

Abstract
Background
Common types of musculoskeletal conditions include pain in the neck and shoulder areas. This study seeks to identify the genetic variants associated with neck or shoulder pain based on a genome-wide association approach using 203 309 subjects from the UK Biobank cohort and look for replication evidence from the Generation Scotland: Scottish Family Health Study (GS:SFHS) and TwinsUK.
Methods
A genome-wide association study was performed adjusting for age, sex, BMI and nine population principal components. Significant and independent genetic variants were then sent to GS:SFHS and TwinsUK for replication.
Results
We identified three genetic loci that were associated with neck or shoulder pain in the UK Biobank samples. The most significant locus was in an intergenic region in chromosome 17, rs12453010, having P = 1.66 × 10−11. The second most significant locus was located in the FOXP2 gene in chromosome 7 with P = 2.38 × 10−10 for rs34291892. The third locus was located in the LINC01572 gene in chromosome 16 with P = 4.50 × 10−8 for rs62053992. In the replication stage, among four significant and independent genetic variants, rs2049604 in the FOXP2 gene and rs62053992 in the LINC01572 gene were weakly replicated in GS:SFHS (P = 0.0240 and P = 0.0202, respectively).
Conclusions
We have identified three loci associated with neck or shoulder pain in the UK Biobank cohort, two of which were weakly supported in a replication cohort. Further evidence is needed to confirm their roles in neck or shoulder pain.
Introduction
Musculoskeletal pain in the neck and shoulder areas is a major health problem for adults of working age as well as for elderly populations (1). Neck and shoulder pain are prevalent forms of self-reported musculoskeletal pain (2). The etiologies of neck and shoulder pain may be complicated since both regional lesions and systemic disorders outside the cervicobrachial area may cause pain at that location (3,4). In addition, lesions in the neck can lead to pain in the shoulder and vice versa (5). Many people also have difficulty in describing and differentiating pain in these areas accurately. For these reasons, neck or shoulder pain is often discussed as a single entity (6).
Epidemiological studies have suggested that the prevalence of neck pain is 5–8% and 13% for shoulder pain (7–9). The Global Burden of Disease Study 2010 found that of the 291 conditions studied, neck or shoulder pain as a single entity ranked 21st in overall burden on society, and 4th in terms of overall disability (8). The updated Global Burden of Disease Study 2016 also indicated that neck pain was a top five cause of years lived with disability (YLD) in high-income and high-middle-income countries (10). Risk factors associated with neck or shoulder pain conform to the biopsychosocial model; specifically, they include older age, being female, high body mass index (BMI), previous injury, strenuous occupation and diabetes mellitus (3,11–14). Although mechanical exposure is associated with increased risk of pain in the neck and shoulder, this explains only part of these complaints (15). Because of the biopsychosocial factors involved, treating neck or shoulder pain successfully is a challenge. In a study of neck, shoulder and arm pain, only 25% of the patients made a complete recovery after 6 months (16). This is lower than the 35% recovery rate of patients with low back pain after 12 months (17). Estimated rates of remission 1 year after neck or shoulder pain onset were between 33 and 55% (18–21).
Genetic studies have identified genes associated with neck or shoulder pain. Twin studies have shown that there is a genetic role in neck pain (14), though in keeping with many traits the genetic component becomes smaller with age (22,23). Nonetheless, in adolescents as much as 68% of variance in neck pain liability could be attributed to genetic factors (24). So far, there has been no genome-wide association study (GWAS) published on neck or shoulder pain.
This study seeks to identify the genetic variants associated with neck or shoulder pain based on a GWAS approach in a cohort of 203 309 subjects from the UK Biobank cohort and to test significant results for replication in the Generation Scotland: Scottish Family Health Study (GS:SFHS) and TwinsUK. Similar approaches have been used to examine back pain, knee pain and headaches in the UK Biobank cohort (25–27).
Results
GWAS results
In the UK Biobank, 775 252 responses to all options were received for the specific pain question. Of the 501 708 participants in the study, 123 061 participants reported having experienced activity limiting pain in the neck or shoulder in the previous month. 213 408 participants chose the ‘None of the above’ option which meant that they did not have activity limiting pain anywhere in the previous month. To create a homogeneous dataset, we first removed samples according to their ancestry information. In addition, those who were related to one or more others in the cohort (a cut-off value of 0.044 in the generation of the genetic relationship matrix) and those who failed quality control were also removed. The final number of those included in the case group after the above exclusions was 53 994 (28 093 males, 25 901 females). 149 312 (71 480 males, 77 832 females) individuals were included in the control group. After single-nucleotide polymorphism (SNP) quality control, there were 9 304 965 SNPs available for GWAS analysis. Clinical characteristics of the case and control groups were compiled (Table 1). Age, sex and BMI were all found to be significantly different (P < 0.001) between cases and controls. Three genetic loci including four significant and independent SNPs reached a GWAS significance of P < 5 × 10−8 (Fig. 1, Table 2). The most significant locus was located in an intergenic region in chromosome 17. The SNP from this location of highest significance was rs12453010 (P = 1.66 × 10−10). The second locus was found in the FOXP2 gene located in chromosome 7, and the most significant SNP from this locus was rs34291892 (P = 2.38 × 10−10). The third locus was the LINC01572 gene located in chromosome 16, and the most significant SNP in this locus was rs62053992 (P = 4.50 × 10−10). The SNP heritability (liability scale) from genome-wide complex trait analysis (GCTA) was 0.11 ± 0.017.
Table 1.
Clinical characteristics of neck or shoulder pain cases and controls in the UK Biobank
| UK Biobank | |||
|---|---|---|---|
| Covariates | Cases | Controls | P |
| Sex (male:female) | 28 093 (52.0%): 25901 (48.0%) | 71 480 (47.9%): 77832 (52.1%) | <0.001 |
| Age (years) | 57.7 (7.82) | 56.9 (7.97) | <0.001 |
| BMI (kg/m2) | 27.8 (4.85) | 26.7 (4.30) | <0.001 |
BMI: body mass index
A chi-square test was used to test the difference of gender frequency between cases and controls, and an independent t test was used for other covariates.
