

Abstract
Nutritional research in sickle cell disease has been the focus in recent times owing to not only specific nutritional deficiencies, but also the improvements associated with less painful episodes. Though hydroxyurea remains the drug of choice, certain adverse health effects on long term supplementation makes room for researches of different compounds. Macro and micro nutrient deficiencies, along with vitamins, play an important role in not only meeting the calorific needs, but also reducing clinical complications and growth abnormalities. Symptoms of hyper protein metabolism, increased cell turnover, increased cardiac output, and appetite suppression due to enhanced cytokine production, might give us leads for better understanding of the mechanisms involved. Different nutritional approaches comprising of traditional herbal therapies, antioxidants, flavonoids, vitamins, minerals etc., reducing oxidative stress and blood aggregation, have been tried out to increase the health potential. Nutritional therapies may also serve complementary to the newer therapies using ozone, hematopoietic stem cell transplantation, antifungal medications, erythropoietin etc. Herein we try to present a holistic picture of the different patho-physiological mechanisms, and nutritional strategies adopted.
Keywords: Sickle cell disease, Hydroxyurea, Vaso-occlusive crisis, Nutrient deficiencies, Nutritional approaches
Background
Sickle cell disease (SCD) one of the commonest prevalent autosomal recessive disease around the globe [1], is an inherited hematological disorder wherein, the oxygen-carrying molecule namely hemoglobin (Hb) present in the red blood cell, is defective. A mutation in the in the 6th codon of the 11th chromosome of the β globin chain, renders the amino acid valine to be substituted by glutamic acid resulting in HbS, the sickle cell haemoglobin [2].
The deoxygenated HbS undergoes hydrophobic interactions to form rod-like structures which are clusters of hemoglobin protein stuck to each other. These long fibers push the cell membrane out of shape causing the whole cell to become rigid,take a sickle shape, become deformed and adhere to the endothelium of blood vessels producing vasospasms,vasoconstriction, and triggering inflammation [3, 4] Adhesion is also significantly affected by alterations in hydration of erythrocytes. This changes their cellular tone and the cells become sickle shaped [5]. These red blood cells (RBC’s), due to their increased viscosity, sludge in the circulatory system obstructing microvasculature [6], producing oxygen deficiency at the target tissue/ organ. This causes tissue damage leading to ischemia and infarction and a compromised reduced life span [7].
In most of the cases, it requires immediate hospitalization and medical intervention with anti-inflammatory drugs, non-steroidal analgesics, hydroxyurea (HU), opioid analgesics, rehydration and in severe cases transfusion [8] which may cause other long term side effects.
Though born with a normal weight, children affected by SCD show weight deficits by year one which continues until adulthood accompanied by delayed skeletal maturation in both sexes and a delayed menarche in girls [9].
Fetal hemoglobin (HbF) is found in patients with SCD at different levels and is known to reduce the severity of symptoms of the disease. Hydroxyurea therapy has gained momentum as it raises levels of HbF accompanied by decreased morbidity. Though hydroxyurea is a potent HbF inducer in adults and children, it does not possess the ideal combination of efficacy, safety and ease of use [10]). This calls for further researches for compounds to alleviate the pain and improve the condition of patients with SCD. Several approaches have been made to prevent this disease or reverse the sickling phenomenon either through technological applications or the usage of compounds which affect the Hb molecule directly which are enlisted in the given Table 1.
Table 1.
Drug candidates exhibiting benefits in sickle cell disease
| Drug name | Action mechanism | Reference |
|---|---|---|
| Butyrate | HDAC inhibition, mood stabilization | [110, 111] |
| Decitabine | DNA demethylation | [112] |
| Trichostatin A | Increases HbF level; decrease adhesion of cells to vessel wall | [113] |
| Pomalidomide | Gammaglobin activation by Histone deacetylase | [114] |
| Senicapoc | Improves RBC hydration | [115] |
| Nitric Oxide | Increase NO | [116] |
| Tinzaparin | Decreases P-selectin-mediated acute pain episodes | [117] |
| 6R-BH4 | Increases NO; improve endothelial function | [118, 119] |
| Sidenafil | Increases NO | [116] |
| Eptifibatide | Decreases platelet aggregation and decreases CD40 ligand release | [120] |
| Statins | Improves endothelial function | [121] |
| Dexmethasone | Decrease inflammation | [122] |
| Nix-0699 | Uncertain, but inhibits acute painful crisis | [44, 123, 124] |
| Intravenous immunoglobulin (IVIG) | Decreases the number of leukocytes & acute pain episodes | [44, 123, 124] |
| Vorinostat, panobinostat | HDAC inhibition | [113] |
| GMI-1070 | Pan-selectin inhibitor | [45] |
| Propranolol | Inhibits RBC adhesion to the endothelium | [125] |
| Regadenoson | A2AR agonist, blocks iNKT activation | [126] |
| Zileuton | 5-lipoxygenase inhibitor, used in asthma | [127] |
| Fructose-1,6-diphosphate (FDP) | Reduces ischemia–induced tissue damage | [128] |
| Prasugrel | ADP receptor blockade | [129] |
| MP4CO | PEG carboxy-hemoglobin | [130] |
| Acetyl-L-carnitine | Decreases lipid peroxidation | [90] |
| Alpha-lipoic acid | Inhibits NFkB, increases glutathione | [131] |
| NAC | Increased glutathione | [132] |
| Omega-3 fatty acids | Decreases VOC events | [18] |
| Glutamine | Increases NADPH | [133] |
| IV magnesium | Vasodilatation | [134] |
| Aes-103 | Binds sickle hemoglobin and shifts oxy-hemoglobin dissociation curve to the left | [90] |
| Poloxamer-188 | Non-ionic surfactant, improves micro-vascular flow | [135] |
| L-arginine | Substrate for NO | [116] |
HbF fetal hemoglobin, NO nitric oxide, RBC red blood cell, IVIG intravenous immunoglobulin, HDAC Histone deacetylases, Nix-0699 Niprisan, GMI-1070 Rivipansel, FDP Fructose-1,6-diphosphate, NADPH Nicotinamide adenine dinucleotide phosphate, A2AR Adenosine A2A receptor, PEG Polyethylene glycol, ADP Adenosine diphosphate, iNKT Invariant natural killer T cells
Few drug candidates may exhibit multiple mechanisms of action
Supplementation of oral antibiotics for a definite period in childhood to prevent pneumococcal infections is generally practiced in SCD patients. Also it has been observed by the Cochrane Reviewers that prophylactic penicillin considerably reduces the risk of pneumococcal infections and it is related with negligible side effects in SCD homozygous children, [11, 12]. The broad-spectrum antifungal drug Clotrimazole appears to be a well-tolerated drug, with few adverse reactions due to drug resistance in SCD patients, who are immune-compromised. Its metallic complexes have been also shown to exhibit improved efficacy [13]. Pharmacological agents targeting signaling molecules are also being tried out [10]
Though morphine is the opioid of choice, [14] it has been linked to pediatric acute chest syndrome (ACS) in patients hospitalized with severe pain [15], when administered intravenously. The risks of newer therapies using blood and bone marrow stem cell transplant though curative, outweigh the benefits, thereby limiting its usage because they are expensive and unaffordable to the vast majority of affected patients [16].
Multiple nutrient deficiencies have been observed with increased severity of the disease. Prevention of complications is expected from ongoing research in the nutritional scenario. Nutritional intervention with potential key nutrients has been in focus in recent times owing to specific nutritional deficiencies [17] and improvements in SCD associated painful episodes. Nutritional interventions to correct the existing cell membrane structure, composition and function could provide additional benefit to the new preventing and curative aspects of SCD. For example fish oils containing eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) have been found to prevent the blockage of blood flow which could help in alleviating the problems associated with SCD [18]. Reduction of the vaso-occlusive crisis using zinc and piracetam are also quite encouraging, but larger cohorts, and/or longer term multi centric trials over a period of time are required to evaluate their efficacy [19]. A prospective nutritional approach with potentially active molecules like antioxidants might also be of benefit [20].
Interventions that are evidence based, sustainable, affordable and well incorporated into the healthcare structure should therefore be looked into. This review discusses the pros and cons of this much sought after issue in today’s context.
Nutrient insufficiencies/deficiencies
Nutritional intake has been found to be quite poor in SCD patients, and a serious need to correct the situation is implied [17]. Multiple nutrient insufficiencies or deficiencies of some micronutrients, vitamins, antioxidants and certain lipid constituents have been shown to be prevalent in patients with SCD and associated with increased disease severity of the disease (Fig. 1). Many complications associated with the disease, such as growth retardation, delayed sexual maturity, and a weak immune system, could be considered partly due to nutritional deficiencies [21]. In an important study Mandese et al. observed a significant relationship between body weight, body mass index (BMI) and either concentration of Hb or severity of the disease. They found that many of the nutritional components (macro and micro nutrients) are inadequate and affect the days of hospitalization for SCD patients. Also the concentration of HbF was negatively correlated with some of the nutrients like lipids, vitamins and minerals. They observed maximum nutrient deficiency in intake of Ca, Fe, vitamin B1 and C, while carbohydrates, lipids & vitamin B2 were moderately insufficient [22]. A study by Martyres et al. stressed out for the need of larger sample size to establish the relationship between nutrient deficiency and the severity of SCD [23].
Fig. 1.
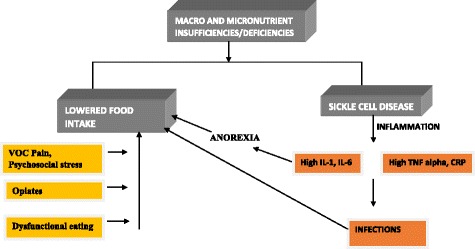
Nutrient deficiencies contributing to the vicious cycle in sickle cell disease
Researchers have found that markers of elevated oxidative stress and inflammation are expressed in adolescents with SCD even in a steady state, which correlated with their resting energy expenditure (REE) [24]. Experimental studies show an imbalance in the chronic state of oxidant and antioxidant factors in red cells of SCD patients, resulting in an increase of oxidative stress and hemolysis [25].
