

Abstract
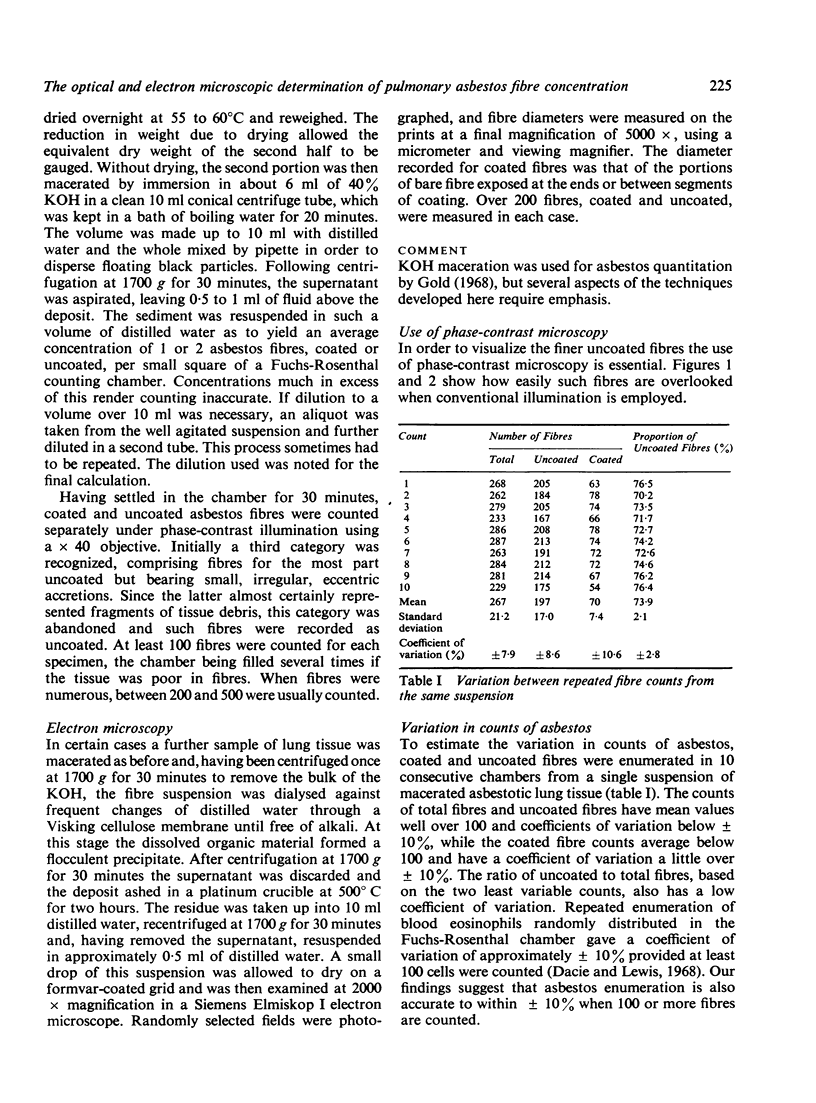
The quantitative extraction of asbestos fibres from asbestotic lung by alkali digestion has been refined by maceration of the tissue without prior drying, the minimum use of centrifugation, and the adoption of phase contrast microscopy. Preliminary experiments suggested that, using this technique, asbestos fibre counts were accurate to within at least ± 20% and in most instances to within ± 10%.
