

Abstract
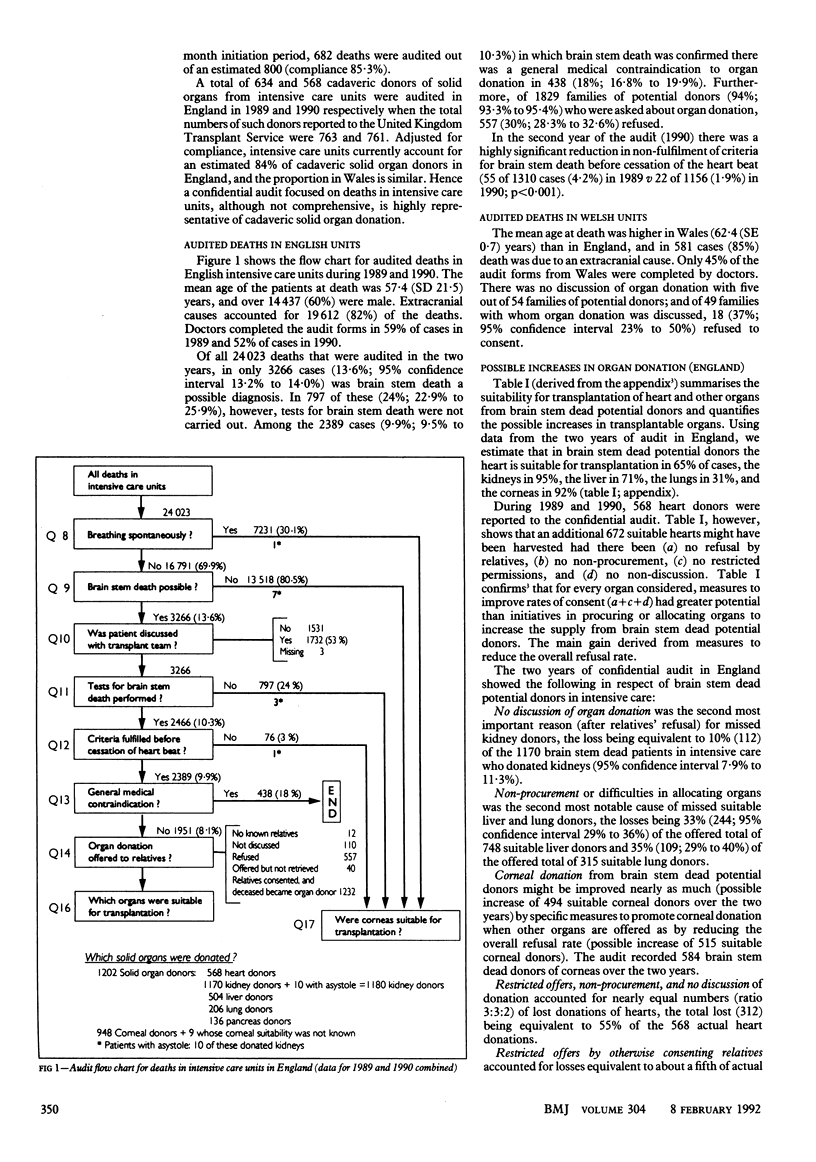
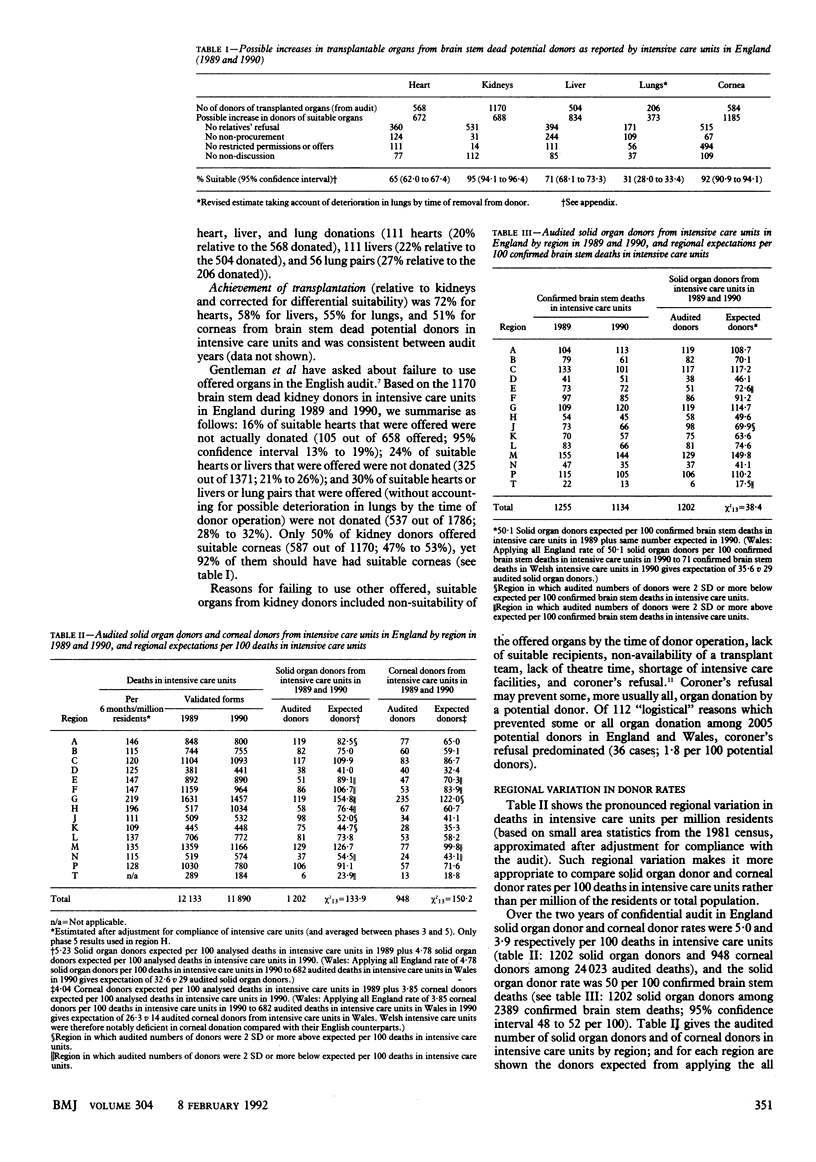
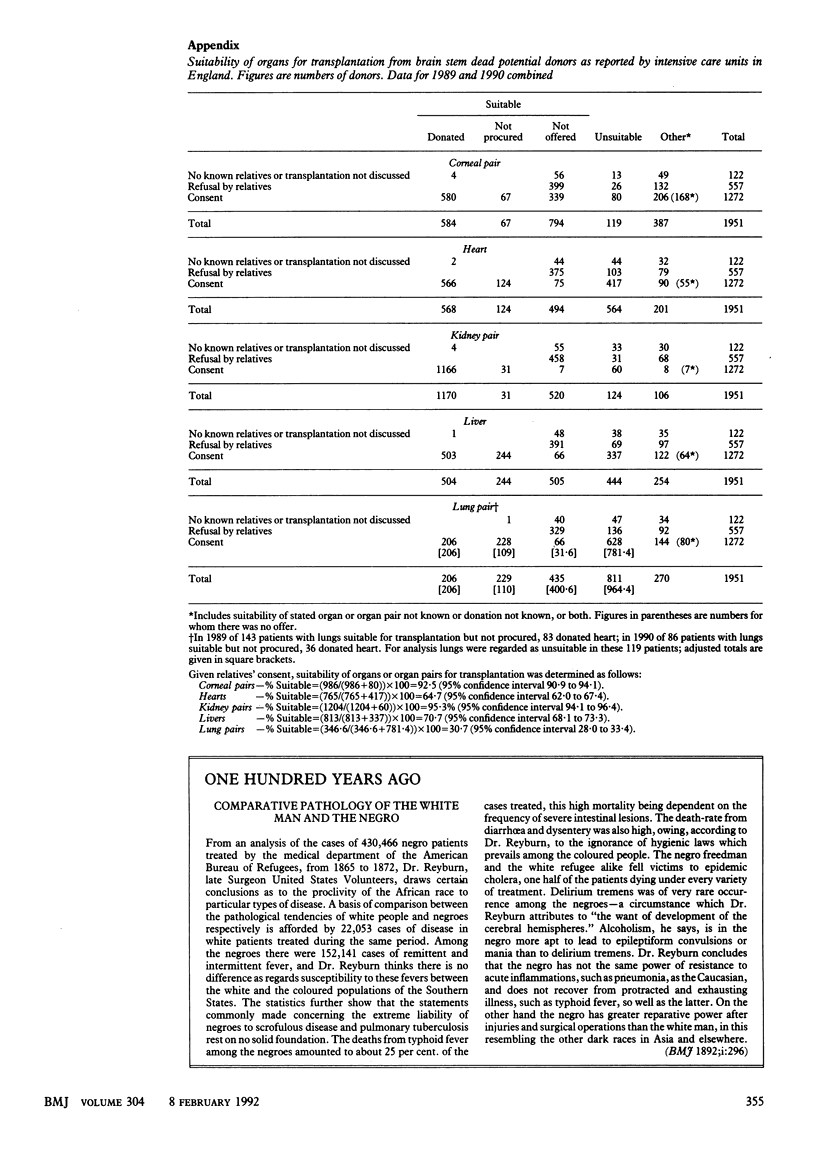
OBJECTIVES--Quantify possible increases in cadaveric organ donation from intensive care units; identify major sources of regional variation. DESIGN--Confidential audit of all deaths in intensive care units in England in 1989 and 1990 and in Wales in 1990. SETTING--15 regional and special health authorities in England; Wales. PATIENTS--24,023 audited deaths in England; 682 in Wales. MAIN OUTCOME MEASURES--Solid organ and corneal donor rates per 100 deaths; solid organ donor rate per 100 confirmed brain stem deaths; regional variation in (a) whether brain stem death was possible diagnosis, (b) general medical contraindications to donation, (c) relatives' refusal. RESULTS--Confirmed brain stem death accounted for 2389 (10%) audited deaths in England. In 438 (18%) there was a general medical contraindication to organ donation, and of 1829 (94%) families asked about donation, 557 (30%) refused. Data for England suggested that among potential donors the heart is suitable for transplantation in 65% of cases, the