

Abstract
Background
Medical therapy for dysmenorrhoea (painful menstrual cramps of the uterus) such as non‐steroidal anti‐inflammatory drugs or the oral contraceptive pill work by reducing myometrial (uterine muscle) activity. Transcutaneous electrical nerve stimulation (TENS) is a non‐pharmacological intervention shown to be effective for pain relief in a variety of conditions. TENS may be able to alter the body's ability to receive and perceive pain signals rather than having a direct effect on uterine contractions.
Objectives
To determine the effectiveness of high and low‐frequency TENS when compared to placebo, no treatment, or medical treatment for primary dysmenorrhoea.
Search methods
Electronic searches of the Cochrane Menstrual Disorders and Subfertility Group Register of controlled trials, The Cochrane Library (Issue 1, 2009), MEDLINE, EMBASE, CINAHL, and AMED were performed (updated April 2009) to identify relevant randomised controlled trials. The Cochrane Complementary Medicine Field Register of controlled trials (CISCOM) was also searched. Attempts were also made to identify trials from the UK National Research Register, the Clinical Trial Register, and the citation lists of review articles and included trials.
Selection criteria
The inclusion criteria were: randomised controlled trials (RCTs) of TENS compared to placebo, no treatment, or medical treatment for primary dysmenorrhoea. Exclusion criteria were: mild, infrequent, or secondary dysmenorrhoea and dysmenorrhoea associated with an intrauterine device (IUD).
Data collection and analysis
Seven RCTs were identified that fulfilled the inclusion criteria for this review. No new studies were identified in the update. Quality assessment and data extraction were performed independently by two review authors. Data unsuitable for meta‐analysis were reported as descriptive data and were included for discussion. The outcome measures were pain relief (dichotomous, visual analogue scale, descriptive), adverse effects, use of analgesics additional to treatment, and absence from work or school.
Main results
Overall, high‐frequency TENS was shown to be more effective for pain relief than placebo TENS (OR 7.2, 95% CI 3.1 to 16.5). Low‐frequency TENS was found to be no more effective in reducing pain than placebo TENS (OR 1.48, 95% CI 0.43 to 5.08). There were conflicting results regarding whether high‐frequency TENS was more effective than low‐frequency TENS.
Authors' conclusions
High‐frequency TENS was found to be effective for the treatment of dysmenorrhoea by a number of small trials. The minor adverse effects reported in one trial require further investigation. There is insufficient evidence to determine the effectiveness of low‐frequency TENS in reducing dysmenorrhoea.
Plain language summary
Transcutaneous electrical nerve stimulation for primary dysmenorrhoea
High‐frequency nerve stimulation may help relieve painful menstrual cramps. Dysmenorrhoea is a very common complaint that refers to painful menstrual cramps in the uterus. Transcutaneous electrical nerve stimulation (TENS) involves the sending of an electric current by placing electrodes on the skin to stimulate the nerves and reduce pain. It is thought to alter the body's ability to receive and understand pain signals rather than by having a direct effect on the uterine contractions. The review of trials found that high‐frequency TENS may help but there is not enough evidence to assess the effect of low‐frequency TENS. More research is needed.
Background
Description of the condition
Dysmenorrhoea refers to the occurrence of painful menstrual cramps of uterine origin. It is a common gynaecological complaint that can affect as many as 50% of women; 10% of these women suffer severely enough to render them incapacitated for one to three days each menstrual cycle (Dawood 1990b). This has a significant impact on personal health and it also has a global economic impact. In the USA alone, it is estimated that annual losses are 600 million work hours and two billion dollars (Dawood 1984).
Dysmenorrhoea is commonly defined within two subcategories. When the pelvic pain is associated with an identifiable pathological condition, such as endometriosis, it is considered to be secondary dysmenorrhoea. In contrast, menstrual pain without organic pathology is called primary dysmenorrhoea (Lichten 1987).
The initial onset of primary dysmenorrhoea is usually at or shortly (six to 12 months) after menarche (the commencement of menstrual periods), when ovulatory cycles are established. The pain duration is commonly 48 to 72 hours and is associated with the menstrual flow. In contrast, secondary dysmenorrhoea is more likely to occur years after the onset of menarche and occurs premenstrually as well as during menstruation. This distinction is not necessarily robust however as severe primary dysmenorrhoea in young women may indicate endometriosis (Punnonen 1980).
Description of the intervention
Dysmenorrhoea is commonly treated with non‐steroidal anti‐inflammatory drugs (NSAIDs) or oral contraceptive pills (OCPs), both of which work by reducing myometrial (uterine muscle) activity. However, these treatments are accompanied by a number of adverse effects making an effective non‐pharmacological method of treating dysmenorrhoea of great potential value.
Transcutaneous electrical nerve stimulation (TENS) involves stimulation of the skin using electrical currents at various pulse rates (frequencies) and intensities in order to provide pain relief. Since the late 19th century, TENS has been used to treat many conditions, such as acne, abscesses, corns, cramps, gout and impotence (Sheon 1984). It is also currently used to manage pain from contractions during labour (Carroll 1997).
TENS machines are portable and can be used in a home situation as well as a clinical setting. Modern day TENS can be divided into two subcategories, high and low frequency. Low‐frequency TENS (also referred to as acupuncture‐like TENS) usually consists of pulses delivered at between 1 Hz to 4 Hz, at high intensity and long pulse width so they evoke visible muscle contractions. High‐frequency TENS (conventional TENS) usually consists of pulses delivered at between 50 Hz and 120 Hz, at a low intensity (Kaplan 1997; Mannheimer 1985).
How the intervention might work
In dysmenorrhoea, TENS seems to work by alteration of the body's ability to receive or perceive pain signals rather than by having a direct effect on the uterine contractions (Smith 1991). The electrodes can be placed on traditional acupuncture sites or at the site of the pain. This modality has been stated to be effective for pain relief in a variety of conditions (Gersh 1985) but more recent systematic reviews have established that TENS is ineffective for postoperative pain (Carroll 1996) and labour pain (Carroll 1997). Evidence for the efficacy of TENS in chronic pain conditions is limited (McQuay 1998) although a systematic review indicates benefit for pain associated with knee osteoarthritis (Osiri 2001).
Why it is important to do this review
Consumers generally perceive complementary medicine to be more natural than conventional medicine and have fewer concerns about side effects. If pain relief can be brought about through non‐pharmacological means then this may be of benefit to both the consumer and healthcare providers.
Objectives
To determine the effectiveness of high and low‐frequency TENS compared to placebo, no treatment, or medical treatment for primary dysmenorrhoea.
Methods
Criteria for considering studies for this review
Types of studies
All prospective randomised controlled trials comparing TENS to placebo, no treatment, or medical treatment for the treatment of primary dysmenorrhoea.
Types of participants
Participants in the trials had to meet all the following inclusion criteria for the trial to be included in the review.
Inclusion criteria:
women of reproductive age;
women with moderate to severe primary dysmenorrhoea (severe or incapacitating pain for at least one day of menses);
women affected by dysmenorrhoea in > 50% of their menstrual cycles.
If participants in the trial meet any of the following exclusion criteria the trial was not included in the review.
Exclusion criteria:
women with secondary dysmenorrhoea (i.e. associated with identifiable pelvic pathology);
women with dysmenorrhoea due to the presence of an intrauterine device (IUD);
women with mild or infrequent dysmenorrhoea.
Types of interventions
The specific interventions to be considered were as follows.
1. High‐frequency TENS versus placebo or no treatment for primary dysmenorrhoea. 2. Low‐frequency TENS versus placebo or no treatment for primary dysmenorrhoea. 3. High‐frequency TENS versus low‐frequency TENS for primary dysmenorrhoea. 4. High‐frequency TENS versus acupuncture for primary dysmenorrhoea. 5. Low‐frequency TENS versus acupuncture for primary dysmenorrhoea. 6. TENS versus other medical treatment for primary dysmenorrhoea.
Low‐frequency TENS (acupuncture‐like TENS) is defined as 1 Hz to 4 Hz pulses delivered at high intensity. High‐frequency TENS (conventional TENS) is defined as 50 Hz to 120 Hz pulses delivered at a low intensity. Placebo TENS is when no electrical current is used, so the settings and amplitude do not produce any electrical stimulation.
Types of outcome measures
Primary outcomes
Pain relief (measured either on a visual analogue scale (VAS), other scales, or a dichotomous scale)
Secondary outcomes
1. Adverse effects from treatment (incidence and types of side effects) 2. Requirements for additional medication (measured as a ratio for women requiring analgesics additional to their assigned treatment) 3. Restriction of daily life activities (measured as a ratio for women who report activity restriction) 4. Absence from work or school (measured as a ratio for women reporting absences from work or school)
Search methods for identification of studies
Electronic searches
All reports which described (or might describe) randomised controlled trials of TENS in the treatment of dysmenorrhoea were obtained using the following search strategies (April 2009). The Menstrual Disorders and Subfertility Group Specialised Register of controlled trials was searched for any trials with dysmenorrhoea or dysmenorrhoea in the title, abstract, or keyword sections; see the Review Group Module (The Cochrane Library) for more details on the makeup of the Specialised Register (Appendix 3). Other databases searched were: CENTRAL (The Cochrane Library) (Appendix 4), MEDLINE (Appendix 1), EMBASE ( Appendix 2), AMED (Appendix 5), and PsycINFO (Appendix 6).
Searching other resources
The National Research Register (NRR), a register of ongoing and recently completed research projects funded by or of interest to the United Kingdom's National Health Service, as well as entries from the Medical Research Council's Clinical Trials Register and details on reviews in progress collected by the NHS Centre for Reviews and Dissemination were searched for any trials with dysmenorrhoea as a keyword. The Clinical Trials register, a registry of both federally and privately funded US clinical trials, was also searched for the same keyword.
The Cochrane Complementary Medicine Field Register of controlled trials (CISCOM) was searched for any trials with dysmenorrhoea in the title, abstract, or keyword fields. No additional trials were found.
A letter was written to the Chinese Cochrane Centre requesting information on any useful Chinese databases, however they were unable to help as they are a newly formed centre and are still under‐resourced at present. We plan to re‐contact them for future updates of this review.
