

Abstract
Several studies have shown that visual recovery after blindness that occurs early in life is never complete. The current study investigated whether an extremely long period of blindness might also cause a permanent impairment of visual performance, even in a case of adult-onset blindness. We examined KP, a 71-year-old man who underwent a successful sight-restoring operation after 53 years of blindness. A set of psychophysical tests designed to assess KP's face perception, object recognition, and visual space perception abilities were conducted six months and eight months after the surgery. The results demonstrate that regardless of a lengthy period of normal vision and rich pre-accident perceptual experience, KP did not fully integrate this experience, and his visual performance remained greatly compromised. This was particularly evident when the tasks targeted finer levels of perceptual processing. In addition to the decreased robustness of his memory representations, which was hypothesized as the main factor determining visual impairment, other factors that may have affected KP's performance were considered, including compromised visual functions, problems with perceptual organization, deficits in the simultaneous processing of visual information, and reduced cognitive abilities.
Keywords: sight recovery, blindness, visual deprivation, object agnosia, prosopagnosia
1. Introduction
Behavioral research on sight-recovery subjects who lost their sight early in life has demonstrated that despite post-surgical improvements in their ability to make sense of the visual world, these individuals still show substantial perceptual deficits across various domains. For instance, patient MM, who lost his sight at the age of three and half and recovered his sight when he was 46, had difficulty with the three-dimensional (3-D) interpretation of retinal images and with object and face recognition (Fine et al., 2003). These deficits are similar to those reported in a variety of earlier case studies on the effects of early visual deprivation, including patients such as Virgil (Sacks, 1995), SB (Gregory & Wallace, 1963), and HB (Ackroyd, Humphrey, & Warrington, 1974). It is commonly assumed that a critical factor in this permanent visual impairment is early visual deprivation occurring near the human critical period (Lewis & Maurer, 2005).
Here, we show that very long term visual loss initiated in adulthood may also have critical consequences on post-treatment visual development. KP, a 71-year-old man, had normal vision until he lost his sight at the age of 17 due to an explosion at the factory where he worked. The accident caused binocular damage to the cornea as a result of exposure to molten metal. During the years of his blindness, KP underwent several optical surgeries, but none were successful. According to his self-report, he was only able to discriminate between light and dark with no ability to perform form discrimination. In September 2009, after 53 years of visual deprivation, KP received the Boston keratoprosthesis type I, and this surgery resulted in restored monocular vision to his right eye.
We tested KP's visual skills using stimuli and methods similar to those described in recent studies of sight-recovery patients who had experienced early-onset blindness (Fine et al., 2003; Ostrovsky, Andalman, & Sinha, 2006; Ostrovsky, Meyers, Ganesh, Mathur, & Sinha, 2009). Using these methods allowed us to make a direct comparison of KP's perceptual performance. Specifically, we conducted a set of psychophysical tests designed to assess KP's object recognition, face perception, and visual space perception abilities, which have previously been identified as the most afflicted domains in sight-recovery patients (Fine, 2009; Fine et al., 2003; Gregory & Wallace, 1963; Ostrovsky et al., 2006).
For a subset of the tests, we performed matched tests on MM, the early-blind and sight-recovery subject described above. In the case of MM, the visual deprivation had continued for 40 years.
Our primary objective in the present study was to assess the contribution of KP's pre-blindness visual experience to recovered vision. We expected that KP's perceptual performance would be superior to that of MM and other patients described in previous studies, especially in tasks that require the subject to match a visual stimulus with a stored memory representation.
2. Experimental methods
2.1. Participants
2.1.1. Examinations—KP
KP's visual skills were assessed during two separate experimental sessions six and eight months after the surgery. Most of the tests were performed during the first examination, which occurred in March 2010 at the Gemini Eye Clinic in Zlín, Czech Republic, where the successful operation on his right eye had been performed. KP's right eye visual acuity at the time of the first examination was assessed as 20/60 after correction. His contrast sensitivity, evaluated using the Pelli-Robson chart, was 0.65 log units (compare to the value of 1.68 that was found to be the average in the 60 years and older group; Mäntyjärvi & Laitinen, 2001). An accompanying neuropsychological examination of his general cognitive abilities did not reveal any cognitive deficits (see the Supplementary Materials). The examination of the visual evoked potentials (VEPs) provided evidence of a preserved projection of visual information to the primary visual area and to the extrastriate areas of the dorsal stream. However, KP's responses already at the level of the primary visual area were severely delayed. Surprisingly, during the visual processing of a cognitive task, such as the oddball task, the interval between sensory detection peaks and the cognitive P300 wave was comparable to that in healthy controls (Kremláček et al., 2013; for the electrophysiological data in patients who underwent cataract removal, see Sloper & Collins, 1995).
