

Abstract
For a growing number of tumors the BRAF V600E mutation carries therapeutic relevance. In histiocytic proliferations the distribution of BRAF mutations and their relevance has not been clarified. Here we present a retrospective genotyping study and a prospective observational study of a patient treated with a BRAF inhibitor.
Genotyping of 69 histiocytic lesions revealed that 23/48 Langerhans cell lesions were BRAF-V600E-mutant whereas all non-Langerhans cell lesions (including dendritic cell sarcoma, juvenile xanthogranuloma, Rosai-Dorfman disease, and granular cell tumor) were wild-type. A metareview of 29 publications showed an overall mutation frequency of 48.5%; and with N=653 samples, this frequency is well defined. The BRAF mutation status cannot be predicted based on clinical parameters and outcome analysis showed no difference. Genotyping identified a 45 year-old woman with an aggressive and treatment-refractory, ultrastructurally confirmed systemic BRAF-mutant LCH. Prior treatments included glucocorticoid/vinblastine and cladribine-monotherapy. Treatment with vemurafenib over 3 months resulted in a dramatic metabolic response by FDG-PET and stable radiographic disease; the patient experienced progression after 6 months.
In conclusion, BRAF mutations in histiocytic proliferations are restricted to lesions of the Langerhans-cell type. While for most LCH-patients efficient therapies are available, patients with BRAF mutations may benefit from the BRAF inhibitor vemurafenib.
Keywords: Langerhans, Biomarker, Erdheim-Chester, V600E
INTRODUCTION
Histiocytic tumors are derived from the mononuclear-phagocytic and histiocyte system[1-3]. The clinical manifestations of the currently recognized disease entities are highly variable and range from benign localized lesions to highly aggressive systemic diseases[4]. A distinction between lesions that share surface markers of Langerhans cells (LCH-like lesions) from those that carry other surface markers of the histiocytic or dendritic cell lineage has been adopted[1]. Briefly, the latter group is composed of various entities that can be summarized as non-LCH-type tumors and is reviewed elsewhere[1, 5]. Due to the lack of robust evidence from randomized controlled clinical trials, therapeutic strategies currently rely on precise histotyping as well as disease classification by involved system[6]. For example, therapeutic regimens for patients with systemic involvement include radiation and/or chemotherapy and, more recently, early evidence for molecular targeted approaches[7-9].
In 2010 BRAF mutations have been described in a significant number of LCH patients[10]. The biological role of BRAF mutations at that time was seen as an oncogenic driver leading to constitutive activation of the RAS/RAF pathway[11-13]. Notably, recent trials (e.g. in melanoma) indicate that pharmacological interference using second-generation BRAF inhibitors produces sustained tumor regressions[14, 15]. Although the original study from 2010 described BRAF V600E mutations in 57% of LCH patients, it is only now that this finding received the appropriate level of attention and several other groups confirmed it (Figure 1). The specific diagnostic value of BRAF mutations in LCH has still not been thoroughly determined. As for now there is no statistical evidence that the BRAF mutation correlates with affected site or outcome[10, 16-18]. A dramatic response to targeted BRAF inhibition in three patients with refractory Erdheim-Chester has been reported[18], implying therapeutic relevance although data in classic LCH and confirmation by an independent group are currently lacking.
Figure 1. Metareview of Reported Mutation Frequencies and our BRAF Genotyping Results in Langerhans cell histiocytosis.
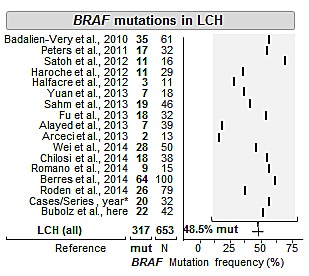
*A total of 13 case reports/series are summarized (see methods). Abbreviations: LCH, Langerhans cell histiocytosis; mut., mutated; N, number of tested samples. In the summary line, the average of all studies is provided along with the 95% confidence interval assuming a binomial distribution for all included cases (line).
We performed a study consisting of three parts: a) a literature review of BRAF mutations in LCH, b) a retrospective genotyping study in a series of histiocytic tumors. The identified patients were screened for being refractory to established treatment regimens and we additionally report c) the prospectively observed transient response to the targeted BRAF inhibitor vemurafenib in one patient. Our data indicate that BRAF mutation testing of tumor tissue should be carried out in LCH patients refractory to conventional treatment to identify those patients that may benefit from the salvage therapeutic option of BRAF inhibition.
RESULTS
Mutation analysis was performed in 69 patient samples and genotyping results by histological subtype are summarized in Table 1. We found no BRAF mutations in the 21 tested non-Langerhans cell lesions. Briefly, by histological subtype, our findings in juvenile xanthogranuloma and Rosai-Dorfman disease are in accord with a prior report[19]. We also genotyped three follicular dendritic cell tumors that were wild-type, which has not been previously examined; however, a BRAF V600E mutant interdigitating dendritic cell sarcoma has been recently reported[20]. The additionally tested granular cell tumors were all wild-type, which has to our knowledge not been previously examined.
Table 1. Results of BRAF Genotyping by Histological Subtype.
| Histological subtype | Total | BRAFV600E | |
|---|---|---|---|
| N=69 | No. | % | |
| Tumors derived from Langerhans cells | 48 | 23 | 48 |
| Langerhans cell histiocytosis | 42 | 22 | 52 |
| Solitary/unifocal | 25 | 12 | 48 |
| Multi-system | 13 | 7 | 54 |
| Disseminated/visceral | 4 | 3 | 75 |
| Langerhans cell sarcoma | 6 | 1 | 17 |
| Tested Non-Langerhans cell entities | 21 | 0 | 0 |
| Dendritic cell sarcoma | 3 | 0 | 0 |
| Juvenile Xanthogranuloma | 3 | 0 | 0 |
| Rosai-Dorfman Disease | 4 | 0 | 0 |
| Granular Cell Tumor | 11 | 0 | 0 |
Abbreviations: N, number of cases, No., number of mutated cases.
