

Abstract
We examined the quality of evidence supporting the effects of Naturalistic Developmental Behavioral Interventions (NBDIs) for facilitating change in young children with autism. We also investigated whether effects varied as a function of specific features of the intervention, samples, and outcomes measured. Twenty-seven studies testing the effects of NDBIs were extracted from data collected for the Autism Intervention Meta-analysis (Project AIM), a comprehensive meta-analysis of group design, non-pharmacological intervention studies for children with autism aged 0-8 years. We extracted effect sizes for 454 outcomes from these studies for use in meta-regression analyses testing associations between intervention effects and mean participant chronological age, language age, autism symptomatology, percentage of sample reported as male, cumulative intervention intensity, interventionist, outcome boundedness, outcome proximity, and risk of parent/teacher training correlated measurement error. The extant literature on NDBIs documents effects on social communication, language, play, and cognitive outcomes. However, our confidence in the positive and significant summary effects for these domains is somewhat limited by methodological concerns. Intervention effects were larger for context-bound outcomes (relative to generalized), and for proximal outcomes (relative to distal). Our results indicate that NDBIs have promise as an approach for supporting development for some, but not all of the core and related features of autism in early childhood. Confidence in summary effect estimates is limited by study quality concerns, particularly an overreliance on measures subject to high detection bias. The results of this review support the use of proximity and boundedness as indicators of the limits of intervention effects.
Keywords: Naturalistic Developmental Behavioral Intervention, autism, child, meta-analysis, review, outcome measures
Lay Summary
Naturalistic Developmental Behavioral Interventions may increase language, social communication, play skills, and cognition in young children with autism, but these increases are largest for skills directly targeted by the intervention, and in contexts that are similar to that of the intervention. These conclusions are tempered by some concerns regarding research design across the studies that have been conducted to date.
In 2015, the developers of several prominent ‘named’ interventions (i.e., established, often manualized interventions associated with specific names and developers) designed for young children with autism1 authored a consensus statement designating that those approaches comprised a new intervention category called Naturalistic Developmental Behavioral Interventions (NDBIs; Schriebman et al., 2015). These interventions blend strategies from behavioral and developmental learning theories to target developmental milestones. Strategies shared among NDBIs include the use of loose teaching to target multiple exemplars across a variety of contexts throughout a child’s daily routines, following the child’s lead and engaging with the object or activity that draws the child’s focus of attention, and creating a naturally reinforcing context for learning where the adult and the child share control of the interaction. Some examples of prevalent NDBIs are Enhanced Milieu Teaching (Hemmeter & Kaiser, 1994; Kaiser, 1994), Pivotal Response Training (Koegel, Koegel, Harrower & Carter, 1999; Schreibman & Koegel, 1996), and the Early Start Denver Model (Dawson et al., 2010; Rogers & Dawson, 2010).
The primary developmental achievements targeted by NDBIs are those that have been identified as predictors of later social communication, language, and cognition, particularly in this population. These include imitation, shared affect, joint attention, turn-taking, attending to others, functional and symbolic play, prelinguistic communication (e.g., gestures, vocalizations, eye gaze, etc.), and emerging word use (Schreibman et al., 2015). The behavioral teaching techniques used in NDBIs include modeling, shaping, chaining, prompting, and differential reinforcement (Schreibman et al., 2015). Natural antecedents and contingencies are leveraged to occasion and reinforce targeted behaviors. For example, a spoken request would be met with the delivery of the requested item or activity, which is a natural consequence for this behavior. These naturalistic teaching strategies are embedded into the daily routines of the child to ensure that activities take place within meaningful and generalized social contexts.
Empirical Support for NDBIs
Group design studies of NDBIs suggest that this type of intervention can facilitate improvements in a number of domains, including social communication (Brian, Smith, Zwaigenbaum, & Bryson, 2017; Dawson et al, 2010; Kasari, Paparella, Freeman, & Jahromi, 2008; Lawton & Kasari, 2012; Shire et al., 2017), language (Chang, Shire, Shih, Gelfand, & Kasari, 2016; Dawson et al., 2010; Drew et al., 2002; Hardan et al., 2015), adaptive behavior (Dawson et al., 2010; Estes et al., 2015; Ingersoll, Wainer, Berger, & Walton, 2017; Wetherby & Woods, 2006), play (Chang et al., 2016; Kasari et al., 2008; Shire et al., 2017), and cognition in children with autism (Drew et al., 2002; Kasari et al., 2008; Wetherby & Woods, 2006). Recent meta-analytic work has suggested that NDBIs effect positive and significant improvements in language, play, cognition, autism symptomatology, and social communication (e.g., joint attention and joint engagement; Tiede & Walton, 2019); however, this work failed to include all available outcomes in summary effect estimation or to describe study quality beyond providing overall categorical ratings (i.e., ‘weak’, ‘adequate’, or ‘strong’). In our own recent meta-analysis of interventions for young children with autism (Sandbank et al., 2020a), we estimated summary effects across all available outcomes from studies of NDBIs in young children with autism. Among the eight outcome domains of interest to the quantitative synthesis, we found positive and significant effects on social communication, language, play, and cognition of children with autism between birth and 8 years of age. We additionally summarized the quality of studies in terms of risk of selection bias, attrition bias, detection bias, and reliance on parent/teacher reports (which constitute a specific subset of measures that are subject to high risk of detection bias, or a ‘placebo-by-proxy’ effect; Grelotti & Katpchuk, 2011). Our systematic review showed that, overall, the quality of empirical support for NDBIs was relatively high compared to that of other intervention approaches. Furthermore, the current body of evidence supporting NDBIs was largely devoid of threats to internal validity such as selection and attrition bias, and was mostly derived from direct measures of child performance/development, rather than from caregiver reports. However, study results were threatened by high detection bias, which can be present when assessors are aware of participants’ group assignment. Though the summary effects of NDBIs and the overall quality of evidence has been reported, less is known about the quality of the evidence supporting the use of NDBIs to improve specific outcomes (e.g., divided by domain). Moreover, little is known about the extent to which NDBI effects vary based on specific aspects of the intervention, the characteristics of the study sample, and the nature of the outcomes measured.
