

Abstract
Exposure to high levels of post-divorce interparental conflict is a well-documented risk factor for the development of psychopathology and there is strong evidence of a subpopulation of families in which conflict persists for many years after divorce. However, existing studies have not elucidated differential trajectories of conflict within families over time, nor have they assessed the risk posed by conflict trajectories for development of psychopathology or evaluated potential protective effects of children’s coping to mitigate such risk. We used growth mixture modeling to identify longitudinal trajectories of child-reported conflict over a period of six to eight years following divorce in a sample of 240 children. We related the trajectories to children’s mental health problems, substance use, and risky sexual behaviors and assessed how children’s coping prospectively predicted psychopathology in the different conflict trajectories. We identified three distinct trajectories of conflict; youth in two high conflict trajectories showed deleterious effects on measures of psychopathology at baseline and the six-year follow-up. We found both main effects of coping and coping by conflict trajectory interaction effects in predicting problem outcomes at the six-year follow-up. The study supports the notion that improving youth’s general capacity to cope adaptively is a potentially modifiable protective factor for all children facing parental divorce and that children in families with high levels of post-divorce conflict are a particularly appropriate group to target for coping-focused preventive interventions.
Keywords: child psychopathology, divorce, interparental conflict, prevention, coping
Parental divorce or separation is the second most prevalent adverse childhood event (Sacks, Murphy, & Moore, 2014), and it affects 30–40% of children prior to the time they reach the age of 15 (Andersson, 2002; Kennedy & Bumpass, 2008). A recent population-based report estimates that more than eight million children in the United States live with a divorced parent (US Census Bureau, 2018). Despite being a highly prevalent stressful life event, the vast majority of children who experience parental divorce do not develop long-lasting problems (Amato, 1993, 2001; Amato & Sobolewski, 2001; Hetherington, Cox, & Cox, 1982). Nevertheless, youth who experience parental divorce, relative to their peers who remain in two-parent households, are at increased risk for a host of difficulties, including higher rates of psychopathology, substance use disorders, and academic underachievement (e.g., Amato, 2000).
Exposure to high levels of interparental conflict is one of the most well-documented factors accounting for the increased risk for problem outcomes of children who experience parental divorce (Amato, 1993, 2001; Amato & Sobolewski, 2001; Johnston, 1994; Kelly, 2012). This is not surprising considering that conflict between parents is a significant risk factor for the development of psychopathology in children, regardless of family structure (Cummings & Davies, 2010). There is a great deal of evidence that interparental conflict is related to internalizing and externalizing problems, as well as academic problems, in children in divorced families (Amato, 1993; Buchanan, Maccoby, & Dornbusch, 1991; Buehler et al., 1997; E. Hetherington & Kelly, 2002; J. R. Johnston, 1994; Kelly & Emery, 2003; Kline, Johnston, & Tschann, 1991; Long, Slater, Forehand, & Fauber, 1988; Shaw & Emery, 1987; Vandewater & Lansford, 1998). Some evidence suggests that interparental conflict may become even more salient for youth after divorce compared to those in married families, due to increases in the intensity of interparental conflict, conflicts over loyalty to the divorced parents (i.e., denigration or badmouthing of the other parent), and an increased focus on child-related issues (Grych, 2005).
Prevalence and Profiles of Post-divorce Interparental Conflict
Some degree of conflict around the time of separation and divorce is typical among divorcing parents (Hetherington et al., 1982) and can be seen as a marker of the stressful, but normal, process that parents experience as they reorganize their family life. Interparental conflict typically diminishes within the first few years of separation, but some parents remain embroiled in conflict for many years following divorce (Hetherington & Kelly, 2002; Hetherington et al., 1982; King & Heard, 1999). For example, the landmark longitudinal study by Hetherington and colleagues documented that 20–25% of parents reported engaging in conflictual behavior six years post-divorce (Hetherington & Kelly, 2002). Another study of families mired in custody disputes found that 15–20% of mothers and fathers reported ongoing conflict at the 12-year follow-up (Sbarra & Emery, 2005). Other researchers have used cross-sectional designs to describe how the level of interparental conflict differs over time following divorce. A large, nationally representative study of divorced adults in the Netherlands showed that among those with children, 56–67% reported antagonistic contact one year after divorce (Fischer, de Graaf, & Kalmijn, 2005). In the group that were 3–10 years post-divorce, 26–29% reported antagonistic contact and among those who had been divorced for more than 10 years, 10% reported antagonistic contact.
These data provide important snapshots of the prevalence of interparental conflict following divorce and establish firm evidence of persistent high levels of conflict in a subpopulation of divorcing families (Fischer et al., 2005; Hetherington & Kelly, 2002). However, the current data are limited in that they only provide percentages of divorced families with high levels of conflict at different points in time, but do not describe differential patterns or trajectories of conflict within families over time. We are not aware of any published peer-reviewed study that has examined profiles of within-family change in interparental conflict over time.1 This is a critical gap in the literature because different trajectories of conflict over time may have different implications for children’s psychopathology and well-being. For example, in some families, interparental conflict may always be relatively low, whereas in others, it may be high at the time of separation but decrease over time, or the level of conflict may start high and remain high for several years following the divorce. Despite many scholars surmising that chronic conflict is likely to be the most damaging for children (e.g., Grych, 2005; Smyth & Moloney, 2017), researchers have not assessed the effects that differential trajectories of exposure to interparental conflict may have on children’s psychopathology. Elucidating distinct longitudinal trajectories and their prospective associations with children’s psychopathology, as well as factors that may predict which trajectory a family is likely to follow (e.g., parental hatred [Smyth & Moloney, 2019], child age, concerns about the other parent’s parenting behavior, legal conflict, parental psychopathology [Johnston, 1994], co-parenting arrangements [Bauserman, 2012; Nielsen, 2017]), is key to identifying high-risk families who may benefit from preventive interventions.
Another limitation of the literature on levels of exposure to conflict over time is that all studies use parent rather than child reports of conflict. The relation between parent and child report of interparental conflict in divorced families is relatively modest and variable, ranging from r = .21 - .61 across studies (Camisasca, Miragoli, Di Blasio, & Grych, 2017; Fear et al., 2009). Research indicates that children’s perception of the conflict is key to the processes that link exposure to mental health problems (Grych & Fincham, 1993; Grych, Harold, & Miles, 2003), and that children’s reports of conflict are more strongly related to measures of their adjustment problems than are parent reports of conflict (Cummings, Davies, & Simpson, 1994; Grych, Seid, & Fincham, 1992).
Theoretical Frameworks for Understanding the Relations between Interparental Conflict and Child Psychopathology
Two major theoretical frameworks have been proposed to describe the processes by which exposure to interparental conflict influences children’s psychopathology and well-being. The Emotional Security Theory (EST) posits that exposure to interparental conflict threatens a child’s sense of emotional security within the family system and specifically within the parental subsystem (Davies & Cummings, 1994). An impaired sense of safety and security in the family system interferes with the child’s capacity to regulate emotions and behaviors in the face of stress, which confers risk of psychopathology and other forms of maladjustment (Cummings & Davies, 2010; Cummings, George, McCoy, & Davies, 2012). Another prominent theory, the Cognitive-Contextual Framework (CCF), focuses on children’s cognitive reactions to the conflict as the key mediators linking exposure and development of psychopathology (Grych & Fincham, 1990). CCF posits that the child’s cognitive appraisal of the conflict event is influenced by the context in which the conflict occurs, which in turn, determines their emotional and behavioral responses, such as reactivity and coping efforts. Research based on this framework found that children’s negative cognitive appraisals of the conflict are critical determinants of their subjective distress and the negative impact of the conflict on their well-being (Grych & Fincham, 1993). For example, studies showed that the extent to which children felt threatened and blamed themselves in response to interparental conflict mediated the association between interparental conflict and the development of internalizing and externalizing problems (Grych, Fincham, Jouriles, & McDonald, 2000; Grych et al., 2003).
Effective Coping as a Protective Factor against the Effects of Interparental Conflict
There is considerable evidence that children’s coping behaviors can be protective, leading to better adjustment for children who experience a wide range of stressors (Compas et al., 2017). For children from divorced families, active coping strategies, such as problem solving and cognitive reframing, have been found to be associated with lower child mental health problems cross-sectionally and five months later (Sandler, Tein, & West, 1994). Similarly, higher use of secondary control coping strategies, such as distraction and acceptance, in response to interpersonal stressors is associated with fewer mental health problems in youth with depressed parents (Jaser et al., 2007). The overarching goal of effective coping is to regulate emotional responding and reduce risk of becoming overwhelmed during stressful moments and to solve problems and marshal resources to enable children to successfully meet the challenges posed by stressful events. In this way, effective coping may mitigate the pathways in the EST and CCF theoretical models that link exposure to interparental conflict and development of psychopathology. For example, from the perspective of EST, coping strategies might counteract the extent to which children’s emotional safety and security is undermined (Cummings & Davies, 2010), thereby decreasing negative appraisals, such as self-blame or threat, (Grych & Fincham, 1990) and reducing emotional reactivity (Cummings, Schermerhorn, Davies, Goeke-Morey, & Cummings, 2006). From the perspective of the CCF, coping strategies may enable children to appraise conflict in ways that involve less blame of themselves or others. Before discussing the ways in which coping may counteract the theoretical pathways through which conflict may affect the development of child psychopathology, it is first necessary to discuss research on the assessment of the dimensions of children’s coping strategies.
There is consensus in the literature that at the broadest level, a useful distinction is made between coping efforts that are active or approach-oriented versus avoidant or disengagement-oriented (Ayers, Sandler, & Twohey, 1998; Billings & Moos, 1981; Compas, Connor-Smith, Saltzman, Thomsen, & Wadsworth, 2001). Within the domain of active coping, however, scholars and researchers have demarcated subtypes that comprise different strategies (i.e., cognitive or behavioral efforts to modify one’s experience of a stressor) in a variety of ways. The most widely recognized model by Lazarus and Folkman (1987) distinguishes subtypes of coping based on whether one’s efforts are focused on regulating emotions that arise in reaction to the stressor (i.e., emotion-focused) or making a direct impact on the stressors itself (i.e., problem-focused). This typology has frequently been applied to the search for matching coping strategies to context, as emotion-focused strategies are often presumed to be adaptive in the face of uncontrollable stressors, whereas problem-focused strategies are seen as adaptive in situations in which the individual has the ability to exert control and modify the stressor itself (Compas, Banez, Malcarne, & Worsham, 1991; Compas et al., 2017; Kerig, 2001). More recently, Compas and colleagues advocated for distinguishing active (i.e., engagement) strategies according to the motivational goals underlying one’s coping efforts, namely primary control (those focused on changing the situation or the consequences of one’s reaction to the situation; e.g., problem solving, emotion regulation, hiding emotional expression) and secondary control (those focused on adapting to the situation; e.g., cognitive reappraisal, distraction, acceptance, positive thinking) (Compas et al., 2001; Connor-Smith, Compas, Wadsworth, Thomsen, & Saltzman, 2000).
A growing area of research has investigated the effects of different coping strategies as vulnerability or protective factors for children exposed to interparental conflict and parental divorce. Several studies with children from married families have investigated whether children’s coping with interparental conflict moderates the relations between exposure to conflict and children’s psychopathology (e.g., Nicolotti, El-Sheikh, & Whitson, 2003; Shelton & Harold, 2008; Tu, Erath, & El-Sheikh, 2016). Illustratively, Tu et al. (2016) found that higher levels of engaged secondary control strategies (e.g., positive thinking) protected against the effects of conflict on externalizing problems, whereas higher levels of both engaged primary (e.g., problem solving) and secondary control coping (e.g., cognitive restructuring) with conflict increased risk from exposure to conflict on internalizing problems. To our knowledge, only one study has investigated whether children’s general style of coping with stressors moderates the effect of conflict on mental health problems (Shelton & Harold, 2007). This study, which was conducted with children in married families, found that higher levels of coping by venting negative emotion exacerbated the prospective relations between conflict and higher levels of anxiety-depression. We know of no study that has studied children’s coping with interparental conflict following divorce and only one has studied children’s coping as a moderator of the effects of post-divorce stressors on children’s psychopathology in divorced families. Although this study did not specifically study coping as a moderator of post-divorce interparental conflict, it did find that an active coping style, comprised of positive cognitive restructuring and problem-focused coping, was a significant moderator of the negative effects of multiple divorce-related stressors (including interparental conflict) on children’s mental health problems (Sandler et al., 1994).
An alternative perspective for understanding the effects of coping on children’s adjustment to interparental conflict is to focus on efficacy of coping rather than specific strategies that are used to cope with stress. Coping efficacy refers to people’s subjective appraisals as to how effective their coping efforts were in dealing with the demands of the stressful situation. Theoretically, an appraisal of coping efficacy can impact the level of emotional arousal in a stressful situation and can influence the likelihood of using effective coping strategies to deal with future stressors (Bandura, 1997; Lazarus & Folkman, 1984; Skinner & Wellborn, 1994). Appraisals of coping efficacy may be made for specific situations, and with repeated success may lead to a general belief that one can successfully deal with the stressors in one’s life. It may be that the feelings of efficacy, rather than the specific coping strategy, most strongly predicts children’s ability to adapt to the stressor. Theoretical models posit that coping efficacy can increase the likelihood that one will use a strategy they expect to work and diminish negative emotional reactivity in response to a stressor (Lazarus, 1991; Lazarus & Folkman, 1984), as well as facilitate effective regulation of thoughts and feelings during stressful situations (Bandura, 1997). Previous evidence indicates that coping efficacy mediates exposure to interparental conflict and children’s distress reactions (Camisasca et al., 2017) and mental health outcomes (Cummings et al., 1994) in married families. In divorced families, general coping efficacy has been shown to mediate the association between active and avoidant coping strategies and children’s psychopathology, with active coping strategies being associated with higher levels of coping efficacy and lower mental health problems and avoidant strategies being associated with lower levels of coping efficacy and higher mental health problems (Sandler, Tein, Mehta, Wolchik, & Ayers, 2000). Based on these findings, in addition to studying which coping strategies are protective or detrimental for children in high conflict situations, it is also crucial to understand the role of general coping efficacy for children who are exposed to different trajectories of interparental conflict over time.
