

Abstract
Background
Intradialytic hypotension (IDH) is a common complication of haemodialysis (HD), and a risk factor of cardiovascular morbidity and death. Several clinical studies suggested that reduction of dialysate temperature, such as fixed reduction of dialysate temperature or isothermal dialysate using a biofeedback system, might improve the IDH rate.
Objectives
This review aimed to evaluate the benefits and harms of dialysate temperature reduction for IDH among patients with chronic kidney disease requiring HD, compared with standard dialysate temperature.
Search methods
We searched Cochrane Kidney and Transplant's Specialised Register up to 14 May 2019 through contact with the Information Specialist using search terms relevant to this review. Studies in the Register are identified through searches of CENTRAL, MEDLINE, EMBASE, conference proceedings, the International Clinical Trials Register (ICTRP) Search Portal, and ClinicalTrials.gov.
Selection criteria
All randomised controlled trials (RCTs), cross‐over RCTs, cluster RCTs and quasi‐RCTs were included in the review.
Data collection and analysis
Two authors independently extracted information including participants, interventions, outcomes, methods of the study, and risks of bias. We used a random‐effects model to perform quantitative synthesis of the evidence. We assessed the risks of bias for each study using the Cochrane ’Risk of bias’ tool. We assessed the certainty of evidence using Grades of Recommendation, Assessment, Development and Evaluation (GRADE).
Main results
We included 25 studies (712 participants). Three studies were parallel RCTs and the others were cross‐over RCTs. Nineteen studies compared fixed reduction of dialysate temperature (below 36°C) and standard dialysate temperature (37°C to 37.5°C). Most studies were of unclear or high risk of bias. Compared with standard dialysate, it is uncertain whether fixed reduction of dialysate temperature improves IDH rate (8 studies, 153 participants: rate ratio 0.52, 95% CI 0.34 to 0.80; very low certainty evidence); however, it might increase the discomfort rate compared with standard dialysate (4 studies, 161 participants: rate ratio 8.31, 95% CI 1.86 to 37.12; very low certainty evidence). There were no reported dropouts due to adverse events. No study reported death, acute coronary syndrome or stroke.
Three studies compared isothermal dialysate and thermoneutral dialysate. Isothermal dialysate might improve the IDH rate compared with thermoneutral dialysate (2 studies, 133 participants: rate ratio 0.68, 95% CI 0.60 to 0.76; I2 = 0%; very low certainty evidence). There were no reports of discomfort rate (1 study) or dropouts due to adverse events (2 studies). No study reported death, acute coronary syndrome or stroke.
Authors' conclusions
Reduction of dialysate temperature may prevent IDH, but the conclusion is uncertain. Larger studies that measure important outcomes for HD patients are required to assess the effect of reduction of dialysate temperature. Six ongoing studies may provide much‐needed high quality evidence in the future.
Plain language summary
Dialysate temperature reduction for intradialytic hypotension for people with chronic kidney disease requiring haemodialysis
What is the issue?
An increasing number of patients with chronic kidney disease need haemodialysis (HD). When the kidneys are not able to remove enough waste from the blood, HD is used to clean the blood and to remove the excess water via a dialysis machine. Intradialytic hypotension (IDH) is a common complication of HD that is characterized by a sudden drop in blood pressure (BP) with hypotensive symptoms such as dizziness, weakness, nausea, and fatigue, and is a risk factor of cardiovascular morbidity and mortality. In general, a decrease in body temperature is associated with contraction of vessels, and an increase in BP. However, the widely used dialysate temperature is 37°C, and the body temperature is likely to increase during standard dialysis. Removal of heat with cool dialysate might be beneficial to haemodynamic stability. Additionally, fixed empirical reduction of dialysate temperature is simple and easy to adopt in daily practice, however it can increase patient discomfort such as cold sensations, shivering, and related symptoms.
What did we do?
We collected all data from studies of patients with CKD requiring HD that reported data on IDH, discomfort rate and other important outcomes. We included 25 studies comprising 712 participants in the review, and performed meta‐analysis to estimate the effect of cooling dialysate.
What did we find?
The quality of included studies was generally very low due to the risk of bias, small sample size, and a lack of information.
We found very low quality evidence that fixed reduction of dialysate temperature decreased the incidence of IDH compared with standard dialysate and increased the discomfort rate. When patient discomfort is minimal, reduction of the dialysate temperature may be an option to reduce IDH. However, no study reported the long‐term outcomes such as death or heart disorders.
Conclusions
There is limited data suggesting that the reduction of dialysate temperature may prevent IDH, but the conclusion is very uncertain. Larger studies that measure important outcomes such as IDH or mortality for HD patients are required to assess the effect of reducing dialysate temperature.
Summary of findings
Background
Description of the condition
Chronic kidney disease (CKD) is a global concern. According to the 2010 Global Burden of Disease study, CKD was ranked 27th in the list of causes of total number of global deaths in 1990 (age‐standardized annual death rate of 15.7 per 100,000), but rose to 18th in 2010 (annual death rate 16.3 per 100,000) (Lozano 2012). The number of end‐stage kidney disease (ESKD) patients receiving renal replacement therapy (RRT) was more than 2 million in 2011, and increased approximately 8% annually (Couser 2011; White 2008). Haemodialysis (HD) is the main modality of RRT, with almost 90% of dialysis patients under maintenance HD (Jain 2012). Patients with maintenance HD gain weight because of their inability to excrete urine. The excess water is removed by ultrafiltration during HD.
Intradialytic hypotension (IDH) is a common complication of HD. There is no consensus on the definition of IDH, but IDH is commonly defined as a drop in blood pressure during dialysis procedure and/or hypotensive symptoms such as dizziness, weakness, nausea, cramps, blurred vision, and fatigue (Assimon 2017; K/DOQI 2005; Santoro 2002). The pathophysiology of IDH is diverse. It could be the result of an inadequate cardiovascular response to the reduction in blood volume that occurs when the ultrafiltration volume is large (Leypoldt 2002). One process may involve an imbalance between a reduced effective circulating volume and the compensatory plasma refilling mechanism, wherein fluid from the interstitial and intracellular space is translocated into the intravascular compartment (Nesrallah 2013). Additionally, IDH can also be induced by several vasoactive substances such as adenosine or nitric oxide, which may be synthesized or released during dialysis (Sulowicz 2006). Recent studies have shown that haemodynamic instability is associated with impaired baroreflex sensitivity; a decrease in asymmetric dimethylarginine (ADMA), a naturally occurring nitric oxide synthase inhibitor, and inadequate vasopressin response (Chesterton 2010; Csiky 2008; Dubin 2011; Thompson 2009). Another study using echocardiography suggests that a blood pressure (BP) drop within a HD session is associated with HD‐induced myocardial stunning (Burton 2009). Repeated decreases in organ perfusion due to IDH can introduce chronic organ injury over time (Nesrallah 2013). Moreover, several studies have shown an association between IDH and cardiovascular morbidity and mortality (Burton 2009; Sands 2014; Shoji 2004; Stefansson 2014; Tisler 2003). IDH is also associated with vascular access thrombosis, dysrhythmias, and mesenteric venous infarction (K/DOQI 2005). Risk factors associated with IDH include old age, female gender, Hispanic ethnicity, long dialysis vintage, high intradialytic weight gain, high dialysis dose, anaemia, diabetes, low predialysis BP, high osmolarity, and high body mass index (Mc Causland 2013; Mc Causland 2015; Sands 2014; Stefansson 2014; K/DOQI 2005).
Description of the intervention
Dialysate is heated by heating elements in the HD machine as the blood temperature decreases through an extracorporeal circuit. The widely used dialysate temperature is 37°C (Daugirdas 2007; K/DOQI 2005; Toth‐Manikowski 2016). The body temperature is likely to increase during standard dialysis with the dialysate temperature of 37°C (Rosales 2000). The dialysis procedure itself affects body temperature regulation. There have been several clinical studies that investigated the effect of reduction of dialysate temperature for haemodynamic stability (Jost 1993; Maggiore 2002; van der Sande 2009; Zitt 2008). A simple intervention for lowering blood temperature is fixed empirical reduction of dialysate temperature. Alternative interventions are implemented by monitoring blood temperature (core temperature) in the arterial and venous bloodline (Selby 2006). This biofeedback system can adjust the dialysate temperature in response to the calculated body temperature and enable the implementation of isothermic dialysis, in which arterial temperature remains unchanged from the patient’s baseline level (van der Sande 2009). In contrast, lower dialysate temperature may cause high frequency of discomfort, a cold sensation, or shivering (K/DOQI 2005).
How the intervention might work
Peripheral and cutaneous vasoconstriction is considered an important component for the ultrafiltration‐induced decrease in blood volume (Schneditz 2003). HD patients tend to be hypovolaemic as ultrafiltration progresses during HD (Bos 2000; Leypoldt 2002). Hypovolaemia causes underfilling in the cardiac chambers, then cardiovascular response increases the arteriolar or venous tone. However, patients with impaired cardiovascular response cannot offset the volume reduction, and suffer a drop in BP (Santoro 2002). In general, a decrease in body temperature is associated with a decrease in blood flow to the compliant cutaneous circulation, an increase in total peripheral resistance, and an increase in BP (Schneditz 2003). One study reported that left ventricular contractility increased during cool dialysis (Levy 1992), while another observed that SBP was higher in the cool dialysate group but core temperature remained stable during dialysis (van der Sande 1999). Removal of heat with cool dialysate might activate autoregulatory mechanisms to preserve core temperature, which results in beneficial haemodynamic stability. In addition, a recent study showed the protective effect of cooling dialysate on dialysis‐induced ischaemic brain injury (Eldehni 2015).
Why it is important to do this review
IDH remains an issue for chronic HD patients. The frequency of IDH was reported as 20% to 30% among patients undertaking HD (Davenport 2008a; Davenport 2008b). In addition, the incidence of IDH is likely to rise because an increasing number of older patients are expected to develop ESKD (K/DOQI 2005). Since IDH could introduce clinically relevant complications such as mortality and cardiovascular morbidity, evaluation of easy, cost‐effective, and safe interventions should be evaluated to address this problem. Reduction of dialysate temperature could be an easy intervention for preventing IDH. The intervention could also be applied to patients in various settings because standard dialysis consoles have a dialysate temperature regulator; therefore, it can be applied universally and reduce the need for nursing involvement (Eldehni 2015; Toth‐Manikowski 2016). Further, no additional cost is needed to conduct fixed reduction of dialysate temperature. While there are various methods of reducing dialysate temperature, optimal temperature or methods of temperature reduction to prevent IDH remain uncertain (Maggiore 2002; Santoro 2002; Selby 2006; Toth‐Manikowski 2016). A recent systematic review has reported the effect of cooling dialysis on IDH; however, the study has several limitations, including non‐reporting of the risk of bias judgment, assessment of the carry‐over effect for the cross‐over studies (if there was IDH in the session before cross‐over, the patients and medical staffs would try to prevent it in the session after cross‐over), exclusion of comparisons between different types of cooling methods, and exclusion of children and modalities other than HD (Mustafa 2016). To that end, we conducted a systematic review of the effects and harms of reduction of dialysate temperature.
Objectives
This review aimed to evaluate the benefits and harms of dialysate temperature reduction for IDH among patients with CKD requiring HD, compared with standard dialysate temperature. In addition, we compared the benefits and harms of different types of dialysate temperature reduction for IDH.
Methods
Criteria for considering studies for this review
Types of studies
We included all published, unpublished and ongoing randomised controlled trials (RCTs) to compare the reduction of dialysate temperature and normal temperature for IDH in HD patients.
Cluster RCTs were eligible if the number of clusters or the average size of each cluster, the outcome data regardless of cluster design for the total number of individuals, and an estimate of intracluster (or intraclass) correlation coefficient (ICC) were available.
We included data from cross‐over RCTs.
We included quasi‐RCTs (RCTs in which allocation to treatment was obtained by alternation, use of alternate medical records, date of birth or other predictable methods) but excluded observational studies. No language restriction was applied.
Types of participants
Inclusion criteria
All patients undergoing maintenance HD, haemofiltration (HF) and haemodiafiltration (HDF) with minimum dialysis vintage of three months.
Exclusion criteria
Patients on peritoneal dialysis
Patients undergoing continuous RRT
Patients undergoing sustained low‐efficiency dialysis (SLED)
Patients undergoing home HD.
