

SYNOPSIS OF RECOMMENDATIONS
Diagnosis and management of community-acquired pneumonia (CAP)
What is the role of chest radiograph in the diagnosis of CAP?
Wherever feasible, a chest radiograph should be obtained in all patients suspected of having CAP (1A).
In the absence of availability of chest radiograph, patients may be treated on the basis of clinical suspicion (3A).
Chest radiograph should be repeated if the patient is not improving and also for all those patients who have persistence or worsening of symptoms/physical signs or those in whom an underlying malignancy needs to be excluded. It is not routinely necessary to repeat a chest radiograph in patients who have improved clinically (2A).
What is the role of computed tomography (CT) in the diagnosis of CAP?
T of the thorax should not be performed routinely in patients with CAP (2A).
CT of the chest should be performed in those with non-resolving pneumonia and for the assessment of complications of CAP (2A).
Which microbiological investigations need to be performed in CAP?
Blood cultures
Blood cultures should be obtained in all hospitalized patients with CAP (2A).
Blood cultures are not required in routine outpatient management of CAP (2A).
Sputum Gram stain and cultures
An initial sputum Gram stain and culture (or an invasive respiratory sample as appropriate) should be obtained in all hospitalized patients with CAP (2A).
Sputum quality should be ensured for interpreting Gram stain results (2A).
Sputum for acid-fast bacilli (AFB) should be obtained as per RNTCP guidelines for non-responders (UPP).
Pneumococcal antigen detection
Pneumococcal antigen detection test is not required routinely for the management of CAP (2A).
Pneumococcal PCR
Pneumococcal PCR is not recommended as a routine diagnostic test in patients with CAP (1A)
Legionella antigen detection
Legionella urinary antigen test is desirable in patients with severe CAP (1B).
Other atypical pathogens
Investigations for atypical pathogens like Mycoplasma, Chlamydia, and viruses need not be routinely done (2A).
What general investigations are required in patients with CAP?
For patients managed in an outpatient setting, no investigations are routinely required apart from a chest radiograph (3A).
Pulse oximetry is desirable in outpatients (2B).
Pulse oximetric saturation, if available, should be obtained as early as possible in admitted patients (2A). Arterial blood gas analysis should be performed in those with an oxygen saturation ≤90% and in those with chronic lung disease (3A).
Blood glucose, urea, and electrolytes should be obtained in all hospitalized patients with CAP (3A).
Full blood count and liver function tests are also helpful in the management of patients with CAP (3B).
What is the role of biomarkers in the diagnosis of CAP?
Procalcitonin and CRP measurement need not be performed as routine investigations for the diagnosis of CAP (2A).
Should patients with CAP be risk stratified? What should be the optimum method of risk stratification?
Patients with community-acquired pneumonia should be risk stratified (1A).
Risk stratification should be performed in two steps [Figure 1] based upon the need for hospital admission followed by assessment of the site of admission (non-ICU vs. ICU). Accordingly, patients can be managed as either outpatient or inpatient (ward or ICU) (1A).
Initial assessment should be done with CRB-65. If the score is >1, patients should be considered for admission (1A).
Clinical judgment should be applied as a decision modifier in all cases (3A).
Pulse oximetry can be used to admit hypoxemic patients (2A). Hypoxemia is defined as pulse oximetric saturation ≤92% and ≤90% for age ≤50 and >50 years, respectively (3A).
Patients selected for admission can be triaged to the ward (non-ICU)/ICU based upon the major/minor criteria outlined in Table 6 (2A).
If any major criterion or ≥3 minor criteria are fulfilled, patients should generally be admitted to the ICU (1A).
Figure 1.
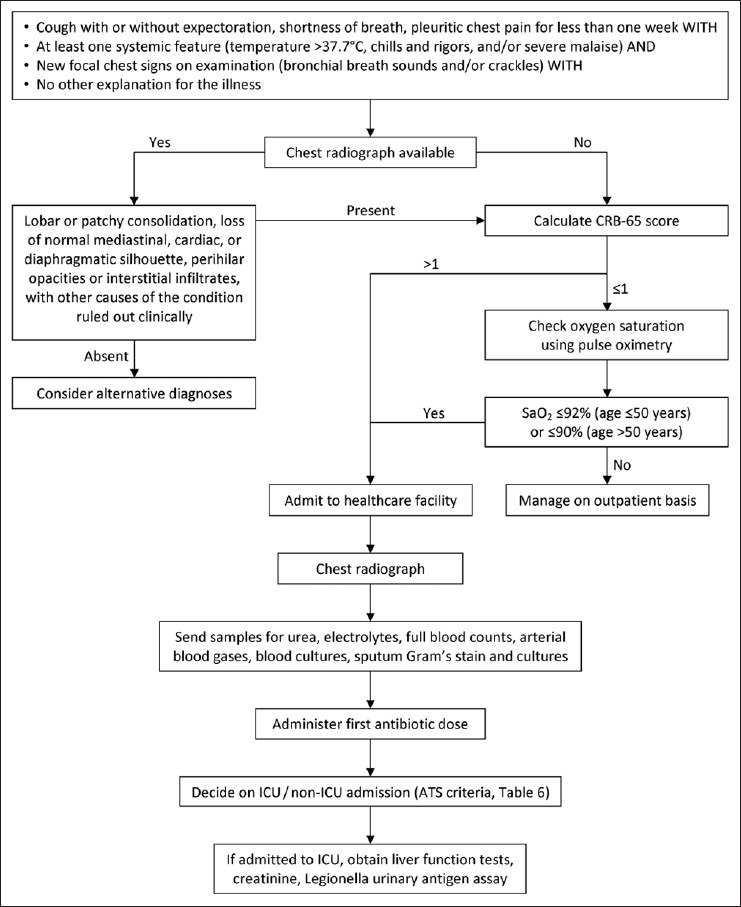
Algorithmic approach to diagnosis and management of CAP (ARDS, acute respiratory distress syndrome; CXR, chest radiograph; ICU, intensive care unit; LFTs, liver function tests; SaO2, arterial saturation)
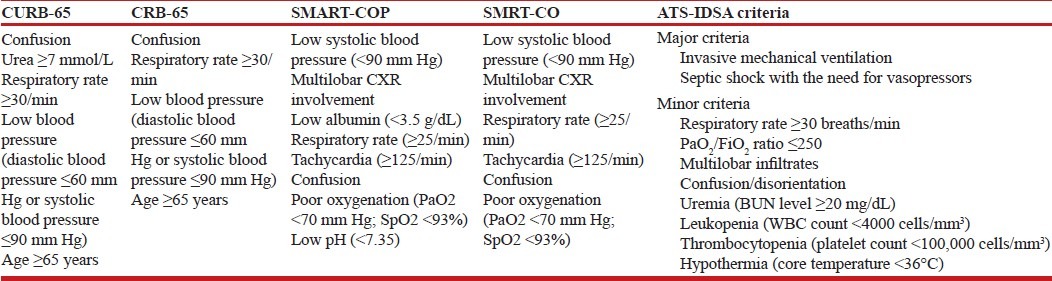
Table 6.
Summary of commonly used criteria for risk stratification in CAP
What practices are recommended regarding use of antibiotics in CAP?
Antibiotics should be administered as early as possible; timing is more important in severe CAP (2A).
What should be the antibiotic therapy in the outpatient setting?
Therapy should be targeted toward coverage of the most common organism, namely Streptococcus pneumoniae (1A).
Outpatients should be stratified as those with or without comorbidities (3A).
Recommended antibiotics [Table 10] are oral macrolides (e.g. azithromycin) or oral β-lactams (e.g. amoxicillin 500–1000 mg thrice daily) for outpatient without comorbidities (1A).
For outpatients with comorbidities [Table 8], oral combination therapy is recommended (β-lactams plus macrolides) (1A).
There is insufficient evidence to recommend tetracyclines (3B).
Fluoroquinolones should not be used for empiric treatment (1A).
Antibiotics should be given in appropriate doses to prevent emergence of resistance (1A).
Table 10.
Doses of drugs used in CAP
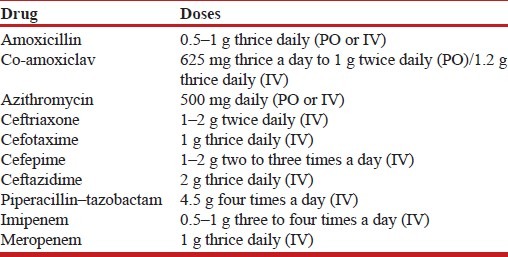
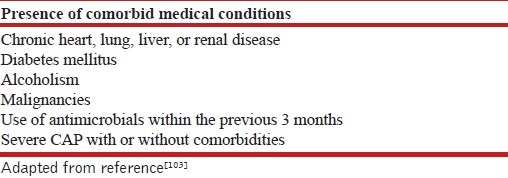
Table 8.
Indications for empiric combination therapy in CAP
What should be the antibiotic therapy in the hospitalized non-ICU setting?
The recommended regimen is a combination of a β-lactam plus a macrolide (preferred β-lactams include cefotaxime, ceftriaxone, and amoxicillin–clavulanic acid) (1A).
In the uncommon scenario of hypersensitivity to β-lactams, respiratory fluoroquinolones (e.g. levofloxacin 750 mg daily) may be used if tuberculosis is not a diagnostic consideration at admission (1A). Patients should also undergo sputum testing for acid-fast bacilli simultaneously if fluoroquinolones are being used in place of β-lactams.
Route of administration (oral or parenteral) should be decided based upon the clinical condition of the patient and the treating physician's judgment regarding tolerance and efficacy of the chosen antibiotics (3A).
Switch to oral from intravenous therapy is safe after clinical improvement in moderate to severe CAP (2A).
What should be the antibiotic therapy in ICU setting?
The recommended regimen is a β-lactam (cefotaxime, ceftriaxone, or amoxicillin–clavulanic acid) plus a macrolide for patients without risk factors for Pseudomonas aeruginosa (2A).
If P. aeruginosa is an etiological consideration, an antipneumococcal antibiotic (e.g. cefepime, ceftazidime, cefoperazone, piperacillin–tazobactam, cefoperazone–sulbactam, imipenem, or meropenem) should be given (2A). Combination therapy may be considered with addition of aminoglycosides/antipseudomonal fluoroquinolones (e.g. ciprofloxacin) (3A). Fluoroquinolones may be used if tuberculosis is not a diagnostic consideration at admission (1A). Patients should also undergo sputum testing for acid-fast bacilli simultaneously if fluoroquinolones are being used.
Antimicrobial therapy should be changed according to specific pathogen(s) isolated (2A).
Diagnostic/therapeutic interventions should be done for complications, e.g. thoracentesis, chest tube drainage, etc. as required (1A).
If a patient does not respond to treatment within 48–72 h, he/she should be evaluated for the cause of non-response, including development of complications, presence of atypical pathogens, drug resistance, etc. (3A).
Switch to oral from intravenous therapy is safe after clinical improvement in moderate to severe CAP (2A).
When should patients be discharged?
Patients can be considered for discharge if they start accepting orally, are afebrile, and are hemodynamically stable for a period of at least 48 h (2A).
Outpatients should be treated for 5 days and inpatients for 7 days (1A).
Antibiotics may be continued beyond this period in patients with bacteremic pneumococcal pneumonia, Staphylococcus aureus pneumonia, and CAP caused by Legionella pneumoniae and non-lactose fermenting Gram-negative bacilli (2A). Antibiotics may also be continued beyond the specified period for those with meningitis or endocarditis complicating pneumonia, infections with enteric Gram-negative bacilli, lung abscess, empyema, and if the initial therapy was not active against the identified pathogen (3A).
What is the role of biomarkers in the treatment of CAP?
Biomarkers should not be routinely used to guide antibiotic treatment as this has not been shown to improve clinical outcomes (1A).
What adjunctive therapies are useful for the management of CAP?
Steroids are not recommended for use in non-severe CAP (2A).
Steroids should be used for septic shock or in ARDS secondary to CAP according to the prevalent management protocols for these conditions (1A).
There is no role of other adjunctive therapies (anticoagulants, immunoglobulin, granulocyte colony-stimulating factor, statins, probiotics, chest physiotherapy, antiplatelet drugs, over-the-counter cough medications, β2 agonists, inhaled nitric oxide, and angiotensin-converting enzyme inhibitors) in the routine management of CAP (1A).
CAP-ARDS and CAP leading to sepsis and septic shock should be managed according to the standard management protocols for these conditions (1A).
Noninvasive ventilation may be used in patients with CAP and acute respiratory failure (2A).
What is the role of immunization and smoking cessation for the prevention of CAP?
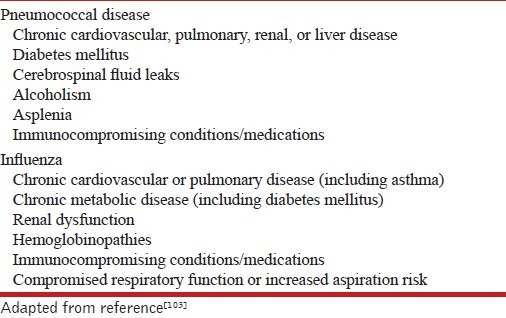
Routine use of pneumococcal vaccine among healthy immunocompetent adults for prevention of CAP is not recommended (1A). Pneumococcal vaccine may be considered for prevention of CAP in special populations who are at high risk for invasive pneumococcal disease [Table 11] (2A).
Influenza vaccination should be considered in adults for prevention of CAP (3A).
Smoking cessation should be advised for all current smokers (1A).
Table 11.
High-risk groups in whom vaccination is recommended
Diagnosis and management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP)
What is the utility of healthcare-associated pneumonia (HCAP)?
The risk stratification regarding acquisition of MDR pathogen should be individualized rather than using an umbrella definition of HCAP for this purpose (UPP).
What is the micro-organism profile of HAP/VAP?
Gram-negative bacteria are the most common pathogens causing HAP/VAP in the Indian setting (UPP), and should be routinely considered as the most common etiological agents of HAP/VAP.
What is the approach to diagnosis of HAP/VAP?
HAP/VAP can be clinically defined [Figure 2] using modified CDC criteria (2A).
In patients with a strong suspicion of VAP/HAP but insufficient evidence for the presence of infection, periodic re-evaluation should be done (2A).
In patients with suspected VAP/HAP, one or more lower respiratory tract samples and blood should be sent for cultures prior to institution of antibiotics (1A).
All patients suspected of having HAP should be further evaluated with good-quality sputum microbiology (3A).
CT scan should not be routinely obtained for diagnosing HAP/VAP (3A).
Semi-quantitative cultures can performed in lieu of qualitative cultures (1A).
Appropriate management should not be delayed in clinically unstable patients for the purpose of performing diagnostic sampling (UPP).
Figure 2.
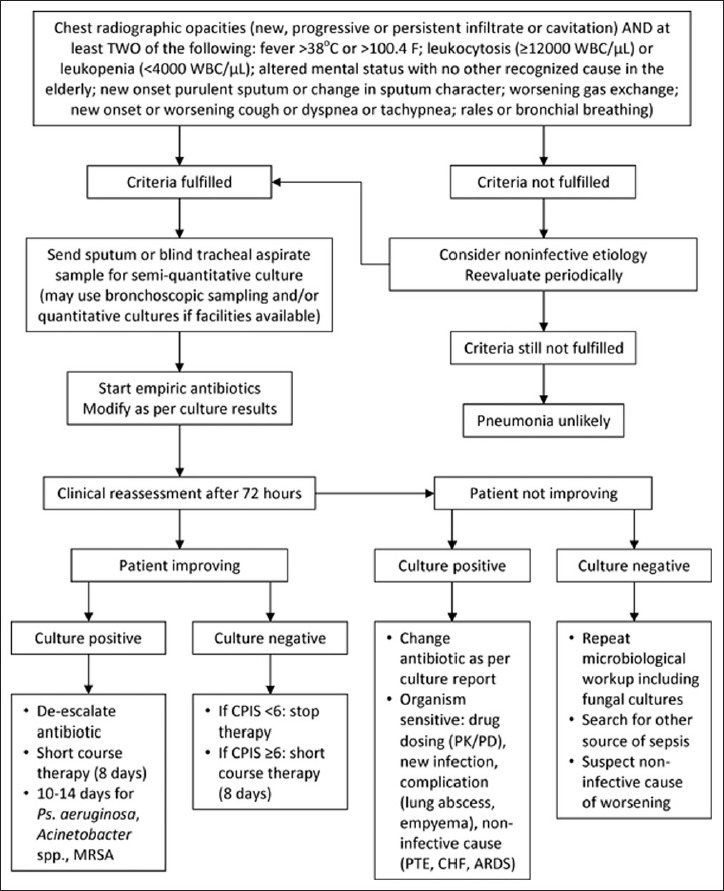
Algorithmic approach to diagnosis and management of HAP
Are quantitative methods of culture better than semi-quantitative methods?
Semi-quantitative cultures of lower respiratory tract secretions are easier and equally discriminatory for the presence of pneumonia, as compared to quantitative cultures (UPP).
Are invasive techniques to collect lower respiratory tract secretions better than blind endotracheal aspirates?
Quantitative and or semi-quantitative cultures using various sampling techniques like ETA, bronchoscopic, or non-bronchoscopic BAL and PSB are equally useful for establishing the diagnosis of HAP/VAP (2A).
Semi-quantitative culture on blind (non-bronchoscopic) ETA sample (preferably obtained through a sterile telescoping catheter system) is a reasonable choice (2A).
In a patient suspected of having VAP, the preferred method for lower respiratory tract sample collection (blind or targeted, bronchoscopic or non-bronchoscopic) depends upon individual preferences, local expertise, and cost; however, blind ETA sampling is the easiest and equally useful (UPP).
What is the role of biomarkers in the diagnosis of HAP/VAP?
Currently available biomarkers should not be used to diagnose HAP/VAP (1A).
Where available, serum procalcitonin levels <0.5 ng/mL may help in differentiating bacterial HAP/VAP form other non-infective etiologies, and may help in decisions for antibiotic cessation (2B).
Is combined clinico-bacteriological strategy better than either strategy used alone?
Both clinical and bacteriological strategies can be combined to better diagnose and manage HAP and VAP (UPP).
How do we decide on the empiric antibiotic regimen to be started in a case of suspected HAP/VAP?
Every ICU/hospital should have its own antibiotic policy for initiating empiric antibiotic therapy in HAP based on their local microbiological flora and resistance profiles (1A). This policy should be reviewed periodically.
In hospitals that do not have their own antibiotic policy, the policy given in these guidelines is recommended (3A). However, they should strive toward formulating their own antibiotic policy.
What is the role of routine endotracheal aspirate culture surveillance?
Routine endotracheal aspirate culture is not recommended. An antibiogram approach should be followed wherever feasible (2A).
Is there a benefit of combination therapy over monotherapy for the treatment of HAP/VAP and HCAP?
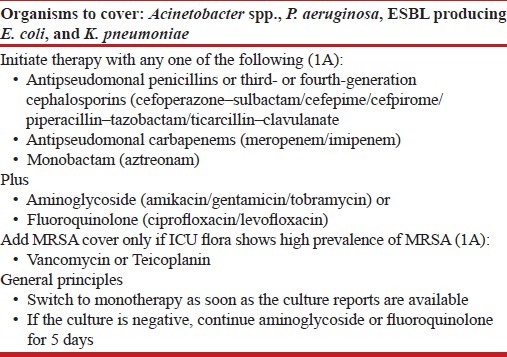
Although there is no evidence to suggest that combination therapy is superior to monotherapy, the expert group recommended initial empiric therapy as a combination due to the high prevalence rates of MDR pathogens in late-onset HAP/VAP [Table 16] and with an aim to ensure the chances of appropriateness of the initial regimen (UPP). However, once the culture reports are available, the regimen should be de-escalated to the appropriate monotherapy (1A).
Table 16.
Initial empiric therapy in patients with late-onset HAP/VAP
What is the recommended strategy for initiating antibiotics in suspected HAP/VAP?
In patients with suspected HAP, antibiotics should be initiated as early as possible after sending the relevant samples for culture (1A).
The exact choice of antibiotic to be started is based on local availability, antibiotic resistance patterns, preferred routes of delivery, other complicating factors, and cost.
The initial combination therapy should be converted to appropriate monotherapy once the culture reports are available (1A).
Colistin is not recommended as an initial empiric therapy for HAP/VAP (3A).
Combination therapy with colistin and meropenem is not recommended (2A).
Is antibiotic de-escalation useful? What is the strategy for antibiotic de-escalation?
The strategy for de-escalation of antibiotics is strongly recommended (1A). However, as the de-escalation strategy entirely rests on microbiology, appropriate microbiological samples should be sent before initiation of antibiotics [Figure 2].
Among patients with suspected VAP in whom an alternate cause for pulmonary infiltrates is identified, it is recommended that antibiotics should be stopped (1A).
If cultures are sent after initiation of antibiotics, and there is clinical improvement with subsequent cultures being sterile, antibiotics should be continued for 7 days followed by assessment of CPIS on the 7th day. If CPIS is <6, antibiotics can be stopped, while if it is ≥6, treatment should be continued for 10–14 days.
If cultures sent before starting antibiotics are negative and there is clinical worsening, it is recommended that a review of the current management plan including the choice of antibiotics be performed. Microbiological workup should be repeated including performance of fungal cultures. One also needs to look for alternate sources of sepsis (especially one or more foci of undrained infection), and consider non-infective causes.
Empiric antifungal therapy (on day 3) should not be used as a routine in all patients if cultures are sterile and there is clinical worsening (3A).
What is the optimal duration of antibiotic therapy?
In patients with VAP due to Pseudomonas, Acinetobacter, and MRSA, a longer duration (14 days) of antibiotic course is recommended (1A). Assessment of CPIS on day 7 may identify the patients in whom therapy could be stopped early (2A).
In other patients with VAP who are clinically improving, a 7-day course of antibiotics is recommended (1A).
Is continuous infusion of antibiotics better than intermittent doses?
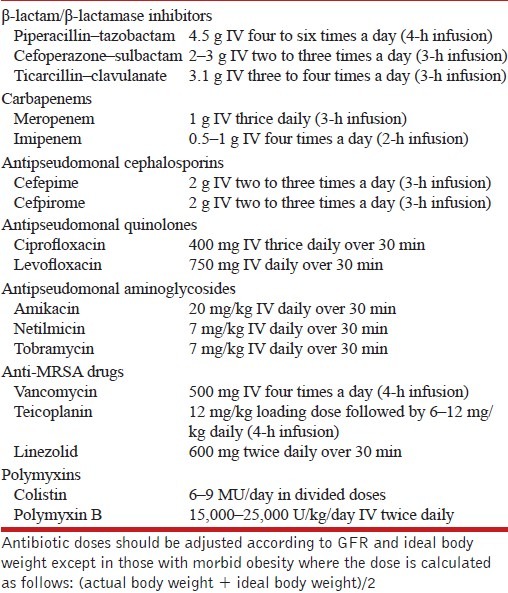
Antibiotic administration in critically ill patients according to their pharmacokinetic/pharmacodynamic profile [Table 17] is recommended as it is associated with superior clinical outcomes (2A).
Table 17.
Doses of intravenous antibiotics used in the treatment of HAP/VAP
What is the role of inhaled antibiotics in the treatment of VAP?
Aerosolized antibiotics (colistin and tobramycin) may be a useful adjunct to intravenous antibiotics in the treatment of MDR pathogens where toxicity is a concern (2A).
Aerosolized antibiotics should not be used as monotherapy and should be used concomitantly with intravenous antibiotics (2A).
Should one treat ventilator-associated tracheobronchitis?
Patients with proven VAT should not be treated with antibiotics (2A).
What are the drugs of choice for treatment of methicillin-resistant Staphylococcus aureus?
In patients with suspected MRSA infection, we recommend the use of empiric vancomycin (1A) or teicoplanin (2A). The use of linezolid in India should be reserved because of its potential use in extensively drug-resistant TB.
Linezolid is an effective alternative to vancomycin (1A) if the patient (a) is vancomycin intolerant, (b) has renal failure, and (c) is harboring vancomycin-resistant organism.
How to treat MDR Acinetobacter infections?
For treatment of MDR Acinetobacter infections, we recommend the following drugs: carbapenems (1A), colistin (1A), sulbactam plus colistin (2B), sulbactam plus carbapenem (2B), and polymyxin B (2A).
Combination therapy with sulbactam and colistin or carbapenem for MDR Acinetobacter (in proven cases or suspected cases with multi-organ dysfunction syndrome) may be initiated. Sulbactam should be stopped after 5 days in patients responding to treatment (2B).
How to treat MDR Pseudomonas infections?
For treatment of MDR Pseudomonas, we recommend initial combination chemotherapy with a carbapenem and either a fluoroquinolone or an aminoglycoside (1A). Treatment should then be de-escalated to appropriate monotherapy.
What are the other good practices to be followed in the ICU?
Stress ulcer prophylaxis: Sucralfate should be used in patients with HAP, while H-2 receptor antagonists or proton pump inhibitors should be used in patients with VAP.
Early enteral feeding: Enteral feeding is superior to parenteral nutrition and should be used whenever tolerated and in those without any contraindications to enteral feeding.
DVT prophylaxis: DVT prophylaxis with unfractionated heparin (5000 U thrice a day) or a low-molecular-weight heparin should be routinely used in all ICU patients with no contraindications to prophylactic anticoagulation.
Glucose control: A plasma glucose target of 140–180 mg/dL is recommended in most patients with HAP/VAP, rather than a more stringent target (80–110 mg/dL) or a more liberal target (180–200 mg/dL).
Blood products: Red cells should be transfused at a hemoglobin threshold of <7 g/dL except in those with myocardial ischemia and pregnancy. Platelet transfusion is indicated in patients with platelet count <10,000/μL, or <20,000/μL if there is active bleeding. Fresh frozen plasma is indicated only if there is a documented abnormality in the coagulation tests and there is active bleeding or if a procedure is planned.
INTRODUCTION
Pneumonia is an important clinical condition which is commonly confronted both by a pulmonologist as well as a general practitioner. In spite of plethora of information on the subject, one often finds it difficult to make critical decisions. There are several evidence-based guidelines to guide treatment decisions. However, there are no Indian guidelines, which consider the differences in healthcare organization, prescription habits of doctors, drug availability, and costs. Moreover, the clinical practice is different at different levels of healthcare in the country. It was therefore, considered important to frame evidence-based, consensus guidelines for the use of physicians.
METHODOLOGY
The process of pneumonia guidelines development was undertaken as a joint exercise by the Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, with sponsorship from two National Pulmonary Associations (Indian Chest Society and National College of Chest Physicians). The committee constituted for this purpose included representation of the two associations, and experts from other institutes and medical colleges including those from the Departments of Internal Medicine, Microbiology, Pharmacology, and Radiodiagnosis.
The methodology comprised desk-review followed by a joint workshop. The review of literature was performed by searching the electronic sources (PubMed, EmBase) using the free-text terms: pneumonia, CAP, VAP, HCAP, HAP. A total of 500 articles were reviewed in detail. All major international guidelines available from the Infectious Disease Society of America (IDSA), American Thoracic Society (ATS), British Thoracic Society (BTS), and European Respiratory Society (ERS) were also reviewed.
The search was conducted under four subgroups [A. Diagnosis of community-acquired pneumonia (CAP); B. Management of CAP; C. Diagnosis of hospital-acquired, healthcare-associated, and ventilator-associated pneumonia (HAP, HCAP, and VAP, respectively); D. Management of HAP, HCAP, and VAP], each with a Group Chair and a Rapporteur. Important questions were framed on the basis of discussions on issues with reference to the Indian context. The available evidence as well as the questions were circulated to all the group members before the joint workshop. Discussions for grading of evidence and recommendations were held in four different groups and thereafter together in the joint meeting of all the groups. Final decisions in the joint group were based on a consensus approach on the majority voting.
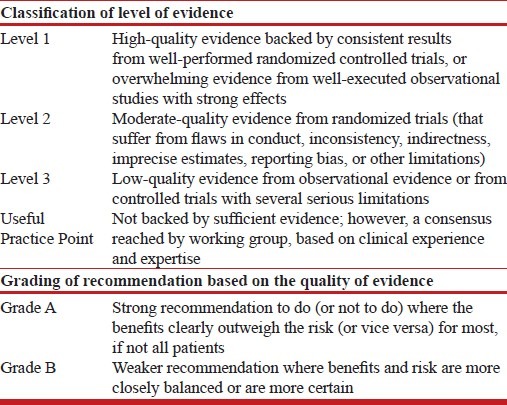
The modified grade system was used for classifying the quality of evidence as 1, 2, 3 or usual practice point (UPP) [Table 1].[1] The strength of recommendation was graded as A or B depending upon the level of evidence [Table 1]. Grade A recommendations in the guidelines should be interpreted as recommended and the grade B recommendations as suggested. While making a recommendation, the issues of practicality, costs, and feasibility in the country at different levels of healthcare was also taken into consideration.[2]
Table 1.
Classification of level of evidence and grading of recommendation based on the quality of evidence supporting the recommendation
The final document was reviewed by the committee members as well as by other external experts.
COMMUNITY-ACQUIRED PNEUMONIA
Definitions
What is the definition of CAP?
CAP can be defined both on clinical and radiographic findings. In the absence of chest radiograph, CAP is defined as: (a) symptoms of an acute lower respiratory tract illness (cough with or without expectoration, shortness of breath, pleuritic chest pain) for less than 1 week; and (b) at least one systemic feature (temperature >37.7°C, chills, and rigors, and/or severe malaise); and (c) new focal chest signs on examination (bronchial breath sounds and/or crackles); with (d) no other explanation for the illness (adapted from Ref[3])
When a chest radiograph is available, CAP is defined as: symptoms and signs as above with new radiographic shadowing for which there is no other explanation (not due to pulmonary edema or infarction).[3] Radiographic shadowing may be seen in the form of a lobar or patchy consolidation, loss of a normal diaphragmatic, cardiac or mediastinal silhouette, interstitial infiltrates, or bilateral perihilar opacities, with no other obvious cause.
Epidemiology and Etiology
What is the epidemiology of CAP in the world?
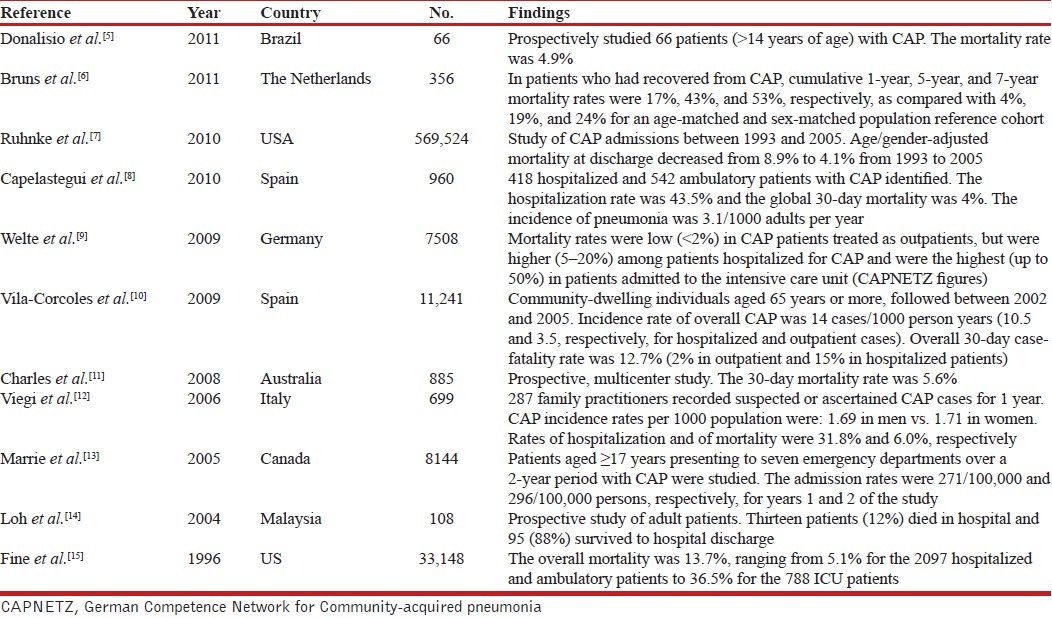
According to the CDC estimates, 1.1 million people in the US were hospitalized with pneumonia and more than 50,000 people died from the disease in 2009.[4] The epidemiological data from various countries are summarized in Table 2.[5–15]
Table 2.