Role of macronutrient deficiencies
An increased plasma level of some acute inflammatory cytokines is observed in mice with sickle cell anemia (SCA) in response to infection. Supplementation of high protein diet resulted in decreased infection which can provide a clue to decreasing the incidents of infection in children with SCA. An increase in TNF -α, TNF- γ, IL-10, and IL-4 cytokines has been noted in the murine model of human SCA which is alleviated by supplementing a high protein diet [26]. In another study, decreased levels of CRP and IL-6 are observed on feeding a high protein diet [27].
Arginine plays an important role in SCD pathogenesis as insufficient / low global arginine bioavailability (GAB) is linked with many complications of the disease. Several mechanisms are proposed for arginine dysregulation in SCD patients. By inhibiting Gardo’s Channel activity arginine decreases the RBC density in transgenic SCD mice [28].
There is increased activity of arginase, increase in asymmetric dimethyl arginine, alteration in arginine transport mechanism and discrepancy in NO synthesis in these patients. Arginine supplementation through exogenous sources can restore low GAB. Arginine supplementation is quite successful in treating patients with leg ulcers, pulmonary hypertension and pain. Arginine supplementation along with hydroxyurea increases level of HbF and nitrite [29]. Preliminarily outcome of phase 2 clinical trial showed that reduced arginine induces pain and vaso-occlusive crisis (VOC) which is alleviated through arginine supplementation in SCD patients [30].
L-arginine is converted to citrulline and nitric oxide (NO) by the enzyme NO synthase (NOS). Beneficial effect of NO has been observed in SCD patients having acute chest syndrome, hypoxia and pulmonary hypertension [31]. NO is pivotal in the expression of sickle cell VOC as it plays an important role in both vascular vasodilatation allowing blood to flow easily, and in reducing the adhesiveness of sickled erythrocytes to the vascular wall. It also reduces platelet aggregation and protects the blood vessels from free radicals [32]. Low level of L-arginine is observed in HbSS adults, which decreases further during severe pain episodes [33, 34]. Over expression of NO synthase under reduces arginine concentration, thereby producing ROS, increasing the oxidative stress and reducing NO availability in these patients [35]. Inhaled NO was found to reduce the time period and episode of an acute VOC in children affected with this disease. Sildenafil, which is an oral phosphodiesterase -5 inhibitor, is known to amplify the production of endogenous NO which in turn causes an increase in HbF production [36].
Role of micronutrients
There is ample evidence linking lower levels of zinc with increased painful crisis in SCD patients. The increased daily zinc requirement in SCD patients, which is not met by the usual intake, is a consequence of hyper zincuria caused by increased hemolysis [37, 38].
Also alterations of several parameters of cellular immune functions in SCD patients have been related to a deficiency of zinc [37]. Zinc supplementation to pre pubertal aged sickle cell anemia patients was found to be beneficial on their linear growth and weight [39]. Zinc sulphate has been found quite effective in reducing RBC’s dehydration. It was also found to reduce sickle cell crises, pain and other life-threatening complications. Zinc supplementation not only improved growth and weight of SCD children, but also gave a boost to their immunity by offering antibacterial protection, thereby making its supplementation essential. Besides zinc, magnesium was found to protect against losses of water and potassium in SCD patients [39, 40]. Magnesium deficiency was found to increase episodes of sickling by causing cell dehydration in sickled erythrocytes [40]. In SCD patients It has been found that magnesium supplementation reduced the number of dense erythrocytes and also improved the erythrocyte membrane transport abnormalities of patients with SCD [41].
Copper deficiency is linked to anemia, being a key ingredient for functioning of metalloenzymes (e.g. ceruloplasmin), and plays an important role in iron metabolism. Ceruloplasmin helps to mobilize stored iron in the liver and make it more available for synthesis of Hb. Importantly, in copper deficiency anemia the synthesis rate of Hb is reduced, despite increased iron levels in the liver [42, 43].
Chromium is another element which helps in the management of SCD. It acts not only as a cofactor, at receptor sites of the insulin sensitive cell membrane but it also plays a role in carbohydrate metabolism which is the body’s much required energy source in SCD.
Manganese (Mn) which helps in glycoprotein synthesis and bone formation is also important for management of SCD. It also acts as cofactor of pyruvate carboxylase which participates in the respiratory chain reaction required for the much needed energy production, for SCD patients [44, 45].
Role of vitamins
As compared to their peers, SCD children are known to show decreased height and weight resulting in poor growth. Blood deficiency of several vitamins such as A, B6, C, D,& E and minerals like zinc, Mg is observed in patients with SCD by many researchers, which are the most factors contributing towards their poor growth and weight [46, 47]. These deficiencies cause a significant reduction in the concentrations of blood antioxidant levels in SCD patients resulting in VOC related ACS [48]. Researches supplementing vitamins E and C and minerals, magnesium and zinc either alone or in combination proved beneficial outcome in reducing the sickling pain crisis [49]. The decrease in concentration of antioxidant vitamins A, C, and E is responsible for increased hemolysis and susceptibility to bacterial infections in SCD. Decreases in arterial blood pressure reduction in the percentage of sickle cells, was observed with a collective supplementation of vitamins like A, C, and E, besides an increase in concentration of hemoglobin and packed cell volume [50, 51]. In vitro studies also established that vitamin E possesses anti-sickling property and therapeutic benefits in sickle cell anemia cases [52]. As nutritional deficiency plays a significant role in SCD complication, educating the patients on specific nutrient and calorie needs should be emphasized. Proper care must be provided about their dietary intake, ways of providing nutritious meals (particularly among the low income group), and means for enhancing protein and calorie consumption [46].
Administration of 1 mg vitamin B12 intramuscularly for a period of around 3 months showed significant symptomatic improvement in SCD patients. This study also confirmed that in cases of severity, these patients may undergo unrecognized deficiency of vitamin B12 [53]. Most of the pediatric patients display an adequate status of vitamins B6 and B12, but raised levels of plasma homocysteine along with a low folate levels. Folate supplementation would be beneficial to these patients, as it lessens their risk for endothelial damage [20]. Vitamin B6 is known for its crucial roles in different metabolic pathways in the body like ingestionof food, derivatization to the fueling molecule glucose and assisting in the metabolism of lipids and proteins. The biological potent form of vitamin B6, namely pyridoxal 5’ phosphate (PLP) functions as a cofactor for many of the enzymes involved in amino acid metabolism as well as the formation of neurotransmitters like serotonin, dopamine, epinephrine, and gamma amino-butyric acid.
SCD patients are prone to bone fractures and often the vitamin D status is found to be very low, putting them at great risk. Routine supplementation with vitamin D helps maintain the vitamin levels in such patients [54].
Proposed mechanisms for developing nutrient deficiencies in SCD
Proposed mechanisms of under nutrition may include dysfunctions in protein metabolism, cytokine related appetite suppression, enhanced cardiac energy output, and increases in erythrocyte levels [55, 56].
Hyper metabolism characterized by increased catabolism and lowered anabolism increases the calorific demand in SCD patients [57]. This is represented as increased resting energy expenditure (REE). A shortened lifespan of sickle cell blood cells causes an increased energy demand of the body. Hence their requirement of energy to sustain the normal functions of growth, physiological functioning and physical activity are not met. Increased energy requirements that are not followed by a concomitant calorific intake render an impaired growth status in these patients. Some researchers propose that frequent bouts of illnesses and hospitalization might have adverse effects on the frequency of food intakes and energy [55]. Also erythropoiesis increases the resting energy required in SCD. Researchers suggest that enhanced production of erythrocytes, increased cardiac output, and increased turnover of protein is possibly responsible for increased REE and protein requirements in SCD [58].
As SCD patients have lowered RBC concentration and are anemic, an elevation in resting cardiac indices is observed. In order to maintain and supply oxygen to the different tissues of the body, workload on the cardiac system is increased, thereby triggering a state of chronic inflammation. A study estimated the average hemoglobin synthesis to be ~ 0.725 g/kg/d in HbSS adults as compared to just 0.094 g/kg/d in their healthy counterparts. This results in an enhanced cell turnover in the bone marrow, and an increased glutamine uptake, thus leading to a depletion of the body’s glutamine levels. Further the study showed that pre-pubertal SCD children utilize 19 % more calories, about 58 % of more protein, and 47 % greater amount of glutamine than healthy children of their ages [59].
Large energy deficits due to a higher basal metabolic rate are regarded as one of the possible factors contributing towards poor growth in SCD individuals. This relatively low energy intake in younger children is also contributory to growth abnormalities [60]. Associations of protein intake and other macronutrients with growth measurements are limited due to studies that are not well structured and also smaller sample sizes. Protein utilization too appears compromised because of certain amino acid deficiencies. Hence the presence of orotic acid is observed in normal subjects with low intakes of protein which is similar to that observed in SCD patients [60].
Dysfunctional signaling of the hypothalamus and the inflammatory cytokines induced reduction in neuropeptide Y (NYP) release; appear to be responsible in causing changes in energy provided to the body. Inflammation may promote energy expenditure in a regulatory feedback manner to fight against energy supply in the peripheral organs/tissues as well as in the central nervous system. Blockage of the N YP leading to the suppression of appetite has been associated with noticeable weight loss and lowered physical activity. Other factors contributing to a reduced food intake may be also due to pain, fear, and other psychological stressors [61]).
