

Abstract
INTRODUCTION:
Occupational stress is a main problem of healthcare workers, which significantly affects their professional and personal performance. The aim of this study was to determine the impact of a stress immunization program on occupational stress of midwives working in health centers.
MATERIALS AND METHODS:
In this quasi-experimental study, 80 midwives working in health centers of Zahedan (2017) were divided into test and control groups based on random allocation. The intervention involved a stress immunization program consisting of two workshops (each lasting 4 h) in two consecutive weeks, which was implemented for the intervention group. As data collection tool, Health and Safety Executive Occupational Stress Questionnaire was completed in three steps before, immediately after, and 1 month after the intervention. Data were analyzed using descriptive and analytical statistics, independent t-test, and repeated measures ANOVA.
RESULTS:
The findings showed that mean stress score in the intervention group was increased from 79.5 ± 9.7 before intervention to 104.5 ± 17.3 immediately after it, which was increased to 110.5 ± 18.3 1 month after intervention (P < 0.001). In the control group, mean stress score was decreased immediately after as well as 1 month after the intervention, which was statistically significant after the intervention and 1 month after it (P > 0.023).
CONCLUSION:
The stress immunization program is an inexpensive and effective way to reduce the stress of midwives; therefore, it is suggested to be used to effectively handle occupational stress among midwives and to improve their quality of care.
Keywords: Midwife, occupational stress, stress immunization program
Introduction
Occupational stress is stress which created by a particular individual in a certain job position. In fact, occupational stress is the stress in which an interaction between working conditions and the characteristics of the employed person is such that the workplace demands and their associated pressures are higher than the ability of that person to cope with them.[1]
Occupational stress occurs when job requirements do not match the abilities, resources, or needs of employees.[2] Several studies have indicated that the jobs dealing with people's health are among stressful jobs.[3] This stress is much more sensitive among midwifery and nursing professions, which account for >80% of direct care of patients.[4] In the field of healthcare jobs, researchers believe that stress can reduce the quality of care and treatment and even pose risks to countless lives in hospitals. In addition, clinics cause individual discomfort, leading to problems such as decreased aptitude, if the occupational stress persists.[5,6]
The Health Transformation Plan is a strategy to improve health systems in Iran, which began in health centers and hospitals affiliated with the Ministry of Health in 2014. The reform in health system is implemented using three approaches as follows: protecting people in terms of finance, creating equity in access to health services, and improving the quality of services. Midwives are among the most important providers of health services in this plan. In addition to tasks such as caring for pregnant women, children under the 6 years, and nonpregnant women, midwives are entrusted with tasks such as the completion of electronic health record (SIB system) as well as care of adolescents, youngsters, adults, and the elderly.[7]
To reduce work stress, various methods such as relaxation, social, and managerial support have been applied to promote the mental health of the staff. These approaches have been effective in reducing stress, but these treatments are mainly concerned with inhibiting stress after its development.[8] Training is another approach to reduce work stress which ultimately improves the quality of life.[9] There are various educational methods to train midwives and nurses in clinical settings, but it is obvious that the techniques being trained should be straightforward and practical to have a favorable outcome.[10]
Several studies have investigated the effectiveness of various methods on reduction of occupational stress, including Hosseini et al., Sarid et al., and Michalsen et al. (2005).[11,12,13] However, in the study of Delvaux et al. (2004), there was no change in occupational stress following training of communication skills.[14]
The problem of occupational stress prevails among nurses despite several educational interventions to control it. Selection of the most effective training method based on skills, abilities, and active participation of learners has been recently reported as one of the most important principles of education.[15] Stress immunization is among these methods which the clients are encouraged to consider stressful conditions as a threat to themselves to be solved. Flexibility, which causes this method to be applicable in different groups within different periods, is the most important feature of this program that distinguishes it from other stress control techniques.[16]
Stress inoculation training program has been used for prevention and treatment in several clinical and nonclinical groups.[16] In a study conducted by Rahgooy et al. (2004), a stress immunization approach was associated with reduced stress among nurses.[17] However, in the study of Kawaharada et al., the mean of variations in response to occupational stress was not significant.[18]
Review of studies on occupational stress revealed that the prevalence of occupational stress was relatively high among different working groups. Given that midwifery is an important profession aimed at maintaining and promoting community health, physical health, and mental well-being of people working in this job can have a significant effect on their performance.[5,6] Midwives have been renamed as healthcare providers, which coupled with the high volume of work, insufficient salary, and benefits associated with this level of work is a major cause of occupational stress among midwives working in health centers. Furthermore, according to a pilot study by the researcher about the occupational stress rate of midwives working in health centers in Zahedan, in the healthcare reform program at the beginning of 1396, it was found that 61.3% of midwives in centers with moderate stress were severely affected.