Continuous covariates were presented as mean (standard deviation).
Figure 1.
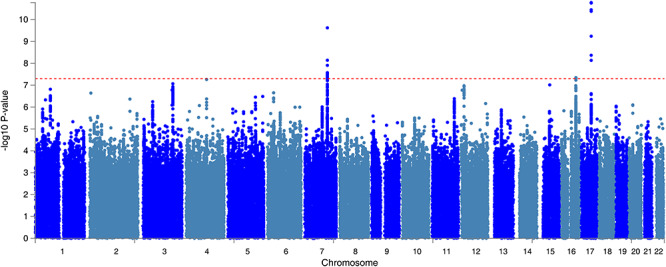
The Manhattan plot of the GWAS on neck or shoulder pain using the UK Biobank cohort (N = 203 309). The dashed red line indicates the cut-off P value of 5 × 10−8.
Table 2.
The summary statistics of the four significant and independent SNPs in the UK Biobank and the replication and meta-analysis results using the GS:SFHS and TwinsUK cohorts
| UK Biobank discovery stage | GS:SFHS replication | TwinsUK replication | Meta-analysis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SNP | Chr | Position | MAF | P | beta | se | P | beta | se | P | beta | se | P | effects | I2 |
| rs2049604 | 7 | 113 990 352 | 0.3648 (T) | 3.26 × 10−8 | −0.0080 | 0.0015 | 0.0240 | −0.0088 | 0.0039 | 0.13 | −0.0188 | 0.0122 | 3.19 × 10−9 | − | 0 |
| rs34291892 | 7 | 114 058 731 | 0.3772 (C) | 2.38 × 10−10 | −0.0092 | 0.0014 | 0.1068 | −0.0064 | 0.0039 | 0.11 | −0.0196 | 0.0124 | 7.07 × 10−12 | − | 0 |
| rs62053992 | 16 | 72 389 872 | 0.1819 (G) | 4.50 × 10−8 | −0.0098 | 0.0018 | 0.0202 | −0.0109 | 0.0047 | 0.94 | 0.0012 | 0.0158 | 4.36 × 10−9 | − − + | 0 |
| rs12453010 | 17 | 50 316 131 | 0.3926 (T) | 1.66 × 10−11 | 0.0095 | 0.0014 | 0.1331 | 0.0058 | 0.0038 | 0.10 | 0.0199 | 0.0121 | 2.20 × 10−12 | +++ | 0 |
rs34291892 was replaced by rs4727799 (r2 = 0.8736) as it does not exist in the GS:SFHS and TwinsUK cohorts.
UK Biobank N = 203 309; GS:SFHS N = 19 632; TwinsUK N = 3982
Chr: chromosome
MAF: minor allele frequency
Significant P values in the replication (P < 0.05) were in bold
These four significant and independent SNPs were tested for replication in GS:SFHS and TwinsUK. Among 20 032 subjects in the GS:SFHS subjects, 19 598 had complete relevant information. The whole-genome fastGWA results did not find any SNPs with GWAS significance associated with neck or shoulder pain. (Supplementary Material, Fig. S1). Among the four SNPs from the discovery cohort, rs2049604 in the forkhead box protein P2 (FOXP2) gene and rs62053992 in the Long Intergenic Non-Protein Coding RNA 1572 (LINC01572) gene were replicated weakly (P = 0.0240 and 0.0202, respectively) (Table 2). Of the 6921 individuals in TwinsUK with genetic information, 3982 of them had valid relevant information on phenotypes and covariates. None of the 4 SNPs were replicated in the TwinsUK cohort (P > 0.05). The clinical characteristics of the GS:SFHS and TwinsUK cohorts are summarized in Supplementary Material, Table S1.
Meta-analysis of the four significant and independent hits, combining UK Biobank, GS:SFHS and Twins UK found that the significance of their associations was increased (Table 2).
FUMA analysis
In gene-based association analysis by MAGMA, 26 genes were found to be associated with neck or shoulder pain, all of which are represented in Supplementary Material, Table S2. The most significant gene was FOXP2 (P = 1.62 × 10−11), which is located in chromosome 7.
In gene-set analysis conducted by MAGMA, 10651 gene-sets were analyzed using the default competitive test model. None of these gene-sets met genome-wide significance (P < 4.7 × 10−6 (0.05/10651)).
Tissue expression analysis was conducted by GTEx, and the relationship between tissue specific gene expression and genetic associations was tested by using the average gene expression in each tissue type as a covariate. Two analyses were carried out, one investigating 30 general tissue types (Fig. 2) and the other looking at 53 specific tissue types (Fig. 3). Tissue expression analysis in 30 tissue types found expression in brain tissue to be the most significant (P = 9.53 × 10−5). Only expression in brain and pituitary tissue reached significant values of P < 1.67 × 10−3 (0.05/30). Tissue expression analysis of 53 specific tissue types by GTEx found expression in the nucleus accumbens of the basal ganglia to be the most significant (P = 3.55 × 10−5). In addition, the top 6 significant associations were all from brain tissues.
Figure 2.
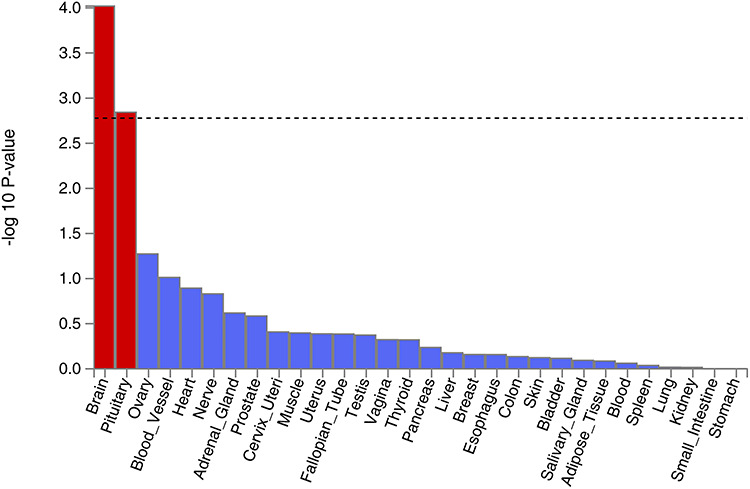
Tissue expression results on 30 specific tissue types by GTEx in the FUMA. The dashed line shows the cut-off P value for significance with Bonferroni adjustment for multiple hypothesis testing.
