

Abstract
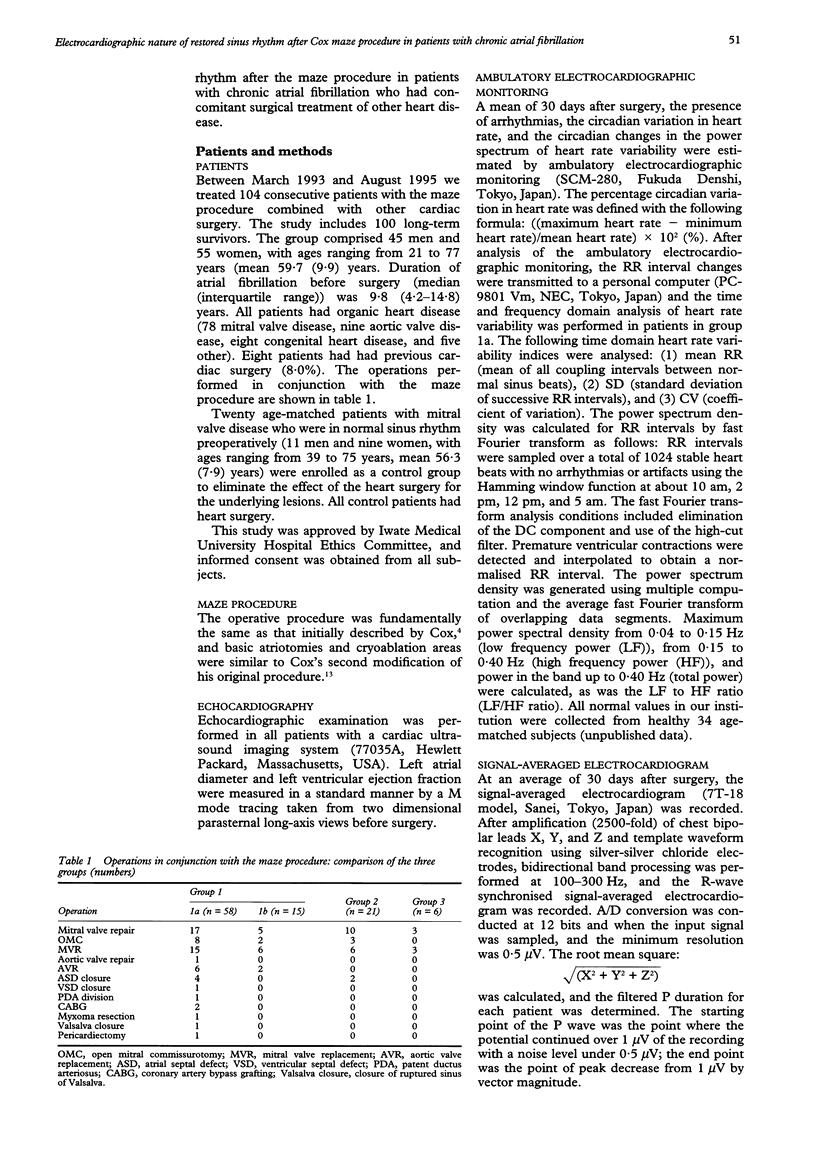
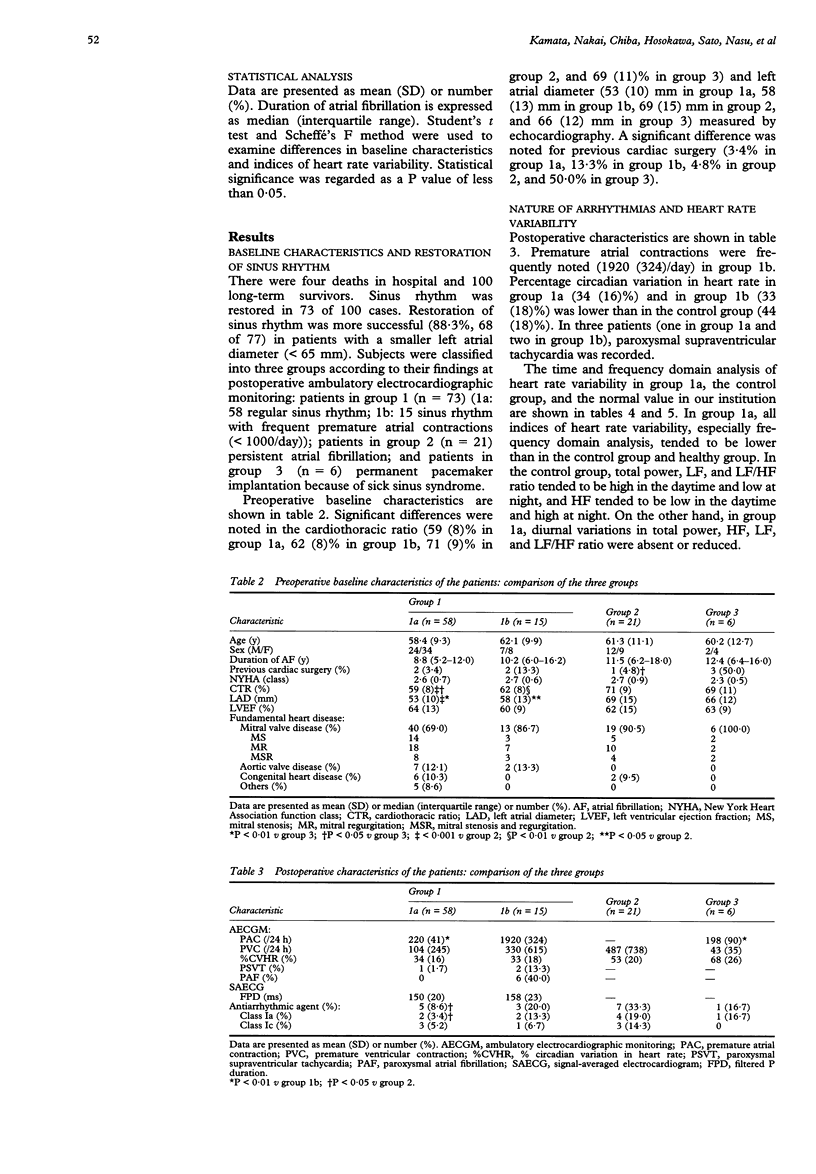
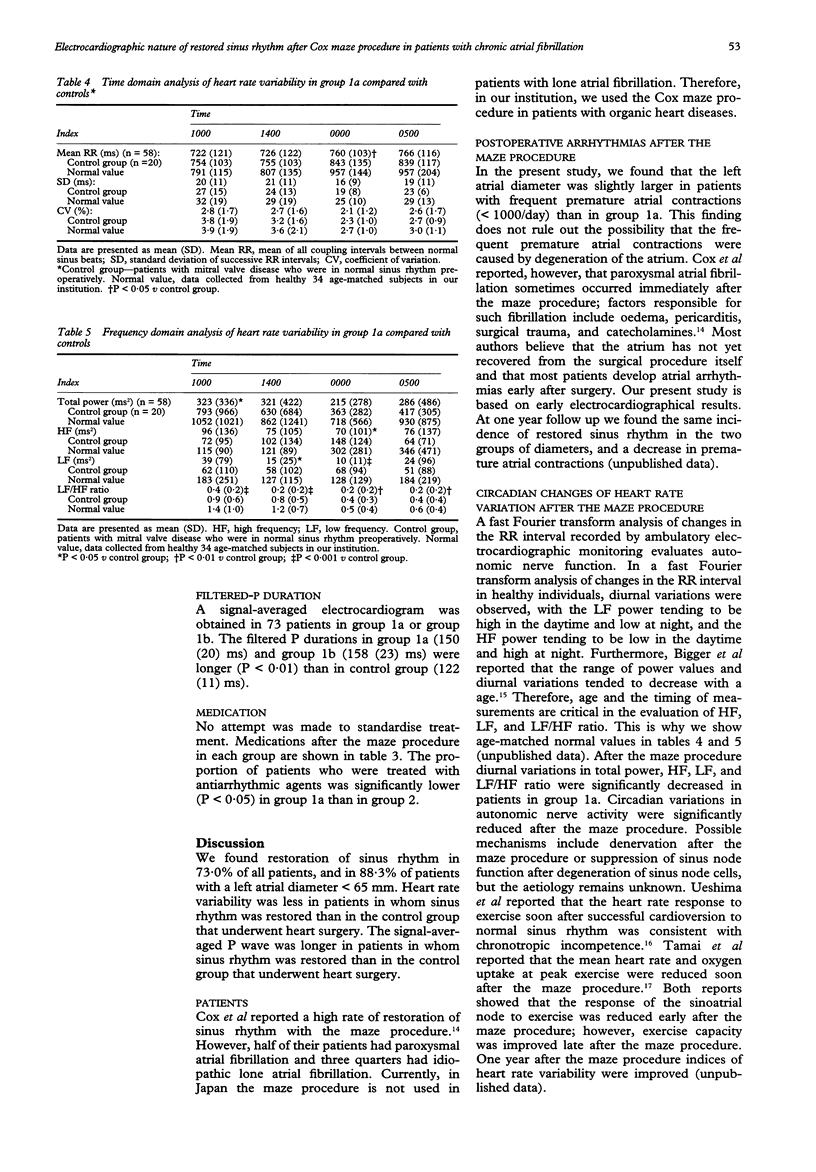
OBJECTIVE: To characterise heart rate variability and high frequency components of restored sinus rhythm after the maze procedure. The maze procedure for chronic atrial fibrillation may prevent thrombotic events and improve the quality of life. However, the electrocardiographic nature of restored sinus rhythm after the maze procedure has not been fully elucidated. PATIENTS AND METHODS: Between March 1993 and August 1995, 104 consecutive patients undergoing the maze procedure in combination with other cardiac surgery were studied. There were 100 long-term survivors (78 with mitral valve disease, 9 with aortic valve disease, 8 with congenital heart disease, and 5 others). Twenty age-matched patients with mitral valve disease who were in normal sinus rhythm preoperatively were enrolled as a control group. 30 days after surgery, the presence of arrhythmias and the circadian changes of heart rate variability were estimated by ambulatory electrocardiographic monitoring and the filtered P duration was evaluated by signal-averaged electrocardiogram. RESULTS: Restoration of sinus rhythm was observed in 73 of 100 cases. Subjects were classified into three groups according to their postoperative ambulatory electro-cardiographic monitoring findings: patients in group 1 (n = 73) (1a: 58 regular sinus rhythm; 1b: 15 sinus rhythm with frequent premature atrial contractions (> 1000/day); patients in group 2 (n = 21) still had persistent atrial fibrillation; and patients in group 3 (n = 6) required permanent pacemaker implantation because of sick sinus syndrome. The success rate of restoration of sinus rhythm was 88.3% if left atrial diameter was small (< 65 mm). Circadian changes in the low frequency