Therefore, considering the importance of maintaining mental health and optimal recruitment of healthy and qualified midwives to enhance the quality of care, as well as lack of a research on occupational stress among midwives working in healthcare centers, the researcher aimed to conduct a study evaluating stress training on occupational stress of midwives working in healthcare centers.
Materials and Methods
This is a quasi-experimental study on two groups with pretest-posttest design conducted on 80 midwives working in healthcare clinics of Zahedan in 2017. Based on the study of Darban et al.[8] and the following two-group formula, the sample size was estimated to be 29 in each group with a confidence level of 95% and statistical test power of 90%. To increase the validity of the study, the likelihood of more relative partial generalization, and possible fall, the total sample size in this study was 80 participants divided into two groups of 40.
After approving the research plan, obtaining the approval of the ethics committee of the university with ethics code IR.ZAUMS.REC.1396.113, and also taking the recommendation from the Faculty of Nursing and Midwifery of Zahedan and its submission to health centers, the researcher attended the research environment and handed informed consent forms to midwives meeting the conditions for entering into the study. The samples were selected using simple random sampling. First, with the help of the administrative department, a list of employed and qualified midwives of Zahedan healthcare centers was provided. Then, from among the qualified midwives, the sample size was randomly selected by draw, which was again randomly divided into intervention and control groups. To prevent the dissemination of information, after random allocation of participants to the test and control groups, sampling was first completed in the control group and was then started in the intervention test group.
Inclusion criteria were as follows: age of 22–50 years, holding at least an associate midwifery degree, employment in urban health centers for at least 6 months, not having more than 2 weeks of leave in the past month, not consuming the drugs affecting psyche, not being divorced or having a dead spouse if married, not being pregnant, and not having a history of pregnancy within the past 6 months, not being a student and not experiencing bad or stressful incidents during the past 6 months such as death of first-degree relatives and major changes in living conditions. Exclusion criteria were not attending over 10% of the period of workshops, the occurrence of any incident or stressful event during the course of the study such as pregnancy, leave, or transfer to other clinics, end of employment in the next 2 months, and participation in other stress management workshops.
Afterward, if the inclusion and exclusion criteria were satisfied, the researcher submitted the informed consent form to midwives and explained the purpose of research to them. On the 1st day of intervention, the demographic information form and the Health and Safety Executive (HSE) job stress questionnaire were completed by the research units before beginning the intervention.
The demographic information questionnaire contained 16 questions about personal and occupational characteristics, which was prepared according to research objectives. Occupational Stress Questionnaire included 35 questions in which the respondents were asked to answer questions concerning their occupational stress in seven domains and on a five-point scale (never, rarely, sometimes, often, and always). The scores of questions ranged from 1 to 5. According to this questionnaire, a higher score indicated a lower occupational stress and a lower score was a sign of higher occupational stress. HSE Job Stress Questionnaire was compiled by the UK HSE, was translated by Azad Marzabadi (2010), and its validity and reliability was confirmed. The reliability of questionnaire was confirmed by Cronbach's alpha coefficient of 0.78.[19] In this study, the reliability of Job Stress Questionnaire HSE was justified using internal consistency method by calculating Cronbach's alpha coefficient of 0.81.
