

Abstract
Background:
Mammographic breast density (MBD) is a strong risk factor and an intermediate phenotype for breast cancer, yet there are limited studies on how environmental pollutants are associated with MBD.
Objective:
We investigated associations of perfluorooctane sulfonate (PFOS), perfluorooctanoic acid (PFOA), and perfluorohexane sulfonate (PFHxS) levels with measures of MBD and evaluated if early life factors modified any associations.
Methods:
Metabolon performed metabolomics analysis using ultrahigh-performance liquid chromatography/tandem accurate mass spectrometry in fasting blood from 705 premenopausal women completing their annual screening mammogram in St. Louis, Missouri. We calculated least square means (LSM) of mammographic volumetric percent density (VPD), dense volume (DV), and nondense volume (NDV) by quartiles (Q) of PFOS, PFOA, and PFHxS from multivariable linear regression modeling overall and stratified by recruitment period, race, age at menarche, and body shape at age 10. Models were adjusted for age, age at menarche, body fat percentage, race, family history of breast cancer, oral contraceptive use, alcohol consumption, parity/age at first birth, and body shape at age 10.
Results:
PFOS, PFOA, and PFHxS were not significantly associated with VPD or NDV. PFHxS was significantly positively associated with DV (, , , ; ). PFOS was positively associated with DV (, , , ; ) with DV being 8.1%, 12%, and 12.3% higher in Q2, Q3, and Q4 compared to Q1. Among women who were underweight/normal weight at age 10, PFOS was positively associated with VPD (, , , ; ) while there was an inverse association among women who were overweight/obese at age 10 (, , , ; ) ().
Discussion:
We report novel associations of PFHxS and PFOS with DV in premenopausal women. PFOS, PFOA, and PFHxS were not associated with VPD and NDV. In addition, body shape at age 10 may modify the associations of PFOS with MBD. Further studies are needed to validate our findings and to evaluate the associations of other per- and polyfluoroalkyl substances (PFAS), as well as mixtures of PFAS, with MBD. https://doi.org/10.1289/EHP14065
Introduction
Pollution is one of the biggest challenges in public health, yet associations of environmental pollutants with mammographic breast density (MBD) are not well understood. MBD is an intermediate phenotype of breast cancer,1 and women with density on mammograms have a 4–6 times greater risk of developing breast cancer compared to women with density.2,3 MBD is a heritable but dynamic trait4 that is influenced by age, adiposity, several reproductive factors, menopausal status, race, family history of breast cancer, oral contraceptive use, and alcohol consumption.5 The Breast Cancer Surveillance Consortium found positive associations between particulate matter in diameter () and MBD,6 while the Nurses’ Health Study found null associations.7 However, these prior studies estimated pollution exposure using emission data.
Biomarkers provide direct measures of environmental exposures. The current literature on environmental exposure biomarkers and MBD focuses on “xenoestrogens” such as persistent organic pollutants (POPs) and their role as potential endocrine disruptors. One study reported weak positive associations between serum polychlorinated biphenyl (PCB) concentrations and percent MBD, especially among younger and middle-aged women,8 while another reported null associations.9 Generally, the literature on this topic is very limited and has been conducted mostly in postmenopausal women.10,11
Even less well studied are the associations of per- and polyfluoroalkyl substances (PFAS) biomarkers such as perfluorooctane sulfonate (PFOS), perfluorooctanoic acid (PFOA), and perfluorohexane sulfonate (PFHxS) with MBD. Resulting from the disposal of industrial waste, PFAS are ubiquitous and found in indoor dust,12 ambient air pollution,13 food packaging,14 and contaminated drinking water.15 Consumption of fish farmed from contaminated water sources can be a surrogate for dietary PFAS, especially PFOS, exposure.16–18 PFAS are detectible in blood19 and breast milk.20 In 2023, the International Agency for Research on Cancer (IARC) classified PFOS as “possibly carcinogenic to humans” and PFOA as “carcinogenic to humans.”21 A recent meta-analysis of eight studies reported positive associations of PFOA and PFHxS but no association of PFOS with breast cancer risk,22 with suggestions that the associations may differ by hormone receptor status.23–25 To the best of our knowledge, only one small study, limited to 116 non-Hispanic white and postmenopausal women, has investigated the associations of PFAS biomarkers with MBD.11 They reported no associations between PFAS and other POPs with MBD.11
Our objective is to address this gap in knowledge by investigating the association of PFAS levels (PFOS, PFOA, and PFHxS) with volumetric measures of MBD in a large and diverse group of premenopausal women. Metabolomics can illuminate the biological mechanisms underlying health outcomes,26,27 and this approach has been used to investigate associations of PFAS28,29 with breast cancer risk.23 We hypothesize positive associations between PFOS, PFOA, and PFHxS with volumetric percent density (VPD) and dense volume (DV) and inverse associations with nondense volume (NDV). Further, given that PFAS are associated with increased adiposity from childhood30 through early adulthood31 and delayed puberty,32 we hypothesize that age at menarche and body shape at age 10 will modify associations between PFAS and MBD; specifically, there are possibly stronger positive associations between PFAS and VPD among women who had greater adiposity at age 10 or later age at menarche.
Materials and Methods
Study Population and Sample Collection
Our study consists of 705 premenopausal women who completed their annual screening mammogram at the Joanne Knight Breast Health Center at the Siteman Cancer Center at Washington University School of Medicine (WUSM) in St. Louis, Missouri. Participants were recruited in two phases using the same eligibility criteria: December 2015 to October 201633 and September 2020 to February 2022.34 We contacted women prior to their routine annual mammogram to assess study eligibility. Women were considered eligible if they met the following criteria: premenopausal, not pregnant, no history of cancer, no history of breast reduction or implants, no selective estrogen receptor modulator use in the last 6 months, and able to comply with study procedures.33 We considered women with at least one regular menstrual cycle in the last 12 months, no history of hormone replacement therapy, and no history of bilateral oophorectomy as premenopausal and eligible. Participants completed a fasting blood draw on the same day as their annual screening mammogram.33 The blood samples were stored at at the Tissue Procurement Core at Siteman Cancer Center.35 We received approval from the institutional review board (IRB) (20200559) at Washington University School of Medicine in St. Louis to conduct this study. All participants provided written informed consent, and the study followed the guidelines outlined by the Declaration of Helsinki.
Covariates
Behavioral, reproductive, and demographic covariate information [age (continuous), age at menarche (continuous), race (non-Hispanic white, non-Hispanic black, Hispanic, Asian, American Indian/Alaska Native/Pacific Islander, and other races), family history of breast cancer (yes, no), oral contraceptive use (never, , 1–4 years, 5–9 years, ), alcohol consumption (never, drink/week, 1–2 drinks/week, 3–5 drinks/week, 6–10 drinks/week, and drinks/week), parity/age at first birth (nulliparous, 1–2 children and , 1–2 children and 25–29 years of age, 1–2 children and , children and , children and ), and body shape at age 10 (1–9 based on the Stunkard pictogram36)] were self-reported using a validated questionnaire administered on the day of study enrollment. The Stunkard pictogram is a validated nine-figure somatotype scale used to evaluate body mass index (BMI) during childhood and is strongly correlated with BMI at age 1033,36–38; the Nurses’ Health Study and Health Professionals Follow-up Study found a Pearson’s correlation coefficient of 0.65 in women when comparing recalled somatotypes and BMI at age 10.37 During the same visit, height and weight were measured to derive BMI,33 and body fat percentage (%) (continuous) was measured using the OMRON Full Body Sensor Body Composition Monitor and Scale model HBF-514C.38
Metabolomics Profiling
Analyses were performed at Metabolon (Durham, North Carolina, USA) using ultrahigh-performance liquid chromatography–mass spectrometry (UHPLC–MS) techniques that have been described in detail.39 Metabolon’s Xenobiotic subpathway included 32 metabolites, but we focused on the 3 PFAS (PFOS, PFOA, and PFHxS) because our current analysis is hypothesis driven to investigate associations of PFAS with MBD. The global biochemical profiling analysis involved reverse phase (RP) UHPLC–MS with positive ionization methods a) optimized for hydrophilic compounds, b) optimized for hydrophobic compounds, c) RP–UHPLC–MS with negative ionization methods, and d) hydrophilic interaction liquid chromatography (HILIC) method coupled to negative ions. PFOS, PFOA, and PFHxS were identified by automated comparisons between samples’ ion features and a reference library of chemical standard entries. Compounds are run in at least three concentrations before being added to the reference library to ensure a linearity of response. Quality control was also performed at Metabolon.40
We performed untargeted metabolomics; hence, peak values are presented rather than absolute concentrations. The peak for a given metabolite across samples is comparable, even though the specific concentration is not known. For instance, a sample with 50% more signal for a particular metabolite has 50% higher level of that metabolite. Importantly, the peak values are highly correlated and reflective of the PFAS levels. Prior studies have shown that serum PFOS, PFOA, and PFHxS levels assayed at Metabolon are strongly correlated with standard, targeted measurements of these biomarkers in the same subjects.23,29,41
Mammographic Breast Density Assessment
We used Volpara 1.5 (Volpara Health) to quantify volumetric measures of mammographic breast density (MBD): volumetric percent density (%) (VPD), dense volume () (DV), and nondense volume () (NDV). We calculated VPD by dividing the maximum fibroglandular volume between the left and right breasts by total breast volume (TBV) and multiplying by 100 [(DV/TBV) × 100]. VPD was also categorized into four categories: a) , b) 3.5%–7.5%, c) , and d) 42 based on the breast imaging reporting and data system (BI-RADS) (fifth edition). The percent ranges correspond to a) almost entirely fatty, b) scattered areas of fibroglandular density, c) heterogeneously dense, and d) extremely dense.42 DV is fibroglandular breast tissue that appears white and opaque on mammography. NDV is fatty breast tissue that appears dark and transparent on mammography. It is calculated as TBV-DV.