Figure 3.
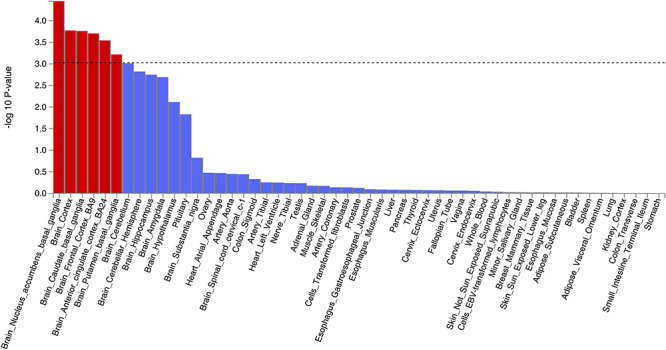
Tissue expression results on 53 specific tissue types by GTEx in the FUMA. The dashed line shows the cut-off P value for significance with Bonferroni adjustment for multiple hypothesis testing.
The genetic correlation analysis using the LD hub (v1.9.0) showed that symptoms of depression had the largest significant and positive genetic correlation with neck or shoulder pain (rg = 0.5522, P = 3.41 × 10−30), followed by insomnia (rg = 0.5377, P = 1.21 × 10−21). It was also found that the age at which they have their first child had the most significant and negative genetic correlations with neck or shoulder pain (rg = −0.4812, P = 8.95 × 10−37), followed by college completion (rg = −0.4706, P = 7.26 × 10−26). All the phenotypes with significant genetic correlation with neck or shoulder pain are shown in Table 3.
Table 3.
The significant genetic correlation results by the LD hub between neck or shoulder pain with other phenotypes
| Trait 1 | Trait 2 | rg | P |
|---|---|---|---|
| Neck or shoulder pain | Depressive symptoms | 0.5522 | 3.41 × 10−30 |
| Neck or shoulder pain | Insomnia | 0.5377 | 1.21 × 10−21 |
| Neck or shoulder pain | Neuroticism | 0.4417 | 2.00 × 10−29 |
| Neck or shoulder pain | Major depressive disorder | 0.3968 | 5.75 × 10−08 |
| Neck or shoulder pain | Ever versus never smoked | 0.3082 | 4.14 × 10−08 |
| Neck or shoulder pain | Number of children ever born | 0.2616 | 2.03 × 10−07 |
| Neck or shoulder pain | Coronary artery disease | 0.1965 | 1.66 × 10−07 |
| Neck or shoulder pain | Waist-to-hip ratio | 0.1547 | 1.31 × 10−05 |
| Neck or shoulder pain | Sleep duration | -0.2468 | 9.46 × 10−07 |
| Neck or shoulder pain | Subjective well being | -0.2626 | 1.14 × 10−06 |
| Neck or shoulder pain | Intelligence | -0.3229 | 2.23 × 10−17 |
| Neck or shoulder pain | Former versus Current smoker | -0.3600 | 5.87 × 10−06 |
| Neck or shoulder pain | Years of schooling 2016 | -0.4373 | 5.18 × 10−54 |
| Neck or shoulder pain | College completion | -0.4706 | 7.26 × 10−26 |
| Neck or shoulder pain | Age of first birth | -0.4812 | 8.95 × 10−37 |
rg: genetic correlation
The cut-off P value is 0.0002 (0.05/234).
Discussion
We have performed a GWAS on neck or shoulder pain using the UK Biobank resource and found three loci that have reached genome-wide significance (P < 0.05 × 10−8). They are the FOXP2 gene in chromosome 7, the LINC01582 gene in chromosome 16 and an intergenic area in chromosome 17. In the replication stage, the FOXP2 and LINC01582 loci were weakly supported by the GS:SFHS cohort but not by TwinsUK.
FOXP2 belongs to the forkhead-box transcription factor family and encodes a 715 amino acid long transcription factor (28). It may have 300–400 transcription targets, and has a forkhead/winged helix binding domain with two polyglutamine tracts adjacent to each other due to a mixture of CAG and CAA repeats (29,30). Both rs2049604 and rs34291892 are intronic variants, and rs34291892 is an Indel type variant. We searched these two SNPs in the GTEx portal, but did not obtain any information on their impact on gene expression or gene function. FOXP2 is a gene shown to be vital in the neural mechanisms underpinning the development of speech and language. A previous study described a family with developmental verbal dyspraxia, where affected individuals had a loss of function mutation in the FOXP2 gene (31). Affected individuals in the family had difficulty with the selection and sequencing of fine orofacial muscular movements needed to articulate words, as well as deficits in language and grammatical skills. FOXP2 also plays a role in regulating ‘hub’ genes Dlx5 and Syt4 in animal models, which are important for brain development and function (32–34). The mutations in the FOXP2 gene were also associated with decreased gray matter in the cerebellum (35).
Notably, FOXP2 is expressed in several regions of the brain, namely the basal ganglia, locus coeruleus, parabrachial nucleus, and thalamus. All of these regions have been previously implicated in the modulation of pain (36–39), and also concur with the tissue expression analysis (Figs 2 and 3) which suggests that the central nervous system modulates neck or shoulder pain. A recent GWAS study suggested that FOXP2 was significantly associated with multisite chronic pain (40). Further studies into the location and function of the transcription targets of FOXP2 would also provide valuable insight.
