

Abstract
Polycystic ovary syndrome is the most common endocrine disorder in women and a major cause of anovulatory infertility. Various medical options are used, alone or in combination, to treat subfertility associated with polycystic ovary syndrome. This narrative review was conducted to provide an update and summarize the available evidence on the management of polycystic ovary syndrome related infertility. A wide literature search was performed and preferably randomized controlled trials and systematic reviews were included. Management is often centered on lifestyle changes. Pharmacological ovulation induction is the next step, with recommended use of letrozole, clomiphene citrate or gonadotropins. When it fails, assisted reproductive technologies or laparoscopic ovarian drilling are frequently advised. Combination treatment with metformin is often recommended. More recent alternative and adjunctive treatments have been suggested, like inositol, vitamin D, bariatric surgery and acupuncture, but further research is needed for recommendation.
Keywords: assisted, female, infertility, metformin, ovulation induction, polycystic ovary syndrome, reproductive techniques
Introduction
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder in women, with an overall prevalence of 5% to 15%, and a frequent cause of infertility.1,2
Currently, the diagnosis is based on the European Society of Human Reproduction and Embryology and the American Society for Reproductive Medicine criteria, also known as Rotterdam criteria, from 2003.3 The patient must meet 2 out of 3 of the following criteria: I, oligo/anovulation; II, clinical (hirsutism, acne, male pattern alopecia) or biochemical signs of hyperandrogenism (raised serum testosterone levels); III, polycystic ovaries, that consist in 12 or more follicles measuring 2 to 9 mm in diameter or increased ovarian volume, over 10 cm3, on transvaginal ultrasound examination. Exclusion of other etiologies of menstrual disturbance and hyperandrogenism is mandatory.3
It is hypothesized that PCOS results from a vicious circle of androgen excess favoring abdominal and visceral adipose tissue deposition, that induces insulin resistance (IR) and compensatory hyperinsulinemia, further facilitating androgen secretion by the ovaries and adrenal glands.4 This cyclical pathogenetic interaction between IR, hyperinsulinemia, and hyperandrogenism, in combination with hypothalamic-pituitary dysfunction, leads to further ovarian dysfunction that can result in anovulation and infertility.4
Ovulation disorders are the cause of infertility in around 25% of couples and PCOS is the major cause of anovulatory infertility, accounting for approximately 70% of all cases.5–7 A range of endocrine and metabolic traits are also associated with PCOS and these include obesity, dyslipidemia, IR, hyperinsulinism and an increased risk of type 2 diabetes mellitus and cardiovascular disease. Women with PCOS may also have an increased risk of miscarriage and pregnancy complications such as gestational diabetes.8,9
Management of subfertility associated with PCOS is often centered on lifestyle changes, pharmacotherapy, surgical treatment and assisted reproductive technologies (ART). Recent alternative and adjunctive treatments have been used, and changes to the treatment algorithm have been suggested.10
This narrative review was conducted to provide an update and summarize the available evidence on the management of PCOS related infertility.
Material and methods
A literature search was performed on PubMed, Web of Science, Scopus and Cochrane Library, using the keywords PCOS, anovulation, infertility, and treatment/management/therapy. Relevant clinical guidelines were also searched. No language restrictions were applied. Preferably, randomized controlled trials and systematic reviews including randomized controlled trials and/or cohort studies were included. The latest search was completed on January 15, 2020.
Management of PCOS related infertility
Lifestyle changes
Lifestyle changes, promoting weight loss, are the first-line treatment recommended for women with PCOS (clinical consensus strong recommendation).10 It is known that a healthy diet and regular physical activity help to reduce IR and hyperandrogenism, and to optimize hormonal imbalance, lipid profile and cardiovascular health.11,12
When it comes to fertility outcomes, there is no robust evidence on the lifestyle changes impact. Some studies state that weight loss in overweight infertile women with PCOS can be associated with sporadic ovulation and better response to ovulation induction treatments with an increase in pregnancy and live birth rates.13,14 A study showed that a reduction in weight of as little as 5% from initial body weight could restore regular menses and improve response to ovulation-inducing and fertility medications.15 In addition, Hakimi and Cameron proposes that consistent physical activity, via modulation of the hypothalamic-pituitary-gonadal axis, can improve fertility outcomes.16
There are currently no specific diet type recommendations for women with PCOS, but an energy deficit of 30% or 500 to 750 kcal/d (1200–1500 kcal/d) could be prescribed.10 General recommendations on exercise include minimum of 150 min/wk of moderate intensity physical activity or 75 min/wk vigorous intensity and muscle strengthening activities on 2 nonconsecutive days per week.10 For modest weight loss, prevention of weight regain and greater health benefits, a minimum of 250 min/wk of moderate intensity activities or 150 min/wk of vigorous intensity and muscle strengthening activities on 2 nonconsecutive days per week is recommended.10 The effectiveness of lifestyle interventions is likely to be improved when including behavioral strategies such as goal setting, self-monitoring, cognitive restructuring, problem solving, and relapse prevention strategies.10,17
Ovulation induction
Since 70% of women with PCOS have anovulation or oligo-ovulation, ovulation induction is the cornerstone for treatment of women with PCOS suffering from infertility.
In women with PCOS and infertility due to anovulation alone with normal semen analysis, tubal patency testing, by hysterosalpingography or hysterosonosalpingography, should be considered prior to ovulation induction in women where there is suspected tubal infertility.10 Tubal pathology is a causative factor in 20% of subfertile couples.18 The WHO evidence report on infertility treatment in PCOS considers the assessment of tubal patency in infertility workup.19
Next, we present the most frequently used drugs for ovulation induction: letrozole, clomiphene citrate (CC), and gonadotropins.