Statistical Analysis
PFAS levels were assessed across self-reported demographic, reproductive, and behavioral characteristics. They are presented as the mean and standard deviation of the peak area data for each PFAS measure (PFOS, PFOA, and PFHxS). In order to reduce bias from batch effect, we normalized the data using the ComBat method.43 Metabolon profiled the metabolomics peak area data in seven batches and then applied the median adjusted approach by dividing the peak area of each metabolite by the median peak area of its batch. As a result, the median-adjusted data is relative. This approach, however, substantially reduces between metabolite differences, with all metabolites having median values around 1, with minimal dispersion. To address this, we applied ComBat normalization, which is model based and applies an empirical Bayes shrinkage to adjust the mean and the variance of each metabolite by pooling information across all metabolites to correct batch effects.43–46 ComBat normalization benefits the batch effects correction for PFOS, PFOA, and PFHxS, as it borrows information from other metabolites. Spearman’s rank correlation analysis was performed to assess correlations among the three PFAS measures.
Missing Values
For the multivariable analyses, five women were excluded due to missing MBD measurements, making the final study population 700 women. Body shape at age 10 was missing in 6% () of women, and body fat percentage was missing in 4% (). Missing PFAS measurements [PFOS (), PFOA (), PFHxS ()] were negligible and robust to any handling of missing data.47 To maintain consistency with our general analysis workflow, we adopted a global imputation approach where missing values in the metabolite data, which includes the three PFAS, were imputed using the 10-nearest neighbors approach [R (version 1.70.0; R Development Core Team)].48 This global imputation approach, compared to the approach that only applies a subset of observations, obtains better imputation of missing values, as it incorporates the interrelationship among features.49 To impute covariates with missing observations, we performed multivariate imputation by chain equations through the mice package in R.50
Linear Regression
We calculated adjusted least square means (LSM) of VPD, DV, and NDV by quartiles of PFAS measures from covariate-adjusted multivariable linear regression modeling. We also calculated LSM of MBD by quartiles of PFAS in 617 women, who had no missing data on any of the variables. Covariates included in statistical analysis (age, age at menarche, body fat percentage, race, family history of breast cancer, oral contraceptive use, alcohol consumption, parity/age at first birth, and body shape at age 10) were selected based on their known associations with MBD in prior studies, including ours within the same study population.5 We adjusted for body fat percentage instead of BMI because it explained more variation in VPD (body fat adjusted vs. BMI-adjusted ). Body fat percentage is highly correlated with BMI () in our study population; hence, we did not adjust for BMI. The Stunkard pictogram was collapsed into four categories corresponding to underweight (1 and 2), normal weight (3 and 4), overweight (5), and obese (6–9).38 Women who did not identify as non-Hispanic white or non-Hispanic black were categorized as “other races,” and women who consumed “6–10 drinks” or “ drinks” were collapsed into “ drinks” due to the small number of women in these categories. The linear regression was performed using -transformed measures of MBD, and the estimated coefficients were then back transformed to the original scale. The -value for linear trend was computed by assigning the median of each quartile to all observations within the quartile and then treating that as an ordinal variable in the model.
We also performed multivariable linear models treating the quartiles of each PFAS measure as a categorical variable, with quartile 1 (Q1) as the reference group. We calculated the percent difference between each quartile compared to quartile 1 as 100 × (). Associations were considered statistically significant if the -value was .
Stratified Analysis
To determine if age at menarche, body shape at age 10, race, or recruitment period modified the associations between PFAS levels and MBD, we performed stratified analyses by age at menarche [below ( old) vs. above the median ( old)], body shape at age 10 [1–4 (underweight/normal weight BMI) vs. 5–9 (overweight/obese BMI)], race (non-Hispanic white vs. non-Hispanic black), and recruitment period (December 2015 to October 2016 vs. September 2020 to February 2022). Body shape at age 10 was selected because it reflects early life exposures. The mean age of thelarche in US females, which signals the beginning of breast development and puberty, is 9.7 years.51 Women who did not identify as non-Hispanic white or non-Hispanic black were excluded from the stratified analysis due to small numbers. Recruitment period was considered due to decreasing PFOA and PFOS levels in US adults.52 The interaction term between continuous PFAS measures and the original categories of each variable were added to the multivariable linear regression models to assess significance.
Nonlinear Associations
To identify potential nonlinear associations between PFAS levels and MBD measures, we performed multiple linear regression, including the cubic spline (linear, quadratic, cubic) terms, for each PFAS measure. We reported the likelihood ratio test (LRT) -values on comparing the full model with cubic spline terms compared to the model with only the linear term of each PFAS measure.
Bayesian Kernel Machine Regression
To account for the strong correlations and potential nonlinear combinatorial effects, we ran Bayesian kernel machine regression (BKMR) to include potential nonlinear mixture effects between the three PFAS on MBD.53,54 Adjusting for covariates, we applied a Gaussian kernel to fit a kernel mixture of the PFAS to estimate the joint effects of the PFAS. The effect of one PFAS on an outcome of mammographic breast density was visualized by holding the other two PFAS at their median values. We ran 10,000 Markov chain Monte Carlo (MCMC) iterations with the first 5,000 as burn-in to fit the BKMR. The R package “bkmr” was used for analysis. R Studio (version 2023.09.1 and version 4.3.1) was used for analysis.
Results
Characteristics of Study Participants
Table 1 presents the characteristics of our study population across PFOS, PFOA, and PFHxS levels as peak area values. Most of our participants were non-Hispanic white (71.8%), and 23.1% were non-Hispanic black. The median age of enrollment was 46 years old, and the median age of menarche was 13 years old. The majority (74.8%) of participants had body shapes 1–4 at age 10 (corresponding to underweight/normal weight), and 20.6% of participants had body shapes 5–9 at age 10 (corresponding to overweight/obese). Women with heterogeneously dense () and extremely dense breasts () had higher mean PFAS levels than women with almost entirely fatty breasts () and scattered areas of fibroglandular densities (3.5–7.5%). Women who were underweight/normal weight at age 10 had higher mean PFOS and PFOA levels than woman who were overweight/obese at age 10. We present MBD measures by recruitment period in Table S1. Distributions of PFAS levels as peak area values in the overall study population, stratified by body shape at age 10, and stratified by recruitment period are presented in Table S2, Table S3, and Table S4, respectively. There were strong positive correlations between the three PFAS ranging from to (Table S5).
Table 1.