Factors That May Influence Intervention Effects
Autism symptomatology.
Prior research has found that children with lower autism symptomatology are more likely to benefit from intervention (Itzchak & Zachor, 2011; Perry et al., 2011; Sallows & Graupner, 2005), though which characteristics of autism best predict intervention outcomes, and why, is less understood (Vivanti, Prior, Williams, & Dissanayake, 2014). It could be that higher rates of stereotypic behaviors and fewer foundational social communication skills may interfere with a child’s ability to socially engage with clinicians, potentially limiting their learning opportunities in an intervention that is largely situated within a dyadic social context. Previous studies have demonstrated that young children who exhibit lower levels of autism symptomatology at the start of intervention derive greater benefit from at least some treatments delivered during early childhood (Ben-Itzchak & Zachor, 2007; Gordon et al., 2011), and differentially benefit from NDBIs delivered at higher intensities (e.g., greater number of hours per week; Yoder et al., 2018, 2019).
Chronological age.
Researchers and clinicians frequently assert that intervention should begin as early as possible in order to maximize benefits for young children with autism (National Institute of Child Health and Human Development, 2017; Zwaigenbaum et al., 2015). This principle stems in part from developmental theory, which suggests that improvements in the earlier stages of development extend into later life by serving as a foundation for subsequent development. Key milestones are also most readily acquired during biologically predetermined periods (e.g., “developmental windows”), which occur early in a child’s life and are marked by high levels of neuronal plasticity, which heighten the brain’s responsiveness to learning experiences and trigger the development of new neural connections (Bornstein, Hahn, & Haynes, 2010; Halfon, Shulman, & Hochstein, 2001; Masten & Cicchetti, 2010; Mundkur, 2005; Ruben, 1997). Though the logical framework of these theories suggests that children with autism should receive intervention as early as possible to capitalize on periods during which we should expect optimal plasticity, intervention research has not definitively shown that children who receive intervention at younger ages benefit more than those who begin intervention later in life. In fact, several previous meta-analyses of early interventions for children with autism have found that chronological age at intervention was not a significant moderator of intervention effects on outcomes of interest (Makrygianni & Reed, 2010; Reichow & Wolery, 2009; Sandbank et al., 2020b; Virues-Ortega, 2010).
Parent-reported sex.2
Prior literature suggests that there are a number of sex-related differences in the diagnosis and presentation of autism. Autism is more prevalent in boys (, with a male-to-female ratio of prevalence of 4-5:1, though several recent epidemiological studies suggest the ratio may be lower, at 2-4:1 (e.g., Fombonne, 2009; Hinkka-Yli-Salomäki et al., 2014; Kim et al., 2011; Saemundsen, Magnússon, Georgsdóttir, Egilsson, & Rafnsson, 2013; Surén et al., 2012). Girls are additionally often diagnosed at a later age compared to boys (Begeer et al., 2013). Differences in prevalence and age at diagnosis may be explained by differences in the presentation of core symptoms in boys and girls (Kreiser & White, 2014; Lai, Lombardo, Auyeung, Chakrabarti, & Baron-Cohen, 2015). For example, girls may demonstrate fewer or different types of repetitive behaviors and restricted interests compared to boys with autism (Antezana et al., 2019). In addition, girls with autism tend to show greater attention to faces, produce more social imitation, and show greater desire for interaction compared to boys with autism, which may mask other social communication differences in this group (Green, Travers, Howe, & McDougle, 2019; Harrop et al., 2019). Given the differences in presentation associated with sex, it is logical to hypothesize that intervention effects may vary by parent-reported sex. For example, it is possible that compensatory social communication behaviors in girls may limit the amount of improvement achievable on NDBI targets; however, it is also possible that a greater desire for interaction and increased social attention may facilitate greater developmental progression through NDBIs for girls.
Language level.
Intervention effects may vary as a function of child language level at the start of intervention. Previous investigations have found that children with higher language level at intervention onset tend to demonstrate larger gains than their counterparts with lower language level (Bono, Daley, & Sigman, 2004; Itzchak & Zachor, 2011; Sandbank et al., 2020b). This may be because children with more advanced language levels have more tools to help them engage in a social dyad with the interventionist administering an NDBI, which is where much (or all) learning is expected to take place. In other words, it is possible that children with higher language ages have a developmental foundation that can facilitate subsequent developmental improvements affected by intervention. This developmental readiness may enable them to advance more quickly than children who enter intervention with lower language ages.
Interventionist type.
Whether an NDBI is implemented by an educator, clinician, caregiver, or caregiver-clinician team may influence the strength of intervention effects. Prior meta-analytic work suggests that caregiver-implemented interventions can have strong positive effects on language outcomes for children with disabilities (Roberts & Kaiser, 2011). However, a recent meta-analysis examining the effect of interventions on language outcomes of children with autism reported that effects of caregiver-implemented interventions were significantly smaller than those of clinician- and combination-led interventions (Sandbank et al., 2020b). NDBIs are designed to be implemented within a child’s natural environment and naturally-occurring daily routines. Caregivers have the most opportunities to utilize NDBI strategies to foster their child’s development in everyday settings, and are arguably able to provide the most meaningful social context for intervention, which theoretically positions them to be the most effective implementers of NDBIs. It is possible, though, that a clinician’s expertise and extensive experience with intervention may lead to more effective and efficient use of NDBI strategies than the typical caregiver can provide, which could lead to larger intervention effects in favor of clinician-implemented versus caregiver-implemented treatment. Many NDBI models recommend that intervention strategies be collaboratively implemented by caregivers and clinicians (Dawson et al., 2010; Hemmeter & Kaiser, 1994; Schreibman & Koegel, 1996; Schreibman et al., 2014). A previous meta-analysis found that effects on spoken language outcomes were largest for interventions implemented by caregivers and clinicians working together compared to those of interventions implemented by either clinicians or caregivers alone (Hampton & Kaiser, 2016). Similarly, prior studies have reported positive results of NDBIs implemented by educators in the preschool setting (Goods, Ishijima, Chang, & Kasari, 2013; Lawton & Kasari, 2012). Although educators may not be able to devote as much undivided attention to a single child as caregivers or clinicians, there are still many opportunities in the preschool setting to implement NDBI strategies during play, meal times, and instruction. Educators may also be particularly skilled at leveraging other resources, such as a child’s peers, to scaffold growth in the school setting. Thus, it is not clear which type of interventionist (or combination thereof) may yield the greatest magnitude of effects for NDBIs.
