

Abstract
A single dose of psilocybin, a psychedelic that acutely causes distortions of space–time perception and ego dissolution, produces rapid and persistent therapeutic effects in human clinical trials1–4. In animal models, psilocybin induces neuroplasticity in cortex and hippocampus5–8. It remains unclear how human brain network changes relate to subjective and lasting effects of psychedelics. Here we tracked individual-specific brain changes with longitudinal precision functional mapping (roughly 18 magnetic resonance imaging visits per participant). Healthy adults were tracked before, during and for 3 weeks after high-dose psilocybin (25 mg) and methylphenidate (40 mg), and brought back for an additional psilocybin dose 6–12 months later. Psilocybin massively disrupted functional connectivity (FC) in cortex and subcortex, acutely causing more than threefold greater change than methylphenidate. These FC changes were driven by brain desynchronization across spatial scales (areal, global), which dissolved network distinctions by reducing correlations within and anticorrelations between networks. Psilocybin-driven FC changes were strongest in the default mode network, which is connected to the anterior hippocampus and is thought to create our sense of space, time and self. Individual differences in FC changes were strongly linked to the subjective psychedelic experience. Performing a perceptual task reduced psilocybin-driven FC changes. Psilocybin caused persistent decrease in FC between the anterior hippocampus and default mode network, lasting for weeks. Persistent reduction of hippocampal-default mode network connectivity may represent a neuroanatomical and mechanistic correlate of the proplasticity and therapeutic effects of psychedelics.
Subject terms: Consciousness, Neuroscience, Neural circuits, Biomarkers, Drug development
Healthy adults were tracked before, during and after high doses of psilocybin and methylphenidate to assess how psychedelics can change human brain networks, and psilocybin was found to massively disrupt functional connectivity in cortex and subcortex with some changes persisting for weeks.
Main
Psychedelic drugs can reliably induce powerful acute changes in the perception of self, time and space by agonism of the serotonin 2A (5-HT2A) receptor9,10. In clinical trials, a single high dose of psilocybin (25 mg) has demonstrated rapid and sustained symptom relief in depression1–3,11–14, addiction4,15 and end-of-life anxiety13,14. Together, these observations indicate that psychedelics should induce potent acute (lasting roughly 6 hours) and persistent (24 hours to 21 days) neurobiological changes.
In rodent models, transient activation of the 5-HT2A receptors by a psychedelic can alter neuronal communication in 5-HT2A-rich regions (for example, the medial frontal lobe) and induce persistent plasticity-related phenomena5–7. Synaptogenesis in the medial frontal lobe and anterior hippocampus is thought to be key to the neurotrophic antidepressant effects of psilocybin5,16,17. Yet, inherent limitations of rodent models, and imperfect homology to the human 5-HT2A receptor18, limit the generalizability of these assertions.
Understanding the effects of psychedelics on human brain networks is critical to unlocking their therapeutic mechanisms. In humans, during the roughly 6 hour duration of action, psilocybin increases glutamate signalling and glucose metabolism19–21, broadly decreases the power of electrophysiological signals22, reduces hemodynamic fluctuations23 and decreases segregation between functional networks24. The drivers of these acute changes are poorly understood, particularly in the subcortex. Preliminary efforts to identify network changes in the weeks after psilocybin have yielded mixed results25–27. Persistent effects of psilocybin on clinically relevant circuits have yet to be characterized in humans.
The ventromedial prefrontal cortex and anterior and middle hippocampus are functionally connected to the default mode network (DMN)28,29. Increased FC between the hippocampus and DMN has been associated with depression symptoms30 and decreased FC is associated with treatment31,32. These 5-HT2A receptor rich33 and depression associated default mode regions34–36 are candidates for mediating the neurotrophic antidepressant effects of psychedelics.
Precision functional mapping uses dense repeated functional magnetic resonance imaging (fMRI) sampling37–41 to reveal the time course of individual-specific intervention-driven brain changes42. This approach accounts for inter-individual variability in brain networks37 and capitalizes on the high stability of networks within individuals from day to day38. Using precision functional mapping, we observed individual-specific acute and persistent brain changes following a single high dose of psilocybin.
Healthy young adults received 25 mg psilocybin and 40 mg methylphenidate (MTP, generic name Ritalin, dose-matched for arousal effects) 1–2 weeks apart and underwent regular MRI sessions (roughly 18 per participant) before, during, between and after the two drug doses (Extended Data Fig. 1, Supplementary Table 1 and Supplementary Video 1: data quality metrics for 129 total MRI visits). Dense predrug sampling familiarized participants with the scanner and established baseline variability.
Extended Data Fig. 1. Quantifying psilocybin effects with precision functional mapping: design.

a) Schematic illustrating the study protocol of the individual-specific precision functional mapping study of acute and persistent effects of psilocybin (single dose: 25 mg). Repeated longitudinal study visits enabled high-fidelity individual brain mapping, measurement of day-to-day variance, and acclimation to the scanner. The open label replication protocol 6-12 months later included one or two scans each of baseline, psilocybin, and after drug. b) Timeline of imaging visits for 7 participants. c) Head motion comparisons across psychedelics studies55,56. Average head motion (FD, framewise displacement, in mm) off and on drug compared between our dataset and prior psychedelic fMRI studies. Unpaired two-sided t-test: nPSIL 2012 = 15, nLSD,2016 = 20, nPSIL(PFM) = 7; off drug PSIL2012-PSIL(PFM) t(274) = −4.57, Puncorr = 7.33 × 10−5; off drug LSD2016-PSIL(PFM) t(286) = −4.03, Puncorr = 7.34 × 10−6; on drug PSIL2012-PSIL(PFM) t(46) = −1.80, Puncorr = 0.079; on drug LSD2016-PSIL(PFM) t(88) = −0.73, Puncorr = 0.46. Dotted line at FD of 0.2 mm. Dark gray bars indicate quartiles, light gray violins indicate distribution. *Puncorr < 0.05, +P < 0.1. d) Timeline for an example participant (P1). e) Participants reported significantly higher scores on all dimensions of the mystical experience questionnaire during psilocybin (red) than placebo (40 mg methylphenidate; blue). Paired two-tailed t-test, n = 7; Mystical t(6) = −3.64, Puncorr = 0.011; Positive Mood t(6) = −5.44, Puncorr = 0.0016; Transcendence t(6) = −4.98, Puncorr = 0.0025; Ineffability t(6) = −2.54, Puncorr = 0.044. Error bars indicate SEM.
Psilocybin disrupts brain connectivity
Psilocybin acutely caused profound and widespread brain FC changes (Fig. 1a) across most of the cerebral cortex (P < 0.05 based on two-sided linear mixed-effects (LME) model and permutation testing), but most prominent in association networks (FC change mean (standard deviation, s.d.): association cortex 0.44 (0.03), primary cortex 0.36 (0.05)). In the subcortex the largest psilocybin-associated FC changes were seen in DMN connected parts of the thalamus, basal ganglia, cerebellum and hippocampus29,43,44 (Fig. 1a and Extended Data Fig. 2). In the hippocampus, foci of strong FC disruption were located in the anterior hippocampus (Montreal Neurological Institute coordinates −24, −22, −16 and 24, −18, −16). Other large FC disruptions were seen in mediodorsal and paraventricular thalamus45 and anteromedial caudate. In the cerebellum, the largest FC changes were seen in the DMN connected areas44 (Fig. 1a).
Fig. 1. Acute psilocybin effects on functional brain organization.

FC change (Euclidean distance) was calculated across the cortex and subcortical structures. Effects of drug condition were tested with an LME model in n = 6 longitudinally sampled participants over ten sessions with psilocybin and six sessions with methylphenidate (MTP) (a and b are thresholded at P < 0.05 based on permutation testing with TFCE; see unthresholded statistical maps in Extended Data Fig. 2). a, Psilocybin-associated FC change, including in subcortex. a, anterior; p, posterior; L, left; R, right. b, MTP-associated FC change. c, Typical day-to-day variability as a control to the drug conditions (unthresholded: not included in LME model). d, Average FC change in individual-defined networks. Open circles represent individual participants. FC change is larger in DMN than other networks. Rotation-based null model (spin test62,97): ten psilocybin doses, 1,000 permutations, one-sided Pspin < 0.001, (Pspin > 0.05 for all other networks). **P < 0.001, uncorrected. e, Whole-brain FC change (Euclidean distance from baseline) for all rest scans across conditions. FC change for MTP, psilocybin and day-to-day are in comparison to same-participant baseline. White dots indicate median, vertical lines indicate quartiles. LME model predicting whole-brain FC change: ten psilocybin doses (275 observations), estimate (95% CI) = 15.83 (13.50, 18.15), t(266) = 13.39, P = 1.36 × 10−31, uncorrected. For the full FC distance matrix with session labels, see Extended Data Fig. 3. f,g, Comparison of the differences in FC change to differences in psychedelic experiences. f, Individual FC change maps and MEQ30 scores for two exemplars (see Extended Data Fig. 4 for all drug sessions). g, The relationship between whole-brain FC change and mystical experience rating is plotted for all drug sessions (psilocybin and MTP). The LME model demonstrated a significant relationship: 16 drug doses (ten psilocybin, six MTP), estimate (95% CI) = 69.78 (50.15, 89.41), t(13) = 7.68, P = 3.5 × 10−6, uncorrected. h, The relationship between FC change and MEQ30 (r2) is mapped across the cortical surface.
Extended Data Fig. 2. Unthresholded vertex-wise FC change maps.

T-statistic maps, resulting from the linear mixed effects (LME) model based on vertex-wise FC change (Euclidean distance from baseline scans) across the cortex and subcortical structures for every scan. Higher t values indicate a larger change from baseline (pre-drug) scans. Effects of drug condition (baseline, psilocybin, methylphenidate, post-psilocybin, post-methylphenidate), were modeled as fixed effects. For example, if drug 1 was psilocybin and drug 2 was methylphenidate, then scans between drug visits were labeled post-psilocybin and scans after drug 2 were labeled post-methylphenidate.
By comparison, MTP-associated FC changes localized to sensorimotor systems (Fig. 1b and Extended Data Fig. 2) and paralleled the map of day-to-day variability (Fig. 1c) probably due to arousal effects39. Psilocybin-associated FC change was largest in the DMN (Fig. 1d and Supplementary Fig. 1; averaged across all psilocybin sessions; spin test, 1,000 permutations, one-sided Pspin < 0.001; Pspin > 0.05 for all other networks). However, MTP-associated FC change was largest in motor and action networks (Pspin = 0.002; Pspin > 0.05 for all other networks; Supplementary Fig. 1b).
Despite MTP and psilocybin causing similar increases in heart rate (Supplementary Fig. 2), the effects of psilocybin on FC were more than threefold larger than the effects of MTP (Fig. 1e; post hoc two-sided t-test; P = 3.6 × 10−6, uncorrected). The psilocybin effects also dwarfed those of other control conditions (Fig. 1e; day-to-day change (normalized) 1; task 1.22, MTP 1.10, high head motion 1.29, psilocybin 3.52, between person 3.53; Extended Data Fig. 3; these effects were robust to preprocessing choices: Supplementary Figs. 3 and 4). To put the effects of psilocybin into perspective, it helps to consider that the mean changes in brain organization caused by the drug were as large as the differences in brain organization between different people (Fig. 1e).
Extended Data Fig. 3. Functional connectivity (FC) distance and condition matrices for all fMRI scans.

Following Gratton et al.38, we compared FC matrices between rs-fMRI sessions to quantify contributors to variability in whole-brain FC. Under this approach, the effects of group, individual, session, and drug (as well as their interactions) are examined by first calculating the Euclidean distance among every pair of FC matrices (i.e., distance among the linearized upper triangles). a) In the resulting second-order distance matrix, each row and column show whole-brain FC from a single study visit. The colours in the matrix indicate distance between functional networks for a pair of visits (i.e., Euclidean distance between the linearized upper triangles of two FC matrices). Panels b and c demonstrate how the distance matrix was subdivided to compare different conditions. b) Black triangles represent distinct individuals. Replication protocol visits are listed at the end. c) Task and rest scans are shown in white and orange, respectively. Note that psilocybin scans (black arrows pointing to P1 psilocybin scans in panel a are very dissimilar to no-drug scans from the same individual (left arrow; in a) but have heightened similarity to psilocybin scans from other individuals (right arrow in a).