Following necessary coordination, the intervention was implemented for the intervention group according to stress immunization phases in two sessions (4 h) over two consecutive weeks by the researcher under supervision of a clinical psychologist in the form of lecture, question and answer, group discussion, and mental imaging using educational tools, board, and PowerPoint. Data collection was done in three stages before the intervention, immediately after intervention, and 1 month after intervention in both groups. The number of members in each training group was 5–10 based on the number of eligible participants and the waiting time of selected individuals from the group. Moreover, the workshop was held at 12–16 pm to prevent disturbing the care of visitors based on the viewpoint of the research team through coordination of research units.
The first session included an explanation of the nature of stress, its consequences and its causes, identification of their common coping skills, relaxation training, and identification of negative thoughts. At the end of the first session, practical assignments were given to the participants during the week. Participants were asked to describe the difference between stress and anxiety, to find the best stress portrait, and to identify the causes of stress encountered during the week. They were also asked to practice relaxation techniques daily. In the second session, cognitive reconstruction and time management techniques were taught. Then, using mental imagery, the participants were encountered a stressful factor and were asked to use the best coping skills against them. The research units were followed up for 1 month after the intervention. During this period, the researcher also contacted the participants of intervention group by phone for follow-up and necessary reinforcement on a 2-weekly basis in compliance with the curriculum. Furthermore, to observe ethical considerations and for the benefit of control group from the content of workshop and retraining points, the inoculation program was conducted for the control group 2 months after the completion of the study in a manner similar to that implemented for the intervention group. To collect information from the control group, the questionnaires were completed on the 1st day. One week later, and 1 month after completing the pretest, the same forms were completed by the participants.
Statistical analysis
In this study, the data were analyzed using SPSS statistical software (version 16, IBM Company Armonk, NY, USA) after collection and encoding. Mean, standard deviation, and frequency distribution table (relative, absolute) were used to describe demographic data and personal characteristics. Chi-square test was used for qualitative variables in terms of homogeneity of the two groups. Independent t-test was used to compare the mean of intervention and control groups. Independent t-test and Chi-square test were used to compare the means of control and intervention groups as well as the frequency of qualitative variables in the two groups, respectively. Repeated-measures ANOVA was used to determine the effectiveness of intervention. 95% of confidence level and α = 0.05 significance level were considered.
Results
In this study, in terms of education, 80% and 90% of research units in intervention and control groups held a bachelor's degree and 17.5% and 7.5% associate midwifery degree, respectively. About 72.5% of research units were married in both immunization and control groups. The mean number of live children in intervention and control groups was 1.38 ± 1.25 and 1.20 ± 1.11, respectively. There were no significant differences between the two groups in terms of underlying variables, and the two groups were homogeneous [Table 1].
Table 1.