Cumulative intervention intensity.
Many practitioners assert the provision of intensive intervention (e.g., intervention provided for 20-40 hours per week) has greater potential to lead to improved outcomes for young children with autism as compared to moderately administered interventions (National Research Council, 2001). However, the evidence to support this rather common recommendation is mixed. Though some primary studies have suggested that children who received more hours of intervention made greater gains (Lovaas, 1987), others have found that children who received different intervention intensities experienced non-significantly different levels of improvement (Fernell et al., 2011; Sallows & Graupner, 2005; Yoder et al., 2018; 2019). Two previous meta-analyses of early intensive behavioral intervention (EIBI) for children with autism found a positive relationship between intervention intensity and adaptive behavior outcomes (Virues-Ortega, 2010; Makrygianni & Reed, 2010), and one found that intervention intensity moderated effects of intervention on IQ outcomes (Makrygianni & Reed, 2010). However, other meta-analyses of interventions for children with autism have failed to find an association between cumulative intensity and intervention effects on IQ (Reichow & Wolery, 2009) or language outcomes (Hampton & Kaiser, 2016; Sandbank et al., 2020b).
Outcome proximity.
One potentially important aspect of intervention outcomes is their proximity to the domains directly targeted by the intervention. Outcome proximity characterizes whether an outcome reflects the exact targets that were taught in an intervention, untaught targets within the targeted domain, or untaught behaviors/skills in other non-targeted domains for which change would reflect ongoing development facilitated by the intervention. For example, in a naturalistic intervention geared towards improving initiations of joint attention by directly teaching participants to point, a measure of the number of times participants point would be considered a proximal outcome, as would other metrics indexing initiating joint attention (e.g., child gives or shows). Measures of broader social communication development would be considered distal outcomes, and measures of outcomes developmentally downstream from early social communication milestones, such as measures of language, would be considered very distal.
Prior systematic reviews and quantitative syntheses have found that investigations of interventions delivered to children with autism in early childhood often report outcomes that are overly proximal to intervention targets (Provenzani et al., 2019), that researchers are more likely to detect positive effects on proximal compared to distal outcomes (Yoder, Bottema-Beutel, Woynaroski, Chandrasekhar, & Sandbank, 2013), and that effect sizes for proximal measures are significantly larger than for distal measures across all intervention studies for young children with autism (Sandbank et al., 2020a). Thus, interventions geared towards young children with autism in general are more likely to improve performance in explicitly targeted skills, and less likely to facilitate broader development in targeted or untargeted domains. Given that the theoretical orientation of NDBIs suggests that targeting developmentally important proximal skills will bootstrap the achievement of downstream developmental milestones, it is likely that this trend will hold for NDBIs as well. However, it is important to assess whether these approaches vary in the degree to which they are actually able to impact proximal versus developmentally distal outcomes.
Outcome boundedness.
Similarly, the boundedness of outcomes to the intervention context likely influences the observed effects of interventions. Outcomes measured in a context that sufficiently differs from that of the intervention on a number of dimensions are more likely to reflect generalized changes, such that any improvement measured can be assumed to be independent from the intervention context. Documenting highly generalized effects not only requires that the assessment or measurement of outcomes take place in a different physical setting than the intervention, but also that the nature of the assessment differs from the nature of the intervention in several ways (Yoder et al., 2013). For example, results from standardized tests administered by unfamiliar assessors index generalized effects because they differ from the intervention context in terms of interaction partner, materials, and interaction style. Alternatively, measures of social behaviors collected within interactions that are similar to the context of intervention (e.g., a coded video of a play sample with the interventionist) are considered to be context-bound, as they may index intervention effects that manifest only when the child interacts with that particular individual, in response to that particular interaction style, or in the particular setting of the intervention.
Prior meta-analyses of autism intervention research have shown that researchers are more likely to detect positive effects on context-bound relative to generalized outcomes (Yoder et al., 2013) and that intervention summary effects for generalized outcomes are significantly smaller than those for context-bound outcomes (Sandbank et al., 2020a). This trend suggests that much of the overall positive effects reported in the early autism intervention literature may have low external and social validity, as the gains demonstrated in context-bound assessments are unlikely to generalize to other measures of the same constructs, or to environments and social situations that matter most for the child. Investigators relying on context-bound measures risk incorrectly interpreting intervention gains as indicative of generalized developmental change, even though the construct validity of these measures is likely poor.
Correlated measurement error (CME) related to parent and teacher training.
The focus on natural agents of intervention (e.g., caregivers and teachers) in NDBIs and the reliance on naturalistic assessment of skills within the context of interactions can lead to another threat to internal validity. Specifically, when caregivers or teachers act as interventionists (e.g., in parent- or teacher-mediated interventions) and then also serve as assessors, either as interaction partners in naturalistic assessments or as reporters on standardized caregiver reports, post-test scores may be positively biased in favor of the intervention group. That is, following intervention and training, the assessors (parents or teachers) in the treatment group are more informed about their children’s capabilities, and likely better able to elicit the behaviors of interest to the study, which may upwardly bias assessments that they complete, even in the absence of actual child gains due to the intervention. For example, in a study of a caregiver mediated social communication intervention, caregivers in the intervention group may be trained to imitate children and be more uniformly responsive as a means to increase their children’s social communicative behaviors. An observational measure of child social communication taken from a caregiver-child interaction might then reflect transiently enhanced social communication acts in the intervention group, because the measurement context featured a parent who was trained to better elicit social communication. This is a threat to internal validity that extends beyond that of detection bias, which is already present in outcomes derived from caregiver reports or observational measures of caregiver-child interactions, because in addition to being able to subtly influence interactions, assessors in the intervention group are specifically given strategies to influence these interactions over the course of the study. We refer to this threat to internal validity as parent/teacher training CME (Sandbank et al., 2020a). Prior evaluations of the NDBI literature have suggested that about half of reported outcomes are subject to this threat (Sandbank et al., 2020a), but no studies to date have examined whether effects for outcomes threatened by parent/teacher training CME are significantly greater than intervention effects on outcomes that are not subject to this threat.