Selective estrogen receptor modulators (SERMs)—clomiphene citrate (CC)
Clomiphene citrate is a selective estrogen receptor modulator (SERM) considered, for many years, the first choice of treatment for ovulation induction in women with PCOS. CC acts as an anti-estrogen, blocking the estrogen receptors at the hypothalamus, which results in an increase in gonadotropin-releasing hormone (GnRH) pulse amplitude, and subsequently increased anterior pituitary production of follicle-stimulating hormone (FSH) and luteinizing hormone (LH), thereby stimulating the final maturation of follicles (Fig. 1).20
Figure 1.
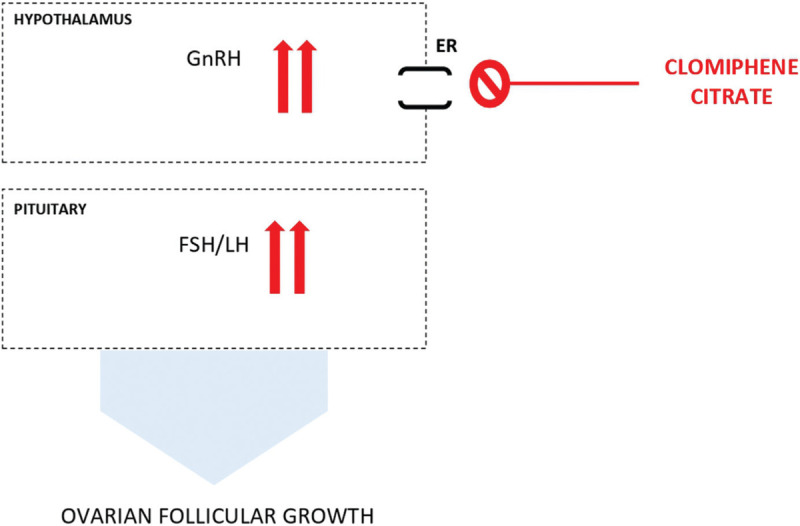
Mechanism of action of clomiphene citrate. Clomiphene citrate blocks the estrogen receptors at the hypothalamus, which results in an increase in GnRH pulse amplitude that leads to increased and prolonged FSH (and LH) secretion, stimulating the final maturation of follicles. ER = estrogen receptor, FSH = follicle-stimulating hormone, GnRH = gonadotropin-releasing hormone, LH = luteinizing hormone.
The anti-estrogenic effect can as well affect the endometrium and cervical mucus, with endometrial proliferation suppression, thus potentially inhibiting implantation.20 CC side effects include hot flushes, nausea, breast tenderness, dizziness and blurred vision.21 Standard treatment is usually a dose of 50 mg/d for 5 days, starting on day 2 to 5 of the cycle.21
CC induces ovulation in 70% to 90% of patients, but pregnancy rate is lower (30%–40%).22 Kafy and Tulandi described an increased twin pregnancy and triplets with CC (5%–7% and 0.3%, respectively), therefore monitoring with ultrasound to detect multifollicular development should be performed.23
Roughly 15% of PCOS patients do not respond to treatment.24 If ovulation is not achieved after 2 cycles, the dose can be gradually increased to 100 to 250 mg/d.21 If ovulation still does not occur, CC resistance is documented.24 Risk factors for resistance include obesity, IR and hyperandrogenemia.25
Current evidence-based guidelines propose the use of CC, as a second-line therapy, in women with PCOS with anovulatory infertility and no other infertility factors to improve ovulation and pregnancy rates (evidence-based conditional recommendation, very low quality of evidence).10
In women with PCOS who are CC-resistant, CC could be combined with metformin (evidence-based conditional recommendation, moderate quality of evidence).10 Combined therapy may have a useful role, suggested by a recent Cochrane review by Morley et al, that found an improved clinical pregnancy and ovulation rate with metformin and CC versus CC alone, despite no significant difference between the groups in live birth rates.26
Aromatase inhibitors (AI)—letrozole
The enzyme aromatase is responsible for androgen-to-estrogen conversion. Letrozole is the most used selective non-steroidal third-generation AI for ovulation induction.27 Letrozole suppresses ovarian estradiol secretion. Due to release from negative feedback on the hypothalamus, and temporary increase of intraovarian androgens, an increase in pituitary secretion of FSH, and follicular sensitivity to FSH occur, with subsequent improved ovulatory rates (Fig. 2).28
Figure 2.

Mechanism of action of letrozole. Letrozole inhibits androgen-to-estrogen conversion. Consecutively, the hypothalamic-pituitary axis is released from estrogenic negative feedback resulting in an increase in pituitary secretion of FSH with subsequent improved ovulatory rates. Also, increase in intraovarian androgens enhances follicular sensitivity to FSH. ER = estrogen receptor, FSH = follicle-stimulating hormone, GnRH = gonadotropin-releasing hormone, LH = luteinizing hormone.
Letrozole has relatively short half-life (approximately 45 hours) compared to CC, so adverse effects on estrogen target tissues are not expected.29
Effective use of letrozole for ovulation induction, in women with an inadequate response to CC, was first described by Mitwally and Casper in 2001.29 A recent Cochrane review, by Franik et al, based on moderate-quality evidence, found higher live birth rates with letrozole compared to CC, and based on high-quality evidence, also found similar ovarian hyperstimulation syndrome (OHSS) rates with letrozole or CC, and no difference for miscarriage or multiple pregnancy.30 Also, the risk of multiple pregnancy appears to be less with letrozole, compared to CC for its highest mono-follicular growth rate.31
Standard treatment is usually a dose of 2.5 mg/d for 5 days, starting on day 2 to 5 of a cycle (spontaneous or progestin-induced).32 Ovulation is monitored by ultrasound follicle tracking.32 When the leading follicle reaches at least 18mm, ovulation can be triggered with human chorionic gonadotropin (hCG) and followed by timed intercourse.32 Ovulation is expected to occur 36 to 48 hours after trigger. Couples should be advised to avoid unprotected intercourse if there are more than 2 mature follicles.32 If ovulation is not achieved, the dose can be doubled in the next cycle.32
Food and Drug Administration has not officially approved Letrozole use, for treatment of infertility and ovulation, nonetheless the latest evidence-based guidelines propose the use of letrozole as the first line pharmacological treatment for ovulation induction in women with PCOS, with anovulatory infertility and no other infertility factors, to improve ovulation, pregnancy and live birth rates (evidence-based strong recommendation, low to moderate quality of evidence).10 At this point, letrozole has been widely studied, and safety in use is documented.