Comparison of some demographic characteristics of subjects in intervention and control groups
| Variables | Control, n (%) | Intervention, n (%) | Chi-square test results (P) |
|---|---|---|---|
| Education | |||
| Associate | 3 (7.5) | 7 (17.5) | 0.399 |
| BSc | 36 (90) | 32 (80) | |
| MSc | 1 (2.5) | 1 (2.5) | |
| Total | 40 (50) | 40 (50) | |
| Marital status | |||
| Single | 11 (13.7) | 11 (13.7) | 0.99 |
| Married | 29 (36.3) | 29 (36.3) | |
| Total | 45 (50) | 40 (50) | |
| Employment status | |||
| Corporate | 13 (16.3) | 7 (8.8) | 0.292 |
| Contractual | 9 (11.3) | 10 (12.5) | |
| Contractual-official | 18 (22.5) | 23 (28.7) | |
| Total | 40 (50) | 40 (50) | |
| Distance between residence and workplace | |||
| Distant | 15 (18.8) | 17 (21.3) | 0.916 |
| Near | 25 (31.2) | 23 (28.7) | |
| Total | 40 (50) | 40 (50) | |
| Work experience | |||
| 1-6 years | 17 (21.3) | 10 (12.5) | 0.402 |
| 6-12 years | 10 (12.5) | 13 (16.3) | |
| 12-18 years | 9 (11.3) | 13 (16.3) | |
| Total | 4 (5.0) | 4 (5.0) | |
| 40 (50) | 40 (50) | ||
| Age | 6.10±32.6 | 6.00±34.8* | 0.973** |
*Mean±SD, **Independent t-test. SD=Standard deviation
It should be noted that a higher score indicated a lower level of job stress in this study, and vice versa. There was no statistically significant difference between the two groups in terms of occupational stress in the preintervention stage, and the two groups were homogeneous (P = 0.866). The results of independent t-test showed a significant difference between the two groups in mean scores of occupational stress in the postintervention stage as well as 1 month after the intervention (P = 0.001) [Table 2].
Table 2.
Comparison of mean job stress score among midwives working in health centers between intervention and control groups in the pre- and post-intervention stages as well as 1 month after intervention
| Job stress score | Group | Independent t-test result (P, t) | |||
|---|---|---|---|---|---|
| Control | Intervention | ||||
| n | Mean±SD | n | Mean±SD | ||
| Before intervention | 40 | 80.8±10.1 | 40 | 79.5±9.7 | 0.866, 0.169 |
| Immediately after intervention | 40 | 79.5±10.3 | 40 | 104.7±17.3 | 0.001, −7.845 |
| 1 month after intervention | 40 | 77.0±10.1 | 40 | 110.7±18.3 | 0.001, −7.845 |
| Repeated measures ANOVA results | 40 | <0.001 | 40 | <0.001 | 0.001, −9.907 |
SD=Standard deviation
To determine the effectiveness of the intervention, repeated-measures ANOVA was used, and the sphericity assumption was established (P = 0.1). There was a reciprocal effect between the group and the time (P = 0.001) [Figure 1]; therefore, it was separately evaluated for each group over time [Table 3]. The results showed that in the intervention group, the difference between the mean of the second and third stages with the pretest and the second stage with the third stage was statistically significant and indicates a decrease in the amount of occupational stress after the intervention (P = 0.001).
Figure 1.
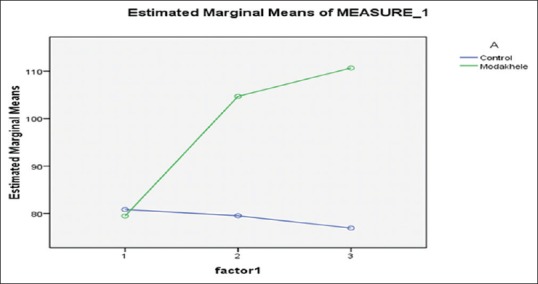
Repeated measurements ANOVA results for occupational stress before, immediately after, and 1 month after intervention in midwives of health centers in intervention and control groups
Table 3.
Repeated measurement ANOVA results in the studied groups
| Groups | Source | S S | df | MS | F | P | Partial η2 |
|---|---|---|---|---|---|---|---|
| Control | Intercept | 750,659.0 | 1 | 750,659.0 | 3.4 | 0.001 | 0.989 |
| Error | 8585.0 | 39 | 220.1 | ||||
| Intervention | Intercept | 1,159,153.6 | 1 | 1,159,153.6 | 3.1 | 0.001 | 0.988 |
| Error | 14,518.3 | 39 | 372.2 |
Comparison of mean stress in preintervention and postintervention stages, as well as follow-up of 1 month later in the intervention group (intra-group comparison) by repeated measures ANOVA, showed a significant difference between the three stages before, immediately and 1 month after the intervention. This test showed a difference between pre- and post-intervention stages (P = 0.001), postintervention of 1 month later (P = 0.033), and preintervention with 1 month later (P = 0.001) [Table 2]. In the control group, repeated-measures ANOVA test results showed a significant difference in mean stress between pre- and post-intervention stages (P = 0.361) as well as between postintervention and 1 month after intervention (P = 0.065), which revealed that the midwives' stress level was not different before the intervention with 1 month after it. Meanwhile, there was a significant difference between mean score of stress in preceding stages with follow-up of 1 month after the intervention (P = 0.023), indicating a significant increase in the level of midwives' stress within 1 month [Figure 2].
