

Key Points
Question
In patients with ST-segment elevation myocardial infarction (STEMI), is a concomitant diagnosis of COVID-19 associated with differences in clinical outcome?
Findings
In this retrospective cohort study that included 80 449 patients, the rates of in-hospital mortality for patients with vs without a concomitant diagnosis of COVID-19 were 15.2% vs 11.2% among those with out-of-hospital STEMI and 78.5% vs 46.1% among those with in-hospital STEMI; both differences were statistically significant.
Meaning
Among patients with STEMI, a concomitant diagnosis of COVID-19 was associated with significantly higher rates of in-hospital mortality.
Abstract
Importance
There has been limited research on patients with ST-segment elevation myocardial infarction (STEMI) and COVID-19.
Objective
To compare characteristics, treatment, and outcomes of patients with STEMI with vs without COVID-19 infection.
Design, Setting, and Participants
Retrospective cohort study of consecutive adult patients admitted between January 2019 and December 2020 (end of follow-up in January 2021) with out-of-hospital or in-hospital STEMI at 509 US centers in the Vizient Clinical Database (N = 80 449).
Exposures
Active COVID-19 infection present during the same encounter.
Main Outcomes and Measures
The primary outcome was in-hospital mortality. Patients were propensity matched on the likelihood of COVID-19 diagnosis. In the main analysis, patients with COVID-19 were compared with those without COVID-19 during the previous calendar year.
Results
The out-of-hospital STEMI group included 76 434 patients (551 with COVID-19 vs 2755 without COVID-19 after matching) from 370 centers (64.1% aged 51-74 years; 70.3% men). The in-hospital STEMI group included 4015 patients (252 with COVID-19 vs 756 without COVID-19 after matching) from 353 centers (58.3% aged 51-74 years; 60.7% men). In patients with out-of-hospital STEMI, there was no significant difference in the likelihood of undergoing primary percutaneous coronary intervention by COVID-19 status; patients with in-hospital STEMI and COVID-19 were significantly less likely to undergo invasive diagnostic or therapeutic coronary procedures than those without COVID-19. Among patients with out-of-hospital STEMI and COVID-19 vs out-of-hospital STEMI without COVID-19, the rates of in-hospital mortality were 15.2% vs 11.2% (absolute difference, 4.1% [95% CI, 1.1%-7.0%]; P = .007). Among patients with in-hospital STEMI and COVID-19 vs in-hospital STEMI without COVID-19, the rates of in-hospital mortality were 78.5% vs 46.1% (absolute difference, 32.4% [95% CI, 29.0%-35.9%]; P < .001).
Conclusions and Relevance
Among patients with out-of-hospital or in-hospital STEMI, a concomitant diagnosis of COVID-19 was significantly associated with higher rates of in-hospital mortality compared with patients without a diagnosis of COVID-19 from the past year. Further research is required to understand the potential mechanisms underlying this association.
This cohort study examines the association between COVID-19 and ST-segment elevation myocardial infarction (STEMI) outcome in a large, nationally representative patient cohort who presented with out-of-hospital STEMI or developed STEMI while hospitalized.
Introduction
The COVID-19 pandemic has negatively affected the care of patients with ST-segment elevation myocardial infarction (STEMI). The number of patients presenting with STEMI declined substantially during pandemic surges,1,2 reperfusion strategies were modified,3,4 and delays in reperfusion were observed around the world.3,4,5 Poorer STEMI-related outcomes have been reported throughout the pandemic, including higher rates of in-hospital mortality.3,5 Whether these outcomes have been the result of pandemic-related factors or SARS-CoV-2 infection is unclear. Data from relatively small cohort studies suggest that outcomes following out-of-hospital STEMI may be worse among those with COVID-19 than among those without COVID-19,6,7,8 but few broadly representative data exist. Few data characterizing acute in-hospital STEMI among patients hospitalized with COVID-19 exist.9,10
To better understand the association between COVID-19 and STEMI outcome in a large, nationally representative patient cohort, the present study used a multicenter clinical database to assess patients with COVID-19 vs those without COVID-19 who presented with out-of-hospital STEMI or developed STEMI while hospitalized. To differentiate between the direct- and pandemic-related association between COVID-19 and clinical outcome, separate control patients from the same year and the past year were used when comparing patients with vs without a COVID-19 diagnosis.
Methods
Study Approval
This study was deemed exempt from the requirements of 45 CFR 46.104(d) by The Miriam Hospital Institutional Review Board given that it involved deidentified data.
Data Source
The Vizient Clinical Database gathers demographic, comorbid, clinical outcome, resource, cost, and readmission data from patients hospitalized at each of its 757 US academic medical centers and affiliated hospitals in 50 states. The distribution of admissions in these centers in 2020 was as follows: 28% from the Midwest, 24.6% from the Northeast, 31.2% from the South, and 16.1% from the West. All data were deidentified prior to extraction.
Study Population
Patients who were hospitalized with STEMI at a percutaneous coronary intervention (PCI)–capable center between January 1, 2019, and December 31, 2020, were included. Patients who presented to non–PCI-capable centers may have entered the analysis if they were subsequently transferred to a PCI-capable center. Exclusion criteria appear in Figure 1. Patients who were transferred into or out from the index hospital were not excluded from the main analyses. Deidentified data do not include individual patient age, so mean/median age could not be calculated, but age is reported as age groupings. Race and ethnicity were included among patient baseline characteristics because both are associated with outcomes in patients with STEMI and COVID-19 infection.11,12 Fixed race and ethnicity categories exist in the database and are determined at each hospital by patient self-report. STEMI diagnosis, comorbidities, and treatments rendered were ascertained using International Classification of Diseases, Tenth Revision (ICD-10) diagnostic and procedure codes (eTable 1 in the Supplement). Prior validation literature for the utilized ICD-10 codes is provided in the eMethods in the Supplement. The Centers for Medicare & Medicaid Services’ “present on admission” indicator was used to differentiate preexisting from incident conditions.13 The Elixhauser comorbidity score incorporates 30 comorbid conditions, with higher scores reflecting greater risk of in-hospital mortality14; the score was determined for each patient in the database and provided for this analysis (eMethods in the Supplement).
Figure 1. Study Flow and Matching of Patients With ST-Segment Elevation Myocardial Infarction (STEMI) With or Without COVID-19.
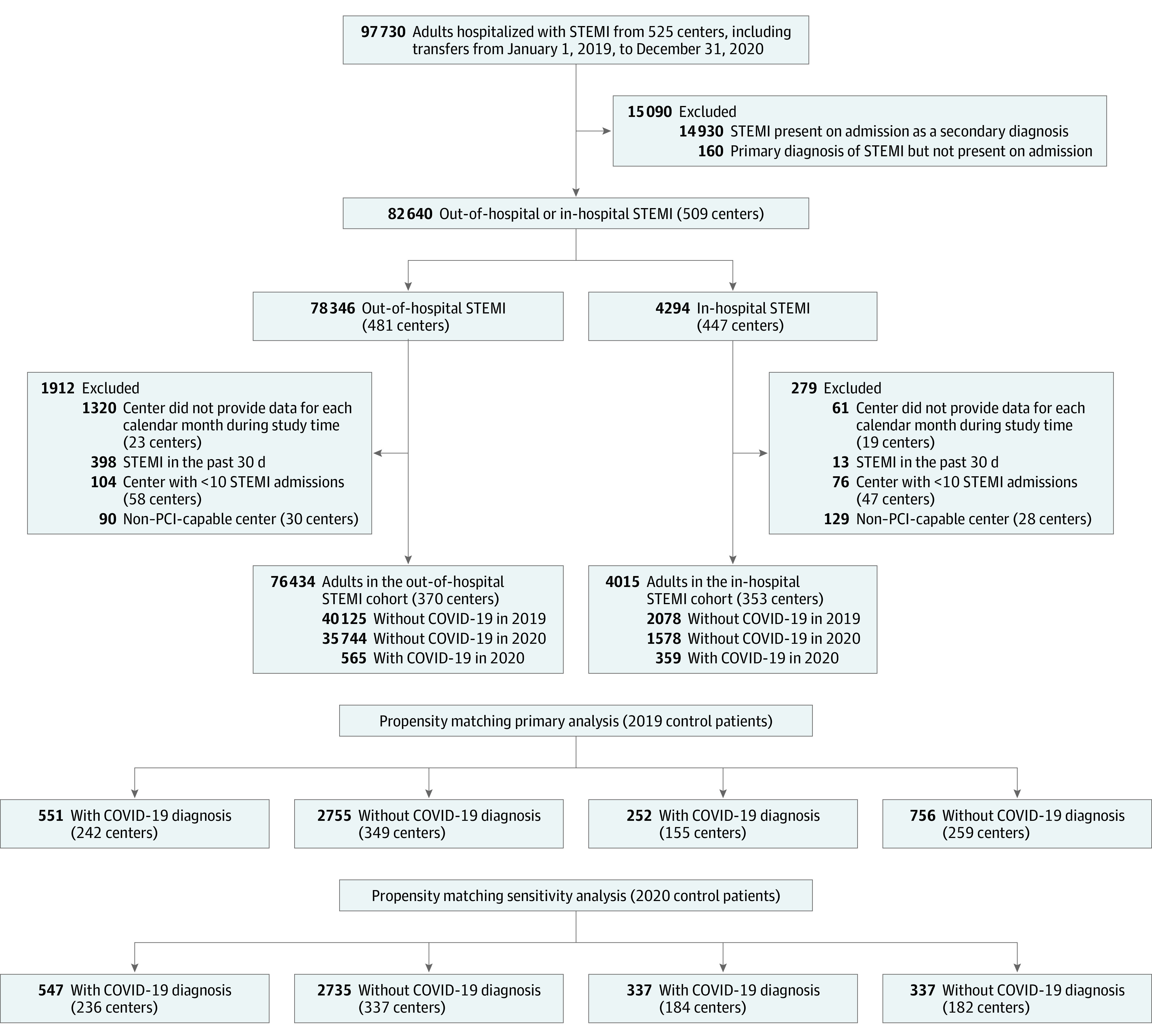
Out-of-hospital STEMI was defined through International Classification of Diseases, Tenth Revision coding (see eTable 1 in the Supplement) as being both present on admission and the primary diagnosis, while in-hospital STEMI was defined as nonprimary diagnosis coding and not present on admission. Patients in whom these were mixed (eg, STEMI present on admission but not the primary diagnosis) were excluded. Patients who presented to centers not capable of percutaneous coronary intervention (PCI), and were therefore excluded, may have entered the analysis if they subsequently transferred to a PCI-capable center.