The LINC01572 gene in chromosome 16 was also replicated in this study, with rs62053992 having the P value at 4.5 × 10−8 in the discovery cohort and at 0.02 in the GS:SFHS. The gene is 384 kb long, and was recently suggested to be related with polycystic ovary syndrome (41). However, studies of this gene have been very limited. Further replication evidence should be sought to confirm its role in neck or shoulder pain. Although the locus in chromosome 17 was not replicated, it was the most significantly associated in the discovery cohort with rs12453010 having the lowest P value of 1.66 × 10−11. The meta-analysis also showed that the effects of the SNP from the GS:SFHS and TwinsUK cohorts were in the same direction as UK Biobank. Analysis of this locus is also difficult as it is a gene desert. The nearest non-protein-coding gene is LOC105371829, and is unlikely to be linked with neck or shoulder pain as its expression was observed only in testis and liver (https://www.ncbi.nlm.nih.gov/gene/105371829#gene-expression). The nearest protein coding gene is CA10, which encodes a protein belonging to the carbonic anhydrase family and is responsible for catalyzing the hydration of carbon dioxide. It is also thought to contribute to central nervous system development particularly in the brain (43).
The results of the meta-analysis of the 4 significant and independent SNPs combining 3 cohorts suggested that the loci identified by the UK Biobank cohort were supported by the GS:SFHS and TwinsUK. It is likely that the sample size in the TwinsUK (N = 3982) was too small to replicate the loci for such a heterogeneous phenotype as neck or shoulder pain. In particular, for the 4 SNPs chosen for replication, the power to achieve a P value < 0.05 in the given TwinsUK sample ranged between 11.6 and 15.8% (44).
The SNP heritability of neck or shoulder pain was 0.11. This is similar to that of back pain (0.11), greater than knee pain (0.08), multisite chronic pain (0.10), and less than hip pain (0.12), stomach or abdominal pain (0.14), headache (0.21), facial pain (0.24), and pain all over the body (0.31) (40,45). Further, the genetic correlation matrix among 8 pain phenotypes in UK Biobank showed that the neck or shoulder pain and back pain shared the highest genetic correlation (rg = 0.83) (45). The heritability of neck or shoulder pain in this study was significantly less than that reported in the teenage Finnish twin study (24). Such a difference between twin-based heritability and SNP-based heritability is common and usually attributable to (1) the effects of rare and other forms of variants not imputed/not taken into account in GWAS; and (2) the fact that twin studies may overestimate heritability due to gene-gene and gene-environment interactions. Also, heritability of neck pain is known to be age-dependent, with genetic effects decreasing with age (22). Age differences between the Finnish teenagers and our cohorts likely contributed to the difference in heritability estimates.
The genetic correlation analysis results were perhaps to be expected. Like knee pain and back pain, which have been shown to be positively correlated with depression and neuroticism (45), neck or shoulder pain was correlated genetically and positively with some mental health and personality phenotypes. We also identified that neck or shoulder pain was genetically and negatively correlated with the age at which they have their first child, college completion, and years of schooling. This means that those who were older when they had their first child, those with more years of schooling, and those with completed college education were less likely to report neck or shoulder pain. These factors could be related to a number of factors including lifestyle, deprivation levels, and occupation. It is interesting to note that males are more likely to report neck or shoulder pain than females in the UK Biobank population. This is matched with the fact that males are more likely to have strenuous occupations. However, we should note that female sex is a risk factor for neck or shoulder pain. It is also noted that the cases were older and had higher BMI than the controls in the UK Biobank.
The primary limitation of this study is that different (albeit similar) case and control definitions were used in the discovery and replication cohorts. This was a consequence of the pre-determined phenotypic information that was present in the relevant cohorts. We defined neck or shoulder pain cases and controls based on the responses by UK Biobank participants to a specific pain question. This question focused on neck or shoulder pain occurrence during the previous month that was sufficient to cause interference with activity. The severity, frequency, and exact location of the neck or shoulder pain were not documented. Hence, our phenotyping should be considered as broadly defined. In the GS:SFHS and Twins UK cohorts, the disease status of participants was also self-reported: while cases were those who reported neck or shoulder pain over the previous 3 months; controls included those who reported neck or shoulder pain for less than 3 months, or pain of any duration in other body sites, as well as those reporting no pain. However, in the UK Biobank, controls were defined as pain free for the previous month. Differences between (albeit similar) case and control definitions could have a negative impact on the power of the replication study and the replication results while this impact is hard to evaluate. There could also be some cases who report neck or shoulder pain as a result of underlying causes such as cancer and osteoarthritis in the neck and shoulder areas. Their impact on the results would be very limited due to the small numbers. In addition, as the cases and controls in the UK Biobank were self-reported, there could be some bias, for example from social desirability, recall period, sampling approach, or selective recall (46). Further, although GTEx covered much expression information on different brain tissues, it does not report relevant expression information on musculoskeletal tissue or dorsal root ganglia which would also be of interest.
In summary, we have identified 3 loci of genome-wide significance (P < 5 × 10−8) associated with neck or shoulder pain in the UK Biobank dataset using a GWAS approach. Two of these loci were replicated weakly in the GS:SFHS cohort. Identification of these loci now provides a foundation for future work into understanding genetic roles and etiology in neck or shoulder pain.
Materials and Methods
Participants and the genetic information of cohorts
Discovery cohort—The UK Biobank (https://www.ukbiobank.ac.uk/) is a project facilitating research into health and disease and involves over 500 000 participants aged between 40 and 69 years old at recruitment. Participants completed a detailed questionnaire which examined lifestyle, demographic factors and clinical history. Participants also underwent clinical measures and baseline body measurements such as height and weight. Biological samples including urine, saliva, and blood were also provided. The National Research Ethics Service granted ethical approval to the UK Biobank (reference 11/NW/0382). The genetic information of 500 000 participants was released to approved researchers in March 2018. The corresponding author of this paper was granted access to the genetic information under UK Biobank application number 4844. Detailed quality control information pertaining to these genotypes was described by Bycroft et al (47).