Figure 2.
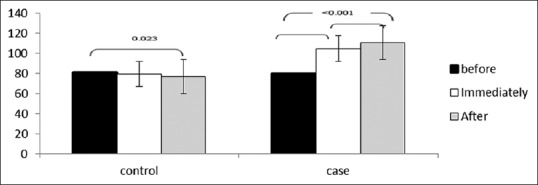
Bonferroni post hoc test results in comparison of means at different times in the two groups
Discussion
The results of this study showed a significant difference between mean scores of occupational stress among midwives in the intervention and control groups 1 week later as well as in follow-up of 1 month later (P = 0.001). Moreover, the results of repeated measures for intra-group comparison revealed that the mean of occupational stress score increased significantly in the intervention group immediately after and 1 month after the intervention; in other words, the stress level of participants was decreased in the intervention test group during the intervention. Meanwhile, the intra-group comparison of means in the control group also showed a significant decrease in mean occupational stress of midwives 1 month after the intervention relative to before it. In the control group, because of high volume of work, the stress of midwives was increased within 1 month, which indicated the need for interventions and programs to reduce the stress level of midwives.
Stress management in Karimyar's study (2015) management was effective in reducing the occupational stress among midwives in comparison to the control group. In the meantime, stress scores in the control group did not change in the three mentioned periods, either. Occupational stress in maternity midwives was not increased within 1 month, and in the intervention group, the significant difference was only observed before and immediately after the intervention, and there was no difference between before intervention and 1 month later, which meant that the management program could not have a lasting effect in reducing stress.[20] In the present study, indicating a decrease in the level of occupational stress and the ability of this method to last for a long time. Perhaps the difference between the two studies is workplace and the level of stress caused by it, the circulation of shifts and thus the lack of contact with the same colleagues in different shifts of the maternity hospital, as well as the Health Transformation Plan of Ministry of Health entailing higher expectations from health centers as the first level of contact with pregnant women. Another reason for this difference may be that in the present research, the researcher contacted the participants of intervention group by phone every 2 weeks during the follow-up period and did necessary follow-up and reinforcement for observing the curriculum.
Mazlum (2011) in a study entitled the impact of an immunization program on perceived stress among nurses working in psychiatry ward that was conducted on 60 nurses working at Ibn Sina Hospital of Mashhad showed that mean stress scores of stress immunization group was increased immediately after and 1 month later; however, mean of stress scores significantly decreased immediately after and 1 month later relative to before intervention.[8] The results of this study were highly consistent with those of the present study. The two studies were similar in terms of method and the difference between the two studies was in their instructors. In the study of Mazlum, a clinical psychologist was recruited who was not familiar with the work environment of nurses, but the researcher who was a midwife and had worked in health centers for a long time and was, therefore, deeply familiar with problems of these centers undertook this task in the present study, which may account for the higher impact observed in this study.