Role of interleukins
Higher levels of IL-1 and IL-6 have been linked with increased morbidity risk in SCD [62]. Patients with enhanced IL-6, C-reactive protein, IL-1β, and TNF-α exhibit threshold changes in their sense of taste,and odor thereby affecting their dietary intakes [63]. Animal experiments associate IL-1 concentrations with food intakes and satiety by triggering the neurons in the hypothalamus. Hence antagonist IL-1beta receptors have been found to be alleviated in anorexia [64].
Leptin is another pro inflammatory cytokine known to regulate the feeding behavior, and energy utilization [65]. The cytokine IL-6 known to modulate the levels of leptin has also been implicated in anorexia though another study shows contrary results. Weight loss has been shown to result in a lowered production of leptin which is proportional to the loss of body fat [66].
Dysfunctional eating patterns
Psychological and social stresses, not to mention the extreme pain and the restricted activity, drive the SCD child to dysfunctional eating. Difficulty in eating and eating things not considered as food which are characteristic symptoms of pica, lead to nutritional deficiencies which go unnoticed by the clinician. Although one fourth of SCD children are affected by pica, it has not gained the focus of health care providers. Searching for biological explanations makes the clinician focus on aspects unrelated to psychological stressors [67].
Dehydration
One of the important factors affecting cell sickling is the loss of water in the cell. The migration of potassium and chloride ions carrying water across the RBCs causes dehydration, which consequently increases the tendency of the hemoglobin to polymerize and sickle. Studies show a potential therapeutic solution to reduce the cell sickling by blocking the loss of electrolytes from erythrocytes through two ion transport pathways, namely the K-Cl co -transporter and the Ca2 + -activated K+ channel [68].
Possible role of lipids
The role of dietary lipids deserves specific mention because, phospholipids composition of the membrane lipids in sickle cell erythrocytes show distinct abnormalities which may have a direct bearing upon the dehydration and abnormal sodium and potassium metabolism known to occur in sickle erythrocytes. This also has a direct impact on cellular function [69]. The increased permeability of sodium and potassium in the deoxygenated sickle cell leads to an overload on the renal system causing its damage [70]. In combination with the protein abnormality of hemoglobin, these molecular changes in membrane phospholipids composition may accentuate the sickling phenomena and perhaps, impart to the crisis in these patients.
Potential nutritional approaches for SCD
Benefits from nutritional supplements in the management of SCD and its associated clinical conditions have strengthened considerations of nutritional aspects apart from the genetic one. Possible approaches for nutritional intervention to attain optimal immune and nutritional status for prevention of the related disease symptoms and reduction of morbidity and mortality in SCD patients are being explored. Use of dietary supplements to patients irrespective of age has shown improvements in growth and protection against infections [71].
Traditional herbal therapy
Many herbs that contain beneficial phyto compounds have been used since ancient times to reduce sickling as well as the painful episodes. Leaf extracts of Carica papaya and Parquetina nigrescens, root extracts of Fagara zanthoxyloides, and seed extracts of Cajanuscajan, contain phyto-antioxidants, which may act either alone or synergistically to augment the anti-sickling activity of these plants.(67) The Congolese plant Justicia secunda containing anthocyanins was found to exhibit potential antisickling effects [72, 73]. Eugenia caryophyllata and Piper guineense contain vanilloids like Shikimic acid and cannaboids that are of benefit in reducing the painful episodes by mechanisms similar to that of the opiates [74], F.zanthoxyloides, natively called fagara has been used for the reduction of painful episodes in SCD. Nicosan is a popular and safe Nigerian anti sickling herbal remedy inhibiting hemoglobin S polymerization [68]. Bioassay experiments show that maximum reduction in sickling was observed by the leaf extracts of C. papaya at concentrations of 5 mg/mL [52] probably due to relatively high total phenol content exhibiting high free radical scavenging activity. Though many of these phyto-medicines have proved beneficial, further multicentric researches are required to validate their usage.
Antioxidant therapy
SCD is one of the many diseases in which oxidative stress plays a significant role affecting the RBCs, and leading to inflammation and the resulting pain. Levels of antioxidants seem to be compromised in SCD [75]. During management of clinical cases, the exacerbated iron load due to hemolysis and multiple transfusions potentiates ROS generation. Among several antioxidants known, the phenolic compounds isolated from plants, namely the flavonoids are very important. Supplementation of natural antioxidants vitamins such as A, C, and E have been shown to decrease the number of irreversibly sickled cells, the arterial blood pressure, and concentration of mean corpuscular Hb concentration with concomitant increases in packed cell volume (PCV} concentration [52].
The cyclic cascade leading to complications of cell adhesion and VOC, triggers production of ROS further intensifying the disease symptoms. As oxidative stress plays a pivotal role in SCD patients during VOC, the use of antioxidants to improve the clinical status seems essential. In-vivo studies on antioxidants using animal models have shown promising results. Ascorbic acid has shown effectivity as a potent antioxidant at as low as 0.1 millimolar concentrations [76]. A 10 week supplementation of vitamin E showed a decrease in the cell sickling from 25 % to 11 % [77].
However, clinical studies using vitamin E have shown poor success rates and found no significant differences in cell adhesion and lipid peroxidation levels [78]. This has prompted Ohnishi etal to advocate a mixture of antioxidants in the suppression of SCD symptoms [20]. It has been suggested that the generation of free radicals in SCD may overpower the strength of exogenous antioxidants and therefore a mixture of antioxidants may prove beneficial. Also the generation of ROS due to external factors of diet, environment, and co-morbidities associated with SCD, needs to be well explored and evaluated. Well defined studies showing effects of the two different types of antioxidants on severity of symptoms in SCD should be performed. Antioxidants providing enzyme defense (such as SOD, catalase, GPX, and hemo- oxygenase -1) and antioxidants scavenging different free radicals (such as vitamins E,C, GSH) should be independently considered [79]. Also in spite of enhanced levels of antioxidant intake in SCD is being advocated so far, no established standardization exists. Therefore it becomes difficult to generalize the results of a particular study for antioxidant usage or future therapy [80]. Future research should target specific ROS generation depots using different antioxidant combinations to reduce SCD complications. However, limited phase three clinical trials are available due to the complex pathophysiology in SCD [77].
Use of dietary lipids and omega- 3 fatty acids
The popular lipid food additive butyric acid has been found to increase levels of HbF in the blood and stabilize the mental mood. Experimental evidence suggests that the two short chain fatty acid derivatives namely α methyl hydrocinnamic acid and 2, 2 dimethyl butyrate offer significant therapeutic benefits as they induce fetal γ globin expression in SCD. They are further found to stimulate HbF cells with erythroid proliferation at quite low doses than the existing phenyl butyrate and butyrate [81].
A striking enhancement in the concentration of lipid constituents in sickle cells is observed when matched with similarly aged erythrocytes. Also the erythrocytes left unsickled, occupy a larger surface area, appearing flattened as compared to normally aged cells [82]. Abnormalities in the membrane lipid composition in SCD appear to have a direct impact on the cellular functions. Phospholipid composition of the membrane in sickle cell erythrocytes shows distinct abnormalities [46]. Deficiencies of certain polyunsaturated fatty acids and their subsequent replacement by monounsaturated and saturated fatty acids may be related to dehydration and the uncharacteristic sodium and potassium transport in sickled erythrocytes. This could not only help in possible corrections through exogenous supplementation of these fatty acids, but also serve as a useful diagnostic marker [46]. Pilot studies suggested that supplements containing omega-3 fatty acids may decrease the painful hemolytic and VOC and improve the membrane fatty acid composition [18]. The omega-3 fatty acids namely eicosapentaenoic acid (EPA), and docosahexaenoic acid(DHA), are two important structural and functional constituents of the RBCs which have been shown to inhibit haemolysis and vasoocclusion, thereby reducing the number of VOC in SCD [18, 83, 84]. In addition, omega-3 fatty acids diminish the expression of intercellular adhesion molecule-1, leukocyte adhesion to vascular endothelium, and the production of four biologically active molecules involved in the pathophysiology of tissue damage in SCD,namely the interleukins (IL)-1β, IL-6, and IL- 8 and tumor necrosis factor-alpha [85]. Furthermore, it has been observed that the greater the quantity of EPA and DHA in the blood, the lower the risk of developing complications of SCD and the lesser the degree of anemia [86, 87]. Their affordability over other current therapies in non-affluent countries where the overwhelming majority of people affected by sickle cell disease live makes it a feasible option. The diverse anti-aggregatory, anti-adhesive, and anti-inflammatory role of omega-3 fatty acids makes it a promising therapeutic candidate for the prevention of cell sickling and reduction of the painful crisis in SCD [18].
Use of amino-acids
Antisickling action of many plants of medicinal value and other naturally existing compounds may be attributed to the presence of amino acids [88]. Phenylalanine present in an herbal plant Cajanuscajan, and hydroxybenzoic acid present in another medicinal plant of the Vitex family are thought to be the reason for their antisickling effect [89]. Amino acids display their antisickling behavior by increasing the cell volume of the RBC’s, thereby decreasing the concentration of intracellular hemoglobin below the gelling threshold [90]. The possible mechanism of action leading to the antisickling effect by phenylalanine, is reported to involve the liposomal transport system, as well as the Na+/K+ transport system [91]. The aromatic compound L-phenylalanine benzyl ester acts as an antisickling agent, and is found to possess potential therapeutic properties beneficial in the treatment of SCD [92].
Use of opioids
Individuals addicted with opiates often experience severe macro and micro nutrient deficiencies which renders their protein and carbohydrate metabolism inefficient. Being indifferent to the basic necessities of life makes them impoverished and undernourished. This makes them underweight with a lowered immunity, hormonal imbalances, prone to infections and organ damage. Alterations in the levels of certain specific nutrients may also hinder their addiction withdrawal. Moreover lack of nutritional education leads them to unhealthy eating behaviors. Unfortunately addiction centers do not identify nutritional programs as a major influencing factor. Effective supplementation of large amounts of protein and amino acids during de addiction, may be required to boost their nutritional status [93].