Coping in Context
Understanding effective coping requires that we consider the context of the stressor (Aldao, 2013; Forsythe & Compas, 1987; Greenaway, Kalokerinos, & Williams, 2018). For example, one contextual factor is whether the conflict occurs between parents who are married or parents who are separated or divorced. In married families, interparental conflict may lead children to experience a lack of security of the continuation of the family unit (Cummings and Davies). In divorced families, the threat from conflict may involve issues such as concern about the well-being of the parents or of the children’s continued relationship with one of the parents (e.g., Sheets, Sandler, & West, 1996). Little research has focused on youth coping processes in the context of post-divorce interparental conflict (for an exception focused on litigating families, see Radovanovic, 1993). More broadly, the vast majority of studies examining the links between interparental conflict and psychopathology has been conducted with youth from married families (Cummings & Davies, 2010; Fosco & Grych, 2008).
Sandler (2001) proposed that the ecology of adversities themselves (i.e., setting, temporal and cumulative nature) as key contextual factors to understanding the associated risks and likely outcomes of experiencing adversity during childhood. Several aspects of the ecology of interparental conflict have been studied in depth and researchers have found that such conflict has a more negative effect on children when it crosses domains (e.g., financial, parenting practices), has a high level of intensity (i.e., anger, hostility, physical aggression), and when it goes unexplained or unresolved (Goeke-Morey, Cummings, & Papp, 2007; Ha, Bergman, Davies, & Cummings, 2018). However, the temporal and cumulative nature of interparental conflict, and how these characteristics are related to the development of children’s psychopathology, have rarely been studied. Although prior research has shown that the mean level of post-divorce conflict decreases over time following divorce, the mean level of change likely masks different trajectories of change in conflict across families. Differential trajectories of exposure to interparental conflict over time is a potentially critical aspect of the ecology of conflict, as the temporal quality of adverse conditions is a well-documented predictor of negative outcomes related to stressful events in general (Danese & McEwen, 2012; Wadsworth, 2015). It may be that different trajectories of conflict over time have differential effects on children. For example, does the effect of post-divorce conflict on children differ if it occurs for a relatively short period following separation and then dissipates over time as compared with divorces in which the level of conflict is never very high and remains low over time, or with divorce in which the children are exposed to chronic high levels of conflict for many years? Furthermore, how do different coping strategies or perceptions of coping efficacy predict child psychopathology outcomes over time in the context of exposure to different trajectories of conflict? We argue that elucidating how different trajectories of exposure to conflict over time are associated with children’s mental health and further, how coping is related to child outcomes in the context of those different trajectories, will provide information that will help identify high-risk families and better understand children’s risk for psychopathology after divorce.
Current Study
The present study addresses critical gaps in the literature on the relations between interparental conflict and the development of psychopathology for children from divorced families by: (1) identifying trajectories of post-divorce interparental conflict over time and factors that predict differential trajectories of conflict, 2) assessing the relations between trajectories of conflict over time and psychopathology of children, and 3) assessing how children’s coping prospectively predicts the development of psychopathology for children exposed to different trajectories of interparental conflict following divorce.
First, we employed growth mixture modeling to identify subgroups of children exposed to different trajectories of interparental conflict over a 6–8-year period following parental divorce. We hypothesized that there would be distinct trajectories of IPC over time, including a group characterized by stable, low levels of conflict; a group characterized by stable, high levels of conflict; and a group demonstrating declines in conflict over time (i.e., high-to-low). Given previous evidence that the majority of families report conflict in the first year following divorce, and a subgroup of approximately 20–30% report some degree of conflict several years after separation (Hetherington & Kelly, 2002; Hetherington et al., 1982; King & Heard, 1999), we expected the smallest group to be represented by a trajectory of chronically high interparental conflict over time. We speculate that there might be groups that have different trajectories than those described above. For example, a fourth group might be characterized by levels of conflict that fluctuate over time based on the presence or absence of other stressors, such as the remarriage of one parent, which we know from previous research is very common by six years post-divorce (i.e., 70–80%; Hetherington & Kelly, 2002). However, given the spacing of our measurement occasions, we were not sure that this group could be identified in the current study.
After identifying subgroups based on longitudinal trajectories of conflict, we then explored the relations between theoretically-derived predictors (e.g., the residential parent’s feelings about the other parent’s relationship with the child, allocation of parenting time, child gender and age, and absence of the non-residential parent) and interparental conflict trajectories. We then examined the relations between interparental conflict trajectories and children’s mental health at the first time point of the trajectories and mental health and substance use problems and risky sexual behavior at the last time point. We expected that the group characterized by chronically high levels of interparental conflict over time would demonstrate the highest levels of problematic outcomes. Finally, we tested main and interactive effects of children’s coping styles (i.e., problem-focused, cognitive restructuring, avoidant) and coping efficacy with trajectories of conflict to prospectively predict mental health problems, substance use, and risky sexual behavior six years later.
Method
Participants
Participants were 240 youth ages 9–12 whose mothers participated in a clinical trial of a preventive intervention, the New Beginnings Program (NBP), within two years of filing a divorce decree (see Wolchik et al., 2002 for full details about the eligibility criteria and intervention). Families were primarily identified through random selection of decrees in a computerized court record system and invited to participate via letters and telephone calls. Eligibility criteria included: (1) fluency in English, (2) no current mental health treatment for mother or child, (3) primary maternal residential custody, (4) no remarriage, cohabitation, or plans to remarry for the mother, and (4) no planned changes to custody arrangements during the study period. Families were referred out for treatment when deemed necessary based on predetermined criteria (i.e., score of higher than 17 on the Children’s Depression Inventory [Kovacs, 1985], endorsement of suicidal ideation, or score higher than the 97th percentile on the Externalizing subscale of the Child Behavior Checklist [Achenbach & Rescorla, 2001]). The average time since the date of parental separation was 26.88 (SD = 17.23) months and the average time since the legal divorce was 12.23 (SD = 6.41) months. Participants were randomly assigned to one of two intervention conditions, mother program (MP) or mother program plus child program (MPCP), or an active literature control condition (LC).
Procedure
The current study used data from the first five waves of the NBP study, which includes baseline (T1), posttest (T2), three-month follow-up (T3), six-month follow-up (T4), and six-year follow-up (T5). The posttest occurred approximately three months after pretest. Of those 240 families who completed the pre-test, 98% (234–236 families) completed assessments at T2-T4 and 91% (218 families) of the sample was retained at the six-year follow-up (T5). Youth and mothers were interviewed in their homes by trained research staff and informed consent/assent was obtained from all participants. Families were compensated $45 at T1-T4 and both mothers and children were compensated $100 at T5.
Measures
Interparental conflict.
Youth’s perception of frequency and intensity of interparental conflict was assessed at each measurement occasion (T1-T5) using the 6-item frequency and 7-item intensity subscales of the Children’s Perception of Interparental Conflict scale (CPIC; (Grych et al., 1992). “Your parents got really mad when they argued” and “You never saw your parents arguing or disagreeing” are examples of intensity and frequency items, respectively. The CPIC was rated on a 3-point scale (1 = true, 3 = false) and scored as an average rating, with higher scores indicating higher levels of perceived interparental conflict. The CPIC has well-established psychometric properties in samples of children and adolescents (Bickham & Fiese, 1997; Grych et al., 1992). Internal consistency for this sample ranged from α = .74 - .88 across T1-T5. At six-year follow-up, items assessing child-report of interparental conflict were skipped for youth who reported no contact with their fathers or no contact between their parents, as it was assumed that under these conditions there was no opportunity for exposure to interparental conflict, making the items irrelevant. Thus, for these participants, the interparental conflict variable was coded as zero, the lowest possible score, to represent no exposure to conflict.
Youth coping efforts and coping efficacy.
Youth dispositional coping was assessed using the 36-item Child Coping Strategies Checklist - Revised (CCSC-R; Ayers, Sandler, West, & Roosa, 1996) at each measurement occasion (T1-T5). Assessments of coping and coping efficacy (see below) at the first four waves (T1-T4) were used in the current study. The 12-item Avoidant Coping (e.g., “You tried to stay away from things that upset you”), 12-item Positive Cognitive Restructuring Coping (e.g., “You told yourself that it would be okay”), and 12-item Problem-focused Coping (e.g., “You tried to make things better by changing what you did”) subscales were treated as separate constructs for the purposes of the current study. CCSC-R items were rated on a 4-point scale (1 = never, 4 = most of the time) and scored as an average, with higher scores indicating more use of coping strategies within the respective category. Ranges of internal consistency for this sample were α = .68 - .81 across T1-T4 for Avoidant Coping, α = .82 - .90 across T1-T4 for Positive Cognitive Restructuring Coping, and α = .79 - .90 across T1-T4 for Problem-focused Coping. Previous research has linked these aspects of children’s coping with mental health problems in children who have experienced divorce (Sandler et al., 2000).
Youth also completed the 7-item Coping Efficacy Scale (CES; (Sandler et al., 2000), a measure of their satisfaction with the way they have handled problems in the past and the way they anticipate handling problems in the future, at each measurement occasion. This scale has been shown to be negatively related to children’s internalizing and externalizing problems in previous studies (Sandler et al., 2000). An illustrative item is “Overall, how well do you think that the things you did during the last month worked to make the situation better?” The CES was rated on a 4-point scale (1 = did not work at all, 4 = worked very well) and scored as an average rating, with higher scores representing higher levels of coping efficacy. Internal consistency for this sample ranged from α = .71 - .83 across T1-T4.
For the purposes of this study, we created longitudinal composite measures of each coping construct by averaging ratings across the first four measurement occasions (T1-T4) to gain a better global assessment of the child’s coping across the first year of the study (which was within approximately 2–3 years of the divorce). To assess longitudinal stability in the measurement of coping, we first examined intercorrelations across the four waves. The correlation coefficients ranged from r = .33 to .61, with adjacent scores being more strongly correlated (e.g., T3 and T4 correlations ranged from r = .56-.61). We further assessed longitudinal stability of our coping measures using the trait-state measurement model (STARTS; Kenny & Zautra, 2001) to increase our confidence in creating a composite of coping assessments across study waves. Results indicated that the stable components (i.e., trait and autoregressive latent factors) accounted for the majority of variance in the repeated assessments of coping at T1-T4, ranging from 62% for problem-focused coping to 91% for avoidant coping. The random component (i.e., state or occasion-specific factor) accounted for 9–38% of the variance. Because the proportion of the total variance explained by the stable components exceeded the variance explained by the random component, which supported the assumption of longitudinal stability of coping style over this period, we created a composite of coping scores across this 1-year period.
Youth mental health problems.
Internalizing and externalizing problems were assessed at each measurement occasion (T1-T5), and data for the current study include baseline (T1) and six-year follow-up (T5) assessments. Youth completed the 27-item Child Depression Inventory (CDI; Kovacs, 1985) and the 28-item revised Children’s Manifest Anxiety Scale (RCMAS; Reynolds & Richmond, 1978). These inventories have well-established reliability and validity data (Lee, Piersel, Friedlander, & Collamer, 1988; Reynolds, 1981; Reynolds & Paget, 1981; Saylor, Finch, Spirito, & Bennett, 1984; Timbremont, Braet, & Dreessen, 2004). For the current sample, internal consistency estimates for the CDI were α = .76 (T1) and .85 (T5) and for the RCMAS were α = .88 (T1) and .89 (T5). Scores from these two measures were standardized and average to form a composite representing internalizing problems. As a measure of externalizing problems, youth completed the 25-item Divorce Adjustment Project Externalizing Scale, based on the Youth Self-report Hostility Scale (Cook, 1986) at T1, and a 27-item questionnaire comprised of the original 25 items and 2 additional items from the Youth Self-Report (Achenbach & Rescorla, 2001) to assess delinquent behavior at T5. In the current study, internal consistency was α = .83 at T1 and α = .84 at T5. We used standardized scores from this sample for youth self-report of internalizing and externalizing problems in all analyses.
Mothers completed the 31-item internalizing subscale and the 33-item externalizing subscale of the Child Behavior Checklist (Achenbach & Rescorla, 2001). This inventory has demonstrated good psychometric properties, including test-retest and internal consistency reliability as well as construct and predictive validity. Internal consistency estimates in this sample were α = .88 at T1 and α = .86 at T5 for the internalizing subscale and α = .87 at T1 and α = .89 at T5 for the externalizing subscale. In the current study, mother reports of internalizing and externalizing problems are represented by norm-referenced T scores.
