

Abstract
BACKGROUND—Magnetic resonance cholangiography (MRC) is currently under investigation for non-invasive biliary tract imaging. AIM—To compare MRC with endoscopic retrograde cholangiography (ERC) for pretreatment evaluation of malignant hilar obstruction. METHODS—Twenty patients (11 men, nine women; median age 74 years) referred for endoscopic palliation of a hilar obstruction were included. The cause of the hilar obstruction was a cholangiocarcinoma in 15 patients and a hilar compression in five (one hepatocarcinoma, one metastatic breast cancer, one metastatic leiomyoblastoma, two metastatic colon cancers). MRC (T2 turbo spin echo sequences; Siemens Magnetomvision 1.5 T) was performed within 12 hours before ERC, which is considered to be the ideal imaging technique. Tumour location, extension, and type according to Bismuth's classification were determined by the radiologist and endoscopist. RESULTS—MRC was of diagnostic quality in all but two patients (90%). At ERC, four patients (20%) had type I, seven (35%) had type II, seven (35%) had type III, and two (10%) had type IV strictures. MRC correctly classified 14/18 (78%) patients and underestimated tumour extension in four (22%). Successful endoscopic biliary drainage was achieved in 11/17 attempted stentings (65%), one of which was a combined procedure (endoscopic + percutaneous). One patient had a percutaneous external drain, one had a surgical bypass, and in a third a curative resection was attempted. Effective drainage was not achieved in six patients (30%). If management options had been based only on MRC, treatment choices would have been modified in a more appropriate way in 5/18 (28%) patients with satisfactory MRC. CONCLUSION—MRC should be considered for planning treatment of malignant hilar strictures. Accurate depiction of high grade strictures for which endoscopic drainage is not the option of choice can preclude unnecessary invasive imaging. Keywords: hilar tumours; endoscopic retrograde cholangiopancreatography; magnetic resonance cholangiography; stenting
Full Text
The Full Text of this article is available as a PDF (88.0 KB).
Figure 1 .
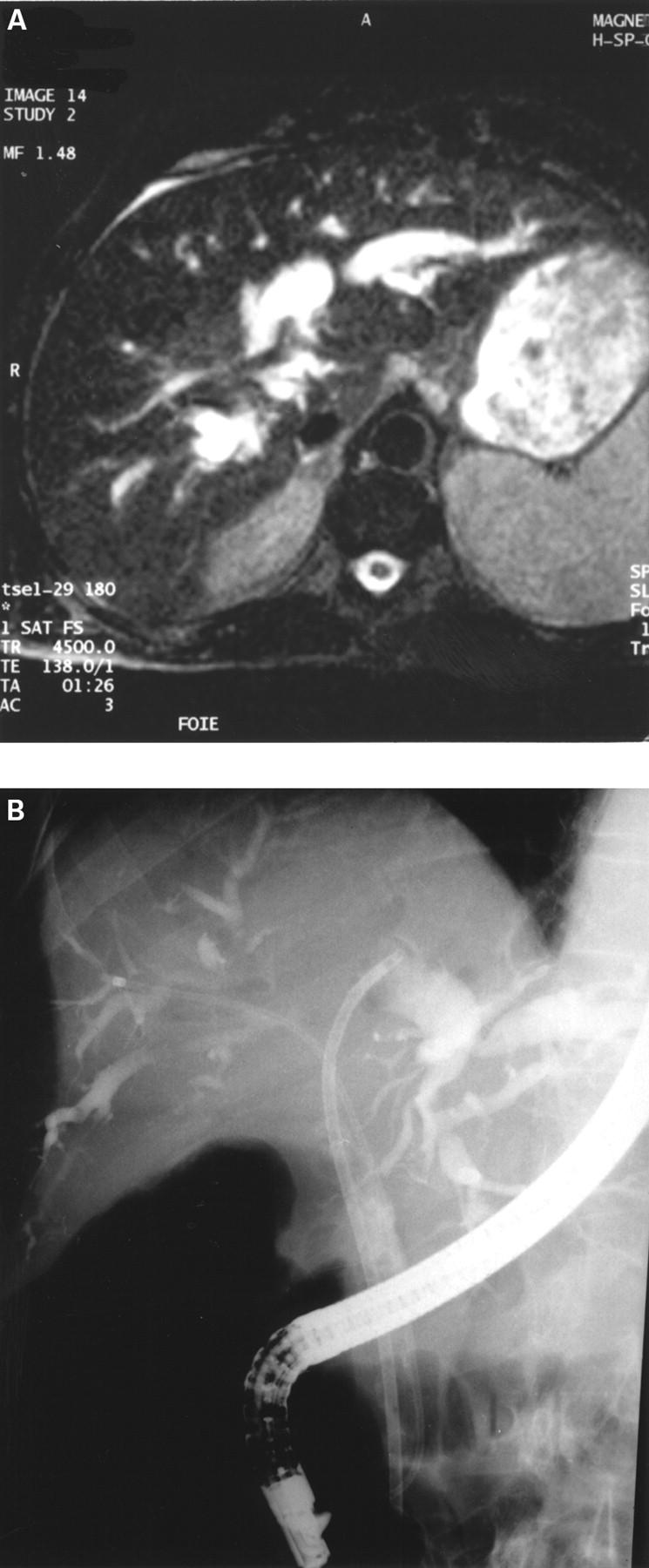
(A) Magnetic resonance cholangiography (MRC) displaying a Bismuth's type II hilar tumour (native axial image). (B) Endoscopic retrograde cholangiography in the same patient, performed 12 hours after MRC, confirms the type II hilar extension and allows selective intubation of both hepatic ducts (see guidewires) and subsequent insertion of two stents (not shown on the figure) for complete biliary drainage.