The citation lists of relevant publications, review articles, included studies, and abstracts of scientific meetings were also searched.
Letters were sent to major investigators of TENS or acupuncture techniques and the authors of included studies to seek information on additional published or unpublished trials.
Data collection and analysis
Selection of studies
One review author scanned the titles and abstracts of articles retrieved by the search and removed those that were clearly not relevant. The full text of potentially relevant articles were retrieved. The selection of trials for inclusion in the review was performed independently by two review authors (MW, CS). Where necessary, primary authors were contacted to provide additional information on patient eligibility criteria and methodologies. Any disagreements were resolved by discussion and consensus, or by a third author.
Data extraction and management
Data were extracted from eligible studies using a data extraction form designed by the review authors. Where studies had multiple publications, the main trial report was used as the reference supplemented by additional details from secondary papers. The review authors corresponded with primary authors, where possible, to resolve any data queries.
Assessment of risk of bias in included studies
The included studies were assessed for risk of bias. The Cochrane risk of bias assessment tool was used to assess:
sequence generation;
allocation concealment;
blinding;
completeness of the outcome data;
selective outcome reporting;
other potential sources of bias.
The selection of trials for inclusion in the original review was performed independently by the two review authors (MW, CS) after employing the search strategy described previously, and by MS and CF in the update (2009). The conclusions can be referred to in the 'Risk of bias' tables and Figure 1 and Figure 2.
1.
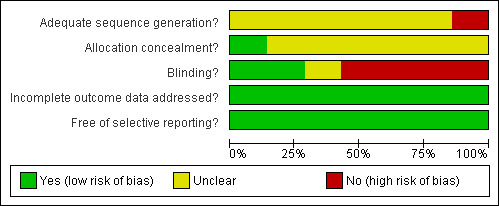
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
2.
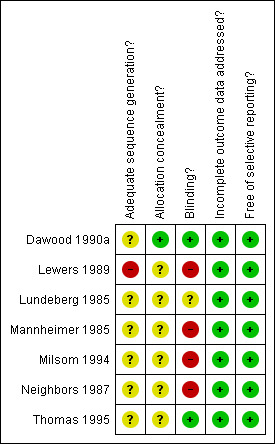
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Additional information on trial methodology, original trial data, or both were sought from the authors of the majority of trials. This additional information was sought by sending letters, e‐mail, or both to the authors of all the trials except Santiesteban 1985 (no current contact details for the authors could be found). Replies were received from Prof Dawood from the Dawood 1990a study, and D Lewers from the Lewers 1989 study; both supplied extra information regarding trial methodology. As no response was received from the trial by Santiesteban 1985 the study has been moved to the studies awaiting classification until we are able to confirm the methodology.
Measures of treatment effect
Statistical analyses were performed in accordance with the guidelines for statistical analysis developed by the Cochrane Menstrual Disorders and Subfertility Group. Where possible, the outcomes were pooled statistically. For dichotomous data (for example, proportion of participants with a specific adverse side effect), results for each study were expressed as an odds ratio (OR) with 95% confidence interval (CI) and combined for meta‐analysis with RevMan software using the Peto‐modified Mantel‐Haenszel method. Continuous differences between groups in the meta‐analysis were shown as a mean difference (MD) and 95% CI. A fixed‐effect model was used and heterogeneity between the results of different studies was examined by inspecting the scatter in the data points and the overlap in their CIs and more formally by checking the results of the Chi2 tests. No significant heterogeneity was found among studies that were combined in the meta‐analysis.
For a number of included studies we were not able to extract data that could be used in the meta‐analysis. These data were included as descriptive data in 'other data' tables and can also be viewed in the 'Data and analyses' tables.
Unit of analysis issues
Four of the included studies were of crossover design (Dawood 1990a; Lundeberg 1985; Milsom 1994; Thomas 1995). Phase‐one data (data prior to crossover) were not available for any of these trials. Crossover trials have been criticised for leading to invalid estimates of effect when the outcome measure used affects entry to subsequent phase of the trial (for example where pregnancy is the outcome of interest those becoming pregnant in phase one of the trial cannot be crossed over to the alternative treatment). In the case of this review, this problem is less of a concern as the main outcome measure is pain relief.
The only real concern is the potential for carryover effects of TENS from one menstrual cycle to another, which is likely to be minimal as all four crossover trials performed treatment during the menses only. Therefore, due to the small likelihood of bias, the small number of trials, and the minimal pooling of data in the meta‐analysis, the results of the crossover trials were included in this review. The only instance where data from a parallel and crossover trial were pooled is for the outcome of overall experience of pain relief for low‐frequency TENS versus placebo TENS. Both trials and the meta‐analysis reported a non‐significant result for this outcome and including or excluding the crossover data did not impact on this conclusion (Lundeberg 1985).
Dealing with missing data
Data were analysed on an intention‐to‐treat basis, as far as possible, and attempts were made to obtain missing data from the primary investigators, where possible.
Assessment of heterogeneity
The review authors considered whether the clinical and methodological characteristics of the included studies were sufficiently similar for meta‐analysis to provide a meaningful summary. Statistical heterogeneity was assessed using the I2 statistic. An I2 > 50% was taken to imply substantial heterogeneity and further exploration was undertaken using sensitivity analyses to explain this, if required.
Assessment of reporting biases
The review authors aimed to minimise the potential impact of reporting bias by ensuring a comprehensive search for eligible studies and by being alert for duplication of data. A funnel plot was not possible due the limited number of studies included in the review.
Data synthesis
The data from the primary studies were combined using a fixed‐effect model in the following comparisons.
High‐frequency TENS versus placebo.
Low‐frequency TENS versus placebo.
High‐frequency TENS versus low‐frequency TENS.
TENS versus medical treatment.
Subgroup analysis and investigation of heterogeneity
There was no planned subgroup analysis in this review.
Sensitivity analysis
In one trial, the mean pain relief figure reported in the trial (26.1) did not correlate with the reported scores for each participant that were also presented (46, 57, 60, 0, 0, 0, 41, 40, 1) (Mannheimer 1985). The authors of the trial did not respond to correspondence, therefore the mean used in the meta‐analysis was not that reported in the report but was recalculated from the individual scores that were also given (a mean of 27.2). A sensitivity analysis using both means showed that there was very little difference in the ORs they elicited.
Updating the review
It is the intention of the review authors that a new search for RCTs will be carried out yearly and the review updated accordingly.
Results
Description of studies
Results of the search
Nine randomised controlled trials were identified that involved TENS for the treatment of dysmenorrhoea. Seven of these trials were included in this review, one was excluded, and one is awaiting classification.
Included studies
Three of the trials were of parallel design (Lewers 1989; Mannheimer 1985; Neighbors 1987) and four used a crossover design (Dawood 1990a; Lundeberg 1985; Milsom 1994; Thomas 1995).
Five of the trials specified the inclusion of women with primary dysmenorrhoea only. Four of these trials performed some type of physical or gynaecological examination to confirm the diagnosis of 'no pathology'. Other common exclusion criteria were the use of oral contraceptives (OCPs) or an IUD. The range of ages of participants included in all the trials was 15 to 38 years.
Physical treatment regimens are particularly difficult to administer consistently and there are additional problems associated with the use of placebo or sham techniques. Summarised below are details on how the included trials dealt with treatment consistency and the use of placebo or sham therapies. For additional information on trial characteristics see the table 'Characteristics of included studies'. For a summary of the TENS modalities used, such as frequencies and pulse width, see TENS modalities (Table 1; Table 2).
1. TENS modalities ‐ high frequency.
| Study | Hz; freq; pulse rate | Pulse width | Intensity | Other |
| Dawood 1990 | 100 | 100 microsec | comfortable tingling | Tenzcare portable unit used |
| Lundeberg 1985 | 100 | 200 microsec | low intensity ‐ below pain threshold | square wave pulses |
| Mannheimer | 50‐100 | 40‐75 microsec | comfortable | |
| Milsom | 70‐100 | 200 microsec | high ‐ 40‐50 mA | |
| Thomas 1995 | 100 | 200 microsec | no info given | monopolar pulses |
2. TENS modalities ‐ low frequency.
| Study | Hz; freq; pulse rate | Pulse width | Intensity | Other |
| Lewers 1989 | 1 | 40 μsec | highest tolerable | Note this trial used msec ‐ also called hyperstimulation |
| Lundeberg 1985 | 2 | 200 μsec | high, muscle contractions produces | pulse trains of 80 msec, 2/sec |
| Mannheimer 1985 | 1‐4 | 100‐250 μsec | to tolerance level, with visible rhythmic muscle contractions | |
| Neighbors 1987 | 1 | 40 μsec | increased to tolerance | |
| Santiesteban 1985 | 5 | 250 μsec | to tolerance level with minimum of palpable contractions | |
| Thomas 1995 | 2 | 200 μsec | no information | Trains of monopolar square wave pulses with a duration of 0.2 msec |
Dawood 1990a (high‐frequency TENS, placebo TENS, ibuprofen) Women were treated with TENS for two cycles, placebo TENS for one cycle, and ibuprofen for one cycle; the treatment sequence was randomised. Portable TENS units were used and for high‐frequency TENS the woman was able to adjust the amplitude to produce a comfortable tingling sensation or achieve satisfactory pain relief. The placebo TENS was set up in exactly the same way except the settings and amplitude did not produce any electrical stimulation. The participants and investigators were blinded to whether real or placebo TENS was being used, however for the ibuprofen cycle blinding was not possible. There was no information on how the investigators ensured that the TENS units were correctly used by the women, however daily logs were kept of the amount of TENS use per day.
Lewers 1989 (low‐frequency TENS, placebo pill) Women were randomly assigned to the experimental or control group. Both groups then participated in another study in which the electrical conductance of four auricular acupuncture points was measured, which involved acupressure to these four points. This additional treatment could have affected the main study results. After this study the women in the control group were given a placebo pill and put into the prone position for 30 minutes. The experimental group were hooked up to the TENS unit and also placed in the same position. The intensity of the TENS treatment was adjusted to the highest level tolerable by the participant.
