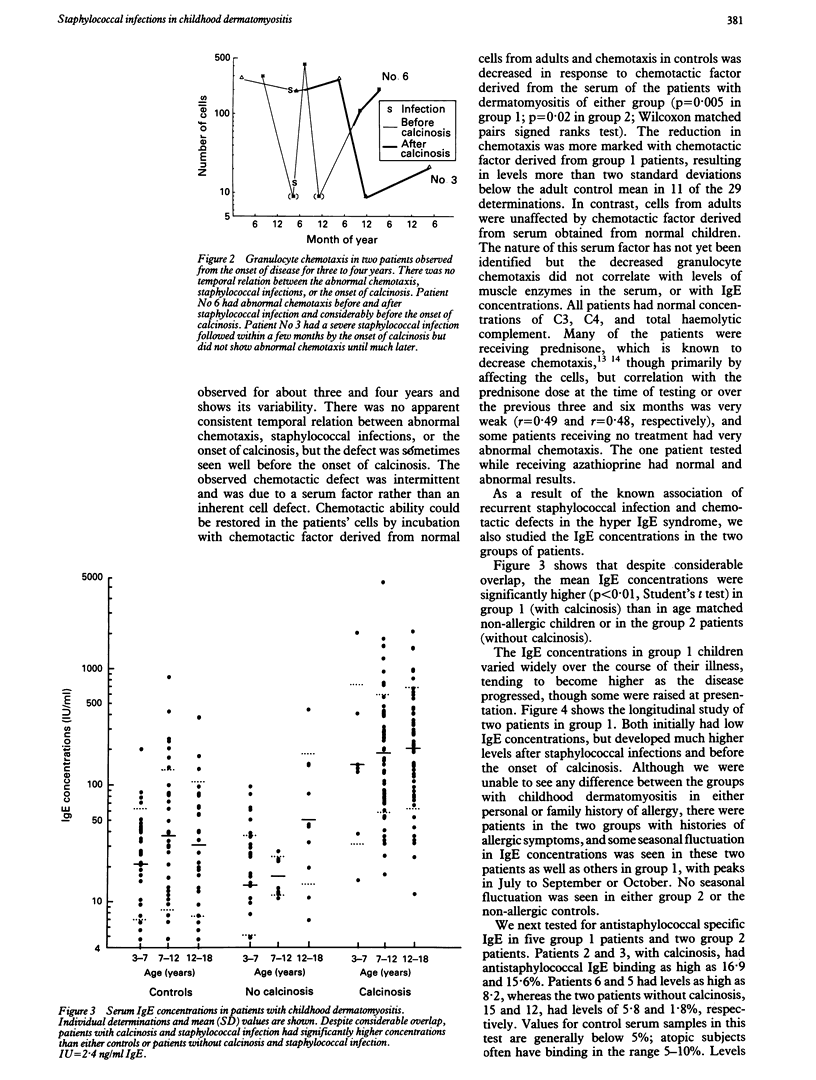
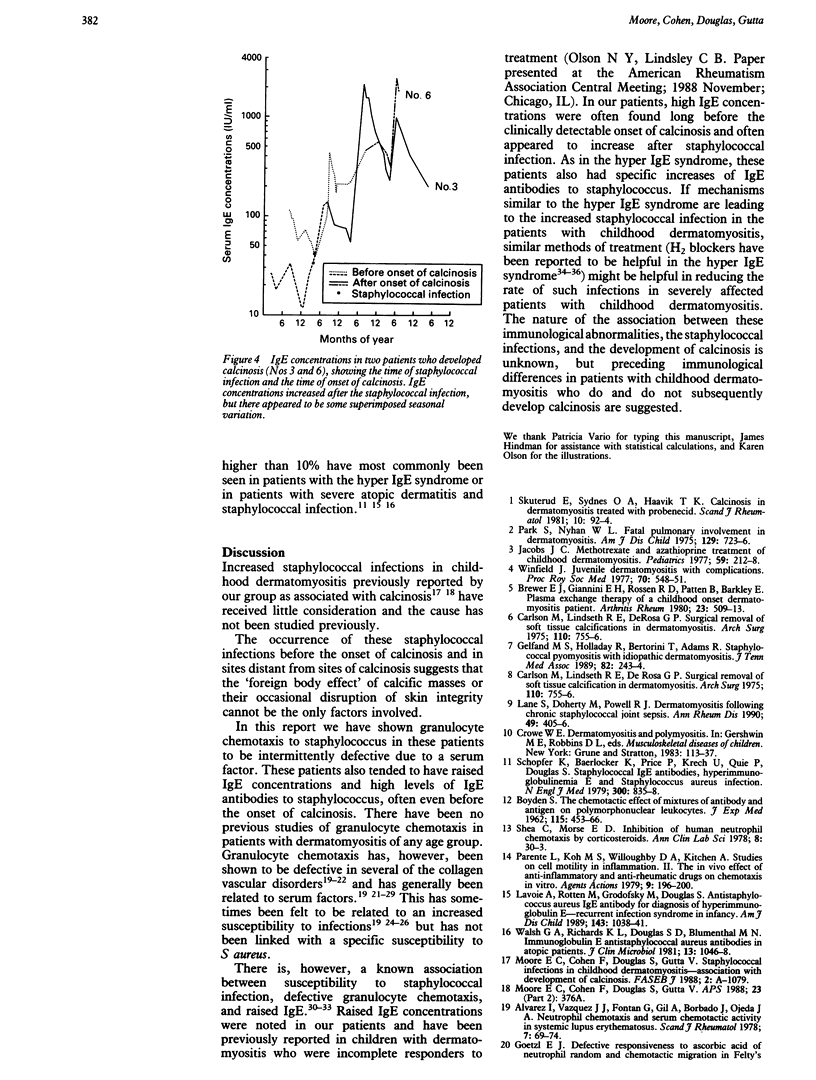
There is a high incidence of staphylococcal infection in children with dermatomyositis, which is limited to those children who either already have or subsequently develop calcinosis. Of 15 children followed up for 3-10 years after diagnosis, all nine who developed calcinosis had infections with Staphylococcus aureus compared with none of six without calcinosis. Of these nine, the occurrence of staphylococcal infections before calcinosis was observed in four, suggested by history in two, and unclear in three children. Granulocyte chemotaxis to Staphylococcus aureus was more severely depressed in those children with calcinosis, whereas those without calcinosis did not differ significantly from controls. The chemotactic defect was due to a serum factor (patients' serum depressed control chemotaxis and control serum corrected the patients' chemotaxis). The nine children with calcinosis also had significantly higher serum IgE concentrations than non-atopic age matched controls; the six without calcinosis did not differ from controls. The increased IgE concentrations appeared to develop after staphylococcal infection and before calcinosis. Two of five patients with calcinosis had increased antistaphylococcal IgE antibodies; neither of the two patients without calcinosis had such increased antibodies. This suggests preceding immunological differences in patients with dermatomyositis who do and do not subsequently develop calcinosis, either increasing susceptibility to Staphylococcus aureus infection or potentially resulting from such infections.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alvarez I., Vazquez J. J., Fontan G., Gil A., Barbado J., Ojeda J. A. Neutrophil chemotaxis and serum chemotactic activity in systemic lupus erythematosus. Scand J Rheumatol. 1978;7(2):69–74. doi: 10.3109/03009747809098837. [DOI] [PubMed] [Google Scholar]
- BOYDEN S. The chemotactic effect of mixtures of antibody and antigen on polymorphonuclear leucocytes. J Exp Med. 1962 Mar 1;115:453–466. doi: 10.1084/jem.115.3.453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brewer E. J., Jr, Giannini E. H., Rossen R. D., Patten B., Barkley E. Plasma exchange therapy of a childhood onset dermatomyositis patient. Arthritis Rheum. 1980 Apr;23(4):509–513. doi: 10.1002/art.1780230415. [DOI] [PubMed] [Google Scholar]