Current Investigation
The purpose of the current study was to extend the results of previous work by Sandbank and colleagues (2020a) that reported summary effects of NDBIs on each of eight different outcome types by (a) examining the quality of the evidence supporting each specific summary effect according to previously established criteria, and (b) evaluating the extent to which NDBI intervention effects vary by other specified sample, intervention, and outcome characteristics hypothesized to influence the magnitude of summary effects. Our research questions were as follows:
What is the quality of the evidence supporting the use of NDBIs for facilitating gains in each of nine outcome domains (i.e., social communication; restricted, repetitive patterns of behavior, interests, or activities; sensory function, overall autism symptomatology; language; play; cognition; social-emotional skills/challenging behavior; and adaptive behavior) in terms of risk of selection bias, detection bias, attrition bias, reliance on parent/teacher report, risk of parent/teacher training CME, and the boundedness and proximity of outcomes?
Do the effects of NDBIs vary as a function of intervention characteristics including cumulative intervention intensity and interventionist type; sample characteristics including autism symptomatology, chronological age, parent-reported sex, and language age; and outcome features hypothesized to influence effect sizes, including outcome proximity, boundedness, and risk of parent/teacher training CME?
Method
Data for the current paper was collected as part of Project AIM (Autism Intervention Meta-analysis; Sandbank et al., 2020a), a scoping review and meta-analysis of all group design studies of non-pharmacological interventions for young children with autism. A brief overview of search and coding procedures is provided below, and additional details are provided in supplementary materials.
Search
A total of nine databases were searched to identify studies eligible for the larger Project AIM meta-analysis. This initial search yielded 12,933 results, which included group design studies of all intervention types on all outcome types for children with autism ages 0-8 years.In an effort to include data from unpublished studies, we contacted 90 researchers who had received federal funds to study autism to request unpublished data. No additional datasets were yielded by these requests.
In the parent meta-analysis, studies were screened for the following inclusion criteria: (a) published in English, (b) published from 1970 - 2018 (the year the initial search was conducted), (c) employed a group design that included both an intervention and control group, (d) included a simple majority of participants reported to have a diagnosis of an autism spectrum disorder (ASD), and (e) comprised a sample for which the average age of included participants was between 0 and 8 years. From these, studies of interventions categorized as NDBIs, based on the list proposed by Schreibman and colleagues (2015), were extracted. A total of 27 studies of NDBIs meeting the aforementioned criteria were identified and included in the current review and synthesis. The PRISMA diagram is presented in Figure 1.
Figure 1.
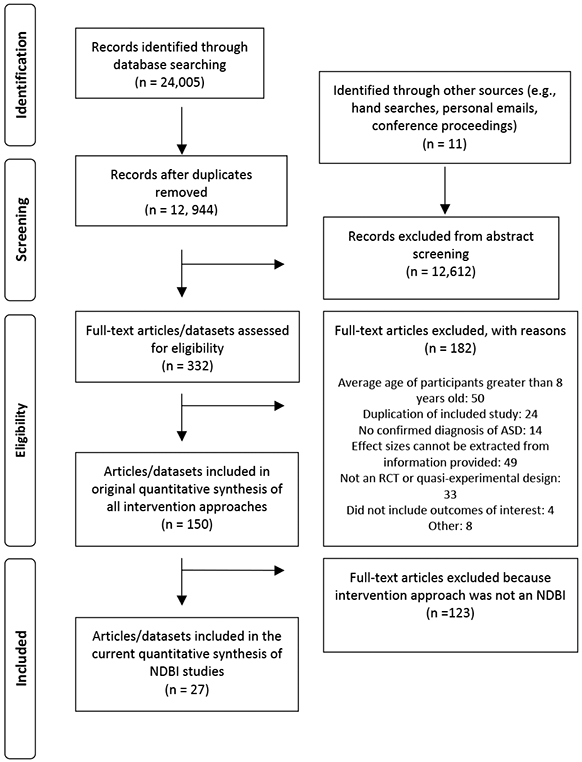
Prisma Flow Diagram of Systematic Search
Coding Procedures
All included studies were coded for sample, intervention, and outcome characteristics, as well as quality indicators by the second author and one additional member of a team of nine reliability coders. The team of coders comprised three PhD-level experts in non-pharmacological interventions for young children with autism and undergraduate and graduate students in their laboratories. Prior to coding, coders were trained to 80% agreement on a set of training studies. All studies were independently coded by two separate coders for the purposes of monitoring reliability. The coding manual is available upon request from the second author, and data has been deposited in a public repository (Open Science Framework, 2019).
Sample characteristics.
Included studies were coded for mean participant age in months at intervention onset, pre-intervention language age (age equivalency, in months), autism symptomatology, and percentage of males included in the sample.
Intervention characteristics.
When reported, cumulative intervention intensity in hours was extracted from the included studies by summing the total hours of intervention delivered to children across the duration of the study. Hours in which parents received coaching with children present were included in this total, but coaching hours during which children were not present were excluded. Individuals administering the intervention were coded as caregiver, clinician, educator, or combination.
Outcome characteristics and quality.
