

Abstract
Aim:
To examine perceived stress as a mediator of the association between weight-related discrimination and physical and psychological wellbeing among persons with type 2 diabetes (T2D).
Methods:
Data were obtained from 5,104 persons with self-reported T2D participating in the All of Us research program in the United States. The Everyday Discrimination Scale (EDS), Cohen’s Perceived Stress Scale (PSS), and PROMIS Global Health Scale were used to measure weight-related discrimination, perceived stress, and health outcomes (physical and psychological) respectively. Mediation effects of PSS were tested by bootstrapping with 5000 random samples.
Results:
Participants were, on average, 63.62 (SD 11.38) years old. Majority of them were female (55.53%), Non-Hispanic White (72.61%), married or living with a partner (56.92%), had a household income of <$35,000 (31.99%), and had some college education (33.54%). We found that approximately 18% of study participants reported having experienced weight-related discrimination. We also found that weight-related discrimination was independently associated with poor physical and psychological wellbeing. These associations were partially mediated by perceived stress such that weight-related discrimination was associated with greater perceived stress, which was in turn associated with poorer physical and psychological wellbeing.
Conclusions:
Given that weight-related discrimination is associated with poor outcomes through elevated stress, interventions that target stress may disrupt this pathway thereby helping to reduce the health impact of weight-related discrimination. This assertion should, however, be tested in future studies.
Keywords: Weight-related discrimination, T2D, All of Us research program
Introduction
Over 530 million adults have diabetes globally.1 Type 2 diabetes (T2D) accounts for 90–95% of global diabetes prevalence. In the United States (US), over 11.6% of the adult population have diabetes.1 Persons with T2D may experience diabetes-related stigma (often manifesting as being unfairly treated by others, shamed, or blamed for the disease) that is associated with negative health outcomes including diabetes distress, depressive symptoms, anxiety, poor glycaemic control, and low engagement in beneficial self-management behaviors.2
Persons with T2D are disproportionately impacted by obesity (body mass index [BMI] ≥ 30kg/m2),3 which exposes them to additional stigma-related stressors based on their weight. While there is substantial stigma surrounding T2D,2 weight-related discrimination is much more pervasive because weight status is highly visible and less likely to be concealed.4 Weight-related discrimination includes overt negative attitudes, stereotypes, misconceptions, and unfair treatments that overweight or obese individuals may experience.5 It often originates from the failure to recognize the complexity of the causal mechanisms underlying obesity and the false perception of obesity as a condition caused by character failure and the lack of self-control. Thus, weight-related discrimination may involve being labeled as “lazy” and “gluttonous”.5
Studies have shown that weight discrimination is associated with increased depressive symptoms, psychological distress, stress, and worse physical health in the general population.5,6 Overweight or obese individuals who experience weight-related discrimination tend to consume more calories, experience lower self-esteem, and are more likely to avoid physical activity and other beneficial health behaviors.7 Longitudinal studies have also shown that, independent of baseline BMI, experiencing weight-related discrimination is associated with higher future BMI.8,9 For instance, in one study, non-obese individuals who experienced weight discrimination had 2.5 times greater odds of becoming obese (OR = 2.54, 95% CI = 1.58–4.08) in 5 years (2006–2010) compared to those who had not experienced such discrimination.9
While the prevalence of weight-related discrimination is higher among persons with T2D compared to the general population,10 the impact of weight-related discrimination in this population has not been extensively studied. The few existing studies highlight that weight-related discrimination is associated with poor glycaemic control, higher diabetes distress, and reduced engagement in self-management behaviors among persons with T2D.11,12 A recent study in the US among 1,227 adults with T2D found that individuals who experience weight discrimination tend to rate their general health as poor.13 There is, however, a substantial gap in the literature regarding how weight-related discrimination produces poor health outcomes in persons with T2D.
Perceived stress, defined as the tendency to appraise one’s life circumstances as stressful,14 can mediate the health effects of discrimination. For instance, the effects of racial discrimination on sleep quality,15 depression and all-cause mortality16 have been found to be mediated by perceived stress. In the context of weight-related discrimination among persons with diabetes, the mediating effect of perceived stress has not been directly examined to the best of our knowledge. However, consistent with a mediation framework, studies among the general population have shown that weight-related discrimination is positively associated with stress17 and that stress is associated with poor health outcomes.16
Informed by the weight-based social identity threat theory,18 the purpose of this study was to explore perceived stress as a mediator of the association between weight-related discrimination and health outcomes in persons with T2D. The social identity threat theory outlines how experienced, suspected, or anticipated weight-related discrimination gets “under the skin” of individuals to affect their health outcomes.18 This study tests the hypotheses that perceived stress significantly mediates the association between weight-related discrimination and 1) psychological wellbeing, 2) physical wellbeing as shown in Figure 1.
Figure 1.