Genotyping in the 48 patient-samples with Langerhans cell-derived lesions identified a total of 23 BRAF V600E mutations (=47.9%). Comparison of detection rates with our literature meta-review findings demonstrated that our detection rate is in line with prior reports and our cohort representative. With over 600 tested cases, enough cases have been reported and the mutation frequency of 48.5% (95% confidence interval: 44.7-52.5%) can now be considered well-defined (Figure 1). Although BRAF variant mutations in LCH have been reported (e.g., V600D)[21], we did not observe such variant mutations in our series. The fractions of mutant LCH-cases were relatively constant between different histological subtypes; however, we noted two exceptions. First, of the 6 tested Langerhans sarcomas we found only one BRAF V600E mutation in a 71 year-old male who died 3 months after diagnosis (Figure 2a). Second, we found BRAF mutations in all 4 tested solitary cutaneous LCHs. Despite the small number of tested samples, these findings raise the question whether the BRAF mutation status can distinguish between solitary and multiple-site or systemic disease.
Figure 2. BRAF Mutation Analysis at the Case Level and Correlation with Tumor Cell Density and Event Rate in Non-Responders.
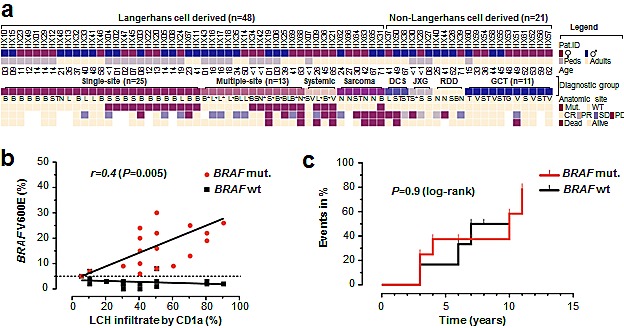
a. Key clinicopathological features of individual patients along with genotyping result and coded outcome data. Samples displayed as columns and arranged by disease entity, BRAF mutation status and age. b. Correlation of histiocytic infiltrate (as determined by CD1a staining) with peak-height quantification from pyrosequencing in 19 BRAF V600E mutant and 19 wild-type LCH cases. c. Stacked cumulative event rate (stable disease, recurrence, progression) in patients with multi-site or multi-system disease according to the BRAF mutation status. Abbreviations: *, multiple sites; +, central nervous system/additional organ involved; B, bone; BS, bone and skin; CR, complete response, DCS, dendritic cell sarcoma; JXG, juvenile xanthogranuloma; G, genital; GCT, granular cell tumor; L, lung; LCH, Langerhans cell histiocytosis; N, lymph node; PD, progressive disease; PR, partial response; RDD, Rosai-Dorfman, disease; S, skin; SD, stable disease; ST, soft-tissue; T, tongue; V, visceral.
To explore the diagnostic value of BRAF genotyping in LCH, we were interested whether quantification of mutant peak heights (by pyrosequencing) can function as a surrogate marker for the estimation of histiocytic infiltrates. We found significant correlation between mutant peak heights and CD1a staining (Figure 2b); thus indicating a robust relationship between total mutated allele content and CD1a-positive infiltrate. Additional diagnostic value may be related to the clinicopathological phenotype; however, we failed to detect significant associations with age, sex, ‘stage’ (i.e. system involvement) or affected organ/site (Table 2). To corroborate these findings we also re-tested the diagnostic distinction for skin, bone, and lung lesions based on BRAF genotype and found no significant associations (Table 2). For example when confronted with a LCH in a lung biopsy, we tested whether the BRAF status can distinguish between local vs. systemic disease. Comparison of our 7 lung samples from patients with systemic involvement vs. 4 ‘lung-only’ cases showed that there was a slightly higher mutation frequency in systemic (2 of 7 = 28.6%) vs. localized cases (1 of 4 = 25%); however, these differences did not reach statistical significance (P=1.00; Fisher's). Collectively, these findings suggest a limited value of BRAF testing to separate single-site from multi-site or multi-system LCH.
Table 2. Demographic and Clinical Characteristics of Genotype-Specific Subsets of Patients with Langerhans cell Histiocytosis.
|
BRAF mutated (n=22) |
BRAF Wild-type (n=20) |
P | |||
|---|---|---|---|---|---|
| Characteristic | No. | % | No. | % | |
| Age, years | |||||
| Median | 13 | 15 | 0.68 | ||
| Range | 0.6-65 | 0.6-57 | |||
| Sex | |||||
| Male | 10 | 45 | 12 | 60 | 0.37 |
| Female | 12 | 55 | 8 | 40 | |
| Stage | |||||
| Single-System | 12 | 55 | 13 | 65 | 0.54 |
| Multi-System | 10 | 45 | 7 | 35 | |
| Affected Site | |||||
| Bone (n=23) | |||||
| Solitary (n=17) | 9 | 53 | 8 | 47 | 0.66 |
| Multi (n=6) | 4 | 67 | 2 | 33 | |
| Lung (n=11) | |||||
| Solitary (n=4) | 1 | 25 | 3 | 75 | 1.0 |
| Multi (n=7) | 2 | 29 | 5 | 71 | |
| Skin (n=6) | |||||
| Solitary (n=4) | 4 | 100 | 0 | 0 | 0.33 |
| Multi (n=2) | 1 | 50 | 1 | 50 |
Abbreviations: n=total number of cases; No., number of cases per characteristic; P-values derived from contingency testing (t-test for age; Fisher's exact test for dichotomous factors); solitary, represents single-site involvement; multi, represents multi-system disease; Note: in the „affected site“ part of the table, percentages represent the fraction of mutated or wild-type cases in each category (line-wise comparisons).