Outcomes were categorized by domain as either social communication; restricted, repetitive patterns of behavior, interests, or activities; sensory functioning; overall autism symptomatology; language; play; cognition; social-emotional skills/challenging behavior; and adaptive behavior. Outcomes were then coded for study- and outcome-level quality indicators, including their risk of selection bias, detection bias, and attrition bias, as well as their proximity to intervention targets, their boundedness to the context of intervention, and their risk of parent/teacher training CME.
Outcomes were categorized as either proximal or distal to intervention targets. An outcome was coded as proximal if it measured a skill that was directly taught, modeled, or prompted in the intervention, and was therefore over-aligned with the intervention targets. By contrast, an outcome was considered distal if it measured a skill that was not directly targeted in the intervention, and/or if the outcome was measured by a developmentally scaled assessment (e.g., the ADOS), following the assumption that such assessments tap broader learning within the targeted developmental domain. For example, if an intervention were to explicitly target, model, and prompt participants to say a set of five specific target words, an outcome which measured the use of those same five words would be coded as a proximal outcome. An outcome for the same intervention that measured expressive language using a standardized assessment would be coded as distal.
Outcomes were also categorized by their boundedness to the intervention context. Outcomes that were measured in a context identical to that of the intervention, or that differed from the intervention context on only one dimension (e.g., different assessor, materials, or activity) were coded as context-bound. Outcomes measured by a standardized instrument or that were measured in a context that differed from the intervention context across two or more dimensions were coded as generalized. In some cases, outcomes of parent-implemented interventions were measured by a standardized parent report assessment, and because it was not possible to know whether the parent completing the assessment was drawing on behaviors exhibited in a context sufficiently different from the intervention context, these outcomes were coded as potentially context-bound.
Parent/teacher training CME was considered high when caregivers or educators served as both the implementers of intervention and assessors of intervention outcomes (e.g., if a parent who was trained to implement the intervention also served as the interaction partner in an outcome measure for that intervention). Otherwise, parent/teacher training CME was considered low.
Effect size information.
Unadjusted post-intervention means, standard deviations, and ns were extracted for intervention and contrast groups. This information was used to calculate the standardized mean difference (d) between groups after intervention, which was then converted to Hedge’s g to correct for small sample sizes. Effect sizes were reflected as necessary so that higher effects consistently represented outcomes that favored the intervention group.
Reliability
Reliability was calculated for all studies in the primary meta-analysis using intraclass correlation coefficients (ICC) and unweighted kappa coefficients for continuous and categorical variables, respectively. Average kappa values across categorical variables included in the current paper ranged from 0.73-0.86, and ICCs across continuous variables ranged from 0.81-0.97. The aforementioned values reflect excellent reliability amongst coders for all variables of interest to the present report.
Preliminary Analyses
Variables were selected for moderator analyses if there were a sufficient number of studies reporting data on the putative moderator, and if there was theoretical and/or empirical justification for testing it. Prior to conducting moderator analyses, continuous predictors were plotted against effect sizes to determine whether linear meta-regression models were appropriate (e.g., rather than quadratic models), and categorical data were examined to ensure that multiple categories featured a minimum of five effect sizes per cell.
Primary Analyses
In order to account for the intercorrelation of multiple effect sizes extracted from single study samples, robust variance estimation (RVE) with small sample adjustments was used to conduct all summary effect estimation and meta-regression analyses using the R package Robumeta (Fisher, Tipton, & Zhipeng, 2017). Meta-regression analyses were conducted on all putative moderators that met preliminary analysis criteria for inclusion.
Results
Study Sample and Intervention Characteristics
A full list of included studies and coded sample and intervention characteristics is included in Supplementary Table S1, and a summary of sample and intervention characteristics across studies is presented in Table 1.
Table 1.
Features of Continuous and Categorical Moderators
| # of studies |
M (SD) | MIN | MAX | |
|---|---|---|---|---|
| Intervention Intensity | 12 | 555.8 (1126.5) | 8.3 | 3276 |
| Chronological Age | 27 | 38.7 (12.2) | 18.2 | 75.4 |
| Language Age | 10 | 20 (4.8) | 12 | 31.5 |
| Interventionist | ||||
| Educator | 6 | |||
| Caregiver | 11 | |||
| Clinician | 5 | |||
| Combination | 5 | |||
| Autism Symptomatology | ||||
| Moderate | 8 | |||
| High | 2 | |||
| Unreported | 17 | |||
| Outcome Proximity | ||||
| Proximal | 17 | |||
| Distal | 22 | |||
| Outcome Boundedness | ||||
| Context-bound | 110 | |||
| Generalized | 234 | |||
| PCB | 110 | |||
| Outcome Risk of CME | ||||
| High | 218 | |||
| Low | 234 |
Note. SD = standard deviation, PCB = potentially context-bound, CME = correlated measurement error related to parent/teacher training
RQ1. Quality of Evidence by Outcome Domain
From the 27 included studies of NDBIs, 454 total outcomes were extracted for analysis. Of these, 10 were coded as measures of overall autism symptomatology, 234 were coded as social communication outcomes, 12 were coded as restricted, repetitive patterns of behavior, interests, or activities outcomes, 12 were coded as adaptive outcomes, 26 were coded as cognitive outcomes, 80 were coded as language outcomes, 53 were coded as play outcomes, and 12 were coded as social emotional/challenging behavior. In addition, 2 were coded as brain-imaging data, 9 were coded as motor outcomes, and 4 were coded as ‘other’. Because less than five studies were represented for each of these three (i.e., brain-imaging, motor, and other) outcome domains, these outcomes were excluded from subgroup examination of quality indicators, but included in moderator analyses. No studies included sensory outcomes. Individual forest plots reflecting primary and summary effects for each outcome type that met the five study threshold are included in Supplementary Figures S1-S8.