Summary of studies on epidemiology of CAP from across the globe
What is the epidemiology of CAP in India?
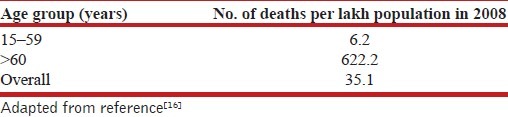
There are no large studies from India on the incidence of CAP, but mortality data on the total number of deaths caused by “lower respiratory tract infections” are available.[16] The number of deaths due to lower respiratory tract infections was 35.1/100,000 population in the year 2008 [Table 3] compared to 35.8/100,000 population for TB, while it was 194.9/100,000 for infectious and parasitic diseases. Thus, around 20% of the mortality due to infectious diseases in India is caused by lower respiratory tract infections. The reported mortality of CAP from India is similar to that reported elsewhere in the world. In one report of 150 patients admitted with CAP, 12 (8%) patients died in-hospital, while 4 (2.7%) succumbed within 30 days after discharge.[17] In another study on 72 consecutive patients with CAP over 18 months, 35% of elderly and 14% of young patients succumbed to fulminant sepsis or respiratory failure.[18] The mortality has been variably reported between 3.3% and 11% in other studies from India.[17,19,20]
Table 3.
WHO mortality figures for lower respiratory tract infections in India
What is the etiology of CAP worldwide?
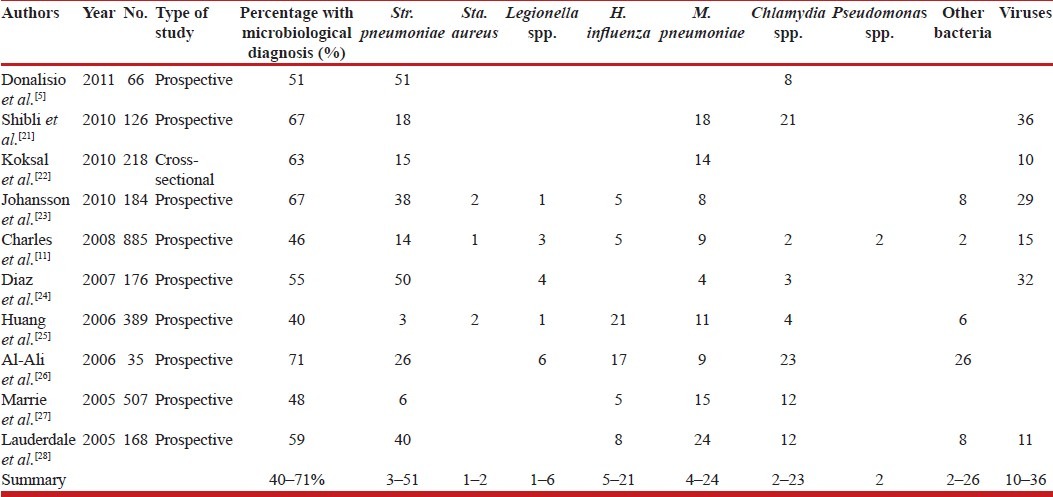
A microbiological diagnosis could be made in only 40-71% of cases of CAP [Table 4]. Streptococcus pneumoniae is the most common etiological agent, but the proportion in different studies is variable [Table 4].[5,11,21–28] Viruses are responsible for CAP in as much as 10–36% of the cases. The widespread antibiotic (mis)use is probably responsible for decreasing culture rates in CAP. In 2009, Medicare data from 17,435 patients hospitalized for CAP showed that an etiological agent was identified in 7.6% as opposed to >90% in the pre-penicillin era.[29]
Table 4.
Summary of studies reporting the etiology of CAP from various countries
What is the etiology of CAP in India?
There are very few Indian reports on the etiological agents of CAP. In a study of blood cultures performed in CAP, Str. pneumoniae (35.3%) was the most common isolate, followed by Staphylococcus aureus (23.5%), Klebsiella pneumoniae (20.5%), and Haemophilus influenzae (8.8%).[20] An earlier study also found Str. pneumoniae to be the most common cause (35.8%), but it also reported Mycoplasma pneumoniae in 15% of the microbiologically positive cases.[19] Legionella pneumophila is an important cause which is often not considered in the Indian setting. In a recent study, 27% of patients with CAP were serologically positive for this organism and around 18% demonstrated L. pneumophila antigenuria.[30] Mycoplasma was found to be the etiological agent in 35% of cases.[18] There are no large studies that have specifically addressed viruses as the cause of CAP apart from pandemic influenza H1N1 virus.
Is the etiology different in different population groups?
Elderly
Str. pneumoniae is the single most common organism identified in hospitalized elderly patients with CAP, accounting for 19–58% of cases.[31–33] H. influenzae was also frequently isolated (5–14%).[32–34] In most cases, the microbiological patterns observed in the elderly do not differ significantly from those of the younger populations.[33]
Chronic obstructive pulmonary disease (COPD)
COPD is a common comorbid condition in patients with CAP. It was the most common underlying comorbid condition among 40 cases (57%) in one study[19] and the second most common predisposing factor in another.[35] The spectrum of responsible microorganisms is largely similar to patients without COPD,[36,37] although the incidence of Pseudomonas aeruginosa and other Gram-negative bacilli may be increased in COPD.[38] COPD does not appear to increase the mortality of CAP.[39]
Alcoholism
Alcohol consumption increases the relative risk for CAP with a dose–response relationship.[40] Str. pneumoniae is found more frequently in patients with alcohol abuse.[34,41] The odds of bacteremic CAP are higher in these patients.[34] CAP was also more severe in alcoholics, but mortality is not different.[41] In contrast to the popular belief, no strong evidence was found to suggest increased prevalence of Klebsiella in alcohol users.
Diabetes mellitus
The etiological agents, the bacteremia or empyema rates are not different in diabetics compared to the non-diabetic population.[42] However, diabetes was significantly associated with higher mortality. Diabetes was also found to be more frequent in patients with bacteremic pneumococcal pneumonia compared to those with either non-bacteremic pneumococcal pneumonia or CAP of other etiologies.[43] Recent studies also suggest that pre-existing diabetes is associated with a higher mortality following CAP.[44,45] The proposed mechanism is due to worsening of pre-existing cardiovascular and kidney disease and not due to an altered immune response.[45] Diabetes is a frequently reported co-morbid condition in Indian reports.[17,19,35]
Risk factors for Pseudomonas pneumonia
Immunocompromised states, chronic respiratory disease, enteral tube feeding, cerebrovascular disease, and other chronic neurological disorders have all been found to be predictors of CAP due to P. aeruginosa.[46] In one study, the presence of a pulmonary comorbidity (which included chronic bronchitis, COPD, asthma, bronchiectasis, or others) was the strongest predictor of P. aeruginosa pneumonia.[47]
Diagnosis
What are the clinical features of CAP and what is their usefulness in diagnosis?
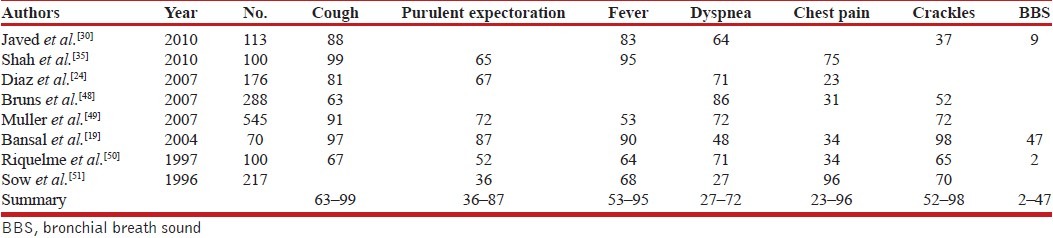
Common symptoms of CAP include fever, cough, sputum production, dyspnea, and pleuritic chest pain. Physical examination may reveal focal areas of bronchial breathing and crackles. The frequency of each symptom is quite variable [Table 5].[19,24,30,35,49,52–54] Bronchial breathing, despite being an important physical sign, does not find mention in most of these studies. Utility of the clinical signs either alone or in combination is debatable, and they are often found to lack sensitivity for the diagnosis of CAP.[52] Temperature >100.4°F, heart rate >110 beats/min, and pulse oximetric saturation <96% have been found to be strong predictors of CAP.[53] However, no single characteristic is adequately sensitive and specific to accurately discriminate CAP from viral illness.[49] Also, respiratory and non-respiratory symptoms associated with a pneumonic illness are less commonly reported by older patients with pneumonia.[54] Certain specific clinical syndromes may be associated with some atypical pathogens like Mycoplasma and Legionella.
Table 5.
Summary of studies analyzing the frequency of symptoms of CAP
What is the role of chest radiograph in the diagnosis of CAP?
A chest radiograph is the cornerstone for the diagnosis of CAP. In a study of 250 ambulatory patients with febrile respiratory tract infections, physicians’ judgment of pneumonia had a sensitivity of 74% (49–90%), specificity of 84% (78–88%), negative predictive value of 97% (94–99%), and a positive predictive value of 27% (16–42%) compared to the chest radiograph.[55] In low-risk patients with a reliable follow-up, chest radiographs are unnecessary for the diagnosis of CAP in the presence of normal vital signs and physical examination findings.[56] A diagnosis of CAP can be suspected if at least one of the following findings is present on the chest radiograph: (i) an asymmetric increase in lung opacification with air bronchogram; (ii) presence of silhouette sign; (iii) an area of increased opacity bounded by a well-defined interface against adjacent aerated lung (such as along a fissure); (iv) if only an anterior–posterior view is obtained (such as a portable examination), increased attenuation of the cardiac shadow; and (v) for radiographs with widespread airspace disease, more asymmetric or multifocal distribution of opacification.[57] There is fair to good inter-observer reliability between radiologists in identifying the presence of infiltrate, multilobar disease, and pleural effusion.[58] A chest radiograph is also helpful in differentiating CAP from other causes of acute respiratory symptoms like pulmonary edema, pulmonary infarction, pleural effusion, or tuberculosis.
Importantly, resolution of chest radiograph findings may lag behind clinical cure during follow-up, and up to 50% of patients may not show complete radiographic resolution at 4 weeks.[48] Radiographic resolution may be delayed in the elderly.[59] Patients with radiologic deterioration would almost always have one or the other clinical feature suggestive of clinical failure (persistent fever, abnormal auscultatory findings, or persistent tachypnea).[60] In the presence of such clinical indicators, it becomes essential to obtain a chest radiograph. Lack of partial radiographic resolution by 6 weeks, even in asymptomatic patients, would require consideration of alternative causes (e.g. endobronchial obstruction or non-infectious causes like pulmonary vasculitis, organizing pneumonia, and others).[61]
Recommendations:
Wherever feasible, a chest radiograph should be obtained in all patients suspected of having CAP (1A).
In the absence of availability of chest radiograph, patients may be treated on the basis of clinical suspicion (3A).
Chest radiograph should be repeated if the patient is not improving and also for all those patients who have persistence or worsening of symptoms/physical signs or those in whom an underlying malignancy needs to be excluded. It is not routinely necessary to repeat a chest radiograph in patients who have improved clinically (2A).
What is the role of computed tomography (CT) in the diagnosis of CAP?
High-resolution CT (HRCT) findings of CAP include air space consolidation, ground-glass attenuation, and thickening of the bronchovascular bundle.[62] In a retrospective study of 75 patients with pneumococcal pneumonia, consolidation (84%) was the most frequently observed finding followed by ground-glass opacity (82.7%), bronchial wall thickening (61.3%), and centrilobular nodules (49.3%). Airway dilatation (21.6%), pleural effusion (33.3%), lymphadenopathy (34.8%), and pulmonary emphysema (21.3%) were also observed.[63] Centrilobular nodules favored non-bacterial pneumonia, while airspace nodules were more common with bacterial pneumonia (specificities of 89% and 94%, respectively) when located in the outer lung areas.[64] When centrilobular nodules were the principal finding, they were specific but lacked sensitivity for non-bacterial pneumonia (specificity 98% and sensitivity 23%). CT could discriminate bacterial pneumonia from non-bacterial pneumonia with a sensitivity and specificity of 70% and 84%, respectively. Thus, HRCT findings are not sufficient for tailoring antibiotic treatment. A CT chest may, however, be useful in the diagnosis of complications of pneumonia like lung abscess and empyema. In up to 27% of cases, pneumonia might be demonstrated on CT with a negative or non-diagnostic chest radiograph.[65] However, studies that have investigated clinical interventions and treatment decisions based on HRCT findings compared to chest radiography are lacking. Therefore, the clinical utility of a CT chest in patients with suspected CAP and a negative chest radiograph remains unclear. Besides, CT scanning is an expensive, resource-intensive diagnostic modality with limited availability, and entails the risk of high radiation exposure.
Recommendations:
CT of the thorax should not be performed routinely in patients with CAP (2A).
CT of the chest should be performed in those with non-resolving pneumonia and for the assessment of complications of CAP (2A).
Which microbiological investigations need to be performed in CAP?
Blood cultures
Blood cultures have a low sensitivity but high specificity in identifying the microbial etiology. The yield of blood cultures ranged between 5% and 33% in various small studies.[66–72] In a large study of 25,805 Medicare patients, bacteremia was detected in 7% of patients and 5% of all patients had at least one contaminated blood culture.[73] In a systematic review, blood cultures were true-positive in 0–14% of cases.[74] They led to antibiotic narrowing in 0–3% and change in antibiotic because of a resistant organism in 0–1% of patients. Despite the low yield of blood culture, the microbial etiology of CAP is identified in a significant proportion of patients with this investigation.
Recommendations:
Blood cultures should be obtained in all hospitalized patients with CAP (2A).
Blood cultures are not required in routine outpatient management of CAP (2A).
Sputum Gram stain and cultures
The yield of sputum cultures varies from 34 to 86%.[75,76] In a meta-analysis of 12 studies, the sensitivity and specificity of sputum Gram stain was 15–100% and 11–100%, respectively, in the diagnosis of pneumococcal CAP, compared to sputum culture.[77] Despite a low sensitivity, Gram stain of sputum is useful as it provides rapid results and can help narrow down the etiology. Twenty to 40 fields from sputum smear should be examined microscopically under low power. The number of epithelial cells in representative fields that contain cells should be averaged. If epithelial cells are >10/low power field, the sample should be rejected for culture. If the number of pus cells is 10 times the number of epithelial cells with 3+ to 4+ of a single morphotype of bacteria, the specimen should be accepted for culture.[78]
[Refer to the section on hospital-acquired pneumonia for discussion of various invasive techniques for the collection of respiratory specimens]
Recommendations:
An initial sputum Gram stain and culture (or an invasive respiratory sample as appropriate) should be obtained in all hospitalized patients with CAP (2A).
Sputum quality should be ensured for interpreting Gram stain results (2A).
Sputum for acid-fast bacilli (AFB) should be obtained as per RNTCP guidelines for non-responders (UPP).
Pneumococcal antigen detection
Pneumococcal antigen can be detected in the urine using proprietary rapid immunochromatographic membrane tests. The sensitivity ranges from 65 to 80% compared to gold standard (Gram stain of sputum or cultures of sputum and blood).[79–81] As all empiric treatment regimens are designed to cover Str. pneumoniae, the test only confirms a pneumococcal etiology without any significant change in the treatment protocol. Considering the cost and availability of the test, it may not have a favorable cost–benefit ratio.
Recommendation:
Pneumococcal antigen detection test is not required routinely for the management of CAP (2A).
Pneumococcal PCR
Pneumococcal PCR has a poor sensitivity. In a recent meta-analysis (22 studies), the summary sensitivity and specificity for pneumococcal PCR (pneumococcal bacteremia as case and healthy people or patients with bacteremia caused by other bacteria as controls) in blood was 57.1% (95% CI, 45.7–67.8%) and 98.6% (95% CI, 96.4–99.5%), respectively.[82]
Recommendation:
Pneumococcal PCR is not recommended as a routine diagnostic test in patients with CAP (1A).
Legionella antigen detection
The pooled sensitivity and specificity of various assays for Legionella urinary antigen detection is 0.74 (95% CI, 0.68–0.81) and 0.991 (95% CI, 0.98–0.997), respectively.[83] In one study, the treatment was altered in more than half the patients from results of the Legionella urinary antigen test.[84] Legionella is an important causative agent of CAP in India. As the sensitivity is relatively low, a negative test does not rule out the possibility of Legionella pneumonia. A positive test is highly specific and potentially changes the duration of antibiotic therapy.
Recommendation:
Legionella urinary antigen test is desirable in patients with severe CAP (1B).
Other atypical pathogens
Mycoplasma, Chlamydia, and respiratory viruses are important etiological agents of pneumonia. However, culture techniques for Mycoplasma pneumoniae are not only insensitive but also time consuming (2–5 weeks).[85] Serological assays, especially the complement fixation test, are widely used. The sensitivity of these assays varies depending on the timing of collection of the serum sample and the availability of paired serum samples (collected at an interval of 2–3 weeks). IgM assays are more sensitive, but IgM response may be absent in adults.[86] PCR based tests done in respiratory samples are rapid, but a recent review found sensitivity of only 62% compared to serological methods.[87] Chlamydophila pneumoniae is very difficult to grow in the laboratory, and the usefulness of serology for the diagnosis of acute infections by C. pneumoniae is doubtful.[88] The micro-immunofluorescence test is currently considered the gold standard for the serodiagnosis of C. pneumoniae infection. There is, however, a high rate of false-positive and false-negative test results, attributed to delayed and unpredictable development of IgM and IgG, and lack of standardized methods.[89] Molecular diagnostic techniques like PCR are not widely available and not appropriately validated. If Legionella, M. pneumoniae, and C. pneumoniae are considered, only Legionella spp. are associated with significant mortality.[90] Due to empiric coverage and a widely favorable outcome for atypical agents, testing for Mycoplasma and Chlamydia in patients with mild to moderate CAP might not be required. Besides, there are no well-validated rapid tests for Mycoplasma and Chlamydia.[29] Although serological and PCR-based tests are available for respiratory viruses, they seldom have any bearing on the management of the patient from influenza. Reverse transcriptase PCR (RT-PCR) is a rapid and accurate method for the detection of influenza virus infection,[91] but is not routinely required except in the setting of an outbreak.
Recommendation:
Investigations for atypical pathogens like Mycoplasma, Chlamydia, and viruses need not be routinely done (2A).
What general investigations are required in patients with CAP?
General
Apart from a chest radiograph, there are few investigations required for outpatient management. Use of pulse oximetry increases the detection of arterial hypoxemia.[92] Arterial saturation ≤90% has good specificity but low sensitivity for adverse outcomes in CAP, and complements clinical severity scoring.[93] In admitted patients, it is a usual practice to perform plasma glucose, urea, and electrolytes, complete blood count, and liver function tests. Urea also forms a part of CURB-65 score for severity assessment. A delay in oxygenation assessment of >1 h is associated with an increase in time to first antibiotic dose, and a delay in oxygenation assessment of >3 h is associated with an increased risk of death in patients admitted to the intensive care unit (ICU).[94]
Recommendations:
For patients managed in an outpatient setting, no investigations are routinely required apart from a chest radiograph (3A).
Pulse oximetry is desirable in outpatients (2B).
Pulse oximetric saturation, if available, should be obtained as early as possible in admitted patients (2A). Arterial blood gas analysis should be performed in those with an oxygen saturation ≤90% and in those with chronic lung disease (3A).
Blood glucose, urea, and electrolytes should be obtained in all hospitalized patients with CAP (3A).
Full blood count and liver function tests are also helpful in the management of patients with CAP (3B).
Role of biomarkers
In most instances, the diagnosis of CAP is made with certainty based on clinical features and chest radiograph findings. However, CAP can occasionally be confused with pulmonary edema or pulmonary embolism. Also, it is difficult to differentiate CAP of viral etiology from that of bacterial etiology. Biomarkers like procalcitonin (PCT) and C-reactive protein (CRP) may be of some value in resolving these issues. PCT levels rise in many inflammatory conditions and more so in bacterial infections. PCT can be considered as an adjunct to clinical acumen.[95] Although PCT cannot be used as a sole marker for taking decisions of initiating antibiotics, it can be helpful in differentiating the presence or absence of bacterial CAP.[96–98] As PCT is not a marker of early infection (increases after 6 h), a single value may be falsely low and serial values should be obtained to guide antibiotic use in the course of a suspected infective illness. Certain studies have also shown a role for CRP as a diagnostic marker for CAP.[99,100] CRP levels can independently distinguish pneumonia from exacerbations of asthma, and CRP levels have been used to guide antibiotic therapy and reduce antibiotic overuse in hospitalized patients with acute respiratory illness.[101] On the contrary, a systematic review concluded that additional diagnostic testing with CRP is unlikely to alter management decisions such as antibiotic prescribing or referral to hospital.[102]
Recommendation:
PCT and CRP measurement need not be performed as routine investigations for the diagnosis of CAP (2A).
Risk Stratification
Should patients with CAP be risk stratified?
The risk assessment of patients with CAP is important for a number of reasons. There is a possibility of adverse outcomes if the initial assessment is not rigorous. On the contrary, one can argue that all patients of CAP should be admitted and treated. However, the high costs of admission and risk of hospital-acquired infections preclude routine admission.[103] Hence, there is a need for risk stratification to decide the site of care and future course of management.
What are the various methods of risk stratification?
There are various scores [Table 6] for assessing the risk in a patient with CAP: pneumonia severity index (PSI), CURB-65, CRB-65, SMART-COP, SMRT-CO, A-DROP, and others.
Pneumonia severity index (PSI)
The PSI is a prognostic prediction rule that defines the severity of illness based on predicted risk of mortality at 30 days.[104] It includes 20 prognostic variables to stratify the risk of death due to CAP into five classes. The mortality risk increases with the increase in class, ranging from 0.4% in class I to 31% with class V. The strengths of the PSI include the rigorous methodology used to derive the score, the reproducibility and the generalizability of the score, and the actual change in the treatment decision based on the score.[105] The limitations are its unwieldiness of use, especially in busy emergencies and outpatient departments, overstress on certain variables, and neglect of social and other important medical factors.[104,106,107]
CURB-65
This score was derived from the pooled data of three large studies on CAP carried out in the United Kingdom, New Zealand, and the Netherlands. Based on this, a 6-point score {Confusion, Urea ≥7 mmol/L, Respiratory rate ≥30 breaths/min, low Blood pressure [diastolic blood pressure (DBP) ≤60 mm Hg or systolic blood pressure (SBP) ≤90 mm Hg], age ≥65 years) was derived, which allowed patients to be stratified according to increasing risk of mortality ranging from 0.7% (score 0) to 40% (score 4).[106] A further model based only on clinical features available from a clinical assessment without laboratory results (confusion, respiratory rate, blood pressure, and age; CRB-65 score) was also tested and found to correlate well with the risk of mortality and need for mechanical ventilation.[108] The CURB-65 and CRB-65 stratified mortality is more clinically useful than the systemic inflammatory response syndrome (SIRS) criteria or the standardized early warning score (SEWS).[109] CURB-65 implementation led to a decrease in antibiotic use without affecting mortality, treatment failure, or clinical response.[110] Also, lack of application of the CURB-65 score led to overtreatment of low-risk patients.[111] CURB-65 was, however, found to be less useful in the age group >65 years compared those below 65 years.[112] Hence, CURB-65 can be supplemented with clinical judgment and/or pulse oximetry.[113–117] In a meta-analysis of 397,875 patients, CRB-65 performed well in stratifying the severity of pneumonia and the resultant 30-day mortality in hospital settings, while it appeared to overpredict the probability of 30-day mortality across all strata of predicted risk in community settings.[118] CRB-65 had an acceptable ability to classify mortality risk in the age group >65 years; patients with CRB-65 ≤1 had a relatively small mortality rate, which suggested that they could be managed as outpatients.[119] The CURB-65 and CRB-65 scores are not as extensively validated as the PSI; however, they are recommended by most societies for the initial assessment and risk stratification of CAP.[3,103,120]
SMART-COP
This score was derived from the Australian CAP Study (ACAPS) of 882 episodes of CAP and was further validated in five external databases, totaling 7464 patients. The SMART-COP is a point-based severity score, consisting of low systolic blood pressure (2 points), multilobar chest radiography involvement (1 point), low albumin level (1 point), high respiratory rate (1 point), tachycardia (1 point), confusion (1 point), poor oxygenation (2 points), and low arterial pH (2 points). A SMART-COP score of ≥3 points identified 92% of patients who received invasive respiratory and vasopressor support.[115]
ATS-IDSA criteria
These criteria are helpful in deciding the level of care (ward vs. ICU) once the admission decision has been made. There are two major and nine minor criteria, and the presence of any of the major criteria or at least three of the minor criteria qualifies for an ICU admission [Table 6].[103] An early transfer to the ICU of a severely ill CAP patient is associated with appropriate utilization of resources and decreased mortality.[103] Most studies have validated the use of these criteria for predicting ICU admission;[121–126] however, there are doubts regarding the use of minor criteria alone in predicting risk.[122,126]
Other criteria
These include the A-DROP, REA-ICU index, CAP-PIRO, and others.[44,68,117,127–135] However, these indices are not as extensively validated as the ones discussed previously and need further validation before being accepted.
What should be the optimum method of risk stratification?
There have been multiple studies comparing these indices.[17,115–117,127,131,136–160] A prospective study from India of 150 patients comparing PSI and CURB-65 found both PSI and CURB-65 to possess equal sensitivity in predicting death from CAP while the specificity of CURB-65 was higher than that of PSI. PSI was more sensitive than CURB-65 in predicting ICU admission.[17] One study found PSI to be the best in stratifying low-risk patients with no difference in overall test performance,[152] while another study comparing PSI, CURB-65, CURB, and CRB-65 found that all four scales had good negative predictive values for mortality in populations with a low prevalence of death but were less useful with regard to positive predictive values.[153] Hence, these indices are more useful in screening out low-risk patients. The use of oxygen saturation or partial pressure of oxygen in blood has been found to be an independent predictor of morbidity and mortality in CAP.[115–117]
Recommendations:
Patients with community-acquired pneumonia should be risk stratified (1A).
Risk stratification should be performed in two steps [Figure 1] based upon the need for hospital admission followed by assessment of the site of admission (non-ICU vs. ICU). Accordingly, patients can be managed as either outpatient or inpatient (ward or ICU) (1A).
Initial assessment should be done with CRB-65. If the score is >1, patients should be considered for admission (1A).
Clinical judgment should be applied as a decision modifier in all cases (3A).
Pulse oximetry can be used to admit hypoxemic patients (2A). Hypoxemia is defined as pulse oximetric saturation ≤92% for age ≤50 years and ≤90% in patients aged >50 years (3A).
Patients selected for admission can be triaged to the ward (non-ICU)/ICU based upon the major/minor criteria outlined in Table 6(2A).
If any major criterion or ≥3 minor criteria are fulfilled, patients should generally be admitted to the ICU (1A).
Antibiotic Use
Which are the antibiotics useful for empiric treatment in various settings?
The initial empiric antibiotic treatment is based on a number of factors: (a) the most likely pathogen(s); (b) knowledge of local susceptibility patterns; (c) pharmacokinetics and pharmacodynamics of antibiotics; (d) compliance, safety, and cost of the drugs; and (e) recently administered drugs.
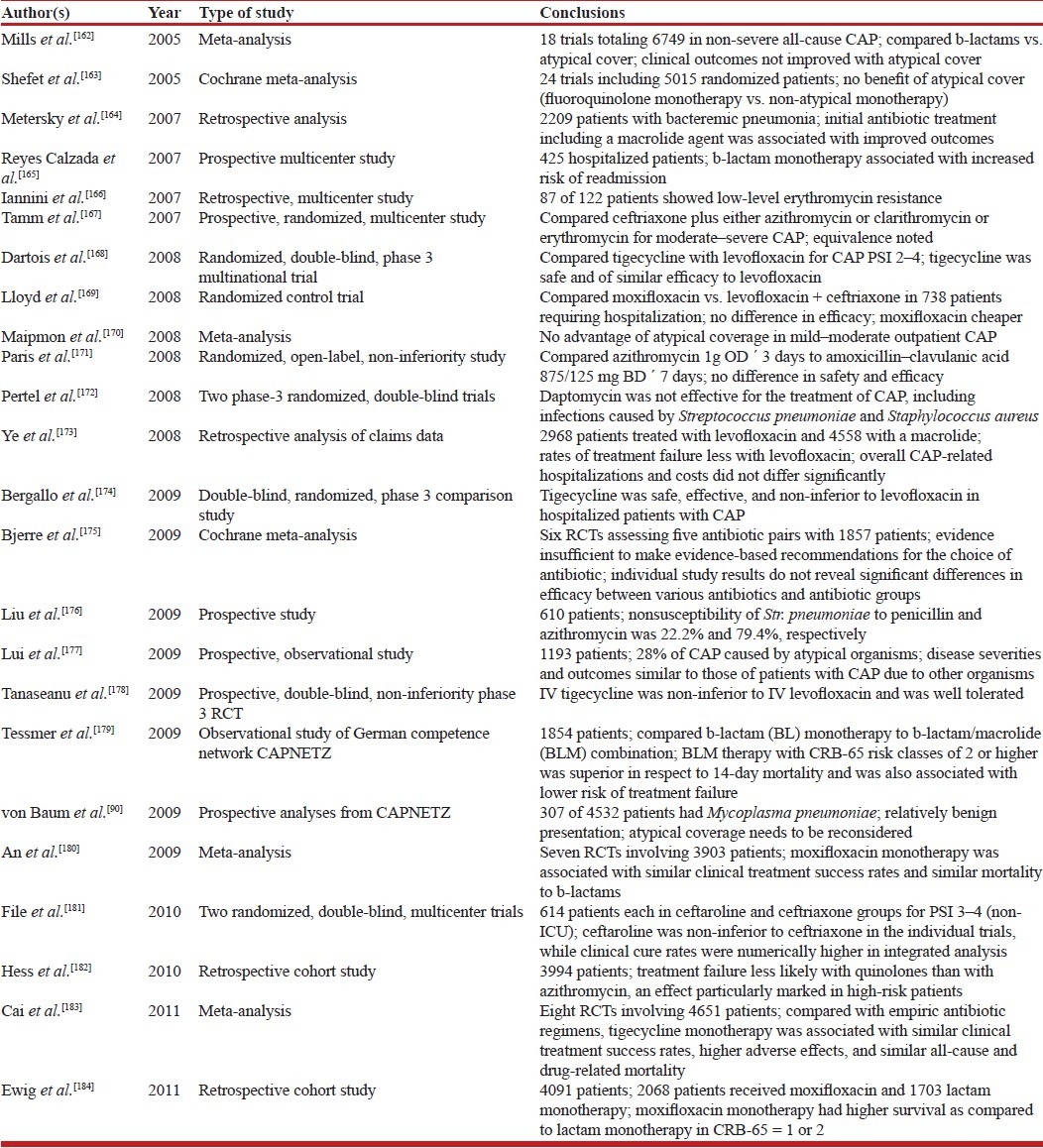
The empiric antibiotic treatment is primarily aimed at Str. pneumoniae as it is the most prevalent organism in CAP. The Indian data show a good response of Str. pneumoniae to commonly administered antibiotics.[17,161] Various studies have shown results favoring different groups of antibiotics [Table 7].[165–169,171–174,178–184] The evidence does not support the choice of any particular antibiotic since individual study results do not reveal significant differences in efficacy between various antibiotics and antibiotic groups.[175] The commonly used antibiotics are either β-lactams or macrolides.
Table 7.
Summary of studies on choice of antibiotics for treatment of CAP
Is there a need to cover atypical organisms?
Atypical organisms, especially Mycoplasma, Chlamydia, and Legionella, also contribute significantly to the incidence of CAP. However, the need for empiric treatment of these organisms in mild CAP in the outpatient setting has been challenged as evidence suggests no benefit of covering these organisms with appropriate antibiotics in the outpatient setting.[90,162,163,170,176,177] Combination therapy should be restricted to patients with severe pneumonia.[103,120] Its advantages include expansion of the antimicrobial spectrum to include atypical pathogens and possibly immunomodulation. Combination therapy in patients with severe pneumonia has been shown to decrease mortality.[185–192] Monotherapy suffices for less severe pneumonia treated on outpatient basis. Indications for combination therapy are given in Table 8. Oral macrolides should be used with caution in the elderly as their use has been associated with increased cardiovascular mortality.[193]
What is the role of fluoroquinolones in empiric treatment of CAP in India?