Opoids exhibit their beneficial anti analgesic activity by either exerting their histaminergic effect, excitatory effect, dopaminergic effect or proserotonergic effect [94]. A fear of addiction to narcotics by patients, giving rise to ethical issues [95] has also led to its controlled usage. Use of intranasal fentanyl in a pediatric emergency setting was related with a considerably reduced time to attain analgesia as compared with morphine, administered parenterally, and caused minimum distress to children [96] Experiences from managing pain in children could well be then extrapolated to adults.
Current new approaches
In response to anemia, the kidneys secrete erythropoietin which is the major non-immunological cytokine that regulates erythropoiesis. Therefore serum levels of erythropoietin are often increased in SCD wherein chronic anemia is observed [94]. Erythropoietin’s ability to provide a stimulus in HbF production could be used for clinical trials. This raise in HbF gives us a lead that human erythropoietin could be used favorably in SCD as it either increases availability of oxygen and nutrients or produces proteins favoring growth and healing. This is also observed in supplementation with HU [53].
The anti-fungal compound clotrimazole, appears to block the Ca2 + -activated K+ channels in RBCs and in smooth muscle cells via the cytochrome P450 [97]. Researches are on to experiment this compound in conjunction with other bioactive compounds for long term treatment.
Ozone being the allotrope of oxygen, possesses healing properties which are yet to be completely understood. Bocci et al. observed that ozone activates a number of biochemical pathways, which are very useful in vasculopathies, particularly chronic limb ischemia [98]. The rationale for using ozone therapy in SCD appears to be based upon its action on the endothelium thereby enhancing the release of NO and prostacyclin and suppressing the release of endothelin-1(a vaso constriction affecting peptide that is increased during cell injury and insult) [99]. Careful blood ozonization appears to be one of the few effective procedures for correcting chronic oxidative stress [99].
Significant progress has been achieved in gene therapy approaches for treatment of SCD [100]. Gene therapy in SCD patients has been known to target major repressor proteins implicated during development [10]. Gene therapy approaches in SCD mice decreased anemia and hyper leukocytosis, reduced the accumulation of iron in liver, and enhanced splenic and renal function. Thus, modest chimerism with the donor cells exhibiting high levels of HbF from a γ-globin lentiviral vector that is insulated can mend the pathological status in SCD mice. This would render a safer and effective option of gene therapeutics in humans [101]. Talano et al. have shown the usage of alternative allogeneic donors which can either be familial haploidentical (FHI) donors, matched unrelated donors (MUD), or unrelated cord blood donors (UCB). These therapies have ensued in high survival rate among SCD patients. Now due to these advanced approaches, a lot of people having chronic SCD conditions are able to receive curative allogenic stem cell therapies [16].
Newer non-invasive therapies like lung extension to ease the airway pressure, pulse oximetry, and incentive spirometry hold potential for future treatments [102]. Continuous positive airway pressure (CPAP) therapy treated subjects exhibited lesser pain, improved cognition, and a decreased apnea-hypopnea index. The intensity of pain days was reduced from 2.3 days to 0.8 days per week for each patient [103]. A dysfunction in the hemoglobin of SCD and a right-shifted oxyhemoglobin dissociation curve (ODC) alter the oxyhemoglobin saturation (SpO2) values that can be measured by pulse oximetry which is a non-invasive method [104]. Incentive spirometry [105],as well as positive expiratory pressure therapies also showed a great promise especially in children who may experience hypoventilation when administered high doses of opiates for painful VOC crisis [106].
Conclusion
SCD is well known to be an inherited disorder with a disruptive metabolic status causing immense pain and a compromised life for the patient. Different patterns of culture, unmet economic needs, lack of health education and nutritional awareness place the sickle cell disease patient to increased risk of dietary deficiencies leading to pain and problems. These nutritional deficiencies may surface either due to lowered intake of specific nutrients or malfunctioning in the metabolic pathway or alterations at the genetic level.
Though HU therapy is clinically very promising, certain areas like lowering of sperm counts in males [107], instability in the genetic makeup through deregulation of telomere repeat binding factor 2 (TRF2) and telomere dysfunction [108] is a matter of concern. This calls for further researches for compounds to alleviate the pain and improve the condition of patients with SCD. Nutrients with their immense benefits could add to the prevention and curative aspects of SCD. Also translation of genetic technology,particularly epigenetic nutrition could well pave the way to better SCD patient care [109].
Though much has been reported about nutritional supplements and their benefits, little has changed in clinical practice. Also larger well-structured multi-centric studies need to be addressed to arrive at conclusive evidence-based recommendations by a scientific body. This would then gain the much required attention on nutritional aspects by clinicians, and benefit the SCD patient.
Acknowledgments
The authors are grateful to King Fahd Medical Research Center (KFMRC), King Abdulaziz University (Jeddah, Saudi Arabia) for the facilities provided. Special thanks are also due to Mr. Mohammad S Gazdar (Librarian, KFMRC) for providing the assistance in searching the scientific literature. Authors would also like to thank KACST, for providing a grant, bearing number: AT35-25, to pursue a research project on the nutritional benefits in sickle cell disease.
Funding
King Abdulaziz City for Science and Technology, Riyadh, Saudi Arabia. (KACST) Grant #AT35-25.
Availability of data and materials
Data sharing not applicable to this article as no datasets were generated or analyzed during the writing of this review-article.
Authors’ contributions
SK, AA, and SK contributed towards acquisition of literature on the subject and drafting of the manuscript. GD, AK, AM, and AB read the draft and contributed with critical assessment and editing of the draft. GAH, SM, and SHH contributed with clinical related inputs on the subject based on published work in the area. All authors critically read the manuscript and approved the final manuscript ensuring integrity.
Competing interests
The authors declare that they have no competing interests.
Abbreviations
- ACS
Acute chest syndrome
- DHA
Docosahexaenoic acid
- EPA
Eicosapentaenoic acid
- HbF
Fetal hemoglobin
- HSCT
Hematopoietic stem cell transplantation
- HU
Hydroxyurea
- IL
Interleukins
- NO
Nitric Oxide
- REE
Resting energy expenditure
- ROS
Reactive oxygen species
- SCD
Sickle cell disease
- VOC
Vaso occlusive crisis
Contributor Information
Shahida A. Khan, Email: sakhan01@kau.edu.sa, Email: shahidakhan2009@gmail.com
Ghazi Damanhouri, Email: gdamanhouri@gmail.com.
Ashraf Ali, Email: ashrafbiochem@gmail.com.
Sarah A. Khan, Email: khan.sarah.aziz@gmail.com
Aziz Khan, Email: azizkfmrc@gmail.com.
Ahmed Bakillah, Email: Ahmed.Bakillah@downstate.edu.
Samy Marouf, Email: samy_marouf@hotmail.com.
Ghazi Al Harbi, Email: Alharbi98@hotmail.com.
Saeed H. Halawani, Email: shhalawani@uqu.edu.sa
Ahmad Makki, Email: ahmedmakki1234@gmail.com.