kidneys in 95%, the liver in 71%, the lungs in 31%, and the corneas in 92%. Reasons for any shortfall in achievement of transplantation varied with organ type. Solid organ and corneal donor rates per 100 deaths were 5.0 and 3.9 respectively in England and 4.3 and 2.1 respectively in Wales. The solid organ donor rate per 100 confirmed brain stem deaths was 50 in England and 41 in Wales. CONCLUSIONS--A 20% increase in number of cadaveric kidney donors from intensive care could be achieved by prompt testing for brain stem death and a quarter reduction in relatives' refusals.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Feest T. G., Riad H. N., Collins C. H., Golby M. G., Nicholls A. J., Hamad S. N. Protocol for increasing organ donation after cerebrovascular deaths in a district general hospital. Lancet. 1990 May 12;335(8698):1133–1135. doi: 10.1016/0140-6736(90)91134-v. [DOI] [PubMed] [Google Scholar]
- Gentleman D., Easton J., Jennett B. Brain death and organ donation in a neurosurgical unit: audit of recent practice. BMJ. 1990 Nov 24;301(6762):1203–1206. doi: 10.1136/bmj.301.6762.1203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gore S. M., Hinds C. J., Rutherford A. J. Organ donation from intensive care units in England. BMJ. 1989 Nov 11;299(6709):1193–1197. doi: 10.1136/bmj.299.6709.1193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gore S. M. Organ donation in a neurosurgical unit. BMJ. 1991 Jan 5;302(6767):52–52. doi: 10.1136/bmj.302.6767.52-b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gore S. M., Taylor R. M., Wallwork J. Availability of transplantable organs from brain stem dead donors in intensive care units. BMJ. 1991 Jan 19;302(6769):149–153. doi: 10.1136/bmj.302.6769.149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Organs for transplantation. BMJ. 1989 Dec 9;299(6713):1463–1464. [PMC free article] [PubMed] [Google Scholar]
- Salih M. A., Harvey I., Frankel S., Coupe D. J., Webb M., Cripps H. A. Potential availability of cadaver organs for transplantation. BMJ. 1991 May 4;302(6784):1053–1055. doi: 10.1136/bmj.302.6784.1053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallwork J. Organs for transplantation. BMJ. 1989 Nov 25;299(6711):1291–1292. doi: 10.1136/bmj.299.6711.1291. [DOI] [PMC free article] [PubMed] [Google Scholar]