Given the relatively high rate of BRAF mutations in multi-system LCH – for example with bone involvement (n=4/6=66.6%), the mutation status may hold prognostic information. Therefore, we compared overall and progression free survival between BRAF wild-type and mutant patients; however, found no significant difference (P=0.68 PFS; P=0.37 OS; log-rank). In addition, we examined whether the BRAF mutation status can distinguish between responders and non-responders. In the 18 mutant cases with outcome information, we found 12 non-responders (66.6%) whereas there were 5 non-responders among the 15 wild-type cases with outcome information (33.3%); however, this difference did not reach significance (P=0.084; Fisher's exact). Thus, the BRAF mutation status does not allow stratification of either responders or non-responders; at least not in our cohort. In addition, we examined whether the BRAF mutation status is associated with a different time course of events (e.g. progress, recurrence) in the non-responder subgroup. Event plots show no difference in the time course when non-responders were separated according to genotype (Figure 2c). Together, our outcome analysis indicates that the BRAF mutation status holds –at this point– no prognostic information.
Due to the compelling rate of BRAF mutations in LCH, we started BRAF testing in therapy refractory LCH patients as a prospective observational study component. At time of review, 10 of the 17 non-responders were lost to follow up, 4 had died and only 3 non-responders were alive, and required additional treatment. Two of the three patients were children (one BRAF mutant; who received second-line chemotherapy) and the third patient was a 45-year-old woman with multifocal and multisystemic BRAF V600E mutant Langerhans cell histiocytosis with multiple bone lesions (Patient HX36). Diagnosis in patient HX36 was established via histology and determination of the typical immunophenotype. The patient also had orbital and meningeal lesions and infiltration of the pituitary gland and hypothalamus without diabetes insipidus. The patient also had a severe insulin-dependent diabetes mellitus with normal cortisol and ACTH-levels. Given the high similarity of affected sites in our patient to the previously reported patients with Erdheim Chester disease[18] we performed electron microscopic analysis (Figure 3b, 3c) and found Birbeck granules in ultrastructural examination thereby corroborating the diagnosis of Langerhans cell histiocytosis. Consequently, the woman was treated with glucocorticoids (prednisolone up to 1mg/kg) and vinblastine (for one month; repeated 4 months later), which was not tolerated due to aggravation of the diabetes mellitus, and which resulted in a progressive disease with new intracranial and meningeal manifestations. Therapy was switched to cladribine monotherapy (2,1mg/m² day 1-5; 2 cycles; for three months), which again resulted in progressive disease with new intracranial lesions. Therefore, we decided to start off-label use of vemurafenib with escalating doses over time (240mg once daily for one week, 240mg twice daily for 5 weeks and 240mg four times a day for another 6 weeks). Overall, treatment was well tolerated. Skin examinations were performed during and after the treatment. The patient had a reduced need for analgesics for the bone lesions, and a slightly lower need for insulin. After 6 weeks (at the lower dosage of 2x 240mg daily), the patient displayed an almost complete metabolic remission in the FDG-PET, without significant reduction of the size of measurable lesions (e.g. hypophyseal-hypothalamic infiltration). After 3 months, the patient still had stable disease according to RECIST criteria with a continued, dramatic metabolic response (Figure 4). Due to a lack of published data, the off-label use had to be discontinued and 6 months later, the patient had progressive disease.
Figure 3. Histology, Immunophenotype and Ultrastructural Findings in Patient HX 36.
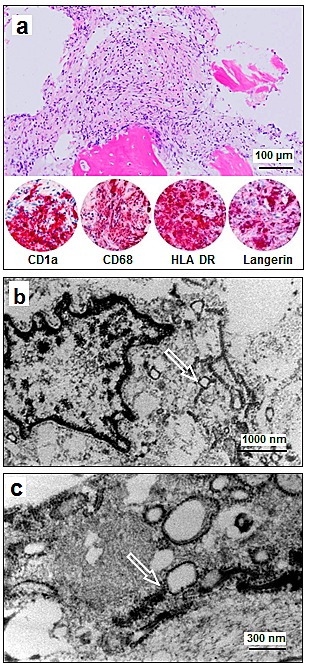
a. Bone marrow biopsy sample shows a dense histiocytic infiltrate with reactive resorption of trabecular bone and replacement of the bone marrow. Morphology and immunophenotype (selected images of the immunophenotype are provided) are diagnostic of LCH (H&E and alkaline phosphatase immunohistochemistry). b: Ultrastructural examination of the histiocytic infiltrate shows lobulated nuclei with open chromatin, lack of prominent nucleoli, and tennis-racket shaped cytoplasmatic Birbeck granules (arrow). c: Ultra high magnification of Birbeck granules shows the rod shaped electron dense configuration and reveal vacuolated blebs, diagnostic of LCH (arrow).
Figure 4. Response of LCH to the BRAF Inhibitor Vemurafenib.
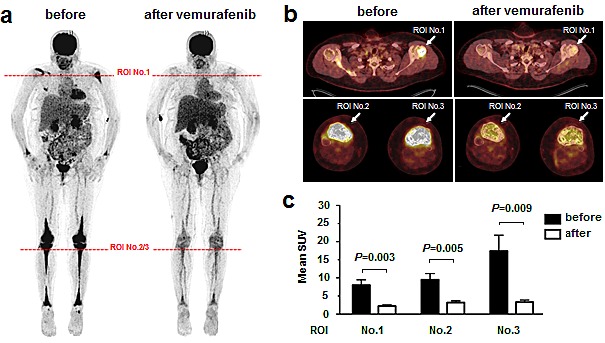
Shown are images pretreatment and after 6 weeks. a: Pretreatment FDG-PET maximum intensity projection (MIP) images before and after 6 weeks of treatment with vemurafenib 240mg/day for 1 week and vemurafenib 480mg/day for 5 weeks. Horizontal lines at full body scan indicate planes for humoral head and tibia plateau cross sections. b. PET-CT fusion images of humoral head and tibia plateau. Arrows indicate region of interest (ROI). c. Quantitative comparison of mean standardized uptake values (+/− standard deviation); P-values from unpaired t-test.
DISCUSSION
In our analysis, BRAF V600E mutations in histiocytic proliferations are restricted to tumors of the Langerhans cell lineage. Of the few refractory patients we identified a patient with a BRAF mutant LCH who had a transient clinical response to the targeted BRAF inhibitor vemurafenib.