Types of interventions
The experimental conditions were any methods of reduction of dialysate temperature. We considered the following comparisons.
Fixed reduction of dialysate temperature (below 36°C) versus standard dialysate temperature (37°C to 37.5°C)
Reduction of core temperature (below 36°C) using a biofeedback device versus standard dialysate temperature (37°C to 37.5°C)
Isothermic dialysis defined as maintenance of core temperature using a biofeedback device versus standard dialysate temperature (37°C to 37.5°C)
Reduction of arterial temperature using a biofeedback device versus fixed reduction of dialysate temperature (below 36°C)
Isothermic dialysis defined as maintenance of artery temperature using a biofeedback device versus fixed reduction of dialysate temperature (below 36°C)
Reduction of arterial temperature using biofeedback device versus isothermic dialysis defined as maintenance of arterial temperature using a biofeedback device
Any other methods of reduction of dialysate temperature versus standard dialysate temperature (37°C to 37.5°C).
Types of outcome measures
Primary outcomes
-
IDH rate (the proportion of dialysis sessions with episodes of IDH during follow‐up) was defined as follows.
Intradialytic decrease in systolic blood pressure (SBP) by 20 mmHg or more, or a decrease in mean arterial pressure (MAP) by 10 mmHg associated with symptoms that include abdominal discomfort, yawning, sighing, nausea, vomiting, muscle cramps, restlessness, dizziness, and anxiety (K/DOQI 2005).
Decrease in SBP by 20 mmHg or more, or in MAP by 10 mmHg or more, associated with a clinical event and the need for nursing intervention (Kooman 2007).
Drop in SBP to < 90 mmHg or an absolute value > 30 mmHg, associated with symptoms of hypotension and lack of response to the supine position, but necessitating resuscitation with intravenous normotonic or hypertonic fluid administration (Tisler 2003).
Decrease in SBP of at least 10 mmHg or a SBP of < 100 mmHg, with symptoms such as cramps, nausea, vomiting, and dizziness (Fortin 2010).
Drop in SBP < 90 mmHg or of at least 20 mmHg with accompanying clinical symptoms (Maheshwari 2015).
Hypotensive episode requiring either saline infusion, lowering of the ultrafiltration rate (UF) or reduction in blood flow during the HD session (Mc Causland 2013).
Intradialytic decrease in SBP by > 30 mmHg to a level of < 90 mmHg (Sands 2014).
40 mmHg drop in SBP (Shoji 2004).
We also accepted criteria that was similar to the above.
Death (all causes)
Discomfort rate defined as a cold sensation, shivering, and related symptoms.
Secondary outcomes
Acute coronary syndrome: diagnosis based on electrocardiographic changes, elevation of enzymes or confirmed during post‐mortem examination.
All strokes: sudden focal neurologic deficit caused by cerebrovascular thrombosis, and categorized as ischaemic, haemorrhagic, or unspecified.
Quality of life (QoL) measured by a validated scale system such as Kidney Disease Quality of Life (KDQoL), or Choices for Healthy Outcomes in Caring for ESRD (CHOICE) Health Experience Questionnaire (CHEQ) (Hays 1994; Wu 2001).
Dropout rate due to adverse events.
Rate of vasoconstrictor use (defined as any use of vasoconstrictor per dialysis session).
Lowest SBP during dialysis. If the authors reported any BP measure other than the lowest SBP during dialysis, we extracted it according to the following hierarchy: i) the lowest mean BP (MBP) during dialysis; ii) SBP at the end of dialysis; iii) MBP at the end of dialysis; iv) mean SBP during dialysis, and v) mean MBP during dialysis.
Lowest body temperature (BT) during dialysis.
Urea clearance‐based dialysis adequacy (Kt/Vurea).
Vascular thrombosis defined as an access that has clotted, without blood flow in patients with arteriovenous fistula or graft.
New onset dysrhythmias.
Mesenteric venous thrombosis.
Post‐HD fatigue measured by a validated scale system such as the Fatigue Severity Scale (Krupp 1989).
Search methods for identification of studies
Electronic searches
We searched the Cochrane Kidney and Transplant Specialised Register up to 14 May 2019 through contact with the Information Specialist using search terms relevant to this review. The Specialised Register contains studies identified from the following sources.
Monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL).
Weekly searches of MEDLINE OVID SP.
Handsearching of kidney‐related journals and the proceedings of major kidney conferences.
Searching of the current year of EMBASE OVID SP.
Weekly current awareness alerts for selected kidney and transplant journals.
Searches of the International Clinical Trials Register (ICTRP) Search Portal and ClinicalTrials.gov.
Studies contained in the Register are identified through searches of CENTRAL, MEDLINE, and EMBASE based on the scope of Cochrane Kidney and Transplant. Details of search strategies, as well as a list of handsearched journals, conference proceedings and current awareness alerts, are available on the Cochrane Kidney and Transplant website.
See Appendix 1 for search terms used in the strategies for this review.
Searching other resources
Reference lists of review articles, relevant studies and clinical practice guidelines.
Letters seeking information about unpublished or incomplete studies to investigators known to be involved in previous studies.
Data collection and analysis
Selection of studies
The search strategy described was used to obtain titles and abstracts of studies that may be relevant to the review. The titles and abstracts were screened independently by two authors, who discarded studies that were not applicable; however, studies and reviews that might include relevant data or information on studies were retained initially. Two authors independently assessed retrieved abstracts and, if necessary, the full text of these studies to determine which studies satisfied the inclusion criteria.
Data extraction and management
Two authors carried out data extraction independently using a structured, pilot‐tested Excel data extraction form. Any disagreements were resolved by discussion with a further author acting as an arbiter. The data extraction form included the following items.
General information: title, authors, year of publication, trial registration number, language, and country.
Study characteristics: design and setting.
Participants: total number, number of each age, sex, and comorbidity.
Interventions and comparisons: types of reduction of dialysate, duration, and co‐intervention.
Outcome: definition of outcomes, number of participants allocated, number of missing participants, number of events (dichotomous outcomes), standard deviation and mean (continuous outcomes).
Risk of bias and publication status.
We translated any studies reported in non‐English language journals before assessment. Where more than one publication of one study existed, we grouped reports together and used the publication with the most complete data in the analyses. Where relevant outcomes were only published in earlier versions, the authors used these data. The authors also highlighted any discrepancies between published versions.
Assessment of risk of bias in included studies
Two authors independently assessed the following items using the risk of bias assessment tool (Higgins 2011) (Appendix 2).
Was there adequate sequence generation (selection bias)?
Was allocation adequately concealed (selection bias)?
-
Was knowledge of the allocated interventions adequately prevented during the study?
Participants and personnel (performance bias)
Outcome assessors (detection bias)
Were incomplete outcome data adequately addressed (attrition bias)?
Are reports of the study free of suggestion of selective outcome reporting (reporting bias)?
Was the study apparently free of other problems that could put it at a risk of bias?
Measures of treatment effect
Dichotomous outcomes results were expressed as risk ratios (RR) with 95% confidence intervals (CI). For rate outcomes, results were expressed as rate ratios with 95% CI. In the case of zero events, we added 0.5 to each count according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Where continuous scales of measurement were used to assess the effects of treatment (BP, body temperature, and heart rate), we used the mean difference (MD).
If the studies included in a review included a mixture of change‐from‐baseline and final value scores, we used the MD method in RevMan according to Chapter 9.4.5.2 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Unit of analysis issues
Cluster randomised studies
For dichotomous data, we applied the design effect and calculated effective sample size and number of events using ICC and the average cluster size, as described in chapter 16.3.5 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
If the ICC was not reported, we used the ICC of similar studies as a substitute. For continuous data, only the sample size was reduced; means and standard deviation remained unchanged (Higgins 2011).
Randomised cross‐over studies
In the protocol, we planned to consider only data from the first period.
However, there was no study that reported first period data, and we could not obtain the data from any included studies by contacting the authors. We therefore used paired data that were potentially affected by carry‐over effects, and judged the risk of bias due to carry‐over effects in the other bias domain.
For multiple‐arm studies, we included all intervention groups that were relevant to the review.
Dealing with missing data
We requested any further information required from the original author by written correspondence (e.g. emailing or writing to corresponding authors) and included any relevant information obtained in this manner in the review. We carefully evaluated important numerical data such as screened, randomised patients as well as intention‐to‐treat, as‐treated and per‐protocol population, and investigated attrition rates, e.g. drop‐outs, losses to follow‐up and withdrawals. The authors also critically appraised issues of missing data and imputation methods (e.g. last‐observation‐carried‐forward) (Higgins 2011).
Assessment of heterogeneity
We first assessed the heterogeneity by visual inspection of the forest plot. Heterogeneity was then analysed using a Chi² test on N‐1 degrees of freedom, with an alpha of 0.10 used for statistical significance, and with the I² test (Higgins 2003). We interpreted the I² values as follows.
0% to 40%: might not be important
30% to 60%: moderate heterogeneity
50% to 90%: might represent substantial heterogeneity
75% to 100%: considerable heterogeneity.
The importance of the observed value of I² depends on the magnitude and direction of treatment effects and the strength of evidence for heterogeneity (e.g. P‐value from the Chi² test, or a CI for I²) (Higgins 2011).
Assessment of reporting biases
We assessed heterogeneity by visual inspection of the forest plot.
If the number of eligible studies was 10 or more, we planned to use Egger’s test to assess the potential existence of reporting bias (Higgins 2011).
Data synthesis
Data were pooled using the random‐effects model.
Subgroup analysis and investigation of heterogeneity
Where possible, we used subgroup analyses for primary outcomes to explore possible sources of heterogeneity. We treated a study as a subgroup with a covariate if more than 80% of the included participants in a study had a covariate. We tested the following subgroups.
Age: children (< 18 years), adults (18 to 75 years), and elderly (≥ 75 years)
Comorbid conditions: history of diabetes mellitus, acute coronary syndrome, IDH, and current use of antihypertensive drugs
Dialysis vintage: < 10 years and ≥ 10 years
Dialysis modality: HD, HF, HDF
-
We performed the following subgroup analysis for IDH outcome:
IDH definition: IDH defined by symptoms or intervention for hypotensive episode (e.g. saline flush, or lowering of the UF), and IDH defined by SBP irrespective of symptoms or intervention
Sensitivity analysis
Where possible, we performed sensitivity analyses in order to explore the influence of the following factors on effect size.
Repeating the analysis excluding unpublished studies
Repeating the analysis restricted to studies with low risk of selection bias (i.e. adequate random sequence generation and random allocation)
Repeating the analysis excluding any very long or large studies to establish how much they dominated the results
Repeating the analysis using a fixed‐effect model instead of random‐effects model
Repeating the analysis restricted to a study protocol that excludes co‐interventions for IDH, such as mannitol, hypertonic saline, or vasoconstrictors.
'Summary of findings' tables
We presented the main results of the review in 'Summary of findings' tables. These tables presented key information concerning the quality of the evidence, the magnitude of the effects of the interventions examined, and the sum of the available data for the main outcomes (Schunemann 2011a). The 'Summary of findings' tables also included an overall grading of the evidence related to each of the main outcomes using the GRADE (Grades of Recommendation, Assessment, Development and Evaluation) approach (GRADE 2008).
The GRADE approach defines the quality of a body of evidence as the extent to which one can be confident that an estimate of effect or association is close to the true quantity of specific interest. The quality of a body of evidence involves consideration of within‐trial risk of bias (methodological quality), directness of evidence, heterogeneity, precision of effect estimates and risk of publication bias (Schunemann 2011b).
We presented the following outcomes in the 'Summary of findings' tables.
Death (all causes)
Acute coronary syndrome
Stroke
IDH rate
Rate of dropout due to adverse events
Discomfort rate.
Results
Description of studies
Results of the search
We identified 67 records. After screening titles and abstracts 52 records potentially met our inclusion criteria and after full‐text review 25 studies (38 records) were included and 7 studies (9 records) were excluded. Four ongoing studies were identified (IRCT201306268140N2; IRCT2016060228219N1; Maheshwari 2015; MY TEMP 2017). One study (Kuhlmann 1996) was potentially eligible but has not been incorporated into the review due to a lack of information. These studies and will be assessed in a future update of this review (Figure 1).