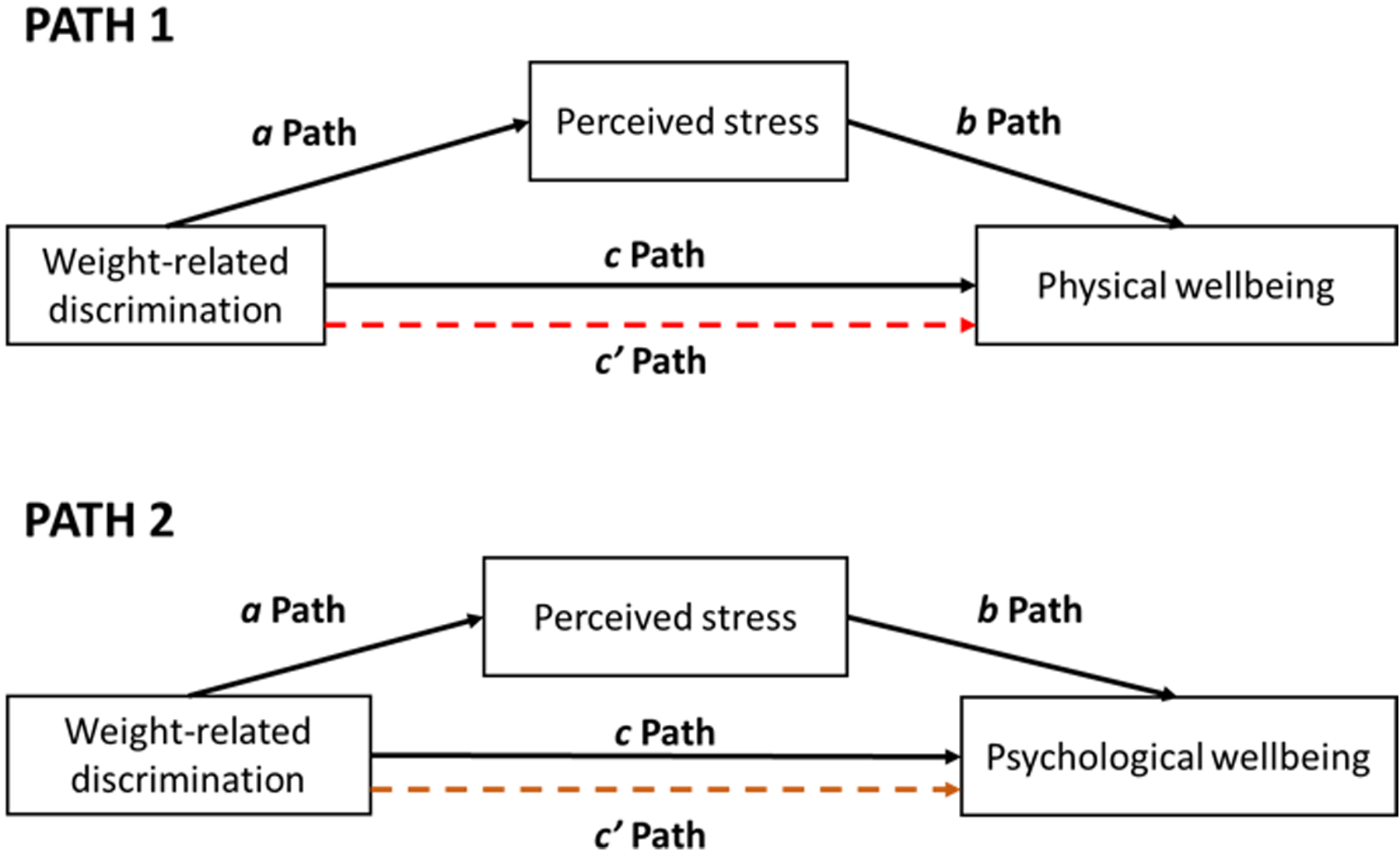
Hypothesized causal pathway of the effect of weight-related discrimination on psychological and physical wellbeing. The a-path shows the effect of the independent variable on the mediator, b-path shows the effect of the mediator on the outcome variable, the c-path shows the total effect of the independent variable on the outcome variable, and the c’-path shows the direct effect of the independent variable on the outcome variable.
Method
Study design
This study was a cross-sectional analysis of survey and anthropometric data obtained from the All of Us research program. The All of Us program is an initiative that seeks to recruit more than a million adults with a special focus on individuals who have been historically underrepresented in medical research in the US.19 Participants are required to complete a basic sociodemographic survey at baseline. Participants are also invited to complete surveys on personal and family health history, COVID-19, overall health, lifestyle, and social determinants of health (SDOH). Participants may also opt to visit a designated health facility for physical assessment, specimen collection, and genomic testing. They have the opportunity to share their Fitbit and electronic health records data with the research program.19 The institutional review board of the All of Us Research Program approved the study protocol for this research program. In the present study, we used the basic, lifestyle, and SDOH surveys as well as on-site height and weight measurement data.
