

Abstract
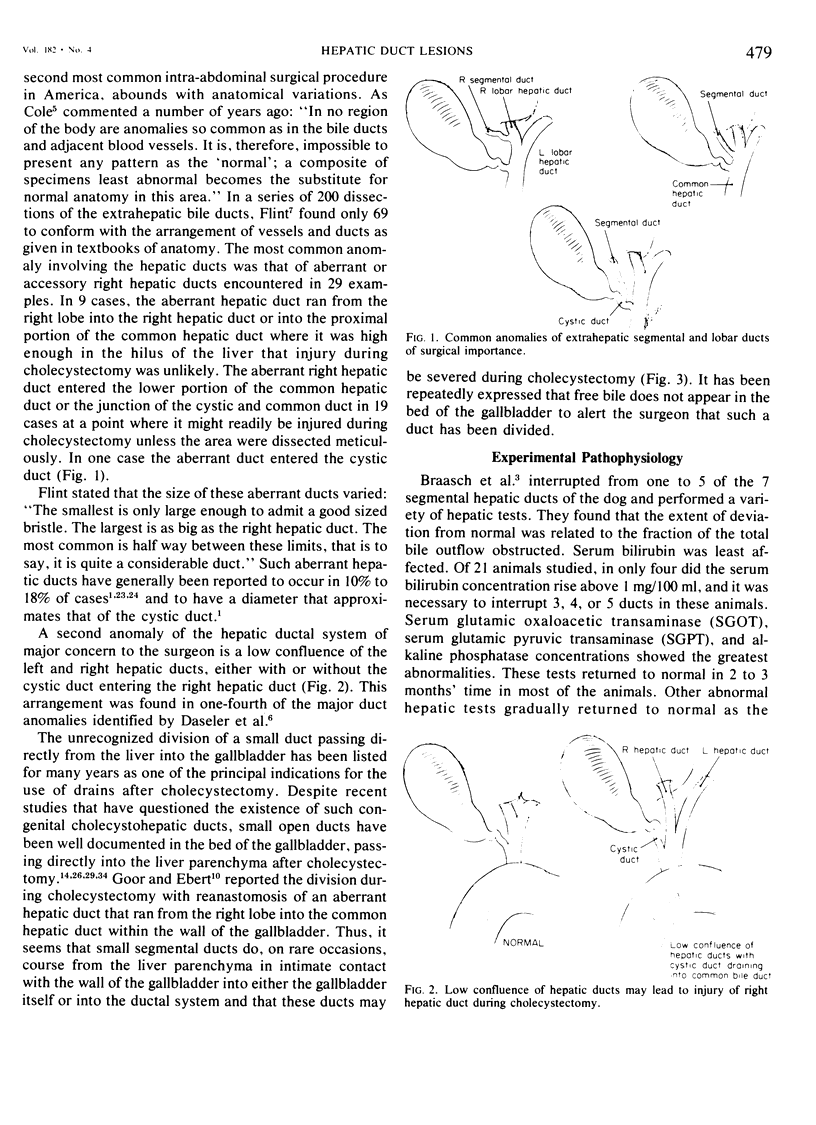
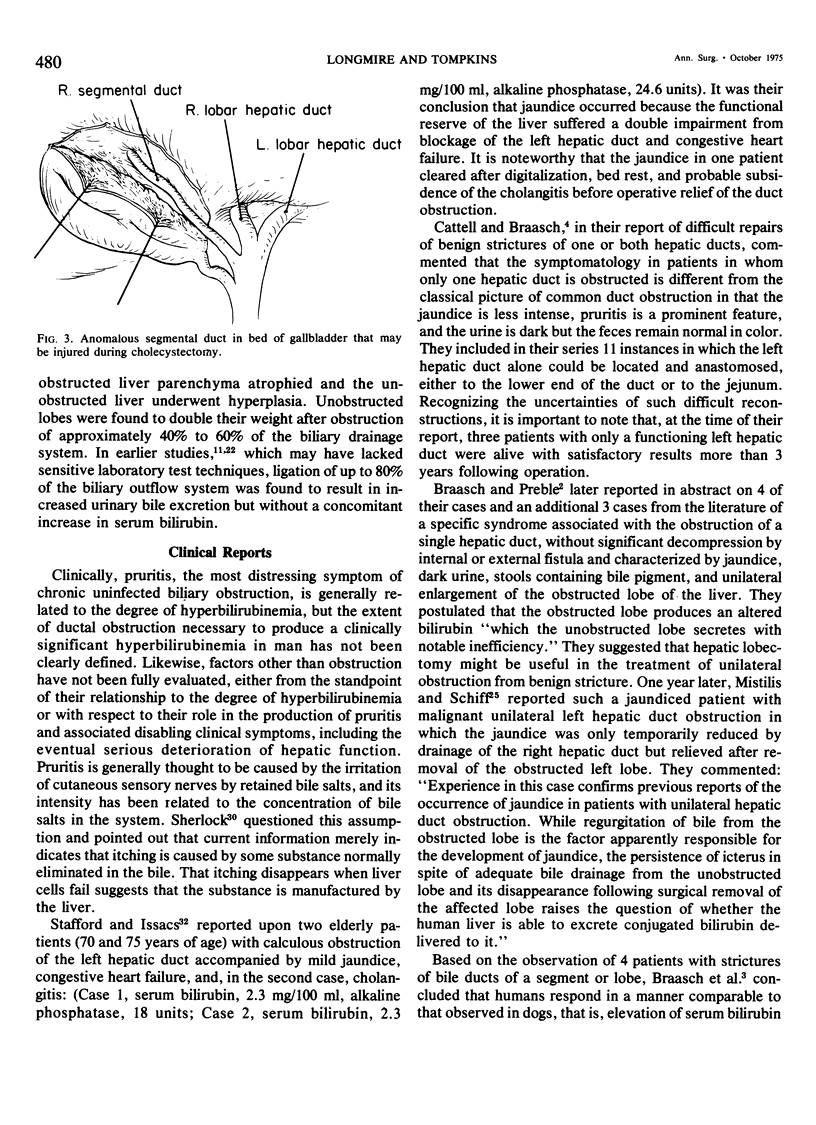
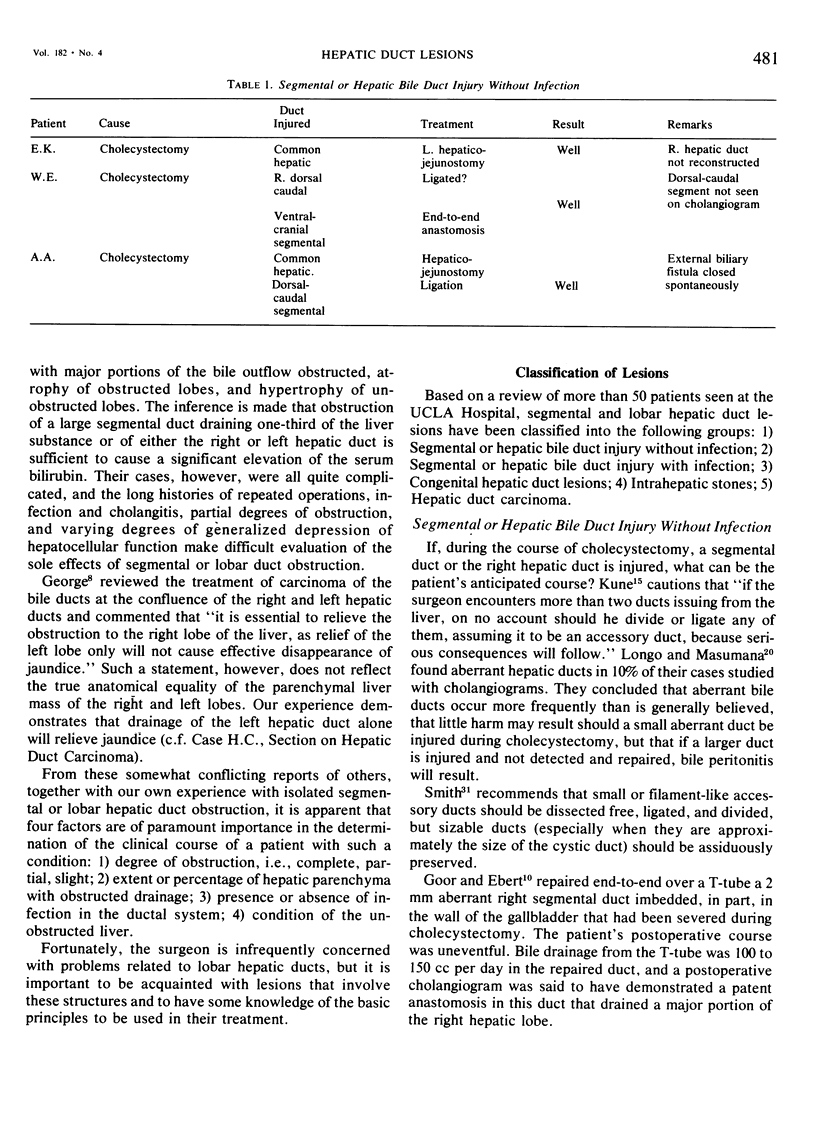
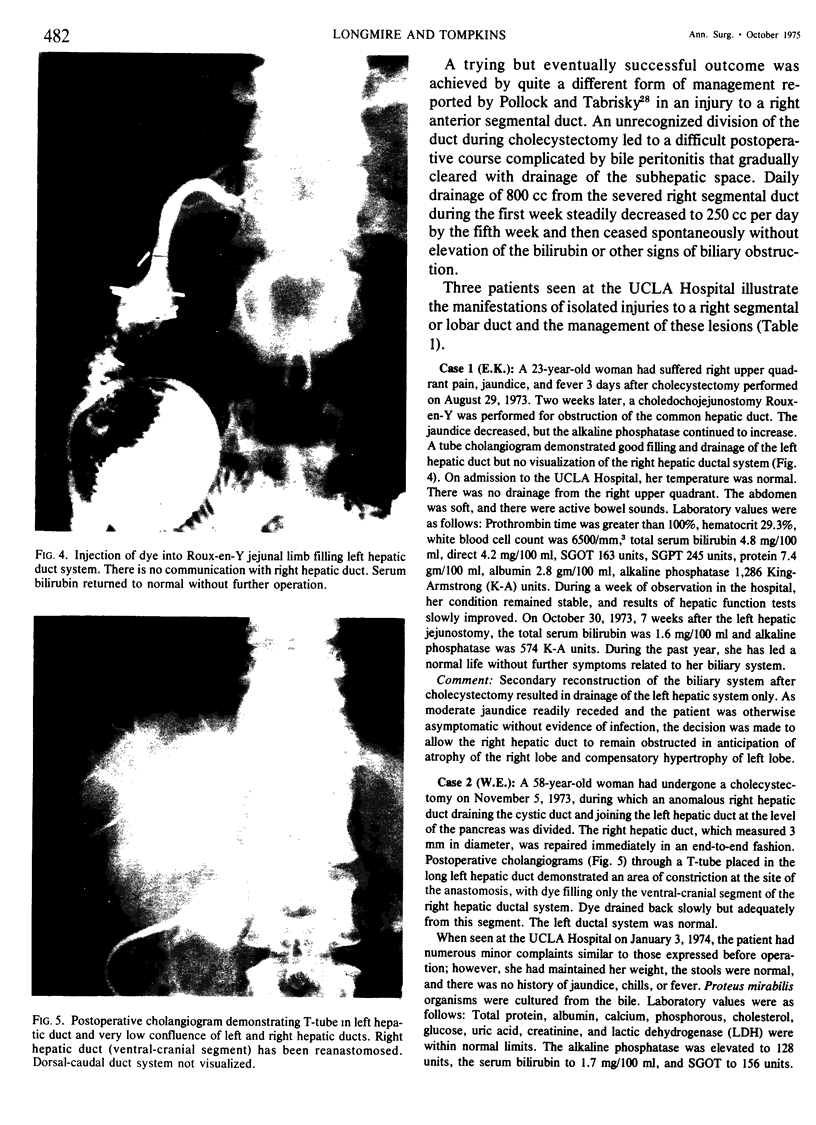
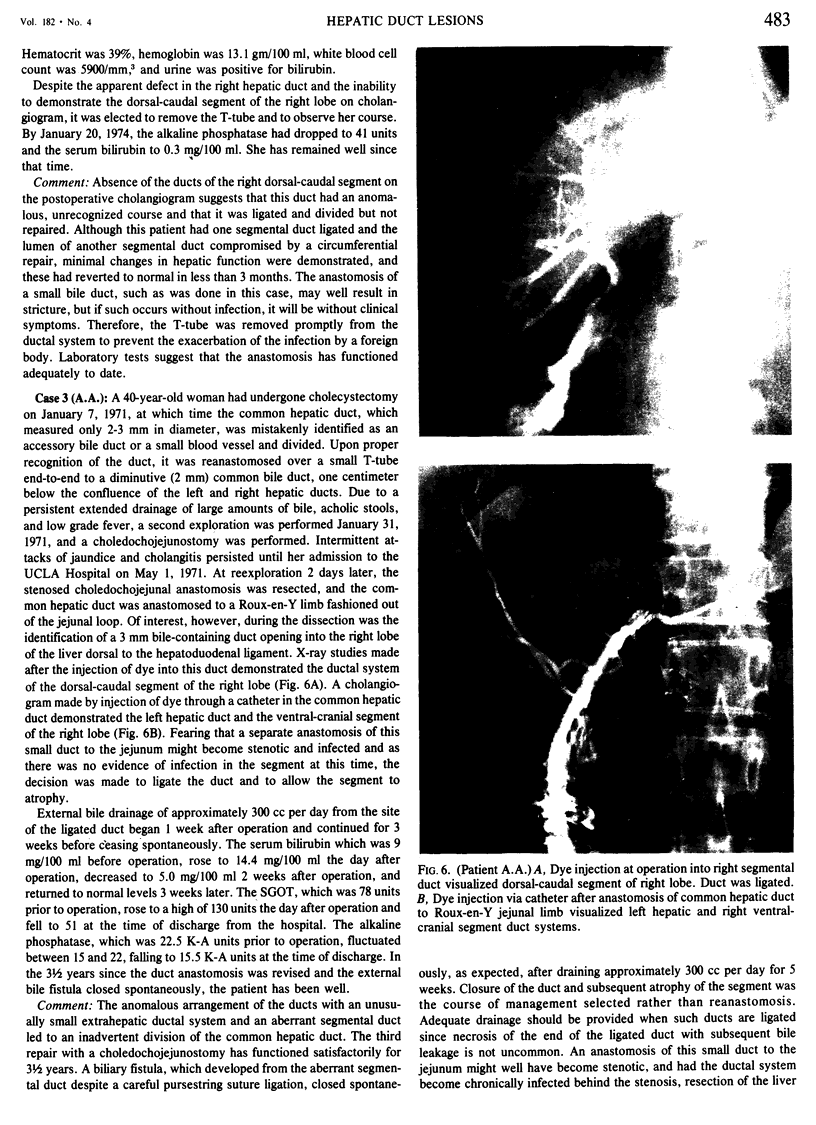
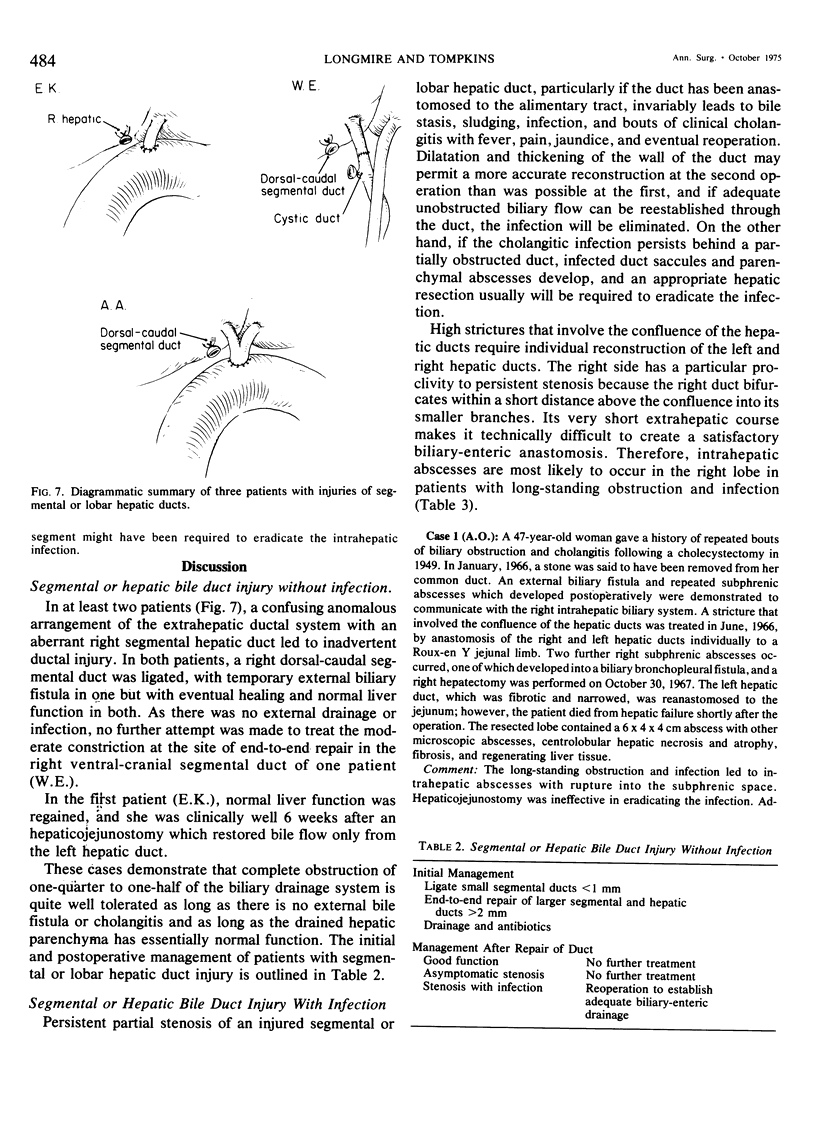
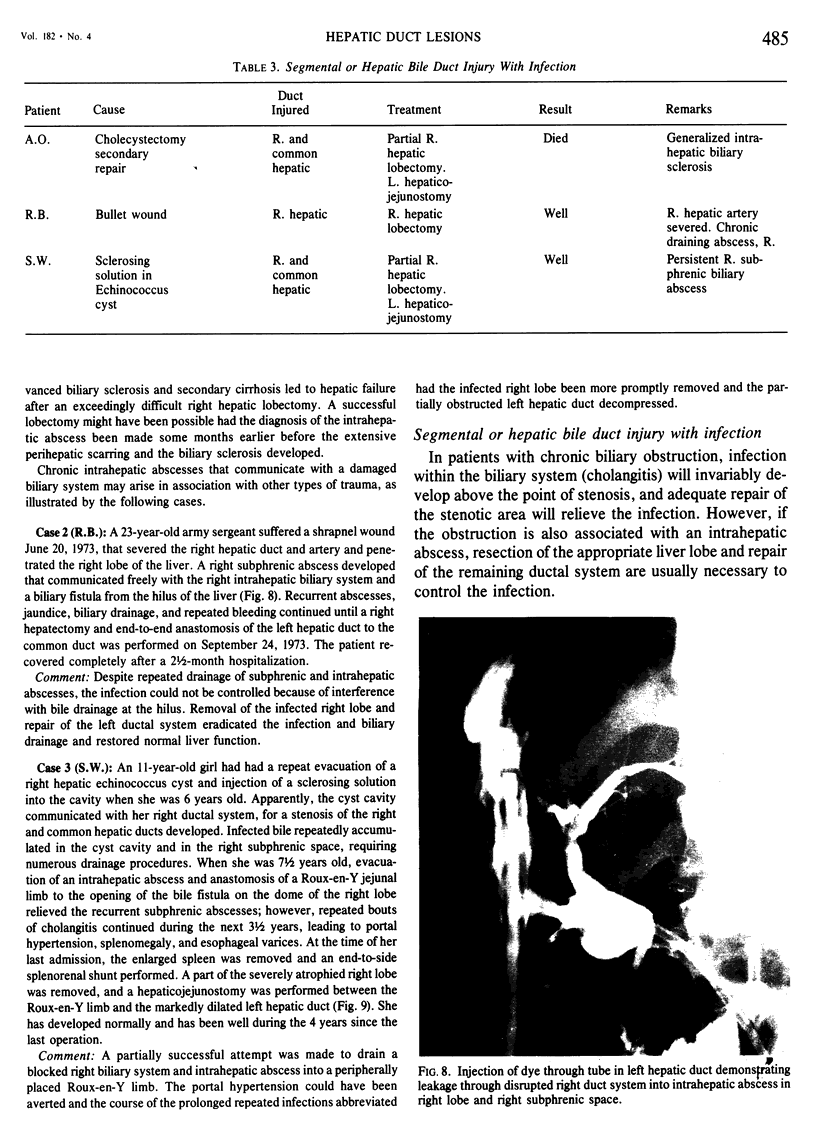
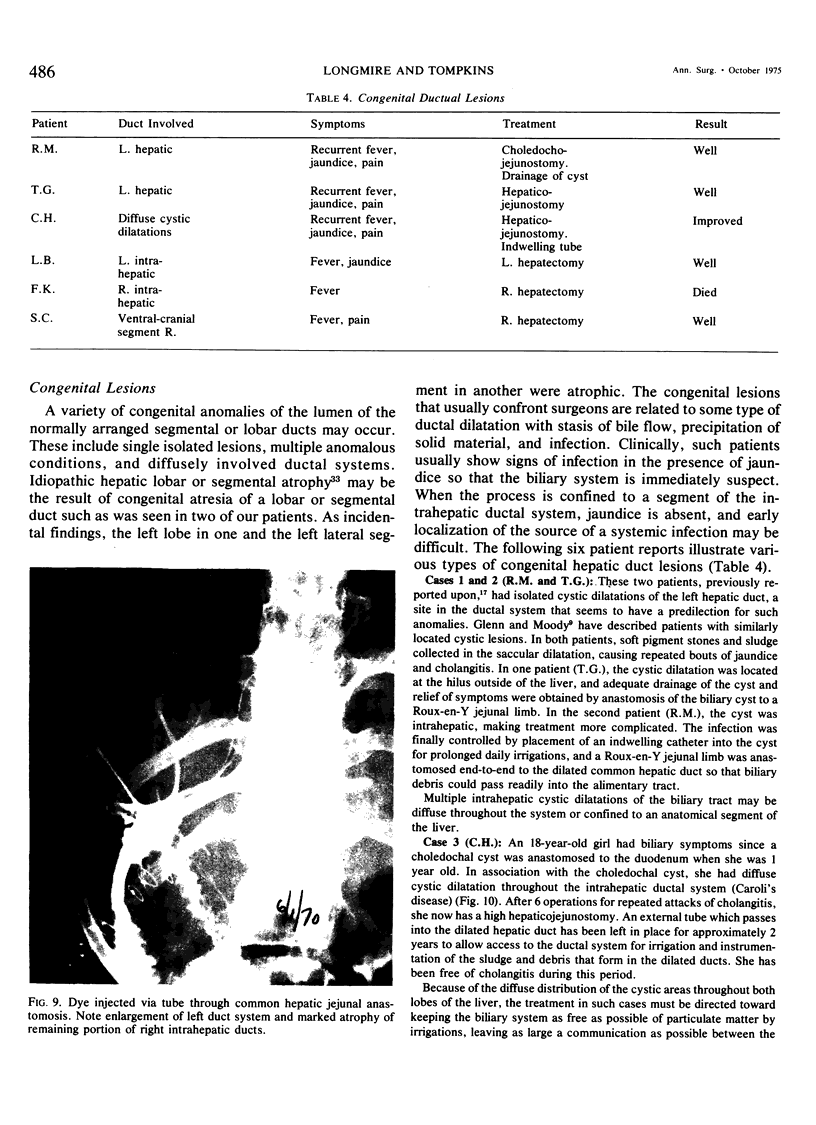
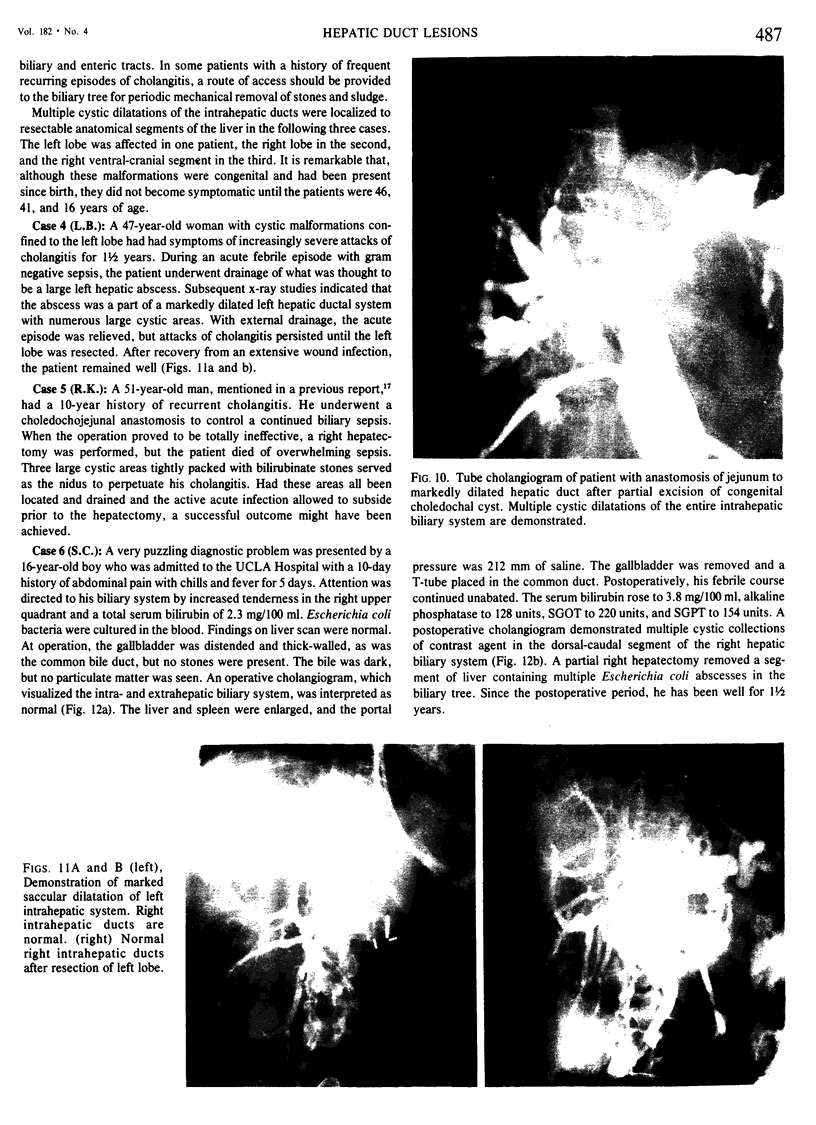
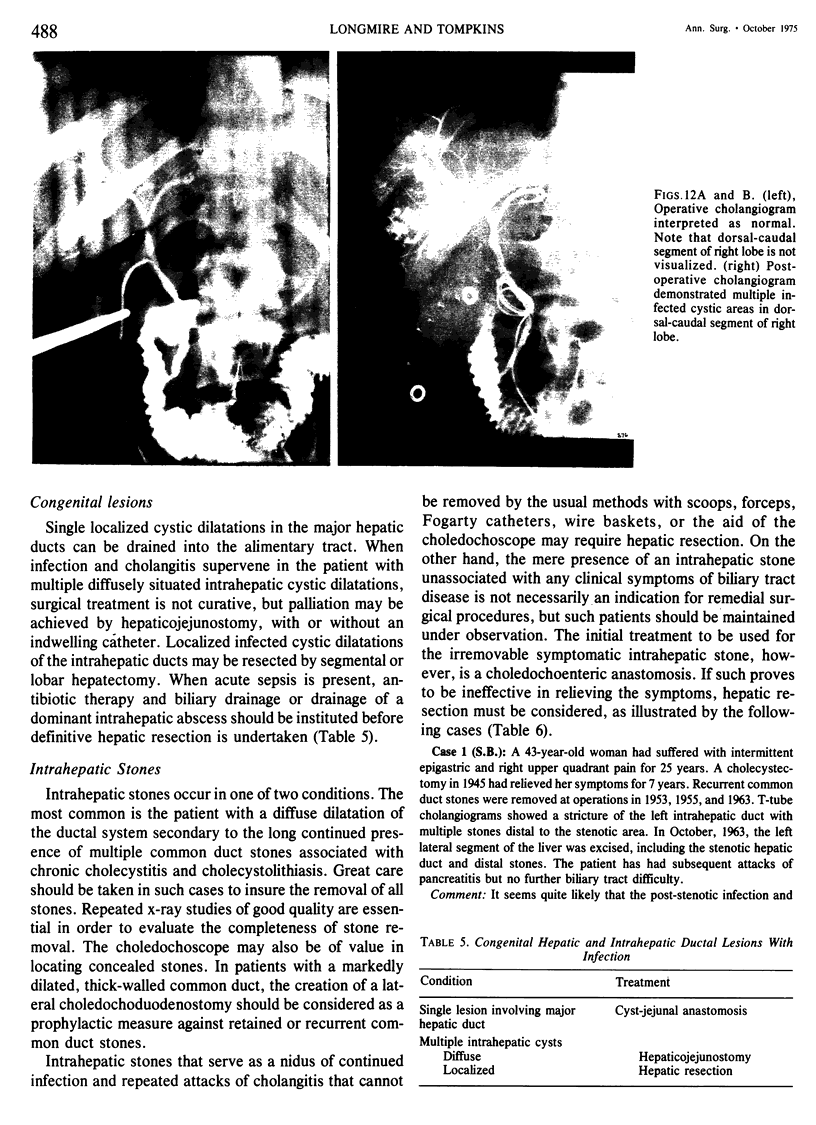
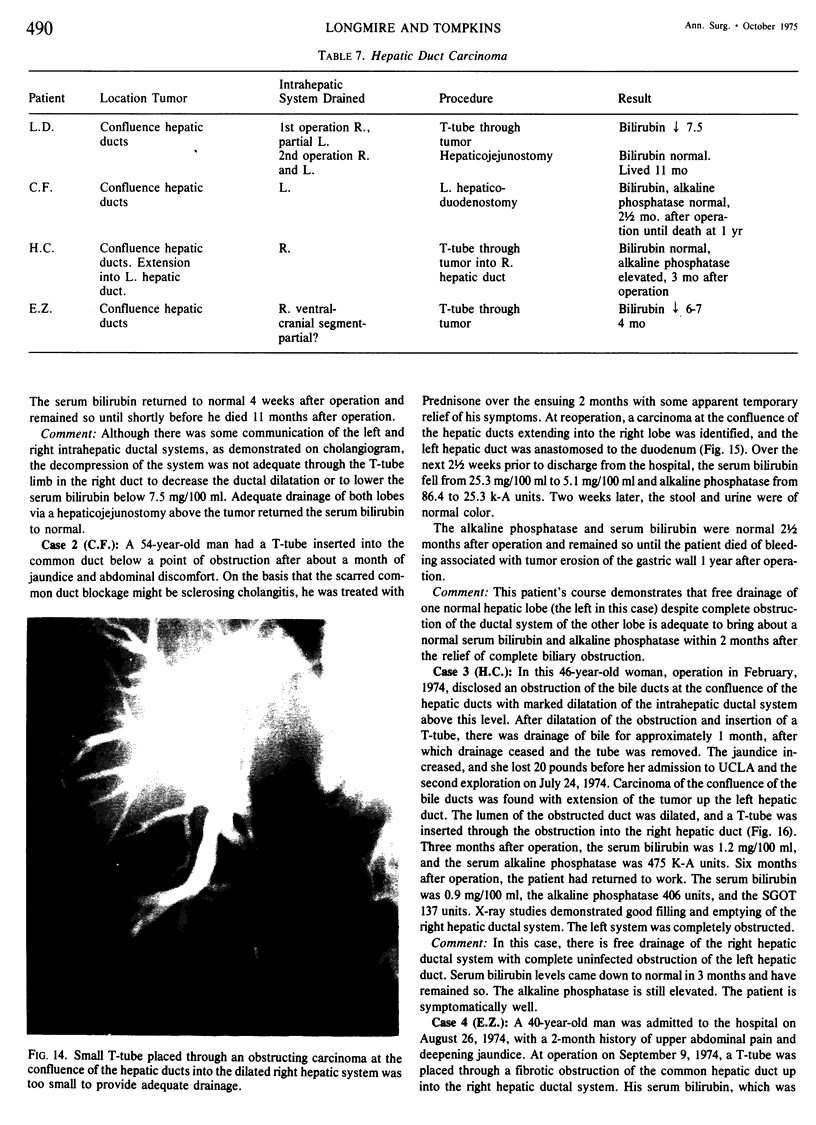
Despite reports to the contrary, unobstructed drainage of 50% of an otherwise normal liver through either the right or left uninfected hepatic duct is adequate to restore normal liver function, even if the obstructed lobe remains in place. An undrained liver lobe, if present, may require no further treatment. As long as it is completely obstructed and uninfected, it