

Abstract
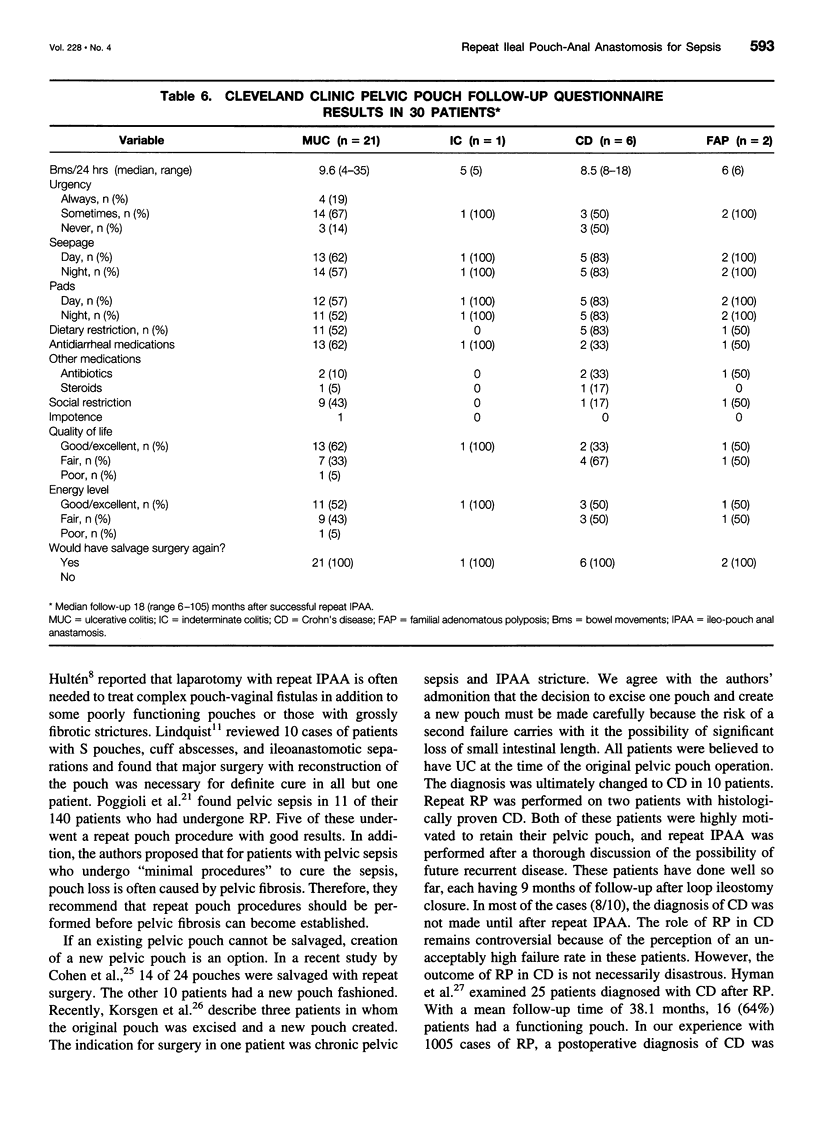
OBJECTIVE: To evaluate the outcome of repeat ileal pouch-anal anastomosis (IPAA) for septic complications of pelvic pouch surgery; to assess the relationship between diagnosis and outcome; to assess quality of life after surgery. SUMMARY BACKGROUND DATA: Pelvic and perineal sepsis due to ileal pouch-anal anastomotic leaks frequently results in pouch loss. Many surgeons believe that pelvic sepsis and/or dense pelvic fibrosis makes salvage surgery unsafe or that pouches salvaged under these circumstances may not function well. As a result, there are few studies of pouch salvage procedures for septic indications. METHODS: The authors reviewed records of Cleveland Clinic Foundation patients who had undergone repeat IPAA surgery after septic complications from previous pelvic pouch surgery and who had completed at least 6 months of follow-up. Final diagnoses included ulcerative colitis (n = 22), Crohn's disease (n = 10), indeterminate colitis (n = 1), and familial polyposis (n = 2). Patients with functioning pouches were interviewed about functional problems and quality of life using an in-house questionnaire and the validated SF-36 Health Survey. RESULTS: Of 35 patients, 30 (86%) had a functioning pouch 6 months after repeat IPAA. In 4 patients, complications led to pouch removal or fecal diversion. One patient declined stoma closure. Of the patients with mucosal ulcerative colitis (MUC), 95% (21/22) had a functioning pouch 6 months after surgery. For patients with Crohn's disease (CD) 60% (6/10) have maintained a functioning pouch. Of the 30 patients with functioning pouches, 17 (57%) rated their quality of life as either "good" or "excellent," the remaining 13 (43%) selected "fair" or "poor." All said they would choose repeat IPAA surgery again. An SF-36 Health Survey completed by all patients with a functioning pouch at follow-up showed a mean physical component scale of 46.4 and a mean mental component scale of 47.6, scores well within the normal limit. CONCLUSIONS: Repeat IPAA can often salvage pelvic pouches in patients with MUC who suffer major chronic perianastomotic and pelvic sepsis. Patients who had successful repeat IPAA surgery often report functional problems but would still choose to have the surgery again. For patients with CD, ultimate pouch excision or fecal diversion have been required in 40% indicating a guarded prognosis for these patients. Data on the success of the procedure for patients with indeterminate colitis and familial adenomatous polyposis were inconclusive because of small sample sizes.