1.
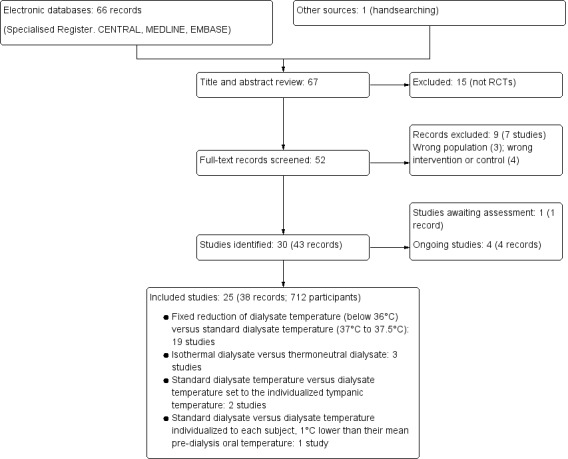
Study flow diagram
Included studies
See Characteristics of included studies.
Study design
Three studies were parallel RCTs (Niyyar 2006; Odudu 2012; Rad 2017) and 22 were cross‐over RCTs.
Sample size
Included studies were mainly small. Samples sizes ranged from 5 to 113 participants. Five studies included 50 or more participants (Ebrahimi 2017; Maggiore 2002; Odudu 2012; Rad 2017; Santoro 2002a).
Setting
Studies were mainly conducted in single centres. Twelve studies did not state the setting of participant recruitment (Beerenhout 2004; Gritters 2005; Manning 1995; Marants 2018; Niyyar 2006; Quereda 1988; Santoro 2002a; Selby 2006b; Shin 1994; Sterrett 1999; van der Sande 2009; Zitt 2008).
Participants
Different types of participants were included in different studies including stable, hypotension‐prone, or those not taking α‐ or β‐adrenergic blocking antihypertensive therapy. Eight studies did not report any eligibility criteria (Manning 1995; Marants 2018; Quereda 1988; Santoro 2002a; Sherman 1984; Sterrett 1999; van der Sande 2000; van der Sande 2001).
Interventions
Nineteen studies compared fixed reduction of dialysate temperature (below 36°C) and standard dialysate temperature (37°C to 37.5°C) (Ayoub 2004; Beerenhout 2004; Ebrahimi 2017; Gritters 2005; Jost 1993; Levy 1992; Manning 1995; Marants 2018; Odudu 2012; Parker 2007; Quereda 1988; Rad 2017; Sajadi 2016; Selby 2006b; Sherman 1984; Shin 1994; van der Sande 2000; van der Sande 2001; Zitt 2008). The differences in the prescribed dialysate temperature in the intervention and the control arms varied from 1°C to 2.2°C. Three studies used a biofeedback device and compared isothermal dialysate and thermoneutral dialysate (Maggiore 2002; Santoro 2002a; van der Sande 2009). In all studies, thermal balance was controlled by means of a Blood Temperature Monitor (BTM; Fresenius Medical Care, Bad Homberg, Germany). Of these, one study also compared reduction of arterial temperature using a biofeedback device, and isothermic dialysate and thermoneutral dialysate (van der Sande 2009). Two studies compared standard dialysate temperature and dialysate temperature set to the individualized tympanic temperature, measured by tympanic thermometer (Jefferies 2011; Sterrett 1999). One study compared standard dialysate and dialysate temperature individualized to each subject, 1°C lower than their mean pre‐dialysis oral temperature (Niyyar 2006).
Outcomes
We requested further information, including the first phase data of cross‐over studies such as baseline characteristics or outcomes, from the corresponding authors. The data were no longer available for Niyyar 2006, and we received no response from any other authors (Ayoub 2004; Beerenhout 2004; Ebrahimi 2017; Gritters 2005; Jefferies 2011; Jost 1993; Levy 1992; Maggiore 2002; Parker 2007; Quereda 1988; Sajadi 2016; Santoro 2002a; Selby 2006b; Sherman 1984; Shin 1994; Sterrett 1999; van der Sande 2000; van der Sande 2001; van der Sande 2009; Zitt 2008). The following reported outcomes included data based on paired comparisons.
IDH: 10 studies (286 participants) (Ayoub 2004; Ebrahimi 2017; Gritters 2005; Jost 1993; Levy 1992; Maggiore 2002; Quereda 1988; Selby 2006b; Sherman 1984; van der Sande 2009). The definition of IDH varied across studies. Five studies used the definition of a fall of systolic BP below 90 to 100 mmHg or a decrease of systolic BP by more than 10 mmHg, accompanied with hypotensive symptoms (Ayoub 2004; Jost 1993; Maggiore 2002; Sherman 1984; van der Sande 2009). Two studies defined IDH as systolic blood pressure < 90 mmHg irrespective of symptoms (Levy 1992; Quereda 1988), and two studies used a composite of those definitions above (Ebrahimi 2017; Selby 2006b). Gritters 2005 did not describe the definition of IDH
Discomfort rate due to cool dialysate: 7 studies (189 participants) (Ayoub 2004; Ebrahimi 2017; Jefferies 2011; Sajadi 2016; Selby 2006b; van der Sande 2000; van der Sande 2009).
QoL: one study (10 participants) examined QoL (Selby 2006b)
Dropout rate due to adverse events: 12 studies (412 participants) (Beerenhout 2004; Ebrahimi 2017; Jefferies 2011; Jost 1993; Levy 1992; Maggiore 2002; Odudu 2012; Parker 2007; Quereda 1988; Rad 2017; Selby 2006b; van der Sande 2009)
Blood pressure: 18 studies (415 participants) (Ayoub 2004; Beerenhout 2004; Ebrahimi 2017; Gritters 2005; Jefferies 2011; Jost 1993; Levy 1992; Manning 1995; Maggiore 2002; Parker 2007; Quereda 1988; Selby 2006b; Sherman 1984; Shin 1994; Sterrett 1999; van der Sande 2000; van der Sande 2001; van der Sande 2009; Zitt 2008).
Body temperature: 8 studies (205 participants) (Ayoub 2004; Beerenhout 2004; Jefferies 2011; Jost 1993; Maggiore 2002; van der Sande 2000; van der Sande 2001; van der Sande 2009).
Kt/Vurea: 2 studies (Ayoub 2004; Maggiore 2002).
Death (all causes), acute coronary syndrome, or all strokes were no reported by any of the included studies.
Excluded studies
Seven studies were excluded (see Characteristics of excluded studies).
Two studies (Lima 2006; Lima 2012) were of participants with acute kidney injury and one study (NCT02593526) was of HD‐naive participants. One study had a co‐intervention other than dialysate temperature in the intervention group (Veljancic 2011): one study (Maggiore 1987) compared standard dialysate and warmer dialysate, one study (Dheenan 2001) compared cold dialysate and different sodium concentration, and one study (Hecking 2012a) used blood volume‐monitored regulation as an intervention.
Risk of bias in included studies
Most studies were of unclear or high risk of bias. See Figure 2 and Figure 3.
2.
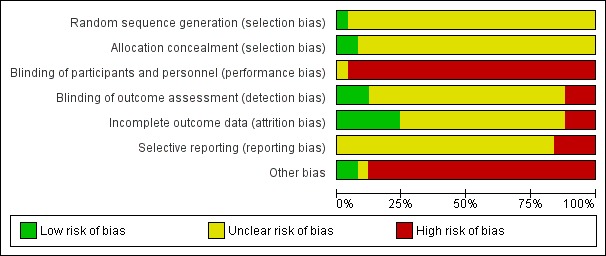
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
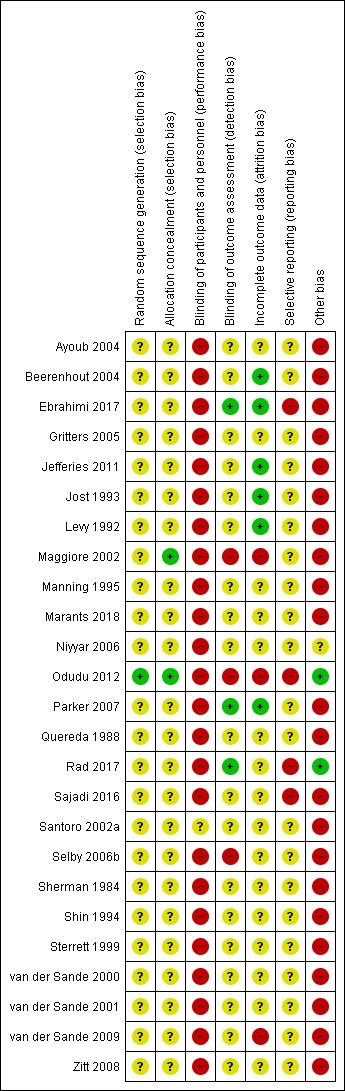
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Random sequence generation
One study (Odudu 2012) used a computer‐generated random sequence. The other studies gave no indication or stated only “block randomisation” and were categorized as unclear.
Allocation concealment
One study (Maggiore 2002) used central randomisation, and one study (Odudu 2012) used sealed envelopes. The other studies gave no description and were categorized as unclear.
Blinding
Performance bias
We judged that blinding of the intervention was broken due to the nature of the intervention when studies compared fixed reduction of dialysate temperature (below 36°C) and standard dialysate temperature. Santoro 2002a compared energetically neutral dialysis (a net thermal energy transfer from the dialysate to the blood circuit equal to zero) and thermally neutral dialysis (the pre‐dialysis patient core temperature was constant). This study was categorized as unclear because it was not clear whether the participants were aware of the intervention and there was no description about blinding.
Detection bias
Outcome assessors were blinded in two studies (Ebrahimi 2017; Rad 2017). Three studies were open label and were judged as high risk (Maggiore 2002; Odudu 2012; Selby 2006b). Other studies gave no description and were categorized as unclear.
Incomplete outcome data
Three studies were classified as high risk for incomplete outcomes because of the exclusion of more than 10% of participants from the final analysis (Maggiore 2002; Odudu 2012; van der Sande 2009). Six studies were classified as low risk (Beerenhout 2004; Ebrahimi 2017; Jefferies 2011; Jost 1993; Levy 1992; Parker 2007) as all or almost all participants were followed up, however, it should be noted that the first phase data of these studies were absent. Other studies were categorized as unclear.
Selective reporting
Five studies referred to their protocols (Ebrahimi 2017; Odudu 2012; Rad 2017; Sajadi 2016; Selby 2006b), but one was not accessible because the registry website was archived (Selby 2006b). Four studies with available protocols did not report pre‐defined outcomes, and did not pre‐define the cut‐off or reported outcomes with multiple cut‐offs (Ebrahimi 2017; Odudu 2012; Rad 2017; Sajadi 2016).
Other potential sources of bias
We judged cross‐over RCTs to be at high risk of bias due to the carry‐over effect. Moreover, we could not assess the baseline imbalance because these studies did not report the baseline characteristics classified by the interventions that the participants were allocated to in the first phase of the studies.