Two nonoverlapping study groups were defined. Both included consecutive patients 18 years or older. The first group (out-of-hospital group) included those in whom STEMI was present on admission, defined by both a principal diagnosis of STEMI and a STEMI present on admission indicator (“Y”). The second group (in-hospital group) included those who experienced STEMI during hospitalization, defined by a diagnosis of STEMI that was neither the principal diagnosis nor present on admission.
Exposure
Active COVID-19 infection was defined as presence of the ICD-10 code U071 during the same encounter.
Outcomes
The primary outcome of interest was all-cause in-hospital mortality. Secondary outcomes included in-hospital composite death, recurrent MI or stroke, composite death or stroke, new acute decompensated heart failure, and cardiogenic shock. In-hospital exploratory outcomes included mechanical complications, bleeding, blood transfusion, acute kidney injury, need for mechanical ventilation, encephalopathy, septic shock, pneumonitis, acute respiratory failure, length of stay (overall and intensive care unit), hospitalization cost, and discharge disposition. The only postdischarge outcome available was 30-day readmission. Outcomes defined using ICD-10 codes appear in eTable 1 in the Supplement.
Statistical Analysis
Continuous variables are presented as mean and SD values or median and interquartile range values, depending on their distribution, and were compared using t tests and Wilcoxon rank-sum tests, respectively. Categorical variables are presented as frequencies and percentages and were compared using χ2 tests. Multivariable logistic regression incorporating demographic, clinical, and facility characteristics was used to develop a propensity score on which those without COVID-19 were matched to those with COVID-19. Only main effects were entered in the models. A full list of variables included in the propensity models appear in the eMethods in the Supplement. To maximize group size, matching was performed at 5:1 for the out-of-hospital group and 3:1 for the in-hospital group. Nearest-neighbor matching with a caliper width of 0.2 times the pooled SD of the logit was used15; in the out-of-hospital group, patients were matched within 4 weeks of the admission date to account for potential seasonal variation. Standardized differences were used to assess the effectiveness of the match, with values less than 10% suggesting well-balanced groups on a given covariate. In the main analyses, patients with out-of-hospital or in-hospital STEMI and COVID-19 were compared with those with STEMI without COVID-19 during the same months of the previous calendar year; the rationale for selecting the comparison group from the past year was to try to remove the influence of pandemic-related factors from the analysis. A 2-sided P value <.05 was considered statistically significant. To maximize the number of eligible patients available for matching, simple imputation was used for variables with missing data, using the most frequently observed category among those with nonmissing values (eResults in the Supplement). Because of the potential for type I error due to multiple comparisons, findings of analyses of secondary end points should be interpreted as exploratory. All analyses were performed with SAS, version 9.4 (SAS Institute).
Sensitivity analyses for the primary end point were conducted separately in the out-of-hospital and in-hospital STEMI group, each comparing patients with a COVID-19 diagnosis to propensity-matched patients without a COVID-19 diagnosis. First, the control group comprised patients admitted during the same (rather than previous) calendar year; the rationale for doing so was to incorporate secular factors (eg, differences in hospital resource availability during the pandemic) as well as the pathophysiological effect of COVID-19 on outcomes after STEMI. Second, the control group patients were matched to the exposed group on center. Third, patients who were transferred from one hospital to another were excluded. Fourth, multivariable regression was used following propensity-score matching to generate the least biased and most efficient estimates possible. Variables included in multivariable regression analysis are summarized in the eMethods in the Supplement.
Results
Among 97 730 patients hospitalized with STEMI at 525 centers during the study period, 82 640 from 509 centers met the study definition of out-of-hospital (n = 78 346; 481 centers) or in-hospital (n = 4294; 447 centers) STEMI. After applying exclusion criteria, the final out-of-hospital STEMI group included 76 434 patients and the in-hospital STEMI group included 4015 patients (Figure 1; Table 1 and Table 2). Of 20 variables used for propensity matching and multivariable regression, only 6 (all categorical) had missing data (eResults in the Supplement).
Table 1. Demographic, Clinical, and Treatment Characteristics in Unmatched and Propensity-Matched Patients With Out-of-Hospital STEMIa.
| Characteristic | Unmatched groups | Propensity-matched groups | ||||
|---|---|---|---|---|---|---|
| Patients, No. (%) | Standardized difference | Patients, No. (%) | Standardized difference | |||
| With COVID-19 (n = 565) | Without COVID-19 (n = 75 869) | With COVID-19 (n = 551) | Without COVID-19 (n = 2755) | |||
| Patient demographics | ||||||
| Age, y | .09 | .05 | ||||
| 31-50 | 90 (15.9) | 12 049 (15.9) | 86 (15.6) | 446 (16.2) | ||
| 51-64 | 208 (36.8) | 29 371 (38.7) | 206 (37.4) | 997 (36.2) | ||
| 65-74 | 158 (28.0) | 19 262 (25.4) | 152 (27.6) | 774 (28.1) | ||
| 75-79 | 49 (8.7) | 6110 (8.1) | 48 (8.7) | 261 (9.5) | ||
| 80-84 | 27 (4.8) | 4260 (5.6) | 27 (4.9) | 126 (4.6) | ||
| 85-89 | 16 (2.8) | 2866 (3.8) | 15 (2.7) | 80 (2.9) | ||
| ≥90 | 17 (3.0) | 1951 (2.6) | 17 (3.1) | 71 (2.6) | ||
| Sex | .008 | .01 | ||||
| Men | 395 (69.9) | 53 321 (70.3) | 385 (69.9) | 1939 (70.4) | ||
| Women | 170 (30.1) | 22 548 (29.7) | 166 (30.1) | 816 (29.6) | ||
| Raceb | (n = 537) | (n = 73 836) | .33 | (n = 551) | (n = 2755) | .09 |
| Asian | 16 (3.0) | 2264 (3.1) | 16 (2.9) | 111 (4.0) | ||
| Black | 90 (16.8) | 8447 (11.4) | 85 (15.4) | 428 (15.5) | ||