The frequency of BRAF mutations in LCH approximates 50% (Figure 1) and raises the question how these genetically distinct tumors differ from LCH wild-type tumors. To this end we performed phenotype comparisons (Table 2); however, with two exceptions we failed to identify distinctive features. These exceptions were: the presence of BRAF mutations in all solitary skin LCHs and a somewhat lower rate of BRAF mutations in Langerhans cell sarcomas (17%). Due to the small number of tested samples in these categories, we abstain from speculations; however, would like to point out two aspects of these orphan-diseases. First, our BRAF mutated Langerhans cell sarcoma patient had died; therefore, given the rarity and aggressiveness of this disease the potential of targeting BRAF mutations should not be ignored. Second, the distinction of localized vs. multi-system disease remains a diagnostic challenge[22]. In particular, in the setting of a histiocytic lung lesion we assessed the value of the BRAF mutation status as a diagnostic biomarker but did not succeed in finding a statistical difference between mutated and wild-type cases. Similarly, the mutation frequency with respect to the involved system did not show any differences. In conjunction with the available literature, our findings indicate that neoplastic lesions related to LCH (e.g., Erdheim-Chester disease)[19, 23] also harbor BRAF mutations. Nonetheless, the specific diagnostic value of BRAF in LCH seems not as straightforward as for example in hairy cell leukemia[24]; although very recent evidence suggests distinct subtypes of Langerhans cell histiocytosis depending on the presence or absence of circulating dendritic cells[16], which could be used for therapeutic monitoring. However, there is currently no convincing evidence that the BRAF status by itself has value as a prognostic biomarker; at least not in our series of non-responders (Figure 2c). Given recent data describing somatic activating ARAF mutations in BRAF wild-type LCH[25], it is expected that the advents of novel sequencing technologies will lead to a more comprehensive delineation of the mutational landscape in LCH.
Finally, the therapeutic relevance of BRAF mutations in LCH has not been clarified and may differ between tumor types. Here we add the transient response of one LCH patient who demonstrated at least partial metabolic response. Besides adding this case as proof of principle in LCH, there are three issues worth noting. First, despite the classical histological, immunophenotypic and ultrastructural findings (that were all diagnostic of LCH), the clinical presentation and distribution of the disease is highly similar –if not identical– to a patient with Erdheim-Chester disease reported by Haroche et al.,[18]. Second, while the formal criteria for a radiographic partial response (by RECIST) were not met, achieving a transient response in such an aggressive version of LCH is striking and we find the metabolic response at least noteworthy (Figure 4). The similarities of our data and those from xenograft models are impressive[26] and indicate a metabolic function of mutant-BRAF in histiocytic neoplasia[26-31]. We interpret the stable radiographic disease as an apparent lack of ‘oncogenic shock’[32, 33]. Third, from an academic perspective, a re-biopsy would have been interesting; however, clinically this was not indicated and the location of lesions was considered “high-risk” (e.g. intracranial). Collectively, the efficacy of vemurafenib beyond melanoma[34], for example in Erdheim-Chester Disease[18] and our data argue for ongoing exploration of the therapeutic value of BRAF mutations in LCH.
In summary, BRAF mutations in histiocytic proliferations are restricted to those of the Langerhans cell-type and our metareview establishes the BRAF mutation frequency of 48.5%. In addition, for the vast majority of LCH-patients efficient therapeutic options are available; however, for treatment refractory patients with lesions harboring the BRAF V600E mutation, targeted BRAF inhibition may represent a therapeutic option.
MATERIAL AND METHODS
Design and Ethical Approval
The retrospective part of the study was conducted as an anonymized case- and specimen review via the Comprehensive Cancer Center Ulm (CCCU). The prospective interventional study in one patient included informed consent for experimental off-label drug treatment. All experiments were performed in accordance with the ethical standards of the local ethics committee and with the Declaration of Helsinki.
Study Cohort, Tissue Sections, Diagnostic Criteria
We searched the pathology- and the hospital information systems using diagnostic terms and ICD-O codes. After removal of duplicates, samples with tissue available for molecular genetic analysis were reviewed. Atleast two board-certified pathologists confirmed each primary diagnosis by review of original sections and immunohistochemical stains. Diagnostic criteria followed the 2008 WHO guidelines.
Microdissection and DNA extraction
Regions for microdissection were identified by immunohistochemistry and H&E stains. The tumor regions were either sectioned (at 2-5μm thickness) and microdissected, or cored using a 2 mm dermal punch-biopsy needle. After deparaffinization and DNA extraction, concentration was determined using an Ultrospec 2100pro (Amersham Biosciences; Upsala; Sweden).
Molecular Genetic Analysis
PCR-reactions using the primers: F-5'-TGC-TTG-CTC-TGA-TAG-GAA-AAT-G-3' and R-5'-AGC-ATC-TCA-GGG-CCA-AAA-AT-3', were followed by pyrosequencing [R-5-GAC-CCA-CTC-CAT-CGA-G-3; PyroMark Q24 (Qiagen, Hilden, Germany)] according to established protocols [35]. Alternatively, mutation analyses was performed using the BRAF 600/601 StripAssay (Vienna Labs, Vienna, Austria) according to the manufacturer's instructions. Mutations were validated using conventional Sanger sequencing.
Electron Microscopy
Electron Microscopy was performed according to established protocols [36]. Briefly, FFPE tissue was microdissected, deparaffinized and post-fixed overnight at 4°C in modified Karnovsky's fixative (3% glutaraldehyde in 1% paraformaldehyde in sodium cacodylate buffer at pH 7.4). After rinsing in sodium cacodylate buffer, samples were postfixed in phosphate cacodylate-buffered 21% OsO4 for 1h, dehydrated in graded ethanol with a final dehydration in propylene oxide, and embedded in epon (Electron Microscopy Sciences, Hatfield, PA). One-micron-thick plastic sections were examined by light microscopy after being stained with toluidine blue. Ultrathin sections (90 nm thick) were cut and mounted onto slot grids. Sections were poststained with uranyl acetate and lead citrate and viewed with an EM10 (Zeiss, Jena, Germany). Digital images were acquired using the TVIPS 1k system (TVIPS, Gauting, Germany).