Effects of interventions
Summary of findings for the main comparison. Fixed reduction of dialysate temperature compared to standard dialysate temperature for patients requiring haemodialysis.
| Fixed reduction of dialysate temperature compared to standard dialysate temperature for patients requiring haemodialysis | |||||
| Patient or population: patients requiring haemodialysis Setting: dialysis centre Intervention: fixed reduction of dialysate temperature Comparison: standard dialysate temperature | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | |
| Risk with standard dialysate temperature | Risk with fixed reduction of dialysate temperature | ||||
| Intradialytic hypotension rate follow up: median 3 weeks | 251 episodes per 1,000 person‐dialysis session | 131 episodes per 1,000 person‐dialysis session (85 to 201) | RR 0.52 (0.34 to 0.80) | 153 (8) | ⊕⊝⊝⊝ VERY LOW 1 2 |
| Discomfort rate Follow up: median 4 weeks | 25 episodes per 1,000 person‐dialysis session | 208 episodes per 1,000 person‐dialysis session (47 to 928) | Rate ratio 8.31 (1.86 to 37.12) | 81 (4) | ⊕⊝⊝⊝ VERY LOW 1 2 |
| Dropout due to adverse events Follow up: median 3 weeks | Nine studies (268 participants) reported there were no dropouts due to adverse events | ‐ | 268 (9) | Not graded | |
| Death (all causes) | No studies reported the outcome | ‐ | ‐ | ‐ | |
| Acute coronary syndrome | No studies reported the outcome | ‐ | ‐ | ‐ | |
| Stroke | No studies reported the outcome | ‐ | ‐ | ‐ | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). RR: risk ratio; CI: Confidence interval | |||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | |||||
1 Downgraded two levels due to serious risk of bias: all included studies were randomised cross‐over studies and carry‐over effects could be biased the result. Additionally, all studies were rated high or unclear risk of bias in at least four domains
2 Downgraded one level due to serious imprecision: the total sample size included in the analysis were less than optimal information size
Summary of findings 2. Isothermal dialysate compared to thermoneutral dialysate in patients requiring haemodialysis.
| Isothermal dialysate compared to thermoneutral dialysate in patients requiring haemodialysis | |||||
| Patient or population: patients requiring haemodialysis Setting: dialysis centre Intervention: isothermal dialysate Comparison: thermoneutral dialysate | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | |
| Risk with thermoneutral dialysate | Risk with Isothermal dialysate | ||||
| Intradialytic hypotension rate follow up: range 3 to 8 weeks | 410 episodes per 1,000 person‐dialysis session | 279 episodes per 1,000 person‐dialysis session (246 to 312) | Rate ratio 0.68 (0.60 to 0.76) | 133 (2) | ⊕⊝⊝⊝ Very low 1 2 |
| Discomfort rate Follow up: mean 3 weeks | One study reported that none of the patients allocated to isothermal or thermoneutral dialysate experienced shivering | ‐ | 17 (1) | Not graded | |
| Dropout due to adverse event follow up: range 3 to 8 weeks | There were no reported dropouts due to adverse events in the 2 studies | ‐ | 133 (2) | Not graded | |
| Death (all causes) | No study reported the outcome | ‐ | ‐ | ‐ | |
| Acute coronary syndrome | No study reported the outcome | ‐ | ‐ | ‐ | |
| Stroke | No study reported the outcome | ‐ | ‐ | ‐ | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval | |||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | |||||
1 Downgraded two levels due to serious risk of bias: all included studies were randomised cross‐over studies and carry‐over effects could be biased the result. Additionally, all studies were rated high or unclear risk of bias in at least four domains
2 Downgraded one level due to serious imprecision: the total sample size included in the analysis were less than optimal information size
The random effects and fixed effect models gave similar results, therefore only the random effects results have been presented.
See: Table 1 and Table 2 for the main comparisons
Fixed reduction of dialysate temperature versus standard dialysate temperature
Intradialytic hypotension rate
Fixed reduction of dialysate temperature might improve IDH rate compared with standard dialysate (Analysis 1.1 (8 studies, 153 participants): rate ratio 0.52, 95% CI 0.34 to 0.80; I2 = 19%; very low certainty evidence).
1.1. Analysis.
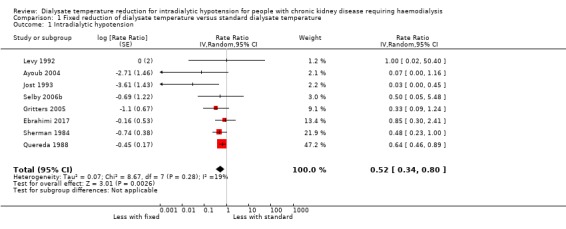
Comparison 1 Fixed reduction of dialysate temperature versus standard dialysate temperature, Outcome 1 Intradialytic hypotension.
Discomfort rate
Fixed reduction of dialysate temperature might increase the discomfort rate compared with standard dialysate (Analysis 1.2 (4 studies, 161 participants): rate ratio 8.31, 95% CI 1.86 to 37.12; I2 = 0%; very low certainty evidence). However, we could not incorporate Ebrahimi 2017 into the meta‐analysis because it did not report the data but only mentioned that the discomfort rate did not differ between the cool dialysate and standard dialysate groups. The discomfort rate in the fixed reduction of the dialysate temperature group varied across the studies and ranged from 6.7% to 34.8%.
1.2. Analysis.
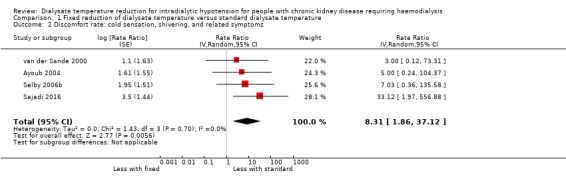
Comparison 1 Fixed reduction of dialysate temperature versus standard dialysate temperature, Outcome 2 Discomfort rate: cold sensation, shivering, and related symptoms.
Death (all causes)
Death was no reported by any of the included studies.
Quality of life
Selby 2006b (10 participants) reported no differences in QoL between fixed reduction and standard dialysate as rated by the SF‐36 questionnaire (median 62 (IQR 50 to 73) with 35°C and median 61 (IQR 39 to 78) with 37°C)
Dropouts due to adverse events
Nine studies (268 participants) reported the number of dropouts, and showed that there were no dropouts due to adverse events (Beerenhout 2004; Ebrahimi 2017; Jost 1993; Levy 1992; Odudu 2012; Parker 2007; Quereda 1988; Rad 2017; Selby 2006b).
Mean blood pressure at the end of haemodialysis
We used mean BP at the end of dialysis because it was the most frequently reported BP measure in the included studies. Fixed reduction of dialysate temperature might improve the mean BP at the end of dialysis (Analysis 1.3 (8 studies, 94 participants): MD 6.46 mmHg, 95% CI 2.84 to 10.08; I2 = 0%; very low certainty evidence).
1.3. Analysis.
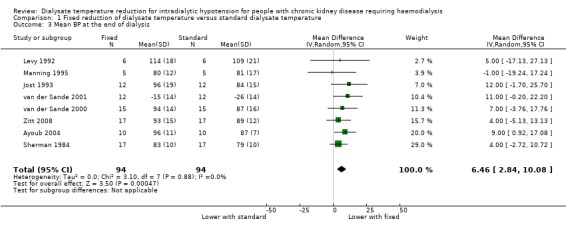
Comparison 1 Fixed reduction of dialysate temperature versus standard dialysate temperature, Outcome 3 Mean BP at the end of dialysis.
All seven studies that did not report the mean BP at the end of dialysis but reported other measures of BP, reported that systolic BP or mean BP was higher in the fixed reduction of dialysate temperature group (Beerenhout 2004; Ebrahimi 2017; Gritters 2005; Parker 2007; Quereda 1988; Selby 2006b; Shin 1994).
Change in body temperature during haemodialysis
We examined change in body temperature during dialysis because the lowest body temperature was not available. Fixed reduction of dialysate temperature might decrease body temperature (Analysis 1.4 (4 studies, 46 participants): MD ‐0.44°C, 95% CI ‐0.56 to ‐0.32; I2 = 0%; very low certainty evidence). We could not incorporate the results from van der Sande 2000 as the data were only presented as a graph (Figure 1, page 1514).
1.4. Analysis.
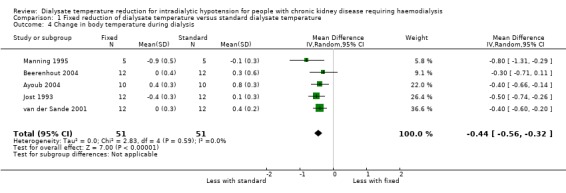
Comparison 1 Fixed reduction of dialysate temperature versus standard dialysate temperature, Outcome 4 Change in body temperature during dialysis.
Urea clearance‐based dialysis adequacy (Kt/Vurea)
Ayoub 2004 reported that there was no significant difference in Kt/Vurea between the cool dialysate and standard dialysate groups.
Post‐haemodialysis fatigue
Sajadi 2016 (46 participants) reported isothermal dialysate might reduce post‐HD fatigue scores using the Piper Fatigue Scale.
Ebrahimi 2017 (80 participants) reported no difference in fatigue between cool dialysate and standard dialysate (data not provided).
Isothermal dialysate versus thermoneutral dialysate
Intradialytic hypotension rate
Isothermal dialysate might improve the IDH rate compared with thermoneutral dialysate (Analysis 2.1 (2 studies, 133 participants): rate ratio 0.68, 95% CI 0.60 to 0.76; I2 = 0%; very low certainty evidence).
2.1. Analysis.
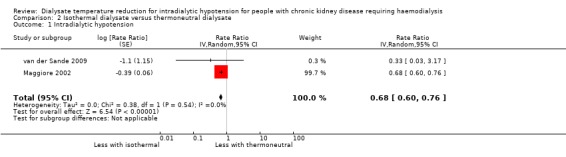
Comparison 2 Isothermal dialysate versus thermoneutral dialysate, Outcome 1 Intradialytic hypotension.
Discomfort rate
Maggiore 2002 (116 participants) reported that none of the participants allocated to isothermal or thermoneutral dialysate experienced shivering.
Death (all causes)
No study reported death.
Dropouts due to adverse events
Two studies (133 participants) reported there were no dropouts due to adverse events (Maggiore 2002; van der Sande 2009).
Changes in systolic blood pressure during haemodialysis
We used change in SBP during dialysis because it was the most frequently reported BP measures in the included studies. Isothermal dialysate might improve SBP during dialysis (Analysis 2.2 (2 studies, 133 participants): MD 6.59 mmHg, 95% CI 2.44 to 10.74; I2 = 0%; very low certainty evidence).
2.2. Analysis.
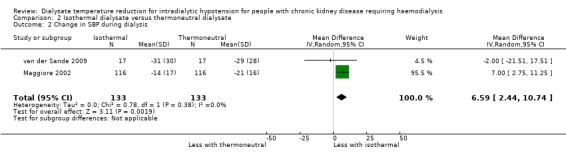
Comparison 2 Isothermal dialysate versus thermoneutral dialysate, Outcome 2 Change in SBP during dialysis.
Change in body temperature during haemodialysis
We examined change in body temperature during dialysis because the lowest body temperature was not available. Isothermal dialysate might decrease the body temperature compared with thermoneutral dialysate (Analysis 2.3 (2 studies, 133 participants); MD ‐0.40°C, 95% CI ‐0.60 to ‐0.21; I2 = 95%; very low certainty evidence).
2.3. Analysis.
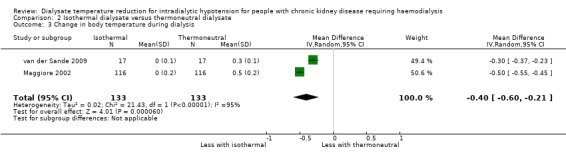
Comparison 2 Isothermal dialysate versus thermoneutral dialysate, Outcome 3 Change in body temperature during dialysis.
Urea clearance‐based dialysis adequacy (Kt/Vurea)
Maggiore 2002 (116 participants) reported isothermal dialysate did not decrease dialysis efficiency.
Reduction of arterial temperature using biofeedback device versus isothermal dialysate
van der Sande 2009 compared reduction of arterial temperature using biofeedback device and isothermal dialysate.
Intradialytic hypotension rate
There were three episodes of hypotension in the cooling group and three episodes in the isothermal group.
Discomfort rate
Three of 17 participants (17.6%) allocated to the reduction of arterial temperature group complained of shivering, however none of the participants allocated to the isothermal dialysate group reported shivering.
Lowest blood pressure during haemodialysis
It was unclear whether reduction of arterial temperature using a biofeedback device improved lowest BP during HD compared with isothermal dialysis.
Other methods of reduction of dialysate temperature versus standard dialysate temperature
Two studies evaluated the effect of dialysate temperature set to the individualized temperature of each individual participant compared with standard dialysate (Jefferies 2011; Sterrett 1999).
One study compared dialysate temperature individualized to each participant 1°C lower than their mean pre‐dialysis oral temperature and standard dialysate temperature (Niyyar 2006).
One study compared reduction of arterial temperature using a biofeedback device with thermoneutral dialysis (van der Sande 2009).
Intradialytic hypotension rate
van der Sande 2009 reported one episode of hypotension in the cooling group and three episodes in the thermoneutral group.
Discomfort rate
van der Sande 2009 reported three patients in the reduction of arterial temperature group complained of shivering and no patients experienced shivering in the thermoneutral group.