| White | 335 (62.4) | 56 369 (76.3) | 354 (64.2) | 1781 (64.6) | ||
| Other | 96 (17.8) | 6756 (9.1) | 96 (17.4) | 435 (15.8) | ||
| Hispanic ethnicityb | 109 (21.8) | 5508 (8.0) | .39 | 108 (19.6) | 546 (19.8) | .005 |
| Admission source | .19 | .23 | ||||
| Non–health care facilityc | 374 (66.2) | 51 391 (67.7) | 366 (66.4) | 1919 (69.7) | ||
| Transfer from another facility | 136 (24.1) | 17 766 (23.4) | 135 (24.5) | 594 (21.6) | ||
| Transfer from a skilled nursing facility or intermediate care facility | 32 (5.7) | 1963 (2.6) | 29 (5.3) | 59 (2.1) | ||
| Clinic referral | 15 (2.7) | 3854 (5.1) | 14 (2.5) | 143 (5.2) | ||
| Law enforcement/court, other transfer, or not availabled | 8 (1.4) | 895 (1.2) | 7 (1.3) | 40 (1.5) | ||
| Payer | .19 | .02 | ||||
| Medicare | 230 (40.7) | 33 687 (44.4) | 223 (40.5) | 1131 (41.1) | ||
| Private | 168 (29.7) | 25 693 (33.9) | 164 (29.8) | 801 (29.1) | ||
| Medicaid | 97 (17.2) | 8745 (11.5) | 96 (17.4) | 480 (17.4) | ||
| Othere | 70 (12.4) | 7744 (10.2) | 68 (12.3) | 343 (12.5) | ||
| Cardiovascular comorbidities | ||||||
| Prior coronary artery disease | 485 (85.8) | 67 334 (88.8) | .09 | 472 (85.7) | 2408 (87.4) | .05 |
| Hypertension | 447 (79.1) | 56 726 (74.8) | .10 | 435 (78.9) | 2207 (80.1) | .03 |
| Hyperlipidemia | 373 (66.0) | 50 956 (67.2) | .02 | 364 (66.1) | 1845 (67.0) | .02 |
| Diabetes | 271 (48.0) | 25 712 (33.9) | .29 | 263 (47.7) | 1345 (48.8) | .02 |
| Obesity | 144 (25.5) | 16 287 (21.5) | .09 | 140 (25.4) | 721 (26.2) | .02 |
| Heart failure on admission | 99 (17.5) | 14 928 (19.7) | .06 | 93 (16.9) | 460 (16.7) | .005 |
| Smoking | 90 (15.9) | 24 009 (31.6) | .38 | 89 (16.2) | 451 (16.4) | .006 |
| Cardiac arrest on admission | 58 (10.3) | 5162 (6.8) | .12 | 56 (10.2) | 254 (9.2) | .03 |
| Cerebrovascular disease | 40 (7.1) | 4068 (5.4) | .07 | 39 (7.1) | 189 (6.9) | .009 |
| Prior stroke | 38 (6.7) | 4653 (6.1) | .02 | 34 (6.2) | 223 (8.1) | .08 |
| Valvular heart disease | 30 (5.3) | 4957 (6.5) | .05 | 30 (5.4) | 136 (4.9) | .02 |
| Prior CABG | 17 (3.0) | 2996 (3.9) | .05 | 15 (2.7) | 72 (2.6) | .007 |
| Prior coronary intervention | 4 (0.7) | 874 (1.2) | .05 | 3 (0.5) | 31 (1.1) | .06 |
| Prior myocardial infarction | 1 (0.2) | 120 (0.2) | .005 | 0 | 2 (0.1) | .04 |
| Other comorbidities | ||||||
| Chronic anemia | 146 (25.8) | 14 722 (19.4) | .15 | 140 (25.4) | 701 (25.4) | .001 |
| Chronic kidney disease | 117 (20.7) | 11 924 (15.7) | .13 | 111 (20.1) | 561 (20.4) | .005 |
| Coagulopathy | 79 (14.0) | 6381 (8.4) | .18 | 75 (13.6) | 355 (12.9) | .02 |
| COPD | 66 (11.7) | 11 300 (14.9) | .09 | 64 (11.6) | 315 (11.4) | .06 |
| Chronic liver disease | 40 (7.1) | 5542 (7.3) | .009 | 38 (6.9) | 198 (7.2) | .01 |
| Pulmonary circulation disorder | 24 (4.2) | 2950 (3.9) | .02 | 22 (4.0) | 105 (3.8) | .009 |
| End-stage kidney disease | 19 (3.4) | 1347 (1.8) | .01 | 18 (3.3) | 87 (3.2) | .006 |
| Elixhauser comorbidity score, median (IQR)f | 2.0 (1.0-3.0) | 1.0 (1.0-3.0) | .19 | 2.0 (1.0-3.0) | 2.0 (1.0-3.0) | .001 |
| Facility characteristics | ||||||
| Beds | .07 | .02 | ||||
| 0-150 | 127 (23.0) | 16 741 (22.7) | 126 (22.9) | 619 (22.5) | ||
| 151-250 | 42 (7.6) | 6949 (9.4) | 42 (7.6) | 203 (7.4) | ||
| 251-500 | 112 (20.3) | 15 468 (20.9) | 112 (20.3) | 568 (20.6) | ||
| >500 | 271 (49.1) | 34 699 (47.0) | 271 (49.2) | 1365 (49.5) | ||
| Urbang | 539 (97.6) | 71 611 (97.0) | .04 | 538 (97.6) | 2682 (97.4) | .02 |
| Region | .23 | .03 | ||||
| Midwest | 177 (33.8) | 22 138 (31.0) | 176 (31.9) | 855 (31.0) | ||
| Northeast | 164 (31.4) | 21 157 (29.6) | 193 (35.0) | 961 (34.9) | ||
| Southeast | 71 (13.6) | 15 140 (21.2) | 71 (12.9) | 378 (13.7) | ||
| Southwest | 57 (10.9) | 5100 (7.1) | 57 (10.3) | 290 (10.5) | ||
| West | 54 (10.3) | 7897 (11.1) | 54 (9.8) | 271 (9.8) | ||
| Ownershiph | .04 | .02 | ||||
| Voluntary | 449 (81.3) | 59 693 (80.8) | 448 (81.3) | 2265 (82.2) | ||
| Governmental | 86 (15.6) | 11 416 (15.5) | 86 (15.6) | 408 (14.8) | ||
| Proprietary | 17 (3.1) | 2748 (3.7) | 17 (3.1) | 82 (3.0) | ||
| No. of patients with STEMI treated per year, mean | .16 | .02 | ||||
| ≤50 | 37 (6.5) | 2822 (3.7) | 35 (6.4) | 169 (6.1) | ||
| 51-99 | 89 (15.8) | 11 873 (15.6) | 84 (15.2) | 413 (15.0) | ||
| 100-149 | 135 (23.9) | 15 822 (20.9) | 130 (23.6) | 634 (23.0) | ||
| 150-199 | 91 (16.1) | 13 323 (17.6) | 91 (16.5) | 469 (17.0) | ||
| ≥200 | 213 (37.7) | 32 029 (42.2) | 211 (38.3) | 1070 (38.8) | ||
| Hospital occupancy at time of admission, median (IQR), % | 70 (60-90) | 80 (70-90) | .10 | 70 (60-90) | 80 (70-90) | .15 |
| ICU occupancy, median (IQR) | 80 (60-100) | 80 (60-90) | .02 | 80 (60-100) | 80 (60-90) | .14 |
| ICU typei | .37 | .05 | ||||
| Medical ICU | 158 (28.0) | 15 135 (19.9) | 154 (27.9) | 748 (27.2) | ||
| CCU | 140 (24.8) | 29 827 (39.3) | 140 (25.4) | 747 (27.1) | ||
| Other ICU | 63 (11.2) | 4590 (6.0) | 61 (11.1) | 288 (10.5) | ||
| Other step-down | 28 (5.0) | 4984 (6.6) | 22 (4.0) | 98 (3.6) | ||
| Cardiac step-down | 19 (3.4) | 2246 (3.0) | 19 (3.4) | 96 (3.5) | ||
| Other | 157 (27.8) | 19 087 (25.2) | 61 (11.1) | 778 (28.2) | ||
| Treatment characteristics | ||||||
| Coronary angiography | 463 (81.9) | 65 392 (86.2) | .12 | 451 (81.9) | 2263 (82.1) | .008 |
| PCI | ||||||
| Any | 451 (79.8) | 62 063 (81.8) | .05 | 440 (79.9) | 2131 (77.4) | .06 |
| Primaryj | 401 (71.0) | 56 344 (74.3) | .07 | 390 (70.8) | 1918 (69.6) | .03 |
| CABG | 20 (3.5) | 3977 (5.2) | .08 | 20 (3.6) | 189 (6.9) | .15 |
| Fibrinolytics only | 11 (1.9) | 156 (0.2) | .17 | 11 (2.0) | 6 (0.2) | .17 |
| Mechanical circulatory support | 62 (11.0) | 7681 (10.1) | .03 | 61 (11.1) | 304 (11.0) | .001 |
| Intra-aortic balloon pump | 57 (10.1) | 6817 (9.0) | .04 | 56 (10.2) | 259 (9.4) | .03 |
| LVAD | 22 (3.9) | 2462 (3.2) | .04 | 22 (4.0) | 108 (3.9) | .004 |
| ECMO | 8 (1.4) | 1252 (1.7) | .02 | 8 (1.5) | 64 (2.3) | .06 |
Abbreviations: CABG, coronary artery bypass grafting; CCU, cardiac care unit; COPD, chronic obstructive pulmonary disease; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; LVAD, left ventricular assist device; PCI, percutaneous coronary intervention.