One additional experiment, specifically the RISE test, was conducted eight months after the surgery. At the time of the second examination, KP's measured visual acuity had deteriorated to 20/100, and his contrast sensitivity was 0.5 (these values varied considerably over time; see also Kremláček et al., 2013).
Experimental stimuli were displayed on a laptop computer with a 17-inch screen. The screen resolution was set to 1440 × 900 pixels. The average viewing distance was 50 cm, which meant that the screen subtended a visual angle of 38° horizontally and 29° vertically.
Responses were made verbally, and there was no limit on how long KP could study an image; sometimes he responded immediately, and sometimes he took tens of seconds to respond. To maintain motivation, feedback was provided after each response.
2.1.2. Examinations—MM
MM's performance was examined once, 12 years after the surgery. Experimental stimuli were displayed on a laptop computer with a 15.6-inch screen. The screen resolution was set to 1280 × 800 pixels. The average viewing distance was 50 cm, which meant that the screen subtended a visual angle of 38° horizontally and 22° vertically.
The responses were made verbally, and there was no limit on how long MM could study an image. No feedback was provided.
2.1.3. Examinations—Controls
Two 71-year-old men served as a control group for KP. These subjects viewed blurred stimuli to simulate KP's loss of image information due to his compromised acuity and contrast sensitivity.1 Some tasks were trivial for them and were not tested. All the other experimental details were matched to those used for KP, as described above.
2.2. Experimental stimuli
A brief description of the individual tests is provided below. For a more detailed description, see the Supplementary Materials.
2.2.1. Face perception
We evaluated the ability of KP and MM to detect, discriminate between, and recognize human faces using four tests (see the upper row of Figure 1): (i) face/non-face discrimination, in which the subjects were asked to determine whether an image represented a face or not; (ii) face localization in complex scenes, in which the task was to count the human faces in an image; (iii) gender classification, in which the task was to assess whether a male or female face was presented; and (iv) face discrimination, in which the subjects were asked to determine whether two faces shown simultaneously belonged to the same person or not. Because of time constraints, task (ii) was not performed with MM.
Figure 1.

Sample stimuli from all the tests conducted with KP (six and eight months after his sight-recovery operation), MM (12 years after his sight-recovery operation) and the control subjects.
2.2.2. Object recognition
We asked KP and MM to identify a variety of object images presented in both canonical and noncanonical forms (see the second row of Figure 1). First, the subjects were shown 10 objects in atypical colors, 10 objects from a less-typical perspective, 10 half-occluded objects, and 10 silhouettes of objects. After completing several other experiments, KP was asked again to identify these 40 objects, which were now presented in canonical form. Because of time constraints, the latter task was not performed with MM.
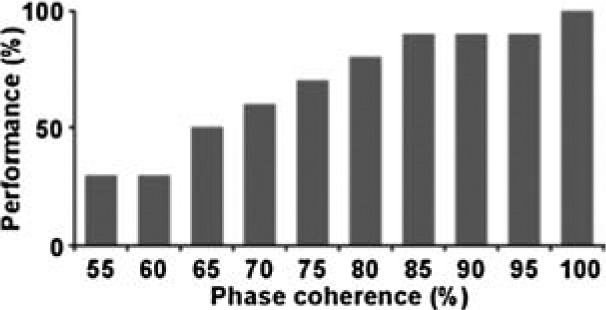
In the second examination, conducted eight months after KP's surgery, another object recognition test was administered. In this test, 10 grayscale images of common objects were used as a source for creating stimuli. Each image was degraded using the Random Image Structure Evolution (RISE) procedure (Sadr & Sinha, 2001, 2004). This procedure changes the spatial structure of an image while preserving its spatial frequency spectrum, overall luminance, and contrast. Each image underwent 10 levels of image degradations, ranging from 50% to 100% phase coherence, in 5% increments (see the third row of Figure 1). No isolated parts of the disintegrated image contained sufficient diagnostic information to allow successful object recognition; therefore, focusing on individual components of the visual input would lead to an incorrect response. Because of time constraints, this task was not performed with MM.