to high frequency power ratio in group 1a were significantly diminished compared with control group (P < 0.01). Furthermore, the filtered P duration in group 1a (150 (20) ms) and group 1b (158 (23) ms) were longer than in the control group (122 (11) ms) (P < 0.01). CONCLUSIONS: The maze procedure may result in a decreased sinus response and non-uniform transmission of impulses in the atrium.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bigger J. T., Jr, Fleiss J. L., Steinman R. C., Rolnitzky L. M., Schneider W. J., Stein P. K. RR variability in healthy, middle-aged persons compared with patients with chronic coronary heart disease or recent acute myocardial infarction. Circulation. 1995 Apr 1;91(7):1936–1943. doi: 10.1161/01.cir.91.7.1936. [DOI] [PubMed] [Google Scholar]
- Bigger J. T., Jr, Fleiss J. L., Steinman R. C., Rolnitzky L. M., Schneider W. J., Stein P. K. RR variability in healthy, middle-aged persons compared with patients with chronic coronary heart disease or recent acute myocardial infarction. Circulation. 1995 Apr 1;91(7):1936–1943. doi: 10.1161/01.cir.91.7.1936. [DOI] [PubMed] [Google Scholar]
- Bonchek L. I., Burlingame M. W., Worley S. J., Vazales B. E., Lundy E. F. Cox/maze procedure for atrial septal defect with atrial fibrillation: management strategies. Ann Thorac Surg. 1993 Mar;55(3):607–610. doi: 10.1016/0003-4975(93)90262-g. [DOI] [PubMed] [Google Scholar]
- Cox J. L., Boineau J. P., Schuessler R. B., Ferguson T. B., Jr, Cain M. E., Lindsay B. D., Corr P. B., Kater K. M., Lappas D. G. Successful surgical treatment of atrial fibrillation. Review and clinical update. JAMA. 1991 Oct 9;266(14):1976–1980. [PubMed] [Google Scholar]