At T5, mental health and substance use disorders were assessed using youth and parent versions of the Diagnostic Interview Schedule for Children (DISC; Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000). Diagnoses were made based on two criteria: (1) youth met diagnostic criteria for at least one mental health or substance use disorder based on either self or parent report, and (2) if diagnostic criteria were met, impairment was rated as intermediate or severe by endorsement of at least two items. For these analyses, we used a dichotomous outcome variable representing presence or absence of any mental health or substance use disorder diagnosis. Mental health disorders and substance use disorders were used as separate outcomes.
Youth substance use.
At T5, youth completed a self-administered questionnaire with selected items from the Monitoring the Future Scale (Johnston et al., 2018), which has established reliability and validity psychometric qualities. Alcohol and marijuana use were measured on a 7-point scale representing the number of times youth had used the substance during the past year (1 = 0 to 7 = >40). We analyzed past year alcohol and marijuana use separately.
Youth risky sexual behavior.
At T5, youth reported on the number of different sexual partners they had since their mothers and/or they had completed the intervention via a self-administrated questionnaire.
Family variables.
Family variables collected at T1 that were used in the current analyses included the number of overnights per month that the child spent with their non-residential parent (ranging from 0–30), time elapsed since the separation, whether or not the child’s father moved out of the geographic area or remarried (dichotomous yes/no), and the extent to which the mother held a positive view of the child’s relationship with their father (assessed by an average rating on 6 items developed in-house; illustrative item is “How do you feel about your ex-spouse having a relationship with your child?” rated on a 7-point scale where 1 = strongly discourage it, 7 = strongly encourage it; α = .85).
Covariates.
For the current study, we used demographic variables of child age and gender, and one study design variable, intervention condition (because the current study did not focus on intervention effects), as covariates in statistical analyses to account for variance explained by these factors extraneous to our primary research questions. Autoregressive controls of baseline mental health problems were included for analyses on youth- and parent-reported internalizing and externalizing problems, but because substance use and risky sexual behaviors were only assessed at T5, no autoregressive controls were included for these outcomes.
Data Analysis Approach
For preliminary analyses, we performed regression diagnostics by examining global influence statistics to identify potentially influential cases and then inspecting the observed change in the coefficients of theoretical predictors when the potentially influential case was included (using cutoffs proposed by Cohen, Cohen, West, & Aiken, 2003). We also identified cases with a Cook’s distance exceeding .20 (Bollen & Jackman, 1985). The results of these procedures identified two potentially influential cases across all analyses. Analyses were run with and without these data; for analyses in which the results changed when the influential case was excluded, we report the discrepancy.
All of the analyses were conducted with Mplus (Version 8; Muthén & Muthén, 1998–2017). We used full information maximum likelihood to handle missing data due to attrition in longitudinal analyses. To characterize longitudinal trajectories of change in interparental conflict, we conducted growth mixture modeling (GMM) analyses to identify the number of unobserved subgroups based on patterns of change in children’s reports of interparental conflict across five waves (T1-T5). Prior to modeling, we assessed longitudinal measurement invariance of our measure of interparental conflict (see Preliminary Analyses section). Specifically, we tested longitudinal measurement invariance using a categorical factor model approach with weighted least squares mean and variance (WLSMV) estimation and the probit link to define observed variable thresholds due to the ordinal nature of the item response options (see Grimm, Ram, & Estabrook, 2016; Millsap & Yun-Tein, 2004).
We evaluated a 2, 3, and 4-class growth mixture models. We repeated models with multiple sets of start values to avoid getting local maximum solutions and ensure the best log-likelihood value was replicated (Muthén & Muthén, 1998–2017). We determined the optimal number of classes based on Bayesian information criterion (BIC; Schwarz, 1978), sample-size adjusted Bayesian information criterion (SABIC; Sclove, 1987), Vuong-Lo-Mendell-Rubin likelihood ratio test (VLMR; Lo, Mendell, & Rubin, 2001), and parameter bootstrapped likelihood ratio test (BLRT; McLachlan & Peel, 2000) and substantive interpretations (see Tein, Coxe, & Cham, 2013). In addition, we relied on entropy to gauge whether the latent classes were highly discriminating (Muthén & Muthén, 1998–2017). We fixed the covariance between intercept and slopes within class to zero to aid model convergence and avoid Heywood cases (i.e., negative variances). Assuming high entropy (> .80) and using the optimal class solution, each child was assigned to the most likely class based on the estimated posterior probabilities for each class. We then used the classification variables to examine the remaining hypotheses: 1) examining trajectory (entered as dummy variables) mean differences in child mental health at baseline (T1) as well as child mental health and risky sexual behavior outcomes at six-year follow-up (T5) and 2) examining the moderation effects of coping styles and global coping efficacy on the relations between conflict trajectories and children’s mental health and substance use problems and risky sexual behavior.
Applying dummy coding for the classification variable of the trajectory, we used multiple regression analyses to examine differences of child mental health and substance use outcomes at baseline and six-year follow-up among the latent classes. We used negative binomial regression for the risky sexual behavior outcome because it was a count variable (i.e., number of sexual partners) with the majority of the sample (57.9%) reporting a value of zero.
Finally, we conducted moderation analyses to test interaction effects between trajectories and the coping subscales on T5 prospective mental health (child-reported internalizing and externalizing problems, mother-reported internalizing and externalizing problems, and mental health diagnoses), substance use (past year alcohol and marijuana use), and risky sexual behavior (number of sexual partners). Following moderation analyses, we conducted post-hoc comparisons for significant interactions to determine which trajectories differed significantly. We plotted the slopes within each trajectory and assessed significance of the within-group simple slope relating the coping measure to the outcome. For analyses in which the interaction effect was non-significant, we removed the interaction term and tested the additive effect of the coping subscales. We report only significant effects from moderation analyses in the results section.
Results
Preliminary Analyses
Table 1 displays descriptive statistics and zero-order Pearson product moment correlations for all study variables and covariates. Children’s reports of interparental conflict were significantly and positively correlated across all time points, with the exception of T2 and T5; in general, T5 had the lowest intercorrelations with other time points. The subscales of coping were positively and significantly correlated, with the exception of avoidant coping and coping efficacy. Mother and youth reports of internalizing and externalizing problems were significantly correlated. There was a strong correlation between past year alcohol and marijuana use and both types of substance use were moderately correlated with risky sexual behavior.
Table 1.
Intercorrelations and Descriptive Statistics for Study Variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. T1 CPIC | 1 | ||||||||||||||||||
| 2. T2 CPIC | .52 | 1 | |||||||||||||||||
| 3. T3 CPIC | .50 | .45 | 1 | ||||||||||||||||
| 4. T4 CPIC | .39 | .47 | .47 | 1 | |||||||||||||||
| 5. T5 CPIC | .16 | .11 | .24 | .24 | 1 | ||||||||||||||
| 6. Coping Efficacy (T1-T4) | −.07 | −.15 | −.17 | −.16 | .00 | 1 | |||||||||||||
| 7. Cognitive Coping (T1-T4) | −.01 | −.07 | .05 | −.12 | .07 | .61 | 1 | ||||||||||||
| 8. Problem-focused Coping (T1-T4) | .04 | −.02 | .08 | −.06 | .12 | .56 | .81 | 1 | |||||||||||
| 9. Avoidant Coping (T1-T4) | .26 | .19 | .21 | .07 | .04 | .15 | .50 | .44 | 1 | ||||||||||
| 10. Youth-reported Externalizing T1 | .28 | .29 | .24 | .23 | −.05 | −.21 | −.13 | −.08 | .08 | 1 | |||||||||
| 11. Youth-reported Internalizing T1 | .29 | .29 | .20 | .19 | .02 | −.33 | −.15 | −.04 | .18 | .52 | 1 | ||||||||
| 12. Youth-reported Externalizing T5 | .06 | .19 | .12 | .10 | .19 | −.23 | −.21 | −.12 | −.02 | .33 | .29 | 1 | |||||||
| 13. Youth-reported Internalizing T5 | .04 | .11 | .05 | .11 | .13 | −.27 | −.19 | −.09 | .00 | .18 | .36 | .61 | 1 | ||||||
| 14. Mother-reported Internalizing T1 | .16 | .18 | .02 | .19 | .03 | −.17 | −.15 | −.09 | .02 | .19 | .30 | .18 | .22 | 1 | |||||
| 15. Mother-reported Externalizing T1 | .14 | .10 | .04 | .14 | .11 | −.11 | −.09 | −.03 | .01 | .26 | .24 | .24 | .18 | .52 | 1 | ||||
| 16. Mother-reported Internalizing T5 | .10 | .10 | .11 | .03 | .11 | −.19 | −.16 | −.14 | .02 | .01 | .11 | .29 | .43 | .50 | .34 | 1 | |||
| 17. Mother-reported Externalizing T5 | .05 | .03 | .08 | .06 | .15 | −.09 | −.04 | −.08 | .04 | .01 | .03 | .34 | .20 | .23 | .58 | .55 | 1 | ||
| 18. Alcohol Use T5 | .05 | .07 | .12 | .11 | .10 | −.13 | −.13 | −.10 | −.05 | .14 | .12 | .33 | .21 | .14 | .15 | .13 | .23 | 1 | |
| 19. Marijuana Use T5 | .10 | .19 | .09 | .13 | .09 | −.12 | −.12 | −.08 | −.01 | .18 | .12 | .32 | .36 | .14 | .19 | .27 | .24 | .61 | 1 |
| 20. Sexual Partners T5 | .07 | .11 | .10 | .10 | .03 | −.18 | −.12 | −.11 | −.01 | .00 | .04 | .22 | .18 | .05 | .05 | .18 | .16 | .34 | .36 |
| Mean | 1.61 | 1.49 | 1.38 | 1.32 | 1.18 | 3.05 | 10.55 | 10.44 | 9.73 | 0.00 | 0.00 | 0.00 | 0.00 | 57.36 | 55.03 | 52.25 | 50.38 | 3.03 | 2.01 |
| SD | 0.45 | 0.44 | 0.38 | 0.34 | 0.37 | 0.34 | 1.76 | 1.74 | 1.58 | 1.00 | 0.89 | 1.00 | 0.92 | 9.59 | 8.48 | 9.34 | 9.82 | 1.99 | 1.75 |
Note. CPIC = Children’s Perception of Interparental Conflict scale (Grych et al., 1992). T1 = baseline, T5 = six-year follow-up.
Given our primary focus on longitudinal change in interparental conflict, we first tested the assumption that the measurement of these items was invariant across time to establish that we were measuring the same construct at different measurement occasions (Grimm et al., 2016; Pitts, West, & Tein, 1996). We first conduct a confirmatory analysis with the 13 items from the CPIC frequency and intensity subscales at T1. The model fit was adequate, χ2 (65) = 221.98, p < .01, RMSEA = .0101 [0.086 – 0.115], CFI = .905, TLI = .886). We dropped 3 items due to low contribution (i.e., low factor loading [β ≤ .30]; e.g., “parents discuss disagreement quietly”) and 1 item (“parents pushed/shoved during argument”) due to lack of variance at T5 (i.e., 99% of the sample gave one response); the final model included 9 items. Good model fit was confirmed at each subsequent time point and the poorest model fit statistics were across all five waves were χ2 (27) = 50.512, p < .01, RMSEA = .062 [0.035 – 0.089], CFI = .972, TLI = .963). We then fitted and evaluated evidence for configural, weak, and strong invariance models through a stepwise process of relaxing model constraints. There was no evidence of significant decreases in model fit according to global (i.e., no significant change in χ2) and absolute (i.e., CFI/TLI change of less than .01, RMSEA remained within confidence interval of less restrictive model) fit statistics. The strong factorial invariance fit the data well, χ2 (1035) = 1209.73, p < .001, RMSEA = .027 [0.019 – 0.003], CFI = .957, TLI = .959), and standardized factor loadings were positive and ranged from 0.56 – 0.98.
Aim 1: Characterize Longitudinal Trajectories of Child-Reported Interparental Conflict
Growth mixture model selection.
As our base model, we fitted a single-group piecewise growth model, with the first piece modeling change from T1-T4 and the second piece modeling change from T4-T5, based on previous research and initial visual inspection of the raw data. First, because previous research suggests that the first few years after parental divorce represents a period of acute change and adjustment (Hetherington & Kelly, 2002), we were interested in differentiating between short-term and long-term trajectories of conflict. Second, plotting the raw data revealed apparent linear change over the initial four waves of data collection (baseline, posttest, 3-month follow-up, 6-month follow-up) and a distinct pattern of linear change between the 6-month and six-year follow-up assessment periods.
Three-class solution of conflict trajectory profiles.
The three-class model was determined to be the best-fitting and most interpretable and useful model (see Table 2 for fit indices for all solutions). A four-class model was also considered based on fit statistics, but ultimately rejected due to two classes (one of which represented only 5% of the sample) having the same patterns of change (i.e., significant linear decline of both slopes), reducing the usefulness of separating them. See Figure 1 for a graphical representation of the three longitudinal trajectory profiles. The average trajectory of the largest class (n = 148, 62%) was characterized by a relatively low initial level of interparental conflict at baseline (g0n = 1.34, SE = .03, z = 42.51, p <.001), which declined over the initial period of 9 months (g1n = −0.25, SE = .04, z = −5.74, p <.001) and remained stable over the follow-up period of 6 years (g2n = −0.01, SE = .01, z = −1.38, p = .168). The next largest class (n = 71, 30%) had a relatively higher mean baseline value of interparental conflict (g0n = 2.01, SE = .10, z = 20.12, p <.001) that declined over initial period (g1n = −0.73, SE = .12, z = −5.98, p <.001) and then declined again over the follow-up period (g2n = −0.06, SE = .01, z = −6.06, p < .001). The smallest group (n = 21, 9%) also had a relatively higher mean baseline value of interparental conflict (g0n = 1.96, SE = .18, z = 10.83, p <.001), but there was no significant change over the initial period (g1n = −0.33, SE = .19, z = −1.70, p =.089) and an increase over the follow-up period (g2n = 0.07, SE = .02, z = 3.02, p =.003). The trajectories were labeled Low Decreasing, High Decreasing, and High Increasing.