Jefferies 2011 reported that 4/11 patients (36.4%) felt cold and used blankets or extra clothing at least once during the week in the individualized temperature group and 1/11 (9.1%) reported shivering, and no patients allocated to standard dialysate experienced discomfort.
Dropouts due to adverse events
Two studies reported that there were no dropouts due to adverse events (Jefferies 2011; van der Sande 2009).
Lowest blood pressure during haemodialysis
Jefferies 2011 and Sterrett 1999 only reported statistical significance or displayed BP in figures. Both studies reported that the SBP was higher among those with a dialysate temperature set to the individualized temperature of each individual patient.
It was unclear whether reduction of arterial temperature using a biofeedback device improved lowest BP during HD compared with thermoneutral dialysis (van der Sande 2009).
Lowest body temperature during haemodialysis
van der Sande 2009 reported reduction of arterial temperature using a biofeedback device might reduce body temperature compared with thermoneutral dialysis.
Jefferies 2011 reported that body temperature was decreased in the group allocated to dialysate temperature set to the individualized temperature of each individual participant, compared with the standard dialysate group (data not provided).
Discussion
Summary of main results
We found very low quality evidence that fixed reduction of dialysate temperature decreased the incidence of IDH compared with standard dialysate and increased the discomfort rate compared with standard dialysate. However, no study reported the long‐term outcomes such as death (all causes) or coronary artery syndrome. Based on very low evidence, isothermal dialysate might reduce the IDH rate without discomfort. It should be noted that these results were not based on parallel comparisons. These results were drawn from comparisons between before and after data from cross‐over studies.
Overall completeness and applicability of evidence
Seventeen of the 23 included studies were conducted over a decade ago. Practice in the treatment of patients undergoing HD has changed significantly over the years, and the difference in practice may lower external validity. Notably, dialysed patients with IDH risk factors such as older age, type II diabetes, and higher dialysate dose are increasing (Mc Causland 2013; National Kidney Foundation 2015; Pippias 2016; Sands 2014). For example, the incidence of patients older than 75 requiring HD has increased in Europe (Pippias 2016). The National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (KDOQI) recommended a target single pool Kt/V (spKt/V) of 1.4/HD session for patients treated three times/week (Mc Causland 2013; National Kidney Foundation 2015). The changes in reimbursement policies might also affect the practice. In 2011, the Centers for Medicare & Medicaid Services (CMS) administered the End‐Stage Renal Disease (ESRD) Quality Incentive Program (QIP) that proposed the target dialysis dose or anaemia level to promote high‐quality care through outpatient dialysis centres (Centers for Medicare & Medicaid Services 2016). In Europe, age at the start of RRT has risen over the last decade and the prevalence of cardiovascular co‐morbidities has decreased, while the prevalence of DM and malignancy has increased (Ceretta 2018).
Additionally, as shown in the Characteristics of included studies table, some studies did not report the eligibility criteria (Manning 1995; Marants 2018; Quereda 1988; Santoro 2002a; Sherman 1984; Sterrett 1999; van der Sande 2000; van der Sande 2001), and most studies did not report whether they used consecutive sampling. We therefore concluded that our evidence had low external validity.
Quality of the evidence
We graded the certainty of the evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (GRADE 2008). As shown in the Table 1, and Table 2 for the main comparison, we rated the overall certainty of evidence in this review as very low because of the serious issues with risks of bias, and the number of participants that comprised quantitative syntheses was less than the optimal information size of 400 (Guyatt 2011). As shown in Figure 3, most studies had high or unclear risks of bias for most domains of the study reporting that we assessed. The design, conduct, and analysis of the included studies were difficult to assess in most studies due to a lack of important methodological detail.
Potential biases in the review process
This review has several limitations. First, the results we have presented were not based on parallel group comparisons but a within‐person comparison. We should note the presence of a carry‐over effect when interpreting the results. For example, if there was an IDH in the first phase, clinicians or medical staff would attempt to prevent the event again. Most studies were cross‐over RCTs and data from the first phase were not available, even though we tried to contact the authors three times. Secondly, as many of the included studies were old, we could not check whether unpublished studies existed, especially those conducted before the compulsory policy of trial registration adopted by the International Committee of Medical Journals in 2004 (De Angelis 2004). Additionally, most studies did not report any information about trial registration. Publication bias might potentially exist even though we performed a comprehensive systematic search strategy of the Cochrane Kidney and Transplant's Specialised Register.
Agreements and disagreements with other studies or reviews
Our findings showed similar results with the findings from a previous systematic review (Mustafa 2016). Cool dialysate might reduce the incidence of IDH, but it might increase the discomfort rate. Additionally, no study reported other serious adverse events, or dropouts due to adverse events. However, most studies that did not report IDH events introduced the effect of cool dialysate on IDH in their background section. From a clinical perspective, IDH events should be routinely noted in medical records, and reported in the publication. The frequency of IDH in the standard dialysate group of the included studies was consistent with previous reports (Davenport 2008a; Davenport 2008b).
Authors' conclusions
Implications for practice.
Fixed reduction of dialysate temperature may be useful to reduce IDH when patient discomfort is minimal. On the other hand, isothermal dialysate may reduce IDH without less discomfort compared with thermoneutral dialysate. However, due to the need to prepare the biofeedback device, it may not be possible to routinely use isothermal dialysate. We should note the conclusion was based on very low certainty evidence. We found six ongoing studies that might provide much‐needed high quality evidence in the future.
Implications for research.
To avoid bias due to the carry‐over effect, a parallel group RCT that evaluates patient‐centred outcomes (e.g. IDH, discomfort rate, or mortality) is warranted. First period data should be presented to permit parallel comparison when cross‐over design is employed. Additionally, evaluations must be carefully planned to ensure that random sequence generation, allocation concealment, and blinding of the outcome assessors are adequate, and sample sizes are appropriate to detect significant effects if they exist.
Acknowledgements
We wish to thank Gail Higgins, the Cochrane Kidney and Transplant Group Information Specialist, for designing our search strategy. The methods section of this review is based on a standard template used by the Cochrane Kidney and Transplant Group. We wish to thank Emma Barber and the Cochrane Japan Centre for assisting with English editing.
The authors are grateful to the following peer reviewers for their time and comments: Swapnil Hiremath (University of Ottawa), Peter Kotanko MD FASN (Renal Research Institute, New York, NY, USA; Icahn School of Medicine at Mount Sinai, New York, NY, USA), Amit X. Garg MD PhD (Professor of Medicine, Epidemiology and Biostatistics, Western University, London, Ontario, Canada; Staff Nephrologist, London Health Sciences Center).
Appendices
Appendix 1. Electronic search strategies
| Database | Search terms |
| CENTRAL |
|
| MEDLINE |
|
| EMBASE |
|
Appendix 2. Risk of bias assessment tool
| Potential source of bias | Assessment criteria |
|
Random sequence generation Selection bias (biased allocation to interventions) due to inadequate generation of a randomised sequence |
Low risk of bias: Random number table; computer random number generator; coin tossing; shuffling cards or envelopes; throwing dice; drawing of lots; minimisation (minimisation may be implemented without a random element, and this is considered to be equivalent to being random). |
| High risk of bias: Sequence generated by odd or even date of birth; date (or day) of admission; sequence generated by hospital or clinic record number; allocation by judgement of the clinician; by preference of the participant; based on the results of a laboratory test or a series of tests; by availability of the intervention. | |
| Unclear: Insufficient information about the sequence generation process to permit judgement. | |
|
Allocation concealment Selection bias (biased allocation to interventions) due to inadequate concealment of allocations prior to assignment |
Low risk of bias: Randomisation method described that would not allow investigator/participant to know or influence intervention group before eligible participant entered in the study (e.g. central allocation, including telephone, web‐based, and pharmacy‐controlled, randomisation; sequentially numbered drug containers of identical appearance; sequentially numbered, opaque, sealed envelopes). |
| High risk of bias: Using an open random allocation schedule (e.g. a list of random numbers); assignment envelopes were used without appropriate safeguards (e.g. if envelopes were unsealed or non‐opaque or not sequentially numbered); alternation or rotation; date of birth; case record number; any other explicitly unconcealed procedure. | |
| Unclear: Randomisation stated but no information on method used is available. | |
|
Blinding of participants and personnel Performance bias due to knowledge of the allocated interventions by participants and personnel during the study |
Low risk of bias: No blinding or incomplete blinding, but the review authors judge that the outcome is not likely to be influenced by lack of blinding; blinding of participants and key study personnel ensured, and unlikely that the blinding could have been broken. |
| High risk of bias: No blinding or incomplete blinding, and the outcome is likely to be influenced by lack of blinding; blinding of key study participants and personnel attempted, but likely that the blinding could have been broken, and the outcome is likely to be influenced by lack of blinding. | |
| Unclear: Insufficient information to permit judgement | |
|
Blinding of outcome assessment Detection bias due to knowledge of the allocated interventions by outcome assessors. |
Low risk of bias: No blinding of outcome assessment, but the review authors judge that the outcome measurement is not likely to be influenced by lack of blinding; blinding of outcome assessment ensured, and unlikely that the blinding could have been broken. |
| High risk of bias: No blinding of outcome assessment, and the outcome measurement is likely to be influenced by lack of blinding; blinding of outcome assessment, but likely that the blinding could have been broken, and the outcome measurement is likely to be influenced by lack of blinding. | |
| Unclear: Insufficient information to permit judgement | |
|
Incomplete outcome data Attrition bias due to amount, nature or handling of incomplete outcome data. |
Low risk of bias: No missing outcome data; reasons for missing outcome data unlikely to be related to true outcome (for survival data, censoring unlikely to be introducing bias); missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups; for dichotomous outcome data, the proportion of missing outcomes compared with observed event risk not enough to have a clinically relevant impact on the intervention effect estimate; for continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes not enough to have a clinically relevant impact on observed effect size; missing data have been imputed using appropriate methods. |
| High risk of bias: Reason for missing outcome data likely to be related to true outcome, with either imbalance in numbers or reasons for missing data across intervention groups; for dichotomous outcome data, the proportion of missing outcomes compared with observed event risk enough to induce clinically relevant bias in intervention effect estimate; for continuous outcome data, plausible effect size (difference in means or standardized difference in means) among missing outcomes enough to induce clinically relevant bias in observed effect size; ‘as‐treated’ analysis done with substantial departure of the intervention received from that assigned at randomisation; potentially inappropriate application of simple imputation. | |
| Unclear: Insufficient information to permit judgement | |
|
Selective reporting Reporting bias due to selective outcome reporting |
Low risk of bias: The study protocol is available and all of the study’s pre‐specified (primary and secondary) outcomes that are of interest in the review have been reported in the pre‐specified way; the study protocol is not available but it is clear that the published reports include all expected outcomes, including those that were pre‐specified (convincing text of this nature may be uncommon). |
| High risk of bias: Not all of the study’s pre‐specified primary outcomes have been reported; one or more primary outcomes is reported using measurements, analysis methods or subsets of the data (e.g. sub‐scales) that were not pre‐specified; one or more reported primary outcomes were not pre‐specified (unless clear justification for their reporting is provided, such as an unexpected adverse effect); one or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta‐analysis; the study report fails to include results for a key outcome that would be expected to have been reported for such a study. | |
| Unclear: Insufficient information to permit judgement | |
|
Other bias Bias due to problems not covered elsewhere in the table |
Low risk of bias: The study appears to be free of other sources of bias. |
| High risk of bias: Had a potential source of bias related to the specific study design used; stopped early due to some data‐dependent process (including a formal‐stopping rule); had extreme baseline imbalance; has been claimed to have been fraudulent; had some other problem. | |
| Unclear: Insufficient information to assess whether an important risk of bias exists; insufficient rationale or evidence that an identified problem will introduce bias. |