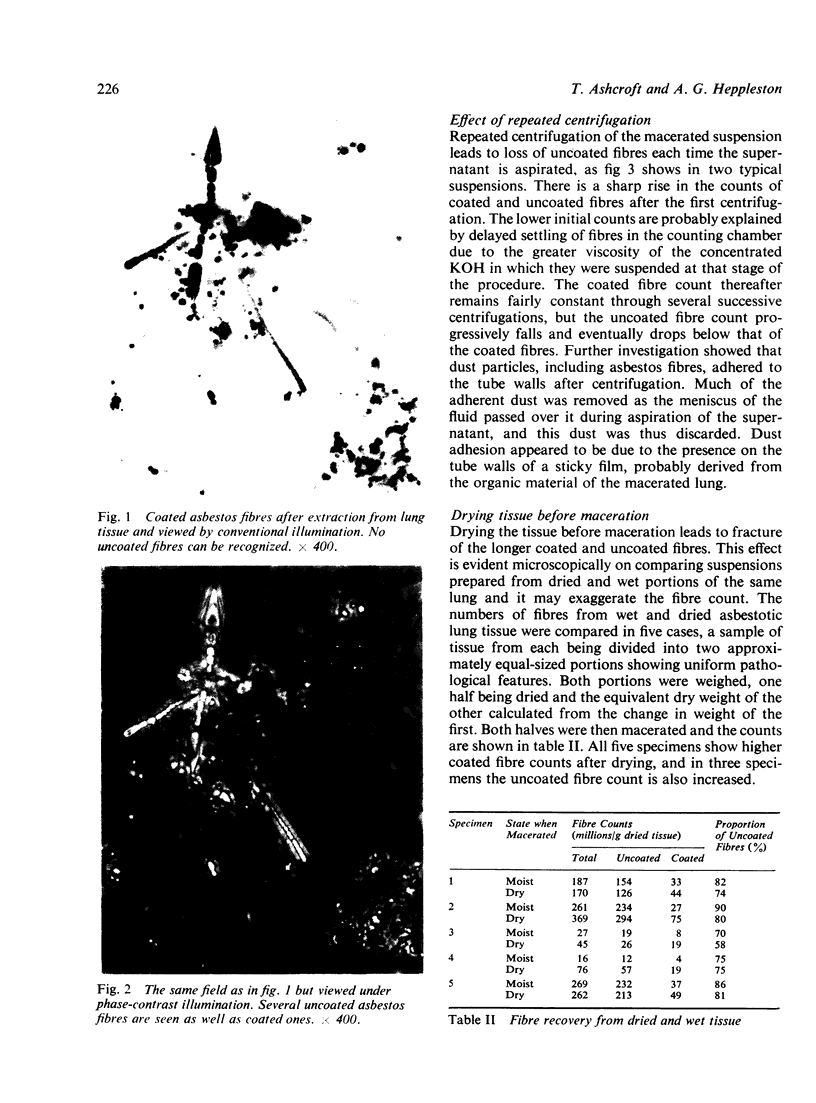
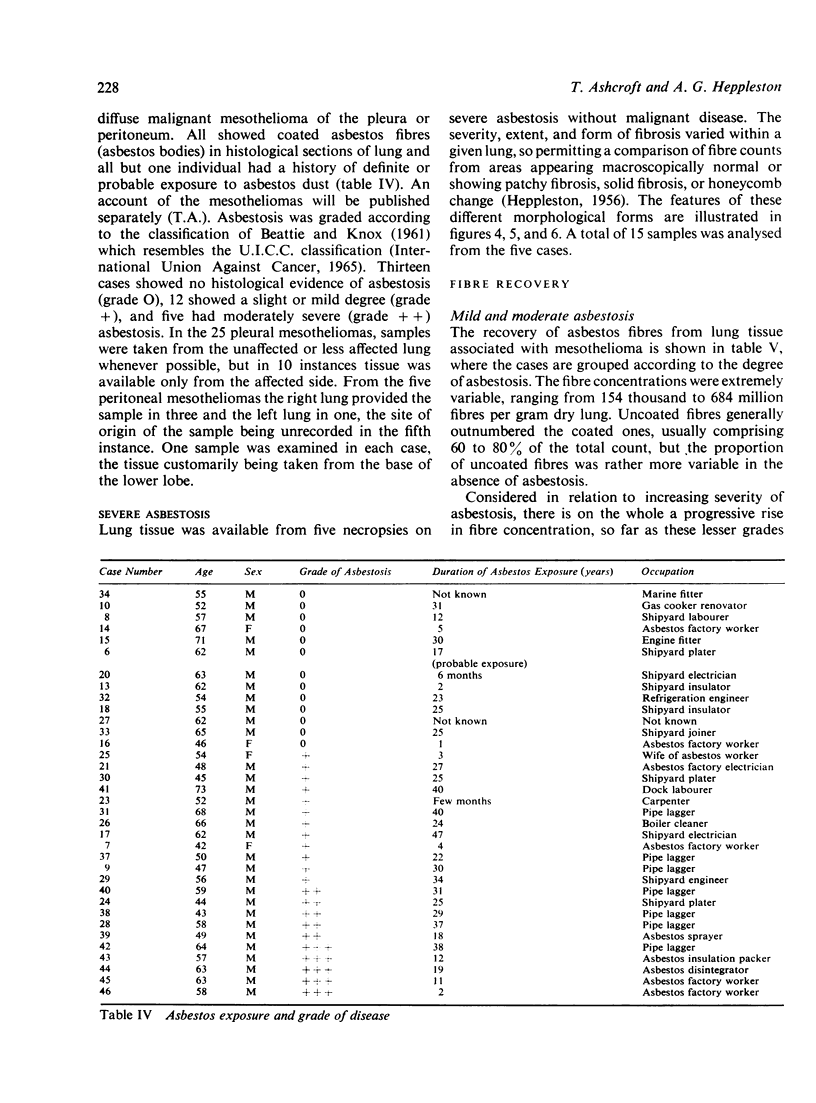
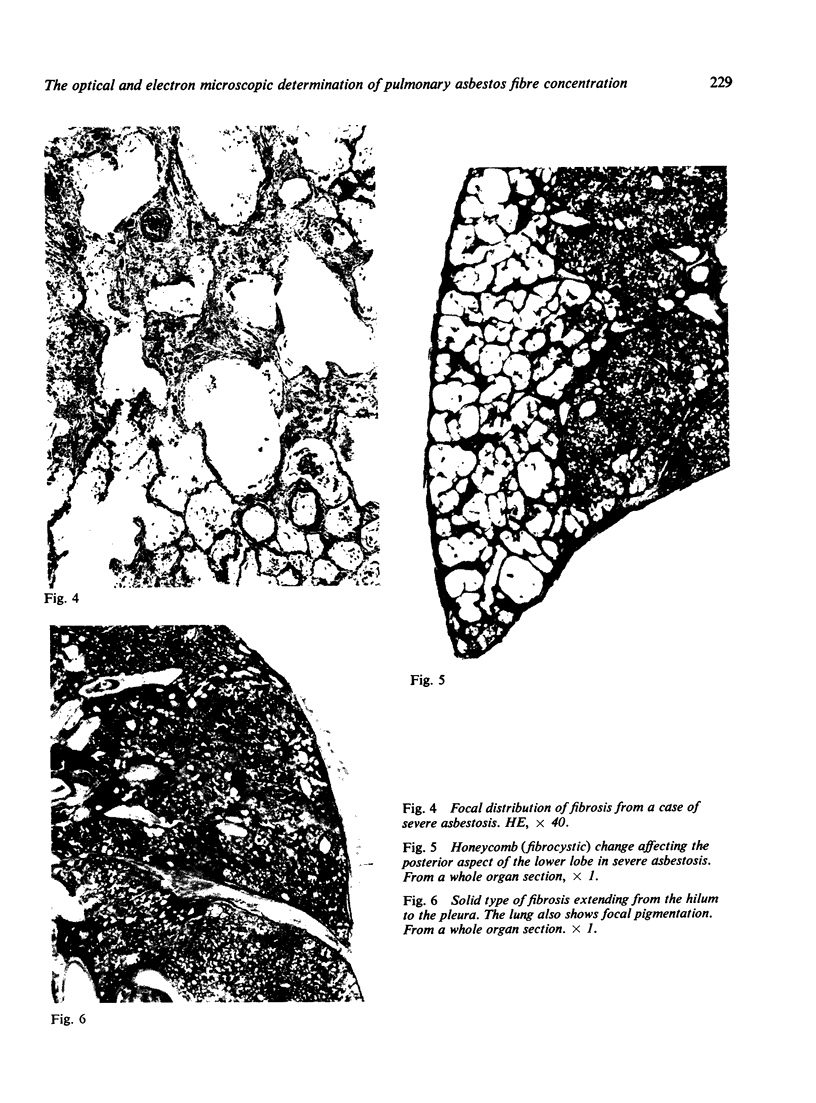
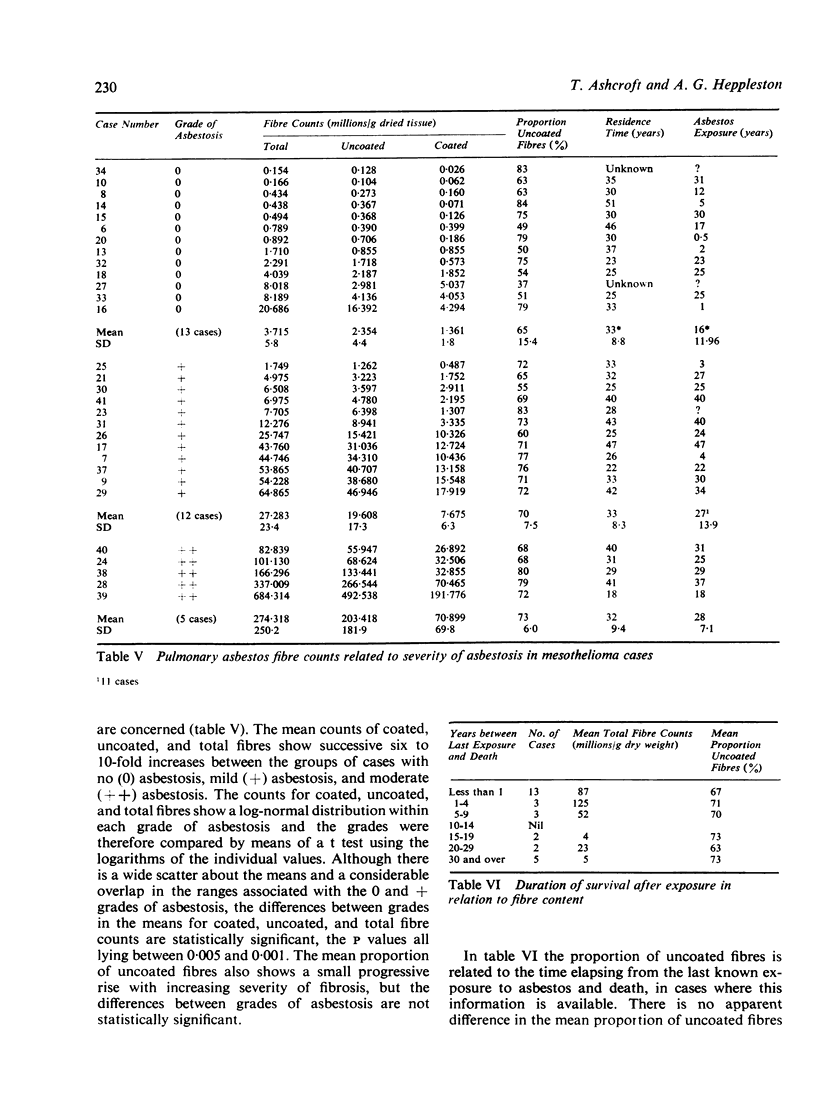
The method was used to assess asbestos concentrations in lung tissue showing various degrees and forms of fibrosis. The results, as determined by light microscopy, indicated that uncoated fibres generally outnumbered coated fibres. In mild and moderate asbestosis there was a progressive increase in concentration of asbestos fibres, both coated and uncoated, with increasing severity of fibrosis, whereas in severe asbestosis no correlation existed between the fibre concentration and the form or the extent of the pathological reaction. It is suggested that the severe fibrosis results from the supervention of non-specific inflammatory processes.