References
- 1.Weatherall DJ, Clegg JB. Inherited haemoglobin disorders: an increasing global health problem. Bull World Health Organ. 2001;79:704–712. [PMC free article] [PubMed] [Google Scholar]
- 2.Adorno EV, Zanette A, Lyra I, Souza CC, Santos LF, Menezes JF, Dupuit MF, Almeida MN, Reis MG, Goncalves MS. The beta-globin gene cluster haplotypes in sickle cell anemia patients from Northeast Brazil: a clinical and molecular view. Hemoglobin. 2004;28:267–271. doi: 10.1081/HEM-120040310. [DOI] [PubMed] [Google Scholar]
- 3.Steinberg MH. Review: sickle cell disease: present and future treatment. Am J Med Sci. 1996;312:166–174. doi: 10.1016/S0002-9629(15)41800-2. [DOI] [PubMed] [Google Scholar]
- 4.Steinberg MH. In the clinic. Sickle cell disease. Ann Intern Med. 2011;155:ITC31–15. doi: 10.7326/0003-4819-155-5-201109060-01003. [DOI] [PubMed] [Google Scholar]
- 5.Wandersee NJ, Punzalan RC, Rettig MP, Kennedy MD, Pajewski NM, Sabina RL, Paul Scott J, Low PS, Hillery CA. Erythrocyte adhesion is modified by alterations in cellular tonicity and volume. Br J Haematol. 2005;131:366–377. doi: 10.1111/j.1365-2141.2005.05767.x. [DOI] [PubMed] [Google Scholar]
- 6.Embury SH. The Not‐So‐Simple Process of Sickle Cell Vasoocclusion. Microcirculation. 2004;11:101–113. doi: 10.1080/10739680490278277. [DOI] [PubMed] [Google Scholar]
- 7.Chakravorty S, Williams TN. Sickle cell disease: a neglected chronic disease of increasing global health importance. Arch Dis Child. 2015;100:48–53. doi: 10.1136/archdischild-2013-303773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stevens MC, Maude GH, Beckford M, Grandison Y, Mason K, Taylor B, Serjeant BE, Higgs DR, Teal H, Weatherall DJ, et al. Alpha thalassemia and the hematology of homozygous sickle cell disease in childhood. Blood. 1986;67:411–414. [PubMed] [Google Scholar]
- 9.Adewoyin AS. Management of sickle cell disease: a review for physician education in Nigeria (sub-saharan Africa) Anemia. 2015;2015:791498. doi: 10.1155/2015/791498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pace BS, Liu L, Li B, Makala LH. Cell signaling pathways involved in drug-mediated fetal hemoglobin induction: Strategies to treat sickle cell disease. Exp Biol Med (Maywood) 2015;240:1050–1064. doi: 10.1177/1535370215596859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hirst C, Owusu-Ofori S. Prophylactic antibiotics for preventing pneumococcal infection in children with sickle cell disease. Cochrane Database Syst Rev. 2014;11:CD003427. doi: 10.1002/14651858.CD003427.pub3. [DOI] [PubMed] [Google Scholar]
- 12.Hirst C, Owusu-Ofori S. Prophylactic antibiotics for preventing pneumococcal infection in children with sickle cell disease. Cochrane Database Syst Rev. 2012;9:CD003427. doi: 10.1002/14651858.CD003427.pub2. [DOI] [PubMed] [Google Scholar]
- 13.Crowley PD, Gallagher HC. Clotrimazole as a pharmaceutical: past, present and future. J Appl Microbiol. 2014;117:611–617. doi: 10.1111/jam.12554. [DOI] [PubMed] [Google Scholar]
- 14.van Beers EJ, van Tuijn CF, Nieuwkerk PT, Friederich PW, Vranken JH, Biemond BJ. Patient-controlled analgesia versus continuous infusion of morphine during vaso-occlusive crisis in sickle cell disease, a randomized controlled trial. Am J Hematol. 2007;82:955–960. doi: 10.1002/ajh.20944. [DOI] [PubMed] [Google Scholar]
- 15.Birken CS, Khambalia A, Dupuis A, Pastor A, Lee M, Padavattan K, Mekky M, Odame I, Parkin PC. Morphine is associated with acute chest syndrome in children hospitalized with sickle cell disease. Hosp Pediatr. 2013;3:149–155. doi: 10.1542/hpeds.2012-0067. [DOI] [PubMed] [Google Scholar]
- 16.Talano JA, Cairo MS. Hematopoietic stem cell transplantation for sickle cell disease: state of the science. Eur J Haematol. 2015;94:391–399. doi: 10.1111/ejh.12447. [DOI] [PubMed] [Google Scholar]
- 17.Kawchak DA, Schall JI, Zemel BS, Ohene-Frempong K, Stallings VA. Adequacy of dietary intake declines with age in children with sickle cell disease. J Am Diet Assoc. 2007;107:843–848. doi: 10.1016/j.jada.2007.02.015. [DOI] [PubMed] [Google Scholar]
- 18.Daak AA, Ghebremeskel K, Hassan Z, Attallah B, Azan HH, Elbashir MI, Crawford M. Effect of omega-3 (n − 3) fatty acid supplementation in patients with sickle cell anemia: randomized, double-blind, placebo-controlled trial. Am J Clin Nutr. 2013;97:37–44. doi: 10.3945/ajcn.112.036319. [DOI] [PubMed] [Google Scholar]
- 19.Riddington C, De Franceschi L. Drugs for preventing red blood cell dehydration in people with sickle cell disease. Cochrane Database Syst Rev 2002;4:CD003426. [DOI] [PubMed]
- 20.Ohnishi ST, Ohnishi T, Ogunmola GB. Sickle cell anemia: a potential nutritional approach for a molecular disease. Nutrition. 2000;16:330–338. doi: 10.1016/S0899-9007(00)00257-4. [DOI] [PubMed] [Google Scholar]
- 21.Serjeant GR. The emerging understanding of sickle cell disease. Br J Haematol. 2001;112:3–18. doi: 10.1046/j.1365-2141.2001.02557.x. [DOI] [PubMed] [Google Scholar]
- 22.Mandese V, Marotti F, Bedetti L, Bigi E, Palazzi G, Iughetti L. Effects of nutritional intake on disease severity in children with sickle cell disease. Nutr J. 2016;15:46. doi: 10.1186/s12937-016-0159-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Martyres DJ, Vijenthira A, Barrowman N, Harris-Janz S, Chretien C, Klaassen RJ. Nutrient Insufficiencies/Deficiencies in Children With Sickle Cell Disease and Its Association With Increased Disease Severity. Pediatr Blood Cancer. 2016;63(6):1060–4. doi: 10.1002/pbc.25940. [DOI] [PubMed] [Google Scholar]
- 24.Akohoue SA, Shankar S, Milne GL, Morrow J, Chen KY, Ajayi WU, Buchowski MS. Energy expenditure, inflammation, and oxidative stress in steady-state adolescents with sickle cell anemia. Pediatr Res. 2007;61:233–238. doi: 10.1203/pdr.0b013e31802d7754. [DOI] [PubMed] [Google Scholar]
- 25.Hundekar PS, Suryakar AN, Karnik AC, Katkam RV, Joshi NG, Ghone RA. Level of nitric oxide and antioxidant vitamins in sickle cell anaemia patients. Indian J Physiol Pharmacol. 2012;56:125–129. [PubMed] [Google Scholar]
- 26.Hyacinth HI, Capers PL, Archer DR, Hibbert JM. TNF-alpha, IFN-gamma, IL-10, and IL-4 levels were elevated in a murine model of human sickle cell anemia maintained on a high protein/calorie diet. Exp Biol Med (Maywood) 2014;239:65–70. doi: 10.1177/1535370213508357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Archer DR, Stiles JK, Newman GW, Quarshie A, Hsu LL, Sayavongsa P, Perry J, Jackson EM, Hibbert JM. C-reactive protein and interleukin-6 are decreased in transgenic sickle cell mice fed a high protein diet. J Nutr. 2008;138:1148–1152. doi: 10.1093/jn/138.6.1148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Romero JR, Suzuka SM, Nagel RL, Fabry ME. Arginine supplementation of sickle transgenic mice reduces red cell density and Gardos channel activity. Blood. 2002;99:1103–1108. doi: 10.1182/blood.V99.4.1103. [DOI] [PubMed] [Google Scholar]
- 29.Morris CR. Alterations of the arginine metabolome in sickle cell disease: a growing rationale for arginine therapy. Hematol Oncol Clin North Am. 2014;28:301–321. doi: 10.1016/j.hoc.2013.11.008. [DOI] [PubMed] [Google Scholar]
- 30.Bakshi N, Morris CR. The role of the arginine metabolome in pain: implications for sickle cell disease. J Pain Res. 2016;9:167–175. doi: 10.2147/JPR.S55571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chang TP, Kriengsoontorkij W, Chan LS, Wang VJ. Clinical factors and incidence of acute chest syndrome or pneumonia among children with sickle cell disease presenting with a fever: a 17-year review. Pediatr Emerg Care. 2013;29:781–786. doi: 10.1097/PEC.0b013e31829829f7. [DOI] [PubMed] [Google Scholar]
- 32.Gladwin MT, Barst RJ, Gibbs JS, Hildesheim M, Sachdev V, Nouraie M, Hassell KL, Little JA, Schraufnagel DE, Krishnamurti L, et al. Risk factors for death in 632 patients with sickle cell disease in the United States and United Kingdom. PLoS One. 2014;9:e99489. doi: 10.1371/journal.pone.0099489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Enwonwu CO, Xu XX, Turner E. Nitrogen metabolism in sickle cell anemia: free amino acids in plasma and urine. Am J Med Sci. 1990;300:366–371. doi: 10.1097/00000441-199012000-00005. [DOI] [PubMed] [Google Scholar]
- 34.Lopez BL, Kreshak AA, Morris CR, Davis-Moon L, Ballas SK, Ma XL. L-arginine levels are diminished in adult acute vaso-occlusive sickle cell crisis in the emergency department. Br J Haematol. 2003;120:532–534. doi: 10.1046/j.1365-2141.2003.04109.x. [DOI] [PubMed] [Google Scholar]
- 35.Xia Y, Dawson VL, Dawson TM, Snyder SH, Zweier JL. Nitric oxide synthase generates superoxide and nitric oxide in arginine-depleted cells leading to peroxynitrite-mediated cellular injury. Proc Natl Acad Sci U S A. 1996;93:6770–6774. doi: 10.1073/pnas.93.13.6770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Villagra J, Shiva S, Hunter LA, Machado RF, Gladwin MT, Kato GJ. Platelet activation in patients with sickle disease, hemolysis-associated pulmonary hypertension, and nitric oxide scavenging by cell-free hemoglobin. Blood. 2007;110:2166–2172. doi: 10.1182/blood-2006-12-061697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Prasad AS, Kaplan J, Brewer GJ, Dardenne M. Immunological effects of zinc deficiency in sickle cell anemia (SCA) Prog Clin Biol Res. 1989;319:629–647. [PubMed] [Google Scholar]
- 38.Prasad AS. Zinc deficiency in patients with sickle cell disease. Am J Clin Nutr. 2002;75:181–182. doi: 10.1093/ajcn/75.2.181. [DOI] [PubMed] [Google Scholar]
- 39.Zemel BS, Kawchak DA, Fung EB, Ohene-Frempong K, Stallings VA. Effect of zinc supplementation on growth and body composition in children with sickle cell disease. Am J Clin Nutr. 2002;75:300–307. doi: 10.1093/ajcn/75.2.300. [DOI] [PubMed] [Google Scholar]
- 40.Zehtabchi S, Sinert R, Rinnert S, Chang B, Heinis C, Altura RA, Altura BT, Altura BM. Serum ionized magnesium levels and ionized calcium-to-magnesium ratios in adult patients with sickle cell anemia. Am J Hematol. 2004;77:215–222. doi: 10.1002/ajh.20187. [DOI] [PubMed] [Google Scholar]
- 41.Oladipo OO, Temiye EO, Ezeaka VC, Obomanu P. Serum magnesium, phosphate and calcium in Nigerian children with sickle cell disease. West Afr J Med. 2005;24:120–123. doi: 10.4314/wajm.v24i2.28180. [DOI] [PubMed] [Google Scholar]
- 42.Okochi VI, Okpurzor J. Micronutrients as therapeutic tools in the management of sickle cell disease, malaria and diabetes. Afr J Biotechnol. 2005;4:1568–1579. [Google Scholar]
- 43.Das AK. A textbook on medinicinal aspects of Bio-inorganic Chemistry. 1st edition CBS Publishers and Distributors India. 1990, 5-9.