Lundeberg 1985 (high‐frequency TENS, low‐frequency TENS, placebo TENS) Women were treated with all three interventions during separate cycles. They were randomised to whichever treatment they received first. The electrodes used, their placement, and the procedure were kept the same for each treatment. For high‐frequency TENS the stimulus intensity was below the pain threshold.
Electrodes were placed on the painful area (all participants complained of lower back pain) and TENS was applied for 20 minutes. If this resulted in pain relief then treatment was continued at the same stimulation point for a further 25 minutes. If there was no pain relief then electrodes were moved to either a trigger point or acupuncture point close to the area of pain. If no pain reduction was achieved at any of these points then electrodes were applied for 25 minutes within the painful area. For low‐frequency TENS stimulus the intensity produced muscular contractions. For placebo TENS the apparatus was lacking electrical output but women were told it was ultra‐high frequency TENS and that they may not experience any cutaneous sensation.
Mannheimer 1985 (high‐frequency TENS, low‐frequency TENS, placebo TENS) All women were instructed separately by the same experimenter in the use of TENS and the expected stimulation sensation for each group. Women were then randomised to: 1) conventional TENS, 2) acupuncture‐like TENS, or 3) placebo TENS. The instructions the women received differed on a group basis by the method of adjusting stimulation parameters, electrode placement, and description of electrical sensations.
All participants used the same type of portable TENS unit and the only non‐fixed variable was intensity of stimulation. Women in the conventional TENS group were instructed to use an intensity that produced a comfortable, perceptible paraesthesia without muscle contraction. The acupuncture‐like TENS group were to use an intensity that produced visible rhythmic muscle contractions. The placebo‐TENS group was told to set it at maximum and that they may or may not experience a mild tingling sensation. The placebo group was also told that if a LED light came on their unit was non‐functional; this was not possible however as dead batteries were used.
All participants were given instruction cards that illustrated electrode placement. Placement was the same for groups one and three. Those in group two placed the electrodes on acupuncture points and were instructed how to find the area of greatest tenderness. Treatment for all groups was 30 minutes in duration then discontinued until pain returned; a record of use was kept. Pain was rated immediately before and after TENS use.
Milsom 1994 (high‐frequency, high‐intensity TENS, naproxen) Women were randomly allocated to either high‐intensity TENS or a single dose of naproxen (500 mg). Randomisation occurred after intrauterine pressure had been recorded for 30 minutes via a catheter. Treatment was performed at an outpatient clinic during the first 24 hours of the women's cycles. For the following cycle, participants received the therapy form not received in the first cycle.
For the TENS treatment electrodes were placed on the lower part of the abdomen and the back. It is unclear whether electrode placement was the same for all participants. The intensity of the electrical stimulation was gradually increased and women were informed that they might experience some pain. After 10 seconds, if the participant had not adapted to the intensity it was reduced to a more acceptable level. At 60 seconds of treatment the stimulator was switched off; if pain had not disappeared by this time then participants received a further 60 to 120 seconds of stimulation. Once analgesia had been achieved in the stimulated area some women felt pain in neighbouring regions. In these cases stimulation was repeated until pain relief was obtained. No information was given about how many women received reduced intensity stimulation or additional stimulation. All measurements lasted at least four hours for both treatment groups; pain relief was measured every 15 minutes with women in the supine position.
Neighbors 1987 (low‐frequency TENS, placebo pill) Treatment was scheduled when the participant called to report pain. Participants were randomly allocated to low‐frequency TENS or a placebo pill. All participants were positioned prone on a treatment table for 30 minutes. The placebo group were told they were taking a "drug that has been used in the past for pain relief". The TENS group had eight electrodes attached to four acupuncture points bilaterally and the TENS unit was started. The intensity was slowly increased to a level as intense as was tolerable. After five minutes the intensity was increased, if tolerable. Total treatment time was 30 minutes. Pain assessment occurred prior to treatment and immediately after; participants were sent home with further measures to be completed at 30, 90, and 150 minutes following treatment.
Thomas 1995 (acupuncture: manual stimulation, low‐frequency electrical stimulation, high‐frequency electrical stimulation, periosteal stimulation; TENS: low‐frequency, high‐frequency, and placebo TENS) Acupuncture treatment was performed by one of two trained professionals, TENS treatment was administered by a trained physiotherapist. It is unclear how participants were placed in the TENS or acupuncture group. The acupuncture group were allocated to four different modes of treatment, one per cycle. Entry to the initial treatment was random and followed by the other treatments in a predetermined order, the fifth‐cycle treatment was a mode of the participants's choice.
The TENS group were allocated to three different modes of treatment, one per cycle. Entry to the initial treatment was random and followed by the other treatments in a predetermined order, the fourth‐cycle treatment was a mode of the participant's choice. For the placebo TENS group there was no electrical output to the electrodes and participants were told it was an ultra‐high frequency mode where skin sensations might or might not be perceptible. All treatments (except periosteal stimulation) lasted 20 minutes; all outcome assessments were performed in the same manner. Two treatments were performed each cycle at approximately seven days and three days prior to the onset of menstruation.
Excluded studies
One trial was excluded from the review (Janke 1984). The trial compared low‐frequency TENS with a control that was a mixture of high‐frequency TENS and placebo TENS. This combination did not clearly fit any of the intended comparisons so the trial was excluded. For more information see the table 'Characteristics of excluded studies'.
Risk of bias in included studies
Allocation
One included study was given an allocation score of A as correspondence with the author revealed that random allocation was performed via a centralised randomisation process (Dawood 1990a). Other included studies were given an allocation score of B due to unclear allocation concealment, except Lewers 1989 which was given an allocation score of C for alternate allocation. One trial reported no information on randomisation or allocation (Thomas 1995). The remaining trials stated that allocation was random but failed to give adequate details regarding the method of allocation or concealment. This represents a source of potential bias.
Blinding
In one trial the participants and the investigators were both blind to assignment status (Dawood 1990a). In two trials only the participants were blinded (Lundeberg 1985; Mannheimer 1985). Two trials were open due to the different types of interventions used (that is TENs versus placebo pill or naproxen) (Lewers 1989; Milsom 1994). The remaining two trials gave no information regarding blinding of assignment status (Neighbors 1987; Thomas 1995); one of these trials was probably open as it compared TENS with a placebo pill, two quite different types of interventions (Neighbors 1987). The other trial involved two arms of treatment, acupuncture and TENS (Thomas 1995). While blinding may have been possible in the TENS arm, the four different types of acupuncture that were compared were too different for the women to have remained unaware of the differences in the interventions so double‐blinding would have been impossible. Lack of blinding represents a potential source of bias.
Incomplete outcome data
All but one of the studies (Lewers 1989) analysed all the patients. Lewers 1989 did not analyse the final data from two patients but did use the last‐observation‐carried‐forward method.
Selective reporting
All of the main outcomes were reported.
Other potential sources of bias
No other potential sources of bias were identified.
Effects of interventions
Overall seven studies that involved transcutaneous electrical nerve stimulation for the treatment of primary dysmenorrhoea were identified and included. The studies involved a total of 164 participants.
1) High‐frequency TENS versus placebo
Refer to Figure 3
3.
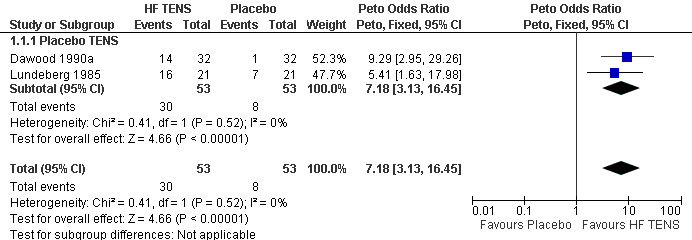
Forest plot of comparison: 1 High Frequency TENS vs Placebo, outcome: 1.1 Pain relief ‐ overall experience.
There were four studies comparing the use of high‐frequency TENS with placebo TENS for the treatment of dysmenorrhoea (Dawood 1990a; Lundeberg 1985; Mannheimer 1985; Thomas 1995). Overall results showed that high‐frequency TENS was more effective for pain relief than placebo TENS. For pain relief reported as a dichotomous variable the OR was 7.2 (95% CI 3.1 to 16.5) in favour of high‐frequency TENS (two trials). When pain relief was measured with a VAS the weighted mean difference (WMD) was 45.0 (95% CI 22.5 to 67.5) in favour of high‐frequency TENS (one trial). One trial could not be included in the meta‐analysis due to the form in which results were reported but was included as descriptive data; it found no difference between high‐frequency TENS and placebo TENS for pain relief.
Only one of the trials reported any adverse effects associated with treatment (Dawood 1990a): 4/32 women using high‐frequency TENS experienced muscle vibrations, tightness, and headaches after use and slight redness or burning of the skin (OR 8.2, 95% CI 1.1 to 60.9). There were no reported adverse effects from placebo TENS.
Two trials reported data on the use of analgesics additional to the TENS treatment (Dawood 1990a;Thomas 1995). There was no significant difference in the number of women needing additional analgesics between high‐frequency and placebo TENS (one trial; OR 0.3, 95% CI 0.1 to 1.1). There was also no significant difference in the number of analgesic tablets taken between the two groups (one trial; WMD 0.1, 95% CI ‐2.1 to 2.4).
One trial reported absence from work or school as the number of lost hours per menstrual cycle (Thomas 1995). There was no significant difference between high‐frequency and placebo TENS for this outcome (WMD 0.04, 95% CI ‐0.4 to 0.5).
2) Low‐frequency TENS versus placebo
Refer to Figure 4 and Figure 5
4.
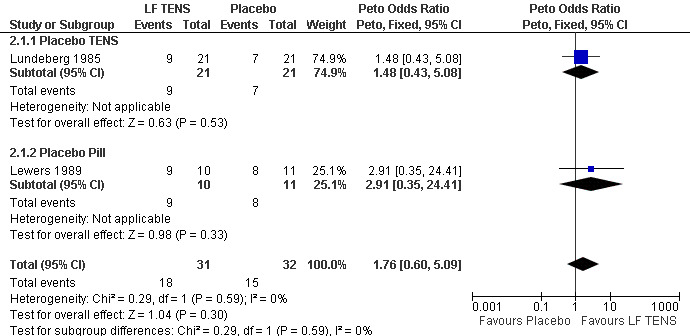
Forest plot of comparison: 2 Low Frequency TENS vs Placebo, outcome: 2.1 Pain relief ‐ overall experience.