Selection of study cohort
Participants for this cross-sectional analysis were selected using the All of Us Researcher Workbench, a cloud-based interactive platform.19 We used the Controlled Tier Curated Data Repository v7. Participants were included in the present analysis if they self-reported having T2D, had completed the SDOH survey (which contained items for measuring weight-related discrimination), were 18 years or older, and had complete data on all variables of interest. Overall, 17,507 participants self-reported having T2D. Out of this, 9,964 completed the SDOH survey. After excluding participants with missing data on variables of interest, 5,104 participants remained which formed the final analytic sample.
Independent variable
The primary independent variable was weight-related discrimination measured by the psychometrically validated Everyday Discrimination Scale (EDS) and administered as part of the SDOH survey of the All of Us program.20 EDS measures the level of discrimination using 9 items on a 6-point scale (1-Never to 6-Almost Every day). Example items include “You are treated with less courtesy than other people are” and “People act as if they’re better than you are”. The EDS has an additional item that asks participants about the main reason for their discriminatory experience with the following response options: ancestry or national origins, gender, race, age, religion, height, weight, some other aspect of participants physical appearance, sexual orientation, and education or income level.20 We defined weight-related discrimination using an indicator variable where 1= attribution of the everyday discrimination experience to weight, and 0=not attributing discrimination experience to weight or not reporting any experience of discrimination. This approach has been used in other studies.11,21
Outcome variables
The main outcome variables were psychological and physical wellbeing measured by the Patient Reported Outcomes Measurement Information System (PROMIS) Global Health scale.22 This validated instrument consists of 10 items rated on a 5-point scale. The instrument has two subscales: psychological (4-items) and physical wellbeing (4-items). The two remaining items were excluded from this study because they do not fit into any of the two subscales.23 Exemplar items of the psychological and physical wellbeing subscales include: “In the past 7 days, how often have you been bothered by emotional problems such as feeling anxious, depressed or irritable?” and “In the past 7 days, how would you rate your fatigue?” respectively. The total score is calculated by summing the items for each subscale. Higher scores are indicative of good psychological and physical well-being. The Cronbach’s alpha for the psychological and physical subscales were 0.85 and 0.75 respectively.
Mediator variable
The mediator variable for this study was perceived stress as measured by Cohen’s Perceived Stress Scale (PSS) and administered as part of the SDOH.24 The PSS is a 10-item validated global measure of perceived stress in the past 30 days. Each item is rated on a five-point Likert scale (0 - “Never”, 1- “Almost Never”, 2- “Sometimes”, 3- “Fairly Often”, 4- “Very Often”). A representative item on the scale is: “In the last month, how often have you felt that things were going your way?”. The total score is calculated by first reversing the scores on items 4, 5, 7, and 8, followed by summing all scores (range:0–40). Higher scores on the scale indicate greater perceived stress. The Cronbach’s alpha for the PSS in this study was 0.91.
Covariates
The covariates for this study included age, body mass index, sex assigned at birth (recoded as male and female), race and ethnicity (recoded as Non-Hispanic White, Non-Hispanic Black, Hispanic, Others), marital status (recoded as partnered, single, and widowed/separated/divorced), highest education (recoded as high school or less, some college education, college degree, and advanced degree), and annual income (recoded as less than $35,000, $35,000-$74,999, $75,000–99,999, and $100,000 or more). The “other” race and ethnicity included Asian, Pacific Islanders, Middle Eastern/North African, identifying with more than one race, and those who “prefer not to say”.
Data analysis
Data were analyzed in the Researcher Workbench of the All of Us program using R. Descriptive statistics such as means, standard deviations, proportions, and frequencies were computed as appropriate. The association between weight-related discrimination and all covariates were assessed using one-way analysis of variance (ANOVA), independent sample t-test, or Pearson’s correlation. Five multivariable linear regression models were developed to reflect the proposed associations among weight-related discrimination, perceived stress, and physical and psychological wellbeing while adjusting for all covariates as shown in Figure 1. Using Baron and Kenny’s causal step approach,25 we determined the appropriateness of a mediation analysis by first and separately testing for the direct association between weight-related discrimination and physical and psychological wellbeing (path c/total effects; models 2 and 4) (Figure 1). We also assessed the association of weight-related discrimination with perceived stress (path a; model 1), and perceived stress with physical and psychological wellbeing while adjusting for weight-related discrimination (path b; models 3 and 5). We observed that whereas the assumption of normality and linearity were met for all models, the Breusch-Pagan test indicated that the data were not homoscedastic as shown in supplementary file S2. We, therefore, used the robust, heteroscedastic-consistent standard errors (Huber-White sandwich estimator) to calculate the 95% confidence intervals for all regression point estimates26. The indirect effect was calculated as the product of the coefficient of path a and path b. The significance and 95% confidence intervals (CI) of the indirect, direct, and total effects were determined by nonparametric percentile bootstrapping with 5000 random samples. All regression coefficients can be interpreted as the mean difference in the scores of the dependent variable for individuals whose predictor scores differ by 1 unit. A 2-sided p-value of ≤5% was considered statistically significant.