Literature review
Two electronic databases (Medline, Scopus) were searched (Jan 1976 – Feb 2014) independently by three authors (AMB/SEW/JKL) using the search terms histiocy*, langerhans*, erdheim*, bone or lung in combination with BRAF or V600E. In addition, we performed review of reference lists in all selected articles to identify additional studies that contained BRAF mutational analysis. For each study [10, 16, 18, 19, 37-48], we noted histological subtype of the lesion, BRAF mutation status, and the total number of mutated and tested cases. We present the overall BRAF mutation frequency along with the 95% confidence interval assuming a binomial distribution for all included cases. For simplicity of display we summarized case reports and small series that contained less or equal to ten patients in one category (Figure 1) [19-21, 49-58].
Outcome and Statistical Analysis
Outcome analysis consisted of four elements: a) overall- and b) progression free survival defined as the time interval between diagnosis and death or recurrence/progression; c) we determined the fraction of responding and non-responding patients and d) determined the time course of the events in the non-responding subgroup. We defined non-responders as those patients with stable disease, progressive disease or relapse (‘events’) whereas patients with partial or complete response were considered responders. For a time to event analysis, we defined the timeframe from initial diagnosis to first event, which we plotted as stacked event curves that we compared by using a log-rank test. For statistical comparisons of mutation frequencies we used the Fisher's exact- or Chi-square test, age comparisons employed the student's t-test, and we considered P<0.05 as statistically significant.
Acknowledgments
We appreciated the support of all participating patients and families. We thank Peter Kuhn from the Comprehensive Cancer Center Ulm and Werner Kugler for administrative support. We thank Dr. Ulrike Kostezka, Julia Kiedaisch, Ywona Nerbas, Elena Moser, Elena Kelsch and Karola Dorsch for expert technical assistance. We thank Renate Kunz for expert technical help with electron microscopy. In addition we thank Dr. Gerstenmaier for help with genotyping. The Else-Kröner Foundation supports JKL.
Footnotes
AMB, AV, JKL conceived and designed the study; AMB, SEW, AA, KS, SB performed experiments; AMB, AA, KS, JKL analyzed mutations; AJB, MG performed PET-CT scans and SUV calculations; AMB, SEW, JKL performed the metareview of the literature; AMB, JKL performed statistical analyses; AMB, AS, SB, HC, AL, CW, IA, TFEB, PM, AV selected and contributed cases or clinical/outcome data; AMB and JKL wrote the initial version of the manuscript, AS, AA, KS, TFEB, AJB, PM, and AV revised, and all authors approved the final version.
The authors declare no competing financial interests.
REFERENCES
- 1.Pileri SA, Grogan TM, Harris NL, Banks P, Campo E, Chan JK, Favera RD, Delsol G, De Wolf-Peeters C, Falini B, Gascoyne RD, Gaulard P, Gatter KC, et al. Tumours of histiocytes and accessory dendritic cells: an immunohistochemical approach to classification from the International Lymphoma Study Group based on 61 cases. Histopathology. 2002;41(1):1–29. doi: 10.1046/j.1365-2559.2002.01418.x. [DOI] [PubMed] [Google Scholar]
- 2.Isaacson P, Jones DB, Sworn MJ, Wright DH. Malignant histiocytosis of the intestine: report of three cases with immunological and cytochemical analysis. J Clin Pathol. 1982;35(5):510–516. doi: 10.1136/jcp.35.5.510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Orfanos CE, Lammer D. [Reticulohistiocytic tumors of the skin. New concepts] Hautarzt. 1980;31(6):297–307. [PubMed] [Google Scholar]
- 4.Nezelof C, Basset F. Langerhans cell histiocytosis research. Past, present, and future. Hematol Oncol Clin North Am. 1998;12(2):385–406. doi: 10.1016/s0889-8588(05)70518-9. [DOI] [PubMed] [Google Scholar]
- 5.Chu T, D'Angio GJ, Favara BE, Ladisch S, Nesbit M, Pritchard J. Histiocytosis syndromes in children. Lancet. 1987;2(8549):41–42. doi: 10.1016/s0140-6736(87)93074-1. [DOI] [PubMed] [Google Scholar]
- 6.Howarth DM, Gilchrist GS, Mullan BP, Wiseman GA, Edmonson JH, Schomberg PJ. Langerhans cell histiocytosis: diagnosis, natural history, management, and outcome. Cancer. 1999;85(10):2278–2290. doi: 10.1002/(sici)1097-0142(19990515)85:10<2278::aid-cncr25>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 7.Willis B, Ablin A, Weinberg V, Zoger S, Wara WM, Matthay KK. Disease course and late sequelae of Langerhans' cell histiocytosis: 25-year experience at the University of California, San Francisco. J Clin Oncol. 1996;14(7):2073–2082. doi: 10.1200/JCO.1996.14.7.2073. [DOI] [PubMed] [Google Scholar]
- 8.Janku F, Amin HM, Yang D, Garrido-Laguna I, Trent JC, Kurzrock R. Response of histiocytoses to imatinib mesylate: fire to ashes. J Clin Oncol. 2010;28(31):e633–636. doi: 10.1200/JCO.2010.29.9073. [DOI] [PubMed] [Google Scholar]