2.2.3. Visual space perception
We used four different tests to examine various aspects of KP's visual space perception (see the bottom row of Figure 1): (i) sensitivity to individual pictorial depth cues in naturalistic photographs; (ii) simple size constancy—KP was asked to make a judgment about the relative lengths of a pair of paper strips placed on a table in front of him, located in either the frontal or sagittal planes; (iii) complex size constancy—KP was asked to adjust the size of one person in a photographic scene so that it would correspond to the size of the another person positioned at a different apparent distance; and (iv) susceptibility to context-induced visual illusions, as a test of the ability to see the stimulus configuration as a perceptual whole. Because of time constraints, these visual space perception tasks were not performed with MM.
3. Results
Table 1 summarizes the results of the study. In general, KP had only minimal trouble performing perceptual tasks that required one-step judgments (e.g., face localization task). However, he experienced serious difficulties performing tasks that required the complex processing of stimulus information (e.g., RISE test) and tasks in which he failed to match a present stimulus with a stored memory representation (e.g., noncanonical object recognition tests). Still, the data are too limited to permit definitive conclusions.
Table 1.
Summary of experimental results.
| KP | MM | Control subjects | Sight-recovery patients in previous studies | |
|---|---|---|---|---|
| Face perception | ||||
| Face/non-face discrimination | 23/26 No false positives |
21/26 Three false positives |
24/26 One false positive |
No errors (SRD) |
| Face localization | 7/10 images, or 39 out of a total of 42 faces localized | – | No errors | No errors (SRD) |
| Gender classification | 4/10 | 3/10 | No errors | 70% (MM); no errors (SRD) |
| Face discrimination | 12/30 | 15/30 | 26/30 | Inability to recognize faces reported (SB); inability to recognize faces reported (Virgil); 60% for 45° depth rotation (SRD) |
| Object recognition | ||||
| Canonical | 36/39 | – | – | 25% (MM; a combination of canonical and noncanonical viewpoints were used); 26% (SK); 34% (JA); 18% (PB) |
| Atypical color | 4/9 | 3/9 | 9/10 | – |
| Less-typical perspective | 6/10 | 4/10 | No errors | – |
| Silhouettes | 9/10 | 4/10 | No errors | – |
| Half-occluded | 9/10 | 0/10 | No errors | – |
| RISE | 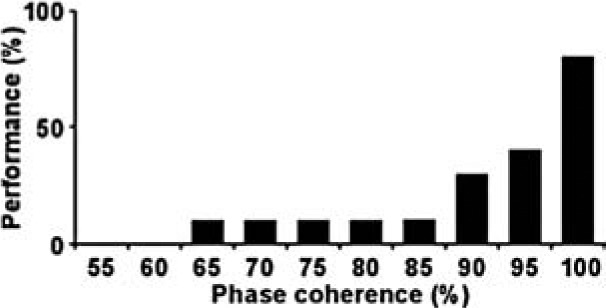 |
– |  |
– |
| Visual space perception | ||||
| Depth cues | 6/8 Sensitivity to interposition, height in the visual field, and texture gradient; at least partial sensitivity to linear perspective |
– | No errors | Sensitivity to shadows and interposition, and insensitivity to perspective (MM); sensitivity to shadows, height in the visual field, and atmospheric perspective cues (SRD); partial sensitivity to interposition (SK) |
| Simple size constancy | In-depth stimuli perceived as smaller than frontal stimuli; more distant stimuli perceived as smaller than closer stimuli | – | – | – |
| Complex size constancy | Mean overestimation of 30%; interquartile range of 60%; low confidence about responses | – | Mean underestimation of 5%; interquartile range of 10% | Inability to estimate distances reported (SB); inability to estimate distances reported (HS, TG, ME, CA); inability to estimate distances reported (Virgil) |
| Visual illusions | Less susceptibility to context-induced visual illusions (Ponzo, Ebbinghaus, Sander, White) | – | Susceptibility to context-induced visual illusions | Less susceptibility to the Müller-Lyer, Poggendorff, Zöllner, and Hering illusions (SB); less susceptibility to Müller-Lyer (LG); susceptibility to simultaneous contrast, Müller-Lyer, and horizontal-vertical illusions (SRD) |
Note. HS, TG, ME, CA, LG (Valvo, 1971); SB (Gregory & Wallace, 1963); Virgil (Sacks, 1995); MM (Fine et al., 2003); SRD (Ostrovsky, Andalman, & Sinha, 2006); SK, JA, PB (Ostrovsky et al., 2009).