- Cox J. L., Canavan T. E., Schuessler R. B., Cain M. E., Lindsay B. D., Stone C., Smith P. K., Corr P. B., Boineau J. P. The surgical treatment of atrial fibrillation. II. Intraoperative electrophysiologic mapping and description of the electrophysiologic basis of atrial flutter and atrial fibrillation. J Thorac Cardiovasc Surg. 1991 Mar;101(3):406–426. [PubMed] [Google Scholar]
- Cox J. L. Evolving applications of the maze procedure for atrial fibrillation. Ann Thorac Surg. 1993 Mar;55(3):578–580. doi: 10.1016/0003-4975(93)90251-c. [DOI] [PubMed] [Google Scholar]
- Cox J. L., Schuessler R. B., Boineau J. P. The surgical treatment of atrial fibrillation. I. Summary of the current concepts of the mechanisms of atrial flutter and atrial fibrillation. J Thorac Cardiovasc Surg. 1991 Mar;101(3):402–405. [PubMed] [Google Scholar]
- Cox J. L., Schuessler R. B., D'Agostino H. J., Jr, Stone C. M., Chang B. C., Cain M. E., Corr P. B., Boineau J. P. The surgical treatment of atrial fibrillation. III. Development of a definitive surgical procedure. J Thorac Cardiovasc Surg. 1991 Apr;101(4):569–583. [PubMed] [Google Scholar]
- Cox J. L. The surgical treatment of atrial fibrillation. IV. Surgical technique. J Thorac Cardiovasc Surg. 1991 Apr;101(4):584–592. [PubMed] [Google Scholar]
- Guidera S. A., Steinberg J. S. The signal-averaged P wave duration: a rapid and noninvasive marker of risk of atrial fibrillation. J Am Coll Cardiol. 1993 Jun;21(7):1645–1651. doi: 10.1016/0735-1097(93)90381-a. [DOI] [PubMed] [Google Scholar]
- Kobayashi J., Kosakai Y., Kawashima Y. Maze procedure and anomalous coronary artery repair. Ann Thorac Surg. 1996 Mar;61(3):1008–1011. doi: 10.1016/0003-4975(95)00917-5. [DOI] [PubMed] [Google Scholar]
- Konings K. T., Kirchhof C. J., Smeets J. R., Wellens H. J., Penn O. C., Allessie M. A. High-density mapping of electrically induced atrial fibrillation in humans. Circulation. 1994 Apr;89(4):1665–1680. doi: 10.1161/01.cir.89.4.1665. [DOI] [PubMed] [Google Scholar]