Gonadotropins
In recent international guidelines, gonadotropin therapy for ovulation induction in anovulatory PCOS women continues to be recommended as a second-line option in women who have failed first line oral ovulation induction therapy, including AIs and SERMs (evidence-based conditional recommendation, low quality of evidence).10
In PCOS patients, gonadotropins are associated with a higher risk of OHSS and multiple pregnancies so they should only be used by clinicians having the requisite training and experience. Exogenous FSH stimulates proliferation of granulosa cells and follicular growth. The goal is to promote the growth and development of a single follicle. Different gonadotropin preparations, FSH or human menopausal gonadotropin appear to be equally effective, with no significant difference in live birth rate, clinical pregnancy rate, multiple pregnancy rate, miscarriage rate or OHSS incidence.33,34
To prevent hyperstimulation and minimize multifollicular development, low-dose step-up or a step-down protocols are preferred.10 In the low-dose step-up protocol, low initial doses of gonadotropins are used, after a menses, starting with 37.5 to 75 IU/d, and increasing in small increments 25 to 37.5 IU after 7 days or more if no follicle >10 mm has developed. Ultrasonography provides measurement of follicular development and generally should be performed after the first 4 to 5 days of treatment and at subsequent intervals of 1 to 3 days according to response. Although 7 to 12 total days of treatment is typical, longer durations of treatment may be required.35
In the step down protocol, high initial doses of gonadotropins are used, and then halved during follicle recruitment and growth, aiming to mimic physiologic changes of endogenous FSH.36 To reduce multiple pregnancy, careful follow-up of follicular development by ultrasound is required. In patients with >2 follicles ≥16 mm or ≥ 3 intermediate-sized follicles, cycle cancelation should be considered. In multifollicular development, conversion to in vitro fertilization (IVF) may also be an option.20 Once a mature follicle has developed, exogenous hCG is administered to stimulate ovulation followed by timed intercourse or intrauterine insemination. Currently, there are insufficient data on women with PCOS to recommend luteal support with progesterone.35
When it comes to combined therapy with metformin, Bordewijk et al found a higher cumulative live birth rate when compared with FSH alone, and insufficient evidence on multiple pregnancy rates and other adverse events.37 Palomba et al demonstrated that metformin administration significantly increases the live birth and pregnancy rates, and reduces the cancellation rate.38 International guidelines suggest the addition of metformin to gonadotropin stimulation to improve ovulation, pregnancy and live birth rates (evidence-based conditional recommendation, moderate quality of evidence).10
Metformin
Metformin is an insulin sensitizer, from the biguanides class, commonly used as a first-line antihyperglycaemic treatment for type 2 diabetes. Metformin increases glucose uptake in the periphery, enhances insulin sensitivity in the liver and peripheral tissues and inhibits hepatic gluconeogenesis, hence lowering blood glucose levels without causing hypoglycemia.39 Directly in the ovary, metformin lowers androgen production by theca cells, decreasing the activity of ovarian cytochrome P450c17a and expression of steroidogenic acute regulatory protein.40,41 Ovarian hyperandrogenism is responsible for premature follicular atresia and anovulation so metformin can theoretically have an ovulation stimulatory effect.42
Morley et al, in a recent Cochrane review, found that metformin alone compared with placebo may have higher rates of ovulation, clinical pregnancy and live birth, but superiority to CC alone was inconclusive.32 New international guidelines suggest that metformin can be used alone in women with PCOS, but patients should be informed that there are more effective ovulation induction agents.10
There is more supportive evidence for metformin use in combination with CC or gonadotropins and as adjunct in IVF ± intracytoplasmic sperm injection (ICSI) therapy, addressed in the respective sections of this review.