5.
Forest plot of comparison: 2 Low Frequency TENS vs Placebo, outcome: 2.2 Pain relief ‐ 100pt VAS.
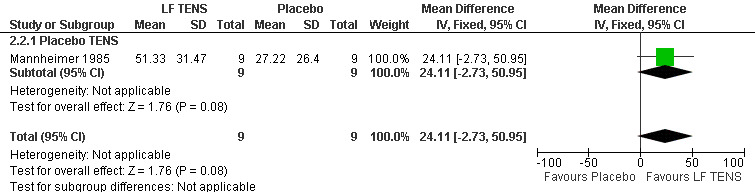
There were three studies comparing the use of low‐frequency TENS with placebo TENS (Lundeberg 1985; Mannheimer 1985; Thomas 1995) and two studies comparing low‐frequency TENS with a placebo pill (Lewers 1989; Neighbors 1987 ) for the treatment of dysmenorrhoea. Overall results suggested no significant difference between low‐frequency TENS and placebo TENS or a placebo pill for pain relief. For pain relief reported as a dichotomous variable the OR was 1.48 (95% CI 0.43 to 5.08) when comparing low‐frequency TENS and placebo TENS (one trial); and the OR was 2.9 (95% CI 0.35, 24.4) when comparing low‐frequency TENS and placebo pill (one trial). When pain relief was measured using a VAS the WMD was 24.1 (95% CI ‐2.73 to 51.95; 1 trial). Two trials could not be included in the meta‐analysis due to the form the results were reported in but they were included as descriptive data. One trial comparing low‐frequency TENS and placebo TENS reported a significant difference between low‐frequency TENS and placebo TENS in pain relief (P < 0.05); the other trial showed that low‐frequency TENS was more effective at reducing pain than a placebo pill (P < 0.05).
Only one trial reported any information on adverse effects (Lewers 1989) and found there were none in either the TENS group or the placebo pill group.
One trial reported on the number of tablets of additional analgesic used (Thomas 1995): the low‐frequency TENS group used significantly less than the placebo TENS group (WMD ‐3.1, 95% CI ‐5.5 to ‐0.7). No significant difference was reported between the two groups for absence from work or school (Thomas 1995) (WMD ‐0.2, 95% CI ‐0.6 to 0.2).
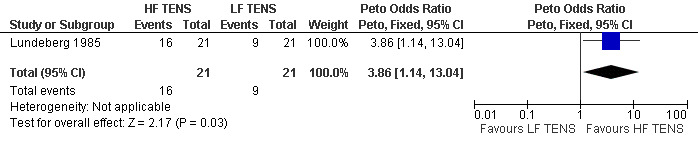
3) High‐frequency TENS versus low‐frequency TENS There were three studies that compared high‐frequency TENS with low‐frequency TENS for the treatment of dysmenorrhoea (Lundeberg 1985; Mannheimer 1985; Thomas 1995). For pain relief reported as a dichotomous variable the OR was 3.9 (95% CI 1.1 to 13.0; 1 trial) in favour of high‐frequency TENS (Figure 6). When pain relief was measured with a VAS the WMD was 20.9 (95% CI ‐4.4 to 46.1) showing no significant difference between the two types of TENS but a trend towards high‐frequency TENS as achieving more pain relief (one trial) (Mannheimer 1985); see Figure 7. One trial could not be included in the meta‐analysis due to the form the results were reported in and was included as descriptive data, it found low‐frequency TENS to be more likely to reduce pain than high‐frequency TENS.
6.
Forest plot of comparison: 3 High Frequency TENS vs Low Frequency TENS, outcome: 3.1 Pain relief ‐ overall experience.
7.

Forest plot of comparison: 3 High Frequency TENS vs Low Frequency TENS, outcome: 3.2 Pain relief ‐ 100pt VAS.
There was a significant difference in favour of low‐frequency TENS for the number of analgesic tablets taken in addition to TENS treatment (WMD 3.2, 95% CI 0.5 to 5.9). There was no significant difference between the two groups for the outcome of absence from work or school (WMD 0.2, 95% CI ‐0.2 to 0.6) (Thomas 1995).
4) TENS versus medical treatment
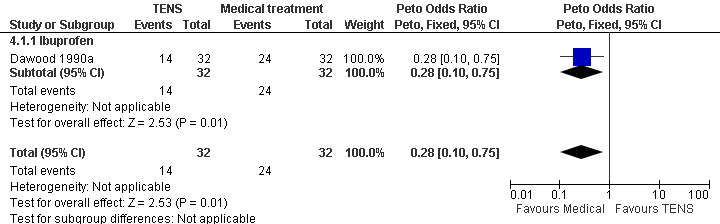
There were two trials that compared a medical therapy with TENS (Dawood 1990a); Milsom 1994). One trial compared ibuprofen (a non‐steroidal anti‐inflammatory drug) with high‐frequency TENS (Dawood 1990a). For the outcome of pain relief reported as a dichotomous variable ibuprofen proved to be significantly better at reducing pain (OR 0.3, 95% CI 0.1 to 0.8). This trial reported no significant difference between the two treatments for additional use of analgesics (OR 0.4, 95% CI 0.1 to 1.4) (Figure 8).
8.
Forest plot of comparison: 4 TENS vs Medical Treatment, outcome: 4.1 Pain relief ‐ overall experience.
Another trial compared high‐frequency, high‐intensity TENS with naproxen (a non‐steroidal anti‐inflammatory drug) (Milsom 1994). For the outcome of pain relief there was no significant difference in the pain scores for each group. This trial is reported as descriptive data as it could not be used in the meta‐analysis.
There was a significant difference between high‐frequency TENS and ibuprofen in the number of adverse effects experienced by participants (OR 26.7, 95% CI 5.5 to 130.9); 10/12 women in the TENS group experienced pain from the treatment while no adverse effects were reported by those taking ibuprofen. The women who reported pain from TENS stated that they were prepared to accept the short‐term pain from the treatment in return for relief of dysmenorrhoea.
Discussion
Summary of main results
This review aimed to assess the effectiveness of TENS and acupuncture for the treatment of primary dysmenorrhoea. Despite the growing popularity of complementary therapies there is a general lack of well‐designed research to evaluate the effectiveness of these therapies to treat specific conditions.
Currently available data suggests that high‐frequency TENS is effective in reducing primary dysmenorrhoea. Overall, high‐frequency TENS was shown to be more effective for pain relief than placebo TENS. Low‐frequency TENS was found to be no different in reducing pain than placebo TENS although there is a trend towards efficacy. There were conflicting results regarding whether high‐frequency TENS is more effective than low‐frequency TENS. The small number of participants in the majority of included trials is reflected by the wide confidence intervals and lack of precision in many of the comparisons, meaning that clear recommendations for practice cannot be made.
TENS may be an alternative treatment option for women with dysmenorrhoea who wish to stop using non‐steroidal anti‐inflammatory drugs (NSAIDs), oral contraceptives, or other analgesics because the existing medication is ineffective, has unacceptable adverse effects, or due to personal choice. An effective non‐pharmacological method of treating dysmenorrhoea would be of great potential value in treating dysmenorrhoea; however, there are a number of problems with the trials included in this review and research into physical therapies in general.
Overall completeness and applicability of evidence
The evidence reported here represents small studies which may not be adequately powered to answer the clinical question. The participants and outcomes are representative and valid.
Quality of the evidence
The data presented in this review were from seven RCTs involving 164 women with dysmenorrhoea. The main methodological problems are explored below in the potential biases but are also represented by the small number of women included in the studies and the lack of data which could be entered into a meta‐analysis. Blinding of this type of intervention is methodologically difficult and rarely conducted.
Potential biases in the review process
Use of a control or placebo group
A difficult issue in all randomised controlled trials of physical and complementary therapies is the choice of an adequate control or placebo treatment. To control adequately for all the factors that may contribute to the treatment as a comparable placebo treatment, rather than a waiting list control or a no‐treatment control, is preferable. Placebo TENS typically consists of TENS units and electrodes set up just like the real TENS but with no electrical output to the electrodes. This means the only potential difference in treatment is the lack of physical stimulation of the skin, making it a good control that can be easily blinded. Placebo TENS can also take the form of working electrodes attached to the wrong meridian points although this is not necessarily an effective control as there is a theoretical opportunity to create adverse effects or possibly a therapeutic effect by stimulating any meridian or acupuncture point. There is no guarantee that using mock TENS on a part of the meridian or other point will have no effect.
Another important aspect to the design of the control arm of these trials is to ensure that participants remain blinded to their group allocation. One way to achieve this is to recruit participants naive to the treatment being evaluated.
Blinding
Double blinding (both the participant and the treatment provider) in physical therapies is generally considered impossible as the treatment provider needs to physically deliver the treatment or placebo. Single blinding (of the participant) is also considered difficult, especially if the control is a different type of treatment for example TENS versus a placebo pill.
Standardisation of treatment
Physical therapies are performed with variations by treatment providers. Treatment is often individually tailored to each participant's set of symptoms. Even if this is not the case the different therapists vary the duration of treatment, the exact placement of electrodes, the frequency of electrical stimulation, frequency of treatments, timing of treatments in the cycle, the number of treatments performed, and the individuality of treatment; for example stimulation intensity and pulse duration are often adjusted to participants' tolerance levels.
Traditional versus western medical approach
TENS uses meridian points for the placement of electrodes. The western approach often advocates placement in the areas that are painful (for example the abdomen and the lower back). These different approaches to dysmenorrhoea can affect how treatments are performed, who receives treatment, and the end results for the outcomes measured. The impact of these factors on treatment outcome is not clear as these types of variations between practitioners of TENS can also be found in conventional medicine.
Other methodological issues
With TENS some of the included trials used self‐administered treatment whereas others were physician administered. For self‐administered treatments the tendency is to place electrodes on the painful areas, while physician‐administered treatments are more likely to be administered on meridian points.
Another aspect that could affect the evaluation of the treatments is the differences in the physiological effects of the two different types of TENS. With high‐frequency TENS a small portable unit can be used, therefore users are able to carry on daily activities. However with low‐frequency TENS the low rate triggers rhythmic muscle contractions which make it difficult for women to carry out daily activities.