- Kosakai Y., Kawaguchi A. T., Isobe F., Sasako Y., Nakano K., Eishi K., Kito Y., Kawashima Y. Modified maze procedure for patients with atrial fibrillation undergoing simultaneous open heart surgery. Circulation. 1995 Nov 1;92(9 Suppl):II359–II364. doi: 10.1161/01.cir.92.9.359. [DOI] [PubMed] [Google Scholar]
- Kosakai Y., Kawaguchi A. T., Isobe F., Sasako Y., Nakano K., Eishi K., Tanaka N., Kito Y., Kawashima Y. Cox maze procedure for chronic atrial fibrillation associated with mitral valve disease. J Thorac Cardiovasc Surg. 1994 Dec;108(6):1049–1055. [PubMed] [Google Scholar]
- McCarthy P. M., Cosgrove D. M., 3rd, Castle L. W., White R. D., Klein A. L. Combined treatment of mitral regurgitation and atrial fibrillation with valvuloplasty and the Maze procedure. Am J Cardiol. 1993 Feb 15;71(5):483–486. doi: 10.1016/0002-9149(93)90466-p. [DOI] [PubMed] [Google Scholar]
- Sato S., Kawashima Y., Hirose H., Nakano S., Matsuda H., Shirakura R. Long-term results of direct-current cardioversion after open commissurotomy for mitral stenosis. Am J Cardiol. 1986 Mar 1;57(8):629–633. doi: 10.1016/0002-9149(86)90848-9. [DOI] [PubMed] [Google Scholar]
- Tamai J., Kosakai Y., Yoshioka T., Ohnishi E., Takaki H., Okano Y., Kawashima Y. Delayed improvement in exercise capacity with restoration of sinoatrial node response in patients after combined treatment with surgical repair for organic heart disease and the Maze procedure for atrial fibrillation. Circulation. 1995 May 1;91(9):2392–2399. doi: 10.1161/01.cir.91.9.2392. [DOI] [PubMed] [Google Scholar]
- Ueshima K., Myers J., Morris C. K., Atwood J. E., Kawaguchi T., Froelicher V. F. The effect of cardioversion on exercise capacity in patients with atrial fibrillation. Am Heart J. 1993 Oct;126(4):1021–1024. doi: 10.1016/0002-8703(93)90732-o. [DOI] [PubMed] [Google Scholar]