will undergo a progressive asymptomatic atrophy. Cholangitis invariably develops behind a partial lobar ductal obstruction, producing jaundice, pruritis, and fever. Unless unobstructed, uninfected biliary flow can be achieved through a segmental or lobar duct, it is better that the duct be completely obstructed and the affected liver parenchyma allowed to atrophy, provided there is normal biliary flow from the residual 50% of liver. This concept is important in the management of injured anomalous segmental or lobar hepatic duct and in the palliative treatment of bile duct carcinoma. Localized intrahepatic infections communicating with abnormal biliary ducts will require hepatic resection of the infected parenchyma and ducts for cure. The abnormality may be saccular dilatation of the intrahepatic ductal system with abscess formation or intrahepatic abscess associated with stenosis of the ductal system from trauma to the duct, to the duct and liver, or to retained intrahepatic stones. Diffusely situated intrahepatic abscesses secondary to ductal abnormalities can be treated with systemic antibiotics, local drainage of a dmoninant abscess, and efforts to improve biliary drainage.
Full text
PDF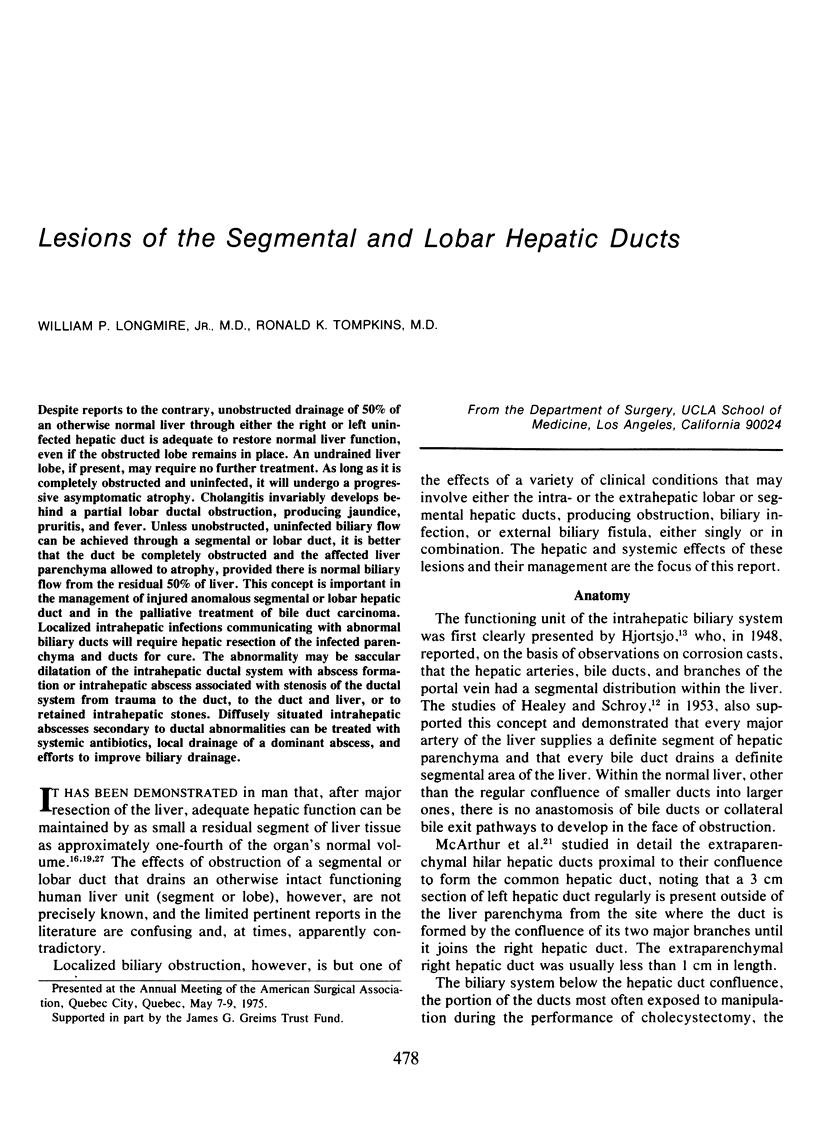



Images in this article





Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Braasch J. W., Whitcomb F. F., Jr, Watkins E., Jr, Maguire R. R., Khazei A. M. Segmental obstruction of the bile duct. Surg Gynecol Obstet. 1972 Jun;134(6):915–920. [PubMed] [Google Scholar]
- GLENN F., MOODY F. G. Intrahepatic calculi. Ann Surg. 1961 May;153:711–724. doi: 10.1097/00000658-196105000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- George P. Disorders of the extrahepatic bile ducts. Clin Gastroenterol. 