Replication cohort 1—Generation Scotland: Scottish Family Health Study (GS:SFHS) is a multi-institutional, family-based cohort involving over 20 000 volunteer participants aged between 18–98 years old at recruitment, who provided blood samples from which DNA was extracted. Similarly, participants also completed questionnaires to provide detailed phenotypic and sociodemographic information. Clinical and biochemical measurements were also collected for the purpose of research. Permission was obtained for linkage of research data to routine health data in the form of electronic health records (48,49). Ethical approval for GS:SFHS was obtained from the Tayside Committee on Medical Research Ethics (on behalf of the National Health Service) with reference Number 05/S1401/89. The genetic information relating 20 000 participants was released to the corresponding author of this paper in March 2018 for pain-related research. Detailed quality control information pertaining to these genotypes was described by Hall et al (50).
Replication cohort 2—The TwinsUK cohort is a UK nationwide registry of volunteer same sex twins. It has recruited 14 274 registered twins aged between 16 and 98 years. Collection of data and biological materials commenced in 1992 and is ongoing. During study participation, participants regularly complete health and lifestyle questionnaires and visit collaborating clinics and hospitals for clinical evaluation. Ethical approval was provided by the Research Ethics Committee at Guy’s and St. Thomas’ NHS Foundation Trust. TwinsUK has the genetic information relating to 6921 participants. Detailed quality control information pertaining to the genetic information was described by Moayyeri et al (51).
Phenotypic definitions on neck or shoulder pain
Discovery cohort—UK Biobank: Participants were offered a pain-related questionnaire, which included the question: ‘in the last month have you experienced any of the following that interfered with your usual activities?’. The options were: 1. Headache; 2. Facial pain; 3. Neck or shoulder pain; 4. Back pain; 5. Stomach or abdominal pain; 6. Hip pain; 7. Knee pain; 8. Pain all over the body; 9. None of the above; 10. Prefer not to say. Participants could select more than one option. (UK Biobank Questionnaire field ID: 6159).
In this study, cases were defined as participants who reported having activity limiting pain in the neck or shoulder in the past month (option 3), regardless of whether they reported pain in other regions. The controls were defined as participants who chose the ‘None of the above’ option.
Replication cohort 1—GS:SFHS: Participants were first asked ‘Are you currently troubled by pain or discomfort, either all the time or on and off?’. If yes was selected, then the participants were asked ‘Have you had this pain or discomfort for more than 3 months?’. If yes was selected once again, then they were asked ‘Where is this pain or discomfort?’ with options of ‘Back pain’, ‘Neck or shoulder pain’, ‘Headache, facial or dental pain’, ‘Stomach ache or abdominal pain’, ‘Pain in your arms, hands, hips, legs or feet’, ‘Chest pain’, and ‘Other pain’. If a participant selected the ‘Neck or shoulder pain’, then he/she was defined as a case. All other subjects were defined as controls.
Replication cohort 2: TwinsUK: participants were asked ‘In the past three months, have you had pain in your neck or shoulders?’ Those who answered ‘Yes’ were defined as cases. Those who answered ‘No’ were defined as controls. Those with missing answers were not included in the study.
Statistical analysis
Discovery cohort—UK Biobank: BGENIE (https://jmarchini.org/bgenie/) was used as the main GWAS software. SNPs with imputation INFO scores < 0.1, minor allele frequency (MAF) < 0.5% were removed, as well as SNPs that failed Hardy-Weinberg tests P < 1.0 × 10−6.
BGENIE was used to perform association studies using linear association tests, adjusting for age, sex, BMI, 9 population principle components, genotyping arrays, and assessment centers. Chi-square testing was used to compare gender difference between cases and controls. T-tests were used to compare age and BMI between case and control groups using IBM SPSS 22 (IBM Corporation, New York). As is standard in GWAS, SNP associations were considered significant when P < 5.0 × 10−8. GCTA software was used to calculate SNP-based or narrow-sense heritability (52). Only significant and independent SNPs from the discovery GWAS were sent to replication cohorts for replication. These significant and independent SNPs were defined by FUMA with r2 (linkage disequilibrium score) <0.6 with any other significant SNPs.
Replication cohort 1—GS:SFHS: GCTA fastGWA1.92.4 was the main software used for replication (https://cnsgenomics.com/software/gcta/#fastGWA). SNPs with INFO scores < 0.3, or MAF <1% were removed, as well as SNPs that failed Hardy-Weinberg tests P < 1.0 × 10−6. FastGWA was used to perform association studies using a mixed-effects linear model adjusting for age, sex, BMI and nine population principal components. Relatedness was adjusted for via a genetic kinship matrix.
Replication cohort 2—TwinsUK: GEMMA v 0.98.1 was used for replication (https://github.com/genetics-statistics/GEMMA). A mixed-effects linear model adjusting for age, sex, BMI and relatedness via a genetic kinship matrix was used.
Meta-analysis of the significant and independent SNPs combining the UK Biobank, GS:SFHS and TwinsUK was performed using GWAMA 2.2.2 (https://genomics.ut.ee/en/tools/gwama).
Post-GWAS analysis: this study used FUMA as a main annotation tool for viewing and annotating GWAS results (53). It applied SNP functional annotations and generated a corresponding GWAS Manhattan plot.
MAGMA v1.06 (integrated in FUMA) was used to perform gene-based association analysis and gene-set analysis, both of which were generated from GWAS summary statistics (54). For gene-based association analysis, all SNPs located in protein coding genes are mapped to one of 19 123 protein coding genes. The default SNP-wise model (mean) was applied. We tested the joint association of all SNPs in the gene with the phenotype by aggregating the SNP summary statistics to the level of whole genes. In gene-set analysis, individual genes were aggregated to groups of genes sharing certain biological, functional or other characteristics. This aims to elucidate the involvement of specific biological pathways or cellular functions in the genetic etiology of a phenotype. GTEx (also integrated in FUMA, https://www.gtexportal.org/home/) provided the results of tissue expression analysis.