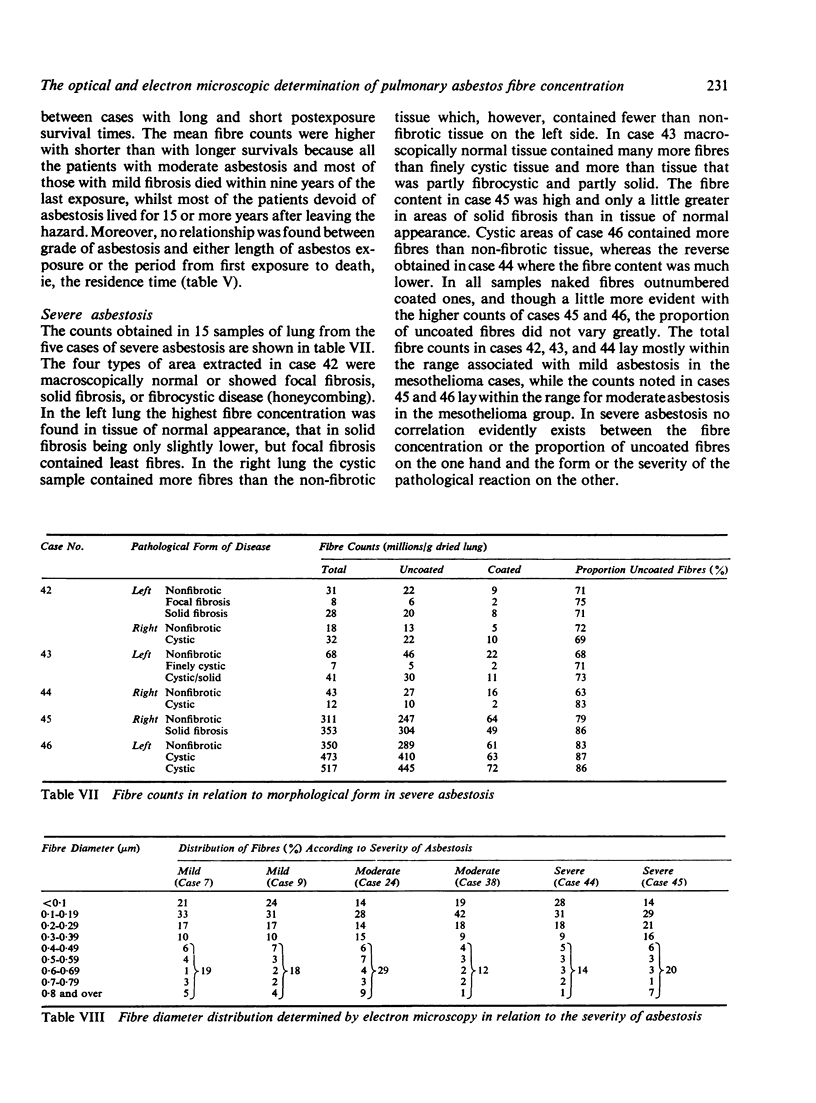
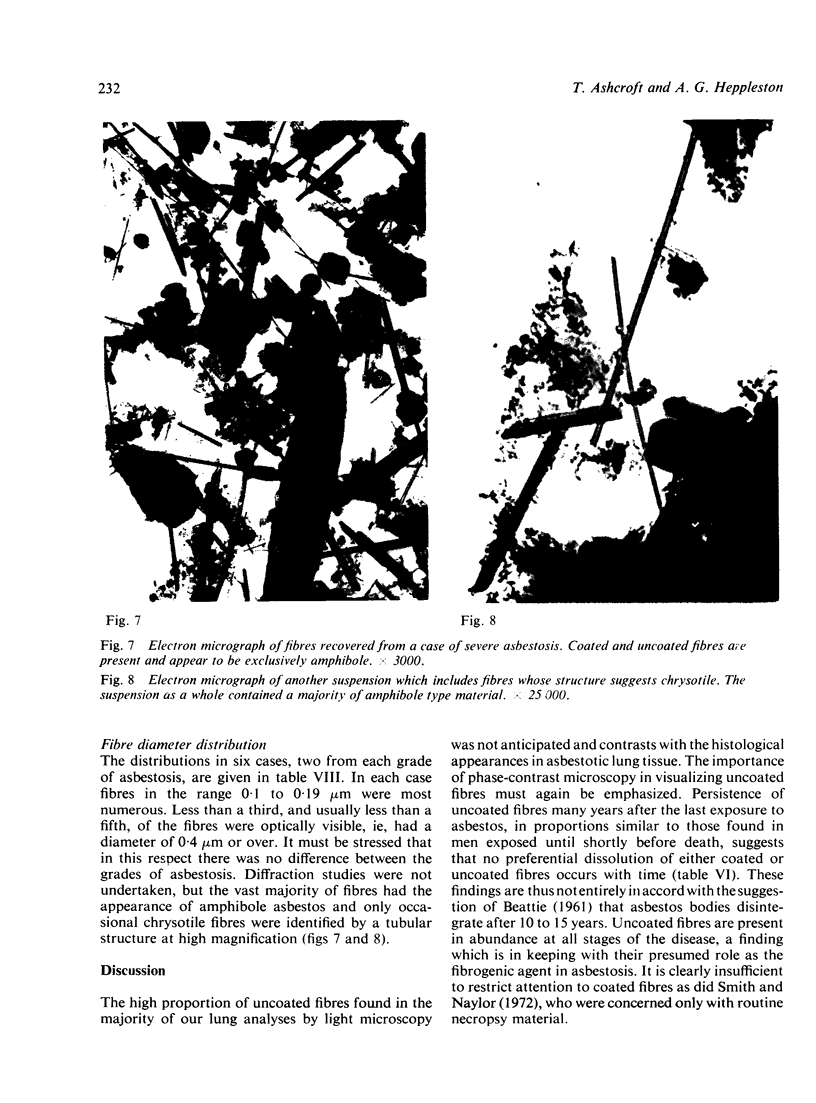
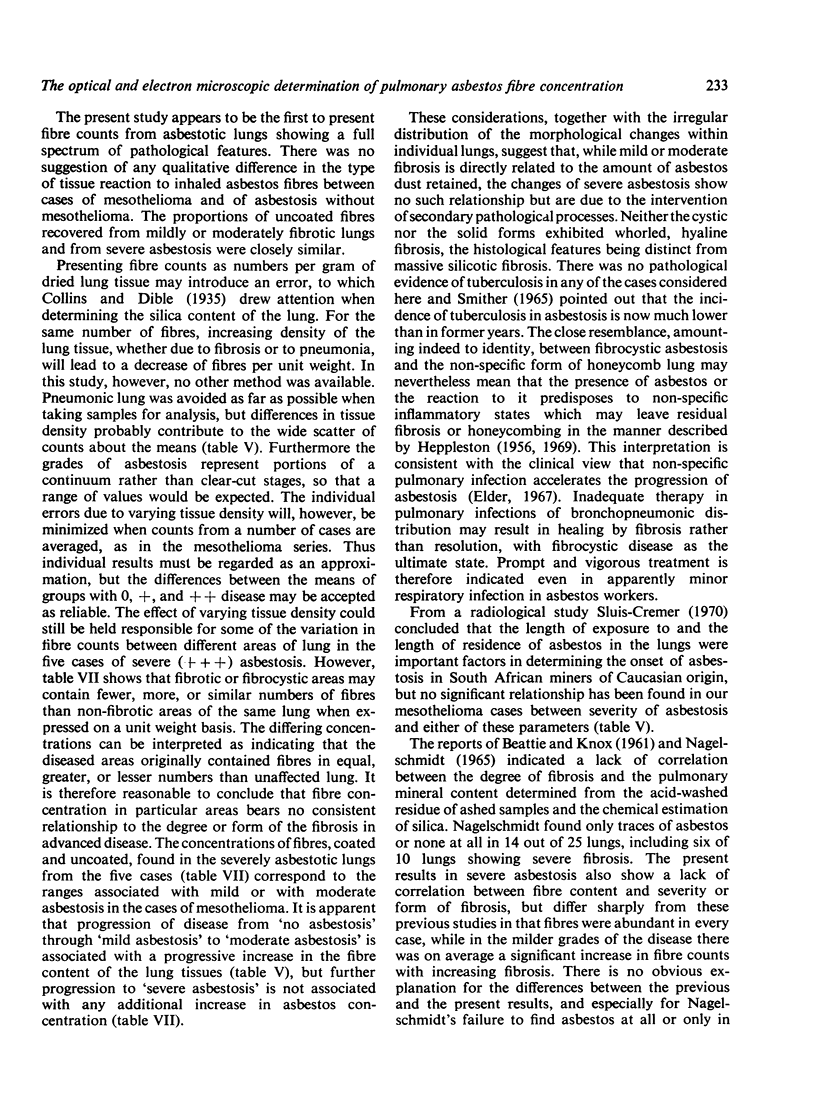
Asbestos fibre diameter distributions, gauged by electron microscopy, were fairly constant irrespective of the degree of fibrosis. Optically visible fibres constituted between 12 and 30% of the total, so that an optical count may be said to give an approximate indication of the total asbestos concentration and, so far as asbestosis is concerned, may well serve for comparative purposes. The relation between asbestos and neoplasia will, however, require identification and quantitation of particular types of the mineral by microanalytical techniques.