Authors' conclusions
Implications for practice.
The available data on high‐frequency TENS suggest it is effective for the treatment of dysmenorrhoea. The clinical importance of the minor adverse effects that were reported in one study is unclear. TENS represents a suitable alternative for women who prefer not to use medication or wish to minimise their NSAID consumption. There are some data to suggest that women using TENS are less likely to require additional analgesia, an observation that supports clinical advice to consider TENS as an option, although the degree of relief obtainable from TENS alone is less than that from analgesic drugs.
The present review has not demonstrated the efficacy of low‐frequency TENS. This may be because the single study was insufficiently powered. Clear recommendations for practice cannot be made.
Implications for research.
It is likely that women experiencing dysmenorrhoea will continue to seek advice on and treatment with TENS, therefore further research is needed to establish the optimal manner in which TENS modalities should be used. The condition is very common and the lifestyle impact and economic burden justifies a search for effective and acceptable treatments. Inclusion of cost comparisons and outcomes in clinical trials will enable better assessment of the true value of treatment interventions. There is a need to improve the quality of future randomised controlled trials. The methods of trials need to be fully described so as to aid the reader as to the validity and relevance of reported studies. In particular, allocation blinding needs to be meticulous within the practical constraints discussed above.
Methodologically sound and adequately powered clinical trials are needed evaluating the role of low‐frequency TENS for primary dysmenorrhoea. More information is needed on the potential adverse effects of high‐frequency TENS and the acceptability of TENS treatments to women needs to be explored using both questionnaires and qualitative methods.
What's new
| Date | Event | Description |
|---|---|---|
| 10 August 2009 | Review declared as stable | No new trials were identified |
| 5 May 2009 | New search has been performed | This review has now been updated. No new trials were identified. Risk of bias tables have been added and the trial has been formatted as per Cochrane guidelines. An earlier version of the review included acupuncture but at the time of updating the review was split into two reviews, one of TENS and one of acupuncture. |
History
Protocol first published: Issue 2, 2000 Review first published: Issue 1, 2002
| Date | Event | Description |
|---|---|---|
| 19 November 2008 | Amended | This published review: Proctor ML, Smith CA, Farquhar CM, Stones RW. Transcutaneous electrical nerve stimulation and acupuncture for primary dysmenorrhoea. Cochrane Database of Systematic Reviews 2002, Issue 1, has now been divided into two reviews 'Transcutaneous electrical nerve stimulation for primary dysmenorrhoea' and 'Acupuncture for primary dysmenorrhoea'. |
| 16 June 2008 | Amended | Converted to new review format. |
| 22 November 2001 | New citation required and conclusions have changed | Substantive amendment |
Notes
Trials relating to acupuncture have now been excluded from this review and will the subject of a new review.
Acknowledgements
The authors acknowledge the helpful comments of those who refereed previous versions of this review, and the authors of included trials that supplied extra information and data. Special thanks are also due to Stephen Kennedy for his work as a co‐author on the protocol; Xu Jin for his attempts to search for trials in China; Sarah Hetrick, Review Group Coordinator, for her help with all the inevitable problems; and to Sue Furness, Trials Search Coordinator, for her assistance with identifying trials; Marian Showell and Julie Brown for their assistance in the update of the review in 2009.
Appendices
Appendix 1. MEDLINE search strategy
1 exp Menstruation disorders/ (21321) 2 Pelvic pain/ (2191) 3 (pelvic adj5 pain).tw. (4323) 4 Dysmenorrhea/ (2469) 5 dysmenorrh$.tw. (2884) 6 (painful adj5 menstrua$).tw. (110) 7 (painful adj5 period$).tw. (212) 8 menstrual disorder.tw. (78) 9 or/1‐8 (26974) 10 Transcutaneous electric nerve stimulation/ (2524) 11 TENS.tw. (4211) 12 electric stimulation therapy/ or electroacupuncture/ (14755) 13 electrostimulat$.tw. (2455) 14 electrotherap$.tw. (795) 15 electric stimulat$.tw. (3097) 16 nerve stimulat$.tw. (14604) 17 electroanalges$.tw. (173) 18 or/10‐17 (36843) 19 9 and 18 (136) 20 randomized controlled trial.pt. (263105) 21 controlled clinical trial.pt. (78151) 22 (randomized or randomised).ab. (207653) 23 placebo.ab. (108884) 24 drug therapy.fs. (1280145) 25 randomly.ab. (126866) 26 trial.ab. (181582) 27 groups.ab. (879682) 28 or/20‐27 (2337353) 29 (animals not (humans and animals)).sh. (3235549) 30 28 not 29 (1980294) 31 30 and 19 (44) 32 limit 31 to yr="2001 ‐ 2009" (26) 33 from 32 keep 1‐26 (26)
Appendix 2. EMBASE search strategy
1 exp Menstruation Disorder/ (23479) 2 Pelvis Pain Syndrome/ (4684) 3 Dysmenorrhea/ (3608) 4 menstru$ disorder$.ti,ab,hw,tn,mf. (3213) 5 (pelvi$ adj5 pain).ti,ab,hw,tn,mf. (6495) 6 (painful adj5 menstrua$).ti,ab,hw,tn,mf. (64) 7 (painful adj5 period$).ti,ab,hw,tn,mf. (165) 8 Dysmenorrh$.ti,ab,hw,tn,mf. (4038) 9 or/1‐8 (29638) 10 nerve stimulation/ or electroacupuncture/ or transcutaneous nerve stimulation/ (19586) 11 electrostimulation therapy/ (3174) 12 TENS.ti,ab,hw,tn,mf. (3963) 13 electrostimulat$.ti,ab,hw,tn,mf. (32173) 14 electrotherap$.ti,ab,hw,tn,mf. (574) 15 electric stimulat$.ti,ab,hw,tn,mf. (1372) 16 nerve stimulat$.ti,ab,hw,tn,mf. (27444) 17 electroanalges$.ti,ab,hw,tn,mf. (155) 18 or/10‐17 (60372) 19 9 and 18 (274) 20 Clinical Trial/ (531633) 21 Randomized Controlled Trial/ (165971) 22 exp randomization/ (26539) 23 Single Blind Procedure/ (7989) 24 Double Blind Procedure/ (71472) 25 Crossover Procedure/ (21005) 26 Placebo/ (123698) 27 Randomi?ed controlled trial$.tw. (32428) 28 Rct.tw. (2659) 29 random allocation.tw. (636) 30 randomly allocated.tw. (10126) 31 allocated randomly.tw. (1347) 32 (allocated adj2 random).tw. (559) 33 Single blind$.tw. (7418) 34 Double blind$.tw. (84352) 35 ((treble or triple) adj blind$).tw. (140) 36 placebo$.tw. (109416) 37 prospective study/ (80141) 38 or/20‐37 (698900) 39 case study/ (5939) 40 case report.tw. (118491) 41 abstract report/ or letter/ (491476) 42 or/39‐41 (613634) 43 38 not 42 (674549) 44 43 and 19 (105) 45 limit 44 to yr="2007 ‐ 2009" (29) 46 from 45 keep 1‐29 (29)
Appendix 3. Menstrual Disorders and Subfertility Group search strategy
Keywords CONTAINS "dysmenorrhea" or "Dysmenorrhea‐Symptoms" or "dysmenorrhoea" or "pain‐dysmenorrhea" or Title CONTAINS "dysmenorrhea" or "Dysmenorrhea‐Symptoms" or "dysmenorrhoea" or "pain‐dysmenorrhea"
AND
Keywords CONTAINS "TENS" or "TENS study" or "electro‐acupuncture" or "electro‐magnetic" or "electroacupuncture" or "electrical activation" or "Transcutaneous Electric Nerve Stimulation" or Title CONTAINS "TENS" or "TENS study" or "electro‐acupuncture" or "electro‐magnetic" or "electroacupuncture" or "electrical activation" or "Transcutaneous Electric Nerve Stimulation"
Appendix 4. CENTRAL search strategy
1 exp Menstruation disorders/ (1067) 2 Pelvic pain/ (157) 3 (pelvic adj5 pain).tw. (364) 4 Dysmenorrhea/ (259) 5 dysmenorrh$.tw. (517) 6 (painful adj5 menstrua$).tw. (10) 7 (painful adj5 period$).tw. (38) 8 menstrual disorder.tw. (8) 9 or/1‐8 (1699) 10 Transcutaneous electric nerve stimulation/ (437) 11 TENS.tw. (450) 12 electric stimulation therapy/ or electroacupuncture/ (1013) 13 electrostimulat$.tw. (166) 14 electrotherap$.tw. (115) 15 electric stimulat$.tw. (141) 16 nerve stimulat$.tw. (1108) 17 electroanalges$.tw. (14) 18 or/10‐17 (2429) 19 9 and 18 (23) 20 limit 19 to yr="2001 ‐ 2008" (9) 21 from 20 keep 1‐9 (9)
Appendix 5. AMED search strategy
1 exp Menstruation disorders/ (348) 2 Pelvic pain/ (0) 3 (pelvic adj5 pain).tw. (148) 4 Dysmenorrhea/ (71) 5 dysmenorrh$.tw. (125) 6 (painful adj5 menstrua$).tw. (4) 7 (painful adj5 period$).tw. (11) 8 menstrual disorder.tw. (1) 9 or/1‐8 (541) 10 Transcutaneous electric nerve stimulation/ (543) 11 TENS.tw. (325) 12 electric stimulation therapy/ or electroacupuncture/ (637) 13 electrostimulat$.tw. (89) 14 electrotherap$.tw. (879) 15 electric stimulat$.tw. (1569) 16 nerve stimulat$.tw. (743) 17 electroanalges$.tw. (8) 18 or/10‐17 (3596) 19 9 and 18 (7) 20 limit 19 to yr="2001 ‐ 2008" (2) 21 from 20 keep 1‐2 (2)
Appendix 6. PsycINFO search strategy
1 exp Menstruation disorders/ (0) 2 Pelvic pain/ (0) 3 (pelvic adj5 pain).tw. (279) 4 Dysmenorrhea/ (136) 5 dysmenorrh$.tw. (248) 6 (painful adj5 menstrua$).tw. (20) 7 (painful adj5 period$).tw. (40) 8 menstrual disorder.tw. (15) 9 or/1‐8 (588) 10 Transcutaneous electric nerve stimulation/ (0) 11 TENS.tw. (492) 12 electric stimulation therapy/ or electroacupuncture/ (0) 13 electrostimulat$.tw. (208) 14 electrotherap$.tw. (110) 15 electric stimulat$.tw. (447) 16 nerve stimulat$.tw. (1215) 17 electroanalges$.tw. (12) 18 or/10‐17 (2337) 19 9 and 18 (3) 20 limit 19 to yr="2001 ‐ 2008" (2) 21 from 20 keep 1‐2 (2)
Data and analyses
Comparison 1. High‐frequency TENS versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain relief ‐ overall experience | 2 | 106 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 7.18 [3.13, 16.45] |
| 1.1 Placebo TENS | 2 | 106 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 7.18 [3.13, 16.45] |
| 2 Pain relief ‐ 100pt VAS | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | 45.0 [22.53, 67.47] |
| 2.1 Placebo TENS | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | 45.0 [22.53, 67.47] |
| 3 Pain relief ‐ descriptive data | Other data | No numeric data | ||
| 3.1 Placebo TENS | Other data | No numeric data | ||
| 4 Adverse effects | 1 | 64 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 8.17 [1.10, 60.85] |
| 4.1 Placebo TENS | 1 | 64 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 8.17 [1.10, 60.85] |
| 5 Use of additional analgesics (n of women) | 1 | 64 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.09, 1.14] |
| 5.1 Placebo TENS | 1 | 64 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.09, 1.14] |
| 6 Use of additional analgesics (n of tablets taken) | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 0.14 [‐2.10, 2.38] |
| 6.1 Placebo TENS | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 0.14 [‐2.10, 2.38] |
| 7 Absence from work/school (lost hours) | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 0.04 [‐0.37, 0.45] |
| 7.1 Placebo TENS | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 0.04 [‐0.37, 0.45] |