Out-of-hospital ST-segment elevation myocardial infarction (STEMI) was defined through International Classification of Diseases, Tenth Revision coding (see eTable 1 in the Supplement) as both present on admission and the primary diagnosis. Not all variables in the table were included in the propensity-score matching. A list of these variables is presented in the eMethods in the Supplement.
Race and ethnicity were determined at the hospital level. Other indicates American Indian or Alaska Native and Native Hawaiian or Other Pacific Islander.
Non–health care facility indicates physician referral of a patient from home, the workplace, or a physician’s office.
Law enforcement/court refers to transfers of incarcerated individuals.
Other includes government-assisted health care, military, auto insurance, workers’ compensation, research, Title V maternal and child health, county medically indigent service, charity, self-pay/uninsured, self-pay cash in full, other, and unknown.
The database provides the Elixhauser score for every patient. The score sums the presence of 30 comorbid conditions, with higher scores reflecting greater risk of in-hospital mortality.
Urban defined as core-based statistical area that encompasses at least 2500 people, at least 1500 of whom reside outside institutional group quarters.
Proprietary ownership indicates for-profit institutions. Voluntary ownership indicates nonprofit institutions.
Intensive care unit type provided by Vizient Clinical Database. Categories were collapsed for simplification. For more details see eMethods in the Supplement.
Primary percutaneous coronary intervention indicates coronary angioplasty/stenting performed in the setting of STEMI without prior administration of fibrinolytic agents.
Table 2. Demographic, Clinical, and Treatment Characteristics in Unmatched and Propensity-Matched Patients With In-Hospital STEMIa.
| Characteristic | Unmatched groups | Propensity-matched groups | ||||
|---|---|---|---|---|---|---|
| Patients, No. (%) | Standardized difference | Patients, No. (%) | Standardized difference | |||
| With COVID-19 (n = 359) | Without COVID-19 (n = 3656) | With COVID-19 (n = 252) | Without COVID-19 (n = 756) | |||
| Patient demographics | ||||||
| Age, y | .11 | .11 | ||||
| 31-50 | 34 (9.5) | 369 (10.1) | 27 (10.7) | 78 (10.3) | ||
| 51-64 | 105 (29.2) | 1062 (29.0) | 66 (26.2) | 212 (28.0) | ||
| 65-74 | 96 (26.7) | 1075 (29.4) | 72 (28.6) | 203 (26.9) | ||
| 75-79 | 55 (15.3) | 448 (12.3) | 38 (15.1) | 94 (12.4) | ||
| 80-84 | 29 (8.1) | 330 (9.0) | 21 (8.3) | 77 (10.2) | ||
| 85-89 | 25 (7.0) | 227 (6.2) | 18 (7.1) | 61 (8.1) | ||
| ≥90 | 15 (4.2) | 145 (4.0) | 10 (4.0) | 31 (4.1) | ||
| Sex | .24 | .06 | ||||
| Men | 255 (71.0) | 2182 (59.7) | 168 (66.7) | 484 (64.0) | ||
| Women | 104 (29.0) | 1474 (40.3) | 84 (33.3) | 272 (36.0) | ||
| Raceb | (n = 353) | (n = 3583) | .48 | .13 | ||
| Asian | 24 (6.8) | 101 (2.8) | 16 (6.3) | 29 (3.8) | ||
| Black | 74 (21.0) | 578 (16.1) | 51 (20.2) | 138 (18.3) | ||
| White | 183 (51.8) | 2606 (72.7) | 159 (63.1) | 502 (66.4) | ||
| Other | 72 (20.3) | 298 (8.3) | 26 (10.3) | 87 (11.5) | ||
| Hispanic ethnicityb | 71 (21.7) | 225 (6.8) | .44 | 26 (10.3) | 65 (8.6) | .06 |
| Admission source | .35 | .31 | ||||
| Non–health care facilityc | 249 (69.4) | 2285 (62.5) | 168 (66.7) | 483 (63.9) | ||
| Transfer from another facility | 67 (18.7) | 761 (20.8) | 52 (20.6) | 149 (19.7) | ||
| Transfer from skilled nursing facility or intermediate care facility | 27 (7.5) | 139 (3.8) | 18 (7.1) | 24 (3.2) | ||
| Clinic referral | 13 (3.6) | 433 (11.8) | 12 (4.8) | 89 (11.8) | ||
| Law enforcement/court, other transfer, or not availabled | 3 (0.8) | 38 (1.0) | 2 (0.8) | 11 (1.5) | ||
| Payer | .13 | .07 | ||||
| Medicare | 208 (57.9) | 2316 (63.3) | 156 (61.9) | 459 (60.7) | ||
| Private | 73 (20.3) | 715 (19.6) | 46 (18.3) | 154 (20.4) | ||
| Medicaid | 48 (13.4) | 398 (10.9) | 34 (13.5) | 90 (11.9) | ||
| Othere | 30 (8.4) | 227 (6.2) | 16 (6.3) | 53 (7.0) | ||
| Cardiac comorbidities | ||||||
| Hypertension | 289 (80.5) | 3073 (84.1) | .09 | 207 (82.1) | 608 (80.4) | .04 |
| Hyperlipidemia | 204 (56.8) | 2199 (60.1) | .07 | 150 (59.5) | 431 (57.0) | .05 |
| Diabetes | 179 (49.9) | 1583 (43.3) | .13 | 123 (48.8) | 339 (44.8) | .08 |
| Prior coronary artery disease | 177 (49.3) | 2617 (71.6) | .47 | 152 (60.3) | 460 (60.8) | .01 |
| Obesity | 106 (29.5) | 849 (23.2) | .14 | 66 (26.2) | 183 (24.2) | .05 |
| Cardiac arrest on admission | 94 (26.2) | 598 (16.4) | .24 | 56 (22.2) | 142 (18.8) | .09 |
| Heart failure on admission | 63 (17.5) | 1052 (28.8) | .27 | 52 (20.6) | 168 (22.2) | .04 |
| Cerebrovascular disease | 58 (16.2) | 786 (21.5) | .14 | 48 (19.0) | 131 (17.3) | .05 |
| Prior stroke | 37 (10.3) | 442 (12.1) | .06 | 30 (11.9) | 81 (10.7) | .04 |
| Prior CABG | 28 (7.8) | 315 (8.6) | .03 | 24 (9.5) | 76 (10.1) | .019 |
| Smoking | 21 (5.8) | 662 (18.1) | .38 | 21 (8.3) | 62 (8.2) | .005 |
| Valvular heart disease | 20 (5.6) | 502 (13.7) | .28 | 18 (7.1) | 53 (7.0) | .005 |
| Prior coronary intervention | 6 (1.7) | 64 (1.8) | .006 | 3 (1.2) | 12 (1.6) | .03 |
| Prior myocardial infarction | 0 | 22 (0.6) | .11 | 0 | 6 (0.8) | .13 |
| Other comorbidities | ||||||
| Chronic anemia | 188 (52.4) | 2336 (63.9) | .24 | 148 (58.7) | 448 (59.3) | .01 |
| Coagulopathy | 144 (40.1) | 1143 (31.3) | .019 | 84 (33.3) | 241 (31.9) | .03 |
| Chronic kidney disease | 119 (33.1) | 1324 (36.2) | .06 | 92 (36.5) | 264 (34.9) | .03 |
| COPD | 85 (23.7) | 975 (26.7) | .07 | 70 (27.8) | 199 (26.3) | .03 |
| Chronic liver disease | 56 (15.6) | 680 (18.6) | .08 | 40 (15.9) | 130 (17.2) | .04 |
| Pulmonary circulation disorder | 47 (13.1) | 613 (16.8) | .10 | 35 (13.9) | 112 (14.8) | .03 |
| End-stage kidney disease | 19 (5.3) | 345 (9.4) | .16 | 17 (6.7) | 53 (7.0) | .01 |
| Elixhauser comorbidity score, median (IQR)f | 4.0 (3.0-6.0) | 4.0 (2.0-6.0) | .06 | 4.0 (3.0-6.0) | 4.0 (3.0-6.0) | .09 |
| Facility characteristics | ||||||
| Beds | .21 | .06 | ||||
| 0-150 | 74 (20.6) | 569 (15.6) | 47 (18.7) | 138 (18.3) | ||
| 151-250 | 35 (9.7) | 217 (5.9) | 24 (9.5) | 60 (7.9) | ||
| 251-500 | 54 (15.0) | 631 (17.3) | 43 (17.1) | 133 (17.6) | ||
| >500 | 196 (54.6) | 2239 (61.2) | 138 (54.8) | 425 (56.2) | ||
| Urbang | 353 (98.3) | 3598 (98.4) | .007 | 247 (98.0) | 743 (98.3) | .02 |
| Region | .18 | .12 | ||||