Characteristics of premenopausal women recruited during annual screening mammogram at Washington University School of Medicine (St. Louis, Missouri) from December 2015 to October 2016 and from September 2020 to February 2022 across PFOS, PFOA, and PFHxS peak area levels from untargeted metabolomics ().
| Characteristic | (%) | PFOSa | PFOAb | PFHxSc |
|---|---|---|---|---|
| Race | ||||
| White | 506 (72) | |||
| Black | 163 (23) | |||
| Other races | 31 (4) | |||
| Missing | 5 (1) | — | — | — |
| Age at enrollment | ||||
| (46 years old) | 386 (55) | |||
| (46 years old) | 319 (45) | |||
| Age at menarche | ||||
| (13 years old) | 514 (73) | |||
| (13 years old) | 189 (27) | |||
| Missing | 2 (0.3) | — | — | — |
| Body shape at age 10d | ||||
| 1–2 | 290 (41) | |||
| 3–4 | 237 (34) | |||
| 5 | 85 (12) | |||
| 6–9 | 53 (8) | |||
| Missing | 40 (6) | — | — | — |
| Percentage body fat | ||||
| (40.5%) | 334 (47) | |||
| (40.5%) | 336 (48) | |||
| Missing | 25 (4) | |||
| Age at first birth | ||||
| Nulliparous | 162 (23) | |||
| (27 years old) | 285 (40) | |||
| (27 years old) | 256 (36) | |||
| Missing | 2 (0.3) | — | — | — |
| Parity, age at first birth | ||||
| Nulliparous | 162 (23) | |||
| 1–2 children, | 107 (15) | |||
| 1–2 children, 25–29 years | 111 (16) | |||
| 1–2 children, | 156 (22) | |||
| children, | 88 (12) | |||
| children, | 79 (11) | |||
| Missing | 2 (0.3) | — | — | — |
| Family history of breast cancer | ||||
| No | 540 (77) | |||
| Yes | 152 (22) | |||
| Don’t know | 13 (2) | |||
| Oral contraceptive use (years) | ||||
| No | 82 (12) | |||
| 55 (8) | ||||
| 1–4 years | 141 (20) | |||
| 5–9 years | 143 (20) | |||
| 281 (40) | ||||
| Missing | 3 (0.4) | — | — | — |
| Alcohol consumption (drinks/week) | ||||
| Never | 211 (3) | |||
| 181 (26) | ||||
| 1–2 | 133 (19) | |||
| 3–5 | 127 (18) | |||
| 52 (7) | ||||
| Missing | 1 (0.1) | — | — | — |
| VPD category (%) | ||||
| 35 (5) | ||||
| and | 314 (45) | |||
| and | 197 (28) | |||
| 154 (22) | ||||
| Missing | 5 (0.7) | — | — | — |
| Overall | — | |||
Note: Peak area data for PFOS, PFOA, and PFHxS are presented as deviations by participant characteristics. Presented values are . Presented values were ComBat normalized to reduce bias from batch effect, and the missing PFAS values were imputed. The missing PFAS observations, prior to imputation, are presented below. —, no data; DV, dense volume; NDV, nondense volume; PFAS, per- and polyfluoroalkyl substances; PFHxS, perfluorohexane sulfonate; PFOA, perfluorooctanoic acid; PFOS, perfluorooctane sulfonate; VPD, volumetric percent density.
Missing PFAS [ (%)] observations: PFOS [1(0.1)].
Missing PFAS [ (%)] observations: PFOA [2(0.3)].
Missing PFAS [ (%)] observations: PFHxS [9(1)].
Self-reported based on Stunkard pictogram.
Associations of PFAS Levels with MBD (VPD, NDV, DV)
In multivariable-adjusted analyses, there were no statistically significant associations between PFOS, PFOA, and PFHxS and VPD and NDV (Table 2). PFOS and PFHxS were positively associated with DV, but only PFHxS was statistically significant (). DV increased across quartiles of PFOS levels ( in Q1, in Q2, in Q3, and in Q4; ). Across quartiles of PFHxS, DV was in Q1, in Q2, in Q3, and in Q4 (). The findings were similar in analyses excluding women with any missing covariate data (Table S6). Compared to women in Q1 of PFOS, DV was 8.1%, 12%, and 12.3% higher in Q2, Q3, and Q4, respectively. Similarly, compared to women in Q1 of PFHxS, DV was 3.4%, 2.1%, and 12% higher in Q2, Q3, and Q4, respectively (Table 3).
Table 2.
PFOS, PFOA, and PFHxS levels and covariate-adjusted least square means of mammographic breast density in 700 premenopausal women who completed their annual screening mammogram at Washington University School of Medicine (St. Louis, Missouri) from December 2015 to October 2016 and from September 2020 to February 2022.
| Category | Quartile 1 LSM (95% CI) | Quartile 2 LSM (95% CI) | Quartile 3 LSM (95% CI) | Quartile 4 LSM (95% CI) | -Trend |
|---|---|---|---|---|---|
| Volumetric percent density (%) | |||||
| PFOSa | 8.06 (7.27, 8.93) | 8.03 (7.23, 8.91) | 8.48 (7.63, 9.41) | 8.43 (7.58, 9.37) | 0.35 |
| PFOAb | 8.24 (7.42, 9.16) | 7.76 (7.00, 8.60) | 8.66 (7.81, 9.61) | 8.30 (7.43, 9.26) | 0.62 |
| PFHxSc | 7.92 (7.14, 8.79) | 8.51 (7.68, 9.43) | 8.25 (7.41, 9.19) | 8.28 (7.44, 9.22) | 0.75 |
| Nondense volume () | |||||
| PFOSa | 785.39 (710.28, 868.44) | 852.42 (769.9, 943.78) | 830.7 (749.78, 920.34) | 839.23 (756.96, 930.45) | 0.43 |
| PFOAb | 820.92 (740.46, 910.12) | 845.59 (764.45, 935.35) | 794.55 (718.12, 879.11) | 848.36 (761.93, 944.58) | 0.59 |
| PFHxSc | 823.66 (744.16, 911.66) | 786.78 (711.99, 869.43) | 815.74 (734.38, 906.12) | 881.8 (794.38, 978.84) | 0.07 |
| Dense volume () | |||||
| PFOSa | 65.45 (59.19, 72.37) | 70.74 (63.9, 78.32) | 73.31 (66.17, 81.22) | 73.52 (66.32, 81.51) | 0.06 |
| PFOAb | 69.98 (63.11, 77.60) | 67.71 (61.2, 74.91) | 71.71 (64.8, 79.35) | 73.36 (65.87, 81.7) | 0.22 |
| PFHxSc | 67.64 (61.1, 74.89) | 69.91 (63.25, 77.28) | 69.06 (62.16, 76.73) | 75.79 (68.26, 84.15) | 0.03 |
Note: Multivariable linear regression models were performed to calculate adjusted least square means of MBD (VPD, NDV, DV) by quartile of PFAS (PFOS, PFOA, PFHxS), and for trend values are presented to assess significance across the quartiles. Measures of MBD were transformed and coefficients back-transformed (). The -value for linear trend was computed by assigning the median of each quartile to all observations within the quartile and then treating it as an ordinal variable in the model. Five women were excluded due to missing MBD measurements. 95% CI, 95% confidence interval; DV, dense volume; LSM, least square mean; MBD, mammographic breast density; NDV, nondense volume; PFAS, per- and polyfluoroalkyl substances; PFHxS, perfluorohexane sulfonate; PFOA, perfluorooctanoic acid; PFOS, perfluorooctane sulfonate; VPD, volumetric percent density. All models were adjusted for age (continuous), age at menarche (continuous), body fat percentage (continuous), race (non-Hispanic white, non-Hispanic black, other), family history of breast cancer (yes, no), oral contraceptive use (never, , 1–4 years, 5–9 years, ), alcohol consumption (never, drink per week, 1–2 drinks per week, 3–5 drinks per week, and per week), parity/age at first birth (nulliparous, 1–2 children and , 1–2 children and 25–29 years, 1–2 children and , children and , children and ), and body shape at age 10 (1 and 2, 3 and 4, 5, 6–9). Quartile values shown are .
Ranges for the quartiles of PFOS (minimum, maximum): Q1 (0.09, 1.84), Q2 (1.84, 2.75), Q3 (2.75, 4.24), Q4 (4.24, 31.3).