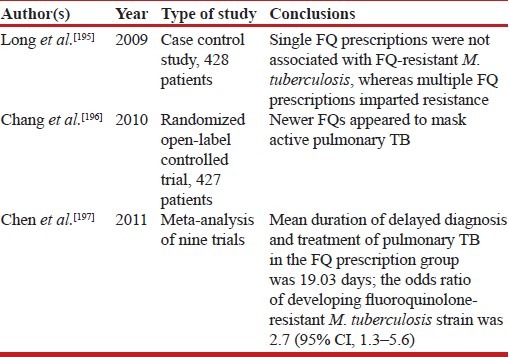
Fluoroquinolones have been recommended in various guidelines for the empiric treatment of CAP.[3,103,120] Although there is significant antimicrobial efficacy of fluoroquinolones,[169,173,180,182,184,194] all studies have been carried out in low prevalence settings of tuberculosis. There is enough evidence to suggest that fluoroquinolone use is associated with masking of tubercular infection and increased risk of drug resistance to M. tuberculosis [Table 9].[195–199] Therefore, the indiscriminate empiric use of these drugs for the treatment of CAP in India should be discouraged.
Table 9.
Summary of studies on the use of fluoroquinolones (FQs) in CAP
What should be the time to first antibiotic dose?
Intuitively, antibiotics should be started as soon as possible after the diagnosis of CAP is established. In severe CAP, antibiotics should be administered as soon as possible, preferably within 1 hour.[200] In non-severe CAP, a diagnosis should be established before starting antibiotics.[201–205]
Recommendations:
Antibiotics should be administered as early as possible; timing is more important in severe CAP (2A).
Outpatient setting
-
2.
Therapy should be targeted toward coverage of the most common organism, namely Str. pneumoniae (1A).
-
3.
Outpatients should be stratified as those with or without comorbidities (3A).
-
4.
Recommended antibiotics [Table 10] are oral macrolides (e.g. azithromycin and others) or oral β-lactams (e.g. amoxicillin 500–1000 mg thrice daily) for outpatient without comorbidities (1A).
-
5.
For outpatients with comorbidities [Table 8], oral combination therapy is recommended (β-lactams plus macrolides) (1A).
There is insufficient evidence to recommend tetracyclines (3B).
Fluoroquinolones should not be used for empiric treatment (1A).
Antibiotics should be given in appropriate doses to prevent emergence of resistance (1A).
Inpatient, non-ICU
-
9.
The recommended regimen is combination of a β-lactam plus a macrolide (preferred β-lactams include cefotaxime, ceftriaxone, and amoxicillin–clavulanic acid) (1A).
-
10.
In the uncommon scenario of hypersensitivity to β-lactams, respiratory fluoroquinolones (e.g. levofloxacin 750 mg daily) may be used if tuberculosis is not a diagnostic consideration at admission (1A). Patients should also undergo sputum testing for acid-fast bacilli simultaneously if fluoroquinolones are being used in place of β-lactams.
-
11.
Route of administration (oral or parenteral) should be decided based upon the clinical condition of the patient and the treating physician's judgment regarding tolerance and efficacy of the chosen antibiotics (3A).
Inpatient, ICU
-
12.
The recommended regimen is a β-lactam (cefotaxime, ceftriaxone, or amoxicillin–clavulanic acid) plus a macrolide for patients without risk factors for P aeruginosa (2A).
-
13.
If P. aeruginosa is an etiological consideration, an antipneumococcal, antipseudomonal antibiotic (e.g. cefepime, ceftazidime, cefoperazone, piperacillin–tazobactam, cefoperazone–sulbactam, imipenem, or meropenem) should be used (2A). Combination therapy may be considered with addition of aminoglycosides/antipseudomonal fluoroquinolones (e.g. ciprofloxacin) (3A). Fluoroquinolones may be used if tuberculosis is not a diagnostic consideration at admission (1A). Patients should also undergo sputum testing for acid-fast bacilli simultaneously if fluoroquinolones are being used.
-
14.
Antimicrobial therapy should be changed according to the specific pathogen(s) isolated (2A).
-
15.
Diagnostic/therapeutic interventions should be done for complications, e.g. thoracentesis, chest tube drainage, etc. as required (1A).
-
16.
If a patient does not respond to treatment within 48–72 h, he/she should be evaluated for the cause of non-response, including development of complications, presence of atypical pathogens, drug resistance, etc. (3A).
Treatment Protocol
What is the optimum duration of treatment?
Outpatients are effectively treated with oral antibiotics. Most non-severe infections would settle within 3–5 days. In ward patients, oral therapies may be given with a functional gastrointestinal tract, although initially the intravenous route is preferable. Patients may be switched to oral medications as soon as they improve clinically and are able to ingest orally. Early conversion to oral antibiotic is as effective as continuous intravenous treatment in moderate to severe CAP and results in substantial reduction in the duration of hospitalization.[103,206] Most patients respond within 3–7 days; longer durations are not required routinely. Also, short course treatment (≤7 days) has been found to be as effective as longer duration treatment, with no difference in short-term or long-term mortality, or risk of relapse or treatment failure.[207–209] Short-course treatment may, however, be suboptimal in certain situations such as meningitis or endocarditis complicating pneumonia, pneumococcal bacteremia, community-acquired methicillin-resistant Sta. aureus and atypical pathogens. Adequate studies on this issue are lacking and decisions have to be individualized in the clinical context.[3,103,120]
When should patients be discharged?
Discharge may be contemplated when the patient starts taking oral medications, is hemodynamically stable, and there are no acute comorbid conditions requiring medical care. At least three recent meta-analyses have shown that short-term treatment (5–7 days) is as effective as conventional treatment (10–14 days), with decrease in the risk of adverse effects, duration of hospitalization, and no increase in mortality.[206,208,209]
Recommendations:
Switch to oral from intravenous therapy is safe after clinical improvement in moderate to severe CAP (2A).
Patients can be considered for discharge if they start accepting orally, are afebrile, and are hemodynamically stable for a period of at least 48 h (2A).
Outpatients should be treated for 5 days and inpatients for 7 days (1A).
Antibiotics may be continued beyond this period in patients with bacteremic pneumococcal pneumonia, Sta. aureus pneumonia, and CAP caused by Legionella pneumoniae and non–lactose-fermenting Gram-negative bacilli (2A). Antibiotics may also be continued beyond the specified period in those with meningitis or endocarditis complicating pneumonia, infections with enteric Gram-negative bacilli, lung abscess, empyema, and if the initial therapy was not active against the identified pathogen (3A).
Role of Biomarkers
The role of biomarkers as a means to guide the duration of antibiotic treatment has been in focus recently, with a slew of studies on this aspect. However, the methodology has hardly been consistent. Data for limiting the duration of treatment are insufficient. A single procalcitonin value at admission led to a reduction in the duration of antibiotics without a change in the mortality.[210] Same conclusions were arrived at in two meta-analyses.[211,212] Some biomarkers, especially procalcitonin, show promise, but data are still not available on the adequate use of these molecules.
Recommendation:
Biomarkers should not be routinely used to guide antibiotic treatment as this has not been shown to improve clinical outcomes (1A).
Adjunctive Therapies
What is the role of steroids?
Few studies advocate the use of steroids in severe CAP.[213–216] Other studies have argued against the use of steroids.[217–220] In a study of 213 patients, prednisolone 40 mg daily for 1 week did not improve outcome in hospitalized patients.[219] In a recent trial of dexamethasone in 304 patients, the use of dexamethasone reduced the length of hospital stay when added to antibiotic treatment in non-immunocompromised patients with mild to moderate CAP (6.5 vs. 7.5 days).[216] There is some benefit of steroids in CAP, but there is no significant reduction in mortality, and the increased risk of arrhythmias, upper gastrointestinal bleeding, and malignant hypertension may be possibly related to corticosteroids.[221] The use of glucocorticoids should be limited to patients with vasopressor-dependent septic shock and patients with early acute respiratory distress syndrome.[222–226]
What is the role of other adjunctive therapies?
There is no evidence to suggest the usefulness of treatments such as activated protein C, anticoagulants, immunoglobulin, granulocyte colony-stimulating factor, statins, probiotics, chest physiotherapy, antiplatelet drugs, cough medications, inhaled nitric oxide, angiotensin-converting enzyme inhibitors, and others in the routine management of CAP.[215,227–229] Noninvasive ventilation appears to be beneficial, and has the potential to reduce endotracheal intubation, shorten the ICU stay, and reduce the risk of death in the ICU if applied early in the course of CAP.[230]
Should ARDS/septic shock due to CAP be treated differently?
Patients with ARDS and septic shock secondary to CAP should be managed according to standard guidelines.[200,231] Noninvasive ventilation should be judiciously used in patients with ARDS.[232]
Recommendations:
Steroids are not recommended for use in non-severe CAP (2A).
Steroids should be used for septic shock or in ARDS secondary to CAP according to the prevalent management protocols for these conditions (1A).
There is no role of other adjunctive therapies (anticoagulants, immunoglobulin, granulocyte colony-stimulating factor, statins, probiotics, chest physiotherapy, antiplatelet drugs, over-the-counter cough medications, β2 agonists, inhaled nitric oxide, and angiotensin-converting enzyme inhibitors) in the routine management of CAP (1A).
CAP-ARDS and CAP leading to sepsis and septic shock should be managed according to the standard management protocols for these conditions (1A).
Noninvasive ventilation may be used in patients with CAP and acute respiratory failure (2A).
Immunization
What is the role of immunization for prevention of CAP?
Most guidelines recommend immunization with pneumococcal and seasonal influenza vaccines for specific groups.[3,103,120] However, the adult immunization guidelines promulgated by the Association of Physicians in India do not recommend the use of these vaccines on a routine basis.[233] Pneumococcal vaccination (preferably at least 2 weeks prior to splenectomy) and one-time revaccination after 5 years was recommended in patients undergoing splenectomy. There was no evidence to support the efficacy of pneumococcal vaccine in preventing invasive pneumococcal disease in populations considered at high risk, particularly healthy individuals aged ≥65 years living in institutions, patients suffering from chronic organ failure, patients with diabetes mellitus, nephrotic syndrome, or immunodeficiency. Pneumococcal vaccination has never been shown to consistently reduce the incidence of pneumococcal pneumonia; however, the incidence of invasive pneumococcal bacteremic disease is reduced.[234–245] Considering this, the use of pneumococcal vaccination is recommended in special high-risk groups [Table 11] but not as a routine in immunocompetent adults. Influenza vaccination is recommended routinely in all persons greater than 6 months of age. However, the success of vaccination depends on the presence of the prevalent strain in the vaccine. The use of influenza vaccination is based on the availability of regular data regarding the prevalent strains. There is insufficient data regarding the use of influenza vaccination in adults greater than 65 years of age.[246,247] The vaccine is especially recommended in high-risk groups.[236,242,246–250]
Recommendations:
Routine use of pneumococcal vaccine among healthy immunocompetent adults for prevention of CAP is not recommended (1A). Pneumococcal vaccine may be considered for prevention of CAP in special populations who are at high risk for invasive pneumococcal disease [Table 11] (2A).
Influenza vaccination should be considered in adults for prevention of CAP (3A).
Smoking cessation should be advised for all current smokers (1A).
HOSPITAL-ACQUIRED PNEUMONIA (HAP)/VENTILATOR-ASSOCIATED PNEUMONIA (VAP)
Definitions
What is the definition of hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP)?
HAP is an inflammatory condition of the lung parenchyma, caused by infectious agents, neither present nor incubating at the time of hospital admission. It is defined as pneumonia developing 48 h after admission to the hospital.[251,252] HAP can further be classified as ICU HAP or non-ICU HAP depending upon whether this infection is acquired in the intensive care unit (ICU) or in other clinical areas (e.g. wards).[253] VAP is defined as pneumonia that develops in patients after 48 h of endotracheal intubation.[251,252] Patients who develop pneumonia while being assisted with non-invasive ventilation (NIV) are considered to have HAP rather than VAP as the upper airway defense mechanisms remain intact.
What is healthcare-associated pneumonia (HCAP)? Is it a distinct entity?
HCAP is a heterogeneous entity which includes pneumonia that occurs in the following patient populations: hospitalization in an acute care hospital for two or more days within 90 days of the infection, residence in a nursing home or long-term care facility, recent intravenous antibiotic therapy, chemotherapy, or wound care within 30 days of the current infection, and attendance at a hemodialysis clinic.[252] However, the definition of HCAP is not as well standardized or accepted as that of HAP or VAP. There is heterogeneity in defining HCAP amongst various studies and guidelines.[254]
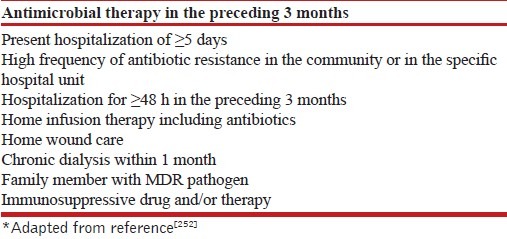
Whether HCAP is a separate entity or a subgroup of CAP or HAP is currently unclear. This is further complicated by variability in defining HCAP in various studies. For example, the duration of preceding hospitalization has ranged from 30 to 360 days in various definitions.[254] Moreover, limited evidence exists on the relationship between prior antibiotic usage and prevalence of multidrug resistant (MDR) pathogens among individuals treated in primary care settings. Healthcare facilities and nursing homes cannot be considered a homogeneous environment with comparable prevalence of MDR pathogens. In the West, nursing homes generally provide long-term basic nursing and medical care with the option of further support if necessary. Similar healthcare establishments are rather uncommon in India. In the Indian setting, nursing homes generally represent private hospitals with smaller infrastructure. Nursing homes in India cannot be routinely considered as a risk factor for drug-resistant pathogens in all patients. Hence, the classification of HCAP is avoided in this document, and the selection of antimicrobial treatment should be judged on an individual basis.[255] The risk factors for acquiring infection with MDR pathogens are enumerated in Table 12.
Table 12.
Risk factors for infection with MDR bacteria
Recommendation:
The risk stratification regarding acquisition of MDR pathogen should be individualized rather than using an umbrella definition of HCAP for this purpose (UPP).
Epidemiology
What is the burden and epidemiology of HAP/VAP?
HAP is the second most common nosocomial infection.[256] It is associated with a high morbidity and mortality. It prolongs the hospital stay and increases the cost of treatment. Overall burden is estimated at 5–10 cases per 1000 hospital admissions with a 6–20-fold increased risk of acquiring HAP/VAP in the mechanically ventilated patient.[257–259] HAP accounts for up to 25% of all ICU infections and more than 50% of the entire antibiotic prescriptions. The crude mortality rate for HAP may be as high as 30–70%, and attributable mortality has been estimated to vary between 33 and 50% in several studies.[252,260,261] The risk of HAP/VAP is the highest early in the course of hospital stay. The risk of developing VAP is estimated at around 3% per day during the first 5 days of ventilation, 2% per day during days 5–10 of ventilation, and 1% per day thereafter.[262,263] Approximately half of all episodes of VAP occur within the first 4 days of mechanical ventilation. The intubation process itself contributes to the risk of infection as evidenced by low occurrence of HAP in those noninvasively ventilated.[264]
The time of onset of pneumonia is an important epidemiologic consideration for acquisition of specific pathogens and outcomes in HAP. Early-onset HAP (and VAP) is defined as pneumonia occurring within the first 4 days of hospitalization (or endotracheal intubation).[265] It usually carries a better prognosis and is more likely to be caused by antibiotic-sensitive bacteria. Late-onset HAP and VAP (day 5 or thereafter) are more likely to be caused by MDR pathogens, and are associated with higher morbidity and mortality. However, patients with early-onset HAP who have received prior antibiotics or who have been recently hospitalized may be at a greater risk for colonization and infection with MDR pathogens.[252,266]
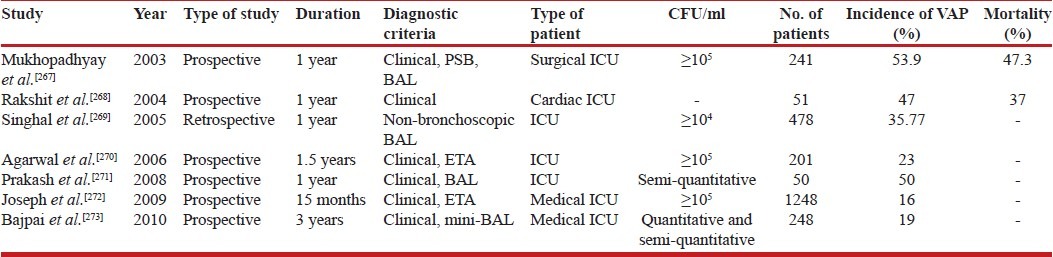
The incidence of VAP as reported in various Indian studies ranges from 16 to 53.9% [Table 13].[267–271,272,273,274] Although these data are limited and heterogeneous, the general incidence appears fairly high. Most Indian data on HAP/VAP originates from tertiary hospitals and medical ICUs and may not be truly representative of other settings. For instance, HAP may be more common than presumed in wards or other ICU areas.
Table 13.
Studies reporting the incidence of HAP/VAP from the Indian subcontinent
How is the organism profile in Indian settings different from the Western data?
HAP and VAP are caused by a wide spectrum of bacterial pathogens and may be polymicrobial. Common pathogens include aerobic Gram-negative bacilli such as P. aeruginosa, E. coli, K. pneumoniae, and Acinetobacter species. Infections due to Gram-positive cocci, such as Sta. aureus, particularly methicillin-resistant Sta. aureus (MRSA), are rapidly emerging in the West. Pneumonia due to Sta. aureus is reportedly more common in patients with diabetes mellitus, head trauma, and those hospitalized in ICUs.[252,261,266] On the other hand, Gram-negative pathogens still remain the most common organisms responsible for causing HAP/VAP in most Indian reports.[270,272–274] Most studies report Acinetobacter species followed by P. aeruginosa as the most common organisms isolated from patients having HAP/VAP.
Does the microorganism profile vary amongst different centers and within the same hospital setting?
The rates of acquiring infection with MDR pathogens have drastically increased over the past few years.[252] The type of MDR pathogens causing HAP may vary by hospital, patient population, exposure to antibiotics, type of ICU, and changes over time, emphasizing the need for constant local microbiological data. The microbial etiology of VAP appears to differ even between different hospitals within the same city and between ICUs within a single hospital. The empiric antibiotic treatment decisions for patients with VAP must take into account local microbiology and antimicrobial susceptibility profile.[252,257,261,275]
Recommendation:
Gram-negative bacteria are the most common pathogens causing HAP/VAP in the Indian setting (UPP) and should be routinely considered as the most common etiological agents of HAP/VAP.
Diagnosis
When should HAP/VAP be suspected?
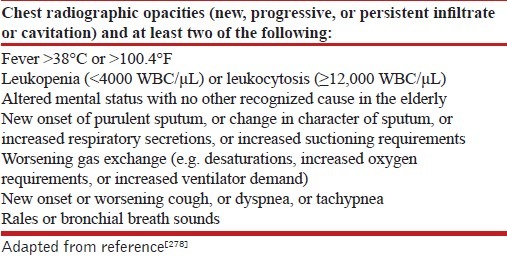
HAP/VAP should be suspected in any hospitalized/ventilated patient with symptoms and signs of pneumonia. Sensitive criteria based on clinical and radiologic parameters should be used to enable early diagnosis.[276] The following findings suggest the presence of HAP/VAP in any patient who has been hospitalized or is being mechanically ventilated and include new or progressive radiologic deterioration along with two of the following: new onset fever, purulent secretions, leukocytosis, and decline in oxygenation.[252,277] Patients with ARDS may be suspected as harboring VAP if there significant decline in oxygen status as indicated by: (a) sustained increase in positive end-expiratory pressure (PEEP) requirement by ≥2.5 cm H2O after being stable or decreasing or (b) FiO2 requirements rise by ≥0.15 after being stable or decreasing.[277] The Centers for Disease Control (CDC) criteria are widely used in the diagnosis of HAP [Table 14].[278]
Table 14.
Modified CDC criteria for diagnosis of HAP/VAP
What is the approach to diagnose HAP/VAP?
The purpose of diagnostic techniques is: (a) to determine whether a patient has pneumonia and (b) to identify the etiological pathogen. An appropriate diagnostic algorithm involves collection of pertinent clinical samples for bacterial cultures, early institution of effective antibiotic therapy, and provision for de-escalation whenever possible. Most of the available literature and guidelines focus on VAP, and very little data are available for HAP. The diagnostic approach revolves around two strategies: the clinical strategy and the bacteriological strategy.[252,253]
Clinical strategy
The clinical strategy combines clinical suspicion with semi-quantitative cultures of sputum and/or tracheal aspirates. Clinical parameters include fever, pulmonary manifestations (e.g. purulent sputum or endotracheal secretions, abnormal respiratory system examination, worsening gas exchange), and basic investigations (e.g. leukocytosis, abnormal chest radiograph). Advanced radiologic investigations such as CT scanning are neither feasible in most patients nor recommended. Clinical data are supplemented by microbiological workup.
Sputum or endotracheal aspirates (ETAs) are easily obtained in most patients and should be sent for culture before initiation of antibiotics. It is important to ensure that a representative sample of the lower respiratory tract is collected. Despite its numerous limitations, sputum appears to be the only representative lower respiratory tract sample in non-intubated patients. Routine culture reporting as either positive or negative is not useful since it cannot discriminate at all between the wide spectrum of light contamination and heavy infection. Semi-quantitative cultures overcome this problem to some extent, and are still technically simple enough to be feasible in most standard microbiology laboratories. Culture growths are reported semi-quantitatively as light, moderate, or heavy. Semi-quantitative tracheal aspirate cultures are highly sensitive, but have low specificity and cannot differentiate colonization from infection. However, their specificity increases when combined with clinical criteria.[252,277] The semi-quantitative cultures, however, have a high negative predictive value. In fact, a sterile ETA culture is strong evidence against pneumonia in the absence of a recent change in antibiotic therapy.[279] In addition, blood cultures, as well as cultures of other clinical specimens (such as pleural fluid) should also be submitted. These additional investigations help in identifying possible extrapulmonary sites of infection, and a concordant isolate from both respiratory and other samples virtually clinches the microbial etiology.
It must be emphasized that a combination of clinical and radiologic features alone has low specificity for diagnosing HAP/VAP due to substantial overlap with non-infectious conditions like congestive heart failure, pulmonary edema, pulmonary hemorrhage, atelectasis, and others.[280] Therefore, supplementary microbiological data are extremely important. No single constellation of clinicoradiological findings is a perfect diagnostic marker of HAP/VAP. There have been several efforts to formulate objective bedside criteria to assist the clinician in diagnosing HAP/VAP. One widely used clinical approach is the CDC algorithm for “clinically defined pneumonia,” which attempts diagnosis based on the presence of two of three radiologic criteria, plus at least one systemic and two pulmonary signs clinically suggestive of pneumonia [Table 14].[278]
In order to increase the specificity of clinical diagnosis, the clinical pulmonary infection score (CPIS) is utilized, which combines clinical, radiographic, physiological (PaO2/FiO2), and microbiological data into a single numerical result [Table 15].[281–284] When the CPIS exceeded 6, good correlation was found with pneumonia diagnosed by quantitative cultures of bronchoscopic and non-bronchoscopic bronchoalveolar lavage (BAL) specimens.[282] Singh and colleagues also proposed a modified CPIS that does not rely on culture data to guide clinical management.[284] Not all recent studies have corroborated the high accuracy initially reported for the CPIS.[285] The accuracy of the CPIS is not high without microbiological data, but can be improved if a reliable lower respiratory tract sample is obtained and studied carefully using Gram staining.[286,287] Although CPIS may not be a good tool for diagnosis of HAP/VAP, it may still help the clinician to evaluate the clinical response to therapy and determine its appropriate duration. The duration of therapy was directly correlated with the CPIS at the time of pneumonia diagnosis. In one study, the CPIS when calculated prospectively and used serially throughout the course of VAP management, decreased in patients who survived, but not in those who did not, thus reflecting the clinical evolution of pneumonia.[288] It is therefore also important that if clinical/microbiological features do not objectively support infection but the clinical suspicion of HAP/VAP is high, patient may be reevaluated after 48–72 h.
Table 15.
Modified Clinical Pulmonary Infection Score[281]
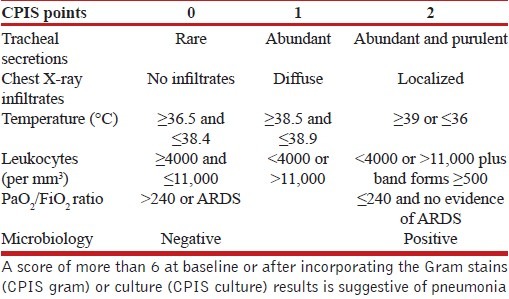
Recommendations:
HAP/VAP can be clinically defined [Figure 2] using modified CDC criteria (2A).
In patients with a strong suspicion of VAP/HAP but insufficient evidence for the presence of infection, periodic reevaluation should be done (2A).
In patients with suspected VAP/HAP, one or more lower respiratory tract samples and blood should be sent for cultures prior to institution of antibiotics (1A).
All patients suspected of having HAP should be further evaluated with good-quality sputum microbiology (3A).
CT scan should not be routinely obtained for diagnosing HAP/VAP (3A).
Semi-quantitative cultures can performed in lieu of qualitative cultures (1A).
Appropriate management should not be delayed in clinically unstable patients for the purpose of performing diagnostic sampling (UPP).
Bacteriological strategy
The bacteriological strategy depends upon “quantitative” cultures of lower respiratory secretions {ETA [105 or 106 colony forming units (CFU)/mL], bronchoalveolar lavage [BAL, 104 CFU/mL] or protected-specimen brush [PSB, 103 CFU/mL] specimens, collected with or without a bronchoscope} to establish both the presence of pneumonia and the etiological pathogen. Growth above a threshold concentration is necessary to determine the causative microorganism. The threshold is obtained through cultures of serial dilutions of the clinical material, and is described in terms of CFU per unit volume of the undiluted sample. Bacteriological approach gives importance to separating colonizers from infecting pathogens.[289–291] However, such an approach is technically demanding, both in terms of equipment/accessories needed for sample collection and the infrastructure required for microbiological standardization. There is hardly any microbiology laboratory in India that routinely performs quantitative cultures, and quantitative cultures are considered more of a research tool.[292] The bacteriological strategy is considerably more expensive in terms of sampling and diagnostics, but may reduce the overall cost of treatment as fewer patients (only microbiologically confirmed pneumonia) are treated with targeted antibiotic therapy.
In several studies, the sensitivity of quantitative tracheal aspirate samples has been >80% for identifying an etiological pathogen, results that were often comparable to bronchoscopic findings in the same patients.[252,293–296] The quality of the PSB sample is difficult to measure and the reproducibility is not exact, with as many as 25% of results on different sides of the diagnostic threshold when comparing two samples collected from the same site in the same patient.[296,297]
Are quantitative methods of culture better than semi-quantitative methods?
The value of quantitative cultures in clinical settings would be negated if there were a high rate of false-positive or false-negative findings. False-positive results would mean that patients without VAP are erroneously diagnosed. This could prove harmful because of resulting overtreatment and can hamper evaluation of the true efficacy of antibiotics. False-positive results have been reported for patients receiving prolonged mechanical ventilation, who are often colonized at high bacterial concentrations.[298] Similarly, a false-negative quantitative culture result means that some patients with VAP are missed. This is possible as many patients with suspected VAP are on antibiotic therapy. Although this is a common concern, it may be less of a consideration if the patient had been receiving the same therapy for at least 72 h before diagnostic samples are obtained.[299] There is no difference in terms of mortality, ICU stay, duration of mechanical ventilation, or rates of antibiotic change when either technique was used for diagnosing HAP/VAP. Quantitative and semi-quantitative cultures, of blind or targeted lower respiratory secretions, have equivalent yield and clinical utility.[300–302]
Recommendation:
Semi-quantitative cultures of lower respiratory tract secretions are easier and equally discriminatory for the presence of pneumonia, as compared to quantitative cultures (UPP).
Are invasive techniques to collect lower respiratory tract secretions better than blind endotracheal aspirates?
The lack of a well-established gold standard remains a challenge in the diagnosis of HAP/VAP. To counter contamination of respiratory secretions, it has been suggested that invasive methods, including bronchoscopy-directed BAL or PSB, or protected BAL or PSB can improve the diagnostic yield over blind ETA, and guide appropriate antibiotic selection. However, results of various comparative studies are inconclusive.[252] Although an initial study suggested lower mortality with the invasive strategy,[280] subsequent studies have failed to demonstrate these results.[300,303] The use of bronchoscopy to collect lower respiratory tract secretions requires additional expertise, which may not be available at all hospitals, and also considerably increases the cost due to expensive accessories required for this purpose. To limit contamination and aspirate secretions from more distal portions, simple telescoping catheter systems can be easily devised using indigenous components, and used to collect more representative and higher-quality specimens in a blind fashion.[297] Quantitative or semi-quantitative cultures can be performed on ETA or samples collected either bronchoscopically or non-bronchoscopically. Each technique has its own diagnostic threshold and methodological limitations. The choice depends on local expertise, availability, and cost.
Recommendations:
Quantitative and or semi-quantitative cultures using various sampling techniques like ETA, bronchoscopic or non-bronchoscopic BAL and PSB are equally useful for establishing the diagnosis of HAP/VAP (2A).
Semi-quantitative culture on blind (non-bronchoscopic) ETA sample (preferably obtained through a sterile telescoping catheter system) is a reasonable choice (2A).
In a patient suspected of having VAP, the preferred method for lower respiratory tract sample collection (blind or targeted, bronchoscopic or non-bronchoscopic) depends upon individual preferences, local expertise, and cost; however, blind ETA sampling is the easiest and equally useful (UPP).
What is the role of biomarkers in diagnosis of HAP/VAP?
An ideal biomarker for VAP should not be detectable when infection is not present, and should be elevated in the presence of infection. Three biomarkers have been studied extensively for predicting VAP: soluble triggering receptor expressed on myeloid cells type 1 (sTREM-1), PCT, and CRP.[304–314] None of the currently available biomarkers has good utility for diagnosis of HAP/VAP. However, PCT can be utilized to differentiate bacterial VAP from non-infective causes of pulmonary infiltrates and to take decisions about stopping antibiotics in the ICU.
Recommendations:
Currently available biomarkers should not be used to diagnose HAP/VAP (1A).
Where available, serum procalcitonin levels <0.5 ng/mL may help in differentiating bacterial HAP/VAP form other non-infective etiologies, and may help in decisions for antibiotic cessation (2B).
Is combined clinicobacteriological strategy better than either strategy used alone?
Beyond issues with the sensitivity and specificity of the CPIS, inter-observer variability in noting clinical parameters remains a major concern, as different clinicians may not absolutely concur with the clinical features in a given patient.[285] Adding microbiological results improves this situation by providing objective evidence of infection. A predominantly clinical approach involves empiric antibiotic therapy in those clinically diagnosed as having pneumonia and can thus result in overtreatment. A bacteriological approach, on the other hand, recommends antibiotics only to those in whom pneumonia is microbiologically confirmed. However, quantitative cultures are not routinely available, and the strategy can result in denying treatment to those with false-negative cultures. A combined approach is logically attractive, with a primary goal of using appropriate therapy in a timely manner, without overusing antibiotics [Figure 2].