Table 2.
Model Fit Information for 1-Class Baseline Piecewise Growth Model and 2, 3, and 4-Class Piecewise Growth Mixture Models
| Fit Statistic | 1-class Model | 2-class Model | 3-class Model | 4-class Model |
|---|---|---|---|---|
| Class Counts & Proportions | 1.0 | 154/86 (.36/.64) | 21/71/148 (.09/.29/.62) | 12/18/75/135 (.05/.08/.31/.56) |
| AIC | 898.401 | 920.758 | 852.994 | 813.139 |
| BIC | 933.208 | 948.603 | 894.761 | 868.829 |
| SABIC | 901.510 | 923.245 | 856.724 | 818.113 |
| Entropy | - | .779 | .829 | .824 |
| VLMR p-value | - | <.001 | .201 | .227 |
| BLRT p-value | - | <.001 | <.001 | <.001 |
Note. AIC = Akaike information criterion; BIC = Bayesian information criterion (Schwarz, 1978); SABIC = sample-size adjusted Bayesian information criterion (Sclove, 1987); VLMR = Vuong-Lo-Mendell-Rubin likelihood ratio test (Lo et al., 2001); BLRT = bootstrapped likelihood ratio test (McLachlan & Peel, 2000).
Figure 1.
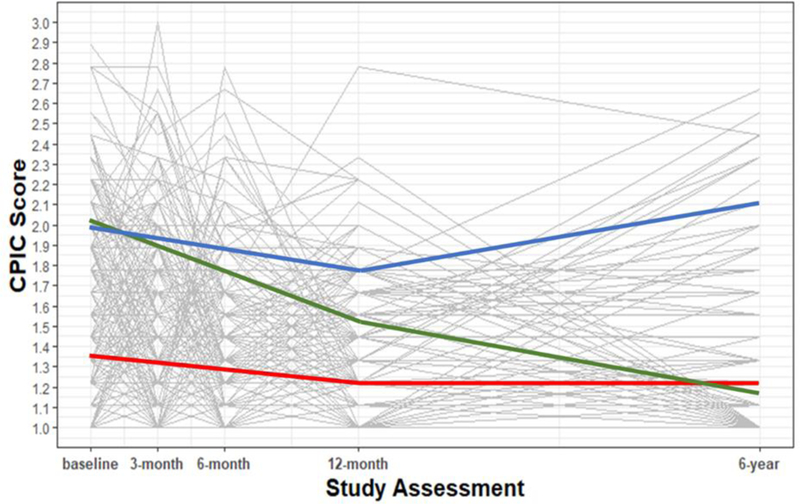
Estimated trajectories and observed individual values. CPIC = Children’s Perception of Interparental Conflict scale (Grych et al., 1992)
Aim 2: Examine Predictors of Group Membership and Group Differences among Trajectory Profiles
Predictors of group membership.
Results of multinomial regression analyses revealed no differences (χ2[2] = .80, p = .670) among the three trajectories of conflict in the proportion of families between the intervention groups (combined MP and MPCP2) and active control group (LC). Neither child age (χ2[2] = 1.05, p = .591) nor gender (χ2[2] = .16, p = .925) significantly predicted trajectory membership. There were no differences in likelihood of group membership based on the number of overnights the child spent with their father (χ2[2] = 1.95, p = .378), time since parental separation (χ2[2] = 2.53, p =. 282), or whether or not the child’s father moved out of the area following the divorce (χ2[2] = 2.21, p = .332) or remarried (χ2[2] = 2.24, p = .327). Finally, the extent to which mothers held a favorable view about the relationship between the child and their father marginally predicted group membership (χ2[2] = 4.86, p = .088). Mothers in the High Decreasing trajectory endorsed less favorable attitudes as compared to those in the Low Decreasing Trajectory (b = −0.05, p = .041, Exp(B) = .948, 95% CI = .902, .998).
Group differences among trajectory profiles.
See Table 3 for means and standard deviations for all dependent variables across the trajectories.
Table 3.
Means and Standard Deviations for Child Mental Health Outcomes by Conflict Trajectories
| Variable | Low Decreasing (n=148) | High Decreasing (n=71) | High Increasing (n=21) | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| Mother Report – Mental Health | ||||||
| Internalizing Problems – T1 | 56.20a | 9.05 | 59.31a | 9.99 | 58.90 | 11.06 |
| Externalizing Problems – T1 | 54.40 | 8.15 | 55.76 | 9.13 | 56.95 | 8.36 |
| Internalizing Problems – T5 | 51.11 | 9.58 | 53.81 | 8.42 | 55.31 | 9.87 |
| Externalizing Problems – T5 | 49.82 | 9.96 | 50.66 | 9.55 | 53.81 | 9.61 |
| Youth Report – Mental Health | ||||||
| Internalizing Problems – T1 | −.13a | .88 | .30a | .83 | −.07 | .94 |
| Externalizing Problems – T1 | −.20a | .85 | .43a,c | 1.17 | −.06c | .93 |
| Internalizing Problems – T5 | −.03 | .91 | -.01 | .96 | .20 | .86 |
| Externalizing Problems – T5 | −.05 | .92 | .02c | 1.10 | .30c | 1.18 |
| Youth Report - Risk Behaviors | ||||||
| Past Year Alcohol Use – T5 | 2.90 | 1.90 | 3.15 | 2.11 | 3.59 | 2.21 |
| Past Year Marijuana Use – T5 | 1.81a | 1.55 | 2.44a | 2.05 | 2.00 | 1.84 |
| Past Year # Sexual Partners – T5^ | .57a | .98 | .89a | 1.79 | .76 | .83 |
Note. T1 = baseline; T5 = six-year follow-up.
indicates that a negative binomial regression model was used for the count outcome of number of sexual partners.
significant mean differences between Low Decreasing and High Decreasing trajectories
significant mean differences between Low Decreasing and High Increasing trajectories
significant mean differences between High Decreasing and High Increasing trajectories
Mother-reported mental health problems.
At T1, mothers reported significantly higher child internalizing problems in the High Decreasing profile compared to the Low Decreasing profile (b = 3.14, p = 0.02). The High Increasing profile was not significantly different from High Decreasing (b = −0.52, p = .82) or the Low Decreasing (b = 2.63, p = .23) trajectories on T1 mother-reported internalizing problems. There were no significant differences in mother-reported externalizing problems at T1, nor in T5 mother-reported internalizing and externalizing problems.
Self-reported mental health problems.
At baseline, youth reported significantly higher internalizing problems in the High Decreasing profile compared to the Low Decreasing profile (b = 0.42, p < 0.001). The High Increasing profile was not significantly different from High Decreasing (b = −0.36, p = .10) or the Low Decreasing (b = 0.07, p = .74) trajectories on T1 self-reported internalizing problems. Youth also reported significantly higher baseline externalizing problems in the High Decreasing profile compared to the High Increasing profile (b = 0.50, p = 0.03) and the Low Decreasing profile (b = 0.62, p < 0.001). At six-year follow-up, youth in the High Increasing profile reported significantly higher externalizing problems, as compared to youth in the High Decreasing profile (b = 0.51, p = 0.05). The difference in means of the Low Decreasing vs. High Increasing (b = 0.38, p = .11) and vs. High Decreasing (b = −0.12, p = .42) trajectories were not significantly different. There were no significant differences in T5 self-reported internalizing problems.
Self-reported risk behaviors.
At T5, youth in the High Decreasing profile reported significantly higher past-year marijuana use (b = 0.69, p < 0.001) and number of sexual partners (b = 0.61, p = 0.04), as compared to youth in the Low Decreasing profile. The High Increasing profile was not significantly different from High Decreasing (b = −0.45, p = .33) or the Low Decreasing (b = .24, p = .58) trajectories on T5 marijuana use. Similarly, the High Increasing profile was not significantly different from High Decreasing (b = −0.10, p = .81) or the Low Decreasing (b = 0.51, p = .18) trajectories on T5 number of sexual partners. There were no significant differences among the trajectories on past year alcohol use.
Mental health and substance use disorders.
At T5, youth in the High Decreasing profile were significantly more likely to meet criteria for a mental health disorder (b = 0.98, p = .012), as compared to youth in the Low Decreasing profile. The odds ratio between the two trajectories was 2.66 (95% CI = 1.238, 5.726), indicating that the odds of being diagnosed with a mental health disorder was 2.66 times as likely in the High Decreasing profile as compared to the Low Decreasing profile. Examination of relative percentages indicated that 13% of youth in the Low Decreasing profile met diagnostic criteria for a mental health disorder compared to 27% in the High Decreasing profile. The youth in the High Decreasing trajectory had a range of mental health disorders, with the most common being: oppositional defiance disorder, attention-deficit hyperactivity disorder, and major depressive disorder. There were no statistically significant differences in diagnoses across the trajectories for substance use disorders.
Aim 3: Interaction Effects between Coping and Conflict Trajectory in the Prospective Prediction of Mental Health Problems and Risk Behaviors
See Table 4 for main effects of each coping subscale and significant coping by trajectory interaction effects for all dependent variables.
Table 4.
Main Effects of Coping Subscales and Interaction Effects of Trajectory by Coping Subscales on Six-Year Follow-Up (T5) Child Mental Health, Substance Use, And Risky Sexual Behavior Outcomes
| T5 outcome | Coping Subscale Main Effects | Coping X Trajectory Interaction Effects | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Avoidant | Positive Cognitive Restructuring | Coping Efficacy | Problem-focused | Coping Subscale | Trajectory Comparison | |||||||
| b | p | b | p | b | p | b | p | b | p | |||
| Externalizing Problems (youth report) | - | - | −0.12 | .002 | −0.51 | .009 | −0.06 | .092 | Avoidant Avoidant |
1 vs. 3 2 vs. 3 |
−0.42 −0.50 |
.050 .024 |
| Internalizing Problems (youth report) | −0.02 | .565 | −0.08 | .026 | −0.44 | .016 | - | - | PF | 2 vs. 1 | −0.16 | .026 |
| Externalizing Problems (mother report) | 0.48 | .184 | 0.00 | .999 | −0.51 | .759 | −0.32 | .306 | none | - | - | - |
| Internalizing Problems (mother report) | −0.01 | .982 | −0.61 | .066 | −3.15 | .057 | −0.63 | .050 | none | - | - | - |
| Alcohol Use (youth report) | −0.17 | .179 | −0.10 | .190 | −0.50 | .183 | −0.09 | .235 | none | - | - | - |
| Marijuana Use (youth report) | −0.05 | .631 | - | - | - | - | −0.07 | .330 | CE | 1 vs. 3 | 4.13 | .002 |
| CE | 2 vs. 3 | 4.64 | .001 | |||||||||
| PCR | 1 vs. 3 | 0.85 | .020 | |||||||||
| PCR | 2 vs. 3 | 0.81 | .032 | |||||||||
| Sexual Partners^ (youth report) | 0.02 | .778 | −0.13 | .050 | −0.89 | .032 | - | - | PF PF |
1 vs. 3 2 vs. 3 |
−0.56 −0.64 |
.038 .027 |
Note. Trajectory 1 = Low Decreasing, Trajectory 2 = High Decreasing, Trajectory 3 = High Increasing; PF = Problem-focused coping; PCR = Positive Cognitive Restructuring coping; CE = Coping Efficacy.
indicates that a negative binomial regression model was used for the count outcome of number of sexual partners. Bolded regression coefficients indicate statistical significance at p ≤ .05.
Problem-focused coping.
We found a significant problem-focused coping by trajectory profile interaction on youth-reported internalizing problems at T5 (see Figure 2). Pairwise comparisons indicated that the prospective association between problem-focused coping and youth reported internalizing problems significantly differed for youth in the High Decreasing trajectory relative to the Low Decreasing trajectory (b = −0.161, p = .026), controlling for T1 youth-reported internalizing problems. The association was not different for youth in the High Increasing as compared to either the High Decreasing or the Low Decreasing trajectory. Simple slope analyses indicated that the within-group slope for High Decreasing trajectory was significant and negative (b = −0.159, p = .008), indicating that higher levels of problem-focused coping were associated with lower levels of internalizing problems for these youth. There was also a significant problem-focused coping by trajectory profile interaction on youth-reported number of sexual partners at T5. Pairwise comparisons indicated that the prospective association between problem-focused coping and youth-reported risky sexual behavior significantly differed for youth in the High Increasing trajectory relative to both Low Decreasing (b = −0.557, p = .038) and High Decreasing (b = −0.636, p = .027). However, simple slope analyses indicated that the within-group slopes did not significantly differ from zero for any trajectory.
Figure 2.