Results
Characteristics of study participants
Overall, the study sample included N=5,104 adults with self-reported diabetes. As shown in Table 1, participants were, on average, 63.62±11.38 years old. Majority of them were female (55.53%), Non-Hispanic White (72.61%), married or living with a partner (56.92%), had a household income of <$35,000 (31.99%), and had some college education (33.54%). The mean BMI of the sample was 34.45 kg/m2 (69.8% had BMI greater than or equal to 30kg/m2 indicating obesity). Overall, 18.3% (n=935) of the participants had experienced weight-related discrimination. Those who reported weight-related discrimination were younger (57.28 vs 65.04 years, p<0.0001) and had a higher BMI (40.62 vs 33.06 kg/m2, p<0.0001). We also observed statistically significant bivariate associations between all sociodemographic characteristics and weight-related discrimination (Table 1).
Table 1.
Sample characteristics
| Characteristic | Total sample (N=5,104) | WD (n=935) | No WD (n=4169) | Test statistic, p-value |
|---|---|---|---|---|
| Age (mean, SD) | 63.62 (11.38) | 57.28 (11.59) | 65.04 (10.84) | = 18.69, p<0.0001 |
| Body Mass Index, kg/m2 (mean, SD) | 34.45 (7.69) | 40.62 (8.28) | 33.06 (6.82) | = −26.01, p<0.0001 |
| Sex at birth | =97.12**, p<0.0001 | |||
| Male | 2270 (44.47) | 280 (29.95) | 1990 (47.73) | |
| Female | 2834 (55.53) | 655 (70.05) | 2179 (52.27) | |
| Race and ethnicity | =20.69, p=0.0001 | |||
| Non-Hispanic White | 3706 (72.61) | 734 (76.99) | 2972 (69.01) | |
| Non-Hispanic Black | 668 (13.09) | 90 (10.49) | 578 (14.87) | |
| Hispanic | 479 (9.38) | 73 (8.25) | 406 (11.07) | |
| Other | 251 (4.92) | 38 (3.59) | 213 (3.05) | |
| Marital status | =53.79, p<0.0001 | |||
| Single | 776 (15.20) | 210 (22.82) | 566 (13.81) | |
| Married/living with partner | 2905 (56.92) | 496 (53.11) | 2409 (57.49) | |
| Widowed/Divorced/Separated | 1423 (27.88) | 229 (24.07) | 1194 (28.70) | |
| Household income | =19.10, p=0.0003 | |||
| <$35,000 | 1633 (31.99) | 348 (37.22) | 1285 (30.82) | |
| $35,000-$74,999 | 1509 (29.57) | 272 (29.09) | 1237 (29.67) | |
| $75,000-$99,999 | 661 (12.95) | 119 (12.73) | 542 (13.00) | |
| ≥$100,000 | 1301 (25.49) | 196 (20.96) | 1105 (26.51) | |
| Education | =9.83, p=0.02 | |||
| High school or less | 787 (15.42) | 127 (13.58) | 660 (15.83) | |
| Some college education | 1712 (33.54) | 353 (37.75) | 1359 (32.60) | |
| College graduate | 1337 (26.20) | 233 (24.92) | 1104 (26.48) | |
| Advanced degree | 1268 (24.84) | 222 (23.74) | 1046 (25.09) |
Unless otherwise stated, numbers represent frequencies and column-wise proportions; WD – Weight-related discrimination.
Yate’s continuity correction applied
Bivariate associations among discrimination, perceived stress, psychological wellbeing, BMI, and physical wellbeing
As shown in Table 2, physical wellbeing was significantly and positively correlated with psychological wellbeing (=0.62) but negatively correlated with BMI (=−0.31). Moreover, perceived stress was negatively correlated with psychological wellbeing (=−0.62) and physical wellbeing (=−0.42). Individuals with higher BMI tended to have higher perceived stress (=0.16.)
Table 2.
Descriptive statistics and correlation matrix for independent and outcome variables
| Descriptive | Correlation coefficients | ||||
|---|---|---|---|---|---|
| Mean (SD) | PS | PW | MW | BMI | |
| Perceived stress (PS) | 13.61 (8.05) | 1 | |||
| Physical wellbeing (PW) | 13.98 (2.89) | −0.42* | 1 | ||
| Psychological wellbeing (MW) | 13.99 (3.48) | −0.62* | 0.62* | 1 | |
| Body Mass Index (BMI) | 34.45 (7.69) | 0.16* | −0.31* | −0.21* | 1 |
p-value < 0.05
Multivariable association between independent, mediator and outcome variables
Persons with T2D who experienced weight-related discrimination had psychological and physical wellbeing scores that were, on average, 1.11 (Model 2: beta = −1.11, 95% CI: −1.35 to −0.87, p<0.0001) and 0.63 (Model 4: beta = −0.63, 95% CI: −0.83 to −0.43, p<0.0001) lower than those who did not experience discrimination, respectively. Weight-related discrimination was also associated with higher perceived stress (Model 1: beta = 3.62, 95% CI: 3.06 to 4.14) p<0.0001). Moreover, while adjusting for weight discrimination, higher perceived stress was significantly associated with poor psychological (Model 3: beta= −0.23, 95% CI: −0.24 to −0.22, p<0.0001) and physical wellbeing (Model 5: beta=−0.11, 95% CI: −0.12 to −0.10, p<0.0001) as shown in Table 3 (full results in supplementary table S2). In models 3 and 5, the associations between weight-related discrimination and psychological and physical wellbeing reduced but remained significant (p<0.05) after adjusting for perceived stress, suggesting that perceived stress may be a partial mediator in these relationships.