1973 Jan;2(1):127–146. [PubMed] [Google Scholar]
- Goor D. A., Ebert P. A. Anomalies of the biliary tree. Report of a repair of an accessory bile duct and review of the literature. Arch Surg. 1972 Mar;104(3):302–309. doi: 10.1001/archsurg.1972.04180030050012. [DOI] [PubMed] [Google Scholar]
- HEALEY J. E., Jr, SCHROY P. C. Anatomy of the biliary ducts within the human liver; analysis of the prevailing pattern of branchings and the major variations of the biliary ducts. AMA Arch Surg. 1953 May;66(5):599–616. doi: 10.1001/archsurg.1953.01260030616008. [DOI] [PubMed] [Google Scholar]
- HJORTSJO C. H. The topography of the intrahepatic duct systems. Acta Anat (Basel) 1951;11(4):599–615. [PubMed] [Google Scholar]
- JACKSON J. B., KELLY T. R. CHOLECYSTOHEPATIC DUCTS: CASE REPORT. Ann Surg. 1964 Apr;159:581–584. doi: 10.1097/00000658-196404000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kune G. A. The influence of structure and function in the surgery of the biliary tract. Ann R Coll Surg Engl. 1970 Aug;47(2):78–91. [PMC free article] [PubMed] [Google Scholar]
- Lin T. Y. Results in 107 hepatic lobectomies with a preliminary report on the use of a clamp to reduce blood loss. Ann Surg. 1973 Apr;177(4):413–421. doi: 10.1097/00000658-197304000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Longmire W. P., Jr, Mandiola S. A., Gordon H. E. Congenital cystic disease of the liver and biliary system. Ann Surg. 1971 Oct;174(4):711–726. doi: 10.1097/00000658-197110000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Longmire W. P., Jr, Trout H. H., 