- Buckley R. H., Wray B. B., Belmaker E. Z. Extreme hyperimmunoglobulinemia E and undue susceptibility to infection. Pediatrics. 1972 Jan;49(1):59–70. [PubMed] [Google Scholar]
- Carlson M., Lindseth R. E., DeRosa G. P. Surgical removal of soft tissue calcifications in dermatomyositis. Arch Surg. 1975 Jun;110(6):755–756. doi: 10.1001/archsurg.1975.01360120073014. [DOI] [PubMed] [Google Scholar]
- Carlson M., Lindseth R. E., DeRosa G. P. Surgical removal of soft tissue calcifications in dermatomyositis. Arch Surg. 1975 Jun;110(6):755–756. doi: 10.1001/archsurg.1975.01360120073014. [DOI] [PubMed] [Google Scholar]
- Clark R. A., Root R. K., Kimball H. R., Kirkpatrick C. H. Defective neutrophil chemotaxis and cellular immunity in a child with recurrent infections. Ann Intern Med. 1973 Apr;78(4):515–519. doi: 10.7326/0003-4819-78-4-515. [DOI] [PubMed] [Google Scholar]
- Gelfand M. S., Holladay R., Bertorini T., Adams R. F. Staphylococcal pyomyositis with idiopathic dermatomyositis. J Tenn Med Assoc. 1989 May;82(5):243–244. [PubMed] [Google Scholar]
- Goetzl E. J. Defective responsiveness to ascorbic acid of neutrophil random and chemotactic migration in Felty's syndrome and systemic lupus erythematosus. Ann Rheum Dis. 1976 Dec;35(6):510–515. doi: 10.1136/ard.35.6.510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanlon S. M., Panayi G. S., Laurent R. Defective polymorphonuclear leucocyte chemotaxis in rheumatoid arthritis associated with a serum inhibitor. Ann Rheum Dis. 1980 Feb;39(1):68–74. doi: 10.1136/ard.39.1.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasegawa S., Baba T., Koitabashi Y., Shimizu Y., Sonozaki H., Hori Y., Nishiyama S. Elevated levels of chemotaxis inhibitory activity in sera of patients with systemic lupus erythematosus. J Dermatol. 1980 Oct;7(5):309–315. doi: 10.1111/j.1346-8138.1980.tb01977.x. [DOI] [PubMed] [Google Scholar]
- Hill H. R., Estensen R. D., Hogan N. A., Quie P. G. Severe staphylococcal disease associated with allergic manifestations, hyperimmunoglobulinemia E, and defective neutrophil chemotaxis. J Lab Clin Med. 1976 Nov;88(5):796–806. [PubMed] [Google Scholar]