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Banerjee B., Teplick S. K. Nonsurgical management of primary cholangiocarcinoma. Retrospective analysis of 40 cases. Dig Dis Sci. 1995 Mar;40(3):701–705. doi: 10.1007/BF02064393. [DOI] [PubMed] [Google Scholar]
- Bismuth H., Castaing D., Traynor O. Resection or palliation: priority of surgery in the treatment of hilar cancer. World J Surg. 1988 Feb;12(1):39–47. doi: 10.1007/BF01658484. [DOI] [PubMed] [Google Scholar]
- Bonnel D., Liguory C., Lefebvre J. F., Cornud F. Traitement percutané des sténoses malignes du hile. Gastroenterol Clin Biol. 1995 Jun-Jul;19(6-7):564–571. [PubMed] [Google Scholar]
- Chang W. H., Kortan P., Haber G. B. Outcome in patients with bifurcation tumors who undergo unilateral versus bilateral hepatic duct drainage. Gastrointest Endosc. 1998 May;47(5):354–362. doi: 10.1016/s0016-5107(98)70218-4. [DOI] [PubMed] [Google Scholar]
- Cotton P. B. Endoscopic methods for relief of malignant obstructive jaundice. World J Surg. 1984 Dec;8(6):854–861. doi: 10.1007/BF01656025. [DOI] [PubMed] [Google Scholar]
- Ducreux M., Liguory C., Lefebvre J. F., Ink O., Choury A., Fritsch J., Bonnel D., Derhy S., Etienne J. P. Management of malignant hilar biliary obstruction by endoscopy. Results and prognostic factors. Dig Dis Sci. 1992 May;37(5):778–783. doi: 10.1007/BF01296439. [DOI] [PubMed] [Google Scholar]
- Farley D. R., Weaver A. L., Nagorney D. M. "Natural history" of unresected cholangiocarcinoma: patient outcome after noncurative intervention. Mayo Clin Proc. 1995 May;70(5):425–429. doi: 10.4065/70.5.425. [DOI] [PubMed] [Google Scholar]
- Gillams A. R., Lees W. R. Recent developments in biliary tract imaging. Gastrointest Endosc Clin N Am. 1996 Jan;6(1):1–15. [PubMed] [Google Scholar]
- Guibaud L., Bret P. M., Reinhold C., Atri M., Barkun A. N. Bile duct obstruction and choledocholithiasis: diagnosis with MR cholangiography. Radiology. 1995 Oct;197(1):109–115. doi: 10.1148/radiology.197.1.7568807. [DOI] [PubMed] [Google Scholar]
- Hadjis N. S., Blenkharn J. I., Alexander N., Benjamin I. S., Blumgart L. H. Outcome of radical surgery in hilar cholangiocarcinoma. Surgery. 1990 Jun;107(6):597–604. [PubMed] [Google Scholar]
- Hall-Craggs M. A., Allen C. M., Owens C. M., Theis B. A., Donald J. J., Paley M., Wilkinson I. D., Chong W. K., Hatfield A. R., Lees W. R. MR cholangiography: clinical evaluation in 40 cases. Radiology. 1993 Nov;189(2):423–427. doi: 10.1148/radiology.189.2.8210370. [DOI] [PubMed] [Google Scholar]