In a combined approach, patients strongly suspected to have HAP/VAP undergo lower respiratory tract sampling. Empiric antibiotics may be started after specimens have been submitted for culture. For patients highly suspected to have pneumonia but not fulfilling the essential clinical criteria for the same, regular monitoring is advocated. Some of these patients may actually have ventilator-associated tracheobronchitis (VAT), which is defined by the presence of fever, increased volume and purulence of respiratory secretions, a positive culture of a respiratory sample, and the absence of a new or an evolving pulmonary infiltrate in the chest X-ray in a patient on mechanical ventilation for >48 h.[315,316] VAT is distinct from VAP, and not all experts advocate antibiotic usage in this situation. If patients deteriorate subsequently and fulfill the diagnostic criteria for pneumonia, they can be managed as above. In either situation, the decision to continue/modify/stop antibiotics can be taken once culture results are available, taking into account the overall clinical features and response to treatment. Several guidelines advocate the use of a combined clinical and bacteriological strategy for better outcomes in diagnosing and treating HAP/VAP.[252,253]
Recommendation:
Both clinical and bacteriological strategies can be combined to better diagnose and manage HAP and VAP (UPP).
Treatment
What are the general principles of managing HAP/VAP?
Once HAP/VAP is suspected, antibiotics should be initiated as soon as possible after taking adequate specimens for microbiological culture. The empiric antibiotic choice is based on the timing of development of HAP and assessment of the patient's risk for MDR pathogens [Figure 3]. Early-onset HAP is arbitrarily classified as pneumonia developing within the first 4 days of hospitalization and late-onset HAP as pneumonia 5 or more days after hospitalization. However, many patients are admitted in other hospitals before being transferred, hence this duration should be kept in mind while deciding the empiric antibiotic therapy. As the treatment is started empirically, the initial cover is generally broad spectrum, and hence all efforts should be made to de-escalate antibiotics once culture reports are available.
Figure 3.
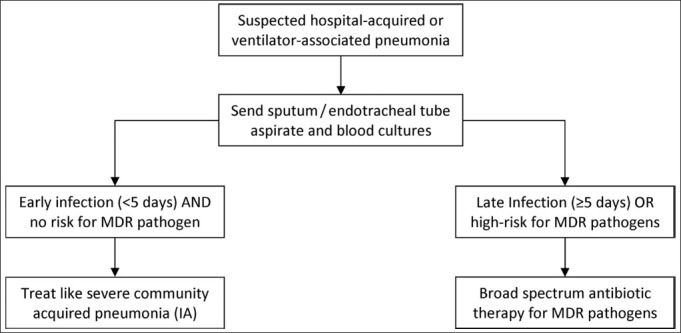
Assessment of the risk of MDR pathogens in HAP/VAP
What are the characteristics of empiric combination therapy for the treatment of VAP/HAP?
The empiric combination therapy should be appropriate, adequate, and optimal. The term “appropriate” means the chosen empiric antibiotic therapy should cover the organism which would eventually be isolated. The odds of mortality are higher in patients receiving initial inappropriate antibiotic therapy.[317–321] An “adequate” antibiotic therapy ensures proper route of administration and proper penetration of the drug, and an “optimal” antibiotic regimen means that the antibiotic dosage should be according to the pharmacokinetics and pharmacodynamics of the chosen drug.
How do we decide on the empiric antibiotic regimen to be started in a case of suspected HAP/VAP?
Every hospital/ICU should have its own written antibiotic policy to initiate empiric antibiotic therapy in suspected nosocomial pneumonia. Any deviation from the policy should be based on strong evidence. Formulation of antibiotic policy should be based on the antibiogram, which is updated as often as possible, and at least once over the previous 6 months. The antibiogram can be periodically changed according to the reports obtained. In the absence of a hospital or ICU antibiotic policy, these guidelines should be employed for the initial empiric therapy.
Recommendations:
Every ICU/hospital should have its own antibiotic policy for initiating empiric antibiotic therapy in HAP based on their local microbiological flora and resistance profiles (1A). This policy should be reviewed periodically.
In hospitals that do not have their own antibiotic policy, the policy given in these guidelines is recommended (3A). However, they should strive toward formulating their own antibiotic policy.
What is the role of routine endotracheal aspirate culture surveillance?
Routine endotracheal aspirate culture surveillance (REAS) is performed by obtaining serial endotracheal aspirate cultures at fixed intervals even in the absence of infection. The results of the cultures obtained are then employed in guiding the antibiotic regimen if the patient develops evidence of HAP. Although some studies suggest the usefulness of this strategy with high concordance between the surveillance culture and the organism subsequently identified during VAP,[322,323] others indicate a limited role.[324] As this strategy is more expensive than the antibiogram strategy, it is not feasible in developing countries.
Recommendation:
Routine endotracheal aspirate culture is not recommended. An antibiogram approach should be followed wherever feasible (2A).
Is there a benefit of combination therapy over monotherapy for the treatment of HAP/VAP and HCAP?
Various societies have given recommendations for deciding on the empiric regimen.[253,325–331] Most guidelines recommend monotherapy if there are no risk factors for MDR pathogens and combination therapy if there are risk factors for MDR pathogens, except for the British Thoracic Society guidelines which recommend monotherapy for MDR pathogens as well.[326] There is evidence both for and against combination therapy. The combination therapy carries a higher chance of the empiric regimen being appropriate and of antibacterial synergy between compounds. However, combination therapy also entails the risks of adverse effects related to therapy, increased emergence of drug-resistant organisms, and increased cost of therapy. There is no conclusive evidence in favor of either combination or monotherapy in several trials and meta-analyses.[332–337]
Recommendation:
Although there is no evidence to suggest that combination therapy is superior to monotherapy, the expert group recommended initial empiric therapy as a combination due to the high prevalence rates of MDR pathogens in late-onset HAP/VAP [Table 16] and with an aim to ensure the chances of appropriateness of the initial regimen (UPP). However, once the culture reports are available, the regimen should be de-escalated to the appropriate monotherapy (1A).
What is the recommended strategy for initiating antibiotics in suspected HAP/VAP?
Antibiotics should be initiated as soon as possible after sending the appropriate microbiological samples as delay in initiation of appropriate antibiotic therapy has also been associated with increased mortality.[338–347] The initial empiric antibiotic therapy should generally cover the MDR pathogen, and should be initiated with an antipseudomonal penicillin, cephalosporin, or carbapenem, along with an aminoglycoside [Table 16]. The exact choice of antibiotic depends on local availability, antibiotic resistance patterns, preferred routes of delivery, other complicating factors, and costs. Fluoroquinolones should be used only in those with contraindications to aminoglycosides so as to reserve the use of fluoroquinolones for the treatment of TB and decrease the probability of emergence of fluoroquinolone-resistant M. tuberculosis. The initial combination therapy should be converted to appropriate monotherapy once culture reports become available. Empiric therapy for MRSA initially is not recommended due to the low prevalence of MRSA in the Indian ICUs; if there is a documented high prevalence of MRSA, the initial empiric therapy should also cover MRSA. Polymyxins are not recommended as empiric therapy in the treatment of HAP/VAP. A combination of meropenem and colistin is being increasingly used in the community despite a study documenting increased mortality with this combination.[348]
Recommendations:
In patients with suspected HAP, antibiotics should be initiated as early as possible after sending the relevant samples for culture (1A).
The exact choice of antibiotic to be started is based on local availability, antibiotic resistance patterns, preferred routes of delivery, other complicating factors, and cost.
The initial combination therapy should be converted to appropriate monotherapy once culture reports are available (1A).
Colistin is not recommended as an initial empiric therapy for HAP/VAP (3A).
Combination therapy with colistin and meropenem is not recommended (2A).
Is antibiotic de-escalation useful? What is the strategy for antibiotic de-escalation?
Antibiotic de-escalation is defined as the shift from broad-spectrum to narrow-spectrum antibiotic once the culture reports become available, to stop antibiotics if no infection is established or to shift from combination to monotherapy, whenever possible.[349] The benefits include: (a) improved or unaltered treatment outcomes; (b) decrease in antimicrobial resistance; (c) decrease in antibiotic-related side effects; (d) decrease in superinfections; and (e) reduction in overall antibiotic costs.[350] Cessation of antibiotics after 3 days when the CPIS was <6 did not alter the mortality and length of ICU stay.[284] Numerous studies have shown improved or unchanged outcome with the de-escalation strategy.[351–358]
Recommendations:
The strategy for de-escalation of antibiotics is strongly recommended (1A). However, as the de-escalation strategy entirely rests on microbiology, appropriate microbiological samples should be sent before initiation of antibiotics [Figure 2].
Among patients with suspected VAP in whom an alternate cause for pulmonary infiltrates is identified, it is recommended that antibiotics should be stopped (1A).
If cultures are sent after initiation of antibiotics and there is clinical improvement with subsequent cultures being sterile, antibiotics should be continued for 7 days followed by assessment of CPIS on the 7th day. If CPIS is <6, antibiotics can be stopped, while if it is ≥6, treatment should be continued for 10–14 days.
If cultures sent before starting antibiotics are negative and there is clinical worsening, it is recommended that a review of the current management plan including the choice of antibiotics be performed. Microbiological workup should be repeated including performance of fungal cultures. One also needs to look for alternate sources of sepsis (especially one or more foci of undrained infection) and consider non-infective causes.
Empiric antifungal therapy (on day 3) should not be used as a routine in all patients if cultures are sterile and there is clinical worsening (3A).
What is the optimal duration of antibiotic therapy?
In a study comparing 8 versus 15 days of antibiotic therapy in VAP, there were more antibiotic-free days, decreased risk of super infections with MDR pathogens, no increased mortality, no recurrent infections, and no change in duration of mechanical ventilation or ICU stay in the 8-day treatment group.[290] Only patients with Pseudomonas infection had increased recurrence of pneumonia. Another study has shown that the fall in CPIS on 3rd and 5th day was significant in survivors compared to non-survivors.[288] This study also suggests that serial monitoring of CPIS could identify those patients with good outcomes and help in shortening the duration of treatment. Various societies have recommended short-course treatment (7–8 days) for the management of VAP if the organism is not non–lactose-fermenting Gram-negative bacteria or P. aeruginosa.[253,325–328]
Recommendations:
In patients with VAP due to Pseudomonas, Acinetobacter, and MRSA, a longer duration (14 days) of antibiotic course is recommended (1A). Assessment of CPIS on day 7 may identify the patients in whom therapy could be stopped early (2A).
In other patients with VAP who are clinically improving, a 7-day course of antibiotics is recommended (1A).
Is continuous infusion of antibiotics better than intermittent doses?
The decision to give continuous infusions or intermittent doses depends on whether the antibiotics being administered follow time-dependent or concentration-dependent kinetics or both.[359,360] Time-dependent antibiotics require drug concentrations greater than the minimum inhibitory concentration or MIC (T > MIC) for a certain period of time between doses, which usually ranges from 40 to 50% of inter-dose interval for their best action. The examples include β-lactams, carbapenems, and lincosamides. These drugs are best given as continuous infusions over a particular duration depending on the stability of the prepared drug at room temperature. On the other hand, concentration-dependent antibiotics like aminoglycosides are best administered as a single daily dose or as intermittent doses. These antibiotics require attainment of peak concentration many times higher than the MIC for their best action and have prolonged post-antibiotic effect (PAE) which makes them effective even after their drug concentration falls below the MIC. Concentration- and time-dependent antibiotics (fluoroquinolones and glycopeptide antibiotics) require both time as well as concentration for their optimal action. The area under the concentration time curve (AUC)/MIC determines the clinical efficacy of these antibiotics. A lower 14-day mortality (12.2 vs. 31.6%) and lower mean duration of hospital stay (21 vs. 38 days) was seen among patients with APACHE II scores ≥17 receiving extended infusions.[361] Several other studies have demonstrated that continuous infusions are associated with numerous clinical benefits including decrease in hospital stay and mortality.[362–366]
Recommendation:
Antibiotic administration in critically ill patients is recommended according to their pharmacokinetic/pharmacodynamic profile [Table 17] as it is associated with superior clinical outcomes (2A).
What is the role of inhaled antibiotics in the treatment of VAP?
Inhaled antimicrobials may be as safe and as efficacious as standard antibiotics for the treatment of VAP.[367] In fact, aerosolized vancomycin and gentamicin have been shown to decrease VAP, facilitate weaning, reduce bacterial resistance, and the use of systemic antibiotics when used in those with ventilator-associated tracheobronchitis.[368] Patients receiving adjunctive aerosolized antibiotics had higher 30-day survival.[369] Recently, nebulized colistin when added to intravenous colistin has been associated with better microbiological outcome (60.9 vs. 38.2%) although the clinical outcomes were similar.[370] Another retrospective cohort study suggested that the clinical cure rates are better when colistin is given simultaneously in both intravenous and inhaled forms.[371] Several smaller retrospective observational studies have shown better clinical response with the combination of intravenous and inhaled antibiotics,[372–374] while some others have used aerosolized colistin monotherapy for treatment of MDR pathogens with good clinical outcomes.[375–377] However, all the aforementioned reports are anecdotal with small sample size; hence, more data are required before the routine use of inhaled antibiotics can be recommended.
Recommendations:
Aerosolized antibiotics (colistin and tobramycin) may be a useful adjunct to intravenous antibiotics in the treatment of MDR pathogens where toxicity is a concern (2A).
Aerosolized antibiotics should not be used as monotherapy and should be used concomitantly with intravenous antibiotics (2A).
Should one treat ventilator-associated tracheobronchitis?
Ventilator-associated tracheobronchitis (VAT) is defined as the presence of elevated temperature (>38°C), leukocytosis (>12,000/μL)/leukopenia (<4000/μL) plus a change in quantity or quality (purulent) of endotracheal secretions without new radiologic infiltrates.[378] This usually, but not necessarily, is accompanied by demonstration of bacteria on Gram stain or semi-quantitative cultures of endotracheal aspirate. VAT has been associated with longer duration of mechanical ventilation and ICU stay among patients without chronic respiratory failure.[379] Administration of systemic antimicrobials with or without concurrent inhaled drug decreases neither the mortality nor the ICU stay or the duration of mechanical ventilation.[380] There is no clear-cut evidence of benefit with treatment of VAT, and treatment of VAT is usually not recommended. However, these patients should be re-evaluated as required for the development of VAP.
Recommendation:
Patients with proven VAT should not be treated with antibiotics (2A).
What are the drugs of choice for treatment of methicillin-resistant Staphylococcus aureus?
Drugs approved for the treatment of MRSA pneumonia include vancomycin, teicoplanin, and linezolid. Newer investigational drugs include lipoglycopeptides (telavancin, dalbavancin, and oritavancin), cephalosporins (ceftobiprole and ceftaroline), and dihydrofolate reductase inhibitors (iclaprim).[381] Vancomycin has certain drawbacks such as poor lung tissue penetration, potential nephrotoxicity, and inferior clinical outcomes.[382] Linezolid has been suggested as a better choice in the management of MRSA pneumonia. Two meta-analyses found no difference in clinical cure rates and microbial eradication rates between vancomycin and linezolid,[383,384] although a recent randomized clinical trial (RCT) showed that clinical response was significantly higher with linezolid compared to vancomycin, but with no difference in mortality.[385]
Recommendations:
In patients with suspected MRSA infection, we recommend the use of empiric vancomycin (1A) or teicoplanin (2A). The use of linezolid in India should be reserved because of its potential use in extensively drug-resistant tuberculosis.
Linezolid is an effective alternative to vancomycin (1A) if the patient (a) is vancomycin intolerant, (b) has renal failure, and (c) is harboring vancomycin-resistant organism.
How to treat MDR Acinetobacter infections?
The treatment options for MDR Acinetobacter include carbapenems, polymyxins [polymyxin B and polymyxin E (colistin)], tigecycline, and combination therapy with sulbactam or rifampicin, or combination of carbapenem with colistin.[386] Colistin is as safe and as efficacious as the standard antibiotics for the treatment of VAP.[387] Although the recommended dose of colistin is 2 MU intravenously thrice a day, some studies suggest using higher doses of colistin (9 MU/day) as the concentration is higher than the MIC breakpoint (2 mg/mL) at this dose.[388–390] Good outcomes have been noted in majority of the patients treated with polymyxin B.[391]
Combination of colistin and imipenem was synergistic in 50% of colistin-susceptible imipenem-resistant K. pneumoniae strains.[392] No difference in clinical response and nephrotoxicity was observed in one retrospective study.[348] In fact, the survival was lower in patients with combination therapy.
Sulbactam is a relatively new agent for the treatment of MDR Acinetobacter. Several in vitro and in vivo animal studies reported intrinsic activity of sulbactam against Acinetobacter.[393,394] The recommended dose for sulbactam is 40–80 mg/kg (at least 6 g/day in divided doses). It is a time-dependent antibiotic and can be used as both a monotherapy or in combination with other antibiotics (meropenem, colistin, amikacin, cefepime). Most clinical trials have been reported with ampicillin/sulbactam. Rifampicin in combination with colistin has also been shown to be beneficial in observational studies.[395–397] Although tigecycline is approved by the Food and Drug Administration (FDA) for the treatment of complicated intra-abdominal infections, complicated skin and soft tissue infections, and community-acquired bacterial pneumonia, emerging resistance of Acinetobacter spp. and limited therapeutic options have forced physicians to use tigecycline for off-label indications like HAP secondary to Acinetobacter. In recently published meta-analyses, tigecycline compared to other antibiotics has been associated with worse outcomes and even increased risk of death when used for treating patients with VAP.[398,399]
Recommendations:
For treatment of MDR Acinetobacter infections, we recommend the following drugs: carbapenems (1A), colistin (1A), sulbactam plus colistin (2B), sulbactam plus carbapenem (2B), and polymyxin B (2A).
Combination therapy with sulbactam and colistin or carbapenem for MDR Acinetobacter (in proven cases or suspected cases with multi-organ dysfunction syndrome) may be initiated. Sulbactam should be stopped after 5 days in patients responding to treatment (2B).
How to treat MDR Pseudomonas infections?
P. aeruginosa can be considered the prototype MDR Gram-negative bacilli causing hospital-acquired pneumonia (HAP) with at least five known mechanisms of resistance.[400] The therapeutic options for MDR Pseudomonas include aminoglycosides (amikacin, tobramycin, netilmicin), β-lactam/β-lactamase inhibitors (piperacillin–tazobactam, cefoperazone–sulbactam, ticarcillin–clavulanate), antipseudomonal cephalosporins (cefepime, cefpirome), monobactam (aztreonam), fluoroquinolones (ciprofloxacin, levofloxacin), carbapenems (imipenem, meropenem), and polymyxins (colistin, polymyxin B). Carbapenems are the drugs of choice for P. aeruginosa that produce extended-spectrum β-lactamases. Adjunctive antibiotic therapy with inhaled antibiotics has been proposed in the management of MDR Pseudomonas; however, there is no clear evidence for its use.[400]
Recommendation
For treatment of MDR Pseudomonas, we recommend initial combination chemotherapy with a carbapenem and either a fluoroquinolone or an aminoglycoside (1A). Treatment should then be de-escalated to appropriate monotherapy.
OTHER ISSUES
What should be the strategy for prevention of VAP/HAP?
A detailed discussion on prevention of HAP/VAP is beyond the scope of these guidelines. We recommend the readers to refer other published documents for detailed discussion on prevention of HAP/VAP.[264,401–442] The strategies for prevention of VAP relevant to local conditions are listed in Table 18. The group re-emphasized staff education programs by hospital infection control committee and the concerned infection control nurse on a weekly basis (2A).
Table 18.
Preventive strategies for VAP
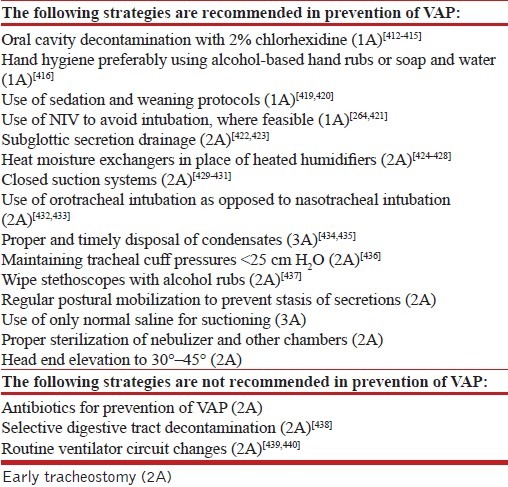
What are the other good practices to be followed in the ICU?
Good practices are associated with improved ICU outcomes that need to be followed in ICUs. These include the following:
Stress ulcer prophylaxis
Stress ulcer prophylaxis should generally be avoided in order to preserve gastric function. Whenever stress ulcer prophylaxis is indicated, sucralfate should be preferred in order to reduce the risk of VAP. The two major risk factors for clinically important gastrointestinal bleeding due to stress ulceration include mechanical ventilation for >48 h and coagulopathy.[443] Proton pump inhibitors (PPI) are superior to H2 receptor antagonists (H2RA),[444] while H2RA are superior to antacids[445] or sucralfate.[446] Prophylactic agents that increase gastric pH (e.g. PPIs, H2RA, and antacids) may increase the risk of nosocomial pneumonia compared to agents that do not alter gastric pH (sucralfate).[447] In those with high risk of stress ulcer bleeding, H2RA and PPIs should be employed, with sucralfate reserved in patients with low to moderate risk of gastrointestinal bleeding.
Early enteral feeding
Enteral feeding is superior to parenteral nutrition and should be used whenever tolerated and in those without any contraindications to enteral feeding. Enteral nutrition is associated with a lower incidence of infection, but not mortality.[448]
Deep venous thrombosis prophylaxis
Pulmonary embolism remains the most common preventable cause of hospital death. DVT prophylaxis with unfractionated heparin (5000 U thrice a day) or a low-molecular-weight heparin should be routinely used in all ICU patients with no contraindications to prophylactic anticoagulation.[449]
Glucose control
We recommend a plasma glucose target of 140–180 mg/dL in most patients with pneumonia, rather than a more stringent target (80–110 mg/dL) or a more liberal target (180–200 mg/dL). This glucose range avoids hyperglycemia, while minimizing the risk of both hypoglycemia and other harms associated with a lower blood glucose target.[450]
Blood products
Red blood cells should be transfused at a hemoglobin threshold of <7 g/dL except in those with myocardial ischemia and pregnancy.[451] Platelet transfusion is indicated in patients with platelet count <10,000/μL, or <20,000/μL if there is active bleeding. Fresh frozen plasma is indicated only if there is a documented abnormality in the coagulation tests and there is active bleeding or if a procedure is planned.
Footnotes
Source of Support: Jointly sponsored by the Indian Chest Society and the National College of Chest Physicians (India)
Conflict of Interest: None declared.
REFERENCES
- 1.Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–6. doi: 10.1136/bmj.39489.470347.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Guyatt GH, Rennie D, Meade MO, Cook DJ. Users’ Guide to the Medical Literature: A Manual for Evidence-based Clinical Practice. 2nd ed. New York: McGraw Hill; 2008. [Google Scholar]
- 3.Lim WS, Baudouin SV, George RC, Hill AT, Jamieson C, Le Jeune I, et al. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009;64(Suppl 3):iii1–55. doi: 10.1136/thx.2009.121434. [DOI] [PubMed] [Google Scholar]
- 4. [Accessed 2012 Mar 10]. http://www.cdc.gov/Features/Pneumonia .
- 5.Donalisio MR, Arca CH, Madureira PR. Clinical, epidemiological, and etiological profile of inpatients with community-acquired pneumonia at a general hospital in the Sumare microregion of Brazil. J Bras Pneumol. 2011;37:200–8. doi: 10.1590/s1806-37132011000200010. [DOI] [PubMed] [Google Scholar]
- 6.Bruns AH, Oosterheert JJ, Cucciolillo MC, El Moussaoui R, Groenwold RH, Prins JM, et al. Cause-specific long-term mortality rates in patients recovered from community-acquired pneumonia as compared with the general Dutch population. Clin Microbiol Infect. 2011;17:763–8. doi: 10.1111/j.1469-0691.2010.03296.x. [DOI] [PubMed] [Google Scholar]
- 7.Ruhnke GW, Coca-Perraillon M, Kitch BT, Cutler DM. Trends in mortality and medical spending in patients hospitalized for community-acquired pneumonia: 1993-2005. Med Care. 2010;48:1111–6. doi: 10.1097/MLR.0b013e3181f38006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Capelastegui A, Espana PP, Bilbao A, Gamazo J, Medel F, Salgado J, et al. Study of community-acquired pneumonia: incidence, patterns of care, and outcomes in primary and hospital care. J Infect. 2010;61:364–71. doi: 10.1016/j.jinf.2010.07.015. [DOI] [PubMed] [Google Scholar]
- 9.Welte T, Kohnlein T. Global and local epidemiology of community-acquired pneumonia: the experience of the CAPNETZ Network. Semin Respir Crit Care Med. 2009;30:127–35. doi: 10.1055/s-0029-1202941. [DOI] [PubMed] [Google Scholar]
- 10.Vila-Corcoles A, Ochoa-Gondar O, Rodriguez-Blanco T, Raga-Luria X, Gomez-Bertomeu F. Epidemiology of community-acquired pneumonia in older adults: a population-based study. Respir Med. 2009;103:309–16. doi: 10.1016/j.rmed.2008.08.006. [DOI] [PubMed] [Google Scholar]
- 11.Charles PG, Whitby M, Fuller AJ, Stirling R, Wright AA, Korman TM, et al. The etiology of community-acquired pneumonia in Australia: why penicillin plus doxycycline or a macrolide is the most appropriate therapy. Clin Infect Dis. 2008;46:1513–21. doi: 10.1086/586749. [DOI] [PubMed] [Google Scholar]
- 12.Viegi G, Pistelli R, Cazzola M, Falcone F, Cerveri I, Rossi A, et al. Epidemiological survey on incidence and treatment of community acquired pneumonia in Italy. Respir Med. 2006;100:46–55. doi: 10.1016/j.rmed.2005.04.013. [DOI] [PubMed] [Google Scholar]
- 13.Marrie TJ, Huang JQ. Epidemiology of community-acquired pneumonia in Edmonton, Alberta: An emergency department-based study. Can Respir J. 2005;12:139–42. doi: 10.1155/2005/672501. [DOI] [PubMed] [Google Scholar]
- 14.Loh LC, Khoo SK, Quah SY, Visvalingam V, Radhakrishnan A, Vijayasingham P, et al. Adult community-acquired pneumonia in Malaysia: Prediction of mortality from severity assessment on admission. Respirology. 2004;9:379–86. doi: 10.1111/j.1440-1843.2004.00604.x. [DOI] [PubMed] [Google Scholar]
- 15.Fine MJ, Smith MA, Carson CA, Mutha SS, Sankey SS, Weissfeld LA, et al. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis. JAMA. 1996;275:134–41. [PubMed] [Google Scholar]
- 16.World Health Organization. Disease and injury country estimates. Accessed from WHO website on 12th Feb, 2012: http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html .