1.1. Analysis.
Comparison 1 High‐frequency TENS versus placebo, Outcome 1 Pain relief ‐ overall experience.
1.2. Analysis.
Comparison 1 High‐frequency TENS versus placebo, Outcome 2 Pain relief ‐ 100pt VAS.
1.3. Analysis.
Comparison 1 High‐frequency TENS versus placebo, Outcome 3 Pain relief ‐ descriptive data.
| Pain relief ‐ descriptive data | ||||
|---|---|---|---|---|
| Study | Pain scale used | HF TENS | Placebo | Conclusion |
| Placebo TENS | ||||
| Thomas 1995 | Total Pain measure on 100mm VAS 3 x day for 3 days Max score = 900 Pretreatment scores mean: 375 std dev: 157 | mean: 353 std dev: 128 n=12 | mean: 387 std dev: 167 n=12 | No difference between High frequency TENS and Placebo TENS in reducing pain (using ANOVA, p>0.05) |
1.4. Analysis.
Comparison 1 High‐frequency TENS versus placebo, Outcome 4 Adverse effects.
1.5. Analysis.
Comparison 1 High‐frequency TENS versus placebo, Outcome 5 Use of additional analgesics (n of women).
1.6. Analysis.
Comparison 1 High‐frequency TENS versus placebo, Outcome 6 Use of additional analgesics (n of tablets taken).
1.7. Analysis.
Comparison 1 High‐frequency TENS versus placebo, Outcome 7 Absence from work/school (lost hours).
Comparison 2. Low‐frequency TENS versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain relief ‐ overall experience | 2 | 63 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.76 [0.60, 5.09] |
| 1.1 Placebo TENS | 1 | 42 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.48 [0.43, 5.08] |
| 1.2 Placebo Pill | 1 | 21 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 2.91 [0.35, 24.41] |
| 2 Pain relief ‐ 100pt VAS | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | 24.11 [‐2.73, 50.95] |
| 2.1 Placebo TENS | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | 24.11 [‐2.73, 50.95] |
| 3 Pain relief ‐ descriptive data | Other data | No numeric data | ||
| 3.1 Placebo TENS | Other data | No numeric data | ||
| 3.2 Placebo Pill | Other data | No numeric data | ||
| 4 Adverse effects | 1 | 21 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.1 Placebo Pill | 1 | 21 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Use of additional analgesics (n of tablets taken) | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | ‐3.07 [‐5.46, ‐0.68] |
| 5.1 Placebo TENS | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | ‐3.07 [‐5.46, ‐0.68] |
| 6 Absence from work/school (lost hours) | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | ‐0.19 [‐0.57, 0.19] |
| 6.1 Placebo TENS | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | ‐0.19 [‐0.57, 0.19] |
2.1. Analysis.
Comparison 2 Low‐frequency TENS versus placebo, Outcome 1 Pain relief ‐ overall experience.
2.2. Analysis.
Comparison 2 Low‐frequency TENS versus placebo, Outcome 2 Pain relief ‐ 100pt VAS.
2.3. Analysis.
Comparison 2 Low‐frequency TENS versus placebo, Outcome 3 Pain relief ‐ descriptive data.
| Pain relief ‐ descriptive data | ||||
|---|---|---|---|---|
| Study | Pain scale used | LF TENS | Placebo | Conclusion |
| Placebo TENS | ||||
| Thomas 1995 | Total Pain measure on 100mm VAS 3 x day for 3 days Max score = 900 Pretreatment scores mean: 375 std dev: 157 | mean: 245 std dev: 187 n=12 | mean: 387 std dev: 167 n=12 | Low Frequency TENS is more effective at reducing pain than Placebo TENS (using ANOVA, p<0.05) |
| Placebo Pill | ||||
| Neighbors 1987 | Mean pain scores on 10cm VAS | mean: 0.54 std dev: 0.79 n: 10 range: 0.00‐2.00 | mean: 3.30 std dev: 2.451 n: 10 range: 0.2‐7.5 | Low frequency TENS is more effective at reducing pain than Placebo pill (using ANOVA, p<0.05) |
2.4. Analysis.
Comparison 2 Low‐frequency TENS versus placebo, Outcome 4 Adverse effects.
2.5. Analysis.
Comparison 2 Low‐frequency TENS versus placebo, Outcome 5 Use of additional analgesics (n of tablets taken).
2.6. Analysis.
Comparison 2 Low‐frequency TENS versus placebo, Outcome 6 Absence from work/school (lost hours).
Comparison 3. High‐frequency TENS versus low‐frequency TENS.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain relief ‐ overall experience | 1 | 42 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 3.86 [1.14, 13.04] |
| 2 Pain relief ‐ 100pt VAS | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | 20.89 [‐4.36, 46.14] |
| 3 Pain relief ‐ descriptive data | Other data | No numeric data | ||
| 4 Use of additional analgesics (n of tablets taken) | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 3.21 [0.50, 5.92] |
| 5 Absence from work/school (lost hours) | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 0.23 [‐0.15, 0.61] |
3.1. Analysis.
Comparison 3 High‐frequency TENS versus low‐frequency TENS, Outcome 1 Pain relief ‐ overall experience.
3.2. Analysis.
Comparison 3 High‐frequency TENS versus low‐frequency TENS, Outcome 2 Pain relief ‐ 100pt VAS.
3.3. Analysis.
Comparison 3 High‐frequency TENS versus low‐frequency TENS, Outcome 3 Pain relief ‐ descriptive data.
| Pain relief ‐ descriptive data | ||||
|---|---|---|---|---|
| Study | Pain scale used | HF TENS | LF TENS | Conclusion |
| Thomas 1995 | Total Pain on 100mm VAS scale ‐ measured 3 x day for 3 days ‐ Max score 900 Pretreatment score mean: 375 std dev: 157 | mean: 553 std dev: 128 n: 12 | mean: 245 std dev: 187 n: 12 | Low frequency TENS more likely to reduce pain than High frequency TENS (using ANOVA p<0.05) |
3.4. Analysis.
Comparison 3 High‐frequency TENS versus low‐frequency TENS, Outcome 4 Use of additional analgesics (n of tablets taken).
3.5. Analysis.
Comparison 3 High‐frequency TENS versus low‐frequency TENS, Outcome 5 Absence from work/school (lost hours).
Comparison 4. TENS versus medical treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain relief ‐ overall experience | 1 | 64 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.28 [0.10, 0.75] |
| 1.1 Ibuprofen | 1 | 64 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.28 [0.10, 0.75] |
| 2 Pain relief ‐ descriptive data | Other data | No numeric data | ||
| 2.1 Naproxen | Other data | No numeric data | ||
| 3 Adverse effects | 1 | 24 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 26.73 [5.46, 130.91] |
| 3.1 Naproxen | 1 | 24 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 26.73 [5.46, 130.91] |
| 4 Use of additional analgesics | 1 | 64 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.41 [0.12, 1.37] |
| 4.1 Ibuprofen | 1 | 64 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.41 [0.12, 1.37] |
4.1. Analysis.
Comparison 4 TENS versus medical treatment, Outcome 1 Pain relief ‐ overall experience.
4.2. Analysis.
Comparison 4 TENS versus medical treatment, Outcome 2 Pain relief ‐ descriptive data.
| Pain relief ‐ descriptive data | ||||
|---|---|---|---|---|
| Study | Pain scale | TENS | Medical treatment | Conclusions |
| Naproxen | ||||
| Milsom 1994 | Pain score 1‐5 measured every 30min up to 240min ‐ reported in graph form | High frequency high intensity TENS (unusual as usually low intensity) n=12 | One dose 500mg n=12 | No significant difference between the two treatments. Both groups had significantly reduced pain from baseline (p<.0001, using the Student t‐test) |
4.3. Analysis.
Comparison 4 TENS versus medical treatment, Outcome 3 Adverse effects.