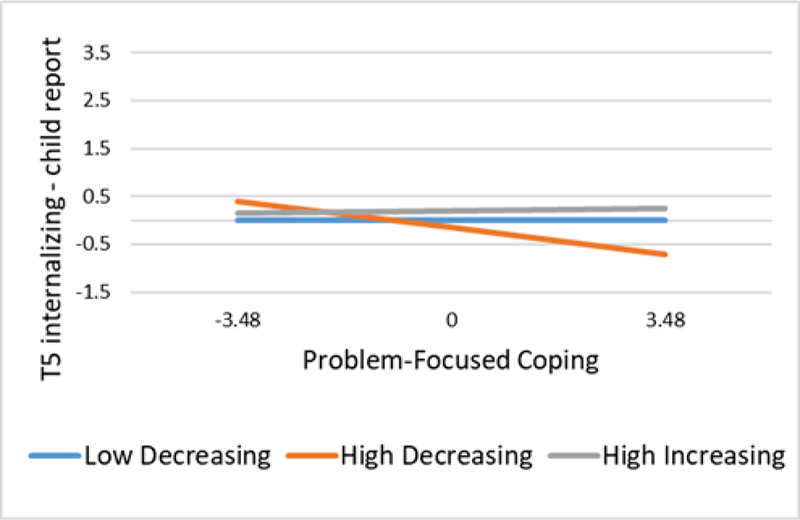
Association between problem-focused coping on T5 (six-year follow-up) child reported internalizing problems as a function of conflict trajectory. Problem-focused coping is mean-centered and displayed range represents ± 2 standard deviations.
We also found a significant main effect of problem-focused coping on mother-reported internalizing problems (b = −0.627, p = .050), indicating that higher levels of problem-focused coping were associated with lower levels of child internalizing problems at T5 across the three trajectory trajectories.
Positive cognitive restructuring coping.
We found a significant positive cognitive restructuring coping by trajectory interaction on T5 marijuana use (see Figure 3). Pairwise comparison tests indicated that the association was significantly different for youth in the High Increasing trajectory as compared to both the Low Decreasing (b = 0.848, p = .020) and compared to the High Decreasing trajectories (b = 0.810, p = .032). The Low Decreasing and High Decreasing trajectories were not significantly different. Simple slope analyses indicated that the within-group slope for High Increasing trajectory was significant and negative (b = - 0.907, p = .010), indicating that higher levels of positive cognitive restructuring coping were associated with lower levels of past year marijuana use.
Figure 3.
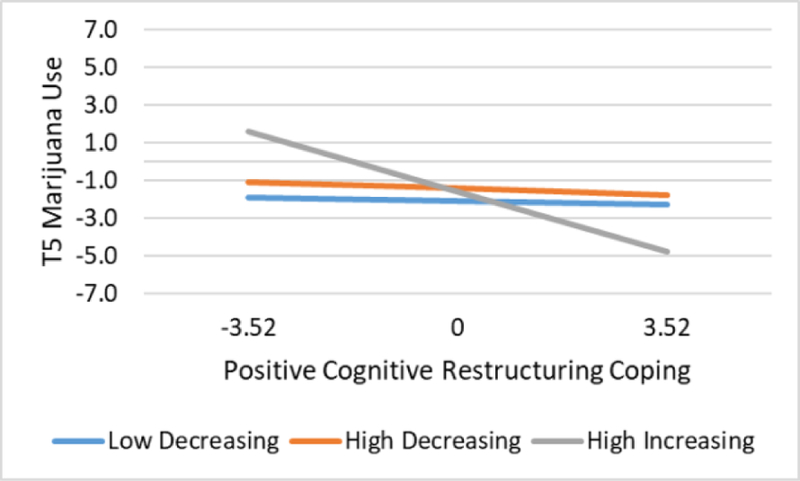
Association between positive cognitive restructuring coping on T5 (six-year follow-up) marijuana use as a function of conflict trajectory. Positive cognitive restructuring coping is mean-centered and displayed range represents ± 2 standard deviations.
We also found a significant main effect of positive cognitive restructuring coping on youth-reported internalizing problems (b = −0.078, p = .026), youth-reported externalizing problems (b = −0.117, p = .002), and number of sexual partners (b = −0.134, p = .050), indicating that higher levels of positive cognitive restructuring coping were associated with lower levels of self-reported youth mental health problems and risky sexual behavior at T5 across all trajectories. Results of regression diagnostics identified one potentially influential case for the analysis involving the number of sexual partners. When this analysis was re-run without the identified case, the main effect was no longer significant (b = −0.105, p = .110). Thus, this finding should be interpreted with caution.
Avoidant coping.
We found a significant avoidant coping by trajectory interaction on child-report externalizing problems at T5. Pairwise comparison tests indicated that the association significantly differed for youth in the High Increasing trajectory as compared to both the Low Decreasing (b = −0.415, p = .050) and High Decreasing trajectories (b = −0.499, p = .024). The Low Decreasing and High Decreasing trajectories were not significantly different. However, simple slope analyses indicated that the within-group slopes did not differ from zero for any trajectory, although the relation between avoidant coping and externalizing problems for the High Increasing trajectory was positive and marginal (b = .386, p = .063). There were no significant main effects of avoidant coping.
Coping efficacy.
We found a significant coping efficacy by trajectory interaction on T5 marijuana use (see Figure 4). Pairwise comparison tests indicated that the association was significantly different for youth in the High Increasing trajectory as compared to both the Low Decreasing (b = 4.128, p = .002) and High Decreasing trajectories (b = 4.644, p = .001). The Low Decreasing and High Decreasing trajectories were not significantly different. Simple slope analyses indicated that the within-group slope for High Increasing trajectory was significant and negative (b = −4.466, p < .001), indicating that higher levels of coping efficacy were associated with lower levels of past year marijuana use.
Figure 4.
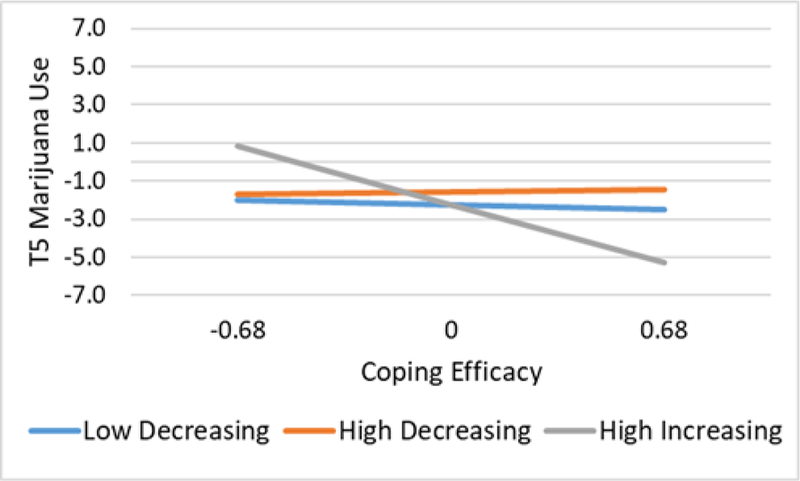
Association between coping efficacy on T5 (six-year follow-up) marijuana use as a function of conflict trajectory. Coping efficacy is mean-centered and displayed range represents ± 2 standard deviations.
We also found a significant main effect of coping efficacy on youth-reported externalizing problems (b = −0.509, p = .009), internalizing problems (b = −0.443, p = .016), and number of sexual partners (b = −0.892, p = .032), indicating that higher levels of coping efficacy were associated with lower levels of self-reported youth mental health problems and risky sexual behavior at T5. When this analysis was re-run without the identified influential case on the outcome of number of sexual partners, the main effect was no longer significant (b = −0.378, p = .234). Thus, this finding should be interpreted with caution.
Discussion
It is fitting that this paper is in the special issue that honors Tom Dishion. Tom was a champion of longitudinal research that probed the pathways that lead to children’s psychopathology. He had a special interest in the measurement of constructs in our developmental theories and he sought to use new and more powerful measures of each of these constructs. Most of all, Tom was devoted to developing and testing theories that had a direct link to interventions to prevent the development of psychopathology. Although the specific population and constructs that are the focus of this paper were not the focus of Tom’s work, this study fits well with his distinguished body of work, which demonstrated the fruitfulness of this kind of rigorous, longitudinal research with its focus on improved methods of measurement and implications for improving the lives of children.
This study makes two noteworthy contributions to the literature on interparental conflict and youth’s coping in the context of parental divorce. First, to our knowledge, it is the first to identify distinct longitudinal trajectories of change in youth-reported interparental conflict over six years and demonstrate that two trajectories (high initial levels that decrease over time and high initial levels that increase over time) confer risk for mental health and substance use problems as compared to low initial conflict that decreases over time. Second, it is the first study to examine how trajectories of conflict interact with various aspects of youth’s coping to predict mental health, substance use, and high-risk sexual behavior outcomes six to eight years after the divorce. Some interaction effects emerged indicating that problem-focused coping, positive cognitive restructuring, and coping efficacy, may be particularly strongly prospectively related to problem outcomes (e.g., marijuana use) for children exposed to higher levels of conflict over time. However, other aspects of coping, mainly positive cognitive restructuring and coping efficacy, exerted prospective main effects on youth’s internalizing and externalizing problems. These findings extend prior research by identifying the long-term prospective effects of children’s coping styles and coping efficacy on mental health problems following parental divorce (Sandler et al., 2000). We discuss results from each study aim and contextualize the findings by discussing how the findings fit with prior literature and theoretical models on youth’s coping in the context of interparental conflict. We end with a discussion of the theoretical and intervention implications of the findings, as well as the limitations of the study and directions for future research.
Longitudinal Trajectories of Child Reported Interparental Conflict
We identified three distinct trajectories of conflict over the course of six to eight years after parental divorce. One group had the lowest relative level of baseline conflict, decreased over the course of the first year of the study and then remained low and stable at the six-year follow-up. We labeled this trajectory Low Decreasing. The size of this group (62%) aligns with previous literature suggesting that despite the ubiquitous nature of some level of conflict around the time of divorce, interparental conflict decreases over the first few years following parental divorce for most families (Hetherington & Kelly, 2002). The second largest group (30%) had a relatively high level of baseline conflict, but the conflict declined over the course of the first year of the study, and then declined even further at six-year follow-up. We labeled this trajectory of conflict High Decreasing. This group is distinguished from the former group because although interparental conflict declines for both trajectories and have a similar level of conflict at the six-year follow-up, the High Decreasing trajectory start out having higher levels of conflict and thus, children spend more time being exposed to a relatively high level of conflict. The smallest group (9%) also had a relatively high level of baseline conflict, but it did not significantly change over the course of the first year of the study, and then it increased at six-year follow-up. We labeled this trajectory of conflict High Increasing. This trajectory likely represents the families who are enmeshed in high levels of chronic conflict for many years following divorce/separation. Theoretically, the youth exposed to this trajectory of interparental conflict are likely to have the most severe consequences. The proportion of families displaying this longitudinal trajectory is smaller than the estimated number of families engaged in high levels of conflict following divorce in previous studies (e.g., 20–25% in Hetherington’s [2002] study and 15–20% in a study by Sbarra and Emery [2005]). However, these point-in-time estimates do not assess the trajectory of change in conflict over time, which the current study finds is important in understanding the long-term association between conflict and children’s post-divorce adjustment problems.
Relations between Theoretical Predictors and Longitudinal Trajectories of Change in Interparental Conflict
Based on previous research, we attempted to relate the conflict trajectories to theoretical predictors (i.e., information collected at baseline) that might help inform how we can prospectively predict which families will end up exhibiting the different trajectories of conflict. We tested variables that were both demonstrated in previous studies to be related to level of conflict and available to use in the dataset. Factors related to child demographics (i.e., age, gender) and post-divorce family circumstance (i.e., father relocation and remarriage, time since separation) were not related to membership in a conflict trajectory. Maternal attitudes toward the relationship between father and child was the only factor that marginally predicted membership in one group versus another. Families in which mothers held less favorable views about their child’s relationship with the father were more likely be in the High Decreasing versus Low Decreasing trajectory. To note, the group means in the High Increasing and High Decreasing trajectories were very similar (within .17 raw units on a scale with a range of 26); the lack of significant differences between the High Increasing and Low Decreasing trajectories is likely due to the small size of the High Increasing trajectory. To the extent that this effect is replicable, parental attitudes about the child’s relationship with the other parent may be a key factor in identifying families at high-risk for damaging trajectories of interparental conflict. Future research on parental attitudes about one another should incorporate new concepts being developed about the fundamental dynamics that characterize the conflict, such as entrenched interparental hatred (Smyth & Moloney, 2017, 2019)
Relations between Concurrent and Prospective Mental Health Problems and Risky Behaviors and Trajectories of Interparental Conflict
The three trajectories of interparental conflict differ in levels of youth’s baseline and six-year mental health and substance use problems. At baseline, there were significant differences among the trajectories in the level of internalizing problems, according to both mother- and self-report. Youth in the High Decreasing trajectory demonstrated higher levels of mother- and child-reported internalizing problems relative to the Low Decreasing trajectory. In addition, according to self-report only, youth in the High Decreasing trajectory had higher levels of externalizing problems relative to the Low Decreasing and High Increasing trajectories. The findings that the High Decreasing trajectory showed higher levels of child mental health problems than the Low Decreasing trajectory likely reflects the impact of their higher levels of conflict at baseline. The finding that the High Decreasing trajectory showed higher levels of externalizing than the High Increasing trajectory at baseline does not continue over the six years, as discussed below. This suggests that there may be other important contextual factors at play beyond exposure to interparental conflict. For example, the High Decreasing trajectory may be more prone to experience a higher number of non-conflict divorce-related stressors, highlighting the importance of future research to extend the investigation of contextual correlates of the different trajectories.