The psychedelic experience
The large amount of data collected per participant, under the individual-specific imaging model, allowed us to move beyond group-analyses and compare the subjective psychedelic experience (30-item Mystical Experience Questionnaire, MEQ30)46 to brain function data session-by-session (Fig. 1f). The MEQ30 is a self-assessment instrument used to measure the intensity and quality of mystical experiences, including feelings of connectedness, transcendence of time and space, and a sense of awe, with a maximum score of 150 (ref. 46). Across psilocybin sessions and participants, FC change tracked with the intensity of the subjective experience (Fig. 1f and Extended Data Fig. 4). Correlating the whole-brain FC change (x axis) against the MEQ30 scores (y axis) for all drug sessions (Fig. 1g) revealed an r2 = 0.81 (LME model predicting MEQ30 score: effect of FC change, t(13) = 7.68; P = 3.5 × 10−6, uncorrected). Head motion was not significantly correlated with MEQ30 scores (effect of framewise displacement, t(13) = −1.26, P = 0.23, uncorrected). Projecting the relationship between someone’s mystical experience and the corresponding FC change onto the brain (Fig. 1h, vertex-wise) showed it to be driven by association cortex, relatively sparing primary motor and sensory regions. Of the four MEQ30 dimensions (mystical, positive mood, transcendence of time and space, and ineffability), the one most strongly correlating with brain change was transcendence (for example, ‘loss of your usual sense of time or space’, r2 = 0.86, Supplementary Fig. 5), however, all dimensions were highly correlated (r > 0.8). Repeated sampling enabled us to determine that the inter-individual variability in the effects of psilocybin in the brain was more likely related to differences in drug effects than measurement error (likelihood ratio test of participant-specific response to psilocybin, P = 0.00245, uncorrected)47,48.
Extended Data Fig. 4. Participant-specific FC change maps for drug sessions.

Individual participant methylphenidate (MTP) and psilocybin (PSIL) FC change maps. Left most column shows individuals’ functional networks. Right 3 columns show FC change maps, generated by calculating Euclidean distance from baseline seedmaps for each vertex. For each session the total score on the Mystical Experience Questionnaire (MEQ30: out of a maximum of 150) is given in the upper right corner. *P5 had an episode of emesis 30 minutes after drug ingestion during PSIL2.
The psychedelic dimension
To examine the latent dimensions of brain network changes we performed multidimensional scaling (MDS) on the parcellated FC matrices from every fMRI scan38. MDS is blind to session labels (for example, drug, participant). Yet, dimension 1, which explained the largest amount of variability, separated psilocybin from other scans (Fig. 2a), apart from one session during which the participant (P5R) had emesis 30 minutes after taking psilocybin (dark red dots on the left of Fig. 2a). The higher score on dimension 1 associated with psilocybin, corresponded to reduced segregation between the DMN and other networks (fronto-parietal49, dorsal attention50, salience51 and action-mode52,53) that are typically anticorrelated with it54 (Fig. 2b and Extended Data Fig. 5). To determine whether this reflects a common effect of psilocybin that generalizes across datasets and psychedelics, we calculated dimension 1 scores for extant datasets from participants receiving intravenous (i.v.) psilocybin55 and lysergic acid diethylamide (LSD)56. Psychedelic treatment increased dimension 1 in nearly every participant in the psilocybin and LSD datasets (Fig. 2c), suggesting that this is a common effect across psychedelic drugs and individuals.
Fig. 2. Data-driven clustering of brain network variability.

MDS blind to session labels was used to assess brain changes across conditions. a, In the scatter plots, each point represents whole-brain FC from a single 15 min scan, plotted in a multidimensional space on the basis of the similarity between scans. Dimensions 1 and 4 showed strong effects of psilocybin. The top shows scans coded on the basis of drug condition. Dark red denotes that the participant had an episode of emesis shortly after taking psilocybin. The bottom shows scans coloured on the basis of participant identity. Dimension 1 separates psilocybin from non-drug and MTP scans in most cases. See Extended Data Fig. 5 for the dimension 1–4 weight matrices. b, Visualization of dimension 1 weights. The top 1% of edges (connections) are projected onto the brain (green indicates connections that are increased by psilocybin). Cerebellar connections are included although the structure is not shown. c, Re-analysis of dimension 1 in extant datasets with intravenous psilocybin (left, ref. 55, paired two-sided t-test of change in dimension 1 score, n = 9, t(8) = 2.97, P = 0.0177, uncorrected) and LSD (right, ref. 56, paired two-sided t-test: n = 16, t(15) = 4.58, P = 3.63 × 10−4, uncorrected). *P < 0.05, **P < 0.001, uncorrected. d, Average effects of psilocybin on network FC, shown separately for within-network integration (left) and between network segregation (right). For network integration (left), blue indicates a loss of FC (correlations) between regions within the same network. For network segregation (right), blue indicates a loss of FC (anticorrelations) to all other regions in different networks; see Extended Data Fig. 6 for a full correlation matrix. Dissolution of functional brain organization corresponds to decreased within-network integration and decreased between network segregation.
Extended Data Fig. 5. Multi-dimensional scaling, dimension edge weights.

a) Group parcellation (324 cortical and 61 subcortical parcels)31 b) Weights from the first 4 dimensions generated by multi-dimensional scaling of the full dataset. The color of each pixel in the plot represents the weight of a given edge. Dimension 1 captures the loss of network integration (on diagonal boxes) and segregation (off diagonal boxes) of psilocybin. Dimensions 2 and 3 primarily explain individual differences and do not show network patterns as clearly. Dimension 4 captures shared effects of psilocybin (PSIL) and methylphenidate (MTP) on sensorimotor systems (suspected arousal effects).
Subtraction of average FC (psilocybin minus baseline) revealed a pattern of FC change similar to dimension 1 (Fig. 2d and Extended Data Figs. 5 and 6). Consistent with previous psychedelics studies24, psilocybin increased FC between networks (particularly fronto-parietal, default mode and dorsal attention), whereas FC within networks was relatively less affected. A similar pattern of loss of segregation between brain networks is produced by nitrous oxide and ketamine57, suggesting that the psychedelic dimension observed here may generalize to psychedelic-like dissociative drugs.
Extended Data Fig. 6. Average functional connectivity (FC) matrices by condition.

a) Group parcellation (324 cortical and 61 subcortical parcels)31. b) Average FC matrices and condition differences. Top left shows the group average FC adjacency matrix. Bottom left shows the effect of psilocybin, e.g. increased correlation between dorsal attention, fronto-parietal, and default mode network to each other and to other cortical, limbic, and cerebellar systems. Top right shows effect of methylphenidate. For comparison and validation, we compared methylphenidate to the main effect of stimulant use within the last 24 hours (bottom right, n = 487 yes, n = 7992 no) in ABCD rs-fMRI data (bottom right).
By comparison, MTP decreased within-network FC in the sensory, motor and auditory regions (Extended Data Fig. 6), consistent with previous reports58 and similar to the effects of caffeine39. To verify that observations in our sample (n = 6) were generalizable, we compared stimulant effects in our study to those in the Adolescent Brain Cognitive Development (ABCD) Study59 (n = 487 taking stimulants). The effect of stimulant use in ABCD was consistent with MTP-associated FC changes in our dataset (Extended Data Fig. 6).
Desynchronization explains FC change
Multi-unit recording studies suggest that agonism of 5-HT2A receptors by psychedelics desynchronizes populations of neurons that typically co-activate60. We proposed that this phenomenon, observed at a larger spatial scale, might account for psilocybin-associated FC change (Fig. 1). We observed that the typically stable spatial structure of resting fMRI fluctuations was disrupted and desynchronized by psilocybin (Supplementary Videos 2–7: brain activity time courses during drug sessions for each participant). Therefore, we quantified brain signal synchrony using normalized global spatial complexity (NGSC): a measure of spatial entropy that is independent of the number of signals61. NGSC calculates cumulative variance explained by subsequent spatiotemporal patterns (Fig. 3a). The lowest value of NGSC (0) means that the time course for every vertex and/or voxel is identical. The highest value of NGSC (equal to one) means that the time course for every vertex and/or voxel is independent, indicating maximal desynchronization (or spatial entropy).
Fig. 3. Spatial desynchronization of cortical activity during psilocybin.

a, NGSC captures the complexity of brain activity patterns. It is derived from the number of spatial principal components needed to explain the underlying structure. Higher entropy equals desynchronized activity. On the right is variance explained by subsequent principal components for psilocybin in red, MTP in blue and no drug in grey for P6. b, Whole-brain entropy (NGSC) is shown for every fMRI scan for a single participant (P6). At right, increases during psilocybin were present in all participants. Sample sizes are provided in Supplementary Table 1. Grey bars indicate condition means. c, Parcel entropy (computed on individual-specific parcels) within functional brain areas shows similar psilocybin-driven increases as whole-brain entropy. d, Psilocybin-associated spatial entropy (individual-specific parcels, averaged across participants) is visualized on the cortical surface. Psilocybin-associated increases in entropy were largest in association cortex. e, LSD-associated increases in spatial entropy were similar to those induced by psilocybin (using data from ref. 56). f, Increases corresponded spatially to 5-HT2A receptor density33. In b–d, n = 6 participants, 272 observations (scans). For e, n = 16 participants.
Psilocybin significantly increased NGSC acutely with values returning to predrug baseline by the following session (Fig. 3b,c). The increase in NGSC was observed at the whole-brain level (Fig. 3b; LME model, estimate (95% confidence interval (CI)) = 0.0510 (0.0343, 0.0676), t(265) = 6.8, P = 2.0 × 10−6, uncorrected) and correlated with the subjective experience (MEQ30: Extended Data Fig. 7; r = 0.80, P = 3.52 × 10−4, uncorrected, after single outlier removal), whereas nuisance variables did not. Increased NGSC was also observed for individual-defined brain areas62 (Fig. 3c; LME model, estimate (95% CI) = 0.0149 (0.0071, 0.0228), t(265) = 3.74, P = 2.30 × 10−4, uncorrected), with the largest increases in association cortex and minimal changes in primary cortex (Fig. 3d). Global and local desynchronization replicated in an LSD dataset56 (Fig. 3e) and the distribution of these effects correlated with 5-HT2A receptor density (Fig. 3f; bivariate correlation NGSCpsilocybin to Cimbi-36 binding, r = 0.39, P = 1.9 × 10−13; NGSCLSD to Cimbi-36 binding, r = 0.32, P = 4.5 × 10−9, uncorrected)33,63.
Extended Data Fig. 7. Correlations with mystical experience scores.
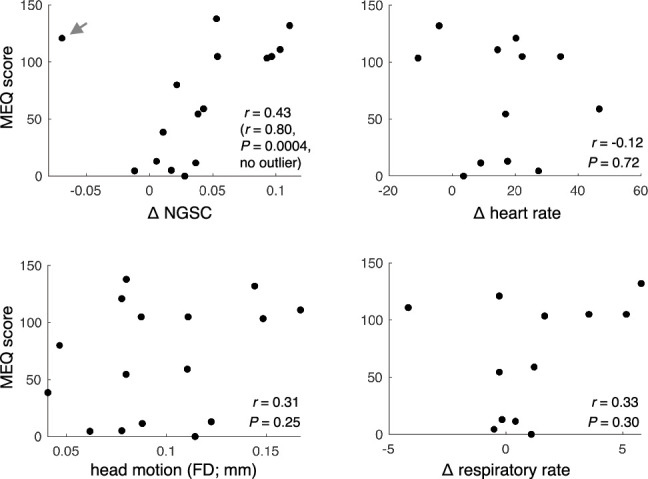
Comparison of MEQ30 score (y-axes) to global desynchronization (top left; NGSC change, drug minus baseline), head motion (bottom left; framewise displacement (FD) in mm), heart rate change (top right; drug minus baseline), and respiratory rate change (bottom right; drug minus baseline), for all drug sessions. Statistics (rho, P) are based on bivariate correlation, two-sided, uncorrected. In the case of Δ NGSC, statistics are reported before and after the removal of an outlier point (> 2 SD lower than mean, indicated by the gray arrow).
Task engagement reduces desynchronization
To investigate how psilocybin-driven brain changes are influenced by task states, participants were asked to complete a simple auditory–visual matching task in the scanner (Methods, perceptual fMRI task). Participants performed this task with more than 80% accuracy during drug sessions (Extended Data Fig. 8a–c). Engagement in the task significantly decreased the magnitude of psilocybin-associated network disruption and desynchronization (Fig. 4; LME model interaction of task × psilocybin: FC change P = 5.49 × 10−5, NGSC P = 4.82 × 10−8, uncorrected). These results were robust to scan order effects (Supplementary Fig. 6) and regression of evoked responses (Supplementary Fig. 7).