4.4. Analysis.
Comparison 4 TENS versus medical treatment, Outcome 4 Use of additional analgesics.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Dawood 1990a.
| Methods | Randomised ‐ method unstated in published trial. Communication from author stated it was a centralised randomisation process Double blind ‐ for type of TENS intervention Crossover design 32 women randomised and analysed Communication from author states that intention‐to‐treat analysis and a power calculation were used however no details were provided | |
| Participants | Inclusion: severe primary dysmenorrhoea (diagnosed according to "predefined clinical criteria", regular cycles) Exclusion: OCP use Age: mean 28.5 (5.2) years Location: USA | |
| Interventions | 1. Ibuprofen 400 mg every 6 hrs for 3 days 2. High‐frequency TENS (conventional) ‐ 100 pulses/sec, 100 μsec pulse width, amplitude comfortable tingling 3. Placebo TENS Location: abdomen (portable unit) Duration: first 8hrs of cycle, then when needed for pain relief 5 cycles ‐ TENS 2 cycles, placebo TENS 1 cycle, ibuprofen 1 cycle (sequence random) | |
| Outcomes | Pain relief ‐ scale 1‐5 Menstrual symptom questionnaire Use of pain medication | |
| Notes | Author supplied some unpublished methodological information No information or baseline comparison on the groups pain characteristics | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | "..enrolled in a randomized crossover study" ‐ method unstated in published trial. |
| Allocation concealment? | Low risk | No details provided. Communication from author stated it was a centralised randomisation process. |
| Blinding? All outcomes | Low risk | Double blind ‐ for type of TENS intervention. "subjects and investigators were blinded as to the type of transcutaneous electrical nerve stimulator..." |
| Incomplete outcome data addressed? All outcomes | Low risk | All patients followed up, no apparent drop outs. |
| Free of selective reporting? | Low risk | All relevant outcomes reported. |
Lewers 1989.
| Methods | Random ‐ unstated in published trial. Correspondence with authors showed randomisation was done by flipping a coin for the first person and alternate assignment for other participants No blinding Parallel design 21 participants randomised and analysed (pain data estimated for two participants for last two recordings, 180min and next morning) | |
| Participants | Inclusion: primary dysmenorrhoea, pelvic exam in previous two years that showed no pathology Age: 20‐38, mean 25.9 years Location: USA | |
| Interventions | 1. Low‐frequency TENS ‐ low rate 1 pulse/sec, highest intensity tolerable, pulse duration low, 40 msec 2. Placebo pill Location: 4 points, bladder 21 and 29 (back), spleen 6 and stomach 36 (legs) Duration: 30 min, 1 cycle | |
| Outcomes | Pain scales ‐ VAS and the pain rating index from McGill measured pre, post, 30, 60, 120, 180 min, next morning upon awakening | |
| Notes | No information on the baseline similarities of the randomised groups Immediately after collection of baseline measurements all women received auricular acupressure, as part of another study prior to the intervention. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | High risk | "Subjects were assigned randomly". No further details in paper. Correspondence with authors showed randomisation was done by flipping a coin for the first person and alternate assignment for other participants. |
| Allocation concealment? | Unclear risk | No details provided. |
| Blinding? All outcomes | High risk | No blinding. |
| Incomplete outcome data addressed? All outcomes | Low risk | Two participants in the experimental group did not complete posttreatment measures as they were asleep and needing to take additional medication, therefore used last value carried forward. |
| Free of selective reporting? | Low risk | Main outcome measures were reported. |
Lundeberg 1985.
| Methods | Random ‐ method unstated Single blind, participant was blind but other unclear Crossover design 21 women randomised and analysed | |
| Participants | Inclusion: primary dysmenorrhoea, gynaecological exam to rule out pathology Age: average 22, 15‐29 years Location: Sweden | |
| Interventions | 1. High‐frequency TENS ‐ duration 0.2 msec, freq 100 Hz 2. Low‐frequency TENS ‐ duration 0.2 msec, freq 2 Hz 3. Placebo TENS Location: source of pain, lower back or abdomen Duration: 45 min treatment once every month On fourth month patient given treatment of choice and asked to compare with 500mg naproxen, fifth month asked to compare with 120mg verapamil (calcium‐channel blocker) | |
| Outcomes | Pain intensity VAS 0‐10 McGill pain questionnaire | |
| Notes | No difference in baseline scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | "Randomly assigned to one of three groups", no further details. |
| Allocation concealment? | Unclear risk | Unclear. |
| Blinding? All outcomes | Unclear risk | Single blind, participant was blind but other unclear. |
| Incomplete outcome data addressed? All outcomes | Low risk | All 21 patients were analysed. |
| Free of selective reporting? | Low risk | All major and relevant outcomes reported on. |
Mannheimer 1985.
| Methods | Random ‐ unstated Parallel design 27 women randomised | |
| Participants | Inclusion: dysmenorrhoea, abdominal pain, women who were not previous users of TENS Exclusion: OCP use, any precautions or contraindications to treatment, only lower back pain Age: 19‐27, mean 22.1 years Location: USA | |
| Interventions | 1. Conventional high‐freq TENS ‐ 50‐100 Hz, narrow pulse 40‐75 μsec, intensity produces no muscle contractions 2. Acupuncture‐like low‐frequency TENS ‐ 1‐4 Hz, pulse 100‐250 μsec, intensity to tolerance 3. Control ‐ placebo TENS Location: conventional and control used electrodes on abdomen, acupuncture‐like TENS used points spleen 6 and 10 (legs) Duration: 30 min ‐ until pain returned | |
| Outcomes | Pain ratings ‐ pre and post treatment Duration of pain relief | |
| Notes | No information on the baseline similarities of the randomised groups | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | "randomly assigned" no further details. |
| Allocation concealment? | Unclear risk | Unclear. |
| Blinding? All outcomes | High risk | No details of blinding. |
| Incomplete outcome data addressed? All outcomes | Low risk | All patients were analysed. |
| Free of selective reporting? | Low risk | All relevant outcomes were reported. |
Milsom 1994.
| Methods | Random ‐ unstated No blinding Crossover design 12 women randomised and analysed | |
| Participants | Inclusion: severe primary dysmenorrhoea, abdomen and back pain Exclusion: OCP, IUD, pelvic pathology on gynaecological exam Age: mean 23.8 (0.8) years Location: Sweden | |
| Interventions | 1. High frequency and intensity TENS ‐ 70‐100 Hz, 0.2 msec current/pulse duration, intensity 40‐50 mA 2. Naproxen ‐ single dose 500mg Location: electrodes placed on lower abdomen and back Duration: until pain free (2 cycles, one treatment per cycle) | |
| Outcomes | Pain score ‐ 1‐5 scale every 15 min for 240 min Uterine activity Side effects | |
| Notes | No difference in baseline scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | "randomised", no further details. |
| Allocation concealment? | Unclear risk | Unclear, no details. |
| Blinding? All outcomes | High risk | Open‐label study, no blinding. |
| Incomplete outcome data addressed? All outcomes | Low risk | All patients analysed. |
| Free of selective reporting? | Low risk | All relevant outcomes were reported. |
Neighbors 1987.
| Methods | Random ‐ unstated No blinding Parallel design, 20 women randomised and analysed | |
| Participants | Inclusion: dysmenorrhoea, pelvic exam in last two years that had shown no pelvic pathology Age: 19‐38 years Location: USA | |
| Interventions | 1. Low‐frequency TENS ‐ pulse width 40 msec, rate 1 pulse/sec, intensity 0 mA then increased to tolerance 2. Placebo pill Location: bladder 21 and 29 (back), spleen 6 and stomach 36 (legs) Duration: 30min | |
| Outcomes | Pain scales ‐ VAS and abbreviated McGill Measured pre, post, 30 min, 1 hr, 2 hr | |
| Notes | Check this is low frequency No difference in baseline scores | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | "randomly assigned" no further details. |
| Allocation concealment? | Unclear risk | Unclear, no details. |
| Blinding? All outcomes | High risk | No evidence of blinding. |
| Incomplete outcome data addressed? All outcomes | Low risk | All patients analysed. |
| Free of selective reporting? | Low risk | All relevant outcomes were reported. |
Thomas 1995.
| Methods | Not stated if random Blinding unclear Crossover design 31 women randomised, 29 analysed | |
| Participants | Inclusion: primary dysmenorrhoea, previous ineffective treatment with NSAIDs, contraindications to NSAIDs, gynaecological exam to rule out pathology, women with no previous use of TENS Age: mean 30.2 (7.3) years Location: Sweden | |
| Interventions | 7 treatments ‐ participants split into two groups: TENS or acupuncture Duration: 20 min treatment, 7 days and 3 days prior to onset of menstruation every month Acupuncture treatments: different mode each month for 4 months then preferred treatment for 5th month Location: 5 points, bladder 32 (back, bilateral), abdomen CV4, spleen 9 and 6 (legs) 1. manual stimulation at insertion, every 5 min 2. low‐frequency electrical stimulation at 2 Hz to evoke muscle contractions 3. high‐frequency 100 Hz, intensity adjusted to comfort level 4. periosteal stimulation (for 30 sec) 3 or 4 times for each point TENS treatments: 3 different modes for 3 months, patients preferred treatment for 4th month, pulse duration 0.2 msec Location: Thoracic 10 to Lumbar 1 1. Low‐frequency TENS, 2 Hz 2. High‐frequency TENS, 100 Hz 3. Placebo TENS | |
| Outcomes | Pain scale ‐ VAS Blood loss Nausea Hours of work lost Analgesics taken (no mention of type or dose) Subjective assessment | |
| Notes | No information on the baseline similarities of the randomised groups | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Adequate sequence generation? | Unclear risk | "randomised although serial order was maintained". |
| Allocation concealment? | Unclear risk | Unclear. |
| Blinding? All outcomes | Low risk | Participants were blinded. |
| Incomplete outcome data addressed? All outcomes | Low risk | All patients analysed. |
| Free of selective reporting? | Low risk | All relevant outcomes were reported. |
OCP: oral contraceptive pill
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Janke 1984 | The trial compared low‐frequency TENS with a control that was a mixture of high‐frequency TENS and placebo TENS. This combination did not clearly fit any of the intended comparisons of the review so the trial was excluded.