| Northeast | 126 (35.1) | 1179 (32.2) | 81 (32.1) | 221 (29.2) | ||
| Midwest | 85 (23.7) | 1043 (28.5) | 71 (28.2) | 215 (28.4) | ||
| Southeast | 71 (19.8) | 789 (21.6) | 52 (20.6) | 168 (22.2) | ||
| Southwest | 41 (11.4) | 267 (7.3) | 24 (9.5) | 59 (7.8) | ||
| West | 36 (10.0) | 378 (10.3) | 24 (9.5) | 93 (12.3) | ||
| Ownershiph | .04 | .06 | ||||
| Voluntary | 261 (74.8) | 2701 (75.7) | 192 (76.2) | 569 (75.3) | ||
| Governmental | 76 (21.8) | 765 (21.4) | 54 (21.4) | 162 (21.4) | ||
| Proprietary | 12 (3.4) | 102 (2.9) | 6 (2.4) | 25 (3.3) | ||
| No. of patients with STEMI treated per year, mean | .27 | .04 | ||||
| ≤50 | 21 (5.8) | 112 (3.1) | 9 (3.6) | 27 (3.6) | ||
| 51-99 | 81 (22.6) | 526 (14.4) | 47 (18.7) | 133 (17.6) | ||
| 100-149 | 74 (20.6) | 800 (21.9) | 56 (22.2) | 162 (21.4) | ||
| 150-199 | 61 (17.0) | 677 (18.5) | 43 (17.1) | 135 (17.9) | ||
| ≥200 | 122 (34.0) | 1541 (42.1) | 97 (38.5) | 299 (39.6) | ||
| Hospital occupancy at time of admission, median (IQR), % | 80 (60-90) | 80 (70-90) | .03 | 80 (60-90) | 80 (70-90) | .003 |
| ICU occupancy, median (IQR) | 80 (70-120) | 80 (70-100) | .39 | 80 (70-110) | 80 (70-100) | .36 |
| ICU typei | .37 | .07 | ||||
| Medical ICU | 140 (39.0) | 901 (24.6) | 83 (32.9) | 237 (31.3) | ||
| CCU | 55 (15.3) | 931 (25.5) | 46 (18.3) | 148 (19.6) | ||
| Other ICU | 49 (13.6) | 679 (18.6) | 39 (15.5) | 129 (17.1) | ||
| Other step-down | 18 (5.0) | 165 (4.5) | 13 (5.2) | 37 (4.9) | ||
| Cardiac step-down | 12 (3.3) | 167 (4.6) | 8 (3.2) | 28 (3.7) | ||
| Other | 85 (23.7) | 813 (22.2) | 63 (25.0) | 177 (23.4) | ||
| Treatment characteristics | ||||||
| Coronary angiography | 109 (30.4) | 1858 (50.8) | .43 | 87 (34.5) | 337 (44.6) | .21 |
| Any PCI | 82 (22.8) | 1335 (36.5) | .37 | 68 (27.0) | 245 (32.4) | .12 |
| Fibrinolytics only | 29 (8.1) | 38 (1.0) | .34 | 17 (6.7) | 11 (1.5) | .27 |
| Primary PCIj | 4 (1.1) | 334 (9.1) | .30 | 3 (1.2) | 71 (9.4) | .37 |
| CABG | 1 (0.3) | 267 (7.3) | .37 | 1 (0.4) | 44 (5.8) | .32 |
| Mechanical circulatory support | 18 (5.0) | 442 (12.1) | .26 | 16 (6.3) | 69 (9.1) | .10 |
| Intra-aortic balloon pump | 11 (3.1) | 355 (9.7) | .27 | 10 (4.0) | 52 (6.9) | .13 |
| LVAD | 7 (1.9) | 131 (3.6) | .10 | 6 (2.4) | 21 (2.8) | .03 |
| ECMO | 2 (0.6) | 139 (3.8) | .22 | 1 (0.4) | 22 (2.9) | .19 |
Abbreviations: CABG, coronary artery bypass grafting; CCU, cardiac care unit; COPD, chronic obstructive pulmonary disease; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; LVAD, left ventricular assist device; PCI, percutaneous coronary intervention; STEMI, ST elevation myocardial infarction.
In-hospital ST-segment elevation myocardial infarction (STEMI) was defined through International Classification of Diseases, Tenth Revision coding (eTable 1 in Supplement) as nonprimary diagnosis coding and not present on admission. Not all variables in the table were included in the propensity-score matching. A list of these variables is presented in the eMethods in the Supplement.
Race and ethnicity were determined at the hospital level. Other indicates American Indian or Alaska Native and Native Hawaiian or Other Pacific Islander.
Non–health care facility indicates physician referral of a patient from home, the workplace, or a physician’s office.
Law enforcement/court refers to transfers of incarcerated individuals.
Other includes government-assisted health care, military, auto insurance, workers’ compensation, research, Title V maternal and child health, county medically indigent service, charity, self-pay/uninsured, self-pay cash in full, other, and unknown.
The database provides the Elixhauser score for every patient. The score sums the presence of 30 comorbid conditions, with higher scores reflecting greater risk of in-hospital mortality.
Urban defined as core-based statistical area that encompasses at least 2500 people, at least 1500 of whom reside outside institutional group quarters.
Proprietary ownership indicates for-profit institutions. Voluntary ownership indicates nonprofit institutions.
Intensive care unit type provided by Vizient Clinical Database. Categories were collapsed for simplification. For more details see eMethods in the Supplement.
Primary percutaneous coronary intervention indicates coronary angioplasty/stenting performed in the setting of STEMI without prior administration of fibrinolytic agents.
Out-of-Hospital STEMI
Study Population
Baseline characteristics of patients with vs without COVID-19 and out-of-hospital STEMI are summarized in Table 1. Characteristics that were not well matched are specified in the eMethods in the Supplement. Standardized mean differences for patient characteristics appear in the eMethods in the Supplement. Across 370 centers, 565 patients were admitted with out-of-hospital STEMI and diagnosed with COVID-19 during the same encounter. During the same months in 2019 and 2020, a total of 75 869 patients (40 125 in 2019 and 35 744 in 2020) were admitted with out-of-hospital STEMI in whom a COVID-19 diagnosis was not present. When comparing patients with vs those without COVID-19, age and sex (69.9% vs 70.3% men; P = .85) were not significantly different, but those with COVID-19 were significantly less likely to be White (62.4% vs 76.3%; P < .001) and significantly more likely to be Hispanic (21.8% vs 8%; P < .001). Multiple comorbidities were prevalent in patients with COVID-19, reflected by a significantly higher median (IQR) Elixhauser comorbidity score than those without COVID-19 (2.0 [1.0-3.0] vs 1.0 [1.0-3.0]; P < .001). Patients with COVID-19 were significantly more likely to present with cardiac arrest (10.3% vs 6.8%; P = .001).
Treatment Characteristics
Although fibrinolytic therapy as standalone therapy was used in a minority of patients, those with COVID-19 were significantly more likely to receive this treatment than patients without COVID-19 (1.9% vs 0.2%; P < .001). Coronary angiography was performed significantly less often in patients with COVID-19 (81.9% vs 86.2%; P = .003), but the rates of primary PCI (71.0% vs 74.3%; P = .07), any PCI (79.8% vs 81.8%; P = .22), and coronary artery bypass grafting (3.5% vs 5.2%; P = .07) during the index encounter were not significantly different between groups. The use of mechanical circulatory support was also not significantly different between the groups (11.0% vs 10.1%; P = .50).