Genetic correlation analysis was also performed to identify genetic correlation between neck or shoulder pain and 234 complex traits based on the online tool LD hub v1.9.0 (http://ldsc.broadinstitute.org/ldhub/). Any P value less than 2.1 × 10−4 (0.05/234) was considered statistically significant by Bonferroni adjusted testing.
Supplementary Material
Acknowledgements
The authors would like to thank all participants of the UK Biobank, Generation Scotland and TwinsUK cohorts who have provided necessary genetic and phenotypic information. This research has been conducted using the UK Biobank Resource under Application Number 4844. Generation Scotland is grateful to all the families who took part, the general practitioners and the Scottish School of Primary Care for their help in recruiting them, and the whole Generation Scotland team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists, healthcare assistants, and nurses.
Conflict of Interest. The authors declare that they have no conflict of interest.
The first 2 authors should be regarded as joint first authors.
Funding Sources
This study was mainly funded by the Wellcome Trust Strategic Award ‘Stratifying Resilience and Depression Longitudinally’ (STRADL) with reference number 104036/Z/14/Z and by the GCRF academic exchange visits to China funded by the University of Dundee. Generation Scotland: Scottish Family Health Studies (GS:SFHS) received core support from the Chief Scientist Office of the Scottish Government Health Directorates (CZD/16/6) and the Scottish Funding Council (HR03006). TwinsUK is funded by the Wellcome Trust, Medical Research Council, European Union, Chronic Disease Research Foundation (CDRF), Zoe Global Ltd, the National Institute for Health Research (NIHR)-funded BioResource, Clinical Research Facility and Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust in partnership with King’s College London.
Data Availability
The GWAS summary statistics of neck or shoulder pain can be accessed through https://figshare.com/articles/fourpainphenotype2/7699583
Author Contributions
WM organized the project, drafted the paper and contributed to the analysis. BWC and CH contributed to drafting the paper. MBF provided the TwinsUK replication. MA performed the main UK Biobank GWAS analysis. AC and CH contributed to GS:SFHS cohorts. HLH, HZ, XZ, CNAP, LC, TGH and FMKW provided essential comments. AM and BS organized the project and provided comments.
References
- 1. Vogt M.T., Simonsick E.M., Harris T.B., Nevitt M.C., Kang J.D., Rubin S.M., Kritchevsky S.B., Newman A.B., Health A. and B. C. S. (2003) Neck and shoulder pain in 70- to 79-year-old men and women: findings from the health, aging and body composition study. Spine J., 3, 435–441. [DOI] [PubMed] [Google Scholar]
- 2. Picavet H.S.J. and Schouten J.S.A.G. (2003) Musculoskeletal pain in the Netherlands: prevalences, consequences and risk groups, the DMC(3)-study. Pain, 102, 167–178. [DOI] [PubMed] [Google Scholar]
- 3. Slater M., Perruccio A.V. and Badley E.M. (2011) Musculoskeletal comorbidities in cardiovascular disease, diabetes and respiratory disease: the impact on activity limitations; a representative population-based study. BMC Public Health, 11, 77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Molsted S., Tribler J. and Snorgaard O. (2012) Musculoskeletal pain in patients with type 2 diabetes. Diabetes Res. Clin. Pract., 96, 135–140. [DOI] [PubMed] [Google Scholar]
- 5. Fernández-de-Las-Peñas C., Galán-Del-Río F., Alonso-Blanco C., Jiménez-García R., Arendt-Nielsen L. and Svensson P. (2010) Referred pain from muscle trigger points in the masticatory and neck-shoulder musculature in women with temporomandibular disoders. J. Pain, 11, 1295–1304. [DOI] [PubMed] [Google Scholar]
- 6. Rossi M., Pasanen K., Kokko S., Alanko L., Heinonen O.J., Korpelainen R., Savonen K., Selänne H., Vasankari T., Kannas L. et al. (2016) Low back and neck and shoulder pain in members and non-members of adolescents’ sports clubs: the Finnish Health promoting sports Club (FHPSC) study. BMC Musculoskelet. Disord., 17, 263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Wright A.R., Shi X.A., Busby-Whitehead J., Jordan J.M. and Nelson A.E. (2009) The prevalence of neck and shoulder symptoms and associations with comorbidities and disability: the Johnston County osteoarthritis project. Myopain, 23, 34–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Hoy D., March L., Woolf A., Blyth F., Brooks P., Smith E., Vos T., Barendregt J., Blore J., Murray C. et al. (2014) The global burden of neck pain: estimates from the global burden of disease 2010 study. Ann. Rheum. Dis., 73, 1309–1315. [DOI] [PubMed] [Google Scholar]
- 9. March L., Smith E.U.R., Hoy D.G., Cross M.J., Sanchez-Riera L., Blyth F., Buchbinder R., Vos T. and Woolf A.D. (2014) Burden of disability due to musculoskeletal (MSK) disorders. Best Pract. Res. Clin. Rheumatol., 28, 353–366. [DOI] [PubMed] [Google Scholar]
- 10. GBD 2016 Disease and Injury Incidence and Prevalence Collaborators (2017) Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet (London, England), 390, 1211–1259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Nilsen T.I.L., Holtermann A. and Mork P.J. (2011) Physical exercise, body mass index, and risk of chronic pain in the low back and neck/shoulders: longitudinal data from the Nord-Trondelag Health study. Am. J. Epidemiol., 174, 267–273. [DOI] [PubMed] [Google Scholar]
- 12. Webb R., Brammah T., Lunt M., Urwin M., Allison T. and Symmons D. (2003) Prevalence and predictors of intense, chronic, and disabling neck and back pain in the UK general population. Spine (Phila. Pa. 1976), 28, 1195–1202. [DOI] [PubMed] [Google Scholar]