Figure 2 depicts quality indicators and outcome attributes for included studies separated by outcome domain, for all domains for which we were able to estimate summary effects. By far, the majority of the evidence supports NDBI effects on social communication outcomes, and to a lesser extent, language, play, and cognition. In this section, we restrict our quality reporting to domains for which summary effect estimates were significant and positive. We designated 50% of intervention effects within a given domain being subject to a given threat as a threshold for identifying serious methodological concerns that limit our confidence in conclusions regarding these specific summary effect estimates. For social communication outcomes, 64% were threatened by detection bias, and 54% were threatened by parent/teacher CME. More than half of social communication outcomes were considered overly proximal to intervention targets (62%) and bound or potentially bound (55%) to intervention contexts. For language outcomes, 59% were potentially or clearly threatened by detection bias. For play outcomes, 71% were threatened by detection bias, and a majority of outcomes were coded as context-bound (67%) and proximal (73%). For cognition, none of the quality indicators met the threshold for serious methodological concerns.
Figure 2.

Quality Indicators for Included Studies
 Low risk of bias
Low risk of bias  Unclear risk of bias
Unclear risk of bias  High risk of bias
High risk of bias
RQ2. Moderator Analyses
Descriptives of continuous and categorical moderators are presented in Table 1, and detailed results of moderator analyses are presented in Table 2.
Table 2.
Results of Meta-regression Analyses
| Predictor | Studies | Outcomes | SE | t | df | p | |
|---|---|---|---|---|---|---|---|
| Model 1: Intervention Intensity | 12 | 265 | |||||
| Intercept | 0.28 | 0.11 | 2.54 | 7.07 | 0.038** | ||
| Cumulative intensity in hours | 0.09 | 0.12 | 0.75 | 1.33 | 0.563 | ||
| Model 2: Interventionist | 27 | 453 | |||||
| Intercept (Reference: Caregiver) | 0.34 | 0.09 | 3.98 | 12.57 | 0.002*** | ||
| Clinician | 0.12 | 0.19 | 0.67 | 4.42 | 0.539 | ||
| Combination | −0.26 | 0.19 | −1.37 | 6.71 | 0.215 | ||
| Educator | 0.01 | 0.16 | 0.09 | 7.30 | 0.931 | ||
| Model 3: Chronological Age | 27 | 453 | |||||
| Intercept | 0.31 | 0.06 | 4.93 | 24.04 | < 0.001*** | ||
| Age in Months | −0.06 | 0.05 | −1.22 | 8.08 | 0.256 | ||
| Model 4: Biological Sex | 25 | 417 | |||||
| Intercept | 0.33 | 0.06 | 5.19 | 18.50 | < 0.001*** | ||
| Percent Male | −0.06 | 0.05 | −1.36 | 9.30 | 0.204 | ||
| Model 5: Language Age | 10 | 228 | |||||
| Intercept | 0.34 | 0.09 | 3.84 | 7.44 | 0.006*** | ||
| Language Age Equivalency | −0.02 | 0.05 | −0.34 | 2.77 | 0.758 | ||
| Model 6: Outcome Boundedness | 27 | 453 | |||||
| Intercept (Reference: Context-bound) | 0.55 | 0.09 | 6.10 | 11.30 | < 0.001*** | ||
| Generalized | −0.40 | 0.11 | −3.53 | 15.00 | 0.003*** | ||
| Potentially Context-bound | −0.31 | 0.13 | −2.49 | 19.30 | 0.022** | ||
| Model 7: CME | 27 | 453 | |||||
| Intercept (Reference: High Risk) | 0.37 | 0.72 | 5.21 | 20.80 | < 0.001*** | ||
| Low Risk | −0.17 | 0.10 | −1.66 | 22.50 | 0.112 | ||
| Model 8: Outcome Proximity | 27 | 453 | |||||
| Intercept (Reference: Distal) | 0.20 | 0.08 | 2.40 | 17.20 | 0.028** | ||
| Proximal | 0.25 | 0.11 | 2.17 | 23.80 | 0.041** | ||
Note. CME = Correlated measurement error.
p < .01
p < .05
p < .10
Sample characteristics.
The results of meta-regression models indicated that neither the mean chronological age (B = −0.06, p = .256), nor the mean language age of samples at study entry (B = −0.02, p = .758), nor the reported percentage of males in each sample (B = −0.06, p = .204) moderated NDBI intervention effects. Because an insufficient number of participant samples with high autism symptomatology were represented (i.e., < 5), autism symptomatology categorization was excluded from moderation analyses.
Intervention characteristics.
Effect sizes did not significantly vary as a function of cumulative intensity of intervention in hours (B = 0.09, p = .563), or by the type of interventionist that implemented the intervention (clinician B = 0.12, p = .539; combination B = −0.26, p = .215; educator B = 0.01, p = .931; reference category = caregiver).
Outcome characteristics.
Effect sizes differed significantly as a function of both proximity and boundedness of the outcome to the intervention. Outcomes that were coded as proximal to the intervention had significantly larger effects (B = 0.25, p = 0.041) than those that were coded as distal. Compared to context-bound outcomes, effect sizes were significantly smaller for outcomes coded as generalized (B = −0.40, p = .003) or potentially context-bound (B = −0.31, p = .022). Figure 3 depicts summary effects for proximal and distal outcomes, and for context-bound, potentially context-bound, and generalized outcomes. Effect sizes for outcomes with a low risk of parent/teacher training CME were smaller on average than those with a high risk for CME, but this difference did not reach statistical significance (B = −0.17, p = .112).
Figure 3.