Primary Outcome
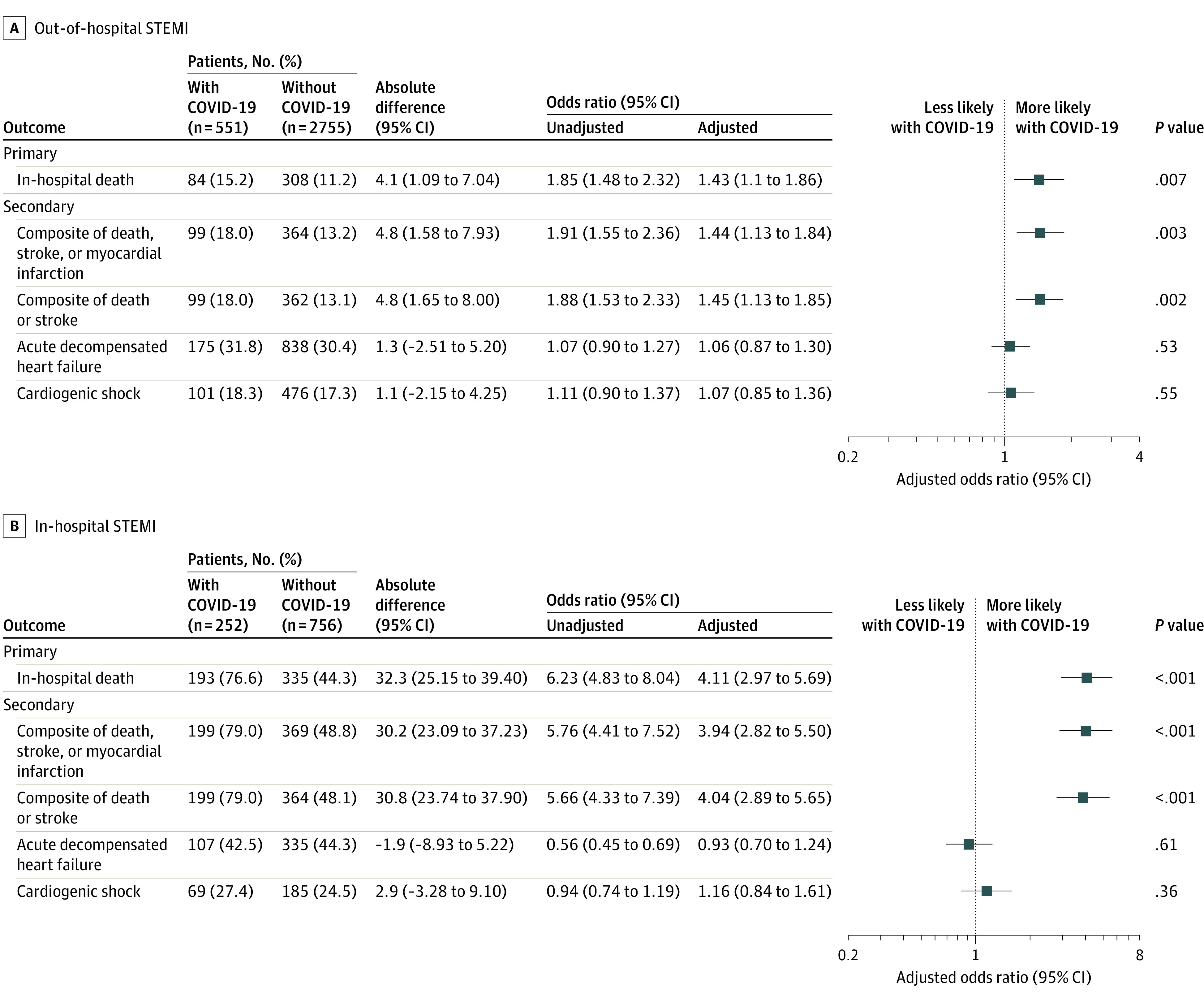
The unadjusted primary outcome in patients with vs without COVID-19 and out-of-hospital STEMI is summarized in eTable 2 and eFigure 1 in the Supplement. The propensity-matched primary outcome is shown in Figure 2. Patients with COVID-19 vs without COVID-19 had significantly higher rates of in-hospital mortality (15.2% vs 11.2%; absolute difference, 4.1% [95% CI, 1.1% to 7.0%]; odds ratio [OR], 1.43 [95% CI, 1.1-1.86]; P = .007) (Figure 2).
Figure 2. Association Between COVID-19 Diagnosis and Outcomes Among Propensity-Matched Patients With Out-of-Hospital and In-Hospital ST-Segment Elevation Myocardial Infarction (STEMI).
Secondary Outcomes
Unadjusted secondary outcomes in patients with vs without COVID-19 and out-of-hospital STEMI are summarized in eTable 2 and eFigure 1 in the Supplement. Propensity-matched secondary outcomes are shown in Figure 2. Patients with COVID-19 vs without COVID-19 had significantly higher rates of composite death, MI, or stroke (18.0% vs 13.2%; absolute difference, 4.8% [95% CI, 1.6%-7.9%]; P = .003) and composite death or stroke (18.0% vs 13.1%; absolute difference, 4.8% [95% CI, 1.7%-8.0%]; P = .002); other secondary outcomes were not significantly different between the groups (Figure 2).
Exploratory Outcomes
Unadjusted and propensity-matched exploratory outcomes in patients with vs without COVID-19 and out-of-hospital STEMI are summarized in eTables 2 and 3 in the Supplement.
Sensitivity Analyses
In sensitivity analyses, rates of in-hospital mortality remained significantly higher in patients with COVID-19 compared with a control group from the same calendar year (ie, 2020) (15.4% vs 11.1%; absolute difference, 4.3% [95% CI, 1.1%-7.5%]; OR, 1.46 [95% CI, 1.12-1.89]; P = .004) (eTable 4 in the Supplement), a control group matched on center (15.0% vs 8.6%; absolute difference, 6.4% [95% CI, 2.1%-10.6%], OR, 1.87 [95% CI, 1.22-2.85]; P = .003) (eTable 5 in the Supplement), and a control group excluding patients who were transferred (14.1% vs 10.3%; absolute difference 3.9% [95% CI, 0.3-7.5]; OR, 1.44 [95% CI, 1.06-1.96]; P = .02) (eTable 6 in the Supplement). On multivariable regression analysis after propensity matching with a control group from the previous calendar year (ie, 2019), COVID-19 remained associated with significantly higher rates of in-hospital mortality (OR, 1.60 [95% CI, 1.17-2.19]; P = .003) (eTable 7 in the Supplement).
In-Hospital STEMI
Study Population
Baseline characteristics of patients with vs without COVID-19 are summarized in Table 2. Characteristics that were not well matched are specified in the eMethods in the Supplement. Standardized mean differences for patient characteristics appear in the eMethods in the Supplement. Across 353 centers, 359 patients with COVID-19 were diagnosed with STEMI while hospitalized for other conditions, 203 (56.6%) of whom had COVID-19 as their primary diagnosis. During the same months in 2019 and 2020, a total of 3656 patients (2078 in 2019 and 1578 in 2020), in whom a COVID-19 diagnosis was not present, were diagnosed with STEMI.
Patient age was not significantly different between the groups, but, compared with those without COVID-19, patients with COVID-19 were significantly more likely to be men (71% vs 59.7%; P < .001), less likely to be White (51.8% vs 72.7%; P < .001), and more likely to be Hispanic (21.7% vs 6.8%; P < .001). The median (IQR) Elixhauser comorbidity score was not significantly different between the groups (4.0 [3.0-6.0] vs 4.0 [2.0-6.0]; P = .27). Patients with COVID-19 were significantly less likely to be admitted with heart failure (17.5% vs 28.8%; P < .001) and significantly more likely to present with cardiac arrest (26.2% vs 16.4%; P < .001) than those without COVID-19.
Treatment Characteristics
Patients with COVID-19 were significantly more likely to receive fibrinolytics as standalone therapy (8.1% vs 1.0%; P < .001), but significantly less likely to undergo coronary angiography (30.4% vs 50.8%; P < .001), any PCI (22.8% vs 36.5%; P < .001), or coronary artery bypass grafting (0.3% vs 7.3%; P < .001) compared with those without COVID-19. Mechanical circulatory support was used significantly less often in patients with COVID-19 (5.0% vs 12.1%; P < .001), a difference that was driven by greater use of intra-aortic balloon pumps and percutaneous left ventricular assist devices.
Primary Outcome
The unadjusted primary outcome in patients with vs without COVID-19 and in-hospital STEMI is summarized in eTable 2 and eFigure 2 in the Supplement. The propensity-matched primary outcome is shown in Figure 2. Patients with COVID-19 vs without COVID-19 had significantly higher rates of in-hospital mortality (78.5% vs 46.1%; absolute difference, 32.4% [95% CI, 29.1%-35.9%], OR, 4.11 [95% CI, 2.97-5.69]; P < .001) (Figure 2).
Secondary Outcomes
Unadjusted secondary outcomes in patients with vs without COVID-19 and in-hospital STEMI are summarized in eTable 2 and eFigure 2 in the Supplement. Propensity-matched secondary outcomes are shown in Figure 2. Patients with COVID-19 had significantly higher rates of composite death, stroke, or MI (80.9% vs 50.9%; absolute difference, 29.9% [95% CI, 26.7%-33.2%]; P < .001) and composite death or stroke (80.9% vs 50.4%; absolute difference, 30.5% [95% CI, 27.2%-33.7%], P < .001); other secondary outcomes were not significantly different between the groups (Figure 2).