- 13. Miranda H., Viikari-Juntura E., Martikainen R., Takala E.P. and Riihimäki H. (2001) A prospective study of work related factors and physical exercise as predictors of shoulder pain. Occup. Environ. Med., 58, 528–534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. MacGregor A.J., Andrew T., Sambrook P.N. and Spector T.D. (2004) Structural, psychological, and genetic influences on low back and neck pain: a study of adult female twins. Arthritis Rheum., 51, 160–167. [DOI] [PubMed] [Google Scholar]
- 15. Ostergren P.-O., Hanson B.S., Balogh I., Ektor-Andersen J., Isacsson A., Orbaek P., Winkel J., Isacsson S.-O. and Malmö Shoulder Neck Study Group (2005) Incidence of shoulder and neck pain in a working population: effect modification between mechanical and psychosocial exposures at work? Results from a one year follow up of the Malmö shoulder and neck study cohort. J. Epidemiol. Community Health, 59, 721–728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Feleus A., Bierma-Zeinstra S.M.A., Miedema H.S., Verhagen A.P., Nauta A.P., Burdorf A., Verhaar J.A.N. and Koes B.W. (2007) Prognostic indicators for non-recovery of non-traumatic complaints at arm, neck and shoulder in general practice--6 months follow-up. Rheumatology (Oxford)., 46, 169–176. [DOI] [PubMed] [Google Scholar]
- 17. Costa L.d.C.M., Maher C.G., McAuley J.H., Hancock M.J., Herbert R.D., Refshauge K.M. and Henschke N. (2009) Prognosis for patients with chronic low back pain: inception cohort study. BMJ, 339, b3829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Bot S.D.M., Waal J.M., Terwee C.B., Windt D.A.W.M., Schellevis F.G., Bouter L.M. and Dekker J. (2005) Incidence and prevalence of complaints of the neck and upper extremity in general practice. Ann. Rheum. Dis., 64, 118–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Enthoven P., Skargren E. and Oberg B. (1976) (2004) clinical course in patients seeking primaryre for back or neck pain: a prospective 5-year follow-up of outcome and health care consumption with subgroup analysis. Spine (Phila. Pa., 29), 2458–2465. [DOI] [PubMed] [Google Scholar]
- 20. Hoving J.L., Vet H.C.W., Twisk J.W.R., Devillé W.L.J.M., Windt D., Koes B.W. and Bouter L.M. (2004) Prognostic factors for neck pain in general practice. Pain, 110, 639–645. [DOI] [PubMed] [Google Scholar]
- 21. Vos C.J., Verhagen A.P., Passchier J. and Koes B.W. (2008) Clinical course and prognostic factors in acute neck pain: an inception cohort study in general practice. Pain Med., 9, 572–580. [DOI] [PubMed] [Google Scholar]
- 22. Fejer R., Hartvigsen J. and Kyvik K.O. (2006) Heritability of neck pain: a population-based study of 33,794 Danish twins. Rheumatology (Oxford)., 45, 589–594. [DOI] [PubMed] [Google Scholar]
- 23. Hartvigsen J., Petersen H.C., Pedersen H.C., Frederiksen H. and Christensen K. (2005) Small effect of genetic factors on neck pain in old age: a study of 2,108 Danish twins 70 years of age and older. Spine (Phila. Pa. 1976), 30, 206–208. [DOI] [PubMed] [Google Scholar]
- 24. Ståhl M.K., El-Metwally A.A., Mikkelsson M.K., Salminen J.J., Pulkkinen L.R., Rose R.J. and Kaprio J.A. (2013) Genetic and environmental influences on non-specific neck pain in early adolescence: a classical twin study. Eur. J. Pain, 17, 791–798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Meng W., Adams M.J., Palmer C.N.A., 23andMe Research Team, Shi J., Auton A., Ryan K.A., Jordan J.M., Mitchell B.D., Jackson R.D. et al. (2019) Genome-wide association study of knee pain identifies associations with GDF5 and COL27A1 in UK biobank. Commun. Biol., 2, 321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Meng W., Adams M.J., Hebert H.L., Deary I.J., McIntosh A.M. and Smith B.H. (2018) A genome-wide association study finds genetic associations with broadly-defined headache in UK biobank (N=223,773). EBioMedicine, 28, 180–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Suri P., Palmer M.R., Tsepilov Y.A., Freidin M.B., Boer C.G., Yau M.S., Evans D.S., Gelemanovic A., Bartz T.M., Nethander M. et al. (2018) Genome-wide meta-analysis of 158,000 individuals of European ancestry identifies three loci associated with chronic back pain. PLoS Genet., 14, e1007601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Lai C.S.L., Fisher S.E., Hurst J.A., Vargha-Khadem F. and Monaco A.P. (2001) A forkhead-domain gene is mutated in a severe speech and language disorder. Nature, 413, 519–523. [DOI] [PubMed] [Google Scholar]
- 29. Spiteri E., Konopka G., Coppola G., Bomar J., Oldham M., Ou J., Vernes S.C., Fisher S.E., Ren B. and Geschwind D.H. (2007) Identification of the transcriptional targets of FOXP2, a gene linked to speech and language, in developing human brain. Am. J. Hum. Genet., 81, 1144–1157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Vernes S.C., Spiteri E., Nicod J., Groszer M., Taylor J.M., Davies K.E., Geschwind D.H. and Fisher S.E. (2007) High-throughput analysis of promoter occupancy reveals direct neural targets of FOXP2, a gene mutated in speech and language disorders. Am. J. Hum. Genet., 81, 1232–1250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Vargha-Khadem F., Watkins K., Alcock K., Fletcher P. and Passingham R. (1995) Praxic and nonverbal cognitive deficits in a large family with a genetically transmitted speech and language disorder. Proc. Natl. Acad. Sci. U. S. A., 92, 930–933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Acampora D., Merlo G.R., Paleari L., Zerega B., Postiglione M.P., Mantero S., Bober E., Barbieri O., Simeone A. and Levi G. (1999) Craniofacial, vestibular and bone defects in mice lacking the distal-less-related gene Dlx5. Development, 126, 3795–3809. [DOI] [PubMed] [Google Scholar]