Extended Data Fig. 8. Auditory-visual matching fMRI task.

a) Schematic of auditory/visual matching task design. b) Comparison of performance (‘No Drug’ and psilocybin conditions are at ceiling). Lines indicate means and standard deviation across sessions. Number of task sessions are indicated in Supplementary Table 1. c) Comparison of reaction time (RT). Lines indicate mean and standard deviation across all trials (48 trials per session). d) Task fMRI activation maps (beta weights) and e) contrasts (simple subtraction) using the canonical hemodynamic response function (HRF). f) Eight a priori regions of interest for timecourse analyses. g) Average timecourses from the regions of interest shown in panel f, calculated using finite impulse response model over 13 TR x 1.761 s/TR = 22.89 seconds, for all trials. Shaded area around each line indicates SEM. ANOVAN of Condition x HRF Beta (Main effect of all trials) magnitude testing effect of drug, two-sided: Left V1, F(2,40) = 3.91, P = 0.030; Right V1, F(2,40) = 4.40, P = 0.020; Left M1 hand, F(2,40) = 0.40, P = 0.68; Left Auditory A1, F(2,40) = 0.22, P = 0.81; Right Auditory A1, F(2,40) = 0.77, P = 0.47; Left Language, F(2,40) = 0.025, P = 0.98; Left DMN, F(2,40) = 1.15, P = 0.33; Right DMN, F(2,40) = 0.14, P = 0.87. *P < 0.05. P-values are uncorrected for multiple comparisons.
Fig. 4. Effects of perceptual task performance on psilocybin-associated FC change and desynchronization.

a, Psilocybin-associated FC change from resting scans (left) and from task scans (right). b, Regional NGSC change (psilocybin minus baseline) from rest scans (left) and from task scans (right). Bar graphs on the bottom indicate the corresponding whole-brain FC change (a) and whole-brain NGSC values (b) during rest and task for baseline and drug conditions. LME models indicated an interaction of task × psilocybin on FC change (n = 7 with task data on psilocybin, estimate (95% CI) = −6.48 (−9.59, −3.37), t(265) = −6.48, P = 5.49 × 10−5, uncorrected) and an interaction of task × psilocybin on NGSC (n = 7 with task data on psilocybin, estimate (95% CI) = −0.042 (−0.056, −0.027), t(265) = −5.62, P = 4.82 × 10−8, uncorrected). Bars indicate mean and error bars indicate s.e.m.. **P < 0.001, uncorrected.
The reduction of psilocybin-driven brain changes during task performance seems to parallel the psychological principle of ‘grounding’: directing one’s attention externally as a means of alleviating intense or distressing thoughts or emotions. Grounding techniques are commonly used in psychedelic-associated psychotherapy to lessen overwhelming or distressing effects of psilocybin64. Task-related reductions in network desynchronization provide strong evidence for context-dependent effects of psilocybin on brain activity and FC65 and fill an important gap between preclinical studies of context dependence66,67 and clinical observations68.
Classical animal studies documented that psychedelics reduce optic tract responses to photic stimulation of the retina, indirectly reducing visual cortex activation69,70. We replicated these effects by documenting reduced task-evoked responses in primary visual cortex (Extended Data Fig. 8d–g). To assess whether psilocybin affects the magnitude of hemodynamic responses elsewhere, we analysed evoked responses during the perceptual task in other task-related regions of interest (Extended Data Fig. 8f,g). But the magnitudes of other evoked responses were not significantly changed by psilocybin (two-way analysis of variance of drug and participant; effect of drug: left V1 P = 0.03, right V1 P = 0.02, all other P > 0.1, uncorrected).
Persistent decrease in hippocampal FC
To assess whether persistent neurotrophic and psychological effects of psychedelics might be associated with persistent FC changes after psilocybin, we compared FC changes 1–21 days post-psilocybin to pre-psilocybin. Whole-brain FC change scores were small (normalized FC change (range) of 1.05 (0.94, 1.27)), indicating that the brain’s network structure had mostly returned to baseline (Extended Data Fig. 2).
Atypical cortico-hippocampal connectivity has been associated with affective symptoms30 and hippocampus neurogenesis is observed after psilocybin6. Further, acute decreases in hippocampal glutamate after psilocybin correlate with decreased DMN connectivity and ego dissolution21. Thus, we investigated whether the same region of the anterior hippocampus that showed strong acute FC change also showed persistent FC change. We observed significant FC change in the 3 week postdrug period (Fig. 5a,b; LME mean change 0.095, Ppre–post-psilocybin = 0.0033, uncorrected). No persistent FC differences were observed post-MTP (Methods, section ‘Persistent effects analysis’; LME ‘FC change’ 90% CI (−0.056, 0.080); equivalence δ = ±0.086, Ppre–post-MTP = 0.77).
Fig. 5. Persistent effects of psilocybin on hippocampal-cortical FC.
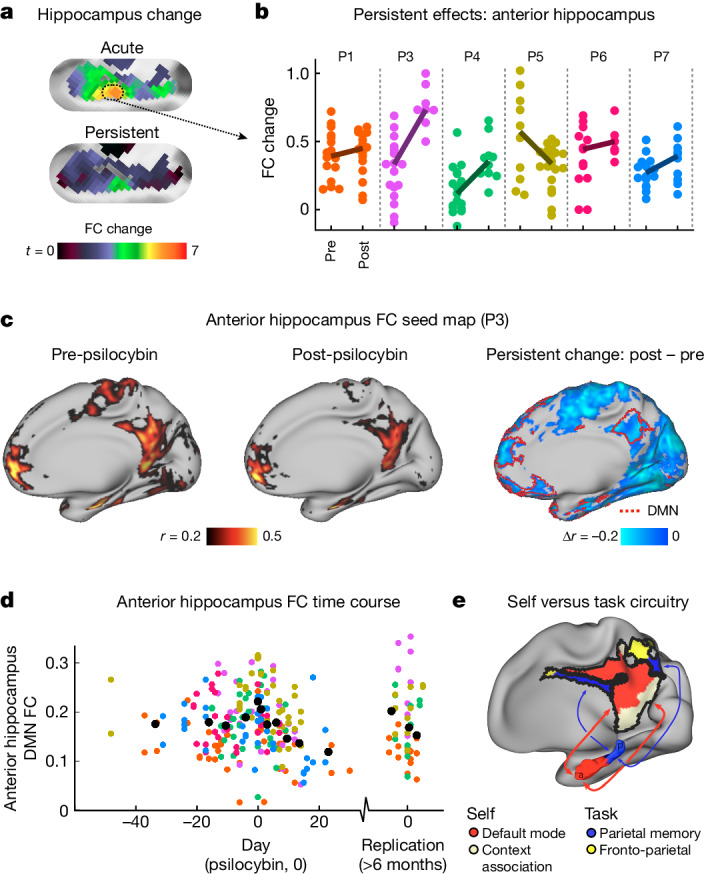
a, Hippocampus FC change maps (left hippocampus; unthresholded t-maps, as in Extended Data Fig. 2). Acute psilocybin FC change is shown on top and persistent FC change (3 weeks after psilocybin) on the bottom. b, Each dot represents the FC change score for the anterior hippocampus for a single scan before (left) and after (right) psilocybin for every participant (coloured as in Fig. 2). Participants showed a post-psilocybin increase in FC change in the anterior hippocampus (LME model, pre- versus post-psilocybin; n = 6 participants, 186 observations, estimate (95% CI) = 0.095 (0.032, 0.168), t(182) = 2.97, P = 0.0033, uncorrected). c, Connectivity from an anterior hippocampus seed (Montreal Neurological Institute coordinates −24, −22, −16 and 24, −18, −16) pre-psilocybin (left), post-psilocybin (middle) and persistent change (post- minus pre-) for an exemplar participant (P3). The red border on the right-most brain outlines the individual-specific DMN. A decrease in hippocampal FC with parietal and frontal components of the DMN is seen. d, Time course of anterior hippocampus minus DMN for all participants and scans (participant colours as in b). A moving average is shown in black. e, Schematic of hippocampal-cortical circuits, reproduced from ref. 29, CC BY 4.0.
FC between the anterior hippocampus and DMN was decreased postpsilocybin (Fig. 5c,d). Time-course visualization, after aligning them so that psilocybin dose was day 0, suggests that connectivity is reduced for 3 weeks following a single psilocybin dose (Fig. 5d; AntHip-DMN FC mean (95% CI): pre-psilocybin was 0.180 (0.169, 0.192); post-psilocybin was 0.163 (0.150, 0.176)). AntHip-DMN FC values returned to pre-psilocybin baseline by the replication visit 6–12 months later, however, the smaller replication sample (n = 4 with one pre-psilocybin visit each) was not statistically powered to detect small changes. This observation is compelling, as it localized to the anterior hippocampus, a brain region showing substantial synaptogenesis following psilocybin6. Reduced hippocampal-cortical FC may reflect increased plasticity of self-oriented hippocampal circuits31 (Fig. 5e).
From micro- to macro-scale psychedelic effects
The synchronized patterns of cofluctuations during the resting state are believed to reflect the brain’s perpetual task of modelling reality71. It follows that the stability of functional network organization across day, task, MTP and arousal levels (but not between individuals), reflects the subjective stability of waking consciousness. By contrast, the much larger changes induced by psilocybin fit with participants’ subjective reports of a radical change in consciousness. The large magnitude of effects of psilocybin, in comparison to the effects of MTP, suggests that observed changes are not merely due to increased arousal or non-specific effects of monoaminergic stimulation72.
Our observation that psychedelics desynchronize brain activity regionally and globally provides a bridge between previous findings at the micro- and macro-scales of neuroscience. Multi-unit recording studies suggest that agonism of 5-HT2A receptors by psychedelics does not uniformly increase or decrease firing of pyramidal neurons, but rather serves to desynchronize pairs or populations of neurons that co-activate under typical conditions60. Meanwhile, previous resting fMRI studies have reported a range of acute changes following ingestion of psilocybin55,63, ayahuasca73 and LSD56,74, which broadly converge on a loss of network connectivity and an increase in global integration24,75. Disruption of synchronized activity at several scales may explain the paradoxical observation that psychedelics produce an increase in metabolic activity19,20, a decrease in the power of local fluctuations22,76 and a loss of the brain’s segregated network structure23,56. This desynchronization of neural activity has been described as an increase in entropy or randomness of brain activity in the psychedelic state77,78. Our results support the hypothesis that these changes underpin the cognitive and perceptual changes associated with psychedelics.
Desynchrony may drive persistent change
The dramatic departure from typical synchronized patterns of co-activity may be key to understanding the acute effects of psilocybin and also its persistent neurotrophic effects. Changes in resting activity are linked to shifts in glutamate-dependent signalling during psilocybin exposure21,79,80. This phenomenon, shared by ketamine and psychedelics, engages homeostatic plasticity mechanisms81,82, a neurobiological response to large deviations in typical network activity patterns83–85. This response to novelty includes rapid upregulation in expression of BDNF, MTOR, EEF2 and other plasticity-related immediate early genes8,80, which are thought to have a key role in the antidepressant response86. Consistent with this notion, psilocybin produced the largest changes in the DMN, frequently associated with neuropsychiatric disorders34,35,87–91, and in a region of the anterior and middle hippocampus associated with the self29,92 and the present moment93.
Psychedelics rapidly induce synaptogenesis in the hippocampus and cortex, effects that seem to be necessary for rapid antidepressant-like effects in animal models7,17. However, understanding the underpinnings of the behavioural effects of psychedelics requires human studies. Advances in precision functional mapping37,94,95 and individual-level characterization enabled us to identify desynchronization of resting-state fMRI signals, connect these changes with subjective psychedelic effects and localize these changes to depression-relevant circuits (DMN, hippocampus). These analyses rely on precise characterization of an individuals’ baseline brain organization (for example, individual definition of brain areas, networks and day-to-day variability) to understand how that organization is altered by an intervention. This precision drug mechanism study was conducted in non-depressed volunteers. Verification of the proposed antidepressant mechanism of psilocybin will require precision patient studies. New methods to measure neurotrophic markers in the human brain96 will provide a critical link between mechanistic observations at the cellular, brain networks and psychological levels.