- 17.Shah BA, Ahmed W, Dhobi GN, Shah NN, Khursheed SQ, Haq I. Validity of pneumonia severity index and CURB-65 severity scoring systems in community acquired pneumonia in an Indian setting. Indian J Chest Dis Allied Sci. 2010;52:9–17. [PubMed] [Google Scholar]
- 18.Dey AB, Chaudhry R, Kumar P, Nisar N, Nagarkar KM. Mycoplasma pneumoniae and community-acquired pneumonia. Natl Med J India. 2000;13:66–70. [PubMed] [Google Scholar]
- 19.Bansal S, Kashyap S, Pal LS, Goel A. Clinical and bacteriological profile of community acquired pneumonia in Shimla, Himachal Pradesh. Indian J Chest Dis Allied Sci. 2004;46:17–22. [PubMed] [Google Scholar]
- 20.Capoor MR, Nair D, Aggarwal P, Gupta B. Rapid diagnosis of community-acquired pneumonia using the BacT/Alert 3D system. Braz J Infect Dis. 2006;10:352–6. doi: 10.1590/s1413-86702006000500010. [DOI] [PubMed] [Google Scholar]
- 21.Shibli F, Chazan B, Nitzan O, Flatau E, Edelstein H, Blondheim O, et al. Etiology of community-acquired pneumonia in hospitalized patients in northern Israel. Isr Med Assoc J. 2010;12:477–82. [PubMed] [Google Scholar]
- 22.Koksal I, Ozlu T, Bayraktar O, Yilmaz G, Bulbul Y, Oztuna F, et al. Etiological agents of community-acquired pneumonia in adult patients in Turkey: A multicentric, cross-sectional study. Tuberk Toraks. 2010;58:119–27. [PubMed] [Google Scholar]
- 23.Johansson N, Kalin M, Tiveljung-Lindell A, Giske CG, Hedlund J. Etiology of community-acquired pneumonia: Increased microbiological yield with new diagnostic methods. Clin Infect Dis. 2010;50:202–9. doi: 10.1086/648678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Diaz A, Barria P, Niederman M, Restrepo MI, Dreyse J, Fuentes G, et al. Etiology of community-acquired pneumonia in hospitalized patients in chile: The increasing prevalence of respiratory viruses among classic pathogens. Chest. 2007;131:779–87. doi: 10.1378/chest.06-1800. [DOI] [PubMed] [Google Scholar]
- 25.Huang HH, Zhang YY, Xiu QY, Zhou X, Huang SG, Lu Q, et al. Community-acquired pneumonia in Shanghai, China: Microbial etiology and implications for empirical therapy in a prospective study of 389 patients. Eur J Clin Microbiol Infect Dis. 2006;25:369–74. doi: 10.1007/s10096-006-0146-7. [DOI] [PubMed] [Google Scholar]
- 26.Al-Ali MK, Batchoun RG, Al-Nour TM. Etiology of community-acquired pneumonia in hospitalized patients in Jordan. Saudi Med J. 2006;27:813–6. [PubMed] [Google Scholar]
- 27.Marrie TJ, Poulin-Costello M, Beecroft MD, Herman-Gnjidic Z. Etiology of community-acquired pneumonia treated in an ambulatory setting. Respir Med. 2005;99:60–5. doi: 10.1016/j.rmed.2004.05.010. [DOI] [PubMed] [Google Scholar]
- 28.Lauderdale TL, Chang FY, Ben RJ, Yin HC, Ni YH, Tsai JW, et al. Etiology of community acquired pneumonia among adult patients requiring hospitalization in Taiwan. Respir Med. 2005;99:1079–86. doi: 10.1016/j.rmed.2005.02.026. [DOI] [PubMed] [Google Scholar]
- 29.Bartlett JG. Diagnostic tests for agents of community-acquired pneumonia. Clin Infect Dis. 2011;52(Suppl 4):S296–304. doi: 10.1093/cid/cir045. [DOI] [PubMed] [Google Scholar]
- 30.Javed S, Chaudhry R, Passi K, Sharma S, K P, Dhawan B, et al. Sero diagnosis of Legionella infection in community acquired pneumonia. Indian J Med Res. 2010;131:92–6. [PubMed] [Google Scholar]
- 31.Chong CP, Street PR. Pneumonia in the elderly: A review of the epidemiology, pathogenesis, microbiology, and clinical features. South Med J. 2008;101:1141–5. doi: 10.1097/SMJ.0b013e318181d5b5. quiz 32, 79. [DOI] [PubMed] [Google Scholar]
- 32.Fernandez-Sabe N, Carratala J, Roson B, Dorca J, Verdaguer R, Manresa F, et al. Community-acquired pneumonia in very elderly patients: Causative organisms, clinical characteristics, and outcomes. Medicine (Baltimore) 2003;82:159–69. doi: 10.1097/01.md.0000076005.64510.87. [DOI] [PubMed] [Google Scholar]
- 33.Stupka JE, Mortensen EM, Anzueto A, Restrepo MI. Community-acquired pneumonia in elderly patients. Aging Health. 2009;5:763–74. doi: 10.2217/ahe.09.74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ruiz M, Ewig S, Marcos MA, Martinez JA, Arancibia F, Mensa J, et al. Etiology of community-acquired pneumonia: Impact of age, comorbidity, and severity. Am J Respir Crit Care Med. 1999;160:397–405. doi: 10.1164/ajrccm.160.2.9808045. [DOI] [PubMed] [Google Scholar]
- 35.Shah BA, Singh G, Naik MA, Dhobi GN. Bacteriological and clinical profile of Community acquired pneumonia in hospitalized patients. Lung India. 2010;27:54–7. doi: 10.4103/0970-2113.63606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Torres A, Dorca J, Zalacain R, Bello S, El-Ebiary M, Molinos L, et al. Community-acquired pneumonia in chronic obstructive pulmonary disease: A Spanish multicenter study. Am J Respir Crit Care Med. 1996;154:1456–61. doi: 10.1164/ajrccm.154.5.8912764. [DOI] [PubMed] [Google Scholar]
- 37.Ostergaard L, Andersen PL. Etiology of community-acquired pneumonia. Evaluation by transtracheal aspiration, blood culture, or serology. Chest. 1993;104:1400–7. doi: 10.1378/chest.104.5.1400. [DOI] [PubMed] [Google Scholar]
- 38.Pifarre R, Falguera M, Vicente-de-Vera C, Nogues A. Characteristics of community-acquired pneumonia in patients with chronic obstructive pulmonary disease. Respir Med. 2007;101:2139–44. doi: 10.1016/j.rmed.2007.05.011. [DOI] [PubMed] [Google Scholar]
- 39.Liapikou A, Polverino E, Ewig S, Cilloniz C, Marcos MA, Mensa J, et al. Severity and outcomes of hospitalised community-acquired pneumonia in COPD patients. Eur Respir J. 2012;39:855–61. doi: 10.1183/09031936.00067111. Epub 2011 Sep 15. [DOI] [PubMed] [Google Scholar]
- 40.Samokhvalov AV, Irving HM, Rehm J. Alcohol consumption as a risk factor for pneumonia: A systematic review and meta-analysis. Epidemiol Infect. 2010;138:1789–95. doi: 10.1017/S0950268810000774. [DOI] [PubMed] [Google Scholar]
- 41.de Roux A, Cavalcanti M, Marcos MA, Garcia E, Ewig S, Mensa J, et al. Impact of alcohol abuse in the etiology and severity of community-acquired pneumonia. Chest. 2006;129:1219–25. doi: 10.1378/chest.129.5.1219. [DOI] [PubMed] [Google Scholar]
- 42.Falguera M, Pifarre R, Martin A, Sheikh A, Moreno A. Etiology and outcome of community-acquired pneumonia in patients with diabetes mellitus. Chest. 2005;128:3233–9. doi: 10.1378/chest.128.5.3233. [DOI] [PubMed] [Google Scholar]
- 43.Marrie TJ. Bacteraemic pneumococcal pneumonia: A continuously evolving disease. J Infect. 1992;24:247–55. doi: 10.1016/s0163-4453(05)80029-5. [DOI] [PubMed] [Google Scholar]
- 44.Murcia J, Llorens P, Sanchez-Paya J, Reus S, Boix V, Merino E, et al. Functional status determined by Barthel Index predicts community acquired pneumonia mortality in general population. J Infect. 2010;61:458–64. doi: 10.1016/j.jinf.2010.08.006. [DOI] [PubMed] [Google Scholar]
- 45.Yende S, van der Poll T, Lee M, Huang DT, Newman AB, Kong L, et al. The influence of pre-existing diabetes mellitus on the host immune response and outcome of pneumonia: Analysis of two multicentre cohort studies. Thorax. 2010;65:870–7. doi: 10.1136/thx.2010.136317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.von Baum H, Welte T, Marre R, Suttorp N, Ewig S. Community-acquired pneumonia through Enterobacteriaceae and Pseudomonas aeruginosa: Diagnosis, incidence and predictors. Eur Respir J. 2010;35:598–605. doi: 10.1183/09031936.00091809. [DOI] [PubMed] [Google Scholar]
- 47.Arancibia F, Bauer TT, Ewig S, Mensa J, Gonzalez J, Niederman MS, et al. Community-acquired pneumonia due to gram-negative bacteria and pseudomonas aeruginosa: Incidence, risk, and prognosis. Arch Intern Med. 2002;162:1849–58. doi: 10.1001/archinte.162.16.1849. [DOI] [PubMed] [Google Scholar]
- 48.Bruns AH, Oosterheert JJ, Prokop M, Lammers JW, Hak E, Hoepelman AI. Patterns of resolution of chest radiograph abnormalities in adults hospitalized with severe community-acquired pneumonia. Clin Infect Dis. 2007;45:983–91. doi: 10.1086/521893. [DOI] [PubMed] [Google Scholar]
- 49.Muller B, Harbarth S, Stolz D, Bingisser R, Mueller C, Leuppi J, et al. Diagnostic and prognostic accuracy of clinical and laboratory parameters in community-acquired pneumonia. BMC Infect Dis. 2007;7:10. doi: 10.1186/1471-2334-7-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Riquelme R, Torres A, el-Ebiary M, Mensa J, Estruch R, Ruiz M, et al. Community-acquired pneumonia in the elderly. Clinical and nutritional aspects. Am J Respir Crit Care Med. 1997;156:1908–14. doi: 10.1164/ajrccm.156.6.9702005. [DOI] [PubMed] [Google Scholar]
- 51.Sow O, Frechet M, Diallo AA, Soumah S, Conde MK, Diot P, et al. Community acquired pneumonia in adults: A study comparing clinical features and outcome in Africa (Republic of Guinea) and Europe (France) Thorax. 1996;51:385–8. doi: 10.1136/thx.51.4.385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Metlay JP, Fine MJ. Testing strategies in the initial management of patients with community-acquired pneumonia. Ann Intern Med. 2003;138:109–18. doi: 10.7326/0003-4819-138-2-200301210-00012. [DOI] [PubMed] [Google Scholar]
- 53.Kyriacou DN, Yarnold PR, Soltysik RC, Self WH, Wunderink RG, Schmitt BP, et al. Derivation of a triage algorithm for chest radiography of community-acquired pneumonia patients in the emergency department. Acad Emerg Med. 2008;15:40–4. doi: 10.1111/j.1553-2712.2007.00011.x. [DOI] [PubMed] [Google Scholar]
- 54.Metlay JP, Schulz R, Li YH, Singer DE, Marrie TJ, Coley CM, et al. Influence of age on symptoms at presentation in patients with community-acquired pneumonia. Arch Intern Med. 1997;157:1453–9. [PubMed] [Google Scholar]
- 55.Lieberman D, Shvartzman P, Korsonsky I. Diagnosis of ambulatory community-acquired pneumonia. Comparison of clinical assessment versus chest X-ray. Scand J Prim Health Care. 2003;21:57–60. doi: 10.1080/02813430310000582. [DOI] [PubMed] [Google Scholar]
- 56.O’Brien WT, Sr, Rohweder DA, Lattin GE, Jr, Thornton JA, Dutton JP, Ebert-Long DL, et al. Clinical indicators of radiographic findings in patients with suspected community-acquired pneumonia: Who needs a chest x-ray? J Am Coll Radiol. 2006;3:703–6. doi: 10.1016/j.jacr.2006.02.007. [DOI] [PubMed] [Google Scholar]
- 57.Hagaman JT, Rouan GW, Shipley RT, Panos RJ. Admission chest radiograph lacks sensitivity in the diagnosis of community-acquired pneumonia. Am J Med Sci. 2009;337:236–40. doi: 10.1097/MAJ.0b013e31818ad805. [DOI] [PubMed] [Google Scholar]
- 58.Albaum MN, Hill LC, Murphy M, Li YH, Fuhrman CR, Britton CA, et al. Interobserver reliability of the chest radiograph in community-acquired pneumonia. PORT Investigators. Chest. 1996;110:343–50. doi: 10.1378/chest.110.2.343. [DOI] [PubMed] [Google Scholar]
- 59.El Solh AA, Aquilina AT, Gunen H, Ramadan F. Radiographic resolution of community-acquired bacterial pneumonia in the elderly. J Am Geriatr Soc. 2004;52:224–9. doi: 10.1111/j.1532-5415.2004.52059.x. [DOI] [PubMed] [Google Scholar]
- 60.Bruns AH, Oosterheert JJ, El Moussaoui R, Opmeer BC, Hoepelman AI, Prins JM. Pneumonia recovery: Discrepancies in perspectives of the radiologist, physician and patient. J Gen Intern Med. 2010;25:203–6. doi: 10.1007/s11606-009-1182-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Kuru T, Lynch JP., 3rd Nonresolving or slowly resolving pneumonia. Clin Chest Med. 1999;20:623–51. doi: 10.1016/s0272-5231(05)70241-0. [DOI] [PubMed] [Google Scholar]
- 62.Tanaka N, Matsumoto T, Kuramitsu T, Nakaki H, Ito K, Uchisako H, et al. High resolution CT findings in community-acquired pneumonia. J Comput Assist Tomogr. 1996;20:600–8. doi: 10.1097/00004728-199607000-00019. [DOI] [PubMed] [Google Scholar]
- 63.Yagihashi K, Kurihara Y, Fujikawa A, Matsuoka S, Nakajima Y. Correlations between computed tomography findings and clinical manifestations of Streptococcus pneumoniae pneumonia. Jpn J Radiol. 2011;29:423–8. doi: 10.1007/s11604-011-0574-x. [DOI] [PubMed] [Google Scholar]
- 64.Ito I, Ishida T, Togashi K, Niimi A, Koyama H, Ishimori T, et al. Differentiation of bacterial and non-bacterial community-acquired pneumonia by thin-section computed tomography. Eur J Radiol. 2009;72:388–95. doi: 10.1016/j.ejrad.2008.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Hayden GE, Wrenn KW. Chest radiograph vs.computed tomography scan in the evaluation for pneumonia. J Emerg Med. 2009;36:266–70. doi: 10.1016/j.jemermed.2007.11.042. [DOI] [PubMed] [Google Scholar]
- 66.Benenson RS, Kepner AM, Pyle DN, 2nd, Cavanaugh S. Selective use of blood cultures in emergency department pneumonia patients. J Emerg Med. 2007;33:1–8. doi: 10.1016/j.jemermed.2006.12.034. [DOI] [PubMed] [Google Scholar]
- 67.Cham G, Yan S, Heng BH, Seow E. Predicting positive blood cultures in patients presenting with pneumonia at an Emergency Department in Singapore. Ann Acad Med Singapore. 2009;38:508–7. [PubMed] [Google Scholar]
- 68.Falguera M, Trujillano J, Caro S, Menendez R, Carratala J, Ruiz-Gonzalez A, et al. A prediction rule for estimating the risk of bacteremia in patients with community-acquired pneumonia. Clin Infect Dis. 2009;49:409–16. doi: 10.1086/600291. [DOI] [PubMed] [Google Scholar]
- 69.Marrie TJ. Blood cultures in ambulatory patients who are discharged from emergency with community-acquired pneumonia. Can J Infect Dis. 2004;15:21–4. doi: 10.1155/2004/530645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Nagata K, Hirota T, Fujiwara H. Analysis of blood cultures in patients presenting with community-acquired pneumonia at the emergency room. Nihon Kokyuki Gakkai Zasshi. 2010;48:661–7. [PubMed] [Google Scholar]
- 71.Paganin F, Lilienthal F, Bourdin A, Lugagne N, Tixier F, Genin R, et al. Severe community-acquired pneumonia: Assessment of microbial aetiology as mortality factor. Eur Respir J. 2004;24:779–85. doi: 10.1183/09031936.04.00119503. [DOI] [PubMed] [Google Scholar]
- 72.Ramanujam P, Rathlev NK. Blood cultures do not change management in hospitalized patients with community-acquired pneumonia. Acad Emerg Med. 2006;13:740–5. doi: 10.1197/j.aem.2006.03.554. [DOI] [PubMed] [Google Scholar]
- 73.Metersky ML, Ma A, Bratzler DW, Houck PM. Predicting bacteremia in patients with community-acquired pneumonia. Am J Respir Crit Care Med. 2004;169:342–7. doi: 10.1164/rccm.200309-1248OC. [DOI] [PubMed] [Google Scholar]
- 74.Afshar N, Tabas J, Afshar K, Silbergleit R. Blood cultures for community-acquired pneumonia: Are they worthy of two quality measures? A systematic review. J Hosp Med. 2009;4:112–23. doi: 10.1002/jhm.382. [DOI] [PubMed] [Google Scholar]
- 75.Cordero E, Pachon J, Rivero A, Giron-Gonzalez JA, Gomez-Mateos J, Merino MD, et al. Usefulness of sputum culture for diagnosis of bacterial pneumonia in HIV-infected patients. Eur J Clin Microbiol Infect Dis. 2002;21:362–7. doi: 10.1007/s10096-002-0729-x. [DOI] [PubMed] [Google Scholar]
- 76.Musher DM, Montoya R, Wanahita A. Diagnostic value of microscopic examination of Gram-stained sputum and sputum cultures in patients with bacteremic pneumococcal pneumonia. Clin Infect Dis. 2004;39:165–9. doi: 10.1086/421497. [DOI] [PubMed] [Google Scholar]
- 77.Reed WW, Byrd GS, Gates RH, Jr, Howard RS, Weaver MJ. Sputum gram's stain in community-acquired pneumococcal pneumonia. A meta-analysis. West J Med. 1996;165:197–204. [PMC free article] [PubMed] [Google Scholar]
- 78.Garcia I. Clinical Microbiology Procedures Handbook ASM. Washington DC: 2007. [Google Scholar]
- 79.Gutierrez F, Masia M, Rodriguez JC, Ayelo A, Soldan B, Cebrian L, et al. Evaluation of the immunochromatographic Binax NOW assay for detection of Streptococcus pneumoniae urinary antigen in a prospective study of community-acquired pneumonia in Spain. Clin Infect Dis. 2003;36:286–92. doi: 10.1086/345852. [DOI] [PubMed] [Google Scholar]
- 80.Roson B, Fernandez-Sabe N, Carratala J, Verdaguer R, Dorca J, Manresa F, et al. Contribution of a urinary antigen assay (Binax NOW) to the early diagnosis of pneumococcal pneumonia. Clin Infect Dis. 2004;38:222–6. doi: 10.1086/380639. [DOI] [PubMed] [Google Scholar]
- 81.Sorde R, Falco V, Lowak M, Domingo E, Ferrer A, Burgos J, et al. Current and potential usefulness of pneumococcal urinary antigen detection in hospitalized patients with community-acquired pneumonia to guide antimicrobial therapy. Arch Intern Med. 2011;171:166–72. doi: 10.1001/archinternmed.2010.347. [DOI] [PubMed] [Google Scholar]
- 82.Avni T, Mansur N, Leibovici L, Paul M. PCR using blood for diagnosis of invasive pneumococcal disease: Systematic review and meta-analysis. J Clin Microbiol. 2010;48:489–96. doi: 10.1128/JCM.01636-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Shimada T, Noguchi Y, Jackson JL, Miyashita J, Hayashino Y, Kamiya T, et al. Systematic review and metaanalysis: Urinary antigen tests for Legionellosis. Chest. 2009;136:1576–85. doi: 10.1378/chest.08-2602. [DOI] [PubMed] [Google Scholar]
- 84.Garbino J, Bornand JE, Uckay I, Fonseca S, Sax H. Impact of positive legionella urinary antigen test on patient management and improvement of antibiotic use. J Clin Pathol. 2004;57:1302–5. doi: 10.1136/jcp.2004.018861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Loens K, Ursi D, Goossens H, Ieven M. Molecular diagnosis of Mycoplasma pneumoniae respiratory tract infections. J Clin Microbiol. 2003;41:4915–23. doi: 10.1128/JCM.41.11.4915-4923.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Uldum SA, Jensen JS, Sondergard-Andersen J, Lind K. Enzyme immunoassay for detection of immunoglobulin M (IgM) and IgG antibodies to Mycoplasma pneumoniae. J Clin Microbiol. 1992;30:1198–204. doi: 10.1128/jcm.30.5.1198-1204.1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Zhang L, Zong ZY, Liu YB, Ye H, Lv XJ. PCR versus serology for diagnosing Mycoplasma pneumoniae infection: A systematic review & meta-analysis. Indian J Med Res. 2011;134:270–80. [PMC free article] [PubMed] [Google Scholar]
- 88.Villegas E, Sorlozano A, Gutierrez J. Serological diagnosis of Chlamydia pneumoniae infection: Limitations and perspectives. J Med Microbiol. 2010;59:1267–74. doi: 10.1099/jmm.0.020362-0. [DOI] [PubMed] [Google Scholar]
- 89.Bartlett JG. Is activity against “atypical” pathogens necessary in the treatment protocols for community-acquired pneumonia? Issues with combination therapy. Clin Infect Dis. 2008;47(Suppl 3):S232–6. doi: 10.1086/591409. [DOI] [PubMed] [Google Scholar]
- 90.von Baum H, Welte T, Marre R, Suttorp N, Luck C, Ewig S. Mycoplasma pneumoniae pneumonia revisited within the German Competence Network for Community-acquired pneumonia (CAPNETZ) BMC Infect Dis. 2009;9:62. doi: 10.1186/1471-2334-9-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Matsuzaki Y. Detection of influenza virus (RT-PCR assay and others) Nihon Rinsho. 2003;61:1909–13. [PubMed] [Google Scholar]
- 92.Levin KP, Hanusa BH, Rotondi A, Singer DE, Coley CM, Marrie TJ, et al. Arterial blood gas and pulse oximetry in initial management of patients with community-acquired pneumonia. J Gen Intern Med. 2001;16:590–8. doi: 10.1046/j.1525-1497.2001.016009590.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Bewick T, Greenwood S, Lim WS. What is the role of pulse oximetry in the assessment of patients with community-acquired pneumonia in primary care? Prim Care Respir J. 2010;19:378–82. doi: 10.4104/pcrj.2010.00049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Blot SI, Rodriguez A, Sole-Violan J, Blanquer J, Almirall J, Rello J. Effects of delayed oxygenation assessment on time to antibiotic delivery and mortality in patients with severe community-acquired pneumonia. Crit Care Med. 2007;35:2509–14. doi: 10.1097/01.CCM.0000287587.43801.9C. [DOI] [PubMed] [Google Scholar]
- 95.Berg P, Lindhardt BO. The role of procalcitonin in adult patients with community-acquired pneumonia - a systemativ review. Dan Med J. 2012;59:A4357. [PubMed] [Google Scholar]
- 96.Christ-Crain M, Jaccard-Stolz D, Bingisser R, Gencay MM, Huber PR, Tamm M, et al. Effect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: Cluster-randomised, single-blinded intervention trial. Lancet. 2004;363:600–7. doi: 10.1016/S0140-6736(04)15591-8. [DOI] [PubMed] [Google Scholar]
- 97.Kruger S, Ewig S, Marre R, Papassotiriou J, Richter K, von Baum H, et al. Procalcitonin predicts patients at low risk of death from community-acquired pneumonia across all CRB-65 classes. Eur Respir J. 2008;31:349–55. doi: 10.1183/09031936.00054507. [DOI] [PubMed] [Google Scholar]
- 98.Christ-Crain M, Stolz D, Bingisser R, Muller C, Miedinger D, Huber PR, et al. Procalcitonin guidance of antibiotic therapy in community-acquired pneumonia: A randomized trial. Am J Respir Crit Care Med. 2006;174:84–93. doi: 10.1164/rccm.200512-1922OC. [DOI] [PubMed] [Google Scholar]
- 99.Garcia Vazquez E, Martinez JA, Mensa J, Sanchez F, Marcos MA, de Roux A, et al. C-reactive protein levels in community-acquired pneumonia. Eur Respir J. 2003;21:702–5. doi: 10.1183/09031936.03.00080203. [DOI] [PubMed] [Google Scholar]
- 100.Flanders SA, Stein J, Shochat G, Sellers K, Holland M, Maselli J, et al. Performance of a bedside C-reactive protein test in the diagnosis of community-acquired pneumonia in adults with acute cough. Am J Med. 2004;116:529–35. doi: 10.1016/j.amjmed.2003.11.023. [DOI] [PubMed] [Google Scholar]
- 101.Bafadhel M, Clark TW, Reid C, Medina MJ, Batham S, Barer MR, et al. Procalcitonin and C-reactive protein in hospitalized adult patients with community-acquired pneumonia or exacerbation of asthma or COPD. Chest. 2011;139:1410–8. doi: 10.1378/chest.10-1747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Falk G, Fahey T. C-reactive protein and community-acquired pneumonia in ambulatory care: Systematic review of diagnostic accuracy studies. Fam Pract. 2009;26:10–21. doi: 10.1093/fampra/cmn095. [DOI] [PubMed] [Google Scholar]
- 103.Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–72. doi: 10.1086/511159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Aujesky D, Fine MJ. The pneumonia severity index: A decade after the initial derivation and validation. Clin Infect Dis. 2008;47(Suppl 3):S133–9. doi: 10.1086/591394. [DOI] [PubMed] [Google Scholar]
- 105.Jo S, Kim K, Jung K, Rhee JE, Cho IS, Lee CC, et al. The effects of incorporating a pneumonia severity index into the admission protocol for community-acquired pneumonia. J Emerg Med. 2012;42:133–8. doi: 10.1016/j.jemermed.2010.04.018. Epub 2010 Jun 12. [DOI] [PubMed] [Google Scholar]
- 106.Aujesky D, McCausland JB, Whittle J, Obrosky DS, Yealy DM, Fine MJ. Reasons why emergency department providers do not rely on the pneumonia severity index to determine the initial site of treatment for patients with pneumonia. Clin Infect Dis. 2009;49:e100–8. doi: 10.1086/644741. [DOI] [PubMed] [Google Scholar]
- 107.Lee RW, Lindstrom ST. A teaching hospital's experience applying the Pneumonia Severity Index and antibiotic guidelines in the management of community-acquired pneumonia. Respirology. 2007;12:754–8. doi: 10.1111/j.1440-1843.2007.01121.x. [DOI] [PubMed] [Google Scholar]
- 108.Lim WS, van der Eerden MM, Laing R, Boersma WG, Karalus N, Town GI, et al. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax. 2003;58:377–82. doi: 10.1136/thorax.58.5.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Barlow G, Nathwani D, Davey P. The CURB65 pneumonia severity score outperforms generic sepsis and early warning scores in predicting mortality in community-acquired pneumonia. Thorax. 2007;62:253–9. doi: 10.1136/thx.2006.067371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Chalmers JD, Singanayagam A, Akram AR, Choudhury G, Mandal P, Hill AT. Safety and efficacy of CURB65-guided antibiotic therapy in community-acquired pneumonia. J Antimicrob Chemother. 2011;66:416–23. doi: 10.1093/jac/dkq426. [DOI] [PubMed] [Google Scholar]
- 111.Guo Q, Li HY, Zhou YP, Li M, Chen XK, Liu H, et al. Compliance with the CURB-65 score and the consequences of non-implementation. Int J Tuberc Lung Dis. 2011;15:1697–702. doi: 10.5588/ijtld.11.0169. [DOI] [PubMed] [Google Scholar]
- 112.Parsonage M, Nathwani D, Davey P, Barlow G. Evaluation of the performance of CURB-65 with increasing age. Clin Microbiol Infect. 2009;15:858–64. doi: 10.1111/j.1469-0691.2009.02908.x. [DOI] [PubMed] [Google Scholar]
- 113.Sanz F, Restrepo MI, Fernandez E, Mortensen EM, Aguar MC, Cervera A, et al. Hypoxemia adds to the CURB-65 pneumonia severity score in hospitalized patients with mild pneumonia. Respir Care. 2011;56:612–8. doi: 10.4187/respcare.00853. [DOI] [PubMed] [Google Scholar]
- 114.Aliberti S, Ramirez J, Cosentini R, Brambilla AM, Zanaboni AM, Rossetti V, et al. Low CURB-65 is of limited value in deciding discharge of patients with community-acquired pneumonia. Respir Med. 2011;105:1732–8. doi: 10.1016/j.rmed.2011.07.006. [DOI] [PubMed] [Google Scholar]
- 115.Charles PG, Wolfe R, Whitby M, Fine MJ, Fuller AJ, Stirling R, et al. SMART-COP: A tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis. 2008;47:375–84. doi: 10.1086/589754. [DOI] [PubMed] [Google Scholar]
- 116.Dwyer R, Hedlund J, Darenberg J, Henriques-Normark B, Naucler P, Runesdotter S, et al. Improvement of CRB-65 as a prognostic scoring system in adult patients with bacteraemic pneumococcal pneumonia. Scand J Infect Dis. 2011;43:448–55. doi: 10.3109/00365548.2011.562529. [DOI] [PubMed] [Google Scholar]
- 117.Moammar MQ, Azam HM, Blamoun AI, Rashid AO, Ismail M, Khan MA, et al. Alveolar-arterial oxygen gradient, pneumonia severity index and outcomes in patients hospitalized with community acquired pneumonia. Clin Exp Pharmacol Physiol. 2008;35:1032–7. doi: 10.1111/j.1440-1681.2008.04971.x. [DOI] [PubMed] [Google Scholar]
- 118.McNally M, Curtain J, O’Brien KK, Dimitrov BD, Fahey T. Validity of British Thoracic Society guidance (the CRB-65 rule) for predicting the severity of pneumonia in general practice: Systematic review and meta-analysis. Br J Gen Pract. 2010;60:e423–33. doi: 10.3399/bjgp10X532422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Vila Corcoles A, Ochoa Gondar O, Rodriguez Blanco T. Usefulness of the CRB-65 scale for prognosis assessment of patients 65 years or older with community-acquired pneumonia. Med Clin (Barc) 2010;135:97–102. doi: 10.1016/j.medcli.2009.09.049. [DOI] [PubMed] [Google Scholar]
- 120.Woodhead M, Blasi F, Ewig S, Garau J, Huchon G, Ieven M, et al. Guidelines for the management of adult lower respiratory tract infections--full version. Clin Microbiol Infect. 2011;17(Suppl 6):E1–59. doi: 10.1111/j.1469-0691.2011.03672.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Sabatier C, Peredo R, Villagra A, Bacelar N, Mariscal D, Ferrer R, et al. Community-acquired pneumonia: A 7-years descriptive study. Usefulness of the IDSA/ATS 2007 in the assessment of ICU admission. Med Intensiva. 2010;34:237–45. doi: 10.1016/j.medin.2009.11.008. [DOI] [PubMed] [Google Scholar]
- 122.Liapikou A, Ferrer M, Polverino E, Balasso V, Esperatti M, Piner R, et al. Severe community-acquired pneumonia: Validation of the Infectious Diseases Society of America/American Thoracic Society guidelines to predict an intensive care unit admission. Clin Infect Dis. 2009;48:377–85. doi: 10.1086/596307. [DOI] [PubMed] [Google Scholar]
- 123.Chalmers JD, Taylor JK, Mandal P, Choudhury G, Singanayagam A, Akram AR, et al. Validation of the Infectious Diseases Society of America/American Thoratic Society minor criteria for intensive care unit admission in community-acquired pneumonia patients without major criteria or contraindications to intensive care unit care. Clin Infect Dis. 2011;53:503–11. doi: 10.1093/cid/cir463. [DOI] [PubMed] [Google Scholar]
- 124.Phua J, See KC, Chan YH, Widjaja LS, Aung NW, Ngerng WJ, et al. Validation and clinical implications of the IDSA/ATS minor criteria for severe community-acquired pneumonia. Thorax. 2009;64:598–603. doi: 10.1136/thx.2009.113795. [DOI] [PubMed] [Google Scholar]
- 125.Kontou P, Kuti JL, Nicolau DP. Validation of the Infectious Diseases Society of America/American Thoracic Society criteria to predict severe community-acquired pneumonia caused by Streptococcus pneumoniae. Am J Emerg Med. 2009;27:968–74. doi: 10.1016/j.ajem.2008.07.037. [DOI] [PubMed] [Google Scholar]
- 126.Guo Q, Li HY, Zhou YP, Li M, Chen XK, Liu H, et al. Weight of the IDSA/ATS minor criteria for severe community-acquired pneumonia. Respir Med. 2011;105:1543–9. doi: 10.1016/j.rmed.2011.06.010. [DOI] [PubMed] [Google Scholar]
- 127.Schaaf B, Kruse J, Rupp J, Reinert RR, Droemann D, Zabel P, et al. Sepsis severity predicts outcome in community-acquired pneumococcal pneumonia. Eur Respir J. 2007;30:517–24. doi: 10.1183/09031936.00021007. [DOI] [PubMed] [Google Scholar]