3.1. Face perception
Regarding the face perception tests, KP and MM identified human faces with only minimal difficulty and were able to differentiate faces from non-face stimuli. When searching for faces present in a complex scene, KP managed to find a great majority of them, especially those shown in a canonical perspective. However, he missed a few faces in the photographs that lacked identifiable facial features, specifically, a face rotated 90° in the frontal plane and a face bent backward. The performances of KP and MM on the gender classification test were at the level of chance. Similarly, both subjects experienced serious difficulty discriminating between two faces that were shown simultaneously, including two faces shown frontally and two faces presented in different orientations or expressing different emotions.
3.2. Object recognition
KP correctly recognized 92% of objects presented in canonical form, much higher than the 20–30% of objects recognized by early sight-recovery patients in other studies (Fine et al., 2003; Ostrovsky et al., 2009). This result in itself indicates that even after half a century of sensory deprivation, the representations of objects retained in KP's memory could still be successfully applied and also that his neural architecture retained the capacity to relearn object representations. KP's performance on the noncanonical object recognition tests was contingent on the type of modification applied to the image: while he correctly identified almost all the half-occluded objects and silhouettes of objects, he had much greater difficulty recognizing objects depicted in atypical colors and in less-typical perspectives. In contrast, the performances of MM and the control subjects were independent of the type of image modification.
KP's ability to recognize objects when the stimulus conditions were degraded was greatly impaired. Most of the objects in the experimental set were recognized only after the level of degradation of the image was reduced to less than 10%. Two objects in the set were not identified even at 0% noise. In comparison, the control subjects recognized seven of the 10 objects even at 25% noise.
3.3. Visual space perception
The basic mechanisms of KP's visual space perception appeared to be intact. He was able to extract information from various pictorial depth cues and to apply it in tasks requiring simple perceptual judgments. When KP was asked to compare the lengths of two objects, he was able to take into account the objects' distance and orientation and rescale the retinal parameters accordingly. Interestingly, KP exhibited the same distortion of visual space in this test as that demonstrated by normal-sighted individuals, specifically, the underconstancy in the in-depth dimension (e.g., Baird & Biersdorf, 1967; Loomis, Da Silva, Fujita, & Fukusima, 1992; Wagner, 1985; see the Supplementary Materials for details). Perceiving complex 3-D visual scenes presented a bigger problem for him. KP's ability to rescale the size of one of two human figures according to its relative distance was severely limited; he was able to correctly identify only which figure was located at a shorter distance and which was located at a greater distance. The accuracy of his responses was very low, and the variability was extremely high, compared with those of the control subjects (see the relevant part of Table 1). Finally, KP was much less susceptible to context-induced visual illusions than were the control subjects.
4. Discussion
When planning our examination of KP's visual skills, we took into account that at the time of his vision loss, KP had extensive visual experience with various objects, faces, and scenes, in contrast to MM and to other early blindness patients. Furthermore, KP had acquired a large body of knowledge related to object and scene properties, such as how objects interact with their environment and how objects relate to their retinal projections. The examination of this late-blindness patient, surely the oldest onset and the longest period reported in the literature, gave us the opportunity to consider additional determinants of post-treatment visual development that cannot be studied in patients who suffered early visual loss. More specifically, we may have addressed the question of whether KP's visual experience gained during his first 17 years of life had been preserved over an extremely long period of blindness and of whether, after the operation, KP remained able to use it effectively. On the other hand, addressing the classic Molyneux's question, which asks whether a man born blind whose sight was restored would be able immediately to recognize objects by sight, would be of little relevance in this context.
Beyond all doubt, extensive pre-blindness experience facilitated KP's post-treatment visual development. In object recognition tests, he was able to successfully recognize the vast majority of the objects presented, even many with a modified appearance, such as the half-occluded objects and the silhouettes. In depth cues test, KP was able to use individual depth cues to determine depth order.
Paradoxically, his strict reliance on preserved visual representations sometimes led him to misinterpretations and erroneous conclusions. For instance, during the gender classification and face/non-face discrimination tests, KP's strategy was to focus on individual facial features instead of the whole facial stimulus and he made his decision according to how the individual features fit his representations. His answers included “this is a male face because females do not have such big teeth” and “this is a male face because females do not have such dense eyebrows.” Because of this strategy, KP incorrectly classified male and female faces the appearance of which was different from the stored memory representation.