Methods: low‐frequency TENS, high‐frequency TENS, and placebo TENS
Participants were divided into two treatment groups. The experimental group received low‐frequency TENS to four acupuncture points bilaterally. Intensity of stimulation was adjusted to a level as intense as tolerable for 30 min (varied from 35‐70 amps). If the participant reached the maximum intensity and could take a stronger stimulation the pulse width was adjusted to a tolerable level for 30 min (varied from 40‐100 msec). The control group received high‐frequency TENS to four non‐acupuncture points close to the acupuncture points used in the experimental group, the intensity was adjusted to a just noticeable level. Electrodes were also placed on the same back points as those used for the experimental group but current was not delivered. Outcome assessment was the same for both treatment groups. Not stated if random No information on blinding Parallel design 20 participants, 10 in each group No drop outs Participants: Inclusion: self‐reported dysmenorrhoea, aged between 18‐40 years Exclusion: known pelvic pathology, other medical problems, use of NSAIDs or other pain medication 4 hr prior to treatment Age: mean 25.7, range 19‐40 years Location: Alabama, USA Source: volunteers from university area Interventions: 1. Experimental group acupuncture‐like (low rate) TENS over four acupuncture points bilaterally, intensity 0 mA initially (adjusted to a level as intense as tolerable between 35‐70 mA), pulse width 40 msec initially (adjusted to within 40‐100 msec as tolerable, rate 1pulse/sec 2. Control group of conventional TENs to 4 non‐acupuncture points, rate 40 pulses/sec width 100msec. Electrodes were also placed on 4 acupuncture points but no current delivered. Location: Acupuncture points Spleen 6, Stomach 36, Bladder 21, Bladder 29 were used for the experimental group. For the control electrodes were placed on B21 and B29 bilaterally but not stimulated. Two non‐acupuncture points on the leg near ST36 and SP6 were stimulated Duration: 30 min treatment while subject was experiencing dysmenorrhoea, for one cycle Outcomes: Pain scores ‐ VAS (0‐10 cm) and McGill Pain Rating Index (scores 1‐78) taken at baseline, 30, 60, 90, 150, 210 min after start of treatment. Raw data reported for each participant |
Characteristics of studies awaiting assessment [ordered by study ID]
Santiesteban 1985.
| Methods | Participants blinded Parallel design 8 women randomised and analysed |
| Participants | Inclusion: dysmenorrhoea Exclusion: any medication Age: average 22 years Location: USA |
| Interventions | 1. Low‐frequency TENS ‐ 5 Hz pulse rate, 250 μsec, pulse duration/intensity to patients tolerance 2. Sham (mock) TENS ‐ no intensity administered Duration: 30 min Location: Spleen 6, Gallbladder 34 (on legs) |
| Outcomes | Pain scale 1‐5 measured pre, post, 4 hrs, 24 hrs, 30 days Abdominal pain Back pain |
| Notes | No difference between the experimental and control group for pretreatment abdominal pain, however there was some difference for pretreatment back pain with the control group having a higher average pain rating |
Differences between protocol and review
The original review contained reference to acupuncture. The trial associated with acupuncture has now been removed from this review and the role of acupuncture in the treatment of dysmenorrhoea will be the subject of a new review.
Contributions of authors
Michelle Proctor: took the lead in writing the original protocol and review, performed initial searches of databases for trials, involved in selecting trials for inclusion, performed independent data extraction and quality assessment of the included trials, was responsible for statistical analysis and interpretation of the data. Caroline Smith: involved in selecting trials for inclusion, performed independent data extraction and quality assessment of the included trials, contributed to discussion and interpretation of results. Cindy Farquhar: initiated and conceptualised the review, commented on drafts of the protocol and review, and participated in the update of the review. Will Stones: commented on drafts of the protocol and review.
Julie Brown: took the lead in the update of the review and the formatting for Revman 5.
Sources of support
Internal sources
University of Auckland, School of Medicine, Auckland, New Zealand.
External sources
Princess of Wales Memorial Trust Fund administered by the Mercia Barnes Fund, New Zealand.
Declarations of interest
None known
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
Dawood 1990a {published data only}
- Dawood MY, Ramos J. Transcutaneous electrical nerve stimulation (TENS) for the treatment of primary dysmenorrhea: a randomized crossover comparison with placebo TENS and ibuprofen. Obstetrics and Gynecology 1990;75(4):656‐60. [PubMed] [Google Scholar]
Lewers 1989 {published data only}
- Lewers D, Clelland JA, Jacksin JR, Varner RE, Bergman J. Transcutaneous electrical nerve stimulation in the relief of primary dysmenorrhoea. Physical Therapy 1989;69(1):3‐9. [DOI] [PubMed] [Google Scholar]
Lundeberg 1985 {published data only}
- Lundeberg T, Bondesson L, Lundstrom V. Relief of primary dysmenorrhea by transcutaneous electrical nerve stimulation. Acta Obstetricia et Gynecologica Scandinavica 1985;64(6):491‐7. [DOI] [PubMed] [Google Scholar]
Mannheimer 1985 {published data only}
- Mannheimer JS, Whalen EC. The efficacy of transcutaneous electrical nerve stimulation in dysmenorrhea. Clinical Journal of Pain 1985;1(2):75‐83. [Google Scholar]
Milsom 1994 {published data only}
- Hedner N, Milsom I, Eliasson T, Mannheimer C. TENS is effective in painful menstruation [Tens bra vid smatsam mens]. Lakartidningen 1996;93(13):1219‐22. [PubMed] [Google Scholar]
- Milsom I, Hedner N, Mannheimer C. A comparative study of the effect of high intensity transcutaneous nerve stimulation and oral naproxen on intrauterine pressure and menstrual pain in patients with primary dysmenorrhea. American Journal of Obstetrics and Gynecology 1994;170(1):123‐9. [DOI] [PubMed] [Google Scholar]
Neighbors 1987 {published data only}
- Neighbors LE, Clelland J, Jacksin JR, Bergman J, Orr J. Transcutaneous electrical nerve stimulation for pain relief in primary dysmenorrhea. Clinical Journal of Pain 1987;3:17‐22. [Google Scholar]
Thomas 1995 {published data only}
- Thomas M, Lundeberg T, Bjork G, Lundstrom‐Lindstedt V. Pain and discomfort in primary dysmenorrhea is reduced by preemptive acupuncture or low frequency TENS. European Journal of Physical Medicine and Rehabilitation 1995;5(3):71‐6. [Google Scholar]
References to studies excluded from this review
Janke 1984 {published data only}
- Janke CL. Transcutaneous electrical nerve stimulation for pain relief in dysmenorrhoea [Master's thesis]. Birmingham, Alabama: University of Alabama in Birmingham, 1984. [Google Scholar]
References to studies awaiting assessment
Santiesteban 1985 {published data only}
- Santiesteban AJ, Burnham TL, George KL, Kita PJ, Mehring EA. Primary spasmodic dysmenorrhea: the use of TENS on acupuncture points. American Journal of Acupuncture 1985;13(1):35‐42. [Google Scholar]
Additional references
Carroll 1996
- Carroll D, Tramer M, McQuay H, Nye B, Moore A. Randomization is important in studies with pain outcomes: Systematic review of transcutaneous electrical nerve stimulation in acute postoperative pain. British Journal of Anaesthesia 1996;77:798‐803. [DOI] [PubMed] [Google Scholar]
Carroll 1997
- Carroll D, Moore RA, Tramr MR, McQuay HJ. Transcutaneous electrical nerve stimulation does not relieve labour pain: updated systematic review. Contemporary Reviews in Obstetrics and Gynecology 1997;Sept:195‐205. [Google Scholar]
Dawood 1984
- Dawood MY. Ibuprofen and dysmenorrhea. The American Journal of Medicine 1984;77(1A):87‐94. [DOI] [PubMed] [Google Scholar]
Dawood 1990b
- Dawood MY. Dysmenorrhea. Clinical Obstetrics and Gynecology 1990;33(1):168‐78. [DOI] [PubMed] [Google Scholar]
Gersh 1985
- Gersh MR, Wolf SL. Applications of transcutaneous electrical nerve stimulation in the management of patients with pain. State‐of‐the‐art update. Physical Therapy 1985;65(3):314‐36. [DOI] [PubMed] [Google Scholar]
Kaplan 1997
- Kaplan B, Rabinerson D, Pardo J, Krieser RU, Neri A. Transcutaneous electrical nerve stimulation (TENS) as a pain‐relief device in obstetrics and gynecology. Clinical and Experimental Obstetrics & Gynecology 1997;24(3):123‐6. [PubMed] [Google Scholar]
Lichten 1987
- Lichten EM, Bombard J. Surgical treatment of primary dysmenorrhea with laparoscopic uterine nerve ablation. The Journal of Reproductive Medicine 1987;32:37‐41. [PubMed] [Google Scholar]
McQuay 1998
- McQuay HJ, Moore RA. Transcutaneous electrical nerve stimulation (TENS) in chronic pain. An evidence‐based resource for pain relief. Oxford: Oxford University Press, 1998:Chapter 25. [Google Scholar]
Osiri 2001
- Osiri M, Welch V, Brosseau L, Shea B, McGowan J, Tugwell P, Wells G. Transcutaneous electrical nerve stimulation for knee osteoarthritis (Cochrane Review). Cochrane Database of Systematic Reviews 2001, Issue 1. [DOI: 10.1002/14651858.CD002823.] [DOI] [PubMed] [Google Scholar]
Punnonen 1980
- Punnonen RH, Nikkanen VP. Endometriosis in young women. Infertility 1980;3:1‐10. [Google Scholar]
Sheon 1984
- Sheon RP. Transcutaneous electrical nerve stimulation: From electric eels to electrodes. Postgraduate Medicine 1984;75(5):71‐4. [DOI] [PubMed] [Google Scholar]
Smith 1991
- Smith RP, Heltzel J. Interrelation of analgesia and uterine activity in women with primary dysmenorrhea: A preliminary report. The Journal of Reproductive Medicine 1991;36(4):260‐4. [PubMed] [Google Scholar]
References to other published versions of this review
Proctor 2002
- Proctor ML, Smith CA, Farquhar CM, Stones RW. Transcutaneous electrical nerve stimulation and acupuncture for primary dysmenorrhoea. Cochrane Database of Systematic Reviews 2002, Issue 1. [DOI: 10.1002/14651858] [DOI] [PMC free article] [PubMed] [Google Scholar]