Full text
PDF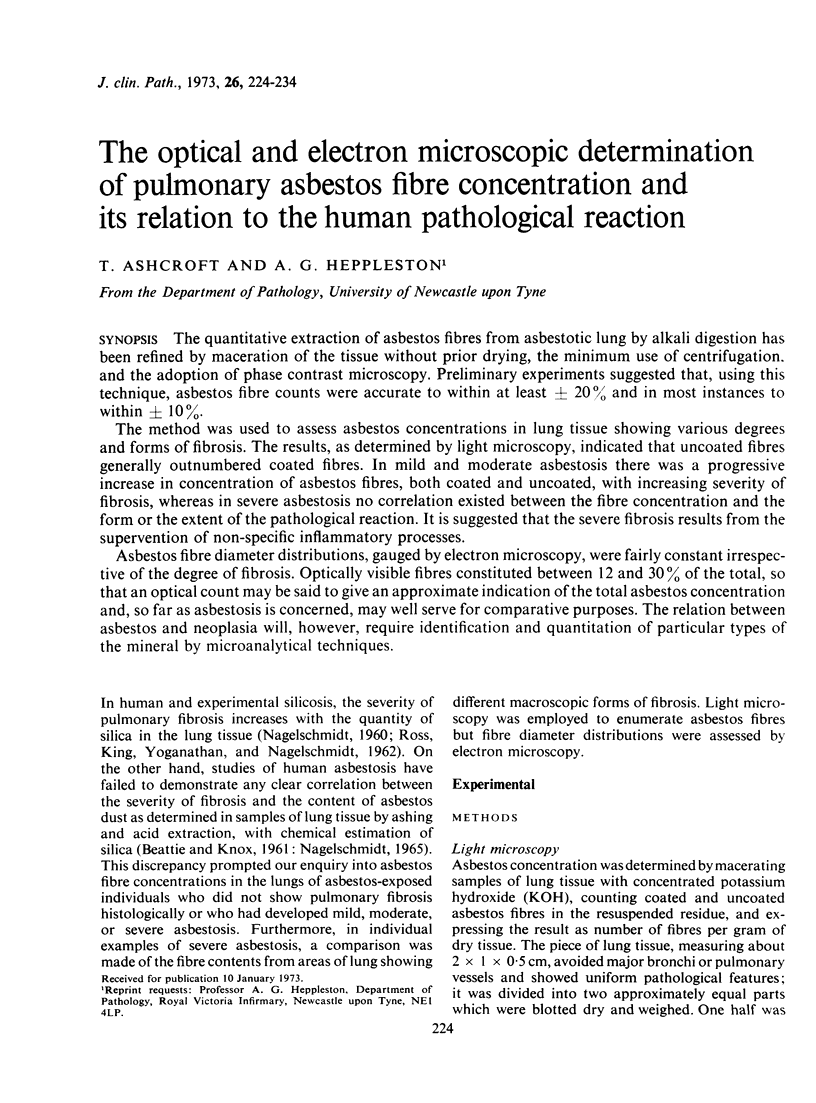

Images in this article



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Elder J. L. Asbestosis in Western Australia. Med J Aust. 1967 Sep 23;2(13):579–583. doi: 10.5694/j.1326-5377.1967.tb74073.x. [DOI] [PubMed] [Google Scholar]
- HEPPLESTON A. G. The pathology of honeycomb lung. Thorax. 1956 Jun;11(2):77–93. doi: 10.1136/thx.11.2.77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- HOLT P. F., MILLS J., YOUNG D. K. THE EARLY EFFECTS OF CHRYSOTILE ASBESTOS DUST ON THE RAT LUNG. J Pathol Bacteriol. 1964 Jan;87:15–23. doi: 10.1002/path.1700870103. [DOI] [PubMed] [Google Scholar]