- 44.Jang JE, Hidalgo A, Frenette PS. Intravenous immunoglobulins modulate neutrophil activation and vascular injury through FcgammaRIII and SHP-1. Circ Res. 2012;110:1057–1066. doi: 10.1161/CIRCRESAHA.112.266411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Chang J, Patton JT, Sarkar A, Ernst B, Magnani JL, Frenette PS. GMI-1070, a novel pan-selectin antagonist, reverses acute vascular occlusions in sickle cell mice. Blood. 2010;116:1779–1786. doi: 10.1182/blood-2009-12-260513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Williams R, George EO, Wang W. Nutrition assessment in children with sickle cell disease. J Assoc Acad Minor Phys. 1997;8:44–48. [PubMed] [Google Scholar]
- 47.Tangney CC, Phillips G, Bell RA, Fernandes P, Hopkins R, Wu SM. Selected indices of micronutrient status in adult patients with sickle cell anemia (SCA) Am J Hematol. 1989;32:161–166. doi: 10.1002/ajh.2830320302. [DOI] [PubMed] [Google Scholar]
- 48.Klings ES, Farber HW. Role of free radicals in the pathogenesis of acute chest syndrome in sickle cell disease. Respir Res. 2001;2:280–285. doi: 10.1186/rr70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Muskiet FA, Muskiet FD, Meiborg G, Schermer JG. Supplementation of patients with homozygous sickle cell disease with zinc, alpha-tocopherol, vitamin C, soybean oil, and fish oil. Am J Clin Nutr. 1991;54:736–744. doi: 10.1093/ajcn/54.4.736. [DOI] [PubMed] [Google Scholar]
- 50.Jaja SI, Aigbe PE, Gbenebitse S, Temiye EO. Changes in erythrocytes following supplementation with alpha-tocopherol in children suffering from sickle cell anaemia. Niger Postgrad Med J. 2005;12:110–114. [PubMed] [Google Scholar]
- 51.Jaja SI, Ikotun AR, Gbenebitse S, Temiye EO. Blood pressure, hematologic and erythrocyte fragility changes in children suffering from sickle cell anemia following ascorbic acid supplementation. J Trop Pediatr. 2002;48:366–370. doi: 10.1093/tropej/48.6.366. [DOI] [PubMed] [Google Scholar]
- 52.Imaga NA. Phytomedicines and nutraceuticals: alternative therapeutics for sickle cell anemia. Sci World J. 2013;2013:269659. doi: 10.1155/2013/269659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Al-Momen AK. Diminished vitamin B12 levels in patients with severe sickle cell disease. J Intern Med. 1995;237:551–555. doi: 10.1111/j.1365-2796.1995.tb00884.x. [DOI] [PubMed] [Google Scholar]
- 54.Arlet JB, Courbebaisse M, Chatellier G, Eladari D, Souberbielle JC, Friedlander G, de Montalembert M, Prie D, Pouchot J, Ribeil JA. Relationship between vitamin D deficiency and bone fragility in sickle cell disease: a cohort study of 56 adults. Bone. 2013;52:206–211. doi: 10.1016/j.bone.2012.10.005. [DOI] [PubMed] [Google Scholar]
- 55.Hyacinth HI, Gee BE, Hibbert JM. The Role of Nutrition in Sickle Cell Disease. Nutr Metab Insights. 2010;3:57–67. doi: 10.4137/NMI.S5048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Hyacinth HI, Adekeye OA, Yilgwan CS. Malnutrition in Sickle Cell Anemia: Implications for Infection, Growth, and Maturation. J Soc Behav Health Sci. 2013;7. http://scholarworks.waldenu.edu/jsbhs/vol7/iss1/2/ [DOI] [PMC free article] [PubMed]
- 57.Hibbert JM, Creary MS, Gee BE, Buchanan ID, Quarshie A, Hsu LL. Erythropoiesis and myocardial energy requirements contribute to the hypermetabolism of childhood sickle cell anemia. J Pediatr Gastroenterol Nutr. 2006;43:680–687. doi: 10.1097/01.mpg.0000228120.44606.d6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Barden EM, Zemel BS, Kawchak DA, Goran MI, Ohene-Frempong K, Stallings VA. Total and resting energy expenditure in children with sickle cell disease. J Pediatr. 2000;136:73–79. doi: 10.1016/S0022-3476(00)90053-2. [DOI] [PubMed] [Google Scholar]
- 59.Taylor SC, Shacks SJ, Qu Z, Wiley P. Type 2 cytokine serum levels in healthy sickle cell disease patients. J Natl Med Assoc. 1997;89:753–757. [PMC free article] [PubMed] [Google Scholar]
- 60.Singhal A, Parker S, Linsell L, Serjeant G. Energy intake and resting metabolic rate in preschool Jamaican children with homozygous sickle cell disease. Am J Clin Nutr. 2002;75:1093–1097. doi: 10.1093/ajcn/75.6.1093. [DOI] [PubMed] [Google Scholar]
- 61.Strasser F, Bruera ED. Update on anorexia and cachexia. Hematol Oncol Clin North Am. 2002;16:589–617. doi: 10.1016/S0889-8588(02)00011-4. [DOI] [PubMed] [Google Scholar]
- 62.Taylor SC, Shacks SJ, Mitchell RA, Banks A. Serum interleukin-6 levels in the steady state of sickle cell disease. J Interferon Cytokine Res. 1995;15:1061–1064. doi: 10.1089/jir.1995.15.27. [DOI] [PubMed] [Google Scholar]
- 63.Richardson RA, Davidson HI. Nutritional demands in acute and chronic illness. Proc Nutr Soc. 2003;62:777–781. doi: 10.1079/PNS2003302. [DOI] [PubMed] [Google Scholar]
- 64.Laviano A, Renvyle T, Meguid MM, Yang ZJ, Cangiano C, Rossi Fanelli F. Relationship between interleukin-1 and cancer anorexia. Nutrition. 1995;11:680–683. [PubMed] [Google Scholar]
- 65.Turrin NP, Ilyin SE, Gayle DA, Plata-Salaman CR, Ramos EJ, Laviano A, Das UN, Inui A, Meguid MM. Interleukin-1beta system in anorectic catabolic tumor-bearing rats. Curr Opin Clin Nutr Metab Care. 2004;7:419–426. doi: 10.1097/01.mco.0000134373.16557.92. [DOI] [PubMed] [Google Scholar]
- 66.Perboni S, Inui A. Anorexia in cancer: role of feeding-regulatory peptides. Philos Trans R Soc Lond B Biol Sci. 2006;361:1281–1289. doi: 10.1098/rstb.2006.1863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Lemanek KL, Brown RT, Amstrong FD, Hood C, Pegelow C, Woods G. Dysfunctional eating patterns and symptoms of pica in children and adolescents with sickle cell disease. Clin Pediatr (Phila) 2002;41:493–500. doi: 10.1177/000992280204100706. [DOI] [PubMed] [Google Scholar]
- 68.Oniyangi O, Cohall DH. Phytomedicines (medicines derived from plants) for sickle cell disease. Cochrane Database Syst Rev. 2015;4:CD004448. doi: 10.1002/14651858.CD004448.pub5. [DOI] [PubMed] [Google Scholar]
- 69.Connor WE, Lin DS, Thomas G, Ey F, DeLoughery T, Zhu N. Abnormal phospholipid molecular species of erythrocytes in sickle cell anemia. J Lipid Res. 1997;38:2516–2528. [PubMed] [Google Scholar]
- 70.Agoreyo F, Nwanze N. Plasma sodium and potassium changes in sickle cell patients. Int J Genet Mol Biol. 2010;2:14–19. [Google Scholar]
- 71.Bao B, Prasad AS, Beck FW, Snell D, Suneja A, Sarkar FH, Doshi N, Fitzgerald JT, Swerdlow P. Zinc supplementation decreases oxidative stress, incidence of infection, and generation of inflammatory cytokines in sickle cell disease patients. Transl Res. 2008;152:67–80. doi: 10.1016/j.trsl.2008.06.001. [DOI] [PubMed] [Google Scholar]
- 72.Mpiana PT, Mudogo V, Tshibangu DS, Kitwa EK, Kanangila AB, Lumbu JB, Ngbolua KN, Atibu EK, Kakule MK. Antisickling activity of anthocyanins from Bombax pentadrum, Ficus capensis and Ziziphus mucronata: photodegradation effect. J Ethnopharmacol. 2008;120:413–418. doi: 10.1016/j.jep.2008.09.012. [DOI] [PubMed] [Google Scholar]
- 73.Mpiana PT, Ngbolua KN, Bokota MT, Kasonga TK, Atibu EK, Tshibangu DS, Mudogo V. In vitro effects of anthocyanin extracts from Justicia secunda Vahl on the solubility of haemoglobin S and membrane stability of sickle erythrocytes. Blood Transfus. 2010;8:248–254. doi: 10.2450/2009.0120-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Ameh SJ, Tarfa FD, Ebeshi BU. Traditional herbal management of sickle cell anemia: lessons from Nigeria. Anemia. 2012;2012:607436. doi: 10.1155/2012/607436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Ray D, Deshmukh P, Goswami K, Garg N. Antioxidant vitamin levels in sickle cell disorders. Natl Med J India. 2007;20:11–13. [PubMed] [Google Scholar]
- 76.Lachant NA, Tanaka KR. Antioxidants in sickle cell disease: the in vitro effects of ascorbic acid. Am J Med Sci. 1986;292:3–10. doi: 10.1097/00000441-198607000-00001. [DOI] [PubMed] [Google Scholar]
- 77.Silva DG, Belini Junior E, de Almeida EA, Bonini-Domingos CR. Oxidative stress in sickle cell disease: an overview of erythrocyte redox metabolism and current antioxidant therapeutic strategies. Free Radic Biol Med. 2013;65:1101–1109. doi: 10.1016/j.freeradbiomed.2013.08.181. [DOI] [PubMed] [Google Scholar]