- 9.Montella L, Insabato L, Palmieri G. Imatinib mesylate for cerebral Langerhans'-cell histiocytosis. N Engl J Med. 2004;351(10):1034–1035. doi: 10.1056/NEJM200409023511022. [DOI] [PubMed] [Google Scholar]
- 10.Badalian-Very G, Vergilio JA, Degar BA, MacConaill LE, Brandner B, Calicchio ML, Kuo FC, Ligon AH, Stevenson KE, Kehoe SM, Garraway LA, Hahn WC, Meyerson M, et al. Recurrent BRAF mutations in Langerhans cell histiocytosis. Blood. 2010;116(11):1919–1923. doi: 10.1182/blood-2010-04-279083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McCubrey JA, Steelman LS, Abrams SL, Lee JT, Chang F, Bertrand FE, Navolanic PM, Terrian DM, Franklin RA, D'Assoro AB, Salisbury JL, Mazzarino MC, Stivala F, et al. Roles of the RAF/MEK/ERK and PI3K/PTEN/AKT pathways in malignant transformation and drug resistance. Adv Enzyme Regul. 2006;46:249–279. doi: 10.1016/j.advenzreg.2006.01.004. [DOI] [PubMed] [Google Scholar]
- 12.Wong KK. Recent developments in anti-cancer agents targeting the Ras/Raf/MEK/ERK pathway. Recent Pat Anticancer Drug Discov. 2009;4(1):28–35. doi: 10.2174/157489209787002461. [DOI] [PubMed] [Google Scholar]
- 13.Hoeflich KP, Herter S, Tien J, Wong L, Berry L, Chan J, O'Brien C, Modrusan Z, Seshagiri S, Lackner M, Stern H, Choo E, Murray L, et al. Antitumor efficacy of the novel RAF inhibitor GDC-0879 is predicted by BRAFV600E mutational status and sustained extracellular signal-regulated kinase/mitogen-activated protein kinase pathway suppression. Cancer Res. 2009;69(7):3042–3051. doi: 10.1158/0008-5472.CAN-08-3563. [DOI] [PubMed] [Google Scholar]
- 14.Heakal Y, Kester M, Savage S. Vemurafenib (PLX4032): an orally available inhibitor of mutated BRAF for the treatment of metastatic melanoma. Ann Pharmacother. 2011;45(11):1399–1405. doi: 10.1345/aph.1Q363. [DOI] [PubMed] [Google Scholar]
- 15.Larkin J, Del Vecchio M, Ascierto PA, Krajsova I, Schachter J, Neyns B, Espinosa E, Garbe C, Sileni VC, Gogas H, Miller WH, Jr, Mandala M, Hospers GA, et al. Vemurafenib in patients with BRAF mutated metastatic melanoma: an open-label, multicentre, safety study. Lancet Oncol. 2014. [DOI] [PubMed]
- 16.Berres ML, Lim KP, Peters T, Price J, Takizawa H, Salmon H, Idoyaga J, Ruzo A, Lupo PJ, Hicks MJ, Shih A, Simko SJ, Abhyankar H, et al. BRAF-V600E expression in precursor versus differentiated dendritic cells defines clinically distinct LCH risk groups. J Exp Med. 2014. [DOI] [PMC free article] [PubMed]
- 17.Bubolz AM, Möller P, Lennerz JK. BRAF V600E mutationstatus in histiocytoses does not allow diagnostic distinction between pulmonary and systemic disease. Der Pathologe. 2013;34(S1):P96–97. [Google Scholar]
- 18.Haroche J, Cohen-Aubart F, Emile JF, Arnaud L, Maksud P, Charlotte F, Cluzel P, Drier A, Hervier B, Benameur N, Besnard S, Donadieu J, Amoura Z. Dramatic efficacy of vemurafenib in both multisystemic and refractory Erdheim-Chester disease and Langerhans cell histiocytosis harboring the BRAF V600E mutation. Blood. 2012;121(9):1495–1500. doi: 10.1182/blood-2012-07-446286. [DOI] [PubMed] [Google Scholar]
- 19.Haroche J, Charlotte F, Arnaud L, von Deimling A, Helias-Rodzewicz Z, Hervier B, Cohen-Aubart F, Launay D, Lesot A, Mokhtari K, Canioni D, Galmiche L, Rose C, et al. High prevalence of BRAF V600E mutations in Erdheim-Chester disease but not in other non-Langerhans cell histiocytoses. Blood. 2012;120(13):2700–2703. doi: 10.1182/blood-2012-05-430140. [DOI] [PubMed] [Google Scholar]
- 20.O'Malley DP, Kim YS, Vergilio JA, Chen ZW, Weiss LM. BRAF V600E Mutation Specific Immunohistochemistry Is a Rare Finding in Dendritic Cell- and Histiocyte-Derived Tumors Mod Pathol. 2014;27(S2):366A. doi: 10.3109/10428194.2014.946028. [DOI] [PubMed] [Google Scholar]
- 21.Kansal R, Quintanilla-Martinez L, Datta V, Lopategui J, Garshfield G, Nathwani BN. Identification of the V600D mutation in Exon 15 of the BRAF oncogene in congenital, benign langerhans cell histiocytosis. Genes Chromosomes Cancer. 2012;52(1):99–106. doi: 10.1002/gcc.22010. [DOI] [PubMed] [Google Scholar]
- 22.Kilpatrick SE, Wenger DE, Gilchrist GS, Shives TC, Wollan PC, Unni KK. Langerhans' cell histiocytosis (histiocytosis X) of bone. A clinicopathologic analysis of 263 pediatric and adult cases. Cancer. 1995;76(12):2471–2484. doi: 10.1002/1097-0142(19951215)76:12<2471::aid-cncr2820761211>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 23.Blombery P, Wong SQ, Lade S, Prince HM. Erdheim-Chester disease harboring the BRAF V600E mutation. J Clin Oncol. 2012;30(32):e331–332. doi: 10.1200/JCO.2012.43.2260. [DOI] [PubMed] [Google Scholar]
- 24.Tiacci E, Trifonov V, Schiavoni G, Holmes A, Kern W, Martelli MP, Pucciarini A, Bigerna B, Pacini R, Wells VA, Sportoletti P, Pettirossi V, Mannucci R, et al. BRAF mutations in hairy-cell leukemia. N Engl J Med. 2011;364(24):2305–2315. doi: 10.1056/NEJMoa1014209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nelson DS, Quispel W, Badalian-Very G, van Halteren AG, van den Bos C, Bovee JV, Tian SY, Van Hummelen P, Ducar M, Macconaill LE, Egeler RM, Rollins BJ. Somatic activating ARAF mutations in Langerhans cell histiocytosis. Blood. 2014. [DOI] [PubMed]