Table 3.
Multiple linear regression models for the causal steps mediation approach.
| Model 1: stress | Model 2: psychological | Model 3: psychological | Model 4: physical | Model 5: Physical | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Beta (95% CI) | p | Beta (95% CI) | p | Beta (95% CI) | p | Beta (95% CI) | p | Beta (95% CI) | p |
| Perceived stress | - | - | - | - | −0.23 (−0.24, −0.22) | <0.0001 | - | −0.11 (−0.12, −0.10) | <0.0001 | |
| Weight-related discrimination | 3.62 (3.06, 4.17) | <0.0001 | −1.11 (−1.35, −0.87) | <0.00001 | −0.29 (−0.50, −0.08) | 0.007 | −0.63 (−0.83, −0.43) | <0.0001 | −0.22 (−0.41, −0.02) | 0.028 |
| Adjusted | 21.18% | 23.35% | 45.14% | 23.75% | 31.57% | |||||
| Model significance | =100.8, p < 0.0001 | = 108.8, p < 0.0001 | = 270.4, p < 0.0001 | = 112.1, p < 0.0001 | = 152.9, p < 0.0001 | |||||
Model 1 tests the effect of weight-related discrimination (independent variable) on perceived stress (mediator); Model 2 tests the direct effect of weight-related discrimination on psychological wellbeing (outcome variable); Model 3 tests the effect of perceived stress on psychological wellbeing while adjusting for weight-related discrimination; Model 4 tests the direct effects of weight-related discrimination on physical wellbeing (outcome variable); Model 5 tests the effects of perceived stress on physical wellbeing while adjusting for weight-related discrimination. All five models were adjusted for age, body mass index, sex at birth, marital status, race and ethnicity, household income, and education. The full linear regression model, showing the effects of covariates, is in supplementary table S2.
CI: Confidence Interval.
In addition, higher household income and education were associated with better physical and psychological wellbeing as well as lower perceived stress (supplementary table S2). Being married or living with a partner was significantly associated with better psychological wellbeing. Higher BMI was significantly associated with poorer psychological and physical wellbeing (p<0.001).
Mediation effect of perceived stress
Perceived stress partially mediated the effect of weight-related discrimination on psychological (Average Causal Mediation Effect [ACME] = −0.82, 95% CI: −0.95, −0.69, p<0.0001) and physical wellbeing (ACME = −0.41; 95% CI: −0.48, −0.34; p<0.0001). The path through perceived stress accounted for 74% of the effect of weight-related discrimination on psychological wellbeing (95% CI 0.62, 0.92; p<0.0001) and 65% of the effect on physical wellbeing (95% CI: 0.48, 0.94; p<0.0001). There was a significant direct negative effect of discrimination on psychological (Average direct effect [ADE] = −0.29; 95% CI: −0.49, −0.08; p =0.008) and physical wellbeing (ADE = −0.22; 95% CI: −0.42, −0.03; p = 0.025) after accounting for the mediation effects of perceived stress, indicating partial mediation as shown in Table 4. In summary, weight-related discrimination was associated with higher perceived stress, which was in turn associated with poorer physical and psychological wellbeing (Figure 2).
Table 4.
Mediation effects (bootstrapping results): direct, indirect, and relative effects and their 95% CI
| Outcome | Effect | Beta | 95% CI | P |
|---|---|---|---|---|
| Psychological wellbeing | ACME | −0.82 | −0.95, −0.69 | <0.0001 |
| ADE | −0.29 | −0.49, −0.08 | 0.008 | |
| Total effect | −1.11 | −1.35, −0.86 | <0.0001 | |
| Proportion mediated | 0.74 | 0.62, 0.92 | <0.0001 | |
| Physical wellbeing | ACME | −0.41 | −0.48, −0.34 | <0.0001 |
| ADE | −0.22 | −0.42, −0.03 | 0.025 | |
| Total effect | −0.63 | −0.84, −0.43 | <0.0001 | |
| Proportion mediated | 0.65 | 0.48, 0.94 | <0.0001 |
ACME – Average Causal Mediation effect; ADE – Average Direct Effect
Figure 2.