An even more complicated situation arose when no visual memory representation was available. During the RISE test, in which no isolated parts of the disintegrated image carried sufficient diagnostic information to allow successful object recognition, KP repeatedly failed to recognize objects with even relatively low degrees of degradation. In the face localization test, KP missed the least typical faces or faces providing the most ambiguous information.
These situations were not uncommon in KP's everyday life, like when his ophthalmologist asked him to seat himself in a chair with a modern design and KP failed to identify the chair and was confused about where to sit. Remarkably, he may have not recognized even familiar objects presented outside of their usual semantic context. For instance, although he was familiar with pipe fittings, when asked to identify one on a table during lunch, KP was unable to do so.
5. General discussion
This report describes the case of KP, a man who lost his vision at the age of 17 and had his sight restored after 53 years of blindness. Most reports of similar cases concern patients who lost their sight shortly after birth (Ackroyd et al., 1974; Carlson, Hyvärinen, & Raninen, 1986; Fine et al., 2003; Gregory & Wallace, 1963; Sacks, 1995; Valvo, 1971) or who were congenitally blind (Le Grand, Mondloch, Maurer, & Brent, 2001; Ostrovsky et al., 2006, 2009; Valvo, 1971). For those patients, the perceptual domains that are particularly afflicted are object and face recognition, visual space perception (Fine, 2009), and a lower level of visual processing, especially perceptual organization (Ostrovsky et al., 2009). In the present study, we focused specifically on these domains of KP's visual skills. Our results demonstrate that, even after an extremely long period of deprivation, KP could still perform some of the face, object, and visual space tasks, if they targeted coarse processing. As cataract-reversal patients (Hadad, Maurer, & Lewis, 2012; Le Grand, Mondloch, Maurer, & Brent, 2004; Le Grand et al., 2001; Maurer, Le Grand, & Mondloch, 2002), he nevertheless experienced problems when the tasks targeted finer levels of processing. While he easily differentiated faces from non-face stimuli, he was unable to recognize them, not even when they were en face and emotionally neutral. While he correctly judged the depth order of a pair of points, he seemed to have little understanding of 3-D space when perceiving complex visual scenes. On the basis of the present data, it is difficult to draw definitive conclusions about the contribution of KP's pre-blindness visual experience to recovered vision. Of course, rich pre-blindness experience certainly helped him to gain visual skills postoperatively. However, because of the decreased flexibility and robustness of KP's representations, this help was quite limited.
In the present study, pre-blindness visual experience and its integration was postulated as the main factor determining KP's visual recovery. Still, we are aware that his visual skills were also negatively affected by numerous other factors; a more detailed consideration, however, is beyond the scope of the present paper. (i) KP's performance at many tasks was undoubtedly affected by his reduced visual acuity and contrast sensitivity. Unfortunately, we cannot determine the exact extent of this effect because the techniques we used could not fully capture the loss of KP's visual functions. (ii) Furthermore, some of our results (and many episodes in his life) indicate that KP had considerable difficulties with perceptual organization. He was often unable to parse a complex scene or to identify partially overlapping objects. Many times he came to an incorrect conclusion about the identity of an object, such as when he mistook a pencil cup filled with pencils on a doctor's desk for a strange hedgehog. (iii) Additionally, KP's perceptual performance was impaired by his strong tendency to focus on details, coupled with his limited ability to integrate partial information. He failed to holistically perceive complex stimuli, such as faces or scenes. He relied on discrete features to infer the identity of an object or the gist of a scene. This piecemeal approach to interpreting stimuli by focusing on isolated items, which was evident during all the tests (see the examples above, as well as the results of the visual illusions test), may have been partly due to KP's restricted eye movements: During the surgery, the cornea was attached to the eyelid that negatively influenced the extents of eye movements. The problem may have also been caused by a restricted window of attention: At any given moment, KP's perception was limited to a single object without an awareness of the presence of other objects, which is characteristic of simultagnosia and integrative agnosia (Coslett & Saffran, 1991; Thaiss & de Bleser, 1992). (iv) Finally, KP's visual skills may have been affected by his general cognitive abilities. A neuropsychological examination did not reveal any cognitive deficits, and his performance matched his age category (see the Supplementary Materials for details). However, it is justifiable to expect that KP's visual working memory would be insufficient for solving numerous perceptual tasks, especially when considering his piecemeal processing of visual stimuli.