However, the results of Kawaharada et al. evaluating the impact of a stress immunization training program on the stress of civil servants in Japan were not consistent with the present study. Their study showed that mean stress of the intervention group was not significantly reduced after three sessions of intervention.[18] Perhaps the reason for this discrepancy is the difference in sociocultural conditions, workplace position, and life of midwives with servicemen, which has also affected the final results. In addition, the results of our study are not consistent with the study of Heinz (1992), which showed that the immunization program did not significantly change the stress level of high school boys.[21] The reason for the inconsistency of our study with Heinz's research was probably that the mean age of research units in Heinz's study was 15–17 years and that they were single, whereas mean age in this study was 34 years and the participants were mostly married. The results of various studies show that married life is effective in preventing stress if there is a positive relationship with the family as well as increased emotional support.[22]
In the present study, the effect of stress immunization program on perceived stress was reinforced in the follow-up stage 1 month later compared to postintervention stage; although, the difference was not statistically significant. This was probably because during the follow-up period, midwives had the opportunity to apply the skills learned in their real-life environments and consolidated them in their daily routine,[16] which led to the increased effect of intervention over time. Furthermore, according to the results of the present study, the highest level of stress in control group was related to the follow-up period, indicating that not only their stress was not reduced over time, but it was increased. The short duration of follow-up was one of the limitations of this study. Therefore, it is recommended to conduct studies with follow-up period of a few months after the implementation of the training.
Conclusion
Because midwives are one of the major providers of healthcare services, they should be in a good mental and psychological situation to be able to provide care to clients in a desirable manner. Therefore, attention should be paid to the level of occupational stress of midwives. It is suggested that the effect of a stress management program on coping skills, professional performance, and quality of life of midwives working in health centers should be investigated in future studies. In addition, considering the stressfulness of midwifery job and according to the findings of this study, which indicate the low level of familiarity with stress coping methods among midwives working in health centers of Zahedan as well as their interest in stress immunization training programs, it is suggested to design and implement educational intervention programs at comprehensive health centers and even hospitals.
Financial support and sponsorship
The Research Deputy on Zahedan University of Medical Sciences supported this study.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
This paper is based on a student thesis approved by Zahedan University of Medical Sciences (No. 6733). The authors appreciate the University for financial and spiritual support of this project as well as the midwives working in healthcare centers in the city of Zahedan.
References
- 1.Bhui K, Dinos S, Galant-Miecznikowska M, de Jongh B, Stansfeld S. Perceptions of work stress causes and effective interventions in employees working in public, private and non-governmental organisations: A qualitative study. BJPsych Bull. 2016;40:318–25. doi: 10.1192/pb.bp.115.050823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bartram T, Joiner TA, Stanton P. Factors affecting the job stress and job satisfaction of australian nurses: Implications for recruitment and retention. Contemp Nurse. 2004;17:293–304. doi: 10.5172/conu.17.3.293. [DOI] [PubMed] [Google Scholar]