- Hill H. R., Quie P. G. Raised serum-IgE levels and defective neutrophil chemotaxis in three children with eczema and recurrent bacterial infections. Lancet. 1974 Feb 9;1(7850):183–187. doi: 10.1016/s0140-6736(74)92493-3. [DOI] [PubMed] [Google Scholar]
- Jacobs J. C. Methotrexate and azathioprine treatment of childhood dermatomyositis. Pediatrics. 1977 Feb;59(2):212–218. [PubMed] [Google Scholar]
- Lane S., Doherty M., Powell R. J. Dermatomyositis following chronic staphylococcal joint sepsis. Ann Rheum Dis. 1990 Jun;49(6):405–406. doi: 10.1136/ard.49.6.405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanzer G., Zielinski C., Knapp W., Eberl R., Steffen C. Leukocyte locomotion and regulative serum effects in rheumatoid arthritis. Z Rheumatol. 1981 Mar-Apr;40(2):66–71. [PubMed] [Google Scholar]
- Mawhinney H., Killen M., Fleming W. A., Roy A. D. The hyperimmunoglobulin E syndrome--a neutrophil chemotactic defect reversible by histamine H2 receptor blockade? Clin Immunol Immunopathol. 1980 Dec;17(4):483–491. doi: 10.1016/0090-1229(80)90144-0. [DOI] [PubMed] [Google Scholar]
- Mowat A. G., Baum J. Chemotaxis of polymorphonuclear leukocytes from patients with rheumatoid arthritis. J Clin Invest. 1971 Dec;50(12):2541–2549. doi: 10.1172/JCI106754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mowat A. G. Neutrophil chemotaxis in patients with rheumatoid arthritis: mechanisms responsible for impairment [Proceedings]. Ann Rheum Dis. 1976 Jun;35(3):286–286. doi: 10.1136/ard.35.3.286-b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parente L., Koh M. S., Willoughby D. A., Kitchen A. Studies on cell motility in inflammation. II. The in vivo effect of anti-inflammatory and anti-rheumatic drugs on chemotaxis in vitro. Agents Actions. 1979 Jun;9(2):196–200. doi: 10.1007/BF02024734. [DOI] [PubMed] [Google Scholar]
- Park S., Nyhan W. L. Fatal pulmonary involvement in dermatomyositis. Am J Dis Child. 1975 Jun;129(6):723–726. doi: 10.1001/archpedi.1975.02120430057016. [DOI] [PubMed] [Google Scholar]
- Perez H. D., Andron R. I., Goldstein I. M. Infection in patients with systemic lupus erythematosus. Association with a serum inhibitor of complement-derived chemotactic activity. Arthritis Rheum. 1979 Dec;22(12):1326–1333. doi: 10.1002/art.1780221202. [DOI] [PubMed] [Google Scholar]