Path diagram for the mediation analysis. *** indicates p-value < 0.05
Discussion
The current study addressed a critical research gap by exploring perceived stress as a mediator of the effect of weight-related discrimination on physical and psychological health outcomes among persons with T2D. We found that approximately 18% of study participants reported having experienced weight-related discrimination. This substantial prevalence is particularly consequential for persons with T2D given the unique challenges they face in managing their health, and the potential for experiencing other forms of stigma related to their diabetes status. We also found that weight-related discrimination was independently associated with poor physical and psychological wellbeing. These associations were partially mediated by perceived stress such that weight-related discrimination was associated with greater perceived stress, and greater perceived stress was associated with poorer physical and psychological wellbeing.
The prevalence of weight-related discrimination in our study sample was much higher than what similar studies that used the Everyday Discrimination Scale report among the general population.8,9,21 For instance, in the Midlife in the United States (MIDUS) study, out of a total of 6,157 participants, 8% reported experiencing weight-related discrimination.9 Moreover, using data from the Nurses’ Health Study, Raffoul and colleagues reported a 7.8% prevalence of weight-related discrimination among cis-gender women.21 Although other studies have recorded a much higher prevalence of weight-related discrimination among persons with T2D10 as well as the general population,27 these studies used different instruments to measure discrimination than what was used in the current study. Our findings of a higher prevalence of weight-related discrimination among persons with T2D compared to the general population were not unexpected given the higher prevalence of obesity in our sample and the evidence linking higher BMI with greater likelihood of experiencing weight-related discrimination.28 For persons with T2D, the experience of weight-related discrimination can serve as a significant obstacle in individuals’ ability to engage in beneficial self-management behaviors and meet glycaemic goals.11
Earlier studies have noted the multiplicity of discriminations that persons with T2D experience, including the potential for being stigmatized for both diabetes and weight status.10 Consistent with the intersectionality framework, which highlights the various ways that multiple identities including a person’s ethnicity, socioeconomic status, weight status, age, and disease status interconnect to influence health behaviors and outcomes,29 the findings from our study highlight how the wellbeing of persons with T2D is shaped by other aspects of their identities. For instance, we found that persons with T2D who had higher income, educational attainment, and lower BMI were more likely to have better psychological and physical well-being.
Perceived stress was found to be a significant mediator of the association between weight-related discrimination and health outcomes. This finding was not surprising given the decades of research evidence linking stigma and stress, and stress and health outcomes. For instance, Hatzenbuehler et al.17 report that individuals who experience instances of weight-related discrimination are three times more likely to experience higher levels of perceived stress when compared to those who did not face such discrimination. The present study is the first known study to examine these associations among persons with T2D who experience weight-related discrimination.
The study has several limitations. First, given the cross-sectional design of this study, our mediation analysis is only exploratory and preclude causal conclusions. Second, the use of self-reported measures may likely lead to social desirability and recall bias. Third, our analysis did not include an exploration of a potential interaction between weight and diabetes-related stigma due to the absence of diabetes stigma variable in the dataset. Understanding the intersection between these two forms of stigmas can provide deeper insight into how different aspects of an individual’s identity interact to affect health outcomes. This could be a future research direction worth exploring. The Everyday Discrimination Scale does not restrict respondents to a particular time period, so it is not clear if the attribution of discrimination to weight occurred when participants had T2D or earlier. Fourth, the American Indian/Alaskan Native population in our final study sample was small, hence was collapsed into the “other race” category. Given that this population has the highest prevalence of diabetes in the US,30 more efforts should be made to increase their representation in diabetes research. Lastly, our analysis did not account for other system-level and disease-related stressors (e.g. unsafe neighborhoods and comorbidities) that may have contributed to how much stress participants reported.
The findings from this study have several implications for research and public health practice. Our study highlights weight-related discrimination among persons with T2D as a public health concern that needs to be addressed. A recent narrative review identified strategies including education on obesity and evoking societal empathy as ways of reducing weight-related discrimination.31 Interventions to mitigate weight discrimination may be best targeted at multiple socio-ecological levels. For instance, interventions may include national or facility-level policies that prohibit discrimination based on one’s weight. Interventions may also target individuals to help relieve distress that is triggered by discriminatory experiences and to build their coping resources. The mediating role of perceived stress found in the current study could also be leveraged. Given that weight-related discrimination is associated with poor health outcomes through elevated stress, interventions that target stress may disrupt this pathway thereby helping to reduce the health impact of weight-related discrimination. This assertion should be tested in future studies.
Supplementary Material
Novelty statement.
What is already known?
Persons with type 2 diabetes (T2D) have high prevalence of obesity and thus, are exposed to stigma-related stressors based on their weight; yet little is known about how these stressors influence health outcomes of persons with T2D.
What this study has found?
Weight-related discrimination is associated with poor physical and psychological wellbeing among persons with T2D.
Perceived stress partially mediates the effect of weight-related discrimination on health outcomes.
What are the implications of the study?