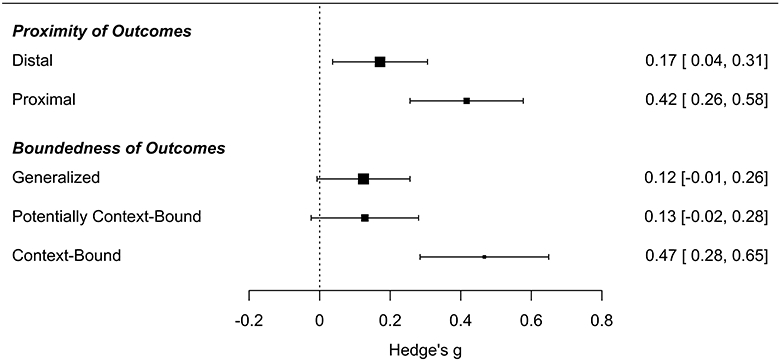
Forest Plot of Outcome Proximity and Boundedness
Discussion
NDBIs have recently amassed a substantial amount of evidence suggesting that they are a promising approach for supporting development in social communication, language, play, and cognition in young children with autism, and the quality of this evidence is relatively high in comparison with that of other intervention approaches commonly used to support development in this population (Sandbank et al., 2020a). However, the designation as promising comes with some caveats related to the nature of the outcomes and study quality concerns. Although a majority of the primary NDBI effects were not threatened by selection and attrition bias and were not derived from caregiver report measures, much of the evidence relies on outcomes that were threatened by high risk of detection bias and high risk of parent/teacher training CME. While we failed to find definitive evidence that parent/teacher training CME significantly inflates estimates of intervention effects, our summary estimates should be interpreted with these quality concerns in mind. In addition, nearly half of outcomes were proximal to intervention targets, and a majority were bound or potentially bound to the intervention context, which our findings suggest significantly influence intervention effect estimates. Thus, while NDBIs have certainly amassed enough evidence to warrant their use for supporting some core (i.e., social communication) and related (i.e., language, play, cognition) areas of need for children with autism, more high quality evidence is needed to ensure that the observed positive effects of NDBIs are not inflated as a result of study design and outcome measurement choices.
When considered without regard to quality, evidence suggests that NDBIs positively affect outcomes in the domains that are most frequently tracked in studies of these approaches. However, the magnitude of our summary estimates – particularly for social communication, language, and play – may have also been inflated by effects from outcomes that were context-bound, and/or threatened by detection bias and parent/teacher training CME. The substantial number of outcomes that were subject to all three of these potential risks of inflation reflects a common reliance on researcher-created observational measures collected during natural interactions with caregivers to index effects of parent-mediated interventions. In addition, while we did not find evidence to suggest that NDBIs are differentially effective according to chronological age, language age, and parent-reported sex composition of the study samples, or implementer or intensity of the intervention, discrepancies in reporting practices, limited power, and restricted range may have obscured true associations between these participant/intervention characteristics and intervention effectiveness. Future primary studies can use innovative research designs to further our understanding of the true impact of these participant and intervention characteristics on intervention effectiveness. Below, we further explore our findings in depth.
Understanding the Influence of Proximity, Boundedness, and Parent/Teacher Training CME
Outcome proximity.
We found that outcomes that measured skills that were highly proximal to intervention targets—that is, skills which were specifically and explicitly taught in the intervention—had significantly larger effects than outcomes coded as distal from intervention targets, although the summary effects for both were significantly different from zero (see Figure 3). This finding is unsurprising, given previous literature investigating the differential likelihood and size of effects for proximal versus distal dependent variables in early childhood autism interventions (Sandbank et al., 2020a; Yoder et al., 2013). Because NDBIs are intended to teach skills of developmental importance in early childhood with the intent of fostering broader development in downstream skills over time, it is important that investigations of this intervention approach include a robust representation of both proximal and distal outcomes, and ideally incorporate mediation analyses to link the two together in a developmental cascade. It is possible, though, that effects on distal outcomes for young children with autism may be present but undetectable for a substantial period of time following intervention. This possibility is supported by the developmental theory upon which NDBIs are, in part, based (Bornstein, Hahn, & Haynes, 2010; Masten & Cicchetti, 2010), as well as evidence from autism intervention research. A delayed effect on distal outcomes, for example, was observed in the landmark PACT study by Green and colleagues (2010; 2016), wherein a significant difference in autism symptom reduction between the intervention and control groups was not detected until follow-up measures were collected, six years after the cessation of a low-intensity parent-led intervention provided in early childhood. Thus, long-term follow-ups are likely necessary to thoroughly vet the theory of change for this intervention approach. Such studies will be time-consuming and costly, but should be a priority for researchers testing the efficacy of NDBIs for your children with autism and for funding agencies.
Outcome boundedness.
Intervention outcomes that were measured in the same or very similar context as the intervention had significantly larger effects than outcomes measured in contexts which differed from that of the intervention across two or more dimensions (i.e., interaction partner, interaction style, materials, and setting). Though it is expected that learned skills are most readily demonstrated in environments highly similar to the context in which the skills were taught, it is vital that the gains observed as a result of intervention be generalized to flexible and socially valid contexts for us to conclude that we have effected meaningful change for children with autism. Teaching generalization from intervention outset is a core tenet of NDBIs (Schreibman et al., 2015), and though the summary effect of NDBIs on generalized outcomes was positive, our findings suggest that further work is needed to increase intervention effects on generalized skills for young children with autism.
Parent/teacher training CME.
Although our results did not support the notion that NDBI effects were significantly inflated by the presence of parent/teacher training CME, this should not be interpreted as definitive proof that this quality indicator poses no threat to the validity of study results. Parent/teacher training CME arises from a change in the assessment context over the course of the study that may produce changes in the outcome that systematically favor the intervention group. Fundamentally, it is an instrumentation threat to validity. Given that this threat was present in approximately half of all outcomes in studies of NDBIs, and that this effect trended towards significance in the anticipated direction, any interpretation of summary effect estimates should give consideration to the potential influence of this and other more established quality indicators.
Measurement Considerations for Primary Research
Many researchers attempting to measure change affected by intervention believe that measures derived from naturalistic samples have more apparent construct validity, in that they are purportedly more likely to reflect changes that are generalized to unstructured contexts. Moreover, if the goal of a given intervention is to facilitate change in parent responsivity, measuring change during parent-child dyadic interactions is a natural choice. Unfortunately, because naturalistic interactions with caregivers serve as the primary intervention context for NDBIs, measures derived from these interactions likely reflect changes that are confined (or at least potentially confined) to that specific context (e.g., responsive play with parents). Improvements in the intervention group on such measures could reflect only transient change in the dyadic context driven by the caregiver’s increased responsivity attributable to training, rather than developmental change in the child that will generalize across communication partners and interaction styles. Our point is that demonstrating change within the context where such change was effected is only an initial step towards demonstrating that an intervention can induce change that extends beyond the context and targets of intervention. Researchers should avoid overstating the developmental ramifications of such findings, and instead interpret them as preliminary evidence establishing the theorized mechanisms of action, while acknowledging that these effects are potentially transient and subject to the risk of detection bias and parent/teacher training CME.