Methods
Regulatory approvals and registrations
Written informed consent was obtained from all participants in accordance with the Declaration of Helsinki and procedures established by the Washington University in Saint Louis Institutional Review Board. All participants were compensated for their time. All aspects of this study were approved by the Washington University School of Medicine (WUSOM) Internal Review Board, the Washington University Human Research Protection Office (WU HRPO), the Federal Drug Administration (IND no. 202002165) and the Missouri Drug Enforcement Agency (DEA) under a federal DEA schedule 1 research licence and registered with ClinicalTrials.gov identifier NCT04501653. Psilocybin was supplied by Usona Institute through Almac Clinical Services.
Study design
Healthy young adults (n = 7, 18–45 years) were enrolled between April 2021 and March 2023 in a randomized cross-over precision functional brain mapping study at Washington University in Saint Louis (see Supplementary Methods for inclusion and exclusion criteria). The purpose of the study was to evaluate differences in individual-level connectomics before, during and after psilocybin exposure. Participants underwent imaging during drug sessions (with MRI starting 1 h after drug ingestion) with 25 mg psilocybin or 40 mg MTP, as well as non-drug imaging sessions. Drug condition categories were (1) baseline, (2) drug 1 (MTP or psilocybin), (3) between, (4) drug 2 and (5) after. Randomization allocation was conducted using REDCap and generated by team members who prepared study materials including drug or placebo but otherwise had no contact with participants. A minimum of three non-drug imaging sessions were completed during each non-drug window: baseline, between and after drug sessions. The number of non-drug MRI sessions was dependent on availability of the participant, scanner and scanner support staff. Dosing day imaging sessions were conducted 60–180 min following drug administration during peak blood concentration98. One participant (P2) was not able tolerate fMRI while on psilocybin, and had trouble staying awake on numerous fMRI visits after psilocybin and was thus excluded from analysis (except for data quality metrics in Extended Data Fig. 1).
MTP was selected as the active control condition to simulate the cardiovascular effects and physiological arousal (that is, controlling for dopaminergic effects) associated with psilocybin99. Usona Institute, a US non-profit medical research organization, provided good manufacturing practices for psilocybin.
Drug sessions were facilitated by two clinical research staff who completed an approved in-person or online facilitator training programme provided by Usona Institute, as part of the phase 2 study (ClinicalTrials.gov identifier NCT03866174). The role of the study facilitators was to build a therapeutic alliance with the participant throughout the study, prepare them for their drug dosing days and to observe and maintain participant safety during dosing day visits64. The pair consisted of an experienced clinician (lead clinical facilitator) and a trainee (cofacilitator).
The predefined primary outcome measure was precision functional mapping (numerous visits, very long scans to produce individual connectomes) examining the effects of psilocybin on cortical and cortico- subcortical brain networks that could explain its rapid and sustained behavioural effects. Predefined secondary outcome measures included (1) assessment of hemodynamic response to evaluate how 5-HT2A receptor agonism by psychedelics may alter neurovascular coupling, (2) assessment of acute psychological effects of psilocybin using the MEQ30 score (Supplementary Methods) and (3) assessment of personality change using the International Personality Item Pool-Five-Factor Model100. Changes in pulse rate and respiratory rate during psilocybin and placebo were later added as secondary outcome measures and personality change was abandoned because it was clear that we would not be powered to detect personality change.
Replication protocol
Participants were invited to return 6–12 months after completing the initial cross-over study for a replication protocol. This included 1–2 baseline fMRIs, a psilocybin session (identical to the initial session, except for lack of blinding) and 1–2 ‘after’ sessions within 4 days of the dose.
Participants
Healthy adults aged 18–45 years were recruited by campus-wide advertisement and colleague referral. Participants (n = 7) were enrolled from March 2021 to May 2023. Participants were required to have had at least one previous lifetime psychedelic exposure (for example, psilocybin, mescaline, ayahuasca, LSD), but no psychedelics exposure within the past 6 months. Individuals with psychiatric illness (depression, psychosis or addiction) based on the DSM-5 were excluded. Demographics and data summary details are provided in Supplementary Table 1. One of the authors (N.U.F.D.) was a study participant.
MRI
Participants were scanned roughly every other day over the course of the experiment (Extended Data Fig. 1). Imaging was performed at a consistent time of day to minimize diurnal effects in FC101. Neuroimaging was performed on a Siemens Prisma scanner (Siemens) in the neuroimaging laboratories at the Washington University Medical Center.
Structural scans (T1w and T2w) were acquired for each participant at 0.9 mm isotropic resolution, with real-time motion correction. Structural scans from different sessions were averaged together for the purposes of Freesurfer segmentation and nonlinear atlas registrations.
To capture high-resolution images of blood oxygenation level-dependent (BOLD) signal, we used an echo-planar imaging sequence102 with 2 mm isotropic voxels, multiband 6, multi-echo 5 (times to echo: 14.20, 38.93, 63.66, 88.39, 113.12 ms)103, repetition or relaxation time: 1,761 ms, flip angle of 68° and in-plane acceleration104 (IPAT or grappa) of 2. This sequence acquired 72 axial slices (144 mm coverage). Each resting scan included 510 frames (lasting 15 min, 49 s) as well as three frames at the end used to provide estimate electronic noise.
Every session included two 15-min resting-state fMRI (rs-fMRI) scans, during which participants were instructed to hold still and look at a white fixation crosshair presented on a black background. Head motion was tracked in real time using Framewise Integrated Real-time MRI Monitoring software (FIRMM)105. An eye-tracking camera (EyeLink) was used to monitor participants for drowsiness.
Perceptual (matching) fMRI task
Participants also completed a previously validated event-related fMRI task. This was a suprathreshold auditory–visual matching task in which participants were presented with a naturalistic visual image (duration 500 ms) and coincident spoken English phrase, and were asked to respond with a button press to indicate whether the image and phrase were ‘congruent’ (for example, an image of a beach and the spoken word ‘beach’) or ‘incongruent’. Both accuracy and response time of button presses were recorded. Each trial was followed by a jittered inter-stimulus interval optimized for event-related designs. In a subset of imaging sessions, two task fMRI scans were completed following the two resting scans. Task fMRI scans used the same sequence used in resting fMRI, included 48 trials (24 congruent, 24 incongruent) and lasted a total of 410 s. In analyses, high motion frames were censored106 and the two task scans were concatenated to better match the length of the rs-fMRI scans. Note the stimulus order in the two trials did not vary across session. The order of rest and task scans was not counterbalanced across sessions to avoid concern that task scans may influence subsequent rest scans.
Resting fMRI processing and resting-state network definition
Resting fMRI data were preprocessed using an in-house processing pipeline. In brief, this included removal of thermal noise using NORDIC denoising107–109, correction for slice timing and field distortions, alignment, optimal combination of many echoes by weighted summation110, normalization, nonlinear registration, bandpass filtering and scrubbing at a movement threshold of 0.3 mm to remove reduce the influence of confounds111. Tissue-based regressors were computed in volume (white matter, ventricles, extra-axial cerebrospinal fluid)112 and applied following projection to surface. Task-based regressors were only applied when indicated. Details on rs-fMRI preprocessing are provided in Supplementary Methods. Visualizations of motion, physiological traces and signal across the brain (‘grayplots’) before and after processing113 are provided in Supplementary Video 1.
Surface generation and brain areal parcellation
Surface generation and processing of functional data followed similar procedures to Glasser et al.114. To compare FC and resting-state networks across participants, we used a group-based surface parcellation and community assignments generated previously62.
For subcortical regions, we used a set of regions of interest115 generated to achieve full coverage and optimal region homogeneity. A subcortical limbic network was defined on the basis of neuroanatomy: amygdala, anteromedial thalamus, nucleus accumbens, anterior hippocampus and posterior hippocampus116,117. These regions were expanded to cover anatomical structures (for example, anterior hippocampus)31.
To generate region-wise connectivity matrices, time courses of all surface vertices or subcortical voxels within a region were averaged. FC was then computed between each region timeseries using a bivariate correlation and then Fisher z-transformed for group comparison.
Individualized network and brain area mapping
We identified canonical large-scale networks using the individual-specific network matching approach described previously43,44,62. In brief, cortical surface and subcortical volume assignments were derived using the graph-theory-based Infomap algorithm118. In this approach, we calculated the correlation matrix from all cortical vertices and subcortical voxels, concatenated across all a participant’s scans. Correlations between vertices within 30 mm of each other were set to zero. The Infomap algorithm was applied to each participant’s correlation matrix thresholded at a range of edge densities spanning from 0.01 to 2%. At each threshold, the algorithm returned community identities for each vertex and voxel. Communities were labelled by matching them at each threshold to a set of independent group average networks described previously62. In each individual and in the average, a ‘consensus’ network assignment was derived by collapsing assignments across thresholds, giving each node the assignment it had at the sparsest possible threshold at which it was successfully assigned to one of the known group networks. See Extended Data Fig. 4 and Supplementary Fig. 1 for individual and group mode assignments, respectively. The following networks were included: the association networks including the DMN, fronto-parietal, dorsal attention, parietal memory, ventral attention, action-mode, salience and context networks; and the primary networks including the visual, somato-motor, somato-motor face and auditory networks.
To compute local (areal) desynchronization, we also defined brain areas at the individual level using a previously described areal parcellation approach39. In brief, for each participant, vertex-wise FC was averaged across all sessions to generate a dense connectome. Then, abrupt transitions in FC values across neighbouring vertices were used to identify boundaries between distinct functional areas.
LME model
To take advantage of the multilevel precision functional mapping study design, a LME model was used. Every scan was labelled on the following dimensions: participant identity (ID), MRI visit, task (task or rest), drug condition (prepsilocybin, psilocybin, MTP, postpsilocybin) and head motion (average framewise displacement). The rs-fMRI metrics (described below) were set as the dependent variable, drug (drug condition), task, framewise displacement (motion) and drug × task were defined as fixed effects, and participant ID and MRI session were random effects.
Let yij be the rs-fMRI metric (for example, FC change score at a given vertex) for the jth observation (15 min fMRI scan) within the ith participant. The LME model can be written as:
| 1 |
β0 is the intercept term.
βdrug, βFD, βtask and βtask-by-drug are the coefficients for the fixed effects predictors.
drugij, frame displacementij (FDij) and taskij are the values of the fixed effects predictors for the jth observation within the ith group.
u0i represents the random intercept for the ith participant, accounting for individual-specific variability.
v0j represents the random intercept for the jth observation within the ith participant, capturing scan-specific variability.
εij is the error term representing unobserved random variation.
In MATLAB (Wilkinsonian notation), this model is expressed for every vertex Y(vertex) = fitlme(groupd, FC_Change(vertex) ~ drug + framewise displacement + task + task-by-drug + (1 |SubID) + (1 |session)).
To compensate for the implementations of this LME model on many rs-fMRI-related dependent variables, differences were highlighted when P < 0.001. All P values reported are not corrected for multiple comparisons.
Vertex-wise FC change
FC change (‘distance’) was calculated at the vertex level to generate FC change maps and a LME model (equation (1)) was used in combination with wild bootstrapping119,120 and threshold-free cluster enhancement (TFCE)95,121 to estimate P values for t-statistic maps resulting from the model (Figs. 1a–d and 4). Wild bootstrapping is an approach to permutation testing that was designed for models that are not independent and identically distributed, and are heteroscedastic.
First, a FC change map was generated for every scan by computing, for each vertex, the average distance between its FC seedmap and the FC seedmap for each of that participant’s baseline scans. As each participant had several baseline visits, FC change was computed for baseline scans by computing distance from all other baseline scans (excluding scans within the same visit). This provided a measure of day-to-day variability. Second, the distance value was used as the dependent variable yij in the LME model to generate a t-statistic. Third, a wild bootstrapping procedure was implemented as follows. Several bootstrap samples (B = 1,000) were generated using the Rademacher procedure120, in which the residuals were randomly inverted. Specifically, a Rademacher vector was generated by randomly assigning −1 or 1 values with equal probability to the residual of each observation. By element-wise multiplication of the original residuals with the Rademacher vector, bootstrap samples were created to capture the variability in the data.
For the observed t-statistic-map and each bootstrap sample, the TFCE algorithm was applied to enhance the sensitivity to clusters of significant voxels or regions while controlling for multiple comparisons. The value of the enhanced cluster statistic derived from the bootstrap samples was used to create a null distribution under the null hypothesis. By comparing the original observed cluster statistic with the null distribution, P values were derived to quantify the statistical significance of the observed effect. The P values were obtained on the basis of the proportion of bootstrap samples that produced a maximum cluster statistic exceeding the observed cluster statistic.