- 3.Giorgi G, Mancuso S, Fiz Perez FJ, Montani F, Courcy F, Arcangeli G. Does leaders' health (and work-related experiences) affect their evaluation of followers' stress? Saf Health Work. 2015;6:249–55. doi: 10.1016/j.shaw.2015.07.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Knezevic B, Milosevic M, Golubic R, Belosevic L, Russo A, Mustajbegovic J. Work-related stress and work ability among croatian university hospital midwives. Midwifery. 2011;27:146–53. doi: 10.1016/j.midw.2009.04.002. [DOI] [PubMed] [Google Scholar]
- 5.Sexton JB, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation: Cross sectional surveys. BMJ. 2000;320:745–9. doi: 10.1136/bmj.320.7237.745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tyler PA, Ellison RN. Sources of stress and psychological well-being in high-dependency nursing. J Adv Nurs. 1994;19:469–76. doi: 10.1111/j.1365-2648.1994.tb01109.x. [DOI] [PubMed] [Google Scholar]
- 7.Ahmadvand AR, Pour Asghari H, Jamshidi HR, Hajimahmoodi H, Hassanzadeh A. Health system reform: Tips for improving health and well-being. Tehran: Big Cultural Institute of Ibn Sina; 2005. [Google Scholar]
- 8.Darban F, Vaghei S, Shad M. The effect of stress inoculation program (SIP) on nurses' perceived stress in psychiatric wards. Evid Based Care. 2012;2:35–44. [Google Scholar]
- 9.van der Klink JJ, Blonk RW, Schene AH, van Dijk FJ. The benefits of interventions for work-related stress. Am J Public Health. 2001;91:270–6. doi: 10.2105/ajph.91.2.270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Taylor C, Lemon P. Fundamentals Nursing: The Art and Science Care. 4th ed. Philadelphia: Lippincott Williams and Wilkins; 2001. pp. 1026–7. [Google Scholar]
- 11.Hosseini Z, Agha Molaee T, Moeini B, Hazavehei MM, Moghimbeigi A. The effect of health education program on female nursses stress. J Health Syst Res. 2015;11:43–52. [Google Scholar]
- 12.Michalsen A, Grossman P, Lehmann N, Knoblauch NT, Paul A, Moebus S, et al. Psychological and quality-of-life outcomes from a comprehensive stress reduction and lifestyle program in patients with coronary artery disease: Results of a randomized trial. Psychother Psychosom. 2005;74:344–52. doi: 10.1159/000087781. [DOI] [PubMed] [Google Scholar]
- 13.Sarid O, Berger R, Segal-Engelchin D. The impact of cognitive behavioral interventions on SOC, perceived stress and mood states of nurses. Procedia Soc Behav Sci. 2010;2:928–32. [Google Scholar]
- 14.Delvaux N, Razavi D, Marchal S, Brédart A, Farvacques C, Slachmuylder JL, et al. Effects of a 105 hours psychological training program on attitudes, communication skills and occupational stress in oncology: A randomised study. Br J Cancer. 2004;90:106–14. doi: 10.1038/sj.bjc.6601459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Saghravanian M. The Effect of Programmed Instruction and Lecture on Students Cognetive Domain. Mashhad: Nursing and Midwifery Faculty, University of Medical Science; 2003. [Google Scholar]
- 16.Meichenbaum D. Stress inoculation training: A preventative and treatment approach. In: Lehrer PM, Woolfolk RL, Sime WS, editors. University of Waterloo, OntarioCanada: Guiford Press; 2007. [Google Scholar]
- 17.Rahgooy A, Fallahi Khshknab M, Karimloo M, Gaeeni M. The effect of application method of stress inoculation on stress of nurses. J Rehabil. 2004;7:61–5. [Google Scholar]
- 18.Kawaharada M, Yoshioka E, Saijo Y, Fukui T, Ueno T, Kishi R. The effects of a stress inoculation training program for civil servants in Japan: A pilot study of a non-randomized controlled trial. Ind Health. 2009;47:173–82. doi: 10.2486/indhealth.47.173. [DOI] [PubMed] [Google Scholar]
- 19.Marzabadi A, Gholami Fesharaki M. Reliability and Validity Assessment for the HSE Job Stress Questionnaire. Journal of Behavioral Sciences. 2011;4(4):291–297. [Google Scholar]
- 20.Karimyar Jahromi M, Minaei S, Abdollahifard S, Maddahfar M. The effect of stress management on occupational stress and satisfaction among midwives in obstetrics and gynecology hospital wards in Iran. Glob J Health Sci. 2016;8:54170. doi: 10.5539/gjhs.v8n9p91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hains AA. A stress inoculation training program for adolescents in a high school setting: A multiple baseline approach. J Adolesc. 1992;15:163–75. doi: 10.1016/0140-1971(92)90045-7. [DOI] [PubMed] [Google Scholar]
- 22.Glasberg AL, Eriksson S, Norberg A. Burnout and ‘stress of conscience’ among healthcare personnel. J Adv Nurs. 2007;57:392–403. doi: 10.1111/j.1365-2648.2007.04111.x. [DOI] [PubMed] [Google Scholar]