The trajectories were also useful in predicting group differences at the six-year follow-up. Youth in the High Decreasing trajectory demonstrated higher marijuana use and risky sexual behavior and were more likely to be diagnosed with a mental health disorder as compared to youth in the Low Decreasing trajectory (OR = 2.66). In terms of clinical significance, youth in the High Decreasing trajectory were more than twice as likely to have a diagnosable mental health disorder six years later as compared to youth in the Low Decreasing trajectory. With regard to relative percentages, 13% of youth in the Low Decreasing trajectory had a diagnosable mental health disorder according to either parent or self-report on the DISC at the six-year follow-up, compared to 24% and 27% of youth in the two high-conflict trajectories (High Increasing and High Decreasing, respectively). This is the first study we know of to identify the long-term consequences of exposure to post-divorce interparental conflict in terms of diagnosable mental disorders. Notably, at the six-year follow-up, the High Decreasing trajectory did not have higher levels of conflict than the Low Decreasing trajectory, indicating that the long-term problems experienced by children in the High Decreasing trajectory may reflect the persistent negative effects of earlier exposure to interparental conflict.
Interestingly, the differences in externalizing problems changed between baseline and six-year follow-up for the High Increasing and High Decreasing trajectories. At baseline, the High Decreasing trajectory had the highest level of externalizing problems, but at the six-year follow-up, the High Increasing trajectory demonstrated the highest level of externalizing problems, significantly higher than the High Decreasing trajectory. Similarly, although the youth in the High Increasing trajectory were indistinguishable from the Low Decreasing trajectory at baseline, higher rates of externalizing problems emerged in this trajectory at the six-year follow-up, potentially reflecting the cumulative effects of exposure to chronic conflict over an extended period of time.
Taken together, it appears that the youth in the two high conflict trajectories – regardless of whether it eventually declines or remains high – show deleterious effects on one or more measures of mental health, substance use, and risky behavior problems at the six-year follow-up. There is some evidence of more consistent adverse effects in the High-Decreasing trajectory than in the High-Increasing trajectory. However, the magnitude of the differences is quite modest. It is possible that there are important differences between the two trajectories in the pattern of conflict to which the children were exposed prior to the study period (i.e., prior to and immediately following separation), the nature and number of other divorce-related stressors that occurred prior to the baseline assessment, or both, that may explain the modest differences. Research that includes a larger trajectory of the High-Increasing families and assesses conflict and other stressors before and immediately after the separation is an important direction for future research.
Together the two high-risk trajectories include 39% of the sample as being at risk due to exposure to post-divorce interparental conflict, which is a considerably higher percentage of high conflict divorces as compared with previous point-in-time estimates (Sbarra & Emery, 2005; Hetherington & Kelly, 2002). These findings are consistent with decades of previous research on youth exposed to interparental conflict (see Rhoades, 2008 for a meta-analysis). However, this is the first study to demonstrate that trajectories of interparental conflict over time are associated with problem outcomes and that exposure to high interparental conflict is associated with higher prevalence of diagnosed mental disorder.
Prospective Relations of Coping with Problem Outcomes across Trajectories of Interparental Conflict
We found both main effects of coping and coping by conflict trajectory interaction effects in predicting problem outcomes at the six-year follow-up. The prospective effects of coping over six years extend prior evidence on the short-term relations between coping and mental health problems of children from divorced families (Sandler et al., 2000, 1994). First, we found unique effects of problem-focused coping on youth-reported and mother-reported internalizing problems. Higher levels of problem-focused coping predicted lower levels of mother-reported internalizing problems for all youth. Using child report, the relation between problem-focused coping and internalizing problems was conditioned by trajectory, demonstrating a protective effect for youth in the High Decreasing trajectory. The finding that the effects of problem-focused coping was particularly strong for the High Decreasing trajectory seems counter to the expectation that the use of problem-focused coping would be ineffective or even iatrogenic in dealing with uncontrollable stressors such as the conflict between parents (e.g., Tu et al., 2016). Children cannot stop their parents from fighting, and attempts to do so are likely to be highly stressful. However, the group for whom problem-focused coping was found to be most helpful was the one in which there was high initial conflict which decreased over six years. These youth may be using their problem-solving skills to find new ways to find satisfying life experiences as their parents’ conflict wanes over time. It is also important to note that problem-focused coping as assessed in this study includes behaviors beyond direct problem solving, such as thinking about all the ways to solve or handle a problem. This highlights the importance of considering differential effects of coping strategies that may fall under a broad category of coping. Although direct problem solving may not be effective in the context of interparental conflict, thinking about one’s options (beyond direct intervention) for handling a seemingly uncontrollable problem may have a very different impact. Taken together, the main and interaction effects indicate that a coping style high in use of problem-focused strategies may be protective against internalizing problems, potentially even more so for youth exposed to high conflict during the first few years following divorce.
The patterns of association related to positive cognitive restructuring coping and coping efficacy were nearly identical. Significant negative main effects of both positive cognitive restructuring and coping efficacy occurred for youth-reported internalizing and externalizing problems. These aspects of coping have been found in previous research to have generally protective effects although this is the first study to show that they prospectively relate to lower levels of child mental health problems over six years for children from divorced families. It is possible that these skills enable children to make positive appraisals of the conflict, reassuring them that although they are in conflict with each other, their parents care about them and that they are not to blame for the conflict. In addition, a subjective sense of coping efficacy may enhance their sense of control over the stressors in their lives. Future research on the mediating processes that explain positive effects of coping on outcomes for children in high conflict families is needed. Interestingly, the effect of positive cognitive restructuring and coping efficacy on youth’s report of past year marijuana use differed by group. Positive cognitive restructuring coping and coping efficacy had a protective effect of for youth in the High Increasing trajectory, but there were no effects of either aspect of coping on marijuana use in the other two trajectories. These results suggest that coping efficacy and positive cognitive restructuring are generally adaptive for all youth who experience divorce and may be particularly important in buffering against substance use for youth exposed to high levels of chronic conflict. The findings of the current study demonstrate that positive cognitive restructuring and coping efficacy may be protective for all children, including those exposed to high conflict.
Finally, we found that for youth in the High Increasing trajectory there was a marginally significant relation between avoidant coping and higher youth-reported externalizing problems. Although this effect was only marginally significant and thus requires replication, it is consistent with prior research showing adverse effects of avoidant coping (Aldao, Nolen-Hoeksema, & Schweizer, 2010; Compas et al., 2017; Nicolotti et al., 2003; Sandler et al., 1994; Tu et al., 2016). These results suggest that high use of avoidant coping may be particularly detrimental for youth who are exposed to high levels of chronic conflict over time.
It is important to emphasize the findings that were corroborated by mothers’ report of child mental health problems given concerns about shared method variance associated with the use of youth report of the study variables in the majority of the models. Both youth and mother reports indicated that youth in the High Decreasing trajectory demonstrated higher internalizing problems relative to those in the Low Decreasing trajectory. In addition, the main effects of positive cognitive restructuring and coping efficacy on internalizing problems at T5 were consistent across youth and mother reports but the effects were marginal for mother report.
The current findings extend prior evidence on the effects of coping with interparental conflict in several ways. First, although there is extensive evidence that the ways in which children respond to or cope with interparental conflict moderates the effect of their exposure to conflict and maladjustment (Cummings et al., 1994; Jenkins, Smith, & Graham, 1989; Nicolotti et al., 2003; Shelton & Harold, 2007; Tu et al., 2016), the majority of this work has been conducted with children from married or two-parent families (Cummings et al., 1994; Jenkins et al., 1989; O’Brien, Bahadur, Gee, Balto, & Erber, 1997; Tu et al., 2016) and most of the focus has been on the child’s proximal responses to conflict. The current findings extend this work by demonstrating a significant long-term prospective protective relation between general coping styles and children’s mental health and risky behaviors in divorced families and showing that the effect is particularly strong for children exposed to high levels of conflict, even if the conflict decreases over time.
Integrating Theoretical Frameworks for Children’s Coping with Post-Divorce Conflict
The findings from this study can be understood from the perspective of a broad conceptual model that identifies the ecology of adversity (Sandler, 2001) as one of two key constructs for understanding adaptation to adversities such as interparental conflict. Sandler (2001) proposed that the ecology of adversity includes factors such as the broader context and the settings in which it occurs, particularly its intensity and temporal and cumulative nature. One way that the current study extends evidence on the effects of conflict across family contexts is by studying conflict in the context of divorced families rather than married families where much of the prior research has been conducted. A second way the current study extends our understanding of the effects of the ecology of conflict is by identifying how the temporal and cumulative nature of interparental conflict is related to the development of children’s mental health outcomes. This study demonstrates that understanding the effects of exposure to interparental conflict following divorce on children’s mental health requires that we integrate understanding of the contextual aspects of exposure to conflict, including the different trajectories of conflict exposure over time, children’s cognitive and behavioral coping strategies, and the interaction between the two.
Implications for Intervention Development
The findings from the current study have several implications for the design of preventive interventions for children exposed to post-divorce interparental conflict. The finding that 39% of the sample was exposed to a high-risk trajectory of post-divorce conflict indicates that although the majority of children adapt well following divorce, a substantial sub-group could benefit from preventive interventions. The finding that the trajectory of exposure to conflict is associated with diagnosable mental disorder and both child and parent report of level of mental health problems emphasizes the potential public health benefit of effective preventive parenting interventions that target reductions in conflict. The prospective relations between coping and children’s mental health and substance use problems provides important information about how improving youth’s general capacity to cope adaptively can be seen as a potentially modifiable protective factor for children exposed to post-divorce interparental conflict. Findings from this study indicate that positive cognitive restructuring coping, problem-focused coping, and coping efficacy appear to be effective for all children facing parental divorce and are particularly helpful for those exposed to trajectories involving high post-divorce conflict. Thus, teaching these strategies may be beneficial as mechanisms of change to be targeted in child-focused preventive interventions. This is consistent with prior studies that have reported positive effects of coping interventions for children from divorced families (Boring, Sandler, Tein, Horan, & Vélez, 2015; Pedro-Carroll, 2005; Pedro-Carroll & Cowen, 1985). Although these trials have not studied long-term effects, the current findings of long-term prospective effects of coping on child mental health problems indicates that it is reasonable to expect that teaching coping will have long-term benefits for children following divorce. The finding that the trajectory of exposure to interparental conflict is associated with long-term problem outcomes indicates that children in families with high levels of post-divorce conflict are a particularly appropriate group to target for coping-focused preventive interventions. From the perspective of precision medicine, or individualized prevention, matching treatment components to an individual’s contextual data, including family-level factors, is crucial to improving effectiveness and efficiency of mental health interventions (Bickman, Lyon, & Wolpert, 2016).
It is important to note that the current study used data from a preventive intervention trial of a parenting program that targeted improvements in positive parenting practices and reductions in interparental conflict. Although the current study is not focused on intervention effects, we did find that intervention condition did not discriminate the conflict trajectories. This finding is consistent with previous reports showing a lack of NBP program effects on interparental conflict (Wolchik et al., 2000). The absence of intervention effects is likely due to the limited attention to interparental conflict in the program (i.e., one session). Future research could test the effects of a modified program that included additional attention to teaching strategies and skills to reduce interparental conflict. It may also be that for significant reductions in conflict to occur, both fathers and mothers need to learn effective conflict management skills.
A limitation of these findings for the design of interventions is that coping was assessed as a general style, and not as coping specifically with the stress of exposure to interparental conflict. The findings of this study are silent as to the effects of youth coping strategies in the moments when they are being exposed to interparental conflict. We know from previous research that conflict between parents can take on many forms and that a range of behaviors, including engaging in intense and hostile arguments, denigrating the other parent to the child, placing the child in the middle of an argument or asking them to act as a go-between, can be damaging to a child (Bradford & Barber, 2005; Buchanan et al., 1991; Davies et al., 2016; Johnston, 1994; Rowen & Emery, 2018). Because the current study assessed general coping strategies rather than coping with the specific challenges posed by different conflict situations research that identifies such situation specific coping strategies is needed to help design preventive interventions.
Limitations and Future Directions for Research
Several limitations must be considered. First, growth mixture modeling is an exciting method of statistically identifying unobserved subgroups, but the exploratory and data-driven nature of the approach should not be dismissed. These findings need to be replicated in an independent sample, preferably a large sample that allows for more precise estimation of the correlates of the smallest group in this sample. Second, we attempted to ensure that our measure of coping was stable enough to represent the construct of youth’s coping across the first year of the study period, which corresponded with coping within the first 2–3 years following parental divorce. However, it should be noted that the stability estimates differed across the coping subscales, with the lowest (problem-focused coping) having an autoregressive standardized path coefficient of .38. Interpretations about the magnitude of stability coefficients are a topic of debate among researchers and inherently subjective, particularly as it relates to theoretical understanding of stability as a continuum that encompasses traits to styles or habits (Kenny & Zautra, 2001). Clearly, more work on longitudinal stability in the measurement of youth’s coping is needed. Third, the current study used data from an intervention study that targeted children with mothers as primary caretakers and that included primarily white, non-Hispanic or Latino families. Given the changing landscape with regard to the demographic characteristics of divorcing families and allocations of parenting time following divorce (Meyer, Cancian, & Cook, 2017) future studies should include youth from more ethnically diverse samples and families with a broad range of parenting time arrangements. Including children in families with a range of parenting time arrangements may be particularly important given the mixed nature of findings from prior research on whether shared parenting in the presence of high interparental conflict is protective or increases risk for children (Mahrer, O’Hara, Sandler, & Wolchik, 2018; Mahrer et al., 2016). Fourth, children and mothers who were participating in mental health treatment at the time of the study were excluded and therefore the findings may not be generalizable to all recently separated families, especially those struggling with significant mental health problems. Finally, interparental conflict is typically at its highest during the first year following parental separation. The average time since physical separation in this study was two years. Thus, the absence of information during the initial months following separation means that the conflict trajectories derived from these data do not capture the period in which conflict is likely to be highest for many families. Similarly, there was a 5-year gap between the 4th and 5th assessments, limiting our ability to describe the changes in conflict that have occurred between these two time points. An important area for future studies will be to prospectively follow families from an earlier time point, ideally prior to or immediately following the separation, using more frequent assessments to provide improved precision about questions pertaining to change over time in levels of interparental conflict.