Full text
PDF


Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cohen Z., Smith D., McLeod R. Reconstructive surgery for pelvic pouches. World J Surg. 1998 Apr;22(4):342–346. [PubMed] [Google Scholar]
- Fazio V. W., Tjandra J. J. Pouch advancement and neoileoanal anastomosis for anastomotic stricture and anovaginal fistula complicating restorative proctocolectomy. Br J Surg. 1992 Jul;79(7):694–696. doi: 10.1002/bjs.1800790734. [DOI] [PubMed] [Google Scholar]
- Fazio V. W., Ziv Y., Church J. M., Oakley J. R., Lavery I. C., Milsom J. W., Schroeder T. K. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg. 1995 Aug;222(2):120–127. doi: 10.1097/00000658-199508000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleshman J. W., McLeod R. S., Cohen Z., Stern H. Improved results following use of an advancement technique in the treatment of ileoanal anastomotic complications. Int J Colorectal Dis. 1988 Aug;3(3):161–165. doi: 10.1007/BF01648360. [DOI] [PubMed] [Google Scholar]
- Galandiuk S., Scott N. A., Dozois R. R., Kelly K. A., Ilstrup D. M., Beart R. W., Jr, Wolff B. G., Pemberton J. H., Nivatvongs S., Devine R. M. Ileal pouch-anal anastomosis. Reoperation for pouch-related complications. Ann Surg. 1990 Oct;212(4):446–454. doi: 10.1097/00000658-199010000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gemlo B. T., Wong W. D., Rothenberger D. A., Goldberg S. M. Ileal pouch-anal anastomosis. Patterns of failure. Arch Surg. 1992 Jul;127(7):784–787. doi: 10.1001/archsurg.1992.01420070036009. [DOI] [PubMed] [Google Scholar]
- Herbst F., Sielezneff I., Nicholls R. J. Salvage surgery for ileal pouch outlet obstruction. Br J Surg. 1996 Mar;83(3):368–371. doi: 10.1002/bjs.1800830324. [DOI] [PubMed] [Google Scholar]
- Hyman N. H., Fazio V. W., Tuckson W. B., Lavery I. C. Consequences of ileal pouch-anal anastomosis for Crohn's colitis. Dis Colon Rectum. 1991 Aug;34(8):653–657. doi: 10.1007/BF02050345. [DOI] [PubMed] [Google Scholar]
- Korsgen S., Nikiteas N., Ogunbiyi O. A., Keighley M. R. Results from pouch salvage. Br J Surg. 1996 Mar;83(3):372–374. doi: 10.1002/bjs.1800830325. [DOI] [PubMed] [Google Scholar]
- Lee P. Y., Fazio V. W., Church J. M., Hull T. L., Eu K. W., Lavery I. C. Vaginal fistula following restorative proctocolectomy. Dis Colon Rectum. 1997 Jul;40(7):752–759. doi: 10.1007/BF02055426. [DOI] [PubMed] [Google Scholar]
- Lewis W. G., Kuzu A., Sagar P. M., Holdsworth P. J., Johnston D. Stricture at the pouch-anal anastomosis after restorative proctocolectomy. Dis Colon Rectum. 1994 Feb;37(2):120–125. doi: 10.1007/BF02047532. [DOI] [PubMed] [Google Scholar]
- Liljeqvist L., Lindquist K. A reconstructive operation on malfunctioning S-shaped pelvic reservoirs. Dis Colon Rectum. 1985 Jul;28(7):506–511. doi: 10.1007/BF02554098. [DOI] [PubMed] [Google Scholar]