- 128.Renaud B, Labarere J, Coma E, Santin A, Hayon J, Gurgui M, et al. Risk stratification of early admission to the intensive care unit of patients with no major criteria of severe community-acquired pneumonia: Development of an international prediction rule. Crit Care. 2009;13:R54. doi: 10.1186/cc7781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Sankaran P, Kamath AV, Tariq SM, Ruffell H, Smith AC, Prentice P, et al. Are shock index and adjusted shock index useful in predicting mortality and length of stay in community-acquired pneumonia? Eur J Intern Med. 2011;22:282–5. doi: 10.1016/j.ejim.2010.12.009. [DOI] [PubMed] [Google Scholar]
- 130.Saldias F, Diaz O. Severity scores for predicting clinically relevant outcomes for immunocompetent adult patients hospitalized with community-acquired pneumococcal pneumonia. Rev Chilena Infectol. 2011;28:303–9. [PubMed] [Google Scholar]
- 131.Rello J, Rodriguez A, Lisboa T, Gallego M, Lujan M, Wunderink R. PIRO score for community-acquired pneumonia: A new prediction rule for assessment of severity in intensive care unit patients with community-acquired pneumonia. Crit Care Med. 2009;37:456–62. doi: 10.1097/CCM.0b013e318194b021. [DOI] [PubMed] [Google Scholar]
- 132.Musonda P, Sankaran P, Subramanian DN, Smith AC, Prentice P, Tariq SM, et al. Prediction of mortality in community-acquired pneumonia in hospitalized patients. Am J Med Sci. 2011;342:489–93. doi: 10.1097/MAJ.0b013e31822cb95f. [DOI] [PubMed] [Google Scholar]
- 133.Li JS, Li SY, Yu XQ, Sun ZK, Zhang W, Jia XH, et al. CCERW: A new rule to predict treatment failure in patients with community-acquired pneumonia in middle aged and elderly people. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2011;23:10–7. [PubMed] [Google Scholar]
- 134.Khalil A, Kelen G, Rothman RE. A simple screening tool for identification of community-acquired pneumonia in an inner city emergency department. Emerg Med J. 2007;24:336–8. doi: 10.1136/emj.2007.045989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Espana PP, Capelastegui A, Quintana JM, Bilbao A, Diez R, Pascual S, et al. Validation and comparison of SCAP as a predictive score for identifying low-risk patients in community-acquired pneumonia. J Infect. 2010;60:106–13. doi: 10.1016/j.jinf.2009.11.013. [DOI] [PubMed] [Google Scholar]
- 136.Bauer TT, Ewig S, Marre R, Suttorp N, Welte T. CRB-65 predicts death from community-acquired pneumonia. J Intern Med. 2006;260:93–101. doi: 10.1111/j.1365-2796.2006.01657.x. [DOI] [PubMed] [Google Scholar]
- 137.Feldman C. Prognostic scoring systems: Which one is best? Curr Opin Infect Dis. 2007;20:165–9. doi: 10.1097/QCO.0b013e328014da75. [DOI] [PubMed] [Google Scholar]
- 138.Man SY, Lee N, Ip M, Antonio GE, Chau SS, Mak P, et al. Prospective comparison of three predictive rules for assessing severity of community-acquired pneumonia in Hong Kong. Thorax. 2007;62:348–53. doi: 10.1136/thx.2006.069740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Rello J, Rodriguez A. Severity of illness assessment for managing community-acquired pneumonia. Intensive Care Med. 2007;33:2043–4. doi: 10.1007/s00134-007-0896-4. [DOI] [PubMed] [Google Scholar]
- 140.Valencia M, Badia JR, Cavalcanti M, Ferrer M, Agusti C, Angrill J, et al. Pneumonia severity index class v patients with community-acquired pneumonia: Characteristics, outcomes, and value of severity scores. Chest. 2007;132:515–22. doi: 10.1378/chest.07-0306. [DOI] [PubMed] [Google Scholar]
- 141.Ananda-Rajah MR, Charles PG, Melvani S, Burrell LL, Johnson PD, Grayson ML. Comparing the pneumonia severity index with CURB-65 in patients admitted with community acquired pneumonia. Scand J Infect Dis. 2008;40:293–300. doi: 10.1080/00365540701663381. [DOI] [PubMed] [Google Scholar]
- 142.Chalmers JD, Singanayagam A, Hill AT. Predicting the need for mechanical ventilation and/or inotropic support for young adults admitted to the hospital with community-acquired pneumonia. Clin Infect Dis. 2008;47:1571–4. doi: 10.1086/593195. [DOI] [PubMed] [Google Scholar]
- 143.Johnstone J, Majumdar SR, Marrie TJ. The value of prognostic indices for pneumonia. Curr Infect Dis Rep. 2008;10:215–22. doi: 10.1007/s11908-008-0036-5. [DOI] [PubMed] [Google Scholar]
- 144.Rello J. Demographics, guidelines, and clinical experience in severe community-acquired pneumonia. Crit Care. 2008;12(Suppl 6):S2. doi: 10.1186/cc7025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Seymann G, Barger K, Choo S, Sawhney S, Davis D. Clinical judgment versus the Pneumonia Severity Index in making the admission decision. J Emerg Med. 2008;34:261–8. doi: 10.1016/j.jemermed.2007.05.050. [DOI] [PubMed] [Google Scholar]
- 146.Chalmers JD. ICU admission and severity assessment in community-acquired pneumonia. Crit Care. 2009;13:156. doi: 10.1186/cc7889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Feldman C, Alanee S, Yu VL, Richards GA, Ortqvist A, Rello J, et al. Severity of illness scoring systems in patients with bacteraemic pneumococcal pneumonia: Implications for the intensive care unit care. Clin Microbiol Infect. 2009;15:850–7. doi: 10.1111/j.1469-0691.2009.02901.x. [DOI] [PubMed] [Google Scholar]
- 148.Myint PK, Sankaran P, Musonda P, Subramanian DN, Ruffell H, Smith AC, et al. Performance of CURB-65 and CURB-age in community-acquired pneumonia. Int J Clin Pract. 2009;63:1345–50. doi: 10.1111/j.1742-1241.2009.02147.x. [DOI] [PubMed] [Google Scholar]
- 149.Usui K, Tanaka Y, Noda H, Ishihara T. Comparison of three prediction rules for prognosis in community acquired pneumonia: Pneumonia Severity Index (PSI), CURB-65, and A-DROP. Nihon Kokyuki Gakkai Zasshi. 2009;47:781–5. [PubMed] [Google Scholar]
- 150.Yandiola PP, Capelastegui A, Quintana J, Diez R, Gorordo I, Bilbao A, et al. Prospective comparison of severity scores for predicting clinically relevant outcomes for patients hospitalized with community-acquired pneumonia. Chest. 2009;135:1572–9. doi: 10.1378/chest.08-2179. [DOI] [PubMed] [Google Scholar]
- 151.Arnold FW, Brock GN, Peyrani P, Rodriguez EL, Diaz AA, Rossi P, et al. Predictive accuracy of the pneumonia severity index vs CRB-65 for time to clinical stability: Results from the Community-Acquired Pneumonia Organization (CAPO) International Cohort Study. Respir Med. 2010;104:1736–43. doi: 10.1016/j.rmed.2010.05.022. [DOI] [PubMed] [Google Scholar]
- 152.Chalmers JD, Singanayagam A, Akram AR, Mandal P, Short PM, Choudhury G, et al. Severity assessment tools for predicting mortality in hospitalised patients with community-acquired pneumonia. Systematic review and meta-analysis. Thorax. 2010;65:878–83. doi: 10.1136/thx.2009.133280. [DOI] [PubMed] [Google Scholar]
- 153.Loke YK, Kwok CS, Niruban A, Myint PK. Value of severity scales in predicting mortality from community-acquired pneumonia: Systematic review and meta-analysis. Thorax. 2010;65:884–90. doi: 10.1136/thx.2009.134072. [DOI] [PubMed] [Google Scholar]
- 154.Torralba MA, Amores-Arriaga B, Olivera S, Perez-Calvo JI. Validity of Fine and CURB scales in the treatment of community-acquired pneumonia in adults. Med Clin (Barc) 2010;135:624–5. doi: 10.1016/j.medcli.2009.08.001. [DOI] [PubMed] [Google Scholar]
- 155.Akram AR, Chalmers JD, Hill AT. Predicting mortality with severity assessment tools in out-patients with community-acquired pneumonia. QJM. 2011;104:871–9. doi: 10.1093/qjmed/hcr088. [DOI] [PubMed] [Google Scholar]
- 156.Falcone M, Corrao S, Venditti M, Serra P, Licata G. Performance of PSI, CURB-65, and SCAP scores in predicting the outcome of patients with community-acquired and healthcare-associated pneumonia. Intern Emerg Med. 2011;6:431–6. doi: 10.1007/s11739-011-0521-y. [DOI] [PubMed] [Google Scholar]
- 157.Fukuyama H, Ishida T, Tachibana H, Nakagawa H, Iwasaku M, Saigusa M, et al. Validation of scoring systems for predicting severe community-acquired pneumonia. Intern Med. 2011;50:1917–22. doi: 10.2169/internalmedicine.50.5279. [DOI] [PubMed] [Google Scholar]
- 158.Heppner HJ, Sehlhoff B, Niklaus D, Pientka L, Thiem U. [Pneumonia Severity Index (PSI), CURB-65, and mortality in hospitalized elderly patients with aspiration pneumonia] Z Gerontol Geriatr. 2011;44:229–34. doi: 10.1007/s00391-011-0184-3. [DOI] [PubMed] [Google Scholar]
- 159.Huaman MA, Diaz-Kuan A, Hegab S, Brar I, Kaatz S. CURB-65 and SMRT-CO in the prediction of early transfers to the intensive care unit among patients with community-acquired pneumonia initially admitted to a general ward. J Hosp Med. 2011;6:513–8. doi: 10.1002/jhm.921. [DOI] [PubMed] [Google Scholar]
- 160.Ochoa-Gondar O, Vila-Corcoles A, Rodriguez-Blanco T, Ramos F, de Diego C, Salsench E, et al. Comparison of three predictive rules for assessing severity in elderly patients with CAP. Int J Clin Pract. 2011;65:1165–72. doi: 10.1111/j.1742-1241.2011.02742.x. [DOI] [PubMed] [Google Scholar]
- 161.Naik M, Dhobi G, Shah B, Singh G. Bacteriological and clinical profile of Community acquired pneumonia in hospitalized patients. Lung India. 2010;27:54–7. doi: 10.4103/0970-2113.63606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Mills GD, Oehley MR, Arrol B. Effectiveness of beta lactam antibiotics compared with antibiotics active against atypical pathogens in non-severe community acquired pneumonia: Meta-analysis. BMJ. 2005;330:456. doi: 10.1136/bmj.38334.591586.82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Shefet D, Robenshtock E, Paul M, Leibovici L. Empiric antibiotic coverage of atypical pathogens for community acquired pneumonia in hospitalized adults. Cochrane Database Syst Rev. 2005:CD004418. doi: 10.1002/14651858.CD004418.pub2. [DOI] [PubMed] [Google Scholar]
- 164.Metersky ML, Ma A, Houck PM, Bratzler DW. Antibiotics for bacteremic pneumonia: Improved outcomes with macrolides but not fluoroquinolones. Chest. 2007;131:466–73. doi: 10.1378/chest.06-1426. [DOI] [PubMed] [Google Scholar]
- 165.Reyes Calzada S, Martinez Tomas R, Cremades Romero MJ, Martinez Moragon E, Soler Cataluna JJ, Menendez Villanueva R. Empiric treatment in hospitalized community-acquired pneumonia. Impact on mortality, length of stay and re-admission. Respir Med. 2007;101:1909–15. doi: 10.1016/j.rmed.2007.04.018. [DOI] [PubMed] [Google Scholar]
- 166.Iannini PB, Paladino JA, Lavin B, Singer ME, Schentag JJ. A case series of macrolide treatment failures in community acquired pneumonia. J Chemother. 2007;19:536–45. doi: 10.1179/joc.2007.19.5.536. [DOI] [PubMed] [Google Scholar]
- 167.Tamm M, Todisco T, Feldman C, Garbino J, Blasi F, Hogan P, et al. Clinical and bacteriological outcomes in hospitalised patients with communityacquired pneumonia treated with azithromycin plus ceftriaxone, or ceftriaxone plus clarithromycin or erythromycin: A prospective, randomised, multicentre study. Clin Microbiol Infect. 2007;13:162–71. doi: 10.1111/j.1469-0691.2006.01633.x. [DOI] [PubMed] [Google Scholar]
- 168.Dartois N, Castaing N, Gandjini H, Cooper A. Tigecycline versus levofloxacin for the treatment of community-acquired pneumonia: European experience. J Chemother. 2008;20(Suppl 1):28–35. doi: 10.1179/joc.2008.20.Supplement-1.28. [DOI] [PubMed] [Google Scholar]
- 169.Lloyd A, Holman A, Evers T. A cost-minimisation analysis comparing moxifloxacin with levofloxacin plus ceftriaxone for the treatment of patients with community-acquired pneumonia in Germany: Results from the MOTIV trial. Curr Med Res Opin. 2008;24:1279–84. doi: 10.1185/030079908x280400. [DOI] [PubMed] [Google Scholar]
- 170.Maipmon N, Nopmaneejumruslers C, Marras TK. Antibacterial class is not obviously important in outpatient pneumonia: A meta-analysis. Eur Respir J. 2008;31:1068–76. doi: 10.1183/09031936.00109007. [DOI] [PubMed] [Google Scholar]
- 171.Paris R, Confalonieri M, Dal Negro R, Ligia GP, Mos L, Todisco T, et al. Efficacy and safety of azithromycin 1 g once daily for 3 days in the treatment of community-acquired pneumonia: An open-label randomised comparison with amoxicillin-clavulanate 875/125 mg twice daily for 7 days. J Chemother. 2008;20:77–86. doi: 10.1179/joc.2008.20.1.77. [DOI] [PubMed] [Google Scholar]
- 172.Pertel PE, Bernardo P, Fogarty C, Matthews P, Northland R, Benvenuto M, et al. Effects of prior effective therapy on the efficacy of daptomycin and ceftriaxone for the treatment of community-acquired pneumonia. Clin Infect Dis. 2008;46:1142–51. doi: 10.1086/533441. [DOI] [PubMed] [Google Scholar]
- 173.Ye X, Sikirica V, Schein JR, Grant R, Zarotsky V, Doshi D, et al. Treatment failure rates and health care utilization and costs among patients with community-acquired pneumonia treated with levofloxacin or macrolides in an outpatient setting: A retrospective claims database analysis. Clin Ther. 2008;30:358–71. doi: 10.1016/j.clinthera.2008.01.023. [DOI] [PubMed] [Google Scholar]
- 174.Bergallo C, Jasovich A, Teglia O, Oliva ME, Lentnek A, de Wouters L, et al. Safety and efficacy of intravenous tigecycline in treatment of community-acquired pneumonia: Results from a double-blind randomized phase 3 comparison study with levofloxacin. Diagn Microbiol Infect Dis. 2009;63:52–61. doi: 10.1016/j.diagmicrobio.2008.09.001. [DOI] [PubMed] [Google Scholar]
- 175.Bjerre LM, Verheij TJ, Kochen MM. Antibiotics for community acquired pneumonia in adult outpatients. Cochrane Database Syst Rev. 2009:CD002109. doi: 10.1002/14651858.CD002109.pub2. [DOI] [PubMed] [Google Scholar]
- 176.Liu Y, Chen M, Zhao T, Wang H, Wang R, Cai B, et al. Causative agent distribution and antibiotic therapy assessment among adult patients with community acquired pneumonia in Chinese urban population. BMC Infect Dis. 2009;9:31. doi: 10.1186/1471-2334-9-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Lui G, Ip M, Lee N, Rainer TH, Man SY, Cockram CS, et al. Role of ‘atypical pathogens’ among adult hospitalized patients with community-acquired pneumonia. Respirology. 2009;14:1098–105. doi: 10.1111/j.1440-1843.2009.01637.x. [DOI] [PubMed] [Google Scholar]
- 178.Tanaseanu C, Milutinovic S, Calistru PI, Strausz J, Zolubas M, Chernyak V, et al. Efficacy and safety of tigecycline versus levofloxacin for community-acquired pneumonia. BMC Pulm Med. 2009;9:44. doi: 10.1186/1471-2466-9-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.Tessmer A, Welte T, Martus P, Schnoor M, Marre R, Suttorp N. Impact of intravenous {beta}-lactam/macrolide versus {beta}-lactam monotherapy on mortality in hospitalized patients with community-acquired pneumonia. J Antimicrob Chemother. 2009;63:1025–33. doi: 10.1093/jac/dkp088. [DOI] [PubMed] [Google Scholar]
- 180.An MM, Zou Z, Shen H, Gao PH, Cao YB, Jiang YY. Moxifloxacin monotherapy versus beta-lactam-based standard therapy for community-acquired pneumonia: A meta-analysis of randomised controlled trials. Int J Antimicrob Agents. 2010;36:58–65. doi: 10.1016/j.ijantimicag.2010.03.010. [DOI] [PubMed] [Google Scholar]
- 181.File TM, Jr, Low DE, Eckburg PB, Talbot GH, Friedland HD, Lee J, et al. Integrated analysis of FOCUS 1 and FOCUS 2: Randomized, doubled-blinded, multicenter phase 3 trials of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in patients with community-acquired pneumonia. Clin Infect Dis. 2010;51:1395–405. doi: 10.1086/657313. [DOI] [PubMed] [Google Scholar]
- 182.Hess G, Hill JW, Raut MK, Fisher AC, Mody S, Schein JR, et al. Comparative antibiotic failure rates in the treatment of community-acquired pneumonia: Results from a claims analysis. Adv Ther. 2010;27:743–55. doi: 10.1007/s12325-010-0062-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 183.Cai Y, Wang R, Liang B, Bai N, Liu Y. Systematic review and meta-analysis of the effectiveness and safety of tigecycline for treatment of infectious disease. Antimicrob Agents Chemother. 2011;55:1162–72. doi: 10.1128/AAC.01402-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 184.Ewig S, Hecker H, Suttorp N, Marre R, Welte T. Moxifloxacin monotherapy versus ss-lactam mono- or combination therapy in hospitalized patients with community-acquired pneumonia. J Infect. 2011;62:218–25. doi: 10.1016/j.jinf.2011.01.009. [DOI] [PubMed] [Google Scholar]
- 185.Waterer GW, Somes GW, Wunderink RG. Monotherapy may be suboptimal for severe bacteremic pneumococcal pneumonia. Arch Intern Med. 2001;161:1837–42. doi: 10.1001/archinte.161.15.1837. [DOI] [PubMed] [Google Scholar]
- 186.Martinez JA, Horcajada JP, Almela M, Marco F, Soriano A, Garcia E, et al. Addition of a macrolide to a beta-lactam-based empirical antibiotic regimen is associated with lower in-hospital mortality for patients with bacteremic pneumococcal pneumonia. Clin Infect Dis. 2003;36:389–95. doi: 10.1086/367541. [DOI] [PubMed] [Google Scholar]
- 187.Baddour LM, Yu VL, Klugman KP, Feldman C, Ortqvist A, Rello J, et al. Combination antibiotic therapy lowers mortality among severely ill patients with pneumococcal bacteremia. Am J Respir Crit Care Med. 2004;170:440–4. doi: 10.1164/rccm.200311-1578OC. [DOI] [PubMed] [Google Scholar]
- 188.Weiss K, Low DE, Cortes L, Beaupre A, Gauthier R, Gregoire P, et al. Clinical characteristics at initial presentation and impact of dual therapy on the outcome of bacteremic Streptococcus pneumoniae pneumonia in adults. Can Respir J. 2004;11:589–93. doi: 10.1155/2004/461392. [DOI] [PubMed] [Google Scholar]
- 189.Chokshi R, Restrepo MI, Weeratunge N, Frei CR, Anzueto A, Mortensen EM. Monotherapy versus combination antibiotic therapy for patients with bacteremic Streptococcus pneumoniae community-acquired pneumonia. Eur J Clin Microbiol Infect Dis. 2007;26:447–51. doi: 10.1007/s10096-007-0307-3. [DOI] [PubMed] [Google Scholar]
- 190.Bordon J, Peyrani P, Brock GN, Blasi F, Rello J, File T, et al. The presence of pneumococcal bacteremia does not influence clinical outcomes in patients with community-acquired pneumonia: Results from the Community-Acquired Pneumonia Organization (CAPO) International Cohort study. Chest. 2008;133:618–24. doi: 10.1378/chest.07-1322. [DOI] [PubMed] [Google Scholar]
- 191.Bratzler DW, Ma A, Nsa W. Initial antibiotic selection and patient outcomes: Observations from the National Pneumonia Project. Clin Infect Dis. 2008;47(Suppl 3):S193–201. doi: 10.1086/591404. [DOI] [PubMed] [Google Scholar]
- 192.Jover F, Cuadrado JM, Andreu L, Martinez S, Canizares R, de la Tabla VO, et al. A comparative study of bacteremic and non-bacteremic pneumococcal pneumonia. Eur J Intern Med. 2008;19:15–21. doi: 10.1016/j.ejim.2007.03.015. [DOI] [PubMed] [Google Scholar]
- 193.Ray WA, Murray KT, Hall K, Arbogast PG, Stein CM. Azithromycin and the risk of cardiovascular death. N Engl J Med. 2012;366:1881–90. doi: 10.1056/NEJMoa1003833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194.Vardakas KZ, Siempos II, Grammatikos A, Athanassa Z, Korbila IP, Falagas ME. Respiratory fluoroquinolones for the treatment of community-acquired pneumonia: A meta-analysis of randomized controlled trials. CMAJ. 2008;179:1269–77. doi: 10.1503/cmaj.080358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 195.Long R, Chong H, Hoeppner V, Shanmuganathan H, Kowalewska-Grochowska K, Shandro C, et al. Empirical treatment of community-acquired pneumonia and the development of fluoroquinolone-resistant tuberculosis. Clin Infect Dis. 2009;48:1354–60. doi: 10.1086/598196. [DOI] [PubMed] [Google Scholar]
- 196.Chang KC, Leung CC, Yew WW, Lau TY, Leung WM, Tam CM, et al. Newer fluoroquinolones for treating respiratory infection: Do they mask tuberculosis? Eur Respir J. 2010;35:606–13. doi: 10.1183/09031936.00104209. [DOI] [PubMed] [Google Scholar]
- 197.Chen TC, Lu PL, Lin CY, Lin WR, Chen YH. Fluoroquinolones are associated with delayed treatment and resistance in tuberculosis: A systematic review and meta-analysis. Int J Infect Dis. 2011;15:e211–6. doi: 10.1016/j.ijid.2010.11.008. [DOI] [PubMed] [Google Scholar]
- 198.Devasia RA, Blackman A, Gebretsadik T, Griffin M, Shintani A, May C, et al. Fluoroquinolone resistance in Mycobacterium tuberculosis: The effect of duration and timing of fluoroquinolone exposure. Am J Respir Crit Care Med. 2009;180:365–70. doi: 10.1164/rccm.200901-0146OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199.Wang JY, Hsueh PR, Jan IS, Lee LN, Liaw YS, Yang PC, et al. Empirical treatment with a fluoroquinolone delays the treatment for tuberculosis and is associated with a poor prognosis in endemic areas. Thorax. 2006;61:903–8. doi: 10.1136/thx.2005.056887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 200.Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med. 2008;34:17–60. doi: 10.1007/s00134-007-0934-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 201.Waterer GW, Kessler LA, Wunderink RG. Delayed administration of antibiotics and atypical presentation in community-acquired pneumonia. Chest. 2006;130:11–5. doi: 10.1378/chest.130.1.11. [DOI] [PubMed] [Google Scholar]
- 202.Yu KT, Wyer PC. Evidence-based emergency medicine/critically appraised topic. Evidence behind the 4-hour rule for initiation of antibiotic therapy in community-acquired pneumonia. Ann Emerg Med. 2008;51:651–62. doi: 10.1016/j.annemergmed.2007.10.022. 62 e1-2. [DOI] [PubMed] [Google Scholar]
- 203.Bruns AH, Oosterheert JJ, Hustinx WN, Gaillard CA, Hak E, Hoepelman AI. Time for first antibiotic dose is not predictive for the early clinical failure of moderate-severe community-acquired pneumonia. Eur J Clin Microbiol Infect Dis. 2009;28:913–9. doi: 10.1007/s10096-009-0724-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 204.Friedberg MW, Mehrotra A, Linder JA. Reporting hospitals’ antibiotic timing in pneumonia: Adverse consequences for patients? Am J Manag Care. 2009;15:137–44. [PMC free article] [PubMed] [Google Scholar]
- 205.Pines JM, Isserman JA, Hinfey PB. The measurement of time to first antibiotic dose for pneumonia in the emergency department: A white paper and position statement prepared for the American Academy of Emergency Medicine. J Emerg Med. 2009;37:335–40. doi: 10.1016/j.jemermed.2009.06.127. [DOI] [PubMed] [Google Scholar]
- 206.Athanassa Z, Makris G, Dimopoulos G, Falagas ME. Early switch to oral treatment in patients with moderate to severe community-acquired pneumonia: A meta-analysis. Drugs. 2008;68:2469–81. doi: 10.2165/0003495-200868170-00005. [DOI] [PubMed] [Google Scholar]
- 207.Dimopoulos G, Matthaiou DK, Karageorgopoulos DE, Grammatikos AP, Athanassa Z, Falagas ME. Short- versus long-course antibacterial therapy for community-acquired pneumonia: A meta-analysis. Drugs. 2008;68:1841–54. doi: 10.2165/00003495-200868130-00004. [DOI] [PubMed] [Google Scholar]
- 208.Capelastegui A, Espana PP, Quintana JM, Gallarreta M, Gorordo I, Esteban C, et al. Declining length of hospital stay for pneumonia and postdischarge outcomes. Am J Med. 2008;121:845–52. doi: 10.1016/j.amjmed.2008.05.010. [DOI] [PubMed] [Google Scholar]
- 209.Li JZ, Winston LG, Moore DH, Bent S. Efficacy of short-course antibiotic regimens for community-acquired pneumonia: A meta-analysis. Am J Med. 2007;120:783–90. doi: 10.1016/j.amjmed.2007.04.023. [DOI] [PubMed] [Google Scholar]
- 210.Kristoffersen KB, Sogaard OSs, Wejse C, Black FT, Greve T, Tarp B, et al. Antibiotic treatment interruption of suspected lower respiratory tract infections based on a single procalcitonin measurement at hospital admission–a randomized trial. Clin Microbiol Infect. 2009;15:481–7. doi: 10.1111/j.1469-0691.2009.02709.x. [DOI] [PubMed] [Google Scholar]
- 211.Schuetz P, Chiappa V, Briel M, Greenwald JL. Procalcitonin algorithms for antibiotic therapy decisions: A systematic review of randomized controlled trials and recommendations for clinical algorithms. Arch Intern Med. 2011;171:1322–31. doi: 10.1001/archinternmed.2011.318. [DOI] [PubMed] [Google Scholar]
- 212.Tang H, Huang T, Jing J, Shen H, Cui W. Effect of procalcitonin-guided treatment in patients with infections: A systematic review and meta-analysis. Infection. 2009;37:497–507. doi: 10.1007/s15010-009-9034-2. [DOI] [PubMed] [Google Scholar]
- 213.Garcia-Vidal C, Calbo E, Pascual V, Ferrer C, Quintana S, Garau J. Effects of systemic steroids in patients with severe community-acquired pneumonia. Eur Respir J. 2007;30:951–6. doi: 10.1183/09031936.00027607. [DOI] [PubMed] [Google Scholar]
- 214.Mikami K, Suzuki M, Kitagawa H, Kawakami M, Hirota N, Yamaguchi H, et al. Efficacy of corticosteroids in the treatment of community-acquired pneumonia requiring hospitalization. Lung. 2007;185:249–55. doi: 10.1007/s00408-007-9020-3. [DOI] [PubMed] [Google Scholar]
- 215.Siempos II, Vardakas KZ, Kopterides P, Falagas ME. Adjunctive therapies for community-acquired pneumonia: A systematic review. J Antimicrob Chemother. 2008;62:661–8. doi: 10.1093/jac/dkn283. [DOI] [PubMed] [Google Scholar]
- 216.Meijvis SC, Hardeman H, Remmelts HH, Heijligenberg R, Rijkers GT, van Velzen-Blad H, et al. Dexamethasone and length of hospital stay in patients with community-acquired pneumonia: A randomised, double-blind, placebo-controlled trial. Lancet. 2011;377:2023–30. doi: 10.1016/S0140-6736(11)60607-7. [DOI] [PubMed] [Google Scholar]
- 217.Gorman SK, Slavik RS, Marin J. Corticosteroid treatment of severe community-acquired pneumonia. Ann Pharmacother. 2007;41:1233–7. doi: 10.1345/aph.1H660. [DOI] [PubMed] [Google Scholar]
- 218.Salluh JI, Povoa P, Soares M, Castro-Faria-Neto HC, Bozza FA, Bozza PT. The role of corticosteroids in severe community-acquired pneumonia: A systematic review. Crit Care. 2008;12:R76. doi: 10.1186/cc6922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 219.Snijders D, Daniels JM, de Graaff CS, van der Werf TS, Boersma WG. Efficacy of corticosteroids in community-acquired pneumonia: A randomized double-blinded clinical trial. Am J Respir Crit Care Med. 2010;181:975–82. doi: 10.1164/rccm.200905-0808OC. [DOI] [PubMed] [Google Scholar]
- 220.Salluh JI, Soares M, Coelho LM, Bozza FA, Verdeal JC, Castro-Faria-Neto HC, et al. Impact of systemic corticosteroids on the clinical course and outcomes of patients with severe community-acquired pneumonia: A cohort study. J Crit Care. 2011;26:193–200. doi: 10.1016/j.jcrc.2010.07.014. [DOI] [PubMed] [Google Scholar]
- 221.Chen Y, Li K, Pu H, Wu T. Corticosteroids for pneumonia. Cochrane Database Syst Rev. 2011:CD007720. doi: 10.1002/14651858.CD007720.pub2. [DOI] [PubMed] [Google Scholar]
- 222.Marik PE, Pastores SM, Annane D, Meduri GU, Sprung CL, Arlt W, et al. Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: Consensus statements from an international task force by the American College of Critical Care Medicine. Crit Care Med. 2008;36:1937–49. doi: 10.1097/CCM.0b013e31817603ba. [DOI] [PubMed] [Google Scholar]
- 223.Annane D, Bellissant E, Bollaert PE, Briegel J, Confalonieri M, De Gaudio R, et al. Corticosteroids in the treatment of severe sepsis and septic shock in adults: A systematic review. JAMA. 2009;301:2362–75. doi: 10.1001/jama.2009.815. [DOI] [PubMed] [Google Scholar]
- 224.Lamontagne F, Briel M, Guyatt GH, Cook DJ, Bhatnagar N, Meade M. Corticosteroid therapy for acute lung injury, acute respiratory distress syndrome, and severe pneumonia: A meta-analysis of randomized controlled trials. J Crit Care. 2010;25:420–35. doi: 10.1016/j.jcrc.2009.08.009. [DOI] [PubMed] [Google Scholar]
- 225.Tang BM, Craig JC, Eslick GD, Seppelt I, McLean AS. Use of corticosteroids in acute lung injury and acute respiratory distress syndrome: A systematic review and meta-analysis. Crit Care Med. 2009;37:1594–603. doi: 10.1097/CCM.0b013e31819fb507. [DOI] [PubMed] [Google Scholar]
- 226.Agarwal R, Nath A, Aggarwal AN, Gupta D. Do glucocorticoids decrease mortality in acute respiratory distress syndrome? A meta-analysis. Respirology. 2007;12:585–90. doi: 10.1111/j.1440-1843.2007.01060.x. [DOI] [PubMed] [Google Scholar]
- 227.Cheng AC, Stephens DP, Currie BJ. Granulocyte-colony stimulating factor (G-CSF) as an adjunct to antibiotics in the treatment of pneumonia in adults. Cochrane Database Syst Rev. 2007:CD004400. doi: 10.1002/14651858.CD004400.pub3. [DOI] [PubMed] [Google Scholar]
- 228.Falagas ME, Makris GC, Matthaiou DK, Rafailidis PI. Statins for infection and sepsis: A systematic review of the clinical evidence. J Antimicrob Chemother. 2008;61:774–85. doi: 10.1093/jac/dkn019. [DOI] [PubMed] [Google Scholar]
- 229.Yang M, Yuping Y, Yin X, Wang BY, Wu T, Liu GJ, et al. Chest physiotherapy for pneumonia in adults. Cochrane Database Syst Rev. 2010:CD006338. doi: 10.1002/14651858.CD006338.pub2. [DOI] [PubMed] [Google Scholar]
- 230.Keenan SP, Sinuff T, Cook DJ, Hill NS. Does noninvasive positive pressure ventilation improve outcome in acute hypoxemic respiratory failure? A systematic review. Crit Care Med. 2004;32:2516–23. doi: 10.1097/01.ccm.0000148011.51681.e2. [DOI] [PubMed] [Google Scholar]
- 231.Keddissi JI, McCaffree DR. Acute respiratory distress syndrome. In: Jindal JI, Shankar PS, Raoof S, Gupta D, Aggarwal AN, Agarwal R, editors. Textbook of Pulmonary and Critical Care Medicine. New Delhi: Jaypee Publications; 2010. pp. 1618–30. [Google Scholar]