Data and analyses
Comparison 1. Fixed reduction of dialysate temperature versus standard dialysate temperature.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Intradialytic hypotension | 8 | Rate Ratio (Random, 95% CI) | 0.52 [0.34, 0.80] | |
| 2 Discomfort rate: cold sensation, shivering, and related symptoms | 4 | Rate Ratio (Random, 95% CI) | 8.31 [1.86, 37.12] | |
| 3 Mean BP at the end of dialysis | 8 | 188 | Mean Difference (IV, Random, 95% CI) | 6.46 [2.84, 10.08] |
| 4 Change in body temperature during dialysis | 5 | 102 | Mean Difference (IV, Random, 95% CI) | ‐0.44 [‐0.56, ‐0.32] |
Comparison 2. Isothermal dialysate versus thermoneutral dialysate.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Intradialytic hypotension | 2 | Rate Ratio (Random, 95% CI) | 0.68 [0.60, 0.76] | |
| 2 Change in SBP during dialysis | 2 | 266 | Mean Difference (IV, Random, 95% CI) | 6.59 [2.44, 10.74] |
| 3 Change in body temperature during dialysis | 2 | 266 | Mean Difference (IV, Random, 95% CI) | ‐0.40 [‐0.60, ‐0.21] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ayoub 2004.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Patients were informed about the temperature of each dialysis session, as they can feel the cool dialysis |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: no description about the first phase data including missing values; dropouts not reported |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: the protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed; no description for the assessment of the baseline imbalance of first period of the cross‐over study |
Beerenhout 2004.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arms
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Sessions were performed in random order": method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Insufficient information to permit judgement: No description about the first phase data including missing values but only 1 participants dropped out |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Ebrahimi 2017.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The researcher was in charge of measuring and recording blood pressure. The data collector and the data analyser were also unaware of this process |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Insufficient information to permit judgement: No description about the first phase data including missing values but there were no dropouts |
| Selective reporting (reporting bias) | High risk | IDH was not a pre‐specified outcome but was reported in the publication |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Gritters 2005.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: no description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Jefferies 2011.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Insufficient information to permit judgement: No description about the first phase data including missing values but there were no dropouts |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Jost 1993.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Insufficient information to permit judgement: No description about the first phase data including missing values but there were no dropouts |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of the first period of the cross‐over study |
Levy 1992.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote "The dialysis procedures were performed in random order..."; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No description about the first phase data including missing values but there were no dropouts |
| Selective reporting (reporting bias) | Unclear risk | The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Maggiore 2002.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
• Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomization was performed centrally in blocks of four patients, and separate randomisation lists were provided for each center." However, there was no description of random sequence generation |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomization was performed centrally in blocks of four patients, and separate randomisation lists were provided for each center." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open‐label study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open‐label study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | More than 15% of participants dropped out (21/116) |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Manning 1995.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Marants 2018.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Niyyar 2006.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment group
Control group
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the missing data |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | Unclear risk | Insufficient information to permit judgement: No description for the assessment of the baseline imbalance |
Odudu 2012.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment group
Control group
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Patients were randomised 1:1 by a computer‐generated sequence placed into sealed envelopes by an independent statistician |
| Allocation concealment (selection bias) | Low risk | Patients were randomised 1:1 by a computer‐generated sequence placed into sealed envelopes by an independent statistician |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Multicentre, prospective, randomised, unblinded, controlled study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Multicentre, prospective, randomised, unblinded, controlled study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 73 patients were enrolled and randomised but 54 patients were analysed |
| Selective reporting (reporting bias) | High risk | IDH was the pre‐specified outcome, but was not reported in the publication |
| Other bias | Low risk | No concern about baseline imbalance |
Parker 2007.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding of key study participants and personnel attempted, but likely that the blinding could have been broken, and the outcome is likely to be influenced by lack of blinding |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The only measured outcome was "dropouts due to adverse events" and no dropouts was occurred |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Quereda 1988.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arms (48 sessions of each)
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Rad 2017.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment group
Control group
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The random permuted block method was used, but there was no description how to generate the random sequence |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The assessors were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: The only measured outcome was "dropouts due to adverse events" and no dropouts occurred |
| Selective reporting (reporting bias) | High risk | Insufficient information to permit judgement: The pruritus outcome was not measured by one of the pre‐specified measures |
| Other bias | Low risk | No concern about the baseline imbalance |
Sajadi 2016.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the first phase data including missing values |
| Selective reporting (reporting bias) | High risk | Primary outcome was reported with multiple cut‐offs |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Santoro 2002a.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
• Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Selby 2006b.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | The outcome assessors were not blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Sherman 1984.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arms
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Shin 1994.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Sterrett 1999.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
van der Sande 2000.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arms
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of the first period of the cross‐over study |
van der Sande 2001.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arms
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
van der Sande 2009.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arms
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | High risk | More than 15% (3/17) of participants were not included in the analysis |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
Zitt 2008.
| Methods |
|
|
| Participants |
|
|
| Interventions | Treatment arm
Control arm
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study was described as randomised; method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding was not feasible because of the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information to permit judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to permit judgement: No description about the first phase data including missing values |
| Selective reporting (reporting bias) | Unclear risk | Insufficient information to permit judgement: The protocol was not available |
| Other bias | High risk | Carry‐over effects potentially existed. No description for the assessment of the baseline imbalance of first period of the cross‐over study |
AKI ‐ acute kidney injury; BP ‐ blood pressure; BT‐ body temperature; Hb ‐ haemoglobin; HCT ‐ haematocrit; HD ‐ haemodialysis; IDH ‐ Intradialytic hypotension; M/F ‐ male/female; MAP ‐ mean arterial pressure; MRI ‐ magnetic resonance imaging; NYHA ‐ New York Heart Association; RCT ‐ randomised controlled trial; SBP ‐ systolic blood pressure; SD ‐ standard deviation; SE; standard error; SEM ‐ standard error of the mean
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Dheenan 2001 | Wrong interventions: cool dialysate versus dialysate with higher sodium concentration |
| Hecking 2012a | Wrong interventions: cool dialysate in combination with blood volume‐monitored regulation |
| Lima 2006 | Wrong population: patients with AKI |
| Lima 2012 | Wrong population: patients with AKI |
| Maggiore 1987 | Wrong interventions: warmer dialysate (39°C to 41°C) versus standard dialysate |
| NCT02593526 | Wrong population: patients were HD naive (Patient may still enrol as long as no more than 12 weeks of in‐centre HD have been performed prior to randomisation) |
| Veljancic 2011 | Wrong interventions: wool dialysate in combination with blood volume monitoring |
AKI ‐ acute kidney injury; HD ‐ haemodialysis
Characteristics of studies awaiting assessment [ordered by study ID]
Kuhlmann 1996.
| Methods |
|
| Participants |
|
| Interventions | Treatment arm
Control arm
|
| Outcomes |
|
| Notes |
|
BT ‐ body temperature; HD ‐ haemodialysis; MAP ‐ mean arterial pressure
Characteristics of ongoing studies [ordered by study ID]
IRCT201306268140N2.
| Trial name or title | Effect of lowering dialysate temperature on the quality of haemodialysis in patients undergoing haemodialysis in 5t Azar hospital |
| Methods | Single‐centre cross‐over RCT |
| Participants | Inclusion criteria
|
| Interventions | In cross‐over study, patients are assessed during 24 dialysis sessions; the first group received HD for 12 sessions using cool dialysate (35.5°C) and the second group is on HD with standard dialysate temperature (37°C). Then the method of treatment is replaced in two groups for the next 12 sessions. Each patient gets dialysis once with routine temperature and once with cool dialysate. Patients are assessed during 24 dialysis sessions; the first group receives HD for 12 sessions using cool dialysate (35.5°C) and the second group is on HD with standard dialysate temperature (37°C). Then the method of treatment is replaced in two groups for the next 12 sessions. During the study, all the dialysis conditions are maintained the same, except temperature of dialysate (37°C or 35.5°C). All patients are on HD using GAMBRO AK96 HD machine |
| Outcomes |
|
| Starting date | 22 June 2013 |
| Contact information | Mollaei Einollah Kilometer 2 Goran‐Sari, Golestan University of Medical Sciences, Gorgan Gorgan Golestan, Islamic Republic of Iran 00981714426900 Mollaei@goums.ac.ir |
| Notes |
IRCT2016060228219N1.
| Trial name or title | Effects of cool dialysate on sleep quality in patients undergoing haemodialysis |
| Methods | Single‐centre cross‐over RCT |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Control
Intervention
|
| Outcomes | No outcome of interest was defined |
| Starting date | 22 Sep 2016 |
| Contact information | |
| Notes |
Maheshwari 2015.
| Trial name or title | Effect of cool vs. warm dialysate on toxin removal: rationale and study design |
| Methods | A single‐centre, randomised cross‐over study |
| Participants | Inclusion criteria
Exclusion criteria
|
| Interventions | Intervention
Control
|
| Outcomes |
|
| Starting date | July 2013 |
| Contact information | Vaibhav Maheshwari LF Dialysis Center, National University Hospital, Singapore, SGN, Singapore, 298135 |
| Notes |
MY TEMP 2017.
| Trial name or title | Major Outcomes With Personalized Dialysate TEMPerature (MyTEMP) |
| Methods | Cluster RCT |
| Participants | Patients undergoing HD in the dialysis centres that meet the following criteria Inclusion criteria
Exclusion criteria
|
| Interventions | Intervention
Control
|
| Outcomes | Primary outcome
Secondary outcomes
|
| Starting date | 3 April, 2017 |
| Contact information | Amit X Garg, London Health Sciences Centre, London, Ontario, Canada, N6A5W9 |
| Notes | Trial registration: NCT02628366 |
HD ‐ haemodialysis; IDH ‐ intradialytic hypotension; RCT ‐ randomised controlled trial
Differences between protocol and review
We attempted to contact study authors to ask for more detail, but they were unable to provide further information, or we were not able to make contact. Information on the outcomes reported was insufficient (e.g. lowest SBP or lowest BT). We therefore were not able to carry out the qualitative analysis as planned. Additionally, we performed quantitative syntheses based on paired data because of a lack of first phase data of cross‐over studies.
Contributions of authors
Drafting the protocol: YT, HT, YN, YK, MK, SS, TI, S Fukuma, YY, S Fukuhara
Study selection: YT, HT
Extracting data from studies: YT, HT
Entering data into RevMan: YT
Carrying out the analysis: YT, YN, YK, MK, YY
Interpreting the analysis: YT, HT, YK, MK, SS, TI, S Fukuma, YY, S Fukuhara
Drafting the final review: YT
Disagreement resolution: YK
Updating the review: YT, HT, YN, YK, MK, SS, TI, S Fukuma, YY, S Fukuhara
Declarations of interest
All authors declare there are no conflicts of interest.