The combined approach of wild bootstrapping with the Rademacher procedure and TFCE provided the method to estimate P values for our multilevel (drug condition, participant, session, task) design. This methodology accounted for the complex correlation structure, effectively controlled for multiple comparisons and accommodated potential autocorrelation in the residuals through the Rademacher procedure. By incorporating these techniques, association with psilocybin and other conditions was reliably identified amid noise and spatial dependencies.
Whole-brain FC change
For analyses in Figs. 1e,g, 2 and 4a (bottom), Extended Data Fig. 3 and Supplementary Figs. 3, 4 and 6, distance calculations were computed on the FC matrix using z-transformed bivariate correlation of time courses from parcellated brain areas62. The effects of day-to-day, drug condition, task and framewise displacement and drug × task were directly examined by calculating the distance between functional network matrices generated from each scan. Root-mean-squared Euclidean distance was computed between the linearized upper triangles of the parcellated FC matrix between each pair of 15 min fMRI scans, creating a second-order distance matrix (Extended Data Fig. 3). Subsequently, the average distance (reported as ‘whole-brain FC change’) was examined for FC matrices that were from the same individual within a single session, from the same individual across days (‘day-to-day’), from the same participant between drug and baseline (for example, psilocybin), from the same individual but different tasks (‘task:rest’), from the same individual between highest motion scans and baseline (‘hi:lo motion’), from different individuals (‘between person’). In the ‘high head motion’ comparison (‘hi:lo motion’ in Supplementary Fig. 3), the two non-drug scans with the highest average framewise displacement were labelled and compared against all other baseline scans.
A LME model (equation (1)) and post hoc t-tests were used to assess statistical differences between drug conditions. A related approach using z-transformed bivariate correlation (‘similarity’ rather than distance) was also taken and results were unchanged (Supplementary Fig. 3c).
Likelihood ratio test of participant-specific response
To test whether variability in participant-specific response to psilocybin was larger than would be expected by chance, we used a likelihood ratio test for variance of random slopes for a participant-specific response to psilocybin48. The difference in log likelihood ratios was compared to a null distribution of 1 million draws from a mixture of chi-squared distributions with degrees of freedom 1 and 2. We note that the likelihood ratio test of variance components is a non-standard problem47 as the covariance matrix of the random effects is positive definite and the variances of random effects are non-negative. Finally, the test statistic for the likelihood ratio in this LME model was compared against a 50/50 mixture of two independent chi-squared distributions, each with one and two degrees of freedom, respectively.
Assessing subjective experience
Subjective experience was assessed for drug sessions using the MEQ3046 (Supplementary Methods). The MEQ30 is designed to capture the core domains of the subjective effects of psychedelics (as compared to the altered states of consciousness rating scales that more broadly assess effects of psychoactive drugs122) and is related to the therapeutic benefits of psychedelics. We applied a LME model across all drug sessions, similar to the one described above, but with MEQ30 total score as the dependent variable. Whole-brain FC change and framewise displacement were modelled as fixed effects, and participant was modelled as a random effect. The same model was solved using FC change from every vertex to generate a vertex-wise map of the FC change versus MEQ30.
Normalized FC change
The conditions above were compared by calculating normalized FC change scores using the following procedure: we (1) determined FC change for each condition compared to baseline as described above, (2) subtracted within-session distance for all conditions (such that within-session FC change was 0), (3) divided all conditions by day-to-day distance (such that day-to-day FC change was equal to 1). Thus, normalized whole-brain FC change values (for example, psilocybin versus base was 3.52) could be thought of as proportional to day-to-day variability.
Data-driven MDS
We used a classical MDS approach to cluster parcellated connectomes across fMRI scans, as previously described38. This data-driven approach was used to identify how different parameters (for example, task, drug, individual) affect similarity and/or distance between networks. MDS places data in multidimensional space on the basis of the dissimilarity (Euclidean distance) among data points, which in this case means a data point represents the linearized upper triangle of a FC matrix. Every matrix was entered into the classical MDS algorithm (implemented using MATLAB 2019, cmdscale.m). Many dimensions of the data were explored. The eigenvectors were multiplied by the original FC matrices to generate a matrix of eigenweights that corresponded to each dimension. These eigenweights were also applied to other rs-fMRI psychedelics datasets to generate dimensions scores (section ‘Other datasets’).
Rotation-based null model (spin test) for network specificity
To assess network specificity of FC change values, we calculated average FC change of matched null networks consisting of randomly rotated networks with preserved size, shape and relative position to each other62,97. To create matched random networks, we rotated each hemisphere of the original networks a random amount around the x, y and z axes on the spherical expansion of the cortical surface62. This procedure randomly relocated each network while maintaining networks’ sizes, shapes and relative positions to each other. Random rotation followed by computation of network-average FC change score was repeated 1,000 times to generate null distributions of FC change scores. Vertices rotated into the medial wall were not included in the calculation. Actual psilocybin FC change was then compared to null rotation permutations to generate a P value for the 12 networks that were consistently present across every participant’s Infomap parcellation. For bar graph visualization (Fig. 1 and Supplementary Fig. 1b), networks with greater change (P < 0.05 based on null rotation permutations) are shown in their respective colour and other networks are shown in grey.
NGSC
We used an approach previously validated to assess spatial complexity (termed entropy) or neural signals61. Temporal principal component analysis was conducted on the full BOLD dense timeseries, which yielded m principal components (m roughly 80 K surface vertices and subcortical voxels) and associated eigenvalues. The normalized eigenvalue of the ith principal component was calculated as
| 2 |
where m is the number of principal components, and λi and λ′i represent the eigenvalue and the normalized eigenvalue of the ith principal component, respectively. Last, the NGSC, defined as the normalized entropy of normalized eigenvalues, was computed using the equation:
| 3 |
The NGSC computed above attains values from the interval 0 to 1. The lowest value NGSC = 0 would mean the brain-wide BOLD signal consisted of exactly one principal component or spatial mode, and there is maximum global FC between all vertices. The highest value NGSC = 1 would mean the total data variance is uniformly distributed across all m principal components, and a maximum spatial complexity or a lowest FC is found.
NGSC was additionally calculated at the ‘parcel level’. To respect areal boundaries, this was done by first generating a set of individual-specific parcels in every participant (on all available resting fMRI sessions concatenated) using procedures described oreviously39,62.
NGSC maps were compared to PET-based 5-HT2A receptor binding maps published in ref. 33. Similarity was assessed by computing the bivariate correlation between NGSC values and 5-HT2A binding across 324 cortical parcels from the Gordon–Laumann parcellation.
Persistent effects analysis
To assess the persistent effects of psilocybin, we compared FC changes 1–21 days postpsilocybin to predrug baseline. The FC change analysis (described above) indicated that connectivity at the whole-brain level did not change following psilocybin (Supplementary Fig. 1). A screen was conducted with P < 0.05 threshold to identify brain networks or areas showing persistent effects. This analysis identified the anterior hippocampus as a candidate region of interest for persistent FC change (section ‘Baseline/after psilocybin FC change analysis’ in Supplementary Methods).
We assessed change in anterior hippocampus ‘FC change’ pre- versus postpsilocybin using the LME model described previously. In this model, all sessions before psilocybin (irrespective or cross-over order) were labelled as prepsilocybin and all sessions within 21 days after psilocybin were labelled as postpsilocybin.
As a control, we tested anterior hippocampus FC change pre- versus post-MTP using both the LME model, and an equivalence test. To control for potential persistent psilocybin effects, only the block of scans immediately before and after MTP were used (for example, if a participant took MTP as drug 1, then all baseline scans were labelled as ‘pre-MTP’ and all scans between drugs 1 and 2 were labelled ‘post-MTP’).
Equivalence testing (to conclude no change in anterior hippocampus after MTP) was accomplished by setting δ = 0.5 standard deviation of FC change across pre-MTP sessions. We computed the 90% CI of change in FC change between pre- and post-MTP sessions. If the bounds of the 90% CI were within ±δ, then equivalence was determined123.
Other datasets
Raw fMRI and structural data published previously55,56 were run through our in-house registration and processing pipeline described above. These datasets were used for replication, external validation and generalization to another classic psychedelic (that is, LSD) for the measures described above (for example, NGSC and the MDS-derived psilocybin FC dimension, dimension 1).
Using the data from ref. 55: n = 15 healthy adults (five women, mean age 34.1 years, s.d. 8.2) completed two scanning sessions (psilocybin and saline) that included an eyes-closed resting-state BOLD scan for 6 min before and following i.v. infusion of drug. fMRI data were acquired using a gradient-echo-planar imaging sequence, TR and TE of 3,000 and 35 ms, field-of-view 192 mm, 64 × 64 acquisition matrix, parallel acceleration factor of 2 and 90° flip angle.
Using the data from ref. 56: healthy adults completed two scanning sessions (LSD and saline), which included an eyes-closed resting-state BOLD scan acquired for 22 min following i.v. drug infusion lasting 12 min. n = 20 participants completed the protocol, but data were used for n = 15 (four women; mean age 30.5, standard deviation 8.0) deemed suitable for BOLD analyses. fMRI data were acquired using a gradient-echo-planar imaging sequence, TR and TE of 2,000 and 35 ms, field-of-view 220 mm, 64 × 64 acquisition matrix, parallel acceleration factor of 2, 90° flip angle and 3.4 mm isotropic voxels.
The ABCD database resting-state functional MRI59 (annual release v.2.0, 10.15154/1503209) was used to replicate the effects of stimulant use on FC. Preprocessing included framewise censoring with a criterion of frame displacement less than or equal to 0.2 mm in addition the standard predefined preprocessing procedures124. Participants with fewer than 600 frames (equivalent to 8 min of data after censoring) were excluded from the analysis. Parcel-wise group-averaged FC matrices were constructed for each participant as described above for 385 regions on inter-test in the brain.
Use of a stimulant (for example, MTP, amphetamine salts, lisdexamfetamine) in the last 24 h was assessed by parental report. Participants with missing data were excluded. Regression analysis was used to assess the relationship between FC (edges) and stimulant use in the last 24 h. Framewise displacement (averaged over frames remaining after censoring) was used as a covariate to account for motion-related effects. The t-values that reflect the relationship between stimulant use and FC were visualized on a colour scale from −5 to +5 to provide a qualitative information about effect of stimulant use on FC.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Online content
Any methods, additional references, Nature Portfolio reporting summaries, source data, extended data, supplementary information, acknowledgements, peer review information; details of author contributions and competing interests; and statements of data and code availability are available at 10.1038/s41586-024-07624-5.
Supplementary information
This file contains Supplementary Table 1, Figs. 1–7 and Methods.
Quality control plots for every fMRI scan. For each participant (P1, P3–P7, concatenated) the quality control plots are concatenated in the order that the scans were acquired (Extended Data Fig. 1). The top plot shows head position (frame-by-frame, relative to frame 1) separated into x, y, z translation and x, y, z rotation (six parameters). The second plot from the top shows DVARS, which index the rate of change of fMRI signal across the entire brain at each frame of data. The D refers to the temporal derivative of time courses, and VARS refers to the root-mean-square variance over voxels. The third plot shows head motion measured as FD (framewise displacement) in mm. Underneath in the fourth row, the time course for the whole-brain grayordinates (cortex on top, subcortex on the bottom) are shown before preprocessing (known as ‘grayplot’ or ‘carpet plot’). The fifth row shows the same grayordinates, but after preprocessing (bandpass filtering, removal of nuisance signals by regression, and smoothing at 4 mm full-width at half-maximum). The vertical black lines or bars in the grayplots indicate these data frames that were censored due to excessive head motion. At the end, quality control plots are compared to physiology (heart rate, respiratory rate) plots for every session in which physiological monitoring data were acquired.