Given that weight-related discrimination is associated with poor health outcomes through elevated stress, interventions that target stress may disrupt this pathway thereby helping to reduce the health impact of weight-related discrimination. This assertion should be tested in future studies.
Acknowledgments
The All of Us Research Program is supported by the National Institutes of Health, Office of the Director: Regional Medical Centers: 1 OT2 OD026549; 1 OT2 OD026554; 1 OT2 OD026557; 1 OT2 OD026556; 1 OT2 OD026550; 1 OT2 OD 026552; 1 OT2 OD026553; 1 OT2 OD026548; 1 OT2 OD026551; 1 OT2 OD026555; IAA #: AOD 16037; Federally Qualified Health Centers: HHSN 263201600085U; Data and Research Center: 5 U2C OD023196; Biobank: 1 U24 OD023121; The Participant Center: U24 OD023176; Participant Technology Systems Center: 1 U24 OD023163; Communications and Engagement: 3 OT2 OD023205; 3 OT2 OD023206; and Community Partners: 1 OT2 OD025277; 3 OT2 OD025315; 1 OT2 OD025337; 1 OT2 OD025276. In addition, the All of Us Research Program would not be possible without the partnership of its participants.
Funding
The authors received no funding for the present analysis of the All of Us data.
Footnotes
Conflicts of interest: None
Data availability
The data used for this study are available to approved researchers following registration, completion of ethics training and attestation of a data use agreement through the All of Us Research Workbench platform, which can be accessed via https://workbench.researchallofus.org/login. Currently, data is only available to individuals based in the US and working in an institution that has data use agreement with the All of Us research program.
Reference
- 1.International Diabetes Federation. Diabetes Facts & figures. Published 2021. Accessed November 18, 2022. https://idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html
- 2.Akyirem S, Ekpor E, Namumbejja Abwoye D, Batten J, Nelson LE. Type 2 diabetes stigma and its association with clinical, psychological, and behavioral outcomes: a systematic review and meta-analysis. Diabetes Research and Clinical Practice. Published online June 10, 2023:110774. doi: 10.1016/j.diabres.2023.110774 [DOI] [PubMed] [Google Scholar]
- 3.Ekpor E, Akyirem S, Adade Duodu P. Prevalence and associated factors of overweight and obesity among persons with type 2 diabetes in Africa: a systematic review and meta-analysis. Annals of Medicine. 2023;55(1):696–713. doi: 10.1080/07853890.2023.2182909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Brown A, Flint SW, Batterham RL. Pervasiveness, impact and implications of weight stigma. eClinicalMedicine. 2022;47:101408. doi: 10.1016/j.eclinm.2022.101408 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rubino F, Puhl RM, Cummings DE, et al. Joint international consensus statement for ending stigma of obesity. Nat Med. 2020;26(4):485–497. doi: 10.1038/s41591-020-0803-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hayward LE, Vartanian LR, Pinkus RT. Weight Stigma Predicts Poorer Psychological Well-Being Through Internalized Weight Bias and Maladaptive Coping Responses. Obesity. 2018;26(4):755–761. doi: 10.1002/oby.22126 [DOI] [PubMed] [Google Scholar]
- 7.Major B, Hunger JM, Bunyan DP, Miller CT. The ironic effects of weight stigma. Journal of Experimental Social Psychology. 2014;51:74–80. doi: 10.1016/j.jesp.2013.11.009 [DOI] [Google Scholar]
- 8.Jackson SE, Beeken RJ, Wardle J. Perceived weight discrimination and changes in weight, waist circumference, and weight status. Obesity (Silver Spring). 2014;22(12):2485–2488. doi: 10.1002/oby.20891 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sutin AR, Terracciano A. Perceived weight discrimination and obesity. PLoS One. 2013;8(7):e70048. doi: 10.1371/journal.pone.0070048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Himmelstein MS, Puhl RM. At multiple fronts: Diabetes stigma and weight stigma in adults with type 2 diabetes. Diabetic medicine : a journal of the British Diabetic Association. 2021;38(1):e14387. [DOI] [PubMed] [Google Scholar]
- 11.Potter L, Wallston K, Trief P, Ulbrecht J, Juth V, Smyth J. Attributing discrimination to weight: associations with well-being, self-care, and disease status in patients with type 2 diabetes mellitus. J Behav Med. 2015;38(6):863–875. doi: 10.1007/s10865-015-9655-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Puhl RM, Himmelstein MS, Hateley-Browne JL, Speight J. Weight stigma and diabetes stigma in U.S. adults with type 2 diabetes: Associations with diabetes self-care behaviors and perceptions of health care. Diabetes Res Clin Pract. 2020;168:108387. doi: 10.1016/j.diabres.2020.108387 [DOI] [PubMed] [Google Scholar]