We conclude that the extremely long period of blindness had undoubtedly a strong determining effect on different aspects of KP's post-treatment visual development. Still, KP is well equipped, in our opinion, for stepwise improvement. His family is supportive and stimulates him with new tasks. His son constantly instructs him in new exercises, about which he consults with the ophthalmologist. KP himself exhibits many virtues that are important for coping with a profound life change such as sight recovery: he is resilient, optimistic, active, intelligent, and curious. He enjoyed his sight-recovery experience despite all the related health problems, and he greatly valued the gift of vision. He demonstrated great stamina during the examination (which took approximately 4 hr, including breaks!) and we repeatedly observed that he was prepared to modify his strategy, to segment the visual field into differently bounded regions, or to focus on other properties of the visual scene.
We had high expectations for the planned retests. However, in August 2010, after 11 months of the surgery that restored KP's sight, his eye surgeon diagnosed detachment of the retina, which rapidly impaired his vision to the pretreatment level. The surgeon was considering surgery on his left eye that had been previously operated on several times without success. Regardless of this sad ending, KP's ability to see for a short period of time was, in his own words, the greatest gift for him.
Acknowledgments
This work was funded by a grant, P407/12/2528, from the Grant Agency of the Czech Republic and supported by RVO: 68081740. We would like to thank KP's son for providing much valuable information about KP; and Pawan Sinha for providing us with the RISE images.
Biography
 Radovan Šikl is the head of the Department of Cognitive Psychology at the Institute of Psychology, Academy of Sciences of the Czech Republic. He received his Ph.D. in psychology at Masaryk University. He conducts research on the visual space perception and long-term sensory deprivation.
Radovan Šikl is the head of the Department of Cognitive Psychology at the Institute of Psychology, Academy of Sciences of the Czech Republic. He received his Ph.D. in psychology at Masaryk University. He conducts research on the visual space perception and long-term sensory deprivation.
 Michal Šimeček studied psychology at Massaryk University. He works as a researcher at Transport Research Centre in Brno and at the Institute of Psychology, Academy of Sciences of the Czech Republic. His research interests are related to visual perception, especially the depth perception and visual illusions.
Michal Šimeček studied psychology at Massaryk University. He works as a researcher at Transport Research Centre in Brno and at the Institute of Psychology, Academy of Sciences of the Czech Republic. His research interests are related to visual perception, especially the depth perception and visual illusions.
 Michaela Porubanová-Norquist is an assistant professor at Farmingdale State College. She obtained her Ph.D. from Masaryk University in the Czech Republic. Her current research interests involve interplay between arousal and attention, emotion and iconic memory, and recognition memory.
Michaela Porubanová-Norquist is an assistant professor at Farmingdale State College. She obtained her Ph.D. from Masaryk University in the Czech Republic. Her current research interests involve interplay between arousal and attention, emotion and iconic memory, and recognition memory.
 Ondřej Bezdíček is a clinical neuropsychologist who specializes in the assessment of cognitive disorders. He is working at Charles University in Prague, 1st Faculty of Medicine, and General University Hospital, Department of Neurology and Centre of Clinical Neuroscience. He is actively involved in the development of neuropsychological tests with an emphasis on the Boston and Quantified Process Approach.
Ondřej Bezdíček is a clinical neuropsychologist who specializes in the assessment of cognitive disorders. He is working at Charles University in Prague, 1st Faculty of Medicine, and General University Hospital, Department of Neurology and Centre of Clinical Neuroscience. He is actively involved in the development of neuropsychological tests with an emphasis on the Boston and Quantified Process Approach.
 Jan Kremláček is an associate professor of biophysics (2006) at the Charles University in Prague and got his Ph.D. at the Technical University in Brno (modelling of visual evoked responses 1999). His research focuses mainly on studying of electrophysiological responses associated with visual processing for clinical purposes.
Jan Kremláček is an associate professor of biophysics (2006) at the Charles University in Prague and got his Ph.D. at the Technical University in Brno (modelling of visual evoked responses 1999). His research focuses mainly on studying of electrophysiological responses associated with visual processing for clinical purposes.
 Pavel Stodůlka is the head-surgeon of Gemini Eye Clinics; an internationally recognized high volume eye surgeon and innovator; the first in the Czech Republic to perform lasik and laser cataract surgery; and a teacher at the Charles University in Prague. He has delivered over 500 lectures about eye surgery mostly in Europe and North America.