- Holzknecht N., Gauger J., Sackmann M., Thoeni R. F., Schurig J., Holl J., Weinzierl M., Helmberger T., Paumgartner G., Reiser M. Breath-hold MR cholangiography with snapshot techniques: prospective comparison with endoscopic retrograde cholangiography. Radiology. 1998 Mar;206(3):657–664. doi: 10.1148/radiology.206.3.9494483. [DOI] [PubMed] [Google Scholar]
- Ishizaki Y., Wakayama T., Okada Y., Kobayashi T. Magnetic resonance cholangiography for evaluation of obstructive jaundice. Am J Gastroenterol. 1993 Dec;88(12):2072–2077. [PubMed] [Google Scholar]
- Kozarek R. A. Endoscopy in the management of malignant obstructive jaundice. Gastrointest Endosc Clin N Am. 1996 Jan;6(1):153–176. [PubMed] [Google Scholar]
- Levin B. Diagnosis and medical treatment of malignant disorders of the biliary tract. Semin Liver Dis. 1987 Nov;7(4):328–333. doi: 10.1055/s-2008-1040589. [DOI] [PubMed] [Google Scholar]
- Macaulay S. E., Schulte S. J., Sekijima J. H., Obregon R. G., Simon H. E., Rohrmann C. A., Jr, Freeny P. C., Schmiedl U. P. Evaluation of a non-breath-hold MR cholangiography technique. Radiology. 1995 Jul;196(1):227–232. doi: 10.1148/radiology.196.1.7784572. [DOI] [PubMed] [Google Scholar]
- Miyazaki T., Yamashita Y., Tsuchigame T., Yamamoto H., Urata J., Takahashi M. MR cholangiopancreatography using HASTE (half-Fourier acquisition single-shot turbo spin-echo) sequences. AJR Am J Roentgenol. 1996 Jun;166(6):1297–1303. doi: 10.2214/ajr.166.6.8633435. [DOI] [PubMed] [Google Scholar]
- Reding R., Buard J. L., Lebeau G., Launois B. Surgical management of 552 carcinomas of the extrahepatic bile ducts (gallbladder and periampullary tumors excluded). Results of the French Surgical Association Survey. Ann Surg. 1991 Mar;213(3):236–241. doi: 10.1097/00000658-199103000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinhold C., Bret P. M. Current status of MR cholangiopancreatography. AJR Am J Roentgenol. 1996 Jun;166(6):1285–1295. doi: 10.2214/ajr.166.6.8633434. [DOI] [PubMed] [Google Scholar]
- Speer A. G., Cotton P. B., Russell R. C., Mason R. R., Hatfield A. R., Leung J. W., MacRae K. D., Houghton J., Lennon C. A. Randomised trial of endoscopic versus percutaneous stent insertion in malignant obstructive jaundice. Lancet. 1987 Jul 11;2(8550):57–62. doi: 10.1016/s0140-6736(87)92733-4. [DOI] [PubMed] [Google Scholar]