- 26.Sondergaard JN, Nazarian R, Wang Q, Guo D, Hsueh T, Mok S, Sazegar H, MacConaill LE, Barretina JG, Kehoe SM, Attar N, von Euw E, Zuckerman JE, et al. Differential sensitivity of melanoma cell lines with BRAFV600E mutation to the specific Raf inhibitor PLX4032. J Transl Med. 2010;8:39. doi: 10.1186/1479-5876-8-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Grabellus F, Worm K, Schmid KW, Sheu SY. The BRAF V600E mutation in papillary thyroid carcinoma is associated with glucose transporter 1 overexpression. Thyroid. 2012;22(4):377–382. doi: 10.1089/thy.2011.0401. [DOI] [PubMed] [Google Scholar]
- 28.Hall A, Meyle KD, Lange MK, Klima M, Sanderhoff M, Dahl C, Abildgaard C, Thorup K, Moghimi SM, Jensen PB, Bartek J, Guldberg P, Christensen C. Dysfunctional oxidative phosphorylation makes malignant melanoma cells addicted to glycolysis driven by the (V600E)BRAF oncogene. Oncotarget. 2013;4(4):584–599. doi: 10.18632/oncotarget.965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Haq R, Shoag J, Andreu-Perez P, Yokoyama S, Edelman H, Rowe GC, Frederick DT, Hurley AD, Nellore A, Kung AL, Wargo JA, Song JS, Fisher DE, et al. Oncogenic BRAF regulates oxidative metabolism via PGC1alpha and MITF. Cancer Cell. 2013;23(3):302–315. doi: 10.1016/j.ccr.2013.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Parmenter TJ, Kleinschmidt M, Kinross KM, Bond ST, Li J, Kaadige MR, Rao A, Sheppard KE, Hugo W, Pupo GM, Pearson RB, McGee SL, Long GV, et al. Response of BRAF-Mutant Melanoma to BRAF Inhibition Is Mediated by a Network of Transcriptional Regulators of Glycolysis. Cancer Discov. 2014;4(4):423–433. doi: 10.1158/2159-8290.CD-13-0440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sheu JJ, Guan B, Tsai FJ, Hsiao EY, Chen CM, Seruca R, Wang TL, Shih Ie M. Mutant BRAF induces DNA strand breaks, activates DNA damage response pathway, and up-regulates glucose transporter-1 in nontransformed epithelial cells. Am J Pathol. 2012;180(3):1179–1188. doi: 10.1016/j.ajpath.2011.11.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sharma SV, Fischbach MA, Haber DA, Settleman J. “Oncogenic shock”: explaining oncogene addiction through differential signal attenuation. Clin Cancer Res. 2006;12(14 Pt 2):4392s–4395s. doi: 10.1158/1078-0432.CCR-06-0096. [DOI] [PubMed] [Google Scholar]
- 33.Sharma SV, Bell DW, Settleman J, Haber DA. Epidermal growth factor receptor mutations in lung cancer. Nat Rev Cancer. 2007;7(3):169–181. doi: 10.1038/nrc2088. [DOI] [PubMed] [Google Scholar]
- 34.Heakal Y, Kester M, Savage S. Vemurafenib (PLX4032): an orally available inhibitor of mutated BRAF for the treatment of metastatic melanoma. Ann Pharmacother. 45(11):1399–1405. doi: 10.1345/aph.1Q363. [DOI] [PubMed] [Google Scholar]
- 35.Nagel PD, Feld FM, Weissinger SE, Stenzinger A, Moller P, Lennerz JK. Absence of BRAF and KRAS hotspot mutations in primary mediastinal B-cell lymphoma. Leuk Lymphoma. 2014. [DOI] [PubMed]
- 36.Lennerz JK, Hurov JB, White LS, Lewandowski KT, Prior JL, Planer GJ, Gereau RWt, Piwnica-Worms D, Schmidt RE, Piwnica-Worms H. Loss of Par-1a/MARK3/C-TAK1 kinase leads to reduced adiposity, resistance to hepatic steatosis, and defective gluconeogenesis. Mol Cell Biol. 2010;30(21):5043–5056. doi: 10.1128/MCB.01472-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Alayed K, Patel K, Zuo Z, Verma S, Cason R, Galbincea J, Luthra R, Medeiros L, Yin C. BRAF Mutation Occurs More Frequently in Pulmonary Langerhans Cell Histiocytosis and in Younger Patients. J Mol Diagn. 2013;15(6):858–859. [Google Scholar]
- 38.Arceci RJ, Allen CE, Dunkel I, Jacobsen ED, Whitlock J, Vassallo R, Borrello IM, Oliff A, Morris SR, Reedy BAM, Portnoy A, Smith DA, Noble B, et al. Evaluation Of Afuresertib, An Oral Pan-AKT Inhibitor, In Patients With Langerhans Cell Histiocytosis. Blood. 2013;122:2907. doi: 10.1002/pbc.26325. [DOI] [PubMed] [Google Scholar]
- 39.Chilosi M, Facchetti F, Calio A, Zamo A, Brunelli M, Martignoni G, Rossi A, Montagna L, Piccoli P, Dubini A, Tironi A, Tomassetti S, Poletti V, et al. Oncogene-induced senescence distinguishes indolent from aggressive forms of pulmonary and non-pulmonary Langerhans cell histiocytosis. Leuk Lymphoma. 2014. [DOI] [PubMed]
- 40.Fu B, Wang Z, Li X, Wang SA, Zuo Z. Detection of BRAF V600E Mutation in Langerhans Cell Histiocytosis Using High-resolution Melting Analysis in Decalcified, Paraffin-embedded Tissue. J Leuk. 2013;1:101. [Google Scholar]
- 41.Halfacre JA, Gale JM, Vasef MA. Analysis of BRAF V600E Mutation in Langerhans Cell Histiocytosis Using Pyrosequencing Technology. J Mol Diagn. 2012;14(6):660. [Google Scholar]
- 42.Peters TL, Price J, George R, Lim PH, Heym KM, Merad M, McClain KL, Allen CE. Frequent BRAF V600E Mutations Are Identified in CD207+ Cells in LCH Lesions, but BRAF Status does not Correlate with Clinical Presentation of Patients or Transcriptional Profiles of CD207+ Cells. ASH Meeting 2011. 2011. Poster 602.