Ranges for the quartiles of PFOA (minimum, maximum): Q1 (0.10, 0.79), Q2 (0.79, 1.25), Q3 (1.25, 1.82), Q4 (1.82, 34.5).
Ranges for the quartiles of PFHxS (minimum, maximum): Q1 (0.09, 0.70), Q2 (0.70, 1.13), Q3 (1.13, 1.73), Q4 (1.73, 11.3).
Table 3.
PFOS, PFOA, and PFHxS levels and covariate-adjusted percent difference of mammographic breast density in 700 premenopausal women who completed their annual screening mammogram at Washington University School of Medicine (St. Louis, Missouri) from December 2015 to October 2016 and from September 2020 to February 2022.
| Category | Quartile 1 % difference | Quartile 2 % difference | Quartile 3 % difference | Quartile 4 % difference | -Trend |
|---|---|---|---|---|---|
| Volumetric percent density (%) | |||||
| PFOSa | Ref | 5.17 | 4.58 | 0.35 | |
| PFOAb | Ref | 5.11 | 0.63 | 0.62 | |
| PFHxSc | Ref | 7.47 | 4.18 | 4.58 | 0.75 |
| Nondense volume () | |||||
| PFOSa | Ref | 8.54 | 5.77 | 6.86 | 0.43 |
| PFOAb | Ref | 3.01 | 3.34 | 0.59 | |
| PFHxSc | Ref | 7.06 | 0.07 | ||
| Dense volume () | |||||
| PFOSa | Ref | 8.09 | 12.02 | 12.34 | 0.06 |
| PFOAb | Ref | 2.47 | 4.84 | 0.22 | |
| PFHxSc | Ref | 3.36 | 2.09 | 12.04 | 0.03 |
Note: Multivariable linear regression models were performed to calculate the percent difference in MBD (VPD, NDV, DV) by quartile of PFAS (PFOS, PFOA, PFHxS) setting Quartile 1 as the reference, and for trend values are presented to assess significance across the quartiles. Measures of MBD were transformed and coefficients back-transformed (). Percent difference was calculated as 100 × [()]. Five women were excluded due to missing MBD measurements. DV, dense volume; LSM, least square mean; MBD, mammographic breast density; NDV, nondense volume; PFAS, per- and polyfluoroalkyl substances; PFHxS, perfluorohexane sulfonate; PFOA, perfluorooctanoic acid; PFOS, perfluorooctane sulfonate; Ref, reference; VPD, volumetric percent density. All models were adjusted for age (continuous), age at menarche (continuous), body fat percentage (continuous), race (non-Hispanic white, non-Hispanic black, other), family history of breast cancer (yes, no), oral contraceptive use (never, , 1–4 years, 5–9 years, ), alcohol consumption (never, drink per week, 1–2 drinks per week, 3–5 drinks per week, and per week), parity/age at first birth (nulliparous, 1–2 children and , 1–2 children and 25–29 years, 1–2 children and , children and , children and ) and body shape at age 10 (1 and 2, 3 and 4, 5, 6–9). Quartile values shown are .
Ranges for the quartiles of PFOS (minimum, maximum): Q1 (0.09, 1.84), Q2 (1.84, 2.75), Q3 (2.75, 4.24), Q4 (4.24, 31.3).
Ranges for the quartiles of PFOA (minimum, maximum): Q1 (0.10, 0.79), Q2 (0.79, 1.25), Q3 (1.25, 1.82), Q4 (1.82, 34.5).
Ranges for the quartiles of PFHxS (minimum, maximum): Q1 (0.09, 0.70), Q2 (0.70, 1.13), Q3 (1.13, 1.73), Q4 (1.73, 11.3).
Associations of PFAS Levels with VPD, NDV, and DV Stratified by Body Shape at Age 10, Age at Menarche, Race, and Recruitment Period
Body shape at age 10 modified the association between PFOS and VPD (Figure 1; Table S7). Among women with body shape 1–4 at age 10, corresponding to underweight/normal weight, VPD increased across the quartiles of PFOS (, , , ; ) while among women with body shape 5–9, corresponding to overweight/obese, PFOS was inversely associated with VPD (, , , ; ; ). Body shape at age 10 also modified the association of PFOA with NDV (Figure 1). There was no association between PFOA and NDV among women who were underweight/normal weight at age 10 ( vs. ; ), but among women who were overweight/obese at age 10, there was a nonmonotonic positive association between PFOA and NDV, ( vs. ; , ). No other tested interactions were significantly significant; age at menarche (Figure S1; Table S8), race (Figure S2; Table S9), and recruitment period (Figure S3; Table S10) did not significantly modify the relationship between PFAS and MBD.
Figure 1.
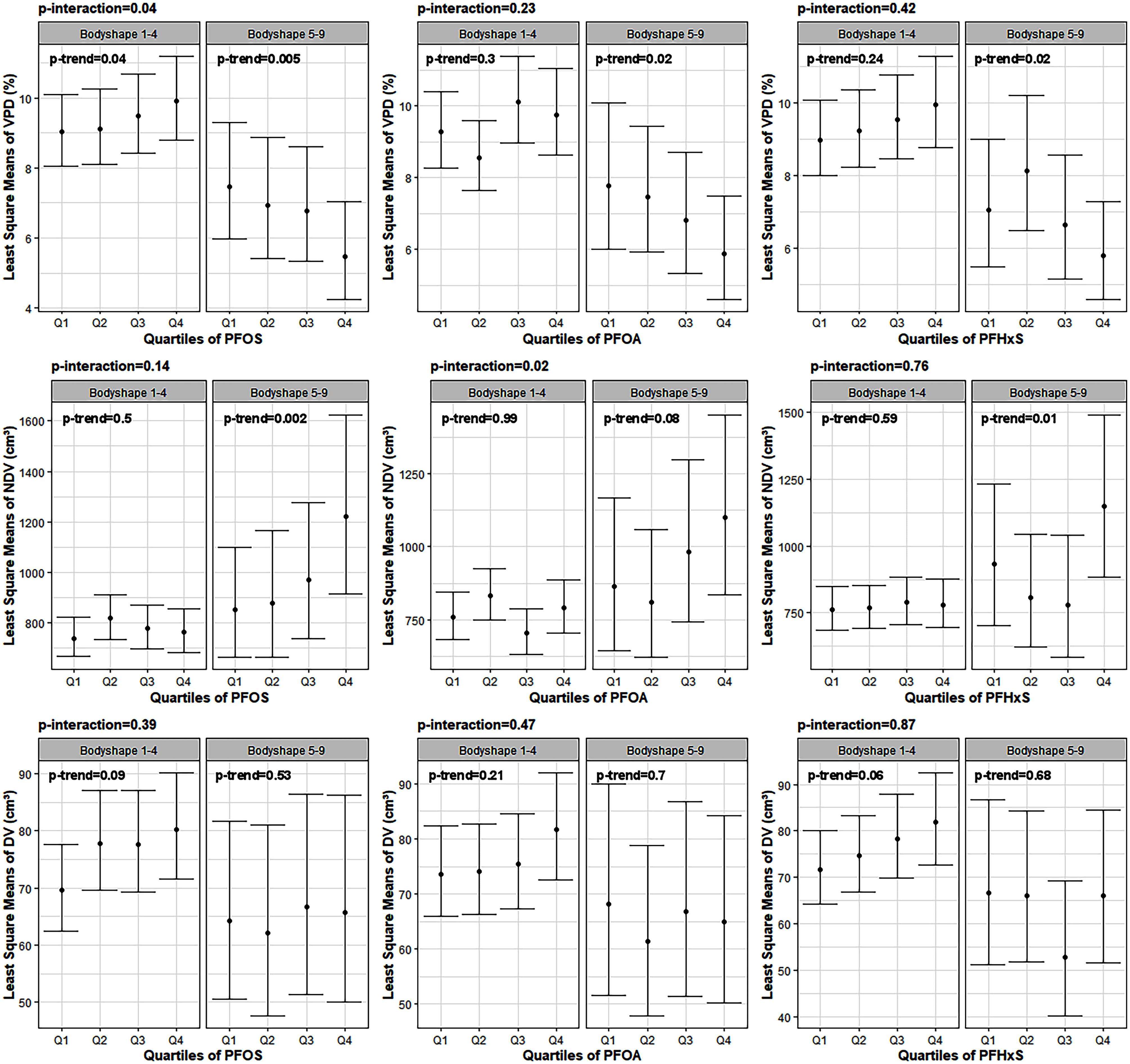
PFOS, PFOA, and PFHxS levels and covariate-adjusted least square means of mammographic breast density (MBD) stratified by body shape at age 10 (underweight/normal weight vs. overweight/obese) in 700 premenopausal women who completed their annual screening mammogram at Washington University School of Medicine (St. Louis, Missouri) from December 2015 to October 2016 and from September 2020 to February 2022. Note: Multivariable linear regression models were performed to calculate adjusted least square means of MBD (VPD, NDV, DV) by quartile of PFAS (PFOS, PFOA, PFHxS) separately for women who reported an underweight/normal weight body shape at age 10 (1–4) and women who reported an overweight/obese body shape at age 10 (5–9) based on the Stunkard pictogram. for trend values are presented to assess significance across the quartiles within each group and -interaction to see if the relationship between PFAS and MBD within each strata were different. All models adjusted for age, age at menarche, body fat percentage, race, family history of breast cancer, oral contraceptive use, alcohol consumption, and parity/age at first birth. Measures of MBD were transformed and coefficients back-transformed (). DV, dense volume; NDV, nondense volume; PFAS, per- and polyfluoroalkyl substances; PFHxS, perfluorohexane sulfonate; PFOA, perfluorooctanoic acid; PFOS, perfluorooctane sulfonate; Q1–Q4, Quartiles 1–4; VPD, volumetric percent density. Body shape at age 10 (1–4, ) quartile ranges (minimum, maximum): PFOS: Q1 (0.09, 1.81), Q2 (1.81, 2.70), Q3 (2.70, 4.22), Q4 (4.22, 31.3); PFOA: Q1 (0.13, 0.78), Q2 (0.78, 1.24), Q3 (1.24, 1.85), Q4 (1.85, 34.5); PFHxS: Q1 (0.09, 0.70), Q2 (0.70, 1.10), Q3 (1.10, 1.71), Q4 (1.71, 10.6). Body shape at age 10 (5–9, ) quartile ranges (minimum, maximum): PFOS: Q1 (0.27, 1.84), Q2 (1.84, 2.80), Q3 (2.80, 4.07), Q4 (4.07, 11.2); PFOA: Q1 (0.10, 0.78), Q2 (0.78, 1.15), Q3 (1.15, 1.69), Q4 (1.69, 4.98); PFHxS: Q1 (0.12, 0.64), Q2 (0.64, 1.13), Q3 (1.13, 1.69), Q4 (1.69, 6.52). Quartile values shown are . All numeric data used to generate these figures can be found in Table S7.