- 232.Agarwal R, Aggarwal AN, Gupta D. Role of noninvasive ventilation in acute lung injury/acute respiratory distress syndrome: A proportion meta-analysis. Respir Care. 2010;55:1653–60. [PubMed] [Google Scholar]
- 233.India EGotAoPoIoAIi. The Association of Physicians of India evidence-based clinical practice guidelines on adult immunization. J Assoc Physicians India. 2009;57:345–56. [PubMed] [Google Scholar]
- 234.Moberley SA, Holden J, Tatham DP, Andrews RM. Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst Rev. 2008:CD000422. doi: 10.1002/14651858.CD000422.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 235.Chang CC, Singleton RJ, Morris PS, Chang AB. Pneumococcal vaccines for children and adults with bronchiectasis. Cochrane Database Syst Rev. 2009:CD006316. doi: 10.1002/14651858.CD006316.pub2. [DOI] [PubMed] [Google Scholar]
- 236.Christenson B, Pauksen K, Sylvan SP. Effect of influenza and pneumococcal vaccines in elderly persons in years of low influenza activity. Virol J. 2008;5:52. doi: 10.1186/1743-422X-5-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 237.Huss A, Scott P, Stuck AE, Trotter C, Egger M. Efficacy of pneumococcal vaccination in adults: A meta-analysis. CMAJ. 2009;180:48–58. doi: 10.1503/cmaj.080734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 238.Johnstone J, Marrie TJ, Eurich DT, Majumdar SR. Effect of pneumococcal vaccination in hospitalized adults with community-acquired pneumonia. Arch Intern Med. 2007;167:1938–43. doi: 10.1001/archinte.167.18.1938. [DOI] [PubMed] [Google Scholar]
- 239.Lee TA, Weaver FM, Weiss KB. Impact of pneumococcal vaccination on pneumonia rates in patients with COPD and asthma. J Gen Intern Med. 2007;22:62–7. doi: 10.1007/s11606-007-0118-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 240.Musher DM, Rueda AM, Nahm MH, Graviss EA, Rodriguez-Barradas MC. Initial and subsequent response to pneumococcal polysaccharide and protein-conjugate vaccines administered sequentially to adults who have recovered from pneumococcal pneumonia. J Infect Dis. 2008;198:1019–27. doi: 10.1086/591629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 241.Ochoa-Gondar O, Vila-Corcoles A, Ansa X, Rodriguez-Blanco T, Salsench E, de Diego C, et al. Effectiveness of pneumococcal vaccination in older adults with chronic respiratory diseases: Results of the EVAN-65 study. Vaccine. 2008;26:1955–62. doi: 10.1016/j.vaccine.2008.02.021. [DOI] [PubMed] [Google Scholar]
- 242.Schembri S, Morant S, Winter JH, MacDonald TM. Influenza but not pneumococcal vaccination protects against all-cause mortality in patients with COPD. Thorax. 2009;64:567–72. doi: 10.1136/thx.2008.106286. [DOI] [PubMed] [Google Scholar]
- 243.Skull SA, Andrews RM, Byrnes GB, Kelly HA, Nolan TM, Brown GV, et al. Prevention of community-acquired pneumonia among a cohort of hospitalized elderly: Benefit due to influenza and pneumococcal vaccination not demonstrated. Vaccine. 2007;25:4631–40. doi: 10.1016/j.vaccine.2007.03.015. [DOI] [PubMed] [Google Scholar]
- 244.Spindler C, Hedlund J, Jasir A, Normark BH, Ortqvist A. Effects of a large-scale introduction of the pneumococcal polysaccharide vaccine among elderly persons in Stockholm, Sweden. Vaccine. 2008;26:5541–6. doi: 10.1016/j.vaccine.2008.06.073. [DOI] [PubMed] [Google Scholar]
- 245.Vila-Corcoles A, Salsench E, Rodriguez-Blanco T, Ochoa-Gondar O, de Diego C, Valdivieso A, et al. Clinical effectiveness of 23-valent pneumococcal polysaccharide vaccine against pneumonia in middle-aged and older adults: A matched case-control study. Vaccine. 2009;27:1504–10. doi: 10.1016/j.vaccine.2009.01.013. [DOI] [PubMed] [Google Scholar]
- 246.Osterholm MT, Kelley NS, Sommer A, Belongia EA. Efficacy and effectiveness of influenza vaccines: A systematic review and meta-analysis. Lancet Infect Dis. 2012;12:36–44. doi: 10.1016/S1473-3099(11)70295-X. [DOI] [PubMed] [Google Scholar]
- 247.Jefferson T, Di Pietrantonj C, Al-Ansary LA, Ferroni E, Thorning S, Thomas RE. Vaccines for preventing influenza in the elderly. Cochrane Database Syst Rev. 2010:CD004876. doi: 10.1002/14651858.CD004876.pub3. [DOI] [PubMed] [Google Scholar]
- 248.Jefferson TO, Rivetti D, Di Pietrantonj C, Rivetti A, Demicheli V. Vaccines for preventing influenza in healthy adults. Cochrane Database Syst Rev. 2007:CD001269. doi: 10.1002/14651858.CD001269.pub3. [DOI] [PubMed] [Google Scholar]
- 249.Jackson ML, Nelson JC, Weiss NS, Neuzil KM, Barlow W, Jackson LA. Influenza vaccination and risk of community-acquired pneumonia in immunocompetent elderly people: A population-based, nested case-control study. Lancet. 2008;372:398–405. doi: 10.1016/S0140-6736(08)61160-5. [DOI] [PubMed] [Google Scholar]
- 250.Campitelli MA, Rosella LC, Stukel TA, Kwong JC. Influenza vaccination and all-cause mortality in community-dwelling elderly in Ontario, Canada, a cohort study. Vaccine. 2010;29:240–6. doi: 10.1016/j.vaccine.2010.10.049. [DOI] [PubMed] [Google Scholar]
- 251.Tablan OC, Anderson LJ, Besser R, Bridges C, Hajjeh R. Guidelines for preventing health-care--associated pneumonia, 2003: Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR Recomm Rep. 2004;53:1–36. [PubMed] [Google Scholar]
- 252.Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416. doi: 10.1164/rccm.200405-644ST. [DOI] [PubMed] [Google Scholar]
- 253.Rotstein C, Evans G, Born A, Grossman R, Light RB, Magder S, et al. Clinical practice guidelines for hospital-acquired pneumonia and ventilator-associated pneumonia in adults. Can J Infect Dis Med Microbiol. 2008;19:19–53. doi: 10.1155/2008/593289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 254.Falcone M, Venditti M, Shindo Y, Kollef MH. Healthcare-associated pneumonia: Diagnostic criteria and distinction from community-acquired pneumonia. Int J Infect Dis. 2011;15:e545–50. doi: 10.1016/j.ijid.2011.04.005. [DOI] [PubMed] [Google Scholar]
- 255.Ewig S, Welte T, Chastre J, Torres A. Rethinking the concepts of community-acquired and health-care-associated pneumonia. Lancet Infect Dis. 2010;10:279–87. doi: 10.1016/S1473-3099(10)70032-3. [DOI] [PubMed] [Google Scholar]
- 256.Nosocomial infection rates for interhospital comparison: Limitations and possible solutions. A Report from the National Nosocomial Infections Surveillance (NNIS) System. Infect Control Hosp Epidemiol. 1991;12:609–21. [PubMed] [Google Scholar]
- 257.Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165:867–903. doi: 10.1164/ajrccm.165.7.2105078. [DOI] [PubMed] [Google Scholar]
- 258.Torres A, Aznar R, Gatell JM, Jimenez P, Gonzalez J, Ferrer A, et al. Incidence, risk, and prognosis factors of nosocomial pneumonia in mechanically ventilated patients. Am Rev Respir Dis. 1990;142:523–8. doi: 10.1164/ajrccm/142.3.523. [DOI] [PubMed] [Google Scholar]
- 259.Celis R, Torres A, Gatell JM, Almela M, Rodriguez-Roisin R, Agusti-Vidal A. Nosocomial pneumonia. A multivariate analysis of risk and prognosis. Chest. 1988;93:318–24. doi: 10.1378/chest.93.2.318. [DOI] [PubMed] [Google Scholar]
- 260.Venditti M FM, Corrao S Study Group of the Italian Society of Internal Medicine. Outcomes of patients hospitalized with community-acquired, health care-associated, and hospital-acquired pneumonia. Ann Intern Med. 2009;150:19–26. doi: 10.7326/0003-4819-150-1-200901060-00005. [DOI] [PubMed] [Google Scholar]
- 261.Jones RN. Microbial etiologies of hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia. Clin Infect Dis. 2010;51(Suppl 1):S81–7. doi: 10.1086/653053. [DOI] [PubMed] [Google Scholar]
- 262.Cook D, Mandell L. Endotracheal aspiration in the diagnosis of ventilator-associated pneumonia. Chest. 2000;117:195S–7S. doi: 10.1378/chest.117.4_suppl_2.195s. [DOI] [PubMed] [Google Scholar]
- 263.Cook DJ, Walter SD, Cook RJ, Griffith LE, Guyatt GH, Leasa D, et al. Incidence of and risk factors for ventilator-associated pneumonia in critically ill patients. Ann Intern Med. 1998;129:433–40. doi: 10.7326/0003-4819-129-6-199809150-00002. [DOI] [PubMed] [Google Scholar]
- 264.Nourdine K, Combes P, Carton MJ, Beuret P, Cannamela A, Ducreux JC. Does noninvasive ventilation reduce the ICU nosocomial infection risk? A prospective clinical survey. Intensive Care Med. 1999;25:567–73. doi: 10.1007/s001340050904. [DOI] [PubMed] [Google Scholar]
- 265.Ibrahim EH, Ward S, Sherman G, Kollef MH. A comparative analysis of patients with early-onset vs late-onset nosocomial pneumonia in the ICU setting. Chest. 2000;117:1434–42. doi: 10.1378/chest.117.5.1434. [DOI] [PubMed] [Google Scholar]
- 266.Napolitano LM. Use of severity scoring and stratification factors in clinical trials of hospital-acquired and ventilator-associated pneumonia. Clin Infect Dis. 2010;51(Suppl 1):S67–80. doi: 10.1086/653052. [DOI] [PubMed] [Google Scholar]
- 267.Mukhopadhyay C, Bhargava A, Ayyagari A. Role of mechanical ventilation & development of multidrug resistant organisms in hospital acquired pneumonia. Indian J Med Res. 2003;118:229–35. [PubMed] [Google Scholar]
- 268.Rakshit P, Nagar VS, Deshpande AK. Incidence, clinical outcome,and risk stratification of ventilator associated pneumonia- a prospective cohort study. Indian J Crit Care Med. 2005;9:211–6. [Google Scholar]
- 269.Singhal R, Mohanty S, Sood S, Das B, Kapil A. Profile of bacterial isolates from patients with ventilator associated pneumonias in a tertiary care hospital in India. Indian J Med Res. 2005;121:63–4. [PubMed] [Google Scholar]
- 270.Agarwal R, Gupta D, Ray P, Aggarwal AN, Jindal SK. Epidemiology, risk factors and outcome of nosocomial infections in a Respiratory Intensive Care Unit in North India. J Infect. 2006;53:98–105. doi: 10.1016/j.jinf.2005.10.021. [DOI] [PubMed] [Google Scholar]
- 271.Prakash S RA, Gogia AR, Prakash S. Nosocomial pneumonia in mechanically ventilated patients receiving ranitidine or sucralfate as stress ulcer prophylaxis. Indian J Anaesth. 2008;52:179–84. [Google Scholar]
- 272.Joseph NM, Sistla S, Dutta TK, Badhe AS, Rasitha D, Parija SC. Ventilator-associated pneumonia in a tertiary care hospital in India: Role of multi-drug resistant pathogens. J Infect Dev Ctries. 2010;4:218–25. doi: 10.3855/jidc.634. [DOI] [PubMed] [Google Scholar]
- 273.Bajpai S KD. De-escalation of antibiotics in nosocomial pneumonia in an Indian intensive care unit. Int J Med Med Sci. 2010;2:148–52. [Google Scholar]
- 274.Chawla R. Epidemiology, etiology, and diagnosis of hospital-acquired pneumonia and ventilator-associated pneumonia in Asian countries. Am J Infect Control. 2008;36:S93–100. doi: 10.1016/j.ajic.2007.05.011. [DOI] [PubMed] [Google Scholar]
- 275.Babcock HM, Zack JE, Garrison T, Trovillion E, Kollef MH, Fraser VJ. Ventilator-associated pneumonia in a multi-hospital system: Differences in microbiology by location. Infect Control Hosp Epidemiol. 2003;24:853–8. doi: 10.1086/502149. [DOI] [PubMed] [Google Scholar]
- 276.Fagon JY, Chastre J, Hance AJ, Domart Y, Trouillet JL, Gibert C. Evaluation of clinical judgment in the identification and treatment of nosocomial pneumonia in ventilated patients. Chest. 1993;103:547–53. doi: 10.1378/chest.103.2.547. [DOI] [PubMed] [Google Scholar]
- 277.Klompas M, Kleinman K, Khan Y, Evans RS, Lloyd JF, Stevenson K, et al. Rapid and reproducible surveillance for ventilator-associated pneumonia. Clin Infect Dis. 2012;54:370–7. doi: 10.1093/cid/cir832. [DOI] [PubMed] [Google Scholar]
- 278.Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309–32. doi: 10.1016/j.ajic.2008.03.002. [DOI] [PubMed] [Google Scholar]
- 279.Kirtland SH, Corley DE, Winterbauer RH, Springmeyer SC, Casey KR, Hampson NB, et al. The diagnosis of ventilator-associated pneumonia: A comparison of histologic, microbiologic, and clinical criteria. Chest. 1997;112:445–57. doi: 10.1378/chest.112.2.445. [DOI] [PubMed] [Google Scholar]
- 280.Fagon JY, Chastre J, Wolff M, Gervais C, Parer-Aubas S, Stephan F, et al. Invasive and noninvasive strategies for management of suspected ventilator-associated pneumonia. A randomized trial. Ann Intern Med. 2000;132:621–30. doi: 10.7326/0003-4819-132-8-200004180-00004. [DOI] [PubMed] [Google Scholar]
- 281.Fartoukh M, Maitre B, Honore S, Cerf C, Zahar JR, Brun-Buisson C. Diagnosing pneumonia during mechanical ventilation: The clinical pulmonary infection score revisited. Am J Respir Crit Care Med. 2003;168:173–9. doi: 10.1164/rccm.200212-1449OC. [DOI] [PubMed] [Google Scholar]
- 282.Pugin J, Auckenthaler R, Mili N, Janssens JP, Lew PD, Suter PM. Diagnosis of ventilator-associated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic “blind” bronchoalveolar lavage fluid. Am Rev Respir Dis. 1991;143:1121–9. doi: 10.1164/ajrccm/143.5_Pt_1.1121. [DOI] [PubMed] [Google Scholar]
- 283.Fabregas N, Ewig S, Torres A, El-Ebiary M, Ramirez J, de La Bellacasa JP, et al. Clinical diagnosis of ventilator associated pneumonia revisited: Comparative validation using immediate post-mortem lung biopsies. Thorax. 1999;54:867–73. doi: 10.1136/thx.54.10.867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 284.Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000;162:505–11. doi: 10.1164/ajrccm.162.2.9909095. [DOI] [PubMed] [Google Scholar]
- 285.Schurink CA, Van Nieuwenhoven CA, Jacobs JA, Rozenberg-Arska M, Joore HC, Buskens E, et al. Clinical pulmonary infection score for ventilator-associated pneumonia: Accuracy and inter-observer variability. Intensive Care Med. 2004;30:217–24. doi: 10.1007/s00134-003-2018-2. [DOI] [PubMed] [Google Scholar]
- 286.Flanagan PG, Findlay GP, Magee JT, Ionescu A, Barnes RA, Smithies M. The diagnosis of ventilator-associated pneumonia using non-bronchoscopic, non-directed lung lavages. Intensive Care Med. 2000;26:20–30. doi: 10.1007/s001340050007. [DOI] [PubMed] [Google Scholar]
- 287.Shan J, Chen HL, Zhu JH. Diagnostic accuracy of clinical pulmonary infection score for ventilator-associated pneumonia: A meta-analysis. Respir Care. 2011;56:1087–94. doi: 10.4187/respcare.01097. [DOI] [PubMed] [Google Scholar]
- 288.Luna CM, Blanzaco D, Niederman MS, Matarucco W, Baredes NC, Desmery P, et al. Resolution of ventilator-associated pneumonia: Prospective evaluation of the clinical pulmonary infection score as an early clinical predictor of outcome. Crit Care Med. 2003;31:676–82. doi: 10.1097/01.CCM.0000055380.86458.1E. [DOI] [PubMed] [Google Scholar]
- 289.Baker AM, Bowton DL, Haponik EF. Decision making in nosocomial pneumonia. An analytic approach to the interpretation of quantitative bronchoscopic cultures. Chest. 1995;107:85–95. doi: 10.1378/chest.107.1.85. [DOI] [PubMed] [Google Scholar]
- 290.Chastre J, Wolff M, Fagon JY, Chevret S, Thomas F, Wermert D, et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: A randomized trial. JAMA. 2003;290:2588–98. doi: 10.1001/jama.290.19.2588. [DOI] [PubMed] [Google Scholar]
- 291.Heyland DK, Cook DJ, Marshall J, Heule M, Guslits B, Lang J, et al. The clinical utility of invasive diagnostic techniques in the setting of ventilator-associated pneumonia. Canadian Critical Care Trials Group. Chest. 1999;115:1076–84. doi: 10.1378/chest.115.4.1076. [DOI] [PubMed] [Google Scholar]
- 292.Rajasekhar T, Anuradha K, Suhasini T, Lakshmi V. The role of quantitative cultures of non-bronchoscopic samples in ventilator associated pneumonia. Indian J Med Microbiol. 2006;24:107–13. doi: 10.4103/0255-0857.25226. [DOI] [PubMed] [Google Scholar]
- 293.Aucar JA, Bongera M, Phillips JO, Kamath R, Metzler MH. Quantitative tracheal lavage versus bronchoscopic protected specimen brush for the diagnosis of nosocomial pneumonia in mechanically ventilated patients. Am J Surg. 2003;186:591–6. doi: 10.1016/j.amjsurg.2003.08.005. [DOI] [PubMed] [Google Scholar]
- 294.Woske HJ, Roding T, Schulz I, Lode H. Ventilator-associated pneumonia in a surgical intensive care unit: Epidemiology, etiology and comparison of three bronchoscopic methods for microbiological specimen sampling. Crit Care. 2001;5:167–73. doi: 10.1186/cc1017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 295.Wu CL, Yang D, Wang NY, Kuo HT, Chen PZ. Quantitative culture of endotracheal aspirates in the diagnosis of ventilator-associated pneumonia in patients with treatment failure. Chest. 2002;122:662–8. doi: 10.1378/chest.122.2.662. [DOI] [PubMed] [Google Scholar]
- 296.Torres A, El-Ebiary M. Bronchoscopic BAL in the diagnosis of ventilator-associated pneumonia. Chest. 2000;117:198S–202S. doi: 10.1378/chest.117.4_suppl_2.198s. [DOI] [PubMed] [Google Scholar]
- 297.Khilnani GC, Arafath TK, Hadda V, Kapil A, Sood S, Sharma SK. Comparison of bronchoscopic and non-bronchoscopic techniques for diagnosis of ventilator associated pneumonia. Indian J Crit Care Med. 2011;15:16–23. doi: 10.4103/0972-5229.78218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 298.Baram D, Hulse G, Palmer LB. Stable patients receiving prolonged mechanical ventilation have a high alveolar burden of bacteria. Chest. 2005;127:1353–7. doi: 10.1378/chest.127.4.1353. [DOI] [PubMed] [Google Scholar]
- 299.Malhotra AK, Riaz OJ, Duane TM, Aboutanos MB, Goldberg AE, Smalara KM, et al. Subthreshold quantitative bronchoalveolar lavage: Clinical and therapeutic implications. J Trauma. 2008;65:580–8. doi: 10.1097/TA.0b013e3181825b9f. [DOI] [PubMed] [Google Scholar]
- 300.A randomized trial of diagnostic techniques for ventilator-associated pneumonia. N Engl J Med. 2006;355:2619–30. doi: 10.1056/NEJMoa052904. [DOI] [PubMed] [Google Scholar]
- 301.Sole Violan J, Fernandez JA, Benitez AB, Cardenosa Cendrero JA, de Castro F Rodriguez. Impact of quantitative invasive diagnostic techniques in the management and outcome of mechanically ventilated patients with suspected pneumonia. Crit Care Med. 2000;28:2737–41. doi: 10.1097/00003246-200008000-00009. [DOI] [PubMed] [Google Scholar]
- 302.Berton DC, Kalil AC, Teixeira PJ. Quantitative versus qualitative cultures of respiratory secretions for clinical outcomes in patients with ventilator-associated pneumonia. Cochrane Database Syst Rev. 2012;1:CD006482. doi: 10.1002/14651858.CD006482.pub3. [DOI] [PubMed] [Google Scholar]
- 303.Ruiz M, Torres A, Ewig S, Marcos MA, Alcon A, Lledo R, et al. Noninvasive versus invasive microbial investigation in ventilator-associated pneumonia: Evaluation of outcome. Am J Respir Crit Care Med. 2000;162:119–25. doi: 10.1164/ajrccm.162.1.9907090. [DOI] [PubMed] [Google Scholar]
- 304.Gibot S, Kolopp-Sarda MN, Bene MC, Bollaert PE, Lozniewski A, Mory F, et al. A soluble form of the triggering receptor expressed on myeloid cells-1 modulates the inflammatory response in murine sepsis. J Exp Med. 2004;200:1419–26. doi: 10.1084/jem.20040708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 305.Anand NJ, Zuick S, Klesney-Tait J, Kollef MH. Diagnostic implications of soluble triggering receptor expressed on myeloid cells-1 in BAL fluid of patients with pulmonary infiltrates in the ICU. Chest. 2009;135:641–7. doi: 10.1378/chest.08-1829. [DOI] [PubMed] [Google Scholar]
- 306.Oudhuis GJ, Beuving J, Bergmans D, Stobberingh EE, ten Velde G, Linssen CF, et al. Soluble Triggering Receptor Expressed on Myeloid cells-1 in bronchoalveolar lavage fluid is not predictive for ventilator-associated pneumonia. Intensive Care Med. 2009;35:1265–70. doi: 10.1007/s00134-009-1463-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 307.Horonenko G, Hoyt JC, Robbins RA, Singarajah CU, Umar A, Pattengill J, et al. Soluble triggering receptor expressed on myeloid cell-1 is increased in patients with ventilator-associated pneumonia: A preliminary report. Chest. 2007;132:58–63. doi: 10.1378/chest.06-2731. [DOI] [PubMed] [Google Scholar]
- 308.Duflo F, Debon R, Monneret G, Bienvenu J, Chassard D, Allaouchiche B. Alveolar and serum procalcitonin: Diagnostic and prognostic value in ventilator-associated pneumonia. Anesthesiology. 2002;96:74–9. doi: 10.1097/00000542-200201000-00018. [DOI] [PubMed] [Google Scholar]
- 309.Determann RM, Millo JL, Gibot S, Korevaar JC, Vroom MB, van der Poll T, et al. Serial changes in soluble triggering receptor expressed on myeloid cells in the lung during development of ventilator-associated pneumonia. Intensive Care Med. 2005;31:1495–500. doi: 10.1007/s00134-005-2818-7. [DOI] [PubMed] [Google Scholar]
- 310.Schuetz P, Christ-Crain M, Thomann R, Falconnier C, Wolbers M, Widmer I, et al. Effect of procalcitonin-based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: The ProHOSP randomized controlled trial. JAMA. 2009;302:1059–66. doi: 10.1001/jama.2009.1297. [DOI] [PubMed] [Google Scholar]
- 311.Bouadma L, Luyt CE, Tubach F, Cracco C, Alvarez A, Schwebel C, et al. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): A multicentre randomised controlled trial. Lancet. 2010;375:463–74. doi: 10.1016/S0140-6736(09)61879-1. [DOI] [PubMed] [Google Scholar]
- 312.Povoa P. Serum markers in community-acquired pneumonia and ventilator-associated pneumonia. Curr Opin Infect Dis. 2008;21:157–62. doi: 10.1097/QCO.0b013e3282f47c32. [DOI] [PubMed] [Google Scholar]
- 313.Oppert M, Reinicke A, Muller C, Barckow D, Frei U, Eckardt KU. Elevations in procalcitonin but not C-reactive protein are associated with pneumonia after cardiopulmonary resuscitation. Resuscitation. 2002;53:167–70. doi: 10.1016/s0300-9572(02)00008-4. [DOI] [PubMed] [Google Scholar]
- 314.Holm A, Pedersen SS, Nexoe J, Obel N, Nielsen LP, Koldkjaer O, et al. Procalcitonin versus C-reactive protein for predicting pneumonia in adults with lower respiratory tract infection in primary care. Br J Gen Pract. 2007;57:555–60. [PMC free article] [PubMed] [Google Scholar]
- 315.Craven DE. Ventilator-associated tracheobronchitis (VAT): Questions, answers, and a new paradigm? Crit Care. 2008;12:157. doi: 10.1186/cc6912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 316.Nseir S, Di Pompeo C, Pronnier P, Beague S, Onimus T, Saulnier F, et al. Nosocomial tracheobronchitis in mechanically ventilated patients: Incidence, aetiology and outcome. Eur Respir J. 2002;20:1483–9. doi: 10.1183/09031936.02.00012902. [DOI] [PubMed] [Google Scholar]
- 317.Kuti EL, Patel AA, Coleman CI. Impact of inappropriate antibiotic therapy on mortality in patients with ventilator-associated pneumonia and blood stream infection: A meta-analysis. J Crit Care. 2008;23:91–100. doi: 10.1016/j.jcrc.2007.08.007. [DOI] [PubMed] [Google Scholar]
- 318.Ulldemolins M, Nuvials X, Palomar M, Masclans JR, Rello J. Appropriateness is critical. Crit Care Clin. 2011;27:35–51. doi: 10.1016/j.ccc.2010.09.007. [DOI] [PubMed] [Google Scholar]
- 319.Kollef KE, Schramm GE, Wills AR, Reichley RM, Micek ST, Kollef MH. Predictors of 30-day mortality and hospital costs in patients with ventilator-associated pneumonia attributed to potentially antibiotic-resistant gram-negative bacteria. Chest. 2008;134:281–7. doi: 10.1378/chest.08-1116. [DOI] [PubMed] [Google Scholar]
- 320.Zilberberg MD, Shorr AF, Micek ST, Mody SH, Kollef MH. Antimicrobial therapy escalation and hospital mortality among patients with health-care-associated pneumonia: A single-center experience. Chest. 2008;134:963–8. doi: 10.1378/chest.08-0842. [DOI] [PubMed] [Google Scholar]
- 321.Miller PR, Partrick MS, Hoth JJ, Meredith JW, Chang MC. A practical application of practice-based learning: Development of an algorithm for empiric antibiotic coverage in ventilator-associated pneumonia. J Trauma. 2006;60:725–9. doi: 10.1097/01.ta.0000214650.92501.76. discussion 9-31. [DOI] [PubMed] [Google Scholar]
- 322.Michel F, Franceschini B, Berger P, Arnal JM, Gainnier M, Sainty JM, et al. Early antibiotic treatment for BAL-confirmed ventilator-associated pneumonia: A role for routine endotracheal aspirate cultures. Chest. 2005;127:589–97. doi: 10.1378/chest.127.2.589. [DOI] [PubMed] [Google Scholar]
- 323.Dennesen PJ, van der Ven AJ, Kessels AG, Ramsay G, Bonten MJ. Resolution of infectious parameters after antimicrobial therapy in patients with ventilator-associated pneumonia. Am J Respir Crit Care Med. 2001;163:1371–5. doi: 10.1164/ajrccm.163.6.2007020. [DOI] [PubMed] [Google Scholar]
- 324.Hayon J, Figliolini C, Combes A, Trouillet JL, Kassis N, Dombret MC, et al. Role of serial routine microbiologic culture results in the initial management of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165:41–6. doi: 10.1164/ajrccm.165.1.2105077. [DOI] [PubMed] [Google Scholar]
- 325.American Thoracic S, Infectious Diseases Society of A. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416. doi: 10.1164/rccm.200405-644ST. [DOI] [PubMed] [Google Scholar]
- 326.Masterton RG, Galloway A, French G, Street M, Armstrong J, Brown E, et al. Guidelines for the management of hospital-acquired pneumonia in the UK: Report of the working party on hospital-acquired pneumonia of the British Society for Antimicrobial Chemotherapy. J Antimicrob Chemother. 2008;62:5–34. doi: 10.1093/jac/dkn162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 327.Froes F, Paiva JA, Amaro P, Baptista JP, Brum G, Bento H, et al. Consensus document on nosocomial pneumonia. Rev Port Pneumol. 2007;13:419–86. [PubMed] [Google Scholar]
- 328.Brink A, Feldman C, Duse A, Gopalan D, Grolman D, Mer M, et al. Guideline for the management of nosocomial infections in South Africa. S Afr Med J. 2006;96:642–52. [PubMed] [Google Scholar]
- 329.Luna CM, Monteverde A, Rodriguez A, Apezteguia C, Zabert G, Ilutovich S, et al. Clinical guidelines for the treatment of nosocomial pneumonia in Latin America: An interdisciplinary consensus document. Recommendations of the Latin American Thoracic Society. Arch Bronconeumol. 2005;41:439–56. doi: 10.1016/s1579-2129(06)60260-7. [DOI] [PubMed] [Google Scholar]
- 330.Sociedade Brasileira de Pneumologia e T. Brazilian guidelines for treatment of hospital acquired pneumonia and ventilator associated pneumonia- 2007. J Bras Pneumol. 2007;33(Suppl 1):S1–30. [PubMed] [Google Scholar]
- 331.[(The JRS Guideline for the management of hospital-acquired pneumonia in adults)] Nihon Naika Gakkai Zasshi. 2008;97:2578–83. [PubMed] [Google Scholar]
- 332.Aarts MA, Hancock JN, Heyland D, McLeod RS, Marshall JC. Empiric antibiotic therapy for suspected ventilator-associated pneumonia: A systematic review and meta-analysis of randomized trials. Crit Care Med. 2008;36:108–17. doi: 10.1097/01.CCM.0000297956.27474.9D. [DOI] [PubMed] [Google Scholar]
- 333.Safdar N, Handelsman J, Maki DG. Does combination antimicrobial therapy reduce mortality in Gram-negative bacteraemia? A meta-analysis. Lancet Infect Dis. 2004;4:519–27. doi: 10.1016/S1473-3099(04)01108-9. [DOI] [PubMed] [Google Scholar]
- 334.Paul M, Silbiger I, Grozinsky S, Soares-Weiser K, Leibovici L. Beta lactam antibiotic monotherapy versus beta lactam-aminoglycoside antibiotic combination therapy for sepsis. Cochrane Database Syst Rev. 2006:CD003344. doi: 10.1002/14651858.CD003344.pub2. [DOI] [PubMed] [Google Scholar]
- 335.Heyland DK, Dodek P, Muscedere J, Day A, Cook D Canadian Critical Care Trials G. Randomized trial of combination versus monotherapy for the empiric treatment of suspected ventilator-associated pneumonia. Crit Care Med. 2008;36:737–44. doi: 10.1097/01.CCM.0B013E31816203D6. [DOI] [PubMed] [Google Scholar]
- 336.Mortensen EM, Restrepo MI, Anzueto A, Pugh J. The impact of empiric antimicrobial therapy with a beta-lactam and fluoroquinolone on mortality for patients hospitalized with severe pneumonia. Crit Care. 2005;10:R8. doi: 10.1186/cc3934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 337.Kett DH, Cano E, Quartin AA, Mangino JE, Zervos MJ, Peyrani P, et al. Implementation of guidelines for management of possible multidrug-resistant pneumonia in intensive care: An observational, multicentre cohort study. Lancet Infect Dis. 2011;11:181–9. doi: 10.1016/S1473-3099(10)70314-5. [DOI] [PubMed] [Google Scholar]
- 338.Davey PG, Marwick C. Appropriate vs.inappropriate antimicrobial therapy. Clin Microbiol Infect. 2008;14(Suppl 3):15–21. doi: 10.1111/j.1469-0691.2008.01959.x. [DOI] [PubMed] [Google Scholar]
- 339.Luna CM, Aruj P, Niederman MS, Garzon J, Violi D, Prignoni A, et al. Appropriateness and delay to initiate therapy in ventilator-associated pneumonia. Eur Respir J. 2006;27:158–64. doi: 10.1183/09031936.06.00049105. [DOI] [PubMed] [Google Scholar]
- 340.Ramphal R. Importance of adequate initial antimicrobial therapy. Chemotherapy. 2005;51:171–6. doi: 10.1159/000086574. [DOI] [PubMed] [Google Scholar]
- 341.Kollef MH. Appropriate empiric antimicrobial therapy of nosocomial pneumonia: The role of the carbapenems. Respir Care. 2004;49:1530–41. [PubMed] [Google Scholar]
- 342.Sandiumenge A, Diaz E, Bodi M, Rello J. Therapy of ventilator-associated pneumonia. A patient-based approach based on the ten rules of “The Tarragona Strategy”. Intensive Care Med. 2003;29:876–83. doi: 10.1007/s00134-003-1715-1. [DOI] [PubMed] [Google Scholar]