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Acknowledgements
This work was supported by the Taylor Family Institute Fund for Innovative Psychiatric Research (J. S. Siegel, T.O.L., G.E.N.); the McDonnell Center for Systems Neuroscience (J. S. Siegel, G.E.N.); the Institute of Clinical and Translational Science (G.E.N.); National Institutes of Health (NIH) grants MH112473 (J. S. Siegel, S.S., D.A.B., C.H., G.E.N.), T32 DA007261 (J. S. Siegel), NS123345 (B.P.K.), MH129616 (T.O.L.), MH121276 (N.U.F.D., E.M.G., D.A.F.), MH118370 (C.G.), NS124738 (C.G.), MH096773 (D.A.F., N.U.F.D.), MH122066 (D.A.F., E.M.G., N.U.F.D.), MH124567 (D.A.F., E.M.G., N.U.F.D.), NS129521 (E.M.G., D.A.F., N.U.F.D.) and NS088590 (N.U.F.D.); the National Spasmodic Dysphonia Association (E.M.G.); the Ralph Metzner Professorship and the Tianqiao and Chrissy Chen Institute (R.C.-H.); the Intellectual and Developmental Disabilities Research Center (N.U.F.D.); by the Kiwanis Foundation (N.U.F.D.); the Washington University Hope Center for Neurological Disorders (E.M.G., N.U.F.D.) and by Mallinckrodt Institute of Radiology pilot funding (E.M.G., N.U.F.D.). Furthermore, this study used data from the ABCD study, supported by National Institutes of Health grant no. U01DA041120. We give a special thanks to our study participants, who completed a demanding protocol with grace for the benefit of scientific inquiry. Data used in the preparation of this article were obtained from the Adolescent Brain Cognitive Development (ABCD) Study (https://abcdstudy.org), held in the NIMH Data Archive (NDA). This is a multisite, longitudinal study designed to recruit more than 10,000 children age 9-10 and follow them over 10 years into early adulthood. The ABCD Study is supported by the National Institutes of Health and additional federal partners under award numbers U01DA041048, U01DA050989, U01DA051016, U01DA041022, U01DA051018, U01DA051037, U01DA050987, U01DA041174, U01DA041106, U01DA041117, U01DA041028, U01DA041134, U01DA050988, U01DA051039, U01DA041156, U01DA041025, U01DA041120, U01DA051038, U01DA041148, U01DA041093, U01DA041089, U24DA041123, U24DA041147. A full list of supporters is available at https://abcdstudy.org/federal-partners.html. A listing of participating sites and a complete listing of the study investigators can be found at https://abcdstudy.org/consortium_members/. ABCD consortium investigators designed and implemented the study and/or provided data but did not necessarily participate in the analysis or writing of this report. This manuscript reflects the views of the authors and may not reflect the opinions or views of the NIH or ABCD consortium investigators.
Extended data figures and tables
Author contributions
The concept came from J. S. Siegel and G.E.N. The study was designed by J. S. Siegel, S.S., T.O.L., C.L.R., E.J.L., A.Z.S. and G.E.N. Data acquisition and processing were done by J. S. Siegel, S.S., T.R.R., D.P., C.H., J. S. Shimony, J.A.S., D.A.B., K.M.S., F.I.W., J.M., E.Y., S.M.N., L.V., D.A.F. and A.Z.S.. Data analysis and interpretation were carried out by J. S. Siegel, B.P.K., E.M.G., T.O.L., N.V.M., C.G., R.V.C., S.R.K., D.F.W., J.A.P.-C., R.T.S., Y.C., R.C.-H., M.E.R., G.E.N. and N.U.F.D. The paper was written and revised by J. S. Siegel, S.S., M.E.R., A.Z.S., G.E.N. and N.U.F.D. Participant 7 was author N.U.F.D.
Peer review
Peer review information
Nature thanks Charles Lynch, Petros Petridis and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Peer reviewer reports are available.
Data availability
All data from individual participants P1–P7 are available at https://wustl.box.com/v/PsilocybinPFM, with a password available on completion of a data use agreement. The ABCD data used in this report came from ABCD the Annual Release 2.0, 10.15154/1503209. The ABCD data repository grows and changes over time (https://nda.nih.gov/abcd). The Imperial College London psilocybin and LSD datasets are available upon request.
Code availability
Data processing code for the psilocybin precision functional mapping data can be found at https://wustl.box.com/s/dmj5s3h9pxt9bcw9mm3ai9c15y756o79. Code specific to analyses can be found at https://gitlab.com/siegelandthebrain1/Psilocybin_PFM/. Data processing code for the ABCD data can be found at https://github.com/DCAN-Labs/abcd-hcp-pipeline. Matching task stimuli are available at https://gitlab.com/siegelandthebrain1/Psilocybin_PFM/-/blob/main/image_task_clean.zip. Software packages incorporated into the above pipelines for data analysis included: MATLAB R2019b, https://www.mathworks.com/ (including Psychtoolbox v.2.0 and Statistics and Machine Learning Toolbox v.11.6); Connectome Workbench v.1.5; http://www.humanconnectome.org/software/connectome-workbench.html; Freesurfer v.6.2, https://surfer.nmr.mgh.harvard.edu/; FSL v.6.0, https://fsl.fmrib.ox.ac.uk/fsl/fslwiki; 4dfp tools, https://4dfp.readthedocs.io/en/latest/; Infomap, https://www.mapequation.org; Cifti MATLAB utilities (including spin test): https://github.com/MidnightScanClub/SCAN and 4dfp tools, https://4dfp.readthedocs.io/en/latest/. MRI pulse sequences used to acquire the data are provided at https://gitlab.com/siegelandthebrain1/Psilocybin_PFM/-/blob/main/NP1161_MRI_sequence.pdf.
Competing interests
Within the past year, J. S. Siegel has been an employee of Sumitomo Pharma America and received consulting fees from Longitude Capital. J. S. Siegel, N.U.F.D., T.O.L. and E.M.G. have submitted a provisional patent (patent no. 020949/US 15060-1787) for the use of precision functional mapping for measuring target engagement by experimental therapeutics. R.T.S. has received consulting compensation from Octave Bioscience and compensation for reviewership duties from the American Medical Association. C.L.R. serves as a consultant to Usona Institute and Novartis and receives research support from the Tiny Blue Dot Foundation. G.E.N. has received research support from Usona Institute (drug only). She has served as a paid consultant for Carelon, Alkermes, Inc., Sunovion Pharmaceuticals, Inc. and Novartis Pharmaceuticals Corp. T.O.L. holds a patent for taskless mapping of brain activity licenced to Sora Neurosciences and a patent for optimizing targets for neuromodulation, implant localization and ablation is pending. J. S. Siegel is a consultant and received stock options in Sora Neuroscience, and company that focuses on resting-state analysis. D.A.F. and N.U.F.D. are cofounders of Turing Medical Inc, have financial interest, may benefit financially if the company is successful in marketing FIRMM motion monitoring software products, may receive royalty income based on FIRMM technology developed at WUSOM and licenced to Turing Medical Inc. S.M.N., E.M.G. and T.O.L. have received consulting fees from Turing Medical Inc. D.F.W. is a consultant for Engrail Therapeutics and receives contract funds for WUSOM research studies from Eisai, Anavex and Roche. These potential conflicts of interest have been reviewed and are managed by WUSOM. The other authors declare no competing interests. All authors report no financial interest in psychedelics companies.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
These authors contributed equally: Ginger E. Nicol, Nico U. F. Dosenbach
Extended data
is available for this paper at 10.1038/s41586-024-07624-5.
Supplementary information
The online version contains supplementary material available at 10.1038/s41586-024-07624-5.
References
- 1.Goodwin, G. M. et al. Single-dose psilocybin for a treatment-resistant episode of major depression. N. Engl. J. Med.387, 1637–1648 (2022). 10.1056/NEJMoa2206443 [DOI] [PubMed] [Google Scholar]
- 2.Raison, C. L. et al. Single-dose psilocybin treatment for major depressive disorder: a randomized clinical trial. JAMA330, 843–853 (2023). [DOI] [PMC free article] [PubMed]
- 3.Carhart-Harris, R. et al. Trial of psilocybin versus escitalopram for depression. N. Engl. J. Med.384, 1402–1411 (2021). 10.1056/NEJMoa2032994 [DOI] [PubMed] [Google Scholar]
- 4.Bogenschutz, M. P. et al. Percentage of heavy drinking days following psilocybin-assisted psychotherapy vs placebo in the treatment of adult patients with alcohol use disorder: a randomized clinical trial. JAMA Psychiatry79, 953–962 (2022). [DOI] [PMC free article] [PubMed]
- 5.Cameron, L. P. et al. A non-hallucinogenic psychedelic analogue with therapeutic potential. Nature589, 474–479 (2020). [DOI] [PMC free article] [PubMed]
- 6.Raval, N. R. et al. A single dose of psilocybin increases synaptic density and decreases 5-HT2A receptor density in the pig brain. Int. J. Mol. Sci.22, 835 (2021). 10.3390/ijms22020835 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shao, L.-X. et al. Psilocybin induces rapid and persistent growth of dendritic spines in frontal cortex in vivo. Neuron109, 2535–2544.e4 (2021). [DOI] [PMC free article] [PubMed]
- 8.Vaidya, V. A., Marek, G. J., Aghajanian, G. K. & Duman, R. S. 5-HT2A receptor-mediated regulation of brain-derived neurotrophic factor mRNA in the hippocampus and the neocortex. J. Neurosci.17, 2785–2795 (1997). 10.1523/JNEUROSCI.17-08-02785.1997 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nichols, D. E. Hallucinogens. Pharmacol. Ther.101, 131–181 (2004). 10.1016/j.pharmthera.2003.11.002 [DOI] [PubMed] [Google Scholar]
- 10.Vollenweider, F. X., Vollenweider-Scherpenhuyzen, M. F. I., Bäbler, A., Vogel, H. & Hell, D. Psilocybin induces schizophrenia-like psychosis in humans via a serotonin-2 agonist action. NeuroReport9, 3897–3902 (1998). 10.1097/00001756-199812010-00024 [DOI] [PubMed] [Google Scholar]
- 11.Carhart-Harris, R. L. et al. Psilocybin with psychological support for treatment-resistant depression: an open-label feasibility study. Lancet Psychiatry3, 619–627 (2016). 10.1016/S2215-0366(16)30065-7 [DOI] [PubMed] [Google Scholar]
- 12.Davis, A. K. et al. Effects of psilocybin-assisted therapy on major depressive disorder: a randomized clinical trial. JAMA Psychiatry78, 481–489 (2020). [DOI] [PMC free article] [PubMed]
- 13.Griffiths, R. R. et al. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: a randomized double-blind trial. J. Psychopharmacol.30, 1181–1197 (2016). 10.1177/0269881116675513 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ross, S. et al. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: a randomized controlled trial. J. Psychopharmacol.30, 1165–1180 (2016). 10.1177/0269881116675512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Carhart-Harris, R. L. & Goodwin, G. M. The therapeutic potential of psychedelic drugs: past, present, and future. Neuropsychopharmacology42, 2105–2113 (2017). 10.1038/npp.2017.84 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ly, C. et al. Psychedelics promote structural and functional neural plasticity. Cell Rep.23, 3170–3182 (2018). 10.1016/j.celrep.2018.05.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Savalia, N. K., Shao, L.-X. & Kwan, A. C. A dendrite-focused framework for understanding the actions of ketamine and psychedelics. Trends Neurosci.44, 260–275 (2021). 10.1016/j.tins.2020.11.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Canal, C. E. et al. Molecular pharmacology and ligand docking studies reveal a single amino acid difference between mouse and human serotonin 5-HT2A receptors that impacts behavioral translation of novel 4-phenyl-2-dimethylaminotetralin ligands. J. Pharmacol. Exp. Ther.347, 705–716 (2013). 10.1124/jpet.113.208637 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gouzoulis-Mayfrank, E. et al. Neurometabolic effects of psilocybin, 3,4-methylenedioxyethylamphetamine (MDE) and d-methamphetamine in healthy volunteers: a double-blind, placebo-controlled PET study with [18F]FDG. Neuropsychopharmacol.20, 565–581 (1999). 10.1016/S0893-133X(98)00089-X [DOI] [PubMed] [Google Scholar]
- 20.Vollenweider, F. X. et al. Positron emission tomography and fluorodeoxyglucose studies of metabolic hyperfrontality and psychopathology in the psilocybin model of psychosis. Neuropsychopharmacology16, 357–372 (1997). 10.1016/S0893-133X(96)00246-1 [DOI] [PubMed] [Google Scholar]
- 21.Mason, N. L. et al. Me, myself, bye: regional alterations in glutamate and the experience of ego dissolution with psilocybin. Neuropsychopharmacol.45, 2003–2011 (2020). [DOI] [PMC free article] [PubMed]
- 22.Muthukumaraswamy, S. D. et al. Broadband cortical desynchronization underlies the human psychedelic state. J. Neurosci.33, 15171–15183 (2013). 10.1523/JNEUROSCI.2063-13.2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tagliazucchi, E. et al. Increased global functional connectivity correlates with LSD-induced ego dissolution. Curr. Biol.26, 1043–1050 (2016). 10.1016/j.cub.2016.02.010 [DOI] [PubMed] [Google Scholar]
- 24.Girn, M. et al. A complex systems perspective on psychedelic brain action. Trends Cogn. Sci. 27, 433–445 (2023). [DOI] [PubMed]
- 25.McCulloch, D. E.-W. et al. Lasting effects of a single psilocybin dose on resting-state functional connectivity in healthy individuals. J. Psychopharmacol.36, 74–84 (2022). 10.1177/02698811211026454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Daws, R. E. et al. Increased global integration in the brain after psilocybin therapy for depression. Nat. Med.28, 844–851 (2022). 10.1038/s41591-022-01744-z [DOI] [PubMed] [Google Scholar]
- 27.Barrett, F. S., Doss, M. K., Sepeda, N. D., Pekar, J. J. & Griffiths, R. R. Emotions and brain function are altered up to one month after a single high dose of psilocybin. Sci. Rep.10, 2214 (2020). 10.1038/s41598-020-59282-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Yeo, B. T. et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol.106, 1125–65 (2011). 10.1152/jn.00338.2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Zheng, A. et al. Parallel hippocampal-parietal circuits for self- and goal-oriented processing. Proc. Natl Acad. Sci. USA118, e2101743118 (2021). 10.1073/pnas.2101743118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Colasanti, A. et al. Hippocampal neuroinflammation, functional connectivity, and depressive symptoms in multiple sclerosis. Biol. Psychiatry80, 62–72 (2016). 10.1016/j.biopsych.2015.11.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Siegel, J. S. et al. Prolonged ketamine infusion modulates limbic connectivity and induces sustained remission of treatment-resistant depression. Psychopharmacology238, 1157–1169 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Yan, C.-G. et al. Reduced default mode network functional connectivity in patients with recurrent major depressive disorder. Proc. Natl Acad. Sci. USA116, 9078–9083 (2019). 10.1073/pnas.1900390116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Beliveau, V. et al. A high-resolution in vivo atlas of the human brain’s serotonin system. J. Neurosci.37, 120–128 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Alagapan, S. et al. Cingulate dynamics track depression recovery with deep brain stimulation. Nature622, 130–138 (2023). 10.1038/s41586-023-06541-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lynch, C. J. et al. Expansion of a frontostriatal salience network in individuals with depression. Preprint at bioRxiv10.1101/2023.08.09.551651 (2023).