- 13.Puhl RM, Himmelstein MS, Speight J. Weight Stigma and Diabetes Stigma: Implications for Weight-Related Health Behaviors in Adults With Type 2 Diabetes. Cd (Clinical Diabetes). 2022;40(1):51–61. doi: 10.2337/cd20-0071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wang S, Zhao Y, Zhang L, et al. Stress and the brain: Perceived stress mediates the impact of the superior frontal gyrus spontaneous activity on depressive symptoms in late adolescence. Hum Brain Mapp. 2019;40(17):4982–4993. doi: 10.1002/hbm.24752 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Majeno A, Tsai KM, Huynh VW, McCreath H, Fuligni AJ. Discrimination and Sleep Difficulties during Adolescence: The Mediating Roles of Loneliness and Perceived Stress. J Youth Adolesc. 2018;47(1):135–147. doi: 10.1007/s10964-017-0755-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lorenzo-Blanco EI, Unger JB. Ethnic Discrimination, Acculturative Stress, and Family Conflict as Predictors of Depressive Symptoms and Cigarette Smoking Among Latina/o Youth: The Mediating Role of Perceived Stress. J Youth Adolesc. 2015;44(10):1984–1997. doi: 10.1007/s10964-015-0339-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hatzenbuehler ML, Keyes KM, Hasin DS. Associations Between Perceived Weight Discrimination and the Prevalence of Psychiatric Disorders in the General Population. Obesity. 2009;17(11):2033–2039. doi: 10.1038/oby.2009.131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hunger JM, Major B, Blodorn A, Miller CT. Weighed down by stigma: How weight-based social identity threat contributes to weight gain and poor health. Social and personality psychology compass. 2015;9(6):255. doi: 10.1111/spc3.12172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ramirez AH, Sulieman L, Schlueter DJ, et al. The All of Us Research Program: Data quality, utility, and diversity. Patterns (N Y). 2022;3(8):100570. doi: 10.1016/j.patter.2022.100570 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Williams DR, Yan Yu null, Jackson JS, Anderson NB. Racial Differences in Physical and Mental Health: Socio-economic Status, Stress and Discrimination. J Health Psychol. 1997;2(3):335–351. doi: 10.1177/135910539700200305 [DOI] [PubMed] [Google Scholar]
- 21.Raffoul A, Beccia AL, Jackson DA, et al. Associations between weight discrimination and the use of potentially harmful dietary supplements during the COVID-19 pandemic in the United States. Social Science & Medicine. 2023;335:116232. doi: 10.1016/j.socscimed.2023.116232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hays RD, Bjorner JB, Revicki DA, Spritzer KL, Cella D. Development of physical and mental health summary scores from the patient-reported outcomes measurement information system (PROMIS) global items. Qual Life Res. 2009;18(7):873–880. doi: 10.1007/s11136-009-9496-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lapin B, Katzan IL. PROMIS global health: potential utility as a screener to trigger construct-specific patient-reported outcome measures in clinical care. Qual Life Res. 2023;32(1):105–113. doi: 10.1007/s11136-022-03206-y [DOI] [PubMed] [Google Scholar]
- 24.Cohen S, Kamarck T, Mermelstein R. A Global Measure of Perceived Stress. Journal of Health and Social Behavior. 1983;24(4):385. doi: 10.2307/2136404 [DOI] [PubMed] [Google Scholar]
- 25.Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51(6):1173–1182. doi: 10.1037/0022-3514.51.6.1173 [DOI] [PubMed] [Google Scholar]
- 26.White H A heteroskedasticity-consistent covariance matrix estimator and a direct test for heteroskedasticity. Econometrica: journal of the Econometric Society. Published online 1980:817–838. [Google Scholar]
- 27.Gerend MA, Zetrenne S, Sutin AR, Naar S, Maner JK. Weight Discrimination and Health Risk Behavior in Racial, Ethnic, and Sexual Minority Adults. Annals of Behavioral Medicine. 2023;57(7):571–581. doi: 10.1093/abm/kaad003 [DOI] [PubMed] [Google Scholar]
- 28.Himmelstein MS, Puhl RM, Quinn DM. Intersectionality: An Understudied Framework for Addressing Weight Stigma. American Journal of Preventive Medicine. 2017;53(4):421–431. doi: 10.1016/j.amepre.2017.04.003 [DOI] [PubMed] [Google Scholar]
- 29.Crenshaw K Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine. The University of Chicago Legal Forum, S. 139–167. New York: Harper Collins; 1989. [Google Scholar]
- 30.Centre for Disease Control and Prevention. National Diabetes Statistics Report | Diabetes | CDC. Published 2022. Accessed August 22, 2022. https://www.cdc.gov/diabetes/data/statistics-report/index.html
- 31.Talumaa B, Brown A, Batterham RL, Kalea AZ. Effective strategies in ending weight stigma in healthcare. Obes Rev. 2022;23(10):e13494. doi: 10.1111/obr.13494 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data used for this study are available to approved researchers following registration, completion of ethics training and attestation of a data use agreement through the All of Us Research Workbench platform, which can be accessed via https://workbench.researchallofus.org/login. Currently, data is only available to individuals based in the US and working in an institution that has data use agreement with the All of Us research program.