Acknowledgments
The research was supported by grants from the National Institute of Mental Health (R01MH057013 and P30MH39346). The first author’s work on this paper was supported by a postdoctoral fellowship provided by the National Institute on Drug Abuse (T32DA039772) through the Psychology Department and the Research and Education Advancing Children’s Health (REACH) Institute at Arizona State University. The third author’s work was supported by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01HD094334).
Footnotes
Data from a technical report to the Australian government describe stability or change in the quality of the interparental relationship across three time periods, indicating that 41% of parents report a positive relationship consistently across time while only 4% consistently report a negative relationship (Qu, Weston, Moloney, Kaspiew, & Dunstan, 2014).
The two intervention conditions were combined based on previous analyses indicating no additive effects of the MPCP over and above the MP. See (Wolchik et al., 2002, 2000, 2007).
References
- Achenbach TM, & Rescorla LA (2001). Manual for the Achenbach system of empirically based assessment school-age forms profiles Burlington, VT. [Google Scholar]
- Aldao A (2013). The future of emotion regulation research: Capturing context. Perspectives on Psychological Science, 8(2), 155–172. 10.1177/1745691612459518 [DOI] [PubMed] [Google Scholar]
- Aldao A, Nolen-Hoeksema S, & Schweizer S (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30(2), 217–237. 10.1016/j.cpr.2009.11.004 [DOI] [PubMed] [Google Scholar]
- Amato PR (1993). Children’s adjustment to divorce: Theories, hypotheses, and empirical support. Journal of Marriage and Family, 55(1), 23–38. 10.2307/352954 [DOI] [Google Scholar]
- Amato PR (2000). The consequences of divorce for adults and children. Journal of Marriage and Family, 62(4), 1269–1287. [Google Scholar]
- Amato PR (2001). Children of divorce in the 1990s: An update of the Amato and Keith (1991) meta-analysis. Journal of Family Psychology, 15(3), 355. [DOI] [PubMed] [Google Scholar]
- Amato PR, & Sobolewski JM (2001). The effects of divorce and marital discord on adult children’s psychological well-being. American Sociological Review, 66(6), 900–921. 10.2307/3088878 [DOI] [Google Scholar]
- Andersson G (2002). Children’s experience of family disruption and family formation: Evidence from 16 FFS countries. Demographic Research, 7, 343–364. 10.4054/DemRes.2002.7.7 [DOI] [Google Scholar]
- Ayers TS, Sandler IN, & Twohey JL (1998). Conceptualization and measurement of coping in children and adolescents. In Advances in clinical child psychology (pp. 243–301). Springer. [Google Scholar]
- Ayers TS, Sandler IN, West SG, & Roosa MW (1996). A dispositional and situational assessment of children’s coping: Testing alternative models of coping. Journal of Personality, 64(4), 923–958. [DOI] [PubMed] [Google Scholar]
- Bandura A (1997). Self-efficacy: The exercise of control New York, NY, US: W H Freeman/Times Books/ Henry Holt & Co. [Google Scholar]
- Bauserman R (2012). A meta-analysis of parental satisfaction, adjustment, and conflict in joint custody and sole custody following divorce. Journal of Divorce & Remarriage, 53(6), 464–488. 10.1080/10502556.2012.682901 [DOI] [Google Scholar]
- Bickham NL, & Fiese BH (1997). Extension of the Children’s Perceptions of Interparental Conflict Scale for use with late adolescents. Journal of Family Psychology, 11(2), 246–250. [Google Scholar]
- Bickman L, Lyon AR, & Wolpert M (2016). Achieving precision mental health through effective assessment, monitoring, and feedback processes: Introduction to the special issue. Administration and Policy in Mental Health and Mental Health Services Research, 43(3), 271–276. 10.1007/s10488-016-0718-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Billings AG, & Moos RH (1981). The role of coping responses and social resources in attenuating the stress of life events. Journal of Behavioral Medicine, 4(2), 139–157. [DOI] [PubMed] [Google Scholar]
- Bollen KA, & Jackman RW (1985). Regression diagnostics: An expository treatment of outliers and influential cases. Sociological Methods & Research, 13(4), 510–542. [Google Scholar]
- Boring JL, Sandler IN, Tein J-Y, Horan JJ, & Vélez CE (2015). Children of Divorce–Coping with Divorce: A randomized control trial of an online prevention program for youth experiencing parental divorce. Journal of Consulting and Clinical Psychology, 83(5), 999–1005. 10.1037/a0039567 [DOI] [PubMed] [Google Scholar]
- Bradford K, & Barber BK (2005). Interparental conflict as intrusive family process. Journal of Emotional Abuse, 5(2/3), 143–167. 10.1300/J135v05n02_07 [DOI] [Google Scholar]
- Buchanan CM, Maccoby EE, & Dornbusch SM (1991). Caught between parents: Adolescents’ experience in divorced homes. Child Development, 62(5), 1008–1029. [DOI] [PubMed] [Google Scholar]
- Buehler C, Anthony C, Krishnakumar A, Stone G, Gerard J, & Pemberton S (1997). Interparental conflict and youth problem behaviors: A meta-analysis. Journal of Child and Family Studies, 6(2), 233–247. [Google Scholar]
- Camisasca E, Miragoli S, Di Blasio P, & Grych J (2017). Children’s coping strategies to inter-parental conflict: The moderating role of attachment. Journal of Child and Family Studies, 26(4), 1099–1111. 10.1007/s10826-016-0645-9 [DOI] [Google Scholar]
- Cohen J, Cohen P, West SG, & Aiken LS (2003). Applied multiple regression/correlation analysis for the behavioral sciences (3rd ed). Mahwah, N.J: L. Erlbaum Associates. [Google Scholar]
- Compas BE, Banez GA, Malcarne V, & Worsham N (1991). Perceived control and coping with stress: A developmental perspective. Journal of Social Issues, 47(4), 23–34. 10.1111/j.1540-4560.1991.tb01832.x [DOI] [Google Scholar]
- Compas BE, Connor-Smith JK, Saltzman H, Thomsen AH, & Wadsworth ME (2001). Coping with stress during childhood and adolescence: Problems, progress, and potential in theory and research. Psychological Bulletin, 127(1), 87–127. 10.1037//0033-2909.127.1.87 [DOI] [PubMed] [Google Scholar]
- Compas BE, Jaser SS, Bettis AH, Watson KH, Gruhn MA, Dunbar JP, … Thigpen JC (2017). Coping, emotion regulation, and psychopathology in childhood and adolescence: A meta-analysis and narrative review. Psychological Bulletin, 143(9), 939–991. 10.1037/bul0000110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connor-Smith JK, Compas BE, Wadsworth ME, Thomsen AH, & Saltzman H (2000). Responses to stress in adolescence: Measurement of coping and involuntary stress responses. Journal of Consulting and Clinical Psychology, 68(6), 976–992. 10.1037//0022-006X.68.6.976 [DOI] [PubMed] [Google Scholar]
- Cook C (1986). The Youth-Self-Report Hostility Scale Unpublished manuscript, Program for Prevention Research, Arizona State University, Tempe, AZ. [Google Scholar]
- Cummings EM, & Davies P (2010). Marital conflict and children: An emotional security perspective New York: Guilford Press. [Google Scholar]
- Cummings EM, Davies P, & Simpson K (1994). Marital conflict, gender, and children’s appraisals and coping efficacy as mediators of child adjustment. Journal of Family Psychology, 8(2), 141–149. 10.1037/0893-3200.8.2.141 [DOI] [Google Scholar]
- Cummings EM, George MR, McCoy KP, & Davies PT (2012). Interparental conflict in kindergarten and adolescent adjustment: Prospective investigation of emotional security as an explanatory mechanism. Child Development, 83(5), 1703–1715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cummings EM, Schermerhorn AC, Davies PT, Goeke-Morey MC, & Cummings JS (2006). Interparental discord and child adjustment: Prospective investigations of emotional security as an explanatory mechanism. Child Development, 77(1), 132–152. [DOI] [PubMed] [Google Scholar]
- Danese A, & McEwen BS (2012). Adverse childhood experiences, allostasis, allostatic load, and age-related disease. Physiology & Behavior, 106(1), 29–39. 10.1016/j.physbeh.2011.08.019 [DOI] [PubMed] [Google Scholar]
- Davies PT, & Cummings EM (1994). Marital conflict and child adjustment: An emotional security hypothesis. Psychological Bulletin, 116(3), 387–411. 10.1037/0033-2909.116.3.387 [DOI] [PubMed] [Google Scholar]
- Davies PT, Hentges RF, Coe JL, Martin MJ, Sturge-Apple ML, & Cummings EM (2016). The multiple faces of interparental conflict: Implications for cascades of children’s insecurity and externalizing problems. Journal of Abnormal Psychology, 125(5), 664–678. 10.1037/abn0000170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fear JM, Champion JE, Reeslund KL, Forehand R, Colletti C, Roberts L, & Compas BE (2009). Parental depression and interparental conflict: Children and adolescents’ self-blame and coping responses. Journal of Family Psychology, 23(5), 762–766. 10.1037/a0016381 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fischer T, de Graaf P, & Kalmijn M (2005). Friendly and antagonistic contact between former spouses after divorce: Patterns and determinants. Journal of Family Issues, 26(8), 1131–1163. 10.1177/0192513X05275435 [DOI] [Google Scholar]
- Forsythe CJ, & Compas BE (1987). Interaction of cognitive appraisals of stressful events and coping: Testing the goodness of fit hypothesis. Cognitive Therapy and Research, 11(4), 473–485. [Google Scholar]
- Fosco GM, & Grych JH (2008). Emotional, cognitive, and family systems mediators of children’s adjustment to interparental conflict. Journal of Family Psychology, 22(6), 843–854. 10.1037/a0013809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goeke-Morey MC, Cummings EM, & Papp LM (2007). Children and marital conflict resolution: Implications for emotional security and adjustment. Journal of Family Psychology, 21(4), 744–753. 10.1037/0893-3200.21.4.744 [DOI] [PubMed] [Google Scholar]
- Greenaway KH, Kalokerinos EK, & Williams LA (2018). Context is everything (in emotion research). Social and Personality Psychology Compass, 0(0), e12393 10.1111/spc3.12393 [DOI] [Google Scholar]
- Grimm KJ, Ram N, & Estabrook R (2016). Growth modeling: Structural equation and multilevel modeling approaches Guilford Publications. [Google Scholar]
- Grych JH (2005). Interparental conflict as a risk factor for child maladjustment: Implications for the development of prevention programs. Family Court Review, 43(1), 97–108. [Google Scholar]
- Grych JH, & Fincham FD (1990). Marital conflict and children’s adjustment: A cognitive-contextual framework. Psychological Bulletin, 108(2), 267–290. 10.1037/0033-2909.108.2.267 [DOI] [PubMed] [Google Scholar]
- Grych JH, & Fincham FD (1993). Children’s appraisals of marital conflict: Initial investigations of the Cognitive-Contextual Framework. Child Development, 64(1), 215–230. [DOI] [PubMed] [Google Scholar]
- Grych JH, Fincham FD, Jouriles EN, & McDonald R (2000). Interparental conflict and child adjustment: Testing the mediational role of appraisals in the cognitive-contextual framework. Child Development, 71(6), 1648–1661. 10.1111/1467-8624.00255 [DOI] [PubMed] [Google Scholar]
- Grych JH, Harold GT, & Miles CJ (2003). A prospective investigation of appraisals as mediators of the link between interparental conflict and child adjustment. Child Development, 74(4), 1176–1193. [DOI] [PubMed] [Google Scholar]
- Grych JH, Seid M, & Fincham FD (1992). Assessing marital conflict from the child’s perspective: The Children’s Perception of Interparental Conflict Scale. Child Development, 63(3), 558–572. [DOI] [PubMed] [Google Scholar]
- Ha AP, Bergman KN, Davies PT, & Cummings EM (2018). Parental Postconflict Explanations: Implications for Children’s Adjustment Outcomes. Family Court Review, 56(2), 219–233. 10.1111/fcre.12336 [DOI] [Google Scholar]
- Hetherington E, & Kelly J (2002). Divorce reconsidered: For better or worse New York: Norton. [Google Scholar]
- Hetherington EM, Cox M, & Cox R (1982). Effects of divorce on parents and children. In Lamb ME (Ed.), Nontraditional families: Parenting and child development (pp. 233–288). Hillsdale, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Jaser SS, Champion JE, Reeslund KL, Keller G, Merchant MJ, Benson M, & Compas BE (2007). Cross-situational coping with peer and family stressors in adolescent offspring of depressed parents. Journal of Adolescence, 30(6), 917–932. 10.1016/j.adolescence.2006.11.010 [DOI] [PubMed] [Google Scholar]
- Jenkins JM, Smith MA, & Graham PJ (1989). Coping with parental quarrels. Journal of the American Academy of Child & Adolescent Psychiatry, 28(2), 182–189. [DOI] [PubMed] [Google Scholar]
- Johnston JR (1994). High-Conflict Divorce. The Future of Children, 4(1), 165 10.2307/1602483 [DOI] [PubMed] [Google Scholar]
- Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, & Patrick ME (2018). Monitoring the Future national survey results on drug use, 1975–2017: Overview, key findings on adolescent drug use [Google Scholar]
- Kelly JB (2012). Risk and protective factors associated with child adolescent adjustment following separation and divorce. In Kuehnle K & Drozd L (Eds.), Parenting plan evaluations: Applied research for the family court (pp. 49–84). New York, NY: Oxford University Press. [Google Scholar]
- Kelly JB, & Emery RE (2003). Children’s adjustment following divorce: Risk and resilience perspectives. Family Relations, 52(4), 352–362. [Google Scholar]
- Kennedy S, & Bumpass L (2008). Cohabitation and children’s living arrangements: New estimates from the United States. Demographic Research, 19, 1663–1692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kenny D, & Zautra A (2001). Trait-state models for longitudinal data. In Collins LM & Sayer AG (Eds.), New methods for the analysis of change (pp. 243–263). 10.1037/10409-000 [DOI] [Google Scholar]
- Kerig PK (2001). Children’s Coping with Interparental Conflict. In Grych JH & Fincham FD (Eds.), Interparental conflict and child development: theory, research, and applications (pp. 213–245). Cambridge; New York, N.Y: Cambridge University Press. [Google Scholar]
- King V, & Heard HE (1999). Nonresident father visitation, parental conflict, and mother’s satisfaction: what’s best for child well-being? Journal of Marriage & Family, 61(2), 385–396. 10.2307/353756 [DOI] [Google Scholar]
- Kline M, Johnston JR, & Tschann JM (1991). The long shadow of marital conflict: A model of children’s postdivorce adjustment. Journal of Marriage and Family, 53(2), 297–309. 10.2307/352900 [DOI] [Google Scholar]
- Kovacs M (1985). The Children’s Depression, Inventory (CDI). Psychopharmacology Bulletin, 21(4), 995–998. [PubMed] [Google Scholar]
- Lazarus RS (1991). Emotion and adaptation Oxford University Press on Demand. [Google Scholar]
- Lazarus RS, & Folkman S (1984). Stress, appraisal, and coping Springer publishing company. [Google Scholar]
- Lazarus RS, & Folkman S (1987). Transactional theory and research on emotions and coping. European Journal of Personality, 1(3), 141–169. [Google Scholar]
- Lee SW, Piersel WC, Friedlander R, & Collamer W (1988). Concurrent validity of the Revised Children’s Manifest Anxiety Scale (RCMAS) for adolescents. Educational and Psychological Measurement, 48(2), 429–433. [Google Scholar]
- Lo Y, Mendell NR, & Rubin DB (2001). Testing the number of components in a normal mixture. Biometrika, 88(3), 767–778. [Google Scholar]
- Long N, Slater E, Forehand R, & Fauber R (1988). Continued high or reduced interparental conflict following divorce: Relation to young adolescent adjustment. Journal of Consulting and Clinical Psychology, 56(3), 467. [DOI] [PubMed] [Google Scholar]
- Mahrer N, O’Hara K, Sandler I, & Wolchik S (2018). Does shared parenting help or hurt children in high-conflict divorced families? Journal of Divorce & Remarriage, 1–24. 10.1080/10502556.2018.1454200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahrer N, Sandler I, Wolchik S, Winslow E, Moran J, & Weinstock D (2016). How do parenting time and interparental conflict affect the relations of quality of parenting and chid well-being following divorce? In Drozd L, Saini M, & Olesen N (Eds.), Parenting plan evaluations: Applied research for the family court (pp. 63–73). [Google Scholar]
- McLachlan G, & Peel D (2000). Finite Mixture Models Retrieved from https://www.wiley.com/en-us/Finite+Mixture+Models-p-9780471006268
- Meyer DR, Cancian M, & Cook ST (2017). The growth in shared custody in the United States: Patterns and implications. Family Court Review, 55(4), 500–512. [Google Scholar]
- Millsap RE, & Yun-Tein J (2004). Assessing factorial invariance in ordered-categorical measures. Multivariate Behavioral Research, 39(3), 479–515. [Google Scholar]
- Muthén LK, & Muthén BO (1998–2017). Mplus User’s Guide Eighth Edition. Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Nicolotti L, El-Sheikh M, & Whitson SM (2003). Children’s coping with marital conflict and their adjustment and physical health: Vulnerability and protective functions. Journal of Family Psychology, 17(3), 315–326. 10.1037/0893-3200.17.3.315 [DOI] [PubMed] [Google Scholar]
- Nielsen L (2017). Re-examining the research on parental conflict, coparenting, and custody arrangements. Psychology, Public Policy, and Law, 23(2), 211–231. 10.1037/law0000109 [DOI] [Google Scholar]
- O’Brien M, Bahadur MA, Gee C, Balto K, & Erber S (1997). Child exposure to marital conflict and child coping responses as predictors of child adjustment. Cognitive Therapy and Research, 21(1), 39–59. [Google Scholar]
- Pedro-Carroll J (2005). Fostering resilience in the aftermath of divorce: The role of evidence-based programs for children. Family Court Review [Google Scholar]
- Pedro-Carroll JL, & Cowen EL (1985). The Children of Divorce Intervention Program: An investigation of the efficacy of a school-based prevention program. Journal of Consulting and Clinical Psychology, 53(5), 603. [DOI] [PubMed] [Google Scholar]
- Pitts SC, West SG, & Tein J-Y (1996). Longitudinal measurement models in evaluation research: Examining stability and change. Evaluation and Program Planning, 19(4), 333–350. 10.1016/S0149-7189(96)00027-4 [DOI] [Google Scholar]
- Qu L, Weston R, Moloney L, Kaspiew R, & Dunstan J (2014). Post-separation parenting, property and relationship dynamics after five years Canberra: Attorney-General’s Department: Australian Institute of Family Studies. [Google Scholar]
- Radovanovic H (1993). Parental conflict and children’s coping styles in litigating separated families: Relationships with children’s adjustment. Journal of Abnormal Child Psychology, 21(6), 697–713. [DOI] [PubMed] [Google Scholar]
- Reynolds CR (1981). Long-term stability of scores on the Revised-Children’s Manifest Anxiety Scale. Perceptual and Motor Skills [DOI] [PubMed] [Google Scholar]
- Reynolds CR, & Paget KD (1981). Factor analysis of the revised Children’s Manifest Anxiety Scale for blacks, whites, males, and females with a national normative sample. Journal of Consulting and Clinical Psychology, 49(3), 352. [DOI] [PubMed] [Google Scholar]
- Reynolds CR, & Richmond BO (1978). What I think and feel: A revised measure of children’s manifest anxiety. Journal of Abnormal Child Psychology, 6(2), 271–280. 10.1007/BF00919131 [DOI] [PubMed] [Google Scholar]
- Rhoades KA (2008). Children’s responses to interparental conflict: A meta-analysis of their associations with child adjustment. Child Development, 79(6), 1942–1956. 10.1111/j.1467-8624.2008.01235.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rowen J, & Emery R (2018). Parental denigration: A form of conflict that typically backfires. Family Court Review, 56(2), 258–268. 10.1111/fcre.12339 [DOI] [Google Scholar]
- Sacks V, Murphy D, & Moore K (2014). Adverse childhood experiences: National and state-level prevalence Retrieved from http://www.childtrends.org/wp-content/uploads/2014/07/Brief-adverse-childhood-experiences_FINAL.pdf
- Sandler IN (2001). Quality and ecology of adversity as common mechanisms of risk and resilience. American Journal of Community Psychology, 29(1), 19–61. [DOI] [PubMed] [Google Scholar]
- Sandler IN, Tein J-Y, Mehta P, Wolchik S, & Ayers T (2000). Coping efficacy and psychological problems of children of divorce. Child Development, 71(4), 1099–1118. [DOI] [PubMed] [Google Scholar]
- Sandler IN, Tein J-Y, & West SG (1994). Coping, stress, and the psychological symptoms of children of divorce: A cross-sectional and longitudinal study. Child Development, 65(6), 1744–1763. 10.1111/j.1467-8624.1994.tb00846.x [DOI] [PubMed] [Google Scholar]
- Saylor CF, Finch AJ, Spirito A, & Bennett B (1984). The Children’s Depression Inventory: A systematic evaluation of psychometric properties. Journal of Consulting and Clinical Psychology, 52(6), 955. [DOI] [PubMed] [Google Scholar]
- Sbarra DA, & Emery RE (2005). Coparenting conflict, nonacceptance, and depression among divorced adults: Results from a 12-year follow-up study of child custody mediation using multiple imputation. The American Journal of Orthopsychiatry, 75(1), 63–75. 10.1037/0002-9432.75.1.63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwarz G (1978). Estimating the dimension of a model. The Annals of Statistics, 6(2), 461–464. [Google Scholar]
- Sclove SL (1987). Application of model-selection criteria to some problems in multivariate analysis. Psychometrika, 52(3), 333–343. [Google Scholar]
- Shaffer D, Fisher P, Lucas CP, Dulcan MK, & Schwab-Stone ME (2000). NIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnoses. Journal of the American Academy of Child & Adolescent Psychiatry, 39(1), 28–38. [DOI] [PubMed] [Google Scholar]
- Shaw DS, & Emery RE (1987). Parental conflict and other correlates of the adjustment of school-age children whose parents have separated. Journal of Abnormal Child Psychology, 15(2), 269–281. 10.1007/BF00916354 [DOI] [PubMed] [Google Scholar]
- Sheets V, Sandler I, & West S (1996). Appraisals of negative events by preadolescent children of divorce. Child Development, 67(5), 2166–2182. [PubMed] [Google Scholar]
- Shelton KH, & Harold GT (2007). Marital conflict and children’s adjustment: The mediating and moderating role of children’s coping strategies. Social Development, 16(3), 497–512. 10.1111/j.1467-9507.2007.00400.x [DOI] [Google Scholar]
- Shelton KH, & Harold GT (2008). Pathways between interparental conflict and adolescent psychological adjustment: Bridging links Through children’s cognitive appraisals and coping strategies. Journal of Early Adolescence, 28(4), 555–582. 10.1177/0272431608317610 [DOI] [Google Scholar]
- Skinner E, & Wellborn J (1994). Coping during childhood and adolescence: A motivational perspective. In Featherman DL, Lerner RM, & Perlmutter M (Eds.), Life-span development and behavior (pp. 91–133). Hillsdale, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Smyth BM, & Moloney LJ (2017). Entrenched postseparation parenting disputes: The role of interparental hatred? Family Court Review, 55(3), 404–416. [Google Scholar]
- Smyth BM, & Moloney LJ (2019). Post-separation parenting disputes and the many faces of high conflict: Theory and research. Australian and New Zealand Journal of Family Therapy, 0(0). 10.1002/anzf.1346 [DOI] [Google Scholar]
- Tein J-Y, Coxe S, & Cham H (2013). Statistical power to detect the correct number of classes in latent profile analysis. Structural Equation Modeling: A Multidisciplinary Journal, 20(4), 640–657. 10.1080/10705511.2013.824781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Timbremont B, Braet C, & Dreessen L (2004). Assessing depression in youth: relation between the Children’s Depression Inventory and a structured interview. Journal of Clinical Child and Adolescent Psychology, 33(1), 149–157. [DOI] [PubMed] [Google Scholar]
- Tu KM, Erath SA, & El-Sheikh M (2016). Coping responses moderate prospective associations between marital conflict and youth adjustment. Journal of Family Psychology, 30(5), 523–532. 10.1037/fam0000169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- US Census Bureau. (2018). America’s Families and Living Arrangements: 2018 Retrieved December 17, 2018, from https://www.census.gov/data/tables/2018/demo/families/cps-2018.html
- Vandewater EA, & Lansford JE (1998). Influences of family structure and parental conflict on children’s well-Being. Family Relations, 47(4), 323–330. [Google Scholar]
- Wadsworth ME (2015). Development of maladaptive coping: A functional adaptation to chronic, uncontrollable stress. Child Development Perspectives, 9(2), 96–100. 10.1111/cdep.12112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolchik SA, Sandler IN, Millsap RE, Plummer BA, Greene SM, Anderson ER, … Haine RA (2002). Six-Year follow-up of preventive interventions for children of divorce: A randomized controlled trial. JAMA, 288(15), 1874–1881. [DOI] [PubMed] [Google Scholar]
- Wolchik SA, West SG, Sandler IN, Tein J-Y, Coatsworth D, Lengua L, … Griffin WA (2000). An experimental evaluation of theory-based mother and mother-child programs for children of divorce. Journal of Consulting and Clinical Psychology, 68(5), 843–856. 10.1037//0022-006X.68.5.843 [DOI] [PubMed] [Google Scholar]
- Wolchik S, Sandler I, Weiss L, & Winslow E (2007). New Beginnings: An empirically-based intervention program for divorced mothers to help children adjust to divorce. In Briesmeister JM & Schaefer CE (Eds.), Handbook of parent training: Helping parents prevent and solve problem behaviors (pp. 25–66). Hoboken, N.J: Wiley. [Google Scholar]