Doses used, alone or in combination, usually range from 1500 mg to 1700 mg/d, divided into 2 to 3 doses, for non-fertility studies.10
Metformin may cause mild, self-limiting, gastrointestinal adverse effects that can be minimized by starting with a low dose of 500 mg and increasing weekly to a maximum dose of 1500 mg.20 Abdominal discomfort, diarrhea, nausea, and vomiting, associated with modest weight loss, are the most commonly encountered symptoms.43
Assisted reproductive technologies (ART)
ART, mainly IVF, ICSI and in vitro maturation (IVM), have a role in PCOS after failure to respond to pharmacological ovulation induction or if there are other indications such as tubal damage or male factor infertility.10 Given the lack of evidence, in PCOS patients, no ART is favored in current international guidelines.10
In vitro fertilization ± intracytoplasmic sperm injection
IVF, with or without ICSI, is recommended as a third-line treatment or in the presence of other infertility factors (clinical consensus conditional recommendation).10 Heijnen et al meta-analysis found a similar chance for pregnancy or live birth per started IVF cycle between woman with PCOS and non-PCOS.44
Women with PCOS, who require IVF ± ICSI, have significantly increased risk of developing OHSS due to excessive response to FSH stimulation.10 A GnRH antagonist protocol should be preferred over an agonist protocol, as a simple safer alternative to reduce the duration of stimulation, total gonadotropin dose and incidence of OHSS.10,45
GnRH agonist versus hCG for oocyte triggering proved effective in reducing OHSS.46 As this negatively impacts pregnancy outcomes in autologous cycles it can be followed by a “freeze-all" program (ie, embryo transfer is not performed in the fresh autologous cycle).46,47 Frozen embryo transfer is performed in a later cycle. The freeze-all strategy is beneficial for pregnancy outcomes in high responders with 15 or more oocytes retrieved.47
The initial phase of IVF ± ICSI comprises ovarian hyperstimulation to enable the recruitment of multiple follicles. For this purpose, the protocol usually includes the co-administration of GnRH-analogues and gonadotropins.48 In women with PCOS, who undergo IVF ± ICSI, there seems to be no difference between the use of urinary or recombinant follicle stimulation hormone, and no benefit in adding exogenous LH supplement.10,27
According to Cochrane Database of Systematic Review, clinicians should consider metformin treatment before and during an ART cycle for women with PCOS to reduce OHSS rates in ART cycles (evidence-based conditional recommendation, low quality of evidence).10,49
In vitro maturation
IVM comprises the retrieval of immature oocytes from antral follicles, followed by in vitro final stages of meiosis maturation, under proper culture media additives.50 Since no exogenous human gonadotropin stimulation is needed for the IVM technique, the risk of OHSS is considerably lower, even excluded, in comparison to the standard IVF technique.51,52 This is a key benefit, as PCOS patients have higher risk of OHSS due to their elevated antral follicle counts.51 Also, children conceived after IVM are not adversely affected.53
Success rates, for live birth, following IVM, remain lower than traditional IVF but seem to have improved in recent years.51,52 A recent Cochrane review found no good quality evidence to support the recommendation of IVM in preference to IVF/ICSI.54 Likewise, international guidelines, given the lack of evidence, do not favored IVM to other options.10
Laparoscopic ovarian drilling
For women with anovulatory infertility who are resistant to pharmacological treatment, a minimally invasive surgical approach, laparoscopic ovarian drilling (LOD), may be an option for ovulation induction (evidence-based conditional recommendation, low quality of evidence).10,55
The most successfully used technique is performing 5 to 10 perforations on the surface of the ovary, bilaterally, using monopolar energy.56
The most suggested mechanism by which LOD leads to restoration of ovulatory function is that the destruction of androgen producing tissue, represented in the ovary by theca cells, leads to a decline in ovarian androgen production, reduction of peripheral androgen levels, with subsequent less conversion to estrogens.57,58 As a result, a reduced negative feedback from estrogens on the hypothalamus leads to a fall in LH levels and an increase in FSH levels, appropriately reestablishing follicles’ stimulation.57,58 Also, inside the ovary, the environment becomes predominantly estrogenic, which promotes follicular maturation and later ovulation.57,58
The surgical approach has some advantages, in comparison to medical therapy, such as reduced risk of OHSS and multiple pregnancy, lower cycle cancellation rates in patients later submitted to IVF, and subsequently fewer direct and indirect costs.57,59 On the other hand, a Cochrane review by Farquhar et al, found no significant difference between LOD and medical therapy on live birth pregnancy, miscarriage or OHSS rates.58
Also, there is concern that this technique may cause diminished ovarian reserve and periadnexal adhesion formation. An unilateral drilling is generally advised, since there is “no evidence of a significant difference in rates of live birth, pregnancy, ovulation or miscarriage” when comparing to bilateral drilling.58,60
Patients who are overweight or obese have higher risk of poor outcome and are more likely to develop complications.10,61 Abu Hashim et al found other possible predictors of poor outcome such as long term infertility, marked hyperandrogenism, high levels of AMH and low levels of LH.61
Bariatric surgery
Bariatric surgery is the most effective way for weight loss.62 It attenuates PCOS's associated clinical symptomatology, such as menstrual irregularity, hirsutism, and, possibly, infertility.20,63 In patients trying to conceive after bariatric surgery, one meta-analysis reported up to 58% spontaneous conception rates.64
It also can improve comorbidities as type 2 diabetes mellitus, hypertension, and dyslipidemia, and lower the risk of pre-eclampsia, gestational diabetes and large-for-gestational-age offspring in the bariatric population.10,20,63,65 On the other hand, bariatric surgery has a potential risk for nutritional deficiencies, in the context of malabsorptive states.20,27 This procedure has also been associated with shorter gestations, increased risk of small-for-gestational-age offspring and an increase in perinatal mortality.20,27,66
The international guidelines suggest that, for the purpose of improving fertility and pregnancy outcomes, bariatric surgery should be considered an experimental therapy in women with PCOS (clinical consensus conditional recommendation against the option).10 Balen et al proposes that bariatric surgery could be considered in women with PCOS, who have a BMI ≥ 35 kg/m2, and who remain infertile despite conservative treatment for a minimum of 6 months (based on low quality evidence).21
Inositol
Inositol (hexahydroxycyclohexane) is a 6-carbon ring chemical compound, having a hydroxyl group linked to each carbon of the ring, with 9 possible stereoisomeric forms.67 Two of these are myo-inositol (MI) and D-chiro-inositol (DCI), which play different relevant biological functions as insulin-sensitizing agents.20 In the ovary, MI mediates glucose uptake and FSH signaling, whereas DCI ameliorates insulin-induced androgen synthesis.20,68
In PCOS patients, an imbalance in tissue availability of these compounds appears to contribute to IR.69 A MI depletion and a DCI overload in the ovary, due to enhanced epimerase activity, also seems to impair oocyte quality.69 There is some emerging data suggesting that PCOS patients’ supplementation with inositol has benefits on ovulation rate and metabolic and hormonal profiles.70 Pundir et al found a significant improvement in ovulation rate and regularized menstrual cycles using inositol, compared with placebo.71 Özay et al found that MI administration increases clinical pregnancy rates, lowers total FSH dose and ovulation induction duration.72
However, 2 recent Cochrane reviews, by Showell et al and Morley et al, found no good quality evidence to support the use of MI to improve live birth rate and clinical pregnancy rate, and to decrease miscarriage rate or multiple pregnancy rate, for subfertile women with PCOS undergoing IVF or ovulation induction.32,73 Currently, given the lack of evidence, international guidelines recommend that inositol should be considered an experimental therapy in PCOS (evidence-based conditional recommendation against the option, very low quality of evidence).10
Vitamin D
The prevalence of vitamin D insufficiency or deficiency in reproductive age women is 45% to 90%.74,75
PCOS and vitamin D deficiency are both associated with IR.76 A study found that vitamin D deficiency in women with PCOS who underwent ovarian stimulation for the treatment of infertility was associated with significantly diminished rates of ovulation, of pregnancy, and ultimately a reduced chance of live birth.77
Vitamin D supplementation may be recommended as a potential therapeutic adjunct for the ovulatory dysfunction and metabolic disorders observed in women with PCOS. Controlled prospective randomized trials are needed to reach definitive conclusions regarding the role of supplementation with vitamin D in female reproduction.