Analyses to Investigate Possible Nonlinear Associations
We found no evidence to suggest the presence of nonlinear associations as seen in the cubic spline plots (Figure S4; Table S11). The likelihood ratio test (LRT) -values (Table S12) showed no significant differences between models using a cubic spline function compared to models using a linear term for each PFAS.
BKMR Modeling
When compared with covariate-adjusted LSM models, BKMR modeling supported a positive association between PFOS and DV (Figure S5). We found a positive association between PFOS and VPD and no association between PFHxS and DV, which deviated from the overall LSM model, suggesting that additional adjustment for the other PFAS attenuated the association of PFHxS with DV.
Discussion
In this racially diverse population of premenopausal women, PFOS, PFOA, and PFHxS levels were not associated with VPD. PFOS and PFHxS were associated with DV. Further, body shape at age 10 modified the associations of PFOS with VPD and PFOA with NDV.
Research on environmental pollutants and their associations with MBD has yielded mixed findings with limited studies on PFAS specifically.8–11 To the best of our knowledge, our study is the first to investigate the associations of PFAS levels with MBD in premenopausal women and the potential interactions with early life factors. A previous small study reported no associations between PFAS and percent density, but the study did not evaluate associations with DV or NDV.11 We report novel associations of PFOS and PFHxS with DV. Additionally, while the previous study included only 116 non-Hispanic white postmenopausal women,11 our study is much larger and included a racially diverse population, including 23.1% non-Hispanic black women. Further, we stratified our analysis by early life factors, which provides insight into differences in susceptibility that may not have been detected in an unstratified analysis.
The positive associations that we observed with DV are biologically plausible. PFAS have been shown to induce cell proliferation and cell cycle dysregulation via increased transition from the G0/G1 phase to the S phase; down-regulation of p53, p21, and p27; and up-regulation of CDK4 levels in experimental models of human epithelial breast cells.55,56 Furthermore, PFOS and PFHxS have been positively associated with progesterone levels,57 a hormone associated with MBD in premenopausal women.58 Our findings may, thus, provide novel insights into how PFAS impacts MBD.
Findings from our stratified analysis also provide important new insight into the potential interplay between early life factors, PFAS levels, and MBD. We observed that women who were underweight/normal weight at age 10 had positive associations between PFOS and VPD, while women who were overweight/obese at age 10 had inverse associations. Exposure to endocrine disruptors during critical periods of maturation, such as puberty, could impact breast development and influence MBD and breast cancer risk in adulthood.59,60 PFAS have elimination half-lives that range from 3.8 to 8.5 years61; hence, short-term exposure could have lasting health effects. A prior study in the Project Viva cohort found that BMI trajectories based on prenatal PFOS exposure began diverging at old for females, with higher rates of BMI increases for children with higher prenatal PFOS exposure; this finding persisted throughout adolescence and early adulthood.31 In the European Youth Health Study, PFOS levels at age 9 were associated with increased adiposity at 15 and 21 years old.62 These findings are important in relation to MBD as childhood adiposity is inversely associated with VPD and DV, and positively associated with NDV.38,63 Our results for body shape at age 10, however, were not in the hypothesized direction. This may be due to reported inverse associations between BMI and progesterone64,65 and suggestions that adiposity mediates the relationship between progesterone and MBD.58 PFOA has also been associated with delayed menarche, while PFOS may delay thelarche.32 Delayed menarche and a longer interval between thelarche and menarche are associated with increased MBD.63,66 Childhood adiposity, however, attenuates the association between age at menarche and MBD,63 thus potentially explaining the null associations that we observed when stratifying for age at menarche.
While literature on the associations of PFAS with MBD is limited, prior studies have investigated the associations of PFAS with breast cancer risk. A systematic review and meta-analysis published in 2024 reported no significant associations between PFAS and breast cancer risk; however, a positive association of PFOA with breast cancer was evident when studies with prediagnostic blood samples were included.67 A previous meta-analysis reported positive associations of PFOA and PFHxS, but no association of PFOS with breast cancer risk overall.22 Studies have also reported divergent findings by tumor subtype, but there appears to be positive associations between PFOS and estrogen receptor-positive (ER+) or progesterone receptor-positive (PR+) tumors and positive associations between PFOA and estrogen receptor-negative (ER−) or progesterone receptor-negative (PR−) tumors.23–25 The California Teachers Study, however, found no associations by tumor subtype.68 Given that MBD is an independent risk factor for breast cancer, which also responds to the hormonal environment,69 our study contributes to the limited knowledge of how PFAS may be associated with MBD and potentially breast cancer risk in premenopausal women.