- 78.Fasola F, Adedapo K, Anetor J, Kuti M. Total antioxidants status and some hematological values in sickle cell disease patients in steady state. J Natl Med Assoc. 2007;99:891–894. [PMC free article] [PubMed] [Google Scholar]
- 79.Chirico EN, Pialoux V. Role of oxidative stress in the pathogenesis of sickle cell disease. IUBMB Life. 2012;64:72–80. doi: 10.1002/iub.584. [DOI] [PubMed] [Google Scholar]
- 80.Wright D, Reid M, Stennett R. Antioxidant intake in sickle cell disease. Int J Clin Nutr. 2014;2:53–59. [Google Scholar]
- 81.Pace BS, White GL, Dover GJ, Boosalis MS, Faller DV, Perrine SP. Short-chain fatty acid derivatives induce fetal globin expression and erythropoiesis in vivo. Blood. 2002;100:4640–4648. doi: 10.1182/blood-2002-02-0353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Westerman MP, Zhang Y, McConnell JP, Chezick PA, Neelam R, Freels S, Feldman LS, Allen S, Baridi R, Feldman LE, Fung LW. Ascorbate levels in red blood cells and urine in patients with sickle cell anemia. Am J Hematol. 2000;65:174–175. doi: 10.1002/1096-8652(200010)65:2<174::AID-AJH15>3.0.CO;2-T. [DOI] [PubMed] [Google Scholar]
- 83.Tomer A, Kasey S, Connor WE, Clark S, Harker LA, Eckman JR. Reduction of pain episodes and prothrombotic activity in sickle cell disease by dietary n-3 fatty acids. Thromb Haemost. 2001;85:966–974. [PubMed] [Google Scholar]
- 84.Okpala I, Ibegbulam O, Duru A, Ocheni S, Emodi I, Ikefuna A, Umar G, Asinobi I, Madu A, Okoye A, et al. Pilot study of omega-3 fatty acid supplements in sickle cell disease. APMIS. 2011;119:442–448. doi: 10.1111/j.1600-0463.2011.02751.x. [DOI] [PubMed] [Google Scholar]
- 85.Calder PC. Dietary fatty acids and lymphocyte functions. Proc Nutr Soc. 1998;57:487–502. doi: 10.1079/PNS19980073. [DOI] [PubMed] [Google Scholar]
- 86.Ren H, Obike I, Okpala I, Ghebremeskel K, Ugochukwu C, Crawford M. Steady-state haemoglobin level in sickle cell anaemia increases with an increase in erythrocyte membrane n-3 fatty acids. Prostaglandins Leukot Essent Fatty Acids. 2005;72:415–421. doi: 10.1016/j.plefa.2005.03.005. [DOI] [PubMed] [Google Scholar]
- 87.Ren H, Okpala I, Ghebremeskel K, Ugochukwu CC, Ibegbulam O, Crawford M. Blood mononuclear cells and platelets have abnormal fatty acid composition in homozygous sickle cell disease. Ann Hematol. 2005;84:578–583. doi: 10.1007/s00277-005-1023-7. [DOI] [PubMed] [Google Scholar]
- 88.Abraham DJ, Mehanna AS, Williams FL. Design, synthesis, and testing of potential antisickling agents. 1. Halogenated benzyloxy and phenoxy acids. J Med Chem. 1982;25:1015–1017. doi: 10.1021/jm00351a002. [DOI] [PubMed] [Google Scholar]
- 89.Ogoda Onah J, Akubue PI, Okide GB. The kinetics of reversal of pre-sickled erythrocytes by the aqueous extract of Cajanus cajan seeds. Phytother Res. 2002;16:748–750. doi: 10.1002/ptr.1026. [DOI] [PubMed] [Google Scholar]
- 90.Abdulmalik O, Safo MK, Chen Q, Yang J, Brugnara C, Ohene-Frempong K, Abraham DJ, Asakura T. 5-hydroxymethyl-2-furfural modifies intracellular sickle haemoglobin and inhibits sickling of red blood cells. Br J Haematol. 2005;128:552–561. doi: 10.1111/j.1365-2141.2004.05332.x. [DOI] [PubMed] [Google Scholar]
- 91.Akojie FO, Fung LW. Antisickling activity of hydroxybenzoic acids in Cajanus cajan. Planta Med. 1992;58:317–320. doi: 10.1055/s-2006-961475. [DOI] [PubMed] [Google Scholar]
- 92.Acquaye CT, Young JD, Ellory JC, Gorecki M, Wilchek M. Mode of transport and possible mechanism of action of L-phenylalanine benzyl ester as an anti-sickling agent. Biochim Biophys Acta. 1982;693:407–416. doi: 10.1016/0005-2736(82)90448-5. [DOI] [PubMed] [Google Scholar]
- 93.Nabipour S, Ayu Said M, Hussain Habil M. Burden and nutritional deficiencies in opiate addiction- systematic review article. Iran J Public Health. 2014;43:1022–1032. [PMC free article] [PubMed] [Google Scholar]
- 94.Ballas SK, Marcolina MJ. Determinants of red cell survival and erythropoietic activity in patients with sickle cell anemia in the steady state. Hemoglobin. 2000;24:277–286. doi: 10.3109/03630260008993134. [DOI] [PubMed] [Google Scholar]
- 95.Edwards C, Whitfield K, Sudhakar S, Pearce M, Byrd G, Wood M, Feliu M, Leach-Beale B, DeCastro L, Whitworth E, et al. Parental substance abuse, reports of chronic pain and coping in adult patients with sickle cell disease. J Natl Med Assoc. 2006;98:420–428. [PMC free article] [PubMed] [Google Scholar]
- 96.Borland ML, Clark LJ, Esson A. Comparative review of the clinical use of intranasal fentanyl versus morphine in a paediatric emergency department. Emerg Med Australas. 2008;20:515–520. doi: 10.1111/j.1742-6723.2008.01138.x. [DOI] [PubMed] [Google Scholar]
- 97.Tofukuji M, Metais C, Wang SY, Alper SL, Sellke FW. Clotrimazole is a potent vasodilator of the rat coronary microcirculation. J Surg Res. 1998;77:6–10. doi: 10.1006/jsre.1998.5320. [DOI] [PubMed] [Google Scholar]
- 98.Bocci V. The case for oxygen-ozonetherapy. Br J Biomed Sci. 2007;64:44–49. doi: 10.1080/09674845.2007.11732755. [DOI] [PubMed] [Google Scholar]
- 99.Bocci V, Aldinucci C, Mosci F, Carraro F, Valacchi G. Ozonation of human blood induces a remarkable upregulation of heme oxygenase-1 and heat stress protein-70. Mediators Inflamm. 2007;2007:26785. doi: 10.1155/2007/26785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Hoban MD, Orkin SH, Bauer DE. Genetic treatment of a molecular disorder: gene therapy approaches to sickle cell disease. Blood. 2016;127(7):839–48. doi: 10.1182/blood-2015-09-618587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Pestina TI, Hargrove PW, Zhao H, Mead PE, Smeltzer MP, Weiss MJ, Wilber A, Persons DA. Amelioration of murine sickle cell disease by nonablative conditioning and gamma-globin gene-corrected bone marrow cells. Mol Ther Methods Clin Dev. 2015;2:15045. doi: 10.1038/mtm.2015.45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Caboot JB, Allen JL. Hypoxemia in sickle cell disease: significance and management. Paediatr Respir Rev. 2014;15:17–23. doi: 10.1016/j.prrv.2013.12.004. [DOI] [PubMed] [Google Scholar]
- 103.Friedman M, Wilson M, Lin HC, Chang HW. Updated systematic review of tonsillectomy and adenoidectomy for treatment of pediatric obstructive sleep apnea/hypopnea syndrome. Otolaryngol Head Neck Surg. 2009;140:800–808. doi: 10.1016/j.otohns.2009.01.043. [DOI] [PubMed] [Google Scholar]
- 104.Needleman JP, Setty BN, Varlotta L, Dampier C, Allen JL. Measurement of hemoglobin saturation by oxygen in children and adolescents with sickle cell disease. Pediatr Pulmonol. 1999;28:423–428. doi: 10.1002/(SICI)1099-0496(199912)28:6<423::AID-PPUL7>3.0.CO;2-C. [DOI] [PubMed] [Google Scholar]
- 105.Bellet PS, Kalinyak KA, Shukla R, Gelfand MJ, Rucknagel DL. Incentive spirometry to prevent acute pulmonary complications in sickle cell diseases. N Engl J Med. 1995;333:699–703. doi: 10.1056/NEJM199509143331104. [DOI] [PubMed] [Google Scholar]
- 106.Hsu LL, Batts BK, Rau JL. Positive expiratory pressure device acceptance by hospitalized children with sickle cell disease is comparable to incentive spirometry. Respir Care. 2005;50:624–627. [PubMed] [Google Scholar]
- 107.Kovacic P. Hydroxyurea (therapeutics and mechanism): metabolism, carbamoyl nitroso, nitroxyl, radicals, cell signaling and clinical applications. Med Hypotheses. 2011;76:24–31. doi: 10.1016/j.mehy.2010.08.023. [DOI] [PubMed] [Google Scholar]
- 108.Snyder AR, Zhou J, Deng Z, Lieberman PM. Therapeutic doses of hydroxyurea cause telomere dysfunction and reduce TRF2 binding to telomeres. Cancer Biol Ther. 2009;8:1136–1145. doi: 10.4161/cbt.8.12.8446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Egger G, Liang G, Aparicio A, Jones PA. Epigenetics in human disease and prospects for epigenetic therapy. Nature. 2004;429:457–463. doi: 10.1038/nature02625. [DOI] [PubMed] [Google Scholar]