Alternative therapies
Currently, the use of acupuncture for infertility treatment in women with PCOS is not supported by the very low quality evidence available.78–80 In regards to Chinese Herbal Medicine, there is also preliminary very low quality evidence on the enhancement of fertility outcomes.81–83
Conclusion
PCOS is a complex reproductive, metabolic, and psychological disorder characterized by a variety of clinical manifestations and a major cause of infertility.
Lifestyle changes should be considered first-line treatment recommendation for PCOS related infertility, before resorting to pharmacological options. Ovulation induction is the next step, being letrozole the first choice, followed by CC. In women who have failed first line oral ovulation induction therapy, gonadotropins are the next line. For women who do not become pregnant with ovulation induction drugs or have additional infertility factors, ART or LOD can be used (Fig. 3).
Figure 3.
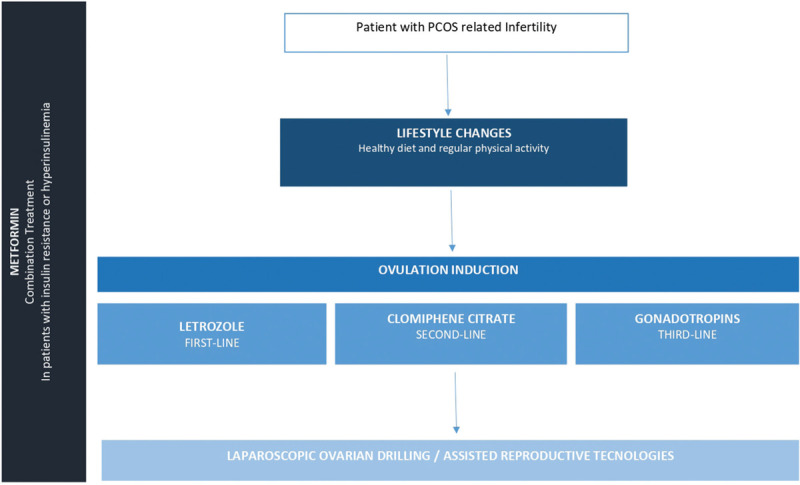
Proposed management of polycystic ovary syndrome related infertility.
In patients with IR or hyperinsulinemia, metformin use in combination with CC or gonadotropins and as adjunct in IVF ± ICSI therapy is still the best regimen recommended (Fig. 3).
Bariatric surgery can improve comorbidities associated with PCOS, but, at this time, should be considered experimental as a fertility therapy. Inositol and vitamin D may be useful, but further research is needed to be recommended.
Alternative therapies have no clear evidence for efficacy.
Conflicts of interest
Authors have declared no conflict of interest.
References
- [1].Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz BO. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod. 2016;31:2841–2855. [DOI] [PubMed] [Google Scholar]
- [2].Fauser BC, Tarlatzis BC, Rebar RW, et al. Consensus on women's health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertil Steril. 2012;97:28–38.e25. [DOI] [PubMed] [Google Scholar]
- [3].Rotterdam ESHRE/ASRM-Sponsored PCOS consensus Workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004;19:41–7. [DOI] [PubMed]
- [4].Escobar-Morreale HF. Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Nat Rev Endocrinol. 2018;14:270–284. [DOI] [PubMed] [Google Scholar]
- [5].National Collaborating Centre for Women's and Children's Health UK Fertility: Assessment and Treatment for People with Fertility Problems. 2013;Royal College of Obstetricians & Gynaecologists, London:139. [PubMed] [Google Scholar]
- [6].Hamilton-Fairley D, Taylor A. Anovulation. BMJ. 2003;327:546–549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].ESHRE Capri Workshop Group Health and fertility in World Health Organization group 2 anovulatory women. Hum Reprod Update. 2012;18:586–599. [DOI] [PubMed] [Google Scholar]
- [8].Rees DA, Jenkins-Jones S, Morgan CL. Contemporary reproductive outcomes for patients with polycystic ovary syndrome: a retrospective observational study. J Clin Endocrinol Metab. 2016;101:1664–1672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Bruyneel A, Catteau-Jonard S, Decanter C, et al. Polycystic ovary syndrome: what are the obstetrical risks? Gynecol Obstet Fertil. 2014;42:104–111. [DOI] [PubMed] [Google Scholar]
- [10].Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril. 2018;110:364–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Moran LJ, Hutchison SK, Norman RJ, Teede HJ. Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2011;2:CD007506. [DOI] [PubMed] [Google Scholar]
- [12].Pasquali R, Casimirri F, Vicennati V. Weight control and its beneficial effect on fertility in women with obesity and polycystic ovary syndrome. Hum Reprod. 1997;12 (Suppl 1):82–87. [DOI] [PubMed] [Google Scholar]
- [13].Kiddy DS, Hamilton-Fairley D, Bush A, et al. Improvement in endocrine and ovarian function during dietary treatment of obese women with polycystic ovary syndrome. Clin Endocrinol (Oxf). 1992;36:105–111. [DOI] [PubMed] [Google Scholar]
- [14].Legro RS, Dodson WC, Kunselman AR, et al. Benefit of delayed fertility therapy with preconception weight loss over immediate therapy in obese women with PCOS. J Clin Endocrinol Metab. 2016;101:2658–2666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Moran LJ, Pasquali R, Teede HJ, Hoeger KM, Norman RJ. Treatment of obesity in polycystic ovary syndrome: a position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertil Steril. 2009;92:1966–1982. [DOI] [PubMed] [Google Scholar]
- [16].Hakimi O, Cameron LC. Effect of exercise on ovulation: a systematic review. Sports Med. 2017;47:1555–1567. [DOI] [PubMed] [Google Scholar]
- [17].Brennan L, Teede H, Skouteris H, Linardon J, Hill B, Moran L. Lifestyle and behavioral management of polycystic ovary syndrome. J Womens Health (Larchmt). 2017;26:836–848. [DOI] [PubMed] [Google Scholar]