Pavel Stodůlka is the head-surgeon of Gemini Eye Clinics; an internationally recognized high volume eye surgeon and innovator; the first in the Czech Republic to perform lasik and laser cataract surgery; and a teacher at the Charles University in Prague. He has delivered over 500 lectures about eye surgery mostly in Europe and North America.
 Yuri Ostrovsky studied computer science at Harvard University and completed his Ph.D. in Neuroscience at MIT. He has studied the development of vision in the treated blind for nearly a decade under Project Prakash with Pawan Sinha. He now leads a research group in Wenzhou Medical College exploring functional visual deficits in neurological patients with emphasis on uncovering the core processes that underlie seemingly complex, and perhaps misunderstood, visual syndromes.
Yuri Ostrovsky studied computer science at Harvard University and completed his Ph.D. in Neuroscience at MIT. He has studied the development of vision in the treated blind for nearly a decade under Project Prakash with Pawan Sinha. He now leads a research group in Wenzhou Medical College exploring functional visual deficits in neurological patients with emphasis on uncovering the core processes that underlie seemingly complex, and perhaps misunderstood, visual syndromes.
Footnotes
To blur the presented stimuli, a rotationally symmetric Gaussian lowpass filter was used. The filter properties were empirically determined using a calibration image to approximate KP's visual acuity. Furthermore, the luminance range was compressed to decrease the contrast of the images to the level of KP's contrast sensitivity. The full range was divided by the ratio of KP's contrast sensitivity to that of the controls.
Contributor Information
Radovan Šikl, Institute of Psychology, Academy of Sciences of the Czech Republic, Brno, Czech Republic; e-mail: sikl@psu.cas.cz.
Michal Šimecček, Institute of Psychology, Academy of Sciences of the Czech Republic, Brno, Czech Republic; e-mail: michal.simecek@volny.cz.
Michaela Porubanová-Norquist, Institute of Psychology, Academy of Sciences of the Czech Republic, Brno, Czech Republic; e-mail: misel99@gmail.com.
Ondřej Bezdíček, Department of Neurology, First Faculty of Medicine, Charles University in Prague, Prague, Czech Republic; e-mail: ondrejb@yahoo.com.
Jan Kremláček, Department of Pathophysiology, Faculty of Medicine in Hradec Králové, Charles University in Prague, Hradec Králové, Czech Republic; e-mail: Kremlack@lfhk.cuni.cz.
Pavel Stodůlka, Gemini Eye Clinic, Zlín, Czech Republic; e-mail: stodulka@lasik.cz.
Ione Fine, Department of Psychology, University of Washington, Seattle, WA, USA; e-mail: ionefine@uw.edu.
Yuri Ostrovsky, Department of Brain and Cognitive Sciences, Massachusetts Institute of Technology, Cambridge, MA, USA; e-mail: yostr@mit.edu.
References
- Ackroyd C., Humphrey N. K., Warrington E. K. Lasting effects of early blindness: A case study. Quarterly Journal of Experimental Psychology. (1974);26:114–124. doi: 10.1080/14640747408400393. [DOI] [PubMed] [Google Scholar]
- Baird J. C., Biersdorf W. R. Quantitative functions for size and distance judgments. Perception & Psychophysics. (1967);2:161–166. doi: 10.3758/BF03210312. [DOI] [Google Scholar]
- Carlson S., Hyvärinen L., Raninen A. Persistent behavioural blindness after early visual deprivation and active visual rehabilitation: A case report. British Journal of Ophthalmology. (1986);70:607–611. doi: 10.1136/bjo.70.8.607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coslett H. B., Saffran E. Simultanagnosia: To see but not two see. Brain. (1991);114:1523–1545. doi: 10.1093/brain/114.4.1523. [DOI] [PubMed] [Google Scholar]
- Fine I. Recovery of vision following blindness. In: Goldstein E. B., editor. Encyclopedia of perception. Thousands Oaks, CA: Sage; (2009). pp. 864–866. (pp. [Google Scholar]
- Fine I., Wade A. R., Brewer A. A., May M. G., Goodman D. F., Boynton G. M., MacLeod D. I. A. Long-term deprivation affects visual perception and cortex. Nature Neuroscience. (2003);6:915–916. doi: 10.1038/nn1102. [DOI] [PubMed] [Google Scholar]