- 110.Reid ME, El Beshlawy A, Inati A, Kutlar A, Abboud MR, Haynes J, Jr, Ward R, Sharon B, Taher AT, Smith W, et al. A double-blind, placebo-controlled phase II study of the efficacy and safety of 2,2-dimethylbutyrate (HQK-1001), an oral fetal globin inducer, in sickle cell disease. Am J Hematol. 2014;89:709–713. doi: 10.1002/ajh.23725. [DOI] [PubMed] [Google Scholar]
- 111.Steliou K, Boosalis MS, Perrine SP, Sangerman J, Faller DV. Butyrate histone deacetylase inhibitors. Biores Open Access. 2012;1:192–198. doi: 10.1089/biores.2012.0223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Saunthararajah Y, Hillery CA, Lavelle D, Molokie R, Dorn L, Bressler L, Gavazova S, Chen YH, Hoffman R, DeSimone J. Effects of 5-aza-2'-deoxycytidine on fetal hemoglobin levels, red cell adhesion, and hematopoietic differentiation in patients with sickle cell disease. Blood. 2003;102:3865–3870. doi: 10.1182/blood-2003-05-1738. [DOI] [PubMed] [Google Scholar]
- 113.Hebbel RP, Vercellotti GM, Pace BS, Solovey AN, Kollander R, Abanonu CF, Nguyen J, Vineyard JV, Belcher JD, Abdulla F, et al. The HDAC inhibitors trichostatin A and suberoylanilide hydroxamic acid exhibit multiple modalities of benefit for the vascular pathobiology of sickle transgenic mice. Blood. 2010;115:2483–2490. doi: 10.1182/blood-2009-02-204990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Meiler SE, Wade M, Kutlar F, Yerigenahally SD, Xue Y, Moutouh-de Parseval LA, Corral LG, Swerdlow PS, Kutlar A. Pomalidomide augments fetal hemoglobin production without the myelosuppressive effects of hydroxyurea in transgenic sickle cell mice. Blood. 2011;118:1109–1112. doi: 10.1182/blood-2010-11-319137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Ataga KI, Stocker J. Senicapoc (ICA-17043): a potential therapy for the prevention and treatment of hemolysis-associated complications in sickle cell anemia. Expert Opin Investig Drugs. 2009;18:231–239. doi: 10.1517/13543780802708011. [DOI] [PubMed] [Google Scholar]
- 116.Morris CR, Kim HY, Wood J, Porter JB, Klings ES, Trachtenberg FL, Sweeters N, Olivieri NF, Kwiatkowski JL, Virzi L, et al. Sildenafil therapy in thalassemia patients with Doppler-defined risk of pulmonary hypertension. Haematologica. 2013;98:1359–1367. doi: 10.3324/haematol.2012.082065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Qari MH, Aljaouni SK, Alardawi MS, Fatani H, Alsayes FM, Zografos P, Alsaigh M, Alalfi A, Alamin M, Gadi A, Mousa SA. Reduction of painful vaso-occlusive crisis of sickle cell anaemia by tinzaparin in a double-blind randomized trial. Thromb Haemost. 2007;98:392–396. [PubMed] [Google Scholar]
- 118.Katusic ZS, d'Uscio LV, Nath KA. Vascular protection by tetrahydrobiopterin: progress and therapeutic prospects. Trends Pharmacol Sci. 2009;30:48–54. doi: 10.1016/j.tips.2008.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Belfer I, Youngblood V, Darbari DS, Wang Z, Diaw L, Freeman L, Desai K, Dizon M, Allen D, Cunnington C, et al. A GCH1 haplotype confers sex-specific susceptibility to pain crises and altered endothelial function in adults with sickle cell anemia. Am J Hematol. 2014;89:187–193. doi: 10.1002/ajh.23613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Desai PC, Brittain JE, Jones SK, McDonald A, Wilson DR, Dominik R, Key NS, Parise LV, Ataga KI. A pilot study of eptifibatide for treatment of acute pain episodes in sickle cell disease. Thromb Res. 2013;132:341–345. doi: 10.1016/j.thromres.2013.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Hoppe C, Kuypers F, Larkin S, Hagar W, Vichinsky E, Styles L. A pilot study of the short-term use of simvastatin in sickle cell disease: effects on markers of vascular dysfunction. Br J Haematol. 2011;153:655–663. doi: 10.1111/j.1365-2141.2010.08480.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Provan D, Stasi R, Newland AC, Blanchette VS, Bolton-Maggs P, Bussel JB, Chong BH, Cines DB, Gernsheimer TB, Godeau B, et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood. 2010;115:168–186. doi: 10.1182/blood-2009-06-225565. [DOI] [PubMed] [Google Scholar]
- 123.Turhan A, Jenab P, Bruhns P, Ravetch JV, Coller BS, Frenette PS. Intravenous immune globulin prevents venular vaso-occlusion in sickle cell mice by inhibiting leukocyte adhesion and the interactions between sickle erythrocytes and adherent leukocytes. Blood. 2004;103:2397–2400. doi: 10.1182/blood-2003-07-2209. [DOI] [PubMed] [Google Scholar]
- 124.Chang J, Shi PA, Chiang EY, Frenette PS. Intravenous immunoglobulins reverse acute vaso-occlusive crises in sickle cell mice through rapid inhibition of neutrophil adhesion. Blood. 2008;111:915–923. doi: 10.1182/blood-2007-04-084061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Zennadi R, Moeller BJ, Whalen EJ, Batchvarova M, Xu K, Shan S, Delahunty M, Dewhirst MW, Telen MJ. Epinephrine-induced activation of LW-mediated sickle cell adhesion and vaso-occlusion in vivo. Blood. 2007;110:2708–2717. doi: 10.1182/blood-2006-11-056101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Field JJ, Lin G, Okam MM, Majerus E, Keefer J, Onyekwere O, Ross A, Campigotto F, Neuberg D, Linden J, Nathan DG. Sickle cell vaso-occlusion causes activation of iNKT cells that is decreased by the adenosine A2A receptor agonist regadenoson. Blood. 2013;121:3329–3334. doi: 10.1182/blood-2012-11-465963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Kuvibidila S, Baliga BS, Gardner R, Yu L, Warrier R, Velez M, Ode D, Haynes J. Differential effects of hydroxyurea and zileuton on interleukin-13 secretion by activated murine spleen cells: implication on the expression of vascular cell adhesion molecule-1 and vasoocclusion in sickle cell anemia. Cytokine. 2005;30:213–218. doi: 10.1016/j.cyto.2005.01.010. [DOI] [PubMed] [Google Scholar]
- 128.Marangos PJ, Fox AW, Riedel BJ, Royston D, Dziewanowska ZE. Potential therapeutic applications of fructose-1,6-diphosphate. Expert Opin Investig Drugs. 1998;7:615–623. doi: 10.1517/13543784.7.4.615. [DOI] [PubMed] [Google Scholar]
- 129.Wun T, Soulieres D, Frelinger AL, Krishnamurti L, Novelli EM, Kutlar A, Ataga KI, Knupp CL, McMahon LE, Strouse JJ, et al. A double-blind, randomized, multicenter phase 2 study of prasugrel versus placebo in adult patients with sickle cell disease. J Hematol Oncol. 2013;6:17. doi: 10.1186/1756-8722-6-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Beckman JD, Belcher JD, Vineyard JV, Chen C, Nguyen J, Nwaneri MO, O'Sullivan MG, Gulbahce E, Hebbel RP, Vercellotti GM. Inhaled carbon monoxide reduces leukocytosis in a murine model of sickle cell disease. Am J Physiol Heart Circ Physiol. 2009;297:H1243–1253. doi: 10.1152/ajpheart.00327.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Martins VD, Manfredini V, Peralba MC, Benfato MS. Alpha-lipoic acid modifies oxidative stress parameters in sickle cell trait subjects and sickle cell patients. Clin Nutr. 2009;28:192–197. doi: 10.1016/j.clnu.2009.01.017. [DOI] [PubMed] [Google Scholar]
- 132.Pace BS, Shartava A, Pack-Mabien A, Mulekar M, Ardia A, Goodman SR. Effects of N-acetylcysteine on dense cell formation in sickle cell disease. Am J Hematol. 2003;73:26–32. doi: 10.1002/ajh.10321. [DOI] [PubMed] [Google Scholar]
- 133.Niihara Y, Matsui NM, Shen YM, Akiyama DA, Johnson CS, Sunga MA, Magpayo J, Embury SH, Kalra VK, Cho SH, Tanaka KR. L-glutamine therapy reduces endothelial adhesion of sickle red blood cells to human umbilical vein endothelial cells. BMC Blood Disord. 2005;5:4. doi: 10.1186/1471-2326-5-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Brousseau DC, Scott JP, Hillery CA, Panepinto JA. The effect of magnesium on length of stay for pediatric sickle cell pain crisis. Acad Emerg Med. 2004;11:968–972. doi: 10.1111/j.1553-2712.2004.tb00791.x. [DOI] [PubMed] [Google Scholar]
- 135.Ballas SK, Files B, Luchtman-Jones L, Benjamin L, Swerdlow P, Hilliard L, Coates T, Abboud M, Wojtowicz-Praga S, Grindel JM. Safety of purified poloxamer 188 in sickle cell disease: phase I study of a non-ionic surfactant in the management of acute chest syndrome. Hemoglobin. 2004;28:85–102. doi: 10.1081/HEM-120035919. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the writing of this review-article.