- [18].van Rijswijk J, van Welie N, Dreyer K, et al. The FOAM study: is hysterosalpingo foam sonography (HyFoSy) a cost-effective alternative for hysterosalpingography (HSG) in assessing tubal patency in subfertile women? Study protocol for a randomized controlled trial. BMC Womens Health. 2018;18:64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Costello MF, Misso ML, Balen A, et al. Evidence summaries and recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome: assessment and treatment of infertility. Hum Reprod Open. 2019;2019:hoy021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Homburg R. Clomiphene citrate—end of an era? A mini-review. Hum Reprod. 2005;20:2043–2051. [DOI] [PubMed] [Google Scholar]
- [21].Balen AH, Morley LC, Misso M, et al. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update. 2016;22:687–708. [DOI] [PubMed]
- [22].Messinis IE. Ovulation induction: a mini review. Hum Reprod. 2005;20:2688–2697. [DOI] [PubMed] [Google Scholar]
- [23].Kafy S, Tulandi T. New advances in ovulation induction. Curr Opin Obstet Gynecol. 2007;19:248–252. [DOI] [PubMed] [Google Scholar]
- [24].Jin P, Xie Y. Treatment strategies for women with polycystic ovary syndrome. Gynecol Endocrinol. 2018;34:272–277. [DOI] [PubMed] [Google Scholar]
- [25].Imani B, Eijkemans MJ, te Velde ER, Habbema JD, Fauser BC. Predictors of patients remaining anovulatory during clomiphene citrate induction of ovulation in normogonadotropic oligoamenorrheic infertility. J Clin Endocrinol Metab. 1998;83:2361–2365. [DOI] [PubMed] [Google Scholar]
- [26].Sharpe A, Morley LC, Tang T, Norman RJ, Balen AH. Metformin for ovulation induction (excluding gonadotrophins) in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2019;12:CD013505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Tanbo T, Mellembakken J, Bjercke S, Ring E, Abyholm T, Fedorcsak P. Ovulation induction in polycystic ovary syndrome. Acta Obstet Gynecol Scand. 2018;97:1162–7. [DOI] [PubMed]
- [28].Casper RF. Aromatase inhibitors in ovarian stimulation. J Steroid Biochem Mol Biol. 2007;106:71–75. [DOI] [PubMed] [Google Scholar]
- [29].Mitwally MF, Casper RF. Use of an aromatase inhibitor for induction of ovulation in patients with an inadequate response to clomiphene citrate. Fertil Steril. 2001;75:305–309. [DOI] [PubMed] [Google Scholar]
- [30].Franik S, Eltrop SM, Kremer JAM, Kiesel L, Farquhar C. Aromatase inhibitors (letrozole) for subfertile women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2018;5:CD010287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Huang S, Du X, Wang R, et al. Ovulation induction and intrauterine insemination in infertile women with polycystic ovary syndrome: A comparison of drugs. Eur J Obstet Gynecol Reprod Biol. 2018;231:117–121. [DOI] [PubMed] [Google Scholar]
- [32].Al-Fadhli R, Sylvestre C, Buckett W, Tan SL, Tulandi T. A randomized trial of superovulation with two different doses of letrozole. Fertil Steril. 2006;85:161–164. [DOI] [PubMed] [Google Scholar]
- [33].Weiss NS, Kostova E, Nahuis M, Mol BWJ, van der Veen F, van Wely M. Gonadotrophins for ovulation induction in women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2019;1:CD010290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Ikenaga H, Tanaka Y, Shiotani M, et al. Phase III trial comparing the efficacy and safety of recombinant- or urine-derived human chorionic gonadotropin for ovulation triggering in Japanese women diagnosed with anovulation or oligo-ovulation and undergoing ovulation induction with follitropin-alfa. Reprod Med Biol. 2017;16:45–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Practice Committees of the American Society for Reproductive Medicine and Society for Reproductive Endocrinology and Infertility Use of exogenous gonadotropins for ovulation induction in anovulatory women: a committee opinion. Fertil Steril. 2020;113:66–70. [DOI] [PubMed] [Google Scholar]
- [36].Morgante G, Massaro MG, Di Sabatino A, Cappelli V, De Leo V. Therapeutic approach for metabolic disorders and infertility in women with PCOS. Gynecol Endocrinol. 2018;34:4–9. [DOI] [PubMed] [Google Scholar]
- [37].Bordewijk EM, Nahuis M, Costello MF, et al. Metformin during ovulation induction with gonadotrophins followed by timed intercourse or intrauterine insemination for subfertility associated with polycystic ovary syndrome. Cochrane Database Syst Rev. 2017;1:CD009090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Palomba S, Falbo A, La Sala GB. Metformin and gonadotropins for ovulation induction in patients with polycystic ovary syndrome: a systematic review with meta-analysis of randomized controlled trials. Reprod Biol Endocrinol. 2014;12:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Dunn CJ, Peters DH. Metformin. A review of its pharmacological properties and therapeutic use in non-insulin-dependent diabetes mellitus. Drugs. 1995;49:721–749. [DOI] [PubMed] [Google Scholar]
- [40].Nestler JE, Jakubowicz DJ. Decreases in ovarian cytochrome P450c17 alpha activity and serum free testosterone after reduction of insulin secretion in polycystic ovary syndrome. N Engl J Med. 1996;335:617–623. [DOI] [PubMed] [Google Scholar]