Exploratory Outcomes
Unadjusted and propensity-matched exploratory outcomes in patients with vs without COVID-19 and in-hospital STEMI are summarized in eTables 2 and 3 in the Supplement.
Sensitivity Analyses
In sensitivity analyses, rates of in-hospital mortality remained significantly higher in patients with COVID-19 compared with a control group from the same calendar year (ie, 2020) (79.2% vs 49.9%; absolute difference, 29.4% [95% CI, 22.5%-36.2%]; OR, 3.84 [95% CI, 2.73-5.38]; P < .001) (eTable 4 in the Supplement), a control group matched on center (74.0% vs 45.9%; absolute difference, 28.2% [95% CI, 18.6%-37.8%]; OR, 3.37 [95% CI, 2.16-5.24]; P < .001) (eTable 5 in the Supplement), and a control group excluding patients who were transferred (76.4% vs 42.2%; absolute difference, 34.2% [95% CI, 27.0%- 41.3%]; OR, 4.43 [95% CI, 3.06-6.41]; P < .001) (eTable 6 in the Supplement). Results from a multivariable regression analysis after propensity matching with a control group from the previous calendar year (ie, 2019) showed that COVID-19 was associated with significantly higher rates of in-hospital mortality (OR, 5.77 [95% CI, 3.93-8.46]; P < .001) (eTable 7 in the Supplement).
Discussion
In this retrospective cohort study, patients with out-of-hospital or in-hospital STEMI and a concomitant diagnosis of COVID-19 had a higher rate of in-hospital mortality compared with propensity-matched groups of patients without COVID-19 admitted during the previous calendar year. Results were consistent in multiple sensitivity analyses, including an analysis using a control group of patients without COVID-19 from the same calendar year.
In previous studies, the incidence of cardiovascular events, including cardiovascular death and MI, was higher among those with influenza and influenza-like illnesses, such as SARS-CoV-1 and Middle East respiratory syndrome–related coronavirus.16,17,18,19 Additionally, the likelihood of admission for acute MI during a 7-day risk interval after a laboratory diagnosis of influenza was increased 6-fold.20 Differential treatment strategies and poorer in-hospital outcomes have also been observed among patients with acute MI and concomitant viral respiratory illness.21
Multiple studies have examined the prevalence and management of STEMI during the COVID-19 pandemic. Significant alterations in volume,1,2,3,4 disruptions in systems of care and management protocols,3,4,5 and potentially poorer outcomes compared with historical control patients have been described.3,5 However, there are no broadly representative robust data on patients with STEMI and a concomitant COVID-19 diagnosis. In an uncontrolled, descriptive study of 78 patients with COVID-19 who presented with STEMI at 4 hospitals in Italy, Lithuania, Spain, and Iraq, a higher-than-anticipated rate of stent thrombosis was observed.22 A single-center unadjusted analysis found higher rates of coronary stent thrombosis in patients with STEMI undergoing primary PCI when a COVID-19 diagnosis was present (n = 39) than when it was not.7 In an unadjusted analysis from 7 heart attack centers in London, patients with a COVID-19 diagnosis (n = 46) had longer length of stay and were at greater risk of mortality after an MI compared with patients without COVID-19.23 In the North American COVID-19 ST-Segment-Elevation Myocardial Infarction registry,6 which included patients with STEMI or new left bundle-branch block from 64 US and Canadian centers and propensity matched those with a COVID-19 diagnosis (n = 171) to approximately 15 000 historical control patients treated at 6 Midwest PCI-capable hospitals between 2003 through prepandemic 2020,24 adjusted in-hospital mortality (32% vs 6%; P < .001) and stroke (3.4% vs 0.6%; P = .039) were significantly more common among patients with vs without COVID-19. In the international COVID–acute coronary syndrome registry, 144 patients from 55 international centers who underwent invasive coronary angiography in the setting of STEMI and confirmed or suspected COVID-19 were propensity matched to 21 675 control patients enrolled in the 2018 and 2019 British Cardiovascular Intervention Society registry; in-hospital mortality was significantly higher in patients with COVID-19 on both unmatched and multivariable propensity-matched analyses (OR, 3.33 [95% CI, 2.04-5.42]).25
Data from patients with STEMI who were hospitalized for other illnesses are relatively limited, and current clinical trials, system initiatives, and guidelines are mainly directed toward those with out-of-hospital STEMI.26 Few studies suggest that patients who have in-hospital STEMI are older,26,27 are less likely to undergo PCI,26 and have higher rates of in-hospital death26 and 1-year death27 compared with those with out-of-hospital STEMI.
As in other studies of COVID-19, patients with COVID-19 were younger, less likely to be White, and more likely to be Hispanic compared with those who did not have COVID-19.28,29 Patients with COVID-19 were also more likely to present with cardiac arrest, which is consistent with increased rates of in-hospital and out-of-hospital cardiac arrest observed elsewhere during the pandemic.30,31 In contrast, the study observations about primary treatment strategies were novel. Fibrinolytics were used as reperfusion therapy in patients with out-of-hospital STEMI more often in those with a COVID-19 diagnosis than without, but the efficacy and safety of this strategy relative to primary PCI is unknown in patients with COVID-19. PCI remained the dominant therapy in both groups, with overall rates approximating those reported in other large nationwide cohorts.32 In contrast, among patients with in-hospital STEMI, the rates of coronary revascularization were significantly lower in those with COVID-19 than without COVID-19, although rates were quite low in both groups. Whether this change in approach resulted from a perceived futility of invasive therapy in these patients, perceived risk to health care workers, or both is unknown.
Limitations
This study has several limitations. First, as an observational study, an unknown amount of residual unmeasured confounding and bias may remain, despite propensity matching. Second, the clinical database includes primarily US academic medical centers; the findings may not be generalizable to all centers. Third, although most of the clinical characteristics and outcomes included in the study were well defined through 1 or more ICD-10 codes, some variables did not have validation literature, and miscoding cannot be excluded. Fourth, the clinical database does not collect information on cause of death. Similarly, it does not collect data on patient symptoms, so it is not possible to ascertain whether COVID-19 diagnosis was suspected clinically or diagnosed solely based on routine testing. Nevertheless, the overlap of symptoms between STEMI and COVID-19 (eg, shortness of breath, chest pain) would make this distinction clinically challenging. Fifth, although models of in-hospital mortality after STEMI included all available demographic and comorbid characteristics, other information that has been prognostic in models33 was not available, such as in-hospital vital signs, test results (eg, from electrocardiograms, cardiac biomarkers, and echocardiograms), time to reperfusion (eg, door-to-balloon time, door-to-needle time), and procedural detail (eg, angiographic and treatment characteristics). Likewise, scores such as the Acute Physiology and Chronic Health Evaluation II34 and Sequential Organ Failure Assessment35 have been applied to predict mortality in patients with COVID-19; these scores include vital signs, laboratory variables, and other measurements that were not routinely available in the database, and imbalances in these measurements may have accounted in part for the differential outcomes observed. Sixth, in contrast to the out-of-hospital STEMI group, it was not possible to discern the timing of PCI relative to the timing of the STEMI diagnosis in the in-hospital STEMI group; hence, rates of primary PCI were not presented for the latter. Seventh, this study primarily examined in-hospital outcomes. Longer-term data are needed to fully understand the effect of COVID-19 infection on patients with STEMI.