- Schopfer K., Baerlocher K., Price P., Krech U., Quie P. G., Douglas S. D. Staphylococcal IgE antibodies, hyperimmunoglobulinemia E and Staphylococcus aureus infections. N Engl J Med. 1979 Apr 12;300(15):835–838. doi: 10.1056/NEJM197904123001506. [DOI] [PubMed] [Google Scholar]
- Simon G. L., Miller H. G., Scott S. J. Cimetidine in the treatment of hyperimmunoglobulinemia E with impaired chemotaxis. J Infect Dis. 1983 Jun;147(6):1121–1122. doi: 10.1093/infdis/147.6.1121. [DOI] [PubMed] [Google Scholar]
- Skuterud E., Sydnes O. A., Haavik T. K. Calcinosis in dermatomyositis treated with probenecid. Scand J Rheumatol. 1981;10(2):92–94. doi: 10.3109/03009748109095279. [DOI] [PubMed] [Google Scholar]
- Van Scoy R. E., Hill H. R., Ritts R. E., Quie P. G. Familial neutrophil chemotaxis defect, recurrent bacterial infections, mucocutaneous candidiasis, and hyperimmunoglobulinemia E. Ann Intern Med. 1975 Jun;82(6):766–771. doi: 10.7326/0003-4819-82-6-766. [DOI] [PubMed] [Google Scholar]
- Walker J. R., James D. W., Smith M. J. Directed migration of circulating polymorphonuclear leucocytes in patients with rheumatoid arthritis: a defect in the plasma. Ann Rheum Dis. 1979 Jun;38(3):215–218. doi: 10.1136/ard.38.3.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker J. R., Smith M. J. An inhibitor of leucocyte movement in the plasma of patients with rheumatoid arthritis. Ann Rheum Dis. 1980 Dec;39(6):563–565. doi: 10.1136/ard.39.6.563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker J. R., Smith M. J., James D. W. A comparison of two in vitro methods for studying a defect in leucocyte movement in rheumatoid arthritis. Int Arch Allergy Appl Immunol. 1979;59(3):343–348. doi: 10.1159/000232279. [DOI] [PubMed] [Google Scholar]
- Walsh G. A., Richards K. L., Douglas S. D., Blumenthal M. N. Immunoglobulin E anti-Staphylococcus aureus antibodies in atopic patients. J Clin Microbiol. 1981 Jun;13(6):1046–1048. doi: 10.1128/jcm.13.6.1046-1048.1981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winfield J. Juvenile dermatomyositis with complications. Proc R Soc Med. 1977 Aug;70(8):548–551. [PMC free article] [PubMed] [Google Scholar]