- [41].Attia GR, Rainey WE, Carr BR. Metformin directly inhibits androgen production in human thecal cells. Fertil Steril. 2001;76:517–524. [DOI] [PubMed] [Google Scholar]
- [42].Utiger RD. Insulin and the polycystic ovary syndrome. N Engl J Med. 1996;335:657–658. [DOI] [PubMed] [Google Scholar]
- [43].Practice Committee of the American Society for Reproductive Medicine Role of metformin for ovulation induction in infertile patients with polycystic ovary syndrome (PCOS): a guideline. Fertil Steril. 2017;108:426–441. [DOI] [PubMed] [Google Scholar]
- [44].Heijnen EM, Eijkemans MJ, Hughes EG, Laven JS, Macklon NS, Fauser BC. A meta-analysis of outcomes of conventional IVF in women with polycystic ovary syndrome. Hum Reprod Update. 2006;12:13–21. [DOI] [PubMed] [Google Scholar]
- [45].Al-Inany HG, Youssef MA, Ayeleke RO, Brown J, Lam WS, Broekmans FJ. Gonadotrophin-releasing hormone antagonists for assisted reproductive technology. Cochrane Database Syst Rev. 2016;4:CD001750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Youssef MA, Van der Veen F, Al-Inany HG, et al. Gonadotropin-releasing hormone agonist versus HCG for oocyte triggering in antagonist-assisted reproductive technology. Cochrane Database Syst Rev. 2014;10:CD008046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Acharya KS, Acharya CR, Bishop K, Harris B, Raburn D, Muasher SJ. Freezing of all embryos in vitro fertilization is beneficial in high responders, but not intermediate and low responders: an analysis of 82,935 cycles from the Society for Assisted Reproductive Technology registry. Fertil Steril. 2018;110:880–887. [DOI] [PubMed] [Google Scholar]
- [48].Orvieto R. HMG versus recombinant FSH plus recombinant LH in ovarian stimulation for IVF: does the source of LH preparation matter? Reprod Biomed Online. 2019;39:1001–1006. [DOI] [PubMed] [Google Scholar]
- [49].Mourad S, Brown J, Farquhar C. Interventions for the prevention of OHSS in ART cycles: an overview of Cochrane reviews. Cochrane Database Syst Rev. 2017;1:CD012103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Yang ZY, Chian RC. Development of in vitro maturation techniques for clinical applications. Fertil Steril. 2017;108:577–584. [DOI] [PubMed] [Google Scholar]
- [51].Walls ML, Hart RJ. In vitro maturation. Best Pract Res Clin Obstet Gynaecol. 2018;53:60–72. [DOI] [PubMed] [Google Scholar]
- [52].Walls ML, Hunter T, Ryan JP, Keelan JA, Nathan E, Hart RJ. In vitro maturation as an alternative to standard in vitro fertilization for patients diagnosed with polycystic ovaries: a comparative analysis of fresh, frozen and cumulative cycle outcomes. Hum Reprod. 2015;30:88–96. [DOI] [PubMed] [Google Scholar]
- [53].Roesner S, von Wolff M, Elsaesser M, et al. Two-year development of children conceived by IVM: a prospective controlled single-blinded study. Hum Reprod. 2017;32:1341–1350. [DOI] [PubMed] [Google Scholar]
- [54].Siristatidis CS, Maheshwari A, Vaidakis D, Bhattacharya S. In vitro maturation in subfertile women with polycystic ovarian syndrome undergoing assisted reproduction. Cochrane Database Syst Rev. 2018;2018:CD006606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Neven ACH, Laven J, Teede HJ, Boyle JA. A summary on polycystic ovary syndrome: diagnostic criteria, prevalence, clinical manifestations, and management according to the latest international guidelines. Semin Reprod Med. 2018;36:5–12. [DOI] [PubMed] [Google Scholar]
- [56].Hueb CK, Dias Junior JA, Abrao MS, Filho EK. Drilling: medical indications and surgical technique. Rev Assoc Med Bras. 2015;61:530–535. [DOI] [PubMed] [Google Scholar]
- [57].Flyckt RL, Goldberg JM. Laparoscopic ovarian drilling for clomiphene-resistant polycystic ovary syndrome. Semin Reprod Med. 2011;29:138–146. [DOI] [PubMed] [Google Scholar]
- [58].Farquhar C, Brown J, Marjoribanks J. Laparoscopic drilling by diathermy or laser for ovulation induction in anovulatory polycystic ovary syndrome. Cochrane Database Syst Rev. 2012;6:CD001122. [DOI] [PubMed] [Google Scholar]
- [59].Farquhar CM. An economic evaluation of laparoscopic ovarian diathermy versus gonadotrophin therapy for women with clomiphene citrate-resistant polycystic ovarian syndrome. Curr Opin Obstet Gynecol. 2005;17:347–353. [DOI] [PubMed] [Google Scholar]
- [60].Abu Hashim H, Foda O, El Rakhawy M. Unilateral or bilateral laparoscopic ovarian drilling in polycystic ovary syndrome: a meta-analysis of randomized trials. Arch Gynecol Obstet. 2018;297:859–870. [DOI] [PubMed] [Google Scholar]
- [61].Abu Hashim H. Predictors of success of laparoscopic ovarian drilling in women with polycystic ovary syndrome: an evidence-based approach. Arch Gynecol Obstet. 2015;291:11–18. [DOI] [PubMed] [Google Scholar]