We performed untargeted metabolomics, which provides peak area values instead of absolute concentrations. Nevertheless, there is a strong correlation between the peak values and absolute concentrations.23,29,41 Chang et al. reported a strong correlation between serum PFOS () and PFOA () concentrations and peak area data from Metabolon in their study on PFAS and breast cancer.23 Salihovic et al. recently reported very strong correlations of 0.83 for PFOS, 0.92 for PFOA, and 0.96 for PFHxS when comparing targeted absolute concentrations using isotope dilution ultrahigh-performance liquid chromatography coupled to tandem mass spectrometry (UHPLC–MS/MS) with Metabolon’s nontargeted relative quantification in healthy individuals.29
Strengths of our study include the large sample of diverse premenopausal women. Additionally, we have data on early life factors, which enabled us to evaluate their potential roles as effect modifiers, justifying further research in this area. Limitations include the cross-sectional nature of this study; hence, a temporal association between PFAS and MBD cannot be established. Additionally, PFOS and PFOA levels in US adults have been decreasing over time,52 suggesting that PFAS levels in our study participants, who were on average 46 years old during the time of enrollment, may not reflect levels in childhood. This trend may attenuate the effects of these PFAS on MBD, making it challenging to detect true associations. The timing of PFAS exposure may also play a role. Adolescent exposure may have stronger effects on measures of MBD, as puberty is a period of rapid breast development, and prior research indicates that the period between menarche and first birth is particularly important in determining future breast cancer risk.70 The only PFAS reported in Metabolon’s untargeted panels are PFOS, PFOA, and PFHxS; hence, we could not determine the associations of other PFAS, such as perfluorononanoic acid (PFNA) and perfluorodecanoic acid (PFDA), with MBD in our study. These limitations made mixture analyses less robust and informative, as we had no information regarding other PFAS that may have impacted our outcomes. Lastly, although our study population is large and diverse, they are not necessarily representative of the US population. Nevertheless, our study population is representative of the women who undergo screening mammogram at Washington University School of Medicine (WUSM) in St. Louis, Missouri and is generalizable to the study population that study participants were recruited from.5,71 Additional studies are needed to validate our findings and to evaluate the associations of other PFAS, as well as mixtures of PFAS, with MBD. In conclusion, we report novel associations of PFOS and PFHxS with DV in premenopausal women but no associations of PFOS, PFOA, and PFHxS with VPD and NDV. Notably, the impact of body shape at age 10 on the associations of PFOS with VPD and PFOA with NDV warrant further investigation.
Supplementary Material
Acknowledgments
A.T.T. conceptualized and collected data for the study. M.S.J., C.L., and J.L. analyzed the data. A.T.T. and K.R.G. interpreted the results. Y.S.N., J.K.K., and K.R.G. wrote the manuscript. A.T.T. provided revisions and feedback. All authors read and approved the final manuscript.
We would like to thank all of the women who participated in this study.
This work was supported by funding from NIH/NCI (R01CA246592 to A.T. Toriola) and Susan G. Komen Foundation (CCR15332379 to A.T. Toriola). K.R. Getz was supported by T32CA190194.
The content is solely the responsibility of the authors and does not represent the official view of the NIH.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conclusions and opinions are those of the individual authors and do not necessarily reflect the policies or views of EHP Publishing or the National Institute of Environmental Health Sciences.
References
- 1.Boyd NF, Rommens JM, Vogt K, Lee V, Hopper JL, Yaffe MJ, et al. 2005. Mammographic breast density as an intermediate phenotype for breast cancer. Lancet Oncol 6(10):798–808, PMID: 16198986, 10.1016/S1470-2045(05)70390-9. [DOI] [PubMed] [Google Scholar]
- 2.Boyd NF, Guo H, Martin LJ, Sun L, Stone J, Fishell E, et al. 2007. Mammographic density and the risk and detection of breast cancer. N Engl J Med 356(3):227–236, PMID: 17229950, 10.1056/NEJMoa062790. [DOI] [PubMed] [Google Scholar]
- 3.McCormack VA, dos Santos Silva I. 2006. Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev 15(6):1159–1169, PMID: 16775176, 10.1158/1055-9965.EPI-06-0034. [DOI] [PubMed] [Google Scholar]
- 4.Ursin G, Lillie EO, Lee E, Cockburn M, Schork NJ, Cozen W, et al. 2009. The relative importance of genetics and environment on mammographic density. Cancer Epidemiol Biomarkers Prev 18(1):102–112, PMID: 19124487, 10.1158/1055-9965.EPI-07-2857. [DOI] [PubMed] [Google Scholar]
- 5.Moore JX, Han Y, Appleton C, Colditz G, Toriola AT. 2020. Determinants of mammographic breast density by race among a large screening population. JNCI Cancer Spectr 4(2):pkaa010, PMID: 32373777, 10.1093/jncics/pkaa010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yaghjyan L, Arao R, Brokamp C, O’Meara ES, Sprague BL, Ghita G, et al. 2017. Association between air pollution and mammographic breast density in the breast cancer surveilance consortium. Breast Cancer Res 19(1):36, PMID: 28381271, 10.1186/s13058-017-0828-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.DuPre NC, Hart JE, Bertrand KA, Kraft P, Laden F, Tamimi RM. 2017. Residential particulate matter and distance to roadways in relation to mammographic density: results from the nurses’ health studies. Breast Cancer Res 19(1):124, PMID: 29169389, 10.1186/s13058-017-0915-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rusiecki JA, Denic-Roberts H, Byrne C, Cash J, Raines CF, Brinton LA, et al. 2020. Serum concentrations of DDE, PCBs, and other persistent organic pollutants and mammographic breast density in Triana, Alabama, a highly exposed population. Environ Res 182:109068, PMID: 31918312, 10.1016/j.envres.2019.109068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Diorio C, Dumas I, Sandanger TM, Ayotte P. 2013. Levels of circulating polychlorinated biphenyls and mammographic breast density. Anticancer Res 33(12):5483–5489, PMID: 24324085. [PubMed] [Google Scholar]
- 10.Sprague BL, Trentham-Dietz A, Hedman CJ, Wang J, Hemming JD, Hampton JM, et al. 2013. Circulating serum xenoestrogens and mammographic breast density. Breast Cancer Res 15(3):R45, PMID: 23710608, 10.1186/bcr3432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lee E, Kinninger A, Ursin G, Tseng C, Hurley S, Wang M, et al. 2020. Serum levels of commonly detected persistent organic pollutants and per- and polyfluoroalkyl substances (PFASs) and mammographic density in postmenopausal women. Int J Environ Res Public Health 17(2):606, PMID: 31963577, 10.3390/ijerph17020606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Savvaides T, Koelmel JP, Zhou Y, Lin EZ, Stelben P, Aristizabal-Henao JJ, et al. 2021. Prevalence and implications of per- and polyfluoroalkyl substances (PFAS) in settled dust. Curr Environ Health Rep 8(4):323–335, PMID: 34985714, 10.1007/s40572-021-00326-4. [DOI] [PubMed] [Google Scholar]
- 13.Prevedouros K, Cousins IT, Buck RC, Korzeniowski SH. 2006. Sources, fate and transport of perfluorocarboxylates. Environ Sci Technol 40(1):32–44, PMID: 16433330, 10.1021/es0512475. [DOI] [PubMed] [Google Scholar]
- 14.Tittlemier SA, Pepper K, Seymour C, Moisey J, Bronson R, Cao XL, et al. 2007. Dietary exposure of Canadians to perfluorinated carboxylates and perfluorooctane sulfonate via consumption of meat, fish, fast foods, and food items prepared in their packaging. J Agric Food Chem 55(8):3203–3210, PMID: 17381114, 10.1021/jf0634045. [DOI] [PubMed] [Google Scholar]
- 15.Sunderland EM, Hu XC, Dassuncao C, Tokranov AK, Wagner CC, Allen JG. 2019. A review of the pathways of human exposure to poly- and perfluoroalkyl substances (PFASs) and present understanding of health effects. J Expo Sci Environ Epidemiol 29(2):131–147, PMID: 30470793, 10.1038/s41370-018-0094-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Barbo N, Stoiber T, Naidenko OV, Andrews DQ. 2023. Locally caught freshwater fish across the United States are likely a significant source of exposure to PFOS and other perfluorinated compounds. Environ Res 220:115165, PMID: 36584847, 10.1016/j.envres.2022.115165. [DOI] [PubMed] [Google Scholar]
- 17.Ruffle B, Vedagiri U, Bogdan D, Maier M, Schwach C, Murphy-Hagan C. 2020. Perfluoroalkyl substances in U.S. market basket fish and shellfish. Environ Res 190:109932, PMID: 32798898, 10.1016/j.envres.2020.109932. [DOI] [PubMed] [Google Scholar]
- 18.von Stackelberg K, Li M, Sunderland E. 2017. Results of a national survey of high-frequency fish consumers in the United States. Environ Res 158:126–136, PMID: 28623747, 10.1016/j.envres.2017.05.042. [DOI] [PubMed] [Google Scholar]
- 19.Kannan K, Corsolini S, Falandysz J, Fillmann G, Kumar KS, Loganathan BG, et al. 2004. Perfluorooctanesulfonate and related fluorochemicals in human blood from several countries. Environ Sci Technol 38(17):4489–4495, PMID: 15461154, 10.1021/es0493446. [DOI] [PubMed] [Google Scholar]