- 43.Roden AC, Hu X, Kip S, Parrilla Castellar ER, Rumilla KM, Vrana JA, Vassallo R, Ryu JH, Yi ES. BRAF V600E Expression in Langerhans Cell Histiocytosis: Clinical and Immunohistochemical Study on 25 Pulmonary and 54 Extrapulmonary Cases. Am J Surg Pathol. 2014;38(4):548–551. doi: 10.1097/PAS.0000000000000129. [DOI] [PubMed] [Google Scholar]
- 44.Romano RC, Shon W, Fritche KL. BRAF V600E Immunohistochemistry in Cutaneous Langerhans Cell Histiocytosis. Mod Pathol. 2014;27(S2):142A. [Google Scholar]
- 45.Sahm F, Capper D, Preusser M, Meyer J, Stenzinger A, Lasitschka F, Berghoff AS, Habel A, Schneider M, Kulozik A, Anagnostopoulos I, Mullauer L, Mechtersheimer G, et al. BRAFV600E mutant protein is expressed in cells of variable maturation in Langerhans cell histiocytosis. Blood. 2012;120(12):e28–34. doi: 10.1182/blood-2012-06-429597. [DOI] [PubMed] [Google Scholar]
- 46.Satoh T, Smith A, Sarde A, Lu HC, Mian S, Trouillet C, Mufti G, Emile JF, Fraternali F, Donadieu J, Geissmann F. B-RAF mutant alleles associated with Langerhans cell histiocytosis, a granulomatous pediatric disease. PLoS One. 2012;7(4):e33891. doi: 10.1371/journal.pone.0033891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wei R, Wang Z, Li X, Shu Y, Fu B. Frequent mutation has no effect on tumor invasiveness in patients with Langerhans cell histiocytosis. Biomed Rep. 2014;1(3):365–368. doi: 10.3892/br.2013.62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Yuan J, Caponetti GC, Lytle D, Greiner TC. Detection of BRAF V600E Mutations in Langerhans Cell Histiocytosis by Pyrosequencing. Mod Pathol. 2013;26(S2):369A. [Google Scholar]
- 49.Yousem SA, Dacic S, Nikiforov YE, Nikiforova M. Pulmonary Langerhans cell histiocytosis: profiling of multifocal tumors using next-generation sequencing identifies concordant occurrence of BRAF V600E mutations. Chest. 2013;143(6):1679–1684. doi: 10.1378/chest.12-1917. [DOI] [PubMed] [Google Scholar]
- 50.West DS, Dogan A, Quint PS, Tricker-Klar ML, Porcher JC, Ketterling RP, Law ME, McPhail ED, Viswanatha DS, Kurtin PJ, Dao LN, Ritzer RD, Nowakowski GS, et al. Clonally related follicular lymphomas and Langerhans cell neoplasms: expanding the spectrum of transdifferentiation. Am J Surg Pathol. 2013;37(7):978–986. doi: 10.1097/PAS.0b013e318283099f. [DOI] [PubMed] [Google Scholar]
- 51.Bates SV, Lakshmanan A, Green AL, Terry J, Badalian-Very G, Rollins BJ, Fleck P, Aslam M, Degar BA. BRAF V600E-Positive Multisite Langerhans Cell Histiocytosis in a Preterm Neonate. AJP Rep. 2013;3(2):63–66. doi: 10.1055/s-0033-1338168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ducassou S, Seyrig F, Thomas C, Lambilliotte A, Marec-Berard P, Berger C, Plat G, Brugiere L, Ouache M, Barkaoui M, Armari-Alla C, Lutz P, Leverger G, et al. Thymus and mediastinal node involvement in childhood Langerhans cell histiocytosis: long-term follow-up from the French national cohort. Pediatr Blood Cancer. 2013;60(11):1759–1765. doi: 10.1002/pbc.24603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kamionek M, Welch M, Tomaszewicz K, Hutchinson L, Cosar EF, Dresser K, Fraire AE. BRAF Mutation Analysis in Pulmonary Langerhans Cell Histiocytosis. Mod Pathol. 2012;25(101):479A. [Google Scholar]
- 54.Milne P, Bigley V, McGovern N, Collin M. Revisiting the origin of Langerhans cell histiocytosis: mutated BRAF gene identifies potential circulating precursor cells. Abstract booklet, 13th International workshop on Langerhans Cells. 2013. Oct 10-13, 2013. p. 13.
- 55.Mitchell JM, Terrano D, Lee J, Alobeid B, Bhagat G, Mansukhani M, Remotti H. BRAF V600E Mutation in Langerhans Cell Histiocytosis of the Liver. Arch Pathol Lab Med. 2012;136:1024. [Google Scholar]
- 56.Sun F, Sun X, Zhen Z, Zhu J. Case report: Response to BRAF V600E Inhibitor Vemurafenib and Adoptive Immunotherapy in a Patient with Multisystemic and Refractory Langerhans Cell Histiocytosis. Pediatr Blood Cancer. 2013;60(S3):P152. [Google Scholar]
- 57.Yoon JH, Park HJ, Park SY, Park BK. Langerhans cell histiocytosis in non-twin siblings. Pediatr Int. 2013;55(3):e73–76. doi: 10.1111/ped.12034. [DOI] [PubMed] [Google Scholar]
- 58.Oishi N, Kondo T, Mochizuki K, Inoue T, Kasai K, Nakazawa T, Mitsumori T, Katoh R. Localized Langerhans cell histiocytosis of the thymus with BRAF V600E mutation: a case report with immunohistochemical and genetic analyses. Hum Pathol. 2014. ePub ahead of print. [DOI] [PubMed]