- Gregory R. L., Wallace J. G. Recovery from early blindness: A case study. (Experimental Psychology Monograph No. 2). London; Heffer: (1963). [Google Scholar]
- Hadad B., Maurer D., Lewis T. L. Sparing of sensitivity to biological motion but not of global motion after early visual deprivation. Developmental Science. (2012);15:474–481. doi: 10.1111/j.1467-7687.2012.01145.x. [DOI] [PubMed] [Google Scholar]
- Kremláček J., Šikl R., Kuba M., Szanyi J., Kubová Z., Langrová J., Stodůlka P. Spared cognitive processing of visual oddballs despite delayed visual evoked potentials in patient with partial recovery of vision after 53 years of blindness. Vision Research. (2013);81:1–5. doi: 10.1016/j.visres.2012.12.013. [DOI] [PubMed] [Google Scholar]
- Le Grand R., Mondloch C., Maurer D., Brent H. P. Early visual experience and face processing. Nature. (2001);410:890. doi: 10.1038/35073749. [DOI] [PubMed] [Google Scholar]
- Le Grand R., Mondloch C., Maurer D., Brent H. P. Impairment in holistic face processing following early visual deprivation. Psychological Science. (2004);15:762–768. doi: 10.1111/j.0956-7976.2004.00753.x. [DOI] [PubMed] [Google Scholar]
- Lewis T. L., Maurer D. Multiple sensitive periods in human visual development: Evidence from visually deprived children. Developmental Psychobiology. (2005);46:163–183. doi: 10.1002/dev.20055. [DOI] [PubMed] [Google Scholar]
- Loomis J. M., Da Silva J. A., Fujita N., Fukusima S. S. Visual space perception and visually directed action. Journal of Experimental Psychology: Human Perception & Performance. (1992);18:906–921. doi: 10.1037/0096-1523.18.4.906. [DOI] [PubMed] [Google Scholar]
- Mäntyjärvi M., Laitinen T. Normal values for the Pelli–Robson contrast sensitivity test. Journal of Cataract and Refractive Surgery. (2001);27:261–266. doi: 10.1016/S0886-3350(00)00562-9. [DOI] [PubMed] [Google Scholar]
- Maurer D., Le Grand R., Mondloch C. The many faces of configural processing. Trends in Cognitive Sciences. (2002);6:255–260. doi: 10.1016/S1364-6613(02)01903-4. [DOI] [PubMed] [Google Scholar]
- Ostrovsky Y., Andalman A., Sinha P. Vision following extended congenital blindness. Psychological Science. (2006);17:1009–1014. doi: 10.1111/j.1467-9280.2006.01827.x. [DOI] [PubMed] [Google Scholar]
- Ostrovsky Y., Meyers E., Ganesh S., Mathur U., Sinha P. Visual parsing after recovery from blindness. Psychological Science. (2009);20:1467–1491. doi: 10.1111/j.1467-9280.2009.02471.x. [DOI] [PubMed] [Google Scholar]
- Pelli D. G., Robson J. G., Wilkins A. J. The design of a new letter chart for measuring contrast sensitivity. Clinical Vision Sciences. (1988);2(3):187–199. [Google Scholar]
- Sacks O. An anthropologist on Mars. New York: Vintage Books; (1995). To see and not see; pp. 108–152. (pp. [Google Scholar]
- Sadr J., Sinha P. Exploring object perception with random image structure evolution. MIT Artificial Intelligence Laboratory Memo. (2001) No. 2001–6. [Google Scholar]
- Sadr J., Sinha P. Object recognition and random image structure evolution. Cognitive Science. (2004);28:259–287. doi: 10.1016/j.cogsci.2003.09.003. [DOI] [Google Scholar]
- Sloper J. J., Collins A. D. Delayed visual evoked potentials in adults after monocular visual deprivation by a dense cataract. Investigative Ophthalmology & Visual Science. (1995);36:2662–2671. [PubMed] [Google Scholar]
- Thaiss L., de Bleser R. Visual agnosia: A case of reduced attentional “spotlight”? Cortex. (1992);28(4):601–621. doi: 10.1016/s0010-9452(13)80230-4. [DOI] [PubMed] [Google Scholar]
- Valvo A. New York: American Foundation for the Blind; (1971). Sight restoration after long-term blindness: The problems and behavior patterns of visual rehabilitation. [Google Scholar]
- Wagner M. The metric of visual space. Perception & Psychophysics. (1985);38:483–495. doi: 10.3758/BF03207058. [DOI] [PubMed] [Google Scholar]