- 36.Mayberg, H. S. et al. Deep brain stimulation for treatment-resistant depression. Neuron45, 651–660 (2005). 10.1016/j.neuron.2005.02.014 [DOI] [PubMed] [Google Scholar]
- 37.Gordon, E. M. et al. Precision functional mapping of individual human brains. Neuron95, 791–807.e7 (2017). 10.1016/j.neuron.2017.07.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Gratton, C. et al. Functional brain networks are dominated by stable group and individual factors, not cognitive or daily variation. Neuron98, 439–452.e5 (2018). 10.1016/j.neuron.2018.03.035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Laumann, T. O. et al. Functional system and areal organization of a highly sampled individual human brain. Neuron87, 657–670 (2015). 10.1016/j.neuron.2015.06.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Poldrack, R. A. et al. Long-term neural and physiological phenotyping of a single human. Nat. Commun.6, 8885 (2015). 10.1038/ncomms9885 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Siddiqi, S. H. et al. Precision functional MRI mapping reveals distinct connectivity patterns for depression associated with traumatic brain injury. Sci. Transl. Med.15, eabn0441 (2023). 10.1126/scitranslmed.abn0441 [DOI] [PubMed] [Google Scholar]
- 42.Newbold, D. J. et al. Plasticity and spontaneous activity pulses in disused human brain circuits. Neuron107, 580–589.e6 (2020). 10.1016/j.neuron.2020.05.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Greene, D. J. et al. Integrative and network-specific connectivity of the basal ganglia and thalamus defined in individuals. Neuron105, 742–758.e6 (2020). 10.1016/j.neuron.2019.11.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Marek, S. et al. Spatial and temporal organization of the individual human cerebellum. Neuron100, 977–993.e7 (2018). 10.1016/j.neuron.2018.10.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kiilerich, K. F. et al. Repeated low doses of psilocybin increase resilience to stress, lower compulsive actions, and strengthen cortical connections to the paraventricular thalamic nucleus in rats. Mol. Psychiatry28, 3829–3841 (2023). [DOI] [PubMed]
- 46.Barrett, F. S., Johnson, M. W. & Griffiths, R. R. Validation of the revised Mystical Experience Questionnaire in experimental sessions with psilocybin. J. Psychopharmacol.29, 1182–1190 (2015). 10.1177/0269881115609019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Chen, Y. & Liang, K.-Y. On the asymptotic behaviour of the pseudolikelihood ratio test statistic with boundary problems. Biometrika97, 603–620 (2010). 10.1093/biomet/asq031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Stram, D. O. & Lee, J. W. Variance components testing in the longitudinal mixed effects model. Biometrics50, 1171–1177 (1994). 10.2307/2533455 [DOI] [PubMed] [Google Scholar]
- 49.Bertolero, M. A., Yeo, B. T. T. & D’Esposito, M. The modular and integrative functional architecture of the human brain. Proc. Natl Acad. Sci. USA112, E6798–6807 (2015). 10.1073/pnas.1510619112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Fox, M. D., Corbetta, M., Snyder, A. Z., Vincent, J. L. & Raichle, M. E. Spontaneous neuronal activity distinguishes human dorsal and ventral attention systems. Proc. Natl Acad. Sci. USA103, 10046–51 (2006). 10.1073/pnas.0604187103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Seeley, W. W. et al. Dissociable intrinsic connectivity networks for salience processing and executive control. J. Neurosci.27, 2349–56 (2007). 10.1523/JNEUROSCI.5587-06.2007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Dosenbach, N. U. et al. Distinct brain networks for adaptive and stable task control in humans. Proc. Natl Acad. Sci. USA104, 11073–8 (2007). 10.1073/pnas.0704320104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Dosenbach, N. U. F., Raichle, M. & Gordon, E. M. The brain’s cingulo-opercular action-mode network. Preprint at PsyArXivhttps://osf.io/2vt79 (2024).
- 54.Fox, M. D. et al. The human brain is intrinsically organized into dynamic, anticorrelated functional networks. Proc. Natl Acad. Sci. USA102, 9673–9678 (2005). 10.1073/pnas.0504136102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Carhart-Harris, R. L. et al. Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proc. Natl Acad. Sci. USA109, 2138–2143 (2012). 10.1073/pnas.1119598109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Carhart-Harris, R. L. et al. Neural correlates of the LSD experience revealed by multimodal neuroimaging. Proc. Natl Acad. Sci. USA113, 4853–4858 (2016). 10.1073/pnas.1518377113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Dai, R. et al. Classical and non-classical psychedelic drugs induce common network changes in human cortex. NeuroImage273, 120097 (2023). 10.1016/j.neuroimage.2023.120097 [DOI] [PubMed] [Google Scholar]
- 58.Mueller, S. et al. The effects of methylphenidate on whole brain intrinsic functional connectivity. Hum. Brain Mapp.35, 5379–5388 (2014). 10.1002/hbm.22557 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Casey, B. J. et al. The Adolescent Brain Cognitive Development (ABCD) study: imaging acquisition across 21 sites. Dev. Cogn. Neurosci.32, 43–54 (2018). 10.1016/j.dcn.2018.03.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Celada, P., Puig, M. V., Díaz-Mataix, L. & Artigas, F. The hallucinogen DOI reduces low-frequency oscillations in rat prefrontal cortex: reversal by antipsychotic drugs. Biol. Psychiatry64, 392–400 (2008). 10.1016/j.biopsych.2008.03.013 [DOI] [PubMed] [Google Scholar]
- 61.Jia, H., Li, Y. & Yu, D. Normalized spatial complexity analysis of neural signals. Sci. Rep.8, 7912 (2018). 10.1038/s41598-018-26329-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Gordon, E. M. et al. Generation and evaluation of a cortical area parcellation from resting-state correlations. Cereb. Cortex26, 288–303 (2016). 10.1093/cercor/bhu239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Preller, K. H. et al. Psilocybin induces time-dependent changes in global functional connectivity. Biol. Psychiatry88, 197–207 (2020). 10.1016/j.biopsych.2019.12.027 [DOI] [PubMed] [Google Scholar]
- 64.Johnson, M., Richards, W. & Griffiths, R. Human hallucinogen research: guidelines for safety. J. Psychopharmacol.22, 603–620 (2008). 10.1177/0269881108093587 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Mediano, P. A. M. et al. Effects of external stimulation on psychedelic state neurodynamics. ACS Chem. Neurosci.15, 462–471 (2024). [DOI] [PMC free article] [PubMed]
- 66.Nardou, R. et al. Psychedelics reopen the social reward learning critical period. Nature618, 790–798 (2023). [DOI] [PMC free article] [PubMed]
- 67.Rijsketic, D. R. et al. UNRAVELing the synergistic effects of psilocybin and environment on brain-wide immediate early gene expression in mice. Neuropsychopharmacol.48, 1798–1807 (2023) [DOI] [PMC free article] [PubMed]
- 68.Golden, T. L. et al. in Disruptive Psychopharmacology (eds. Barrett, F. S. & Preller, K. H.) 35–70 (Springer International Publishing, 2022).
- 69.Michaiel, A. M., Parker, P. R. L. & Niell, C. M. A hallucinogenic serotonin-2A receptor agonist reduces visual response gain and alters temporal dynamics in mouse V1. Cell Rep.26, 3475–3483.e4 (2019). 10.1016/j.celrep.2019.02.104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Evarts, E. V., Landau, W., Freygang, W. & Marshall, W. H. Some effects of lysergic acid diethylamide and bufotenine on electrical activity in the cat’s visual system. Am. J. Physiol.-Leg. Content182, 594–598 (1955). 10.1152/ajplegacy.1955.182.3.594 [DOI] [PubMed] [Google Scholar]
- 71.Raichle, M. E. Two views of brain function. Trends Cogn. Sci.14, 180–190 (2010). 10.1016/j.tics.2010.01.008 [DOI] [PubMed] [Google Scholar]
- 72.Müller, F. et al. MDMA-induced changes in within-network connectivity contradict the specificity of these alterations for the effects of serotonergic hallucinogens. Neuropsychopharmacology46, 545–553 (2021). 10.1038/s41386-020-00906-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Palhano-Fontes, F. et al. The psychedelic state induced by ayahuasca modulates the activity and connectivity of the default mode network. PLoS ONE10, e0118143 (2015). 10.1371/journal.pone.0118143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Preller, K. H. et al. Changes in global and thalamic brain connectivity in LSD-induced altered states of consciousness are attributable to the 5-HT2A receptor. eLife7, e35082 (2018). 10.7554/eLife.35082 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Wall, M. B. et al. Neuroimaging in psychedelic drug development: past, present, and future. Mol. Psychiatry28, 3573–358 (2023). [DOI] [PMC free article] [PubMed]
- 76.Timmermann, C. et al. Neural correlates of the DMT experience assessed with multivariate EEG. Sci. Rep.9, 16324 (2019). 10.1038/s41598-019-51974-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Carhart-Harris, R. L. et al. The entropic brain: a theory of conscious states informed by neuroimaging research with psychedelic drugs. Front. Hum. Neurosci.8, 20 (2014). 10.3389/fnhum.2014.00020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Savino, A. & Nichols, C. D Lysergic acid diethylamide induces increased signalling entropy in rats’ prefrontal cortex. J. Neurochem.162, 9–23 (2022). [DOI] [PMC free article] [PubMed]
- 79.Aghajanian, G. K. & Marek, G. J. Serotonin, via 5-HT2A receptors, increases EPSCs in layer V pyramidal cells of prefrontal cortex by an asynchronous mode of glutamate release. Brain Res.825, 161–171 (1999). 10.1016/S0006-8993(99)01224-X [DOI] [PubMed] [Google Scholar]
- 80.Halberstadt, A., Vollenweider, F. X. & Nichols, D. E. Behavioral Neurobiology of Psychedelic Drugs (Springer, 2018).