3rd, Greenfield J., Tompkins R. K. Elective hepatic surgery. Ann Surg. 1974 May;179(5):712–721. doi: 10.1097/00000658-197405000-00025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Longmire W. P., McArthur M. S., Bastounis E. A., Hiatt J. Carcinoma of the extrahepatic biliary tract. Ann Surg. 1973 Sep;178(3):333–345. doi: 10.1097/00000658-197309000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Longo O. F., Mammana L. A. Canaux biliaires segmentaires aberrats et cholangiographie. Lyon Chir. 1969 Jul-Aug;65(4):499–505. [PubMed] [Google Scholar]
- MICHELS N. A. The hepatic, cystic and retroduodenal arteries and their relations to the biliary ducts with samples of the entire celiacal blood supply. Ann Surg. 1951 Apr;133(4):503–524. doi: 10.1097/00000658-195104000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McArthur M. S., Hiatt J., Bastounis E. A. The surgical anatomy of the porta hepatis. J Surg Res. 1974 Aug;17(2):111–113. doi: 10.1016/0022-4804(74)90130-9. [DOI] [PubMed] [Google Scholar]
- Mistilis S., Schiff L. A case of jaundice due to unilateral hepatic duct obstruction with relief after hepatic lobectomy. Gut. 1963 Mar;4(1):13–15. doi: 10.1136/gut.4.1.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neuhof H., Bloomfield S. The Surgical Significance of an Anomalous Cholecystohepatic Duct: Case Reports. Ann Surg. 1945 Aug;122(2):260–265. doi: 10.1097/00000658-194508000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ong G. B., Leong C. H. Surgical treatment of primary liver cancer. J R Coll Surg Edinb. 1969 Jan;14(1):42–55. [PubMed] [Google Scholar]
- Pollack E. L., Tabrisky J. The aberrant divisional bile duct: a surgical hazard. Surgery. 1973 Feb;73(2):234–239. [PubMed] [Google Scholar]
- RABINOVITCH J., RABINOVITCH P., ZISK H. J. Rare anomalies of the extrahepatic bile ducts. Ann Surg. 1956 Jul;144(1):93–98. doi: 10.1097/00000658-195607000-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- STAFFORD E. S., ISAACS J. P. Stone in the left hepatic duct causing jaundice. Ann Surg. 1958 Jun;147(6):812–816. [PMC free article] [PubMed] [Google Scholar]
- Tsuzuki T., Hoshino Y., Uchiyama T., Kitazima M., Mikata A. Compensatory hypertrophy of the lateral quadrant of the left hepatic lobe due to atrophy of the rest of the liver, appearing as a mass in the left upper quadrant of the abdomen: report of a case. Ann Surg. 1973 Apr;177(4):406–410. doi: 10.1097/00000658-197304000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]