Conclusions
Among patients with out-of-hospital or in-hospital STEMI, a concomitant diagnosis of COVID-19 was associated with significantly higher rates of in-hospital mortality compared with patients without a diagnosis of COVID-19 from the past year. Further research is required to understand the potential mechanisms underlying this association.
eMethods and eResults
References
- 1.Tam CF, Cheung K-S, Lam S, et al. Impact of coronavirus disease 2019 (COVID-19) outbreak on ST-segment-elevation myocardial infarction care in Hong Kong, China. Circ Cardiovasc Qual Outcomes. 2020;13(4):e006631. doi: 10.1161/CIRCOUTCOMES.120.006631 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.De Filippo O, D’Ascenzo F, Angelini F, et al. Reduced rate of hospital admissions for ACS during COVID-19 outbreak in Northern Italy. N Engl J Med. 2020;383(1):88-89. doi: 10.1056/NEJMc2009166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Xiang D, Xiang X, Zhang W, et al. Management and outcomes of patients with STEMI during the COVID-19 pandemic in China. J Am Coll Cardiol. 2020;76(11):1318-1324. doi: 10.1016/j.jacc.2020.06.039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.De Luca G, Verdoia M, Cercek M, et al. Impact of COVID-19 pandemic on mechanical reperfusion for patients with STEMI. J Am Coll Cardiol. 2020;76(20):2321-2330. doi: 10.1016/j.jacc.2020.09.546 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kwok CS, Gale CP, Kinnaird T, et al. Impact of COVID-19 on percutaneous coronary intervention for ST-elevation myocardial infarction. Heart. 2020;106(23):1805-1811. doi: 10.1136/heartjnl-2020-317650 [DOI] [PubMed] [Google Scholar]
- 6.Garcia S, Dehghani P, Grines C, et al. ; Society for Cardiac Angiography and Interventions, the Canadian Association of Interventional Cardiology, and the American College of Cardiology Interventional Council . Initial findings from the North American COVID-19 myocardial infarction registry. J Am Coll Cardiol. 2021;77(16):1994-2003. doi: 10.1016/j.jacc.2021.02.055 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Choudry FA, Hamshere SM, Rathod KS, et al. High thrombus burden in patients with COVID-19 presenting with ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2020;76(10):1168-1176. doi: 10.1016/j.jacc.2020.07.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rodriguez-Leor O, Cid Alvarez AB, de Prado AP, et al. In-hospital outcomes of COVID-19 ST-elevation myocardial infarction patients. EuroIntervention. 2021;16(17):1426-1433. doi: 10.4244/EIJ-D-20-00935 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bikdeli B, Madhavan MV, Jimenez D, et al. ; Global COVID-19 Thrombosis Collaborative Group, Endorsed by the ISTH, NATF, ESVM, and the IUA, Supported by the ESC Working Group on Pulmonary Circulation and Right Ventricular Function . COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(23):2950-2973. doi: 10.1016/j.jacc.2020.04.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pellegrini D, Kawakami R, Guagliumi G, et al. Microthrombi as a major cause of cardiac injury in COVID-19: a pathologic study. Circulation. 2021;143(10):1031-1042. doi: 10.1161/CIRCULATIONAHA.120.051828 [DOI] [PubMed] [Google Scholar]
- 11.Bradley EH, Herrin J, Wang Y, et al. Racial and ethnic differences in time to acute reperfusion therapy for patients hospitalized with myocardial infarction. JAMA. 2004;292(13):1563-1572. doi: 10.1001/jama.292.13.1563 [DOI] [PubMed] [Google Scholar]
- 12.Rodriguez F, Solomon N, de Lemos JA, et al. Racial and ethnic differences in presentation and outcomes for patients hospitalized with COVID-19: findings from the American Heart Association’s COVID-19 Cardiovascular Disease Registry. Circulation. 2021;143(24):2332-2342. doi: 10.1161/CIRCULATIONAHA.120.052278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Coding. Centers for Medicare & Medicaid Services. Accessed February 20, 2021. Updated August 11, 2021. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalAcqCond/Coding
- 14.van Walraven C, Austin PC, Jennings A, Quan H, Forster AJ. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Med Care. 2009;47(6):626-633. doi: 10.1097/MLR.0b013e31819432e5 [DOI] [PubMed] [Google Scholar]
- 15.Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10(2):150-161. doi: 10.1002/pst.433 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Madjid M, Miller CC, Zarubaev VV, et al. Influenza epidemics and acute respiratory disease activity are associated with a surge in autopsy-confirmed coronary heart disease death: results from 8 years of autopsies in 34,892 subjects. Eur Heart J. 2007;28(10):1205-1210. doi: 10.1093/eurheartj/ehm035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Peiris JSM, Chu CM, Cheng VCC, et al. ; HKU/UCH SARS Study Group . Clinical progression and viral load in a community outbreak of coronavirus-associated SARS pneumonia: a prospective study. Lancet. 2003;361(9371):1767-1772. doi: 10.1016/S0140-6736(03)13412-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O. Potential effects of coronaviruses on the cardiovascular system: a review. JAMA Cardiol. 2020;5(7):831-840. doi: 10.1001/jamacardio.2020.1286 [DOI] [PubMed] [Google Scholar]
- 19.Smeeth L, Thomas SL, Hall AJ, Hubbard R, Farrington P, Vallance P. Risk of myocardial infarction and stroke after acute infection or vaccination. N Engl J Med. 2004;351(25):2611-2618. doi: 10.1056/NEJMoa041747 [DOI] [PubMed] [Google Scholar]
- 20.Kwong JC, Schwartz KL, Campitelli MA, et al. Acute myocardial infarction after laboratory-confirmed influenza infection. N Engl J Med. 2018;378(4):345-353. doi: 10.1056/NEJMoa1702090 [DOI] [PubMed] [Google Scholar]
- 21.Cardoso R, Rivera M, Czarny MJ, et al. In-hospital management and outcomes of patients with acute myocardial infarction and influenza. Am J Cardiol. 2020;125(6):840-844. doi: 10.1016/j.amjcard.2019.12.032 [DOI] [PubMed] [Google Scholar]
- 22.Hamadeh A, Aldujeli A, Briedis K, et al. Characteristics and outcomes in patients presenting with COVID-19 and ST-segment elevation myocardial infarction. Am J Cardiol. 2020;131:1-6. doi: 10.1016/j.amjcard.2020.06.063 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Little CD, Kotecha T, Candilio L, et al. COVID-19 pandemic and STEMI: pathway activation and outcomes from the pan-London heart attack group. Open Heart. 2020;7(2):e001432. doi: 10.1136/openhrt-2020-001432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yildiz M, Sharkey S, Aguirre FV, et al. The Midwest ST-elevation myocardial infarction consortium: design and rationale. Cardiovasc Revasc Med. 2021;23:86-90. doi: 10.1016/j.carrev.2020.08.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kite TA, Ludman PF, Gale CP, et al. ; International COVID-ACS Registry Investigators . International prospective registry of acute coronary syndromes in patients with COVID-19. J Am Coll Cardiol. 2021;77(20):2466-2476. doi: 10.1016/j.jacc.2021.03.309 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kaul P, Federspiel JJ, Dai X, et al. Association of inpatient vs outpatient onset of ST-elevation myocardial infarction with treatment and clinical outcomes. JAMA. 2014;312(19):1999-2007. doi: 10.1001/jama.2014.15236 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Garberich RF, Traverse JH, Claussen MT, et al. ST-elevation myocardial infarction diagnosed after hospital admission. Circulation. 2014;129(11):1225-1232. doi: 10.1161/CIRCULATIONAHA.113.005568 [DOI] [PubMed] [Google Scholar]
- 28.Muñoz-Price LS, Nattinger AB, Rivera F, et al. Racial disparities in incidence and outcomes among patients with COVID-19. JAMA Netw Open. 2020;3(9):e2021892. doi: 10.1001/jamanetworkopen.2020.21892 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Dai CL, Kornilov SA, Roper RT, et al. Characteristics and factors associated with COVID-19 infection, hospitalization, and mortality across race and ethnicity. Clin Infect Dis. 2021;ciab154. doi: 10.1093/cid/ciab154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Holland M, Burke J, Hulac S, et al. Excess cardiac arrest in the community during the COVID-19 pandemic. JACC Cardiovasc Interv. 2020;13(16):1968-1969. doi: 10.1016/j.jcin.2020.06.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hayek SS, Brenner SK, Azam TU, et al. ; STOP-COVID Investigators . In-hospital cardiac arrest in critically ill patients with covid-19: multicenter cohort study. BMJ. 2020;371:m3513. doi: 10.1136/bmj.m3513 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Culler SD, Kugelmass AD, Cohen DJ, et al. Understanding readmissions in Medicare beneficiaries during the 90-day follow-up period of an acute myocardial infarction admission. J Am Heart Assoc. 2019;8(21):e013513. doi: 10.1161/JAHA.119.013513 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.McNamara RL, Kennedy KF, Cohen DJ, et al. Predicting in-hospital mortality in patients with acute myocardial infarction. J Am Coll Cardiol. 2016;68(6):626-635. doi: 10.1016/j.jacc.2016.05.049 [DOI] [PubMed] [Google Scholar]
- 34.Rodríguez A, Ruiz-Botella M, Martín-Loeches I, et al. ; COVID-19 SEMICYUC Working Group . Deploying unsupervised clustering analysis to derive clinical phenotypes and risk factors associated with mortality risk in 2022 critically ill patients with COVID-19 in Spain. Crit Care. 2021;25(1):63. doi: 10.1186/s13054-021-03487-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Rivera-Izquierdo M, Del Carmen Valero-Ubierna M, R-delAmo JL, et al. Sociodemographic, clinical and laboratory factors on admission associated with COVID-19 mortality in hospitalized patients: a retrospective observational study. PLoS One. 2020;15(6):e0235107. doi: 10.1371/journal.pone.0235107 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods and eResults