- NAGELSCHMIDT G. The relation between lung dust and lung pathology in pneumoconiosis. Br J Ind Med. 1960 Oct;17:247–259. doi: 10.1136/oem.17.4.247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nagelschmidt G. Some observations of the dust content and composition in lungs with asbestosis, made during work on coal miners pneumoconiosis. Ann N Y Acad Sci. 1965 Dec 31;132(1):64–76. doi: 10.1111/j.1749-6632.1965.tb41090.x. [DOI] [PubMed] [Google Scholar]
- ROSS H. F., KING E. J., YOGANATHAN M., NAGELSCHMIDT G. Inhalation experiments with coal dust containing 5 per cent, 10 per cent, 20 per cent and 40 per cent quartz: tissue reactions in the lungs of rats. Ann Occup Hyg. 1962 Jul-Sep;5:149–161. [PubMed] [Google Scholar]
- Sluis-Cremer G. K. Asbestosis in South African asbestos miners. Environ Res. 1970 Nov;3(4):310–319. doi: 10.1016/0013-9351(70)90024-1. [DOI] [PubMed] [Google Scholar]
- Smith M. J., Naylor B. A method for extracting ferruginous bodies from sputum and pulmonary tissue. Am J Clin Pathol. 1972 Sep;58(3):250–254. doi: 10.1093/ajcp/58.3.250. [DOI] [PubMed] [Google Scholar]
- Smither W. J. Secular changes in asbestosis in an asbestos factory. Ann N Y Acad Sci. 1965 Dec 31;132(1):166–181. doi: 10.1111/j.1749-6632.1965.tb41099.x. [DOI] [PubMed] [Google Scholar]