- 20.Cariou R, Veyrand B, Yamada A, Berrebi A, Zalko D, Durand S, et al. 2015. Perfluoroalkyl acid (PFAA) levels and profiles in breast milk, maternal and cord serum of French women and their newborns. Environ Int 84:71–81, PMID: 26232143, 10.1016/j.envint.2015.07.014. [DOI] [PubMed] [Google Scholar]
- 21.Zahm S, Bonde JP, Chiu WA, Hoppin J, Kanno J, Abdallah M, et al. 2023. Carcinogenicity of perfluorooctanoic acid and perfluorooctanesulfonic acid. Lancet Oncol 25(1):16–17, PMID: 38043561, 10.1016/S1470-2045(23)00622-8. [DOI] [PubMed] [Google Scholar]
- 22.Jiang H, Liu H, Liu G, Yu J, Liu N, Jin Y, et al. 2022. Associations between polyfluoroalkyl substances exposure and breast cancer: a meta-analysis. Toxics 10(6):318, PMID: 35736926, 10.3390/toxics10060318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chang VC, Rhee J, Berndt SI, Moore SC, Freedman ND, Jones RR, et al. 2023. Serum perfluorooctane sulfonate and perfluorooctanoate and risk of postmenopausal breast cancer according to hormone receptor status: an analysis in the prostate, lung, colorectal and ovarian cancer screening trial. Int J Cancer 153(4):775–782, PMID: 36843273, 10.1002/ijc.34487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mancini FR, Cano-Sancho G, Gambaretti J, Marchand P, Boutron-Ruault MC, Severi G, et al. 2020. Perfluorinated alkylated substances serum concentration and breast cancer risk: evidence from a nested case-control study in the French E3N cohort. Int J Cancer 146(4):917–928, PMID: 31008526, 10.1002/ijc.32357. [DOI] [PubMed] [Google Scholar]
- 25.Tsai M-S, Chang S-H, Kuo W-H, Kuo C-H, Li S-Y, Wang M-Y, et al. 2020. A case-control study of perfluoroalkyl substances and the risk of breast cancer in Taiwanese women. Environ Int 142:105850, PMID: 32580117, 10.1016/j.envint.2020.105850. [DOI] [PubMed] [Google Scholar]
- 26.Guo P, Furnary T, Vasiliou V, Yan Q, Nyhan K, Jones DP, et al. 2022. Non-targeted metabolomics and associations with per- and polyfluoroalkyl substances (PFAS) exposure in humans: a scoping review. Environ Int 162:107159, PMID: 35231839, 10.1016/j.envint.2022.107159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wang R, Li B, Lam SM, Shui G. 2020. Integration of lipidomics and metabolomics for in-depth understanding of cellular mechanism and disease progression. J Genet Genomics 47(2):69–83, PMID: 32178981, 10.1016/j.jgg.2019.11.009. [DOI] [PubMed] [Google Scholar]
- 28.Petrick LM, Wolff MS, Barupal D, Teitelbaum SL. 2022. Comparison of untargeted and targeted perfluoroalkyl acids measured in adolescent girls. Chemosphere 290:133303, PMID: 34921852, 10.1016/j.chemosphere.2021.133303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Salihovic S, Dunder L, Lind M, Lind L. 2024. Assessing the performance of a targeted absolute quantification isotope dilution liquid chromatograhy tandem mass spectrometry assay versus a commercial nontargeted relative quantification assay for detection of three major perfluoroalkyls in human blood. J Mass Spectrom 59(2):e4999, PMID: 38263897, 10.1002/jms.4999. [DOI] [PubMed] [Google Scholar]
- 30.Mora AM, Oken E, Rifas-Shiman SL, Webster TF, Gillman MW, Calafat AM, et al. 2017. Prenatal exposure to perfluoroalkyl substances and adiposity in early and mid-childhood. Environ Health Perspect 125(3):467–473, PMID: 27352404, 10.1289/EHP246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zhang M, Rifas-Shiman SL, Aris IM, Fleisch AF, Lin PD, Nichols AR, et al. 2023. Associations of prenatal per- and polyfluoroalkyl substance (PFAS) exposures with offspring adiposity and body composition at 16–20 years of age: project viva. Environ Health Perspect 131(12):127002, PMID: 38054701, 10.1289/EHP12597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Pinney SM, Fassler CS, Windham GC, Herrick RL, Xie C, Kushi LH, et al. 2023. Exposure to perfluoroalkyl substances and associations with pubertal onset and serum reproductive hormones in a longitudinal study of young girls in greater Cincinnati and the San Francisco Bay area. Environ Health Perspect 131(9):097009, PMID: 37751325, 10.1289/EHP11811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Alimujiang A, Appleton C, Colditz GA, Toriola AT. 2017. Adiposity during early adulthood, changes in adiposity during adulthood, attained adiposity, and mammographic density among premenopausal women. Breast Cancer Res Treat 166(1):197–206, PMID: 28702890, 10.1007/s10549-017-4384-4. [DOI] [PubMed] [Google Scholar]
- 34.Getz KR, Jeon MS, Luo C, Luo J, Toriola AT. 2023. Lipidome of mammographic breast density in premenopausal women. Breast Cancer Res 25(1):121, PMID: 37814330, 10.1186/s13058-023-01725-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Toriola AT, Appleton CM, Zong X, Luo J, Weilbaecher K, Tamimi RM, et al. 2018. Circulating receptor activator of nuclear factor-kappaB (RANK), RANK ligand (RANKL), and mammographic density in premenopausal women. Cancer Prev Res (Phila) 11(12):789–796, PMID: 30352839, 10.1158/1940-6207.CAPR-18-0199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Stunkard AJ, Sorensen T, Schulsinger F. 1983. Use of the danish adoption register for the study of obesity and thinness. Res Publ Assoc Res Nerv Ment Dis 60:115–120, PMID: 6823524. [PubMed] [Google Scholar]
- 37.Song M, Hu FB, Wu K, Must A, Chan AT, Willett WC, et al. 2016. Trajectory of body shape in early and Middle life and all cause and cause specific mortality: results from two prospective US cohort studies. BMJ 353:i2195, PMID: 27146280, 10.1136/bmj.i2195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Alimujiang A, Imm KR, Appleton CM, Colditz GA, Berkey CS, Toriola AT. 2018. Adiposity at age 10 and mammographic density among premenopausal women. Cancer Prev Res (Phila) 11(5):287–294, PMID: 29500187, 10.1158/1940-6207.CAPR-17-0309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Collet TH, Sonoyama T, Henning E, Keogh JM, Ingram B, Kelway S, et al. 2017. A metabolomic signature of acute caloric restriction. J Clin Endocrinol Metab 102(12):4486–4495, PMID: 29029202, 10.1210/jc.2017-01020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Evans AM, Bridgewater B, Liu Q, Mitchell M, Robinson R, Dai H, et al. 2014. High resolution mass spectrometry improves data quantity and quality as compared to unit mass resolution mass spectrometry in high-throughput profiling metabolomics. Metabolomics 4(2):1000132, 10.4172/2153-0769.1000132. [DOI] [Google Scholar]
- 41.Kato K, Kalathil AA, Patel AM, Ye X, Calafat AM. 2018. Per- and polyfluoroalkyl substances and fluorinated alternatives in urine and serum by on-line solid phase extraction-liquid chromatography-tandem mass spectrometry. Chemosphere 209:338–345, PMID: 29935462, 10.1016/j.chemosphere.2018.06.085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Volpara Solutions. 2013. Volpara Density User Manual Version 1.5. Wellington, New Zealand: Volpara Solutions from Matakina Technology. [Google Scholar]
- 43.Johnson WE, Li C, Rabinovic A. 2007. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 8(1):118–127, PMID: 16632515, 10.1093/biostatistics/kxj037. [DOI] [PubMed] [Google Scholar]
- 44.Fortin J-P, Parker D, Tunç B, Watanabe T, Elliott MA, Ruparel K, et al. 2017. Harmonization of multi-site diffusion tensor imaging data. Neuroimage 161:149–170, PMID: 28826946, 10.1016/j.neuroimage.2017.08.047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Leek JT, Johnson WE, Parker HS, Jaffe AE, Storey JD. 2012. The sva package for removing batch effects and other unwanted variation in high-throughput experiments. Bioinformatics 28(6):882–883, PMID: 22257669, 10.1093/bioinformatics/bts034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Yu Y, Zhang N, Mai Y, Ren L, Chen Q, Cao Z, et al. 2023. Correcting batch effects in large-scale multiomics studies using a reference-material-based ratio method. Genome Biol 24(1):201, PMID: 37674217, 10.1186/s13059-023-03047-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wei R, Wang J, Su M, Jia E, Chen S, Chen T, et al. 2018. Missing value imputation approach for mass spectrometry-based metabolomics data. Sci Rep 8(1):663, PMID: 29330539, 10.1038/s41598-017-19120-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Petrazzini BO, Naya H, Lopez-Bello F, Vazquez G, Spangenberg L. 2021. Evaluation of different approaches for missing data imputation on features associated to genomic data. BioData Min 14(1):44, PMID: 34479616, 10.1186/s13040-021-00274-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Azur MJ, Stuart EA, Frangakis C, Leaf PJ. 2011. Multiple imputation by chained equations: what is it and how does it work? Int J Methods Psychiatr Res 20(1):40–49, PMID: 21499542, 10.1002/mpr.329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.van Buuren S, Groothuis-Oudshoorn K. 2011. MICE: multivariate imputation by chained equations in R. J Stat Soft 45(3):1–67, 10.18637/jss.v045.i03. [DOI] [Google Scholar]
- 51.Cabrera SM, Bright GM, Frane JW, Blethen SL, Lee PA. 2014. Age of thelarche and menarche in contemporary US females: a cross-sectional analysis. J Pediatr Endocrinol Metab 27(1–2):47–51, PMID: 23959659, 10.1515/jpem-2013-0286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Agency for Toxic Substances and Disease Registry. 2024. PFAS in the U.S. Population. https://www.atsdr.cdc.gov/pfas/health-effects/us-population.html#:∼:text=Since%202002%2C%20the%20production%20and,have%20gone%20down%20as%20well [accessed 15 January 2024].