- [62].Colquitt JL, Pickett K, Loveman E, Frampton GK. Surgery for weight loss in adults. Cochrane Database Syst Rev. 2014;8:CD003641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [63].Skubleny D, Switzer NJ, Gill RS, et al. The impact of bariatric surgery on polycystic ovary syndrome: a systematic review and meta-analysis. Obes Surg. 2016;26:169–176. [DOI] [PubMed] [Google Scholar]
- [64].Milone M, Ýe Placido G, Musella M, et al. Incidence of successful pregnancy after weight loss interventions in infertile women: a systematic review and meta-analysis of the literature. Obes Surg. 2016;26:443–451. [DOI] [PubMed] [Google Scholar]
- [65].Charalampakis V, Tahrani AA, Helmy A, Gupta JK, Singhal R. Polycystic ovary syndrome and endometrial hyperplasia: an overview of the role of bariatric surgery in female fertility. Eur J Obstet Gynecol Reprod Biol. 2016;207:220–226. [DOI] [PubMed] [Google Scholar]
- [66].Legro RS. Ovulation induction in polycystic ovary syndrome: current options. Best Pract Res Clin Obstet Gynaecol. 2016;37:152–159. [DOI] [PubMed] [Google Scholar]
- [67].Showell MG, Mackenzie-Proctor R, Jordan V, Hodgson R, Farquhar C. Inositol for subfertile women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2018;12:CD012378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [68].Monastra G, Unfer V, Harrath AH, Bizzarri M. Combining treatment with myo-inositol and D-chiro-inositol (40:1) is effective in restoring ovary function and metabolic balance in PCOS patients. Gynecol Endocrinol. 2017;33:1–9. [DOI] [PubMed] [Google Scholar]
- [69].Facchinetti F, Bizzarri M, Benvenga S, et al. Results from the international consensus conference on myo-inositol and D-chiro-inositol in obstetrics and gynecology: the link between metabolic syndrome and PCOS. Eur J Obstet Gynecol Reprod Biol. 2015;195:72–76. [DOI] [PubMed] [Google Scholar]
- [70].Unfer V, Nestler J, Kamenov Z, Prapas N, Facchinetti F. Effects of inositol(s) in women with PCOS: a systematic review of randomized controlled trials. Int J Endocrinol. 2016;2016:1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [71].Pundir J, Psaroudakis D, Savnur P, et al. Inositol treatment of anovulation in women with polycystic ovary syndrome: a meta-analysis of randomised trials. Hum Reprod. 2018;125:299–308. [DOI] [PubMed] [Google Scholar]
- [72].Emekci Ozay O, Ozay AC, Cagliyan E, Okyay RE, Gulekli B. Myo-inositol administration positively effects ovulation induction and intrauterine insemination in patients with polycystic ovary syndrome: a prospective, controlled, randomized trial. Gynecol Endocrinol. 2017;33:524–528. [DOI] [PubMed] [Google Scholar]
- [73].Morley LC, Tang T, Yasmin E, Norman RJ, Balen AH. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst Rev. 2017;11:CD003053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [74].Bodnar LM, Simhan HN, Powers RW, Frank MP, Cooperstein E, Roberts JM. High prevalence of vitamin D insufficiency in black and white pregnant women residing in the northern United States and their neonates. J Nutr. 2007;137:447–452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [75].Nesby-O’Dell S, Scanlon KS, Cogswell ME, et al. Hypovitaminosis D prevalence and determinants among African American and white women of reproductive age: third National Health and Nutrition Examination Survey, 1988–1994. Am J Clin Nutr. 2002;76:187–192. [DOI] [PubMed] [Google Scholar]
- [76].Lips P, Eekhoff M, van Schoor N, et al. Vitamin D and type 2 diabetes. J Steroid Biochem Mol Biol. 2017;173:280–285. [DOI] [PubMed] [Google Scholar]
- [77].Butts SF, Seifer DB, Koelper N, et al. Vitamin D deficiency is associated with poor ovarian stimulation outcome in PCOS but not unexplained infertility. J Clin Endocrinol Metab. 2019;104:369–378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [78].Lim CED, Ng RWC, Cheng NCL, Zhang GS, Chen H. Acupuncture for polycystic ovarian syndrome. Cochrane Database Syst Rev. 2019;7:CD007689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [79].Xu L, Qiao X. Acupuncture is not as effective as infertility treatment in women with PCOS. Evid Based Med. 2017;22:229–230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [80].Stener-Victorin E. Acupuncture for infertility in women with polycystic ovary syndrome: What does it add? Semin Reprod Med. 2017;35:353–358. [DOI] [PubMed] [Google Scholar]
- [81].Zhou K, Zhang J, Xu L, Wu T, Lim CE. Chinese herbal medicine for subfertile women with polycystic ovarian syndrome. Cochrane Database Syst Rev. 2016;10:CD007535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [82].Arentz S, Abbott JA, Smith CA, Bensoussan A. Herbal medicine for the management of polycystic ovary syndrome (PCOS) and associated oligo/amenorrhoea and hyperandrogenism; a review of the laboratory evidence for effects with corroborative clinical findings. BMC Complement Altern Med. 2014;14:511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [83].Ong M, Peng J, Jin X, Qu X. Chinese herbal medicine for the optimal management of polycystic ovary syndrome. Am J Chin Med. 2017;45:405–422. [DOI] [PubMed] [Google Scholar]