- Lindquist K., Nilsell K., Liljeqvist L. Cuff abscesses and ileoanal anastomotic separations in pelvic pouch surgery. An analysis of possible etiologic factors. Dis Colon Rectum. 1987 May;30(5):355–359. doi: 10.1007/BF02555454. [DOI] [PubMed] [Google Scholar]
- Longo W. E., Oakley J. R., Lavery I. C., Church J. M., Fazio V. W. Outcome of ileorectal anastomosis for Crohn's colitis. Dis Colon Rectum. 1992 Nov;35(11):1066–1071. doi: 10.1007/BF02252997. [DOI] [PubMed] [Google Scholar]
- Marcello P. W., Roberts P. L., Schoetz D. J., Jr, Coller J. A., Murray J. J., Veidenheimer M. C. Long-term results of the ileoanal pouch procedure. Arch Surg. 1993 May;128(5):500–504. doi: 10.1001/archsurg.1993.01420170030003. [DOI] [PubMed] [Google Scholar]
- O'Kelly T. J., Merrett M., Mortensen N. J., Dehn T. C., Kettlewell M. Pouch-vaginal fistula after restorative proctocolectomy: aetiology and management. Br J Surg. 1994 Sep;81(9):1374–1375. doi: 10.1002/bjs.1800810943. [DOI] [PubMed] [Google Scholar]
- Ogunbiyi O. A., Korsgen S., Keighley M. R. Pouch salvage. Long-term outcome. Dis Colon Rectum. 1997 May;40(5):548–552. doi: 10.1007/BF02055376. [DOI] [PubMed] [Google Scholar]
- Ozuner G., Hull T., Lee P., Fazio V. W. What happens to a pelvic pouch when a fistula develops? Dis Colon Rectum. 1997 May;40(5):543–547. doi: 10.1007/BF02055375. [DOI] [PubMed] [Google Scholar]
- Parks A. G., Nicholls R. J. Proctocolectomy without ileostomy for ulcerative colitis. Br Med J. 1978 Jul 8;2(6130):85–88. doi: 10.1136/bmj.2.6130.85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sagar P. M., Dozois R. R., Wolff B. G., Kelly K. A. Disconnection, pouch revision and reconnection of the ileal pouch-anal anastomosis. Br J Surg. 1996 Oct;83(10):1401–1405. doi: 10.1002/bjs.1800831025. [DOI] [PubMed] [Google Scholar]
- Scott N. A., Dozois R. R., Beart R. W., Jr, Pemberton J. H., Wolff B. G., Ilstrup D. M. Postoperative intra-abdominal and pelvic sepsis complicating ileal pouch-anal anastomosis. Int J Colorectal Dis. 1988 Aug;3(3):149–152. doi: 10.1007/BF01648357. [DOI] [PubMed] [Google Scholar]
- Setti-Carraro P., Ritchie J. K., Wilkinson K. H., Nicholls R. J., Hawley P. R. The first 10 years' experience of restorative proctocolectomy for ulcerative colitis. Gut. 1994 Aug;35(8):1070–1075. doi: 10.1136/gut.35.8.1070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Utsunomiya J., Iwama T., Imajo M., Matsuo S., Sawai S., Yaegashi K., Hirayama R. Total colectomy, mucosal proctectomy, and ileoanal anastomosis. Dis Colon Rectum. 1980 Oct;23(7):459–466. doi: 10.1007/BF02987076. [DOI] [PubMed] [Google Scholar]
- Wexner S. D., Rothenberger D. A., Jensen L., Goldberg S. M., Balcos E. G., Belliveau P., Bennett B. H., Buls J. G., Cohen J. M., Kennedy H. L. Ileal pouch vaginal fistulas: incidence, etiology, and management. Dis Colon Rectum. 1989 Jun;32(6):460–465. doi: 10.1007/BF02554497. [DOI] [PubMed] [Google Scholar]