- 53.Bobb JF, Valeri L, Claus Henn B, Christiani DC, Wright RO, Mazumdar M, et al. 2015. Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics 16(3):493–508, PMID: 25532525, 10.1093/biostatistics/kxu058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Bobb JF, Claus Henn B, Valeri L, Coull BA. 2018. Statistical software for analyzing the health effects of multiple concurrent exposures via Bayesian kernel machine regression. Environ Health 17(1):67, PMID: 30126431, 10.1186/s12940-018-0413-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Pierozan P, Cattani D, Karlsson O. 2022. Tumorigenic activity of alternative per- and polyfluoroalkyl substances (PFAS): mechanistic in vitro studies. Sci Total Environ 808:151945, PMID: 34843762, 10.1016/j.scitotenv.2021.151945. [DOI] [PubMed] [Google Scholar]
- 56.Pierozan P, Kosnik M, Karlsson O. 2023. High-content analysis shows synergistic effects of low perfluorooctanoic acid (PFOS) and perfluorooctane sulfonic acid (PFOA) mixture concentrations on human breast epithelial cell carcinogenesis. Environ Int 172:107746, PMID: 36731186, 10.1016/j.envint.2023.107746. [DOI] [PubMed] [Google Scholar]
- 57.Liu H, Pan Y, Jin S, Li Y, Zhao L, Sun X, et al. 2020. Associations of per-/polyfluoroalkyl substances with glucocorticoids and progestogens in newborns. Environ Int 140:105636, PMID: 32474218, 10.1016/j.envint.2020.105636. [DOI] [PubMed] [Google Scholar]
- 58.Noh JJ, Maskarinec G, Pagano I, Cheung LW, Stanczyk FZ. 2006. Mammographic densities and circulating hormones: a cross-sectional study in premenopausal women. Breast 15(1):20–28, PMID: 16000251, 10.1016/j.breast.2005.04.014. [DOI] [PubMed] [Google Scholar]
- 59.Lopez-Rodriguez D, Franssen D, Heger S, Parent AS. 2021. Endocrine-disrupting chemicals and their effects on puberty. Best Pract Res Clin Endocrinol Metab 35(5):101579, PMID: 34563408, 10.1016/j.beem.2021.101579. [DOI] [PubMed] [Google Scholar]
- 60.Lucaccioni L, Trevisani V, Marrozzini L, Bertoncelli N, Predieri B, Lugli L, et al. 2020. Endocrine-disrupting chemicals and their effects during female puberty: a review of current evidence. Int J Mol Sci 21(6):2078, PMID: 32197344, 10.3390/ijms21062078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Olsen GW, Burris JM, Ehresman DJ, Froehlich JW, Seacat AM, Butenhoff JL, et al. 2007. Half-life of serum elimination of perfluorooctanesulfonate, perfluorohexanesulfonate, and perfluorooctanoate in retired fluorochemical production workers. Environ Health Perspect 115(9):1298–1305, PMID: 17805419, 10.1289/ehp.10009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Domazet SL, Grontved A, Timmermann AG, Nielsen F, Jensen TK. 2016. Longitudinal associations of exposure to perfluoroalkylated substances in childhood and adolescence and indicators of adiposity and glucose metabolism 6 and 12 years later: the European youth heart study. Diabetes Care 39(10):1745–1751, PMID: 27489335, 10.2337/dc16-0269. [DOI] [PubMed] [Google Scholar]
- 63.Schoemaker MJ, Jones ME, Allen S, Hoare J, Ashworth A, Dowsett M, et al. 2017. Childhood body size and pubertal timing in relation to adult mammographic density phenotype. Breast Cancer Res 19(1):13, PMID: 28173872, 10.1186/s13058-017-0804-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Hojeij B, Rousian M, Sinclair KD, Dinnyes A, Steegers-Theunissen RPM, Schoenmakers S. 2023. Periconceptional biomarkers for maternal obesity: a systematic review. Rev Endocr Metab Disord 24(2):139–175, PMID: 36520252, 10.1007/s11154-022-09762-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Bartha I, Joumady I, Cuerva M, Bartha JL. 2023. The effect of maternal obesity and lipid profile on first-trimester serum progesterone levels. Am J Obstet Gynecol MFM 5(7):100959, PMID: 37030509, 10.1016/j.ajogmf.2023.100959. [DOI] [PubMed] [Google Scholar]
- 66.Houghton LC, Jung S, Troisi R, LeBlanc ES, Snetselaar LG, Hylton NM, et al. 2019. Pubertal timing and breast density in young women: a prospective cohort study. Breast Cancer Res 21(1):122, PMID: 31727127, 10.1186/s13058-019-1209-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Chang CJ, Ish JL, Chang VC, Daniel M, Jones RR, White AJ. 2024. Exposure to per- and polyfluoroalkyl substances and breast cancer risk: a systematic review and meta-analysis of epidemiologic studies. Am J Epidemiol 193(8):1182–1196, PMID: 38400646, 10.1093/aje/kwae010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Hurley S, Goldberg D, Wang M, Park JS, Petreas M, Bernstein L, et al. 2018. Breast cancer risk and serum levels of per- and poly-fluoroalkyl substances: a case-control study nested in the California teachers study. Environ Health 17(1):83, PMID: 30482205, 10.1186/s12940-018-0426-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Gabrielson M, Azam S, Hardell E, Holm M, Ubhayasekera KA, Eriksson M, et al. 2020. Hormonal determinants of mammographic density and density change. Breast Cancer Res 22(1):95, PMID: 32847607, 10.1186/s13058-020-01332-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Colditz GA, Frazier AL. 1995. Models of breast cancer show that risk is set by events of early life: prevention efforts must shift focus. Cancer Epidemiol Biomarkers Prev 4(5):567–571, PMID: 7549816. [PubMed] [Google Scholar]
- 71.Han Y, Moore JX, Colditz GA, Toriola AT. 2022. Family history of breast cancer and mammographic breast density in premenopausal women. JAMA Netw Open 5(2):e2148983, PMID: 35175341, 10.1001/jamanetworkopen.2021.48983. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.