- 81.Kavalali, E. T. & Monteggia, L. M. How does ketamine elicit a rapid antidepressant response? Curr. Opin. Pharmacol.20, 35–39 (2015). 10.1016/j.coph.2014.11.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Sahib, A. K. et al. Modulation of the functional connectome in major depressive disorder by ketamine therapy. Psychol. Med.52, 2596–2605 (2022). 10.1017/S0033291720004560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Styr, B. et al. Mitochondrial regulation of the hippocampal firing rate set point and seizure susceptibility. Neuron102, 1009–1024.e8 (2019). 10.1016/j.neuron.2019.03.045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Turrigiano, G. G., Leslie, K. R., Desai, N. S., Rutherford, L. C. & Nelson, S. B. Activity-dependent scaling of quantal amplitude in neocortical neurons. Nature391, 892–896 (1998). 10.1038/36103 [DOI] [PubMed] [Google Scholar]
- 85.Turrigiano, G. G. & Nelson, S. B. Homeostatic plasticity in the developing nervous system. Nat. Rev. Neurosci.5, 97–107 (2004). 10.1038/nrn1327 [DOI] [PubMed] [Google Scholar]
- 86.Duman, R. S. & Monteggia, L. M. A neurotrophic model for stress-related mood disorders. Biol. Psychiatry59, 1116–1127 (2006). 10.1016/j.biopsych.2006.02.013 [DOI] [PubMed] [Google Scholar]
- 87.Cole, E. J. et al. Stanford Neuromodulation Therapy (SNT): a double-blind randomized controlled trial. Am. J. Psychiatry179, 132–141 (2022). 10.1176/appi.ajp.2021.20101429 [DOI] [PubMed] [Google Scholar]
- 88.LeDoux, J. E. & Lau, H. A new vista in psychiatric treatment: using individualized functional connectivity to track symptoms. Proc. Natl Acad. Sci. USA117, 4450–4452 (2020). 10.1073/pnas.2000934117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Menon, V. Large-scale brain networks and psychopathology: a unifying triple network model. Trends Cogn. Sci.15, 483–506 (2011). 10.1016/j.tics.2011.08.003 [DOI] [PubMed] [Google Scholar]
- 90.Sylvester, C. M. et al. Individual-specific functional connectivity of the amygdala: a substrate for precision psychiatry. Proc. Natl Acad. Sci. USA117, 3808–3818 (2020). 10.1073/pnas.1910842117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Williams, L. M. Precision psychiatry: a neural circuit taxonomy for depression and anxiety. Lancet Psychiatry3, 472–480 (2016). 10.1016/S2215-0366(15)00579-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Davey, C. G. et al. Neurodevelopmental correlates of the emerging adult self. Dev. Cogn. Neurosci.36, 100626 (2019). 10.1016/j.dcn.2019.100626 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Montagrin, A. et al. Hippocampal timestamp for goals. Preprint at bioRxiv10.1101/2023.07.27.550892 (2023).
- 94.Gordon, E. M. et al. A somato-cognitive action network alternates with effector regions in motor cortex. Nature617, 351–359 (2023). 10.1038/s41586-023-05964-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Lynch, C. J. et al. Rapid precision functional mapping of individuals using Multi-Echo fMRI. Cell Rep.33, 108540 (2020). 10.1016/j.celrep.2020.108540 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Siegel, J. S. & Nicol, G. E. Plasticity markers in the human brain associated with rapid antidepressants. Neuropsychopharmacology48, 223–224 (2023). 10.1038/s41386-022-01400-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Alexander-Bloch, A. F. et al. On testing for spatial correspondence between maps of human brain structure and function. NeuroImage178, 540–551 (2018). 10.1016/j.neuroimage.2018.05.070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Brown, R. T. et al. Pharmacokinetics of escalating doses of oral psilocybin in healthy adults. Clin. Pharmacokinet.56, 1543–1554 (2017). 10.1007/s40262-017-0540-6 [DOI] [PubMed] [Google Scholar]
- 99.Griffiths, R. R., Richards, W. A., McCann, U. & Jesse, R. Psilocybin can occasion mystical-type experiences having substantial and sustained personal meaning and spiritual significance. Psychopharmacology187, 268–283 (2006). 10.1007/s00213-006-0457-5 [DOI] [PubMed] [Google Scholar]
- 100.Donnellan, M. B., Oswald, F. L., Baird, B. M. & Lucas, R. E. The mini-IPIP scales: tiny-yet-effective measures of the Big Five factors of personality. Psychol. Assess.18, 192–203 (2006). 10.1037/1040-3590.18.2.192 [DOI] [PubMed] [Google Scholar]
- 101.Shannon, B. J. et al. Morning-evening variation in human brain metabolism and memory circuits. J. Neurophysiol.109, 1444–1456 (2013). 10.1152/jn.00651.2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Moeller, S. et al. Multiband multislice GE-EPI at 7 tesla, with 16-fold acceleration using partial parallel imaging with application to high spatial and temporal whole-brain fMRI. Magn. Reson. Med.63, 1144–1153 (2010). 10.1002/mrm.22361 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Kundu, P. et al. Integrated strategy for improving functional connectivity mapping using multiecho fMRI. Proc. Natl Acad. Sci. USA110, 16187–92 (2013). 10.1073/pnas.1301725110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Blaimer, M. et al. SMASH, SENSE, PILS, GRAPPA: how to choose the optimal method. Top. Magn. Reson. Imaging TMRI15, 223–236 (2004). 10.1097/01.rmr.0000136558.09801.dd [DOI] [PubMed] [Google Scholar]
- 105.Dosenbach, N. U. F. et al. Real-time motion analytics during brain MRI improve data quality and reduce costs. NeuroImage161, 80–93 (2017). 10.1016/j.neuroimage.2017.08.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Siegel, J. S. et al. Statistical improvements in functional magnetic resonance imaging analyses produced by censoring high-motion data points. Hum. Brain Mapp.35, 1981–1996 (2014). [DOI] [PMC free article] [PubMed]
- 107.Moeller, S. et al. NOise reduction with DIstribution Corrected (NORDIC) PCA in dMRI with complex-valued parameter-free locally low-rank processing. NeuroImage226, 117539 (2021). 10.1016/j.neuroimage.2020.117539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Vizioli, L. et al. Lowering the thermal noise barrier in functional brain mapping with magnetic resonance imaging. Nat. Commun.12, 5181 (2021). 10.1038/s41467-021-25431-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Moser, J. et al. Multi-echo acquisition and thermal denoising advances infant precision functional imaging. Preprint at bioRxiv10.1101/2023.10.27.564416 (2023).
- 110.Posse, S. et al. Enhancement of BOLD-contrast sensitivity by single-shot multi-echo functional MR imaging. Magn. Reson. Med.42, 87–97 (1999). [DOI] [PubMed] [Google Scholar]
- 111.Siegel, J. S. et al. Data quality influences observed links between functional connectivity and behavior. Cereb. Cortex27, 4492–4502 (2017). 10.1093/cercor/bhw253 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Behzadi, Y., Restom, K., Liau, J. & Liu, T. T. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. NeuroImage37, 90–101 (2007). 10.1016/j.neuroimage.2007.04.042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Power, J. D. A simple but useful way to assess fMRI scan qualities. NeuroImage154, 150–158 (2017). 10.1016/j.neuroimage.2016.08.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Glasser, M. F. et al. The minimal preprocessing pipelines for the Human Connectome Project. NeuroImage80, 105–124 (2013). 10.1016/j.neuroimage.2013.04.127 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Seitzman, B. A. et al. A set of functionally-defined brain regions with improved representation of the subcortex and cerebellum. NeuroImage206, 116290 (2020). 10.1016/j.neuroimage.2019.116290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.LeDoux, J. E. Emotion circuits in the brain. Annu. Rev. Neurosci.23, 155–184 (2000). 10.1146/annurev.neuro.23.1.155 [DOI] [PubMed] [Google Scholar]
- 117.Price, J. L. & Drevets, W. C. Neurocircuitry of mood disorders. Neuropsychopharmacology35, 192–216 (2010). 10.1038/npp.2009.104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Rosvall, M. & Bergstrom, C. T. Maps of random walks on complex networks reveal community structure. Proc. Natl Acad. Sci. USA105, 1118–1123 (2008). 10.1073/pnas.0706851105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Mammen, E. Bootstrap and wild bootstrap for high dimensional linear models. Ann. Stat.21, 255–285 (1993). 10.1214/aos/1176349025 [DOI] [Google Scholar]
- 120.Davidson, J., Monticini, A. & Peel, D. Implementing the wild bootstrap using a two-point distribution. Econ. Lett.96, 309–315 (2007). 10.1016/j.econlet.2007.01.020 [DOI] [Google Scholar]
- 121.Smith, S. M. & Nichols, T. E. Threshold-free cluster enhancement: addressing problems of smoothing, threshold dependence and localisation in cluster inference. NeuroImage44, 83–98 (2009). 10.1016/j.neuroimage.2008.03.061 [DOI] [PubMed] [Google Scholar]
- 122.Dittrich, A. The Standardized Psychometric Assessment of Altered States of Consciousness (ASCs) in humans. Pharmacopsychiatry31, 80–84 (1998). 10.1055/s-2007-979351 [DOI] [PubMed] [Google Scholar]
- 123.Lakens, D. Equivalence tests. Soc. Psychol. Personal. Sci.8, 355–362 (2017). 10.1177/1948550617697177 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Feczko, E. et al. Adolescent Brain Cognitive Development (ABCD) community MRI collection and utilities. Preprint at bioRiv10.1101/2021.07.09.451638 (2021).
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
This file contains Supplementary Table 1, Figs. 1–7 and Methods.
Quality control plots for every fMRI scan. For each participant (P1, P3–P7, concatenated) the quality control plots are concatenated in the order that the scans were acquired (Extended Data Fig. 1). The top plot shows head position (frame-by-frame, relative to frame 1) separated into x, y, z translation and x, y, z rotation (six parameters). The second plot from the top shows DVARS, which index the rate of change of fMRI signal across the entire brain at each frame of data. The D refers to the temporal derivative of time courses, and VARS refers to the root-mean-square variance over voxels. The third plot shows head motion measured as FD (framewise displacement) in mm. Underneath in the fourth row, the time course for the whole-brain grayordinates (cortex on top, subcortex on the bottom) are shown before preprocessing (known as ‘grayplot’ or ‘carpet plot’). The fifth row shows the same grayordinates, but after preprocessing (bandpass filtering, removal of nuisance signals by regression, and smoothing at 4 mm full-width at half-maximum). The vertical black lines or bars in the grayplots indicate these data frames that were censored due to excessive head motion. At the end, quality control plots are compared to physiology (heart rate, respiratory rate) plots for every session in which physiological monitoring data were acquired.
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Time series of fully preprocessed resting-state fMRI (rs-fMRI) data (roughly 9 min), taken from the first resting scan of the MRI session. Frame-by-frame rs-fMRI data, excluding high head motion frames (FD > 0.3), are shown for the drug scans (psilocybin, MTP) for each participant (P1, P3–P7).
Data Availability Statement
All data from individual participants P1–P7 are available at https://wustl.box.com/v/PsilocybinPFM, with a password available on completion of a data use agreement. The ABCD data used in this report came from ABCD the Annual Release 2.0, 10.15154/1503209. The ABCD data repository grows and changes over time (https://nda.nih.gov/abcd). The Imperial College London psilocybin and LSD datasets are available upon request.
Data processing code for the psilocybin precision functional mapping data can be found at https://wustl.box.com/s/dmj5s3h9pxt9bcw9mm3ai9c15y756o79. Code specific to analyses can be found at https://gitlab.com/siegelandthebrain1/Psilocybin_PFM/. Data processing code for the ABCD data can be found at https://github.com/DCAN-Labs/abcd-hcp-pipeline. Matching task stimuli are available at https://gitlab.com/siegelandthebrain1/Psilocybin_PFM/-/blob/main/image_task_clean.zip. Software packages incorporated into the above pipelines for data analysis included: MATLAB R2019b, https://www.mathworks.com/ (including Psychtoolbox v.2.0 and Statistics and Machine Learning Toolbox v.11.6); Connectome Workbench v.1.5; http://www.humanconnectome.org/software/connectome-workbench.html; Freesurfer v.6.2, https://surfer.nmr.mgh.harvard.edu/; FSL v.6.0, https://fsl.fmrib.ox.ac.uk/fsl/fslwiki; 4dfp tools, https://4dfp.readthedocs.io/en/latest/; Infomap, https://www.mapequation.org; Cifti MATLAB utilities (including spin test): https://github.com/MidnightScanClub/SCAN and 4dfp tools, https://4dfp.readthedocs.io/en/latest/. MRI pulse sequences used to acquire the data are provided at https://gitlab.com/siegelandthebrain1/Psilocybin_PFM/-/blob/main/NP1161_MRI_sequence.pdf.