- 343.Mathevon T, Souweine B, Traore O, Aublet B, Caillaud D. ICU-acquired nosocomial infection: Impact of delay of adequate antibiotic treatment. Scand J Infect Dis. 2002;34:831–5. doi: 10.1080/0036554021000026934. [DOI] [PubMed] [Google Scholar]
- 344.Iregui M, Ward S, Sherman G, Fraser VJ, Kollef MH. Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator-associated pneumonia. Chest. 2002;122:262–8. doi: 10.1378/chest.122.1.262. [DOI] [PubMed] [Google Scholar]
- 345.Kollef MH, Ward S. The influence of mini-BAL cultures on patient outcomes: Implications for the antibiotic management of ventilator-associated pneumonia. Chest. 1998;113:412–20. doi: 10.1378/chest.113.2.412. [DOI] [PubMed] [Google Scholar]
- 346.Luna CM, Vujacich P, Niederman MS, Vay C, Gherardi C, Matera J, et al. Impact of BAL data on the therapy and outcome of ventilator-associated pneumonia. Chest. 1997;111:676–85. doi: 10.1378/chest.111.3.676. [DOI] [PubMed] [Google Scholar]
- 347.Muscedere JG, Shorr AF, Jiang X, Day A, Heyland DK. The adequacy of timely empiric antibiotic therapy for ventilator-associated pneumonia: An important determinant of outcome. J Crit Care. 2012;27:322.e7–14. doi: 10.1016/j.jcrc.2011.09.004. Epub 2011 Dec 1. [DOI] [PubMed] [Google Scholar]
- 348.Falagas ME, Rafailidis PI, Kasiakou SK, Hatzopoulou P, Michalopoulos A. Effectiveness and nephrotoxicity of colistin monotherapy vs.colistin-meropenem combination therapy for multidrug-resistant Gram-negative bacterial infections. Clin Microbiol Infect. 2006;12:1227–30. doi: 10.1111/j.1469-0691.2006.01559.x. [DOI] [PubMed] [Google Scholar]
- 349.Niederman MS, Soulountsi V. De-escalation therapy: Is it valuable for the management of ventilator-associated pneumonia? Clin Chest Med. 2011;32:517–34. doi: 10.1016/j.ccm.2011.05.009. [DOI] [PubMed] [Google Scholar]
- 350.Masterton RG. Antibiotic de-escalation. Crit Care Clin. 2011;27:149–62. doi: 10.1016/j.ccc.2010.09.009. [DOI] [PubMed] [Google Scholar]
- 351.Rello J, Vidaur L, Sandiumenge A, Rodriguez A, Gualis B, Boque C, et al. De-escalation therapy in ventilator-associated pneumonia. Crit Care Med. 2004;32:2183–90. doi: 10.1097/01.ccm.0000145997.10438.28. [DOI] [PubMed] [Google Scholar]
- 352.Micek ST, Ward S, Fraser VJ, Kollef MH. A randomized controlled trial of an antibiotic discontinuation policy for clinically suspected ventilator-associated pneumonia. Chest. 2004;125:1791–9. doi: 10.1378/chest.125.5.1791. [DOI] [PubMed] [Google Scholar]
- 353.Kollef MH, Kollef KE. Antibiotic utilization and outcomes for patients with clinically suspected ventilator-associated pneumonia and negative quantitative BAL culture results. Chest. 2005;128:2706–13. doi: 10.1378/chest.128.4.2706. [DOI] [PubMed] [Google Scholar]
- 354.Kollef MH, Morrow LE, Niederman MS, Leeper KV, Anzueto A, Benz-Scott L, et al. Clinical characteristics and treatment patterns among patients with ventilator-associated pneumonia. Chest. 2006;129:1210–8. doi: 10.1378/chest.129.5.1210. [DOI] [PubMed] [Google Scholar]
- 355.Alvarez-Lerma F, Alvarez B, Luque P, Ruiz F, Dominguez-Roldan JM, Quintana E, et al. Empiric broad-spectrum antibiotic therapy of nosocomial pneumonia in the intensive care unit: A prospective observational study. Crit Care. 2006;10:R78. doi: 10.1186/cc4919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 356.Leone M, Garcin F, Bouvenot J, Boyadjev I, Visintini P, Albanese J, et al. Ventilator-associated pneumonia: Breaking the vicious circle of antibiotic overuse. Crit Care Med. 2007;35:379–85. doi: 10.1097/01.CCM.0000253404.69418.AA. quizz 86. [DOI] [PubMed] [Google Scholar]
- 357.Giantsou E, Liratzopoulos N, Efraimidou E, Panopoulou M, Alepopoulou E, Kartali-Ktenidou S, et al. De-escalation therapy rates are significantly higher by bronchoalveolar lavage than by tracheal aspirate. Intensive Care Med. 2007;33:1533–40. doi: 10.1007/s00134-007-0619-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 358.Eachempati SR, Hydo LJ, Shou J, Barie PS. Does de-escalation of antibiotic therapy for ventilator-associated pneumonia affect the likelihood of recurrent pneumonia or mortality in critically ill surgical patients? J Trauma. 2009;66:1343–8. doi: 10.1097/TA.0b013e31819dca4e. [DOI] [PubMed] [Google Scholar]
- 359.Amsden GW. Interrelationship of pharmacokinetics/pharmacodynamics: Antibiotic dosing for the future. Eur Respir Mon. 2004;28:1–12. [Google Scholar]
- 360.Lodise TP, Drusano GL. Pharmacokinetics and pharmacodynamics: Optimal antimicrobial therapy in the intensive care unit. Crit Care Clin. 2011;27:1–18. doi: 10.1016/j.ccc.2010.11.003. [DOI] [PubMed] [Google Scholar]
- 361.Lodise TP, Jr, Lomaestro B, Drusano GL. Piperacillin-tazobactam for Pseudomonas aeruginosa infection: Clinical implications of an extended-infusion dosing strategy. Clin Infect Dis. 2007;44:357–63. doi: 10.1086/510590. [DOI] [PubMed] [Google Scholar]
- 362.Lorente L, Jimenez A, Palmero S, Jimenez JJ, Iribarren JL, Santana M, et al. Comparison of clinical cure rates in adults with ventilator-associated pneumonia treated with intravenous ceftazidime administered by continuous or intermittent infusion: A retrospective, nonrandomized, open-label, historical chart review. Clin Ther. 2007;29:2433–9. doi: 10.1016/j.clinthera.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 363.Georges B, Conil JM, Cougot P, Decun JF, Archambaud M, Seguin T, et al. Cefepime in critically ill patients: Continuous infusion vs.an intermittent dosing regimen. Int J Clin Pharmacol Ther. 2005;43:360–9. doi: 10.5414/cpp43360. [DOI] [PubMed] [Google Scholar]
- 364.Roberts JA, Boots R, Rickard CM, Thomas P, Quinn J, Roberts DM, et al. Is continuous infusion ceftriaxone better than once-a-day dosing in intensive care? A randomized controlled pilot study. J Antimicrob Chemother. 2007;59:285–91. doi: 10.1093/jac/dkl478. [DOI] [PubMed] [Google Scholar]
- 365.Yost RJ, Cappelletty DM, group RS. The Retrospective Cohort of Extended-Infusion Piperacillin-Tazobactam (RECEIPT) study: A multicenter study. Pharmacotherapy. 2011;31:767–75. doi: 10.1592/phco.31.8.767. [DOI] [PubMed] [Google Scholar]
- 366.Lorente L, Lorenzo L, Martin MM, Jimenez A, Mora ML. Meropenem by continuous versus intermittent infusion in ventilator-associated pneumonia due to gram-negative bacilli. Ann Pharmacother. 2006;40:219–23. doi: 10.1345/aph.1G467. [DOI] [PubMed] [Google Scholar]
- 367.Ioannidou E, Siempos II, Falagas ME. Administration of antimicrobials via the respiratory tract for the treatment of patients with nosocomial pneumonia: A meta-analysis. J Antimicrob Chemother. 2007;60:1216–26. doi: 10.1093/jac/dkm385. [DOI] [PubMed] [Google Scholar]
- 368.Palmer LB, Smaldone GC, Chen JJ, Baram D, Duan T, Monteforte M, et al. Aerosolized antibiotics and ventilator-associated tracheobronchitis in the intensive care unit. Crit Care Med. 2008;36:2008–13. doi: 10.1097/CCM.0b013e31817c0f9e. [DOI] [PubMed] [Google Scholar]
- 369.Arnold HM, Sawyer AM, Kollef MH. Use of Adjunctive Aerosolized Antimicrobial Therapy in the Treatment of Pseudomonas aeruginosa and Acinetobacter baumannii Ventilator-Associated Pneumonia. Respir Care. 2012 doi: 10.4187/respcare.01556. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 370.Rattanaumpawan P, Lorsutthitham J, Ungprasert P, Angkasekwinai N, Thamlikitkul V. Randomized controlled trial of nebulized colistimethate sodium as adjunctive therapy of ventilator-associated pneumonia caused by Gram-negative bacteria. J Antimicrob Chemother. 2010;65:2645–9. doi: 10.1093/jac/dkq360. [DOI] [PubMed] [Google Scholar]
- 371.Korbila IP, Michalopoulos A, Rafailidis PI, Nikita D, Samonis G, Falagas ME. Inhaled colistin as adjunctive therapy to intravenous colistin for the treatment of microbiologically documented ventilator-associated pneumonia: A comparative cohort study. Clin Microbiol Infect. 2010;16:1230–6. doi: 10.1111/j.1469-0691.2009.03040.x. [DOI] [PubMed] [Google Scholar]
- 372.Michalopoulos A, Fotakis D, Virtzili S, Vletsas C, Raftopoulou S, Mastora Z, et al. Aerosolized colistin as adjunctive treatment of ventilator-associated pneumonia due to multidrug-resistant Gram-negative bacteria: A prospective study. Respir Med. 2008;102:407–12. doi: 10.1016/j.rmed.2007.10.011. [DOI] [PubMed] [Google Scholar]
- 373.Lin CC, Liu TC, Kuo CF, Liu CP, Lee CM. Aerosolized colistin for the treatment of multidrug-resistant Acinetobacter baumannii pneumonia: Experience in a tertiary care hospital in northern Taiwan. J Microbiol Immunol Infect. 2010;43:323–31. doi: 10.1016/S1684-1182(10)60050-3. [DOI] [PubMed] [Google Scholar]
- 374.Michalopoulos A, Kasiakou SK, Mastora Z, Rellos K, Kapaskelis AM, Falagas ME. Aerosolized colistin for the treatment of nosocomial pneumonia due to multidrug-resistant Gram-negative bacteria in patients without cystic fibrosis. Crit Care. 2005;9:R53–9. doi: 10.1186/cc3020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 375.Berlana D, Llop JM, Fort E, Badia MB, Jodar R. Use of colistin in the treatment of multiple-drug-resistant gram-negative infections. Am J Health Syst Pharm. 2005;62:39–47. doi: 10.1093/ajhp/62.1.39. [DOI] [PubMed] [Google Scholar]
- 376.Falagas ME, Siempos II, Rafailidis PI, Korbila IP, Ioannidou E, Michalopoulos A. Inhaled colistin as monotherapy for multidrug-resistant gram (-) nosocomial pneumonia: A case series. Respir Med. 2009;103:707–13. doi: 10.1016/j.rmed.2008.11.018. [DOI] [PubMed] [Google Scholar]
- 377.Kwa AL, Loh C, Low JG, Kurup A, Tam VH. Nebulized colistin in the treatment of pneumonia due to multidrug-resistant Acinetobacter baumannii and Pseudomonas aeruginosa. Clin Infect Dis. 2005;41:754–7. doi: 10.1086/432583. [DOI] [PubMed] [Google Scholar]
- 378.Craven DE, Hjalmarson KI. Ventilator-associated tracheobronchitis and pneumonia: Thinking outside the box. Clin Infect Dis. 2010;51(Suppl 1):S59–66. doi: 10.1086/653051. [DOI] [PubMed] [Google Scholar]
- 379.Nseir S, Di Pompeo C, Soubrier S, Lenci H, Delour P, Onimus T, et al. Effect of ventilator-associated tracheobronchitis on outcome in patients without chronic respiratory failure: A case-control study. Crit Care. 2005;9:R238–45. doi: 10.1186/cc3508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 380.Agrafiotis M, Siempos II, Falagas ME. Frequency, prevention, outcome and treatment of ventilator-associated tracheobronchitis: Systematic review and meta-analysis. Respir Med. 2010;104:325–36. doi: 10.1016/j.rmed.2009.09.001. [DOI] [PubMed] [Google Scholar]
- 381.Stryjewski ME, Corey GR. New treatments for methicillin-resistant Staphylococcus aureus. Curr Opin Crit Care. 2009;15:403–12. doi: 10.1097/MCC.0b013e32832f0a74. [DOI] [PubMed] [Google Scholar]
- 382.Ferrara AM. Treatment of hospital-acquired pneumonia caused by methicillin-resistant Staphylococcus aureus. Int J Antimicrob Agents. 2007;30:19–24. doi: 10.1016/j.ijantimicag.2007.02.011. [DOI] [PubMed] [Google Scholar]
- 383.Kalil AC, Murthy MH, Hermsen ED, Neto FK, Sun J, Rupp ME. Linezolid versus vancomycin or teicoplanin for nosocomial pneumonia: A systematic review and meta-analysis. Crit Care Med. 2010;38:1802–8. doi: 10.1097/CCM.0b013e3181eb3b96. [DOI] [PubMed] [Google Scholar]
- 384.Walkey AJ, O’Donnell MR, Wiener RS. Linezolid vs glycopeptide antibiotics for the treatment of suspected methicillin-resistant Staphylococcus aureus nosocomial pneumonia: A meta-analysis of randomized controlled trials. Chest. 2011;139:1148–55. doi: 10.1378/chest.10-1556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 385.Wunderink RG, Niederman MS, Kollef MH, Shorr AF, Kunkel MJ, Baruch A, et al. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: A randomized, controlled study. Clin Infect Dis. 2012;54:621–9. doi: 10.1093/cid/cir895. [DOI] [PubMed] [Google Scholar]
- 386.Garnacho-Montero J, Amaya-Villar R. Multiresistant Acinetobacter baumannii infections: Epidemiology and management. Curr Opin Infect Dis. 2010;23:332–9. doi: 10.1097/QCO.0b013e32833ae38b. [DOI] [PubMed] [Google Scholar]
- 387.Florescu DF, Qiu F, McCartan MA, Mindru C, Fey PD, Kalil AC. What is the efficacy and safety of colistin for the treatment of ventilator-associated pneumonia? A systematic review and meta-regression. Clin Infect Dis. 2012;54:670–80. doi: 10.1093/cid/cir934. [DOI] [PubMed] [Google Scholar]
- 388.Markou N, Markantonis SL, Dimitrakis E, Panidis D, Boutzouka E, Karatzas S, et al. Colistin serum concentrations after intravenous administration in critically ill patients with serious multidrug-resistant, gram-negative bacilli infections: A prospective, open-label, uncontrolled study. Clin Ther. 2008;30:143–51. doi: 10.1016/j.clinthera.2008.01.015. [DOI] [PubMed] [Google Scholar]
- 389.Plachouras D, Karvanen M, Friberg LE, Papadomichelakis E, Antoniadou A, Tsangaris I, et al. Population pharmacokinetic analysis of colistin methanesulfonate and colistin after intravenous administration in critically ill patients with infections caused by gram-negative bacteria. Antimicrob Agents Chemother. 2009;53:3430–6. doi: 10.1128/AAC.01361-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 390.Imberti R, Cusato M, Villani P, Carnevale L, Iotti GA, Langer M, et al. Steady-state pharmacokinetics and BAL concentration of colistin in critically Ill patients after IV colistin methanesulfonate administration. Chest. 2010;138:1333–9. doi: 10.1378/chest.10-0463. [DOI] [PubMed] [Google Scholar]
- 391.Zavascki AP, Goldani LZ, Li J, Nation RL. Polymyxin B for the treatment of multidrug-resistant pathogens: A critical review. J Antimicrob Chemother. 2007;60:1206–15. doi: 10.1093/jac/dkm357. [DOI] [PubMed] [Google Scholar]
- 392.Souli M, Galani I, Antoniadou A, Papadomichelakis E, Poulakou G, Panagea T, et al. An outbreak of infection due to beta-Lactamase Klebsiella pneumoniae Carbapenemase 2-producing K.pneumoniae in a Greek University Hospital: Molecular characterization, epidemiology, and outcomes. Clin Infect Dis. 2010;50:364–73. doi: 10.1086/649865. [DOI] [PubMed] [Google Scholar]
- 393.Cisneros JM, Reyes MJ, Pachon J, Becerril B, Caballero FJ, Garcia-Garmendia JL, et al. Bacteremia due to Acinetobacter baumannii: Epidemiology, clinical findings, and prognostic features. Clin Infect Dis. 1996;22:1026–32. doi: 10.1093/clinids/22.6.1026. [DOI] [PubMed] [Google Scholar]
- 394.Wood GC, Hanes SD, Croce MA, Fabian TC, Boucher BA. Comparison of ampicillin-sulbactam and imipenem-cilastatin for the treatment of acinetobacter ventilator-associated pneumonia. Clin Infect Dis. 2002;34:1425–30. doi: 10.1086/340055. [DOI] [PubMed] [Google Scholar]
- 395.Motaouakkil S, Charra B, Hachimi A, Nejmi H, Benslama A, Elmdaghri N, et al. Colistin and rifampicin in the treatment of nosocomial infections from multiresistant Acinetobacter baumannii. J Infect. 2006;53:274–8. doi: 10.1016/j.jinf.2005.11.019. [DOI] [PubMed] [Google Scholar]
- 396.Bassetti M, Repetto E, Righi E, Boni S, Diverio M, Molinari MP, et al. Colistin and rifampicin in the treatment of multidrug-resistant Acinetobacter baumannii infections. J Antimicrob Chemother. 2008;61:417–20. doi: 10.1093/jac/dkm509. [DOI] [PubMed] [Google Scholar]
- 397.Song JY, Lee J, Heo JY, Noh JY, Kim WJ, Cheong HJ, et al. Colistin and rifampicin combination in the treatment of ventilator-associated pneumonia caused by carbapenem-resistant Acinetobacter baumannii. Int J Antimicrob Agents. 2008;32:281–4. doi: 10.1016/j.ijantimicag.2008.04.013. [DOI] [PubMed] [Google Scholar]
- 398.Yahav D, Lador A, Paul M, Leibovici L. Efficacy and safety of tigecycline: A systematic review and meta-analysis. J Antimicrob Chemother. 2011;66:1963–71. doi: 10.1093/jac/dkr242. [DOI] [PubMed] [Google Scholar]
- 399.Tasina E, Haidich AB, Kokkali S, Arvanitidou M. Efficacy and safety of tigecycline for the treatment of infectious diseases: A meta-analysis. Lancet Infect Dis. 2011;11:834–44. doi: 10.1016/S1473-3099(11)70177-3. [DOI] [PubMed] [Google Scholar]
- 400.Sun HY, Fujitani S, Quintiliani R, Yu VL. Pneumonia due to Pseudomonas aeruginosa: Part II: Antimicrobial resistance, pharmacodynamic concepts, and antibiotic therapy. Chest. 2011;139:1172–85. doi: 10.1378/chest.10-0167. [DOI] [PubMed] [Google Scholar]
- 401.Coppadoro A, Bittner E, Berra L. Novel preventive strategies for ventilator-associated pneumonia. Crit Care. 2012;16:210. doi: 10.1186/cc11225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 402.Alroumi F, Sarwar A, Grgurich PE, Lei Y, Hudcova J, Craven DE. Strategies for prevention of ventilator-associated pneumonia: Bundles, devices, and medications for improved patient outcomes. Hosp Pract (Minneap) 2012;40:81–92. doi: 10.3810/hp.2012.02.949. [DOI] [PubMed] [Google Scholar]
- 403.Maselli DJ, Restrepo MI. Strategies in the prevention of ventilator-associated pneumonia. Ther Adv Respir Dis. 2011;5:131–41. doi: 10.1177/1753465810395655. [DOI] [PubMed] [Google Scholar]
- 404.Leasure AR, Stirlen J, Lu SH. Prevention of ventilator-associated pneumonia through aspiration of subglottic secretions: A systematic review and meta-analysis. Dimens Crit Care Nurs. 2012;31:102–17. doi: 10.1097/DCC.0b013e3182445ff3. [DOI] [PubMed] [Google Scholar]
- 405.Roberts N, Moule P. Chlorhexidine and tooth-brushing as prevention strategies in reducing ventilator-associated pneumonia rates. Nurs Crit Care. 2011;16:295–302. doi: 10.1111/j.1478-5153.2011.00465.x. [DOI] [PubMed] [Google Scholar]
- 406.Muscedere J, Rewa O, McKechnie K, Jiang X, Laporta D, Heyland DK. Subglottic secretion drainage for the prevention of ventilator-associated pneumonia: A systematic review and meta-analysis. Crit Care Med. 2011;39:1985–91. doi: 10.1097/CCM.0b013e318218a4d9. [DOI] [PubMed] [Google Scholar]
- 407.Labeau SO, Van de Vyver K, Brusselaers N, Vogelaers D, Blot SI. Prevention of ventilator-associated pneumonia with oral antiseptics: A systematic review and meta-analysis. Lancet Infect Dis. 2011;11:845–54. doi: 10.1016/S1473-3099(11)70127-X. [DOI] [PubMed] [Google Scholar]
- 408.Blot S, Rello J, Vogelaers D. What is new in the prevention of ventilator-associated pneumonia? Curr Opin Pulm Med. 2011;17:155–9. doi: 10.1097/MCP.0b013e328344db65. [DOI] [PubMed] [Google Scholar]
- 409.Klompas M. Prevention of ventilator-associated pneumonia. Expert Rev Anti Infect Ther. 2010;8:791–800. doi: 10.1586/eri.10.59. [DOI] [PubMed] [Google Scholar]
- 410.Kollef MH. Prevention of hospital-associated pneumonia and ventilator-associated pneumonia. Crit Care Med. 2004;32:1396–405. doi: 10.1097/01.ccm.0000128569.09113.fb. [DOI] [PubMed] [Google Scholar]
- 411.van Saene HK, Baines PB. The prevention of ventilator-associated pneumonia. N Engl J Med. 1999;341:293–4. doi: 10.1056/nejm199907223410419. [DOI] [PubMed] [Google Scholar]
- 412.Tantipong H, Morkchareonpong C, Jaiyindee S, Thamlikitkul V. Randomized controlled trial and meta-analysis of oral decontamination with 2% chlorhexidine solution for the prevention of ventilator-associated pneumonia. Infect Control Hosp Epidemiol. 2008;29:131–6. doi: 10.1086/526438. [DOI] [PubMed] [Google Scholar]
- 413.Zamora Zamora F. Effectiveness of oral care in the prevention of ventilator-associated pneumonia.systematic review and meta-analysis of randomised clinical trials. Enferm Clin. 2011;21:308–19. doi: 10.1016/j.enfcli.2011.09.008. [DOI] [PubMed] [Google Scholar]
- 414.Chan EY, Ruest A, Meade MO, Cook DJ. Oral decontamination for prevention of pneumonia in mechanically ventilated adults: Systematic review and meta-analysis. BMJ. 2007;334:889. doi: 10.1136/bmj.39136.528160.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 415.Chlebicki MP, Safdar N. Topical chlorhexidine for prevention of ventilator-associated pneumonia: A meta-analysis. Crit Care Med. 2007;35:595–602. doi: 10.1097/01.CCM.0000253395.70708.AC. [DOI] [PubMed] [Google Scholar]
- 416.Rabie T, Curtis V. Handwashing and risk of respiratory infections: A quantitative systematic review. Trop Med Int Health. 2006;11:258–67. doi: 10.1111/j.1365-3156.2006.01568.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 417.Alexiou VG, Ierodiakonou V, Dimopoulos G, Falagas ME. Impact of patient position on the incidence of ventilator-associated pneumonia: A meta-analysis of randomized controlled trials. J Crit Care. 2009;24:515–22. doi: 10.1016/j.jcrc.2008.09.003. [DOI] [PubMed] [Google Scholar]
- 418.Li Bassi G, Torres A. Ventilator-associated pneumonia: Role of positioning. Curr Opin Crit Care. 2011;17:57–63. doi: 10.1097/MCC.0b013e3283428b31. [DOI] [PubMed] [Google Scholar]
- 419.Girard TD, Kress JP, Fuchs BD, Thomason JW, Schweickert WD, Pun BT, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): A randomised controlled trial. Lancet. 2008;371:126–34. doi: 10.1016/S0140-6736(08)60105-1. [DOI] [PubMed] [Google Scholar]
- 420.Robertson TE, Mann HJ, Hyzy R, Rogers A, Douglas I, Waxman AB, et al. Multicenter implementation of a consensus-developed, evidence-based, spontaneous breathing trial protocol. Crit Care Med. 2008;36:2753–62. doi: 10.1097/ccm.0b013e3181872833. [DOI] [PubMed] [Google Scholar]
- 421.Girou E, Schortgen F, Delclaux C, Brun-Buisson C, Blot F, Lefort Y, et al. Association of noninvasive ventilation with nosocomial infections and survival in critically ill patients. JAMA. 2000;284:2361–7. doi: 10.1001/jama.284.18.2361. [DOI] [PubMed] [Google Scholar]
- 422.Bouza E, Perez MJ, Munoz P, Rincon C, Barrio JM, Hortal J. Continuous aspiration of subglottic secretions in the prevention of ventilator-associated pneumonia in the postoperative period of major heart surgery. Chest. 2008;134:938–46. doi: 10.1378/chest.08-0103. [DOI] [PubMed] [Google Scholar]
- 423.Dezfulian C, Shojania K, Collard HR, Kim HM, Matthay MA, Saint S. Subglottic secretion drainage for preventing ventilator-associated pneumonia: A meta-analysis. Am J Med. 2005;118:11–8. doi: 10.1016/j.amjmed.2004.07.051. [DOI] [PubMed] [Google Scholar]
- 424.Boots RJ, George N, Faoagali JL, Druery J, Dean K, Heller RF. Double-heater-wire circuits and heat-and-moisture exchangers and the risk of ventilator-associated pneumonia. Crit Care Med. 2006;34:687–93. doi: 10.1097/01.CCM.0000201887.51076.31. [DOI] [PubMed] [Google Scholar]
- 425.Bench S. Humidification in the long-term ventilated patient: A systematic review. Intensive Crit Care Nurs. 2003;19:75–84. doi: 10.1016/s0964-3397(03)00024-7. [DOI] [PubMed] [Google Scholar]
- 426.Lorente L, Lecuona M, Jimenez A, Mora ML, Sierra A. Ventilator-associated pneumonia using a heated humidifier or a heat and moisture exchanger: A randomized controlled trial [ISRCTN88724583] Crit Care. 2006;10:R116. doi: 10.1186/cc5009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 427.Ricard JD, Boyer A, Dreyfuss D. The effect of humidification on the incidence of ventilator-associated pneumonia. Respir Care Clin N Am. 2006;12:263–73. doi: 10.1016/j.rcc.2006.03.007. [DOI] [PubMed] [Google Scholar]
- 428.Lacherade JC, Auburtin M, Cerf C, Van de Louw A, Soufir L, Rebufat Y, et al. Impact of humidification systems on ventilator-associated pneumonia: A randomized multicenter trial. Am J Respir Crit Care Med. 2005;172:1276–82. doi: 10.1164/rccm.200408-1028OC. [DOI] [PubMed] [Google Scholar]
- 429.Subirana M, Sola I, Benito S. Closed tracheal suction systems versus open tracheal suction systems for mechanically ventilated adult patients. Cochrane Database Syst Rev. 2007:CD004581. doi: 10.1002/14651858.CD004581.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 430.Harada N. Closed suctioning system: Critical analysis for its use. Jpn J Nurs Sci. 2010;7:19–28. doi: 10.1111/j.1742-7924.2010.00143.x. [DOI] [PubMed] [Google Scholar]
- 431.Siempos II, Vardakas KZ, Falagas ME. Closed tracheal suction systems for prevention of ventilator-associated pneumonia. Br J Anaesth. 2008;100:299–306. doi: 10.1093/bja/aem403. [DOI] [PubMed] [Google Scholar]
- 432.Holzapfel L, Chastang C, Demingeon G, Bohe J, Piralla B, Coupry A. A randomized study assessing the systematic search for maxillary sinusitis in nasotracheally mechanically ventilated patients. Influence of nosocomial maxillary sinusitis on the occurrence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 1999;159:695–701. doi: 10.1164/ajrccm.159.3.9712076. [DOI] [PubMed] [Google Scholar]
- 433.Holzapfel L, Chevret S, Madinier G, Ohen F, Demingeon G, Coupry A, et al. Influence of long-term oro- or nasotracheal intubation on nosocomial maxillary sinusitis and pneumonia: Results of a prospective, randomized, clinical trial. Crit Care Med. 1993;21:1132–8. doi: 10.1097/00003246-199308000-00010. [DOI] [PubMed] [Google Scholar]
- 434.Craven DE, Goularte TA, Make BJ. Contaminated condensate in mechanical ventilator circuits. A risk factor for nosocomial pneumonia? Am Rev Respir Dis. 1984;129:625–8. [PubMed] [Google Scholar]
- 435.Craven DE, Lichtenberg DA, Goularte TA, Make BJ, McCabe WR. Contaminated medication nebulizers in mechanical ventilator circuits. Source of bacterial aerosols. Am J Med. 1984;77:834–8. doi: 10.1016/0002-9343(84)90520-5. [DOI] [PubMed] [Google Scholar]
- 436.Rello J, Sonora R, Jubert P, Artigas A, Rue M, Valles J. Pneumonia in intubated patients: Role of respiratory airway care. Am J Respir Crit Care Med. 1996;154:111–5. doi: 10.1164/ajrccm.154.1.8680665. [DOI] [PubMed] [Google Scholar]
- 437.Mehta AK, Halvosa JS, Gould CV, Steinberg JP. Efficacy of alcohol-based hand rubs in the disinfection of stethoscopes. Infect Control Hosp Epidemiol. 2010;31:870–2. doi: 10.1086/655437. [DOI] [PubMed] [Google Scholar]
- 438.van Essen EH, de Jonge E. Selective decontamination of the digestive tract (SDD): Is the game worth the candle? Semin Respir Crit Care Med. 2011;32:236–42. doi: 10.1055/s-0031-1275536. [DOI] [PubMed] [Google Scholar]
- 439.Fink JB, Krause SA, Barrett L, Schaaff D, Alex CG. Extending ventilator circuit change interval beyond 2 days reduces the likelihood of ventilator-associated pneumonia. Chest. 1998;113:405–11. doi: 10.1378/chest.113.2.405. [DOI] [PubMed] [Google Scholar]
- 440.Hess DR, Kallstrom TJ, Mottram CD, Myers TR, Sorenson HM, Vines DL. Care of the ventilator circuit and its relation to ventilator-associated pneumonia. Respir Care. 2003;48:869–79. [PubMed] [Google Scholar]
- 441.Lorente L, Blot S, Rello J. New issues and controversies in the prevention of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2010;182:870–6. doi: 10.1164/rccm.201001-0081CI. [DOI] [PubMed] [Google Scholar]
- 442.Gomes Silva BN, Andriolo RB, Saconato H, Atallah AN, Valente O. Early versus late tracheostomy for critically ill patients. Cochrane Database Syst Rev. 2012;3:CD007271. doi: 10.1002/14651858.CD007271.pub2. [DOI] [PubMed] [Google Scholar]
- 443.Cook DJ, Fuller HD, Guyatt GH, Marshall JC, Leasa D, Hall R, et al. Risk factors for gastrointestinal bleeding in critically ill patients. Canadian Critical Care Trials Group. N Engl J Med. 1994;330:377–81. doi: 10.1056/NEJM199402103300601. [DOI] [PubMed] [Google Scholar]
- 444.Lin PC, Chang CH, Hsu PI, Tseng PL, Huang YB. The efficacy and safety of proton pump inhibitors vs histamine-2 receptor antagonists for stress ulcer bleeding prophylaxis among critical care patients: A meta-analysis. Crit Care Med. 2010;38:1197–205. doi: 10.1097/CCM.0b013e3181d69ccf. [DOI] [PubMed] [Google Scholar]
- 445.Cook DJ, Witt LG, Cook RJ, Guyatt GH. Stress ulcer prophylaxis in the critically ill: A meta-analysis. Am J Med. 1991;91:519–27. doi: 10.1016/0002-9343(91)90189-5. [DOI] [PubMed] [Google Scholar]
- 446.Cook D, Guyatt G, Marshall J, Leasa D, Fuller H, Hall R, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. N Engl J Med. 1998;338:791–7. doi: 10.1056/NEJM199803193381203. [DOI] [PubMed] [Google Scholar]
- 447.Cook DJ, Reeve BK, Guyatt GH, Heyland DK, Griffith LE, Buckingham L, et al. Stress ulcer prophylaxis in critically ill patients. Resolving discordant meta-analyses. JAMA. 1996;275:308–14. [PubMed] [Google Scholar]
- 448.Heyland DK, Dhaliwal R, Drover JW, Gramlich L, Dodek P. Canadian clinical practice guidelines for nutrition support in mechanically ventilated, critically ill adult patients. JPEN J Parenter Enteral Nutr. 2003;27:355–73. doi: 10.1177/0148607103027005355. [DOI] [PubMed] [Google Scholar]
- 449.Wein L, Wein S, Haas SJ, Shaw J, Krum H. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients: A meta-analysis of randomized controlled trials. Arch Intern Med. 2007;167:1476–86. doi: 10.1001/archinte.167.14.1476. [DOI] [PubMed] [Google Scholar]
- 450.Egi M, Finfer S, Bellomo R. Glycemic control in the ICU. Chest. 2011;140:212–20. doi: 10.1378/chest.10-1478. [DOI] [PubMed] [Google Scholar]
- 451.Hebert PC, Tinmouth A, Corwin HL. Controversies in RBC transfusion in the critically ill. Chest. 2007;131:1583–90. doi: 10.1378/chest.06-1055. [DOI] [PubMed] [Google Scholar]