New
References
References to studies included in this review
Ayoub 2004 {published data only}
- Ayoub A, Finlayson M. Effect of cool temperature dialysate on the quality and patients' perception of haemodialysis. Nephrology Dialysis Transplantation 2004;19(1):190‐4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Beerenhout 2004 {published data only}
- Beerenhout C, Dejagere T, Sande FM, Bekers O, Leunissen KM, Kooman JP. Haemodynamics and electrolyte balance: a comparison between on‐line pre‐dilution haemofiltration and haemodialysis. Nephrology Dialysis Transplantation 2004;19(9):2354‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Ebrahimi 2017 {published data only}
- Ebrahimi H, Safavi M, Saeidi MH, Emamian MH. Effects of sodium concentration and dialysate temperature changes on blood pressure in hemodialysis patients: a randomized, triple‐blind crossover clinical trial. Therapeutic Apheresis & Dialysis 2017;21(2):117‐25. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Gritters 2005 {published data only}
- Gritters M, Borgdorff P, Schoorl M, Schoorl M, Grooteman MP, Bartels PC, et al. Effects of cool temperature dialysate on platelet activity in intradialytic hypotension [abstract no: SP311]. Nephrology Dialysis Transplantation 2005;20(Suppl 5):v123‐4. [Google Scholar]
Jefferies 2011 {published data only}
- Jefferies HJ, Burton JO, McIntyre CW. Individualised dialysate temperature improves intradialytic haemodynamics and abrogates haemodialysis‐induced myocardial stunning, without compromising tolerability. Blood Purification 2011;32(1):63‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Jost 1993 {published data only}
- Jost CM, Agarwal R, Khair‐el‐Din T, Grayburn PA, Victor RG, Henrich WL. Effects of cooler temperature dialysate on hemodynamic stability in "problem" dialysis patients. Kidney International 1993;44(3):606‐12. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Levy 1992 {published data only}
- Levy FL, Grayburn PA, Foulks CJ, Brickner ME, Henrich WL. Improved left ventricular contractility with cool temperature hemodialysis. Kidney International 1992;41(4):961‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Maggiore 2002 {published data only}
- Maggiore Q, Pizzarelli F, Santoro A, Panzetta G, Bonforte G, Hannedouche T, et al. The effects of control of thermal balance on vascular stability in hemodialysis patients: results of the European randomized clinical trial. American Journal of Kidney Diseases 2002;40(2):280‐90. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Maggiore Q, Multicentre Study Group on Thermal Balance on Vascular Stability in Hemodialysis (HD) Patients. Multicentre randomized study on the effect of thermal balance on vascular stability in hemodialysis (HD) patients [abstract no: A1473]. Journal of the American Society of Nephrology 1999;10(Program & Abstracts):291A. [CENTRAL: CN‐00626014] [Google Scholar]
Manning 1995 {published data only}
- Manning EC, Cheung JY, Demers LM, Ahsan N. Hemodialysis (HD) hypotension is mediated by cytokines [abstract no: 1659]. Journal of the American Society of Nephrology 1995;6(3):548. [CENTRAL: CN‐00484963] [Google Scholar]
Marants 2018 {published data only}
- Marants R, Qirjazi E, McIntyre C, Lee T. Dialysate cooling during hemodialysis: assessment of liver hemodynamics using CT perfusion imaging [abstract]. Medical Physics 2018;45(6):e638. [EMBASE: 622805409] [Google Scholar]
Niyyar 2006 {published data only}
- Niyyar VD, Parker K, Viswanathan B, Bailey J. Cool dialysate decreases pre‐hemodialysis blood pressure ‐ a new look at an old problem [abstract no: 116]. American Journal of Kidney Diseases 2006;47(4):A47. [CENTRAL: CN‐00671814] [Google Scholar]
- Niyyar VD, Parker KP, Bailey JL. Cool dialysate and pre‐hemodialysis blood pressure ‐ a new look at an old problem [abstract no: F‐PO580]. Journal of the American Society of Nephrology 2006;17(Abstracts):460A. [Google Scholar]
Odudu 2012 {published data only}
- Eldehni MT, Odudu A, McIntyre CW. Randomized clinical trial of dialysate cooling and effects on brain white matter. Journal of the American Society of Nephrology 2015;26(4):957‐65. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- McIntyre CW, Eldehni MT, Odudu A. Prospective randomized controlled trial of individualized dialysate cooling to provide brain and cardiac protection in haemodialysis patients [abstract no: SA‐PO1083]. Journal of the American Society of Nephrology 2013;24(Abstract Suppl):4B. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odudu A, Eldehni MT, Fakis A, McIntyre CW. Rationale and design of a multi‐centre randomised controlled trial of individualised cooled dialysate to prevent left ventricular systolic dysfunction in haemodialysis patients. BMC Nephrology 2012;13:45. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odudu A, Eldehni MT, McCann GP, McIntyre CW. Randomized controlled trial of individualized dialysate cooling for cardiac protection in hemodialysis patients. Clinical Journal of the American Society of Nephrology: CJASN 2015;10(8):1408‐17. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Parker 2007 {published data only}
- Parker KP, Bailey JL, Rye DB, Bliwise DL, Someren EJ. Insomnia on dialysis nights: the beneficial effects of cool dialysate. Journal of Nephrology 2008;21 Suppl 13:S71‐7. [MEDLINE: ] [PubMed] [Google Scholar]
- Parker KP, Bailey JL, Rye DB, Bliwise DL, Someren EJ. Lowering dialysate temperature improves sleep and alters nocturnal skin temperature in patients on chronic hemodialysis. Journal of Sleep Research 2007;16(1):42‐50. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Quereda 1988 {published data only}
- Quereda C, Orofino L, Marcen R, Lamas S, Sabater J, Ortuno J. Contribution of membrane and dialysate to the incidence of hemodialysis (HD)‐induced symptomatic hypotension (SH) [abstract]. 10th International Congress of Nephrology; 1987 Jul 26‐31; London, UK. 1987:167.
- Quereda C, Orofino L, Marcen R, Sabater J, Matesanz R, Ortuno J. Influence of dialysate and membrane biocompatibility on hemodynamic stability in hemodialysis. International Journal of Artificial Organs 1988;11(4):259‐64. [MEDLINE: ] [PubMed] [Google Scholar]
- Quereda C, Orofino L, Marcen R, Sabater J, Ortuno J. Combined use of low temperature and high sodium dialysate improves symptomatic hypotension (SH) in hemodialysis (HD) [abstract]. 24th Annual Congress. EDTA‐ERA; 1987 Oct 25‐29; West Berlin, Germany. 1987:132.
Rad 2017 {published data only}
- Rad M, Jaghouri E, Sharifipour F, Rakhshani MH. The effects of cool dialysate on pruritus status during hemodialysis of patients with chronic renal failure: a controlled randomized clinical trial. Iranian Red Crescent Medical Journal 2017;19(1):e34759. [EMBASE: 614362274] [Google Scholar]
Sajadi 2016 {published data only}
- Sajadi M, Gholami Z, Hekmatpour D, Soltani P, Haghverdi F. Cold dialysis solution for hemodialysis patients with fatigue ‐ a cross‐over study. Iranian Journal of Kidney Diseases 2016;10(5):319‐24. [MEDLINE: ] [PubMed] [Google Scholar]
Santoro 2002a {published data only}
- Santoro A, Mancini E, Gaggi R, Mambelli E. Isothermic dialysis in patients with left ventricular hypertrophy (LVH) and prone to dialysis hypotension (DH) [abstract no: SA‐FC144]. Journal of the American Society of Nephrology 2002;13(September, Program & Abstracts):30A. [CENTRAL: CN‐00447583] [Google Scholar]
- Santoro A, Mancini E, Gaggi R, Mambelli M. Isothermic dialysis in patients with left ventricular hypertrophy (LVH) and prone to dialyis hypotension (DH) [abstract no: O69]. Nephrology Dialysis Transplantation 2002;17(Suppl 12):22. [CENTRAL: CN‐00550548] [Google Scholar]
Selby 2006b {published data only}
- Burton JO, Selby NM, Chesterton LJ, McIntyre CW. Haemodialysis induced myocardial stunning is reduced by the use of cooled dialysate [abstract no: TH‐PO297]. Journal of the American Society of Nephrology 2006;17(Abstracts):170A. [CENTRAL: CN‐00724901] [Google Scholar]
- Chesterton LJ, Selby NM, Burton JO, McIntyre CW. Cool dialysate reduces asymptomatic intradialytic hypotension and increases baroreflex variability. Hemodialysis International 2009;13(2):189‐96. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Selby NM, Burton JO, Chesterton LJ, McIntyre CW. Dialysis‐induced regional left ventricular dysfunction Is ameliorated by cooling the dialysate. Clinical Journal of the American Society of Nephrology: CJASN 2006;1(6):1216‐25. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Sherman 1984 {published data only}
- Sherman RA, Faustino EF, Bernholc AS, Eisinger RP. Effect of variations in dialysate temperature on blood pressure during hemodialysis. American Journal of Kidney Diseases 1984;4(1):66‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Shin 1994 {published data only}
- Shin J, Cronin R, Henrich W. Effects of cooler temperature dialysis (35ºC) on interdialytic blood pressure [abstract no: 58P]. Journal of the American Society of Nephrology 1994;5(3):528. [Google Scholar]
Sterrett 1999 {published data only}
- Sterrett JR, Vitting KE, Gabor EM, Gabor CD, DeBari VA. Prevention of intradialytic hypotension with patient‐temperature dialysate (PTD): a randomized controlled trial [abstract no: A1543]. Journal of the American Society of Nephrology 1999;10(Program & Abstracts):304A. [Google Scholar]
van der Sande 2000 {published data only}
- Sande FM, Gladziwa U, Bocker G, Kooman JP, Leunissen KM. Differences in vascular reactivity between isolated ultrafiltration (I‐UF) and haemodialysis combined with ultrafiltration (UF+HD): comparison between thermal energy balance (TEB) and different dialysate temperatures (TD) [abstract]. Nephrology Dialysis Transplantation 1999;14(9):A203. [CENTRAL: CN‐00486265] [DOI] [PubMed] [Google Scholar]
- Sande FM, Gladziwa U, Kooman JP, Bocker G, Leunissen KM. Energy transfer is the single most important factor for the difference in vascular response between isolated ultrafiltration and hemodialysis. Journal of the American Society of Nephrology 2000;11(8):1512‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
van der Sande 2001 {published data only}
- Sande FM, Kooman JP, Konings CJ, Leunissen KM. Thermal effects and blood pressure response during postdilution hemodiafiltration and hemodialysis: the effect of amount of replacement fluid and dialysate temperature. Journal of the American Society of Nephrology 2001;12(9):1916‐20. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
van der Sande 2009 {published data only}
- Sande FM, Wystrychowski G, Kooman JP, Rosales L, Raimann J, Kotanko P, et al. Control of core temperature and blood pressure stability during hemodialysis. Clinical Journal of the American Society of Nephrology: CJASN 2009;4(1):93‐8. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Zitt 2008 {published data only}
- Zitt E, Neyer U, Meusburger E, Tiefenthaler M, Kotanko P, Mayer G, et al. Effect of dialysate temperature and diabetes on autonomic cardiovascular regulation during hemodialysis. Kidney & Blood Pressure Research 2008;31(4):217‐25. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Zitt E, Neyer U, Meusburger E, Tiefenthaler M, Kotanko P, Mayer G, et al. Influence of diabetes and dialysate temperature on cardiovascular autonomic regulation during hemodialysis [abstract no: MP518]. Nephrology Dialysis Transplantation 2006;21(Suppl 4):iv475. [CENTRAL: CN‐00716135] [Google Scholar]
References to studies excluded from this review
Dheenan 2001 {published data only}
- Dheenan S, Henrich WL. Preventing dialysis hypotension: a comparison of usual protective maneuvers. Kidney International 2001;59(3):1175‐81. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Hecking 2012a {published data only}
- Antlanger M, Josten P, Kammer M, Exner I, Lorenz‐Turnheim K, Eigner M, et al. Blood volume‐monitored regulation of ultrafiltration to decrease the dry weight in fluid‐overloaded hemodialysis patients: a randomized controlled trial. BMC Nephrology 2017;18(1):238. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hecking M, Antlanger M, Winnicki W, Reiter T, Werzowa J, Haidinger M, et al. Blood volume‐monitored regulation of ultrafiltration in fluid‐overloaded hemodialysis patients: study protocol for a randomized controlled trial. Trials [Electronic Resource] 2012;13:79. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lima 2006 {published data only}
- Lima E, Silva R, Fernandes A, Donadi E, Burdmann E. Effects of dialysate temperature, sodium (Na) and ultrafiltration (UF) profiling on intradialytic hypotension (IH) in acute kidney injury (AKI) patients (PTS) [abstract no: SA‐PO926]. Journal of the American Society of Nephrology 2006;17(Abstracts):769A. [Google Scholar]
Lima 2012 {published data only}
- Lima EQ, Silva RG, Donadi EL, Fernandes AB, Zanon JR, Pinto KR, et al. Prevention of intradialytic hypotension in patients with acute kidney injury submitted to sustained low‐efficiency dialysis. Renal Failure 2012;34(10):1238‐43. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Maggiore 1987 {published data only}
- Maggiore Q, Enia G, Catalano C, Misefari V, Mundo A. Effect of blood cooling on cuprophan‐induced anaphylatoxin generation. Kidney International 1987;32(6):908‐11. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
NCT02593526 {published data only}
- Unruh M. Diuretic/cool dialysate trial (DIDIT). www.clinicalTrials.gov/show/NCT02593526 (first received October 20 2015).
Veljancic 2011 {published data only}
- Veljancic L, Popovic J, Radovic M, Ahrenholz P, Ries W, Frenken L, et al. Less complications during haemodialysis by combined blood temperature control and blood volume control [abstract no: SU574]. World Congress of Nephrology; 2009 May 22‐26; Milan, Italy. 2009.