- 33. Yoshihara M., Adolfsen B., Galle K.T. and Littleton J.T. (2005) Retrograde signaling by Syt 4 induces presynaptic release and synapse-specific growth. Science, 310, 858–863. [DOI] [PubMed] [Google Scholar]
- 34. Konopka G., Bomar J.M., Winden K., Coppola G., Jonsson Z.O., Gao F., Peng S., Preuss T.M., Wohlschlegel J.A. and Geschwind D.H. (2009) Human-specific transcriptional regulation of CNS development genes by FOXP2. Nature, 462, 213–217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Belton E., Salmond C.H., Watkins K.E., Vargha-Khadem F. and Gadian D.G. (2003) Bilateral brain abnormalities associated with dominantly inherited verbal and orofacial dyspraxia. Hum. Brain Mapp., 18, 194–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Yen C.-T. and Lu P.-L. (2013) Thalamus and pain. Acta Anaesthesiol. Taiwan, 51, 73–80. [DOI] [PubMed] [Google Scholar]
- 37. Brightwell J.J. and Taylor B.K. (2009) Noradrenergic neurons in the locus coeruleus contribute to neuropathic pain. Neuroscience, 160, 174–185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Benarroch E.E. (2006) Pain-autonomic interactions. Neurol. Sci., 27, S130–S5133. [DOI] [PubMed] [Google Scholar]
- 39. Chudler E.H. and Dong W.K. (1995) The role of the basal ganglia in nociception and pain. Pain, 60, 3–38. [DOI] [PubMed] [Google Scholar]
- 40. Johnston K.J.A., Adams M.J., Nicholl B.I., Ward J., Strawbridge R.J., Ferguson A., McIntosh A.M., Bailey M.E.S. and Smith D.J. (2019) Genome-wide association study of multisite chronic pain in UK biobank. PLoS Genet., 15, e1008164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Zhao J., Xu J., Wang W., Zhao H., Liu H., Liu X., Liu J., Sun Y., Dunaif A., Du Y. et al. (2018) Long non-coding RNA LINC-01572:28 inhibits granulosa cell growth via a decrease in p27 (Kip1) degradation in patients with polycystic ovary syndrome. EBioMedicine, 36, 526–538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. National Center for Biotechnology Information (2020) LOC105371829 uncharacterized LOC105371829 [Homo sapiens (human)]. LOC105371829 uncharacterized LOC105371829 [Homo sapiens (human)] https://www.ncbi.nlm.nih.gov/gene/105371829#gene-expression (accessed March 15, 2020).
- 43. Okamoto N., Fujikawa-Adachi K., Nishimori I., Taniuchi K. and Onishi S. (2001) cDNA sequence of human carbonic anhydrase-related protein, CA-RP X: mRNA expressions of CA-RP X and XI in human brain. Biochim. Biophys. Acta, 1518, 311–316. [DOI] [PubMed] [Google Scholar]
- 44. Visscher P.M., Wray N.R., Zhang Q., Sklar P., McCarthy M.I., Brown M.A. and Yang J. (2017) 10 years of GWAS discovery: biology, function, and translation. Am. J. Hum. Genet., 101, 5–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Meng W., Adams M.J., Reel P., Rajendrakumar A., Huang Y., Deary I.J., Palmer C.N.A., McIntosh A.M. and Smith B.H. (2019) Genetic correlations between pain phenotypes and depression and neuroticism. Eur. J. Hum. Genet.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Althubaiti A. (2016) Information bias in health research: definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc., 9, 211–217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Bycroft C., Freeman C., Petkova D., Band G., Elliott L.T., Sharp K., Motyer A., Vukcevic D., Delaneau O., O’Connell J. et al. (2018) The UK biobank resource with deep phenotyping and genomic data. Nature, 562, 203–209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Smith B.H., Campbell H., Blackwood D., Connell J., Connor M., Deary I.J., Dominiczak A.F., Fitzpatrick B., Ford I., Jackson C. et al. (2006) Generation Scotland: the Scottish family Health study; a new resource for researching genes and heritability. BMC Med. Genet., 7, 74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Smith B.H., Campbell A., Linksted P., Fitzpatrick B., Jackson C., Kerr S.M., Deary I.J., MacIntyre D.J., Campbell H., McGilchrist M. et al. (2013) Cohort profile: generation Scotland: Scottish family health study (GS: SFHS). The study, its participants and their potential for genetic research on health and illness. Int. J. Epidemiol. [DOI] [PubMed] [Google Scholar]
- 50. Hall L.S., Adams M.J., Arnau-Soler A., Clarke T.-K., Howard D.M., Zeng Y., Davies G., Hagenaars S.P., Maria Fernandez-Pujals A., Gibson J. et al. (2018) Genome-wide meta-analyses of stratified depression in generation Scotland and UK biobank. Transl. Psychiatry, 8, 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Moayyeri A., Hammond C.J., Hart D.J. and Spector T.D. (2013) The UK adult twin registry (TwinsUK resource). Twin Res. Hum. Genet., 16, 144–149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Yang J., Lee S.H., Goddard M.E. and Visscher P.M. (2011) GCTA: a tool for genome-wide complex trait analysis. Am. J. Hum. Genet., 88, 76–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Watanabe K., Taskesen E., Bochoven A. and Posthuma D. (2017) Functional mapping and annotation of genetic associations with FUMA. Nat. Commun., 8, 1826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Leeuw C.A., Mooij J.M., Heskes T. and Posthuma D. (2015) MAGMA: generalized gene-set analysis of GWAS data. PLoS Comput. Biol., 11, e1004219. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The GWAS summary statistics of neck or shoulder pain can be accessed through https://figshare.com/articles/fourpainphenotype2/7699583