- Veljancic L, Popovic J, Radovic M, Ahrenholz P, Ries W, Frenken L, et al. Simultaneous blood temperature control and blood volume control reduces intradialytic symptoms. International Journal of Artificial Organs 2011;34(4):357‐64. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Kuhlmann 1996 {published data only}
- Kuhlmann U, Hermann W, Schwickardi M, Kramer M, Lange H. Influence of thermal exchange between dialysate and blood on body temperature and circulation during haemodialysis [abstract]. Nephrology Dialysis Transplantation 1996;11(7):1473. [Google Scholar]
References to ongoing studies
IRCT201306268140N2 {published data only}
- Einollah M. Effect of lowering dialysate temperature on the quality of hemodialysis in patients undergoing hemodialysis in 5t Azar hospital. en.irct.ir/trial/8568 (first received 14 July 2017).
IRCT2016060228219N1 {published data only}
- Rad M. Effects of cool dialysate on sleep quality in patients undergoing hemodialysis. en.irct.ir/trial/22936?revision=22936 (first received 30 October 2016).
Maheshwari 2015 {published data only}
- Maheshwari V, Lau T, Samavedham L, Rangaiah GP. Effect of cool vs. warm dialysate on toxin removal: rationale and study design. BMC Nephrology 2015;16:25. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
MY TEMP 2017 {published data only}
- Presseau J, Mutsaers B, Al‐Jaishi AA, Squires J, McIntyre CW, Garg AX, et al. Barriers and facilitators to healthcare professional behaviour change in clinical trials using the Theoretical Domains Framework: a case study of a trial of individualized temperature‐reduced haemodialysis. Trials 2017;18(1):227. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Assimon 2017
- Assimon MM, Flythe JE. Definitions of intradialytic hypotension. Seminars in Dialysis 2017;30(6):464‐72. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bos 2000
- Bos WJ, Bruin S, Olden RW, Keur I, Wesseling KH, Westerhof N, et al. Cardiac and hemodynamic effects of hemodialysis and ultrafiltration. American Journal of Kidney Diseases 2000;35(5):819‐26. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Burton 2009
- Burton JO, Jefferies HJ, Selby NM, McIntyre CW. Hemodialysis‐induced cardiac injury: determinants and associated outcomes. Clinical Journal of The American Society of Nephrology: CJASN 2009;4(5):914‐20. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Centers for Medicare & Medicaid Services 2016
- Centers for Medicare & Medicaid Services. ESRD QIP summary: Payment years 2012 – 2016. www.cms.gov/Medicare/Quality‐Initiatives‐Patient‐Assessment‐Instruments/ESRDQIP/Downloads/ESRD‐QIP‐Summary‐Payment‐Years‐2012‐2016.pdf (accessed 19 May 2019).
Ceretta 2018
- Ceretta ML, Noordzij M, Luxardo R, Meester J, Abad Diez JM, Finne P, et al. Changes in co‐morbidity pattern in patients starting renal replacement therapy in Europe‐data from the ERA‐EDTA Registry. Nephrology Dialysis Transplantation 2018;33(10):1794‐804. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Chesterton 2010
- Chesterton LJ, Selby NM, Burton JO, Fialova J, Chan C, McIntyre CW. Categorization of the hemodynamic response to hemodialysis: the importance of baroreflex sensitivity. Hemodialysis International 2010;14(1):18‐28. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Couser 2011
- Couser WG, Remuzzi G, Mendis S, Tonelli M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney International 2011;80(12):1258‐70. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Csiky 2008
- Csiky B, Sulyok E, Lakatos O, Wittmann I, Martens‐Lobenhoffer J, Bode‐Boger SM. Response of asymmetric dimethylarginine to hemodialysis‐associated hypotension in end‐stage renal disease patients. Nephron 2008;108(2):c127‐34. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Daugirdas 2007
- Daugirdas JT, Blake PG, Ing TS. Handbook of Dialysis. 4th Edition. Philadelphia: Lippincott Williams & Wilkins, 2007. [Google Scholar]
Davenport 2008a
- Davenport A, Cox C, Thuraisingham R. Blood pressure control and symptomatic intradialytic hypotension in diabetic haemodialysis patients: a cross‐sectional survey. Nephron 2008;109(2):c65‐71. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Davenport 2008b
- Davenport A, Cox C, Thuraisingham R. Achieving blood pressure targets during dialysis improves control but increases intradialytic hypotension. Kidney International 2008;73(6):759‐64. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
De Angelis 2004
- Angelis C, Drazen JM, Frizelle FA, Haug C, Hoey J, Horton R, et al. Clinical trial registration: a statement from the International Committee of Medical Journal Editors. Annals of Internal Medicine 2004;141(6):477‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Dubin 2011
- Dubin R, Owens C, Gasper W, Ganz P, Johansen K. Associations of endothelial dysfunction and arterial stiffness with intradialytic hypotension and hypertension. Hemodialysis International 2011;15(3):350‐8. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Eldehni 2015
- Eldehni MT, Odudu A, McIntyre CW. Randomized clinical trial of dialysate cooling and effects on brain white matter. Journal of the American Society of Nephrology 2015;26(4):957‐65. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Fortin 2010
- Fortin PM, Bassett K, Musini VM. Human albumin for intradialytic hypotension in haemodialysis patients. Cochrane Database of Systematic Reviews 2010, Issue 11. [DOI: 10.1002/14651858.CD006758.pub2] [DOI] [PubMed] [Google Scholar]
GRADE 2008
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck‐Ytter Y, Alonso‐Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336(7650):924‐6. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Guyatt 2011
- Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso‐Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidence‐‐imprecision. Journal of Clinical Epidemiology 2011;64(12):1283‐93. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Hays 1994
- Hays RD, Kallich JD, Mapes DL, Coons SJ, Carter WB. Development of the kidney disease quality of life (KDQOL) instrument. Quality of Life Research 1994;3(5):329‐38. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jain 2012
- Jain AK, Blake P, Cordy P, Garg AX. Global trends in rates of peritoneal dialysis. Journal of the American Society of Nephrology 2012;23(3):533‐44. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
K/DOQI 2005
- K/DOQI Workgroup. K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. American Journal of Kidney Diseases 2005;45(4 Suppl 3):S1‐153. [MEDLINE: ] [PubMed] [Google Scholar]
Kooman 2007
- Kooman J, Basci A, Pizzarelli F, Canaud B, Haage P, Fouque D, et al. EBPG guideline on haemodynamic instability. Nephrology Dialysis Transplantation 2007;22 Suppl 2:ii22‐44. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Krupp 1989
- Krupp LB, LaRocca NG, Muir‐Nash J, Steinberg AD. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Archives of Neurology 1989;46(10):1121‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Leypoldt 2002
- Leypoldt JK, Cheung AK, Delmez JA, Gassman JJ, Levin NW, Lewis JA, et al. Relationship between volume status and blood pressure during chronic hemodialysis. Kidney International 2002;61(1):266‐75. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Lozano 2012
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010.[Erratum appears in Lancet. 2013 Feb 23;381(9867):628 Note: AlMazroa, Mohammad A [added]; Memish, Ziad A [added]]. Lancet 2013;380(9859):2095‐128. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mc Causland 2013
- Causland FR, Brunelli SM, Waikar SS. Dialysis dose and intradialytic hypotension: results from the HEMO study. American Journal of Nephrology 2013;38(5):388‐96. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mc Causland 2015
- Causland FR, Waikar SS. Association of predialysis calculated plasma osmolarity with intradialytic blood pressure decline. American Journal of Kidney Diseases 2015;66(3):499‐506. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mustafa 2016
- Mustafa RA, Bdair F, Akl EA, Garg AX, Thiessen‐Philbrook H, Salameh H, et al. Effect of lowering the dialysate temperature in chronic hemodialysis: a systematic review and meta‐analysis. Clinical Journal of The American Society of Nephrology: CJASN 2016;11(3):442‐57. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
National Kidney Foundation 2015
- National Kidney Foundation. KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. American Journal of Kidney Diseases 2015;66(5):884‐930. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Nesrallah 2013
- Nesrallah GE, Suri RS, Guyatt G, Mustafa RA, Walter SD, Lindsay RM, et al. Biofeedback dialysis for hypotension and hypervolemia: a systematic review and meta‐analysis. Nephrology Dialysis Transplantation 2013;28(1):182‐91. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Pippias 2016
- Pippias M, Jager KJ, Kramer A, Leivestad T, Sanchez MB, Caskey FJ, et al. The changing trends and outcomes in renal replacement therapy: data from the ERA‐EDTA Registry. Nephrology Dialysis Transplantation 2016;31(5):831‐41. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Rosales 2000
- Rosales LM, Schneditz D, Morris AT, Rahmati S, Levin NW. Isothermic hemodialysis and ultrafiltration. American Journal of Kidney Diseases 2000;36(2):353‐61. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Sands 2014
- Sands JJ, Usvyat LA, Sullivan T, Segal JH, Zabetakis P, Kotanko P, et al. Intradialytic hypotension: frequency, sources of variation and correlation with clinical outcome. Hemodialysis International 2014;18(2):415‐22. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Santoro 2002
- Santoro A, Mancini E, Basile C, Amoroso L, Giulio S, Usberti M, et al. Blood volume controlled hemodialysis in hypotension‐prone patients: a randomized, multicenter controlled trial. Kidney International 2002;62(3):1034‐45. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Schneditz 2003
- Schneditz D, Ronco C, Levin N. Temperature control by the blood temperature monitor. Seminars in Dialysis 2003;16(6):477‐82. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Schunemann 2011a
- Schünemann HJ, Oxman AD, Higgins JP, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and 'Summary of findings' tables. In: Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Schunemann 2011b
- Schünemann HJ, Oxman AD, Higgins JP, Deeks JJ, Glasziou P, Guyatt GH. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Selby 2006
- Selby NM, McIntyre CW. A systematic review of the clinical effects of reducing dialysate fluid temperature. Nephrology Dialysis Transplantation 2006;21(7):1883‐98. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Shoji 2004
- Shoji T, Tsubakihara Y, Fujii M, Imai E. Hemodialysis‐associated hypotension as an independent risk factor for two‐year mortality in hemodialysis patients. Kidney International 2004;66(3):1212‐20. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Stefansson 2014
- Stefansson BV, Brunelli SM, Cabrera C, Rosenbaum D, Anum E, Ramakrishnan K, et al. Intradialytic hypotension and risk of cardiovascular disease. Clinical Journal of The American Society of Nephrology: CJASN 2014;9(12):2124‐32. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sulowicz 2006
- Sulowicz W, Radziszewski A. Pathogenesis and treatment of dialysis hypotension. Kidney International ‐ Supplement 2006;70(104):S36‐9. [EMBASE: 44764126] [Google Scholar]
Thompson 2009
- Thompson AM, Oliver JA. Endogenous and exogenous vasopressin during hemodialysis. Seminars in Dialysis 2009;22(5):472‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Tisler 2003
- Tisler A, Akocsi K, Borbas B, Fazakas L, Ferenczi S, Gorogh S, et al. The effect of frequent or occasional dialysis‐associated hypotension on survival of patients on maintenance haemodialysis. Nephrology Dialysis Transplantation 2003;18(12):2601‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Toth‐Manikowski 2016
- Toth‐Manikowski SM, Sozio SM. Cooling dialysate during in‐center hemodialysis: Beneficial and deleterious effects. World Journal of Nephrology 2016;5(2):166‐71. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
van der Sande 1999
- Sande FM, Kooman JP, Burema JH, Hameleers P, Kerkhofs AM, Barendregt JM, et al. Effect of dialysate temperature on energy balance during hemodialysis: quantification of extracorporeal energy transfer. American Journal of Kidney Diseases 1999;33(6):1115‐21. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
White 2008
- White S, Chadban SJ, Jan S, Chapman JR, Cass A. How can we achieve global equity in provision of renal replacement therapy?. Bulletin of the World Health Organization 2008;86(3):229‐37. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wu 2001
- Wu A, Fink N, Cagney K, Bass E, Rubin H, Meyer K, et al. Developing a health‐related quality‐of‐life measure for end‐stage renal disease: The CHOICE Health Experience Questionnaire. American Journal of Kidney Diseases 2001;37(1):11‐21. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Tsujimoto 2017
- Tsujimoto Y, Tsujimoto H, Nakata Y, Kataoka Y, Kimachi M, Shimizu S, et al. Dialysate temperature reduction for intradialytic hypotension for people with chronic kidney disease requiring haemodialysis. Cochrane Database of Systematic Reviews 2017, Issue 3. [DOI: 10.1002/14651858.CD012598] [DOI] [PMC free article] [PubMed] [Google Scholar]