Future researchers that wish to guard against these risks while still relying on observational measures derived from naturalistic contexts can do so by ensuring the interaction partner within observational measures of child behavior is not trained in the intervention over the course of the study and is not aware of group assignment. For example, in a study examining the effects of a parent-led intervention to support symbolic play development, future researchers could collect observational measures of play using previously developed and validated semi-structured interactions with a naive examiner (e.g., the Developmental Play Assessment; Lifter, 2000; the Structured Play Assessment; Ungerer & Sigman, 1981). Although some studies have employed these types of measures (Boyd et al., 2018; Chang et al., 2016; Kasari et al., 2006), this approach is not yet the norm. Alternatively, researchers may derive observational measures from contexts that feature participants’ untrained teachers or peers as interaction partners (while ensuring they remain naive to group assignment over the course of the study). Yet another approach would be to retain measures of caregiver-child interactions, but use these for mediation analyses that would connect these proximal, context bound effects to developmentally distal and generalized child outcomes that are not threatened by parent/teacher training CME. Doing so would allow researchers to assess whether caregiver-child interactions are the substrate for downstream developmental achievements.
Null Findings
The effects of NDBIs did not vary according to any of the child or intervention characteristics that we hypothesized would moderate the magnitude of effects on outcomes of interest. Notably, summary effects were not moderated by child age at intervention onset. Although it is widely claimed that earlier intervention facilitates greater gains for children with autism, we did not find evidence to support this assertion. While it is possible that the overrepresentation of children aged 2-5 years may obscure a true linear relationship between age at intervention onset and intervention effectiveness, the results of this meta-analysis suggest that children who begin intervention at a later age may experience similar benefits from NDBIs as children who receive intervention starting at a younger age. The absence of this association does not mean that naturalistic interventions provided at early ages (e.g., 2-3 years) are not effective, as several studies included in this meta-analysis demonstrated that even very young children with autism benefitted from early intervention (Dawson et al., 2010; Drew et al., 2002; Estes et al., 2015; Wetherby & Woods, 2006). Rather, we failed to find evidence that the potential for developmental improvements facilitated by NDBIs decreases with advancing age, at least up to age 6 (the highest mean participant age documented in included studies).
We also did not find evidence that intervention effects varied as a function of cumulative intervention intensity. Given that we were unable to code intervention intensity for some studies due to differences in reporting practices, and that there was a risk of incorrect reporting of total intervention hours in studies of parent-implemented interventions, it is possible that measurement error may have limited our ability to detect a potentially true association between intervention intensity and intervention effectiveness. Alternatively, it is possible that NDBIs provided at lower intensities can facilitate substantial developmental gains in children with autism (Brian et al., 2017; Ingersoll, 2012; Kasari et al., 2008).
Finally, we did not find evidence that intervention effects significantly differed by the type of interventionist (e.g., caregiver, clinician, combination, etc). Recent meta-analyses examining the extent to which intervention effects on language and social communication vary according to the type of interventionist have mixed findings (Fuller & Kaiser, 2020; Hampton & Kaiser, 2016; Sandbank et al., 2020b), and the sole prior meta-analysis of NDBIs did not examine this question. Additional primary research might further explore this question by directly comparing caregiver- and clinician-mediated iterations of the same intervention. In the absence of clear evidence supporting added benefits dependent on intervention intensity, interventionist type, and age of intervention onset, clinician recommendations for early intervention should prioritize family-centered intervention approaches which balance the needs of the family and the young child (Sandall, McLean, & Smith, 2000; Sandbank, Bottema-Beutel, & Woynaroski, 2020). Recommendations for high-intensity clinician-led interventions should take into account the potential emotional and financial strain which can be caused when families are compelled to make excessive time commitments to intervention, coordinate the presence of professionals in their home, or interrupt their daily routines to travel to clinics. Intervention providers should consider what amount of intervention is developmentally appropriate for young children, recognizing that we do not yet have definitive empirical support for the notion that more is always better as it relates to NDBIs.
Alignment with Prior Meta-Analysis
Our findings replicate many of those reported in the only prior meta-analysis of NDBIs. Like those recently reported by Tiede and Walton (2019), our summary estimates support the notion that NDBIs have significant positive effects on language, play, and social communication for children with autism. In addition, we expanded on Tiede and Walton’s findings that lower quality studies yield larger effects than more methodologically rigorous ones, by examining specific outcome quality indicators (i.e., risk of parent/teacher training CME) and outcome characteristics (i.e., boundedness and proximity) as putative moderators of intervention effects.
However, in several cases our results depart from prior meta-analytic findings. For example, we did not replicate Tiede and Walton’s finding that NDBIs facilitate a significant reduction of autism symptomatology. This discrepancy may be attributable to the different measures of autism symptomatology represented in the two samples. A larger proportion of autism symptomatology outcomes in the Tiede & Walton meta-analysis were derived from parent report measures, which are at high risk of inflation due to detection bias. We also found little evidence to support the notion that increased intervention intensity was associated with larger intervention effects, which departs slightly from Tiede and Walton’s findings that dosage moderated intervention effects on joint attention (but not on other outcomes). This discrepancy may be due to our different characterization of intervention intensity, as Tiede and Walton only included hours of intervention delivered by trained research staff, while we included reported hours of intervention delivered by caregivers. Finally, while Tiede and Walton selected individual effect sizes from each included study, we employed RVE statistical methods that allowed for the inclusion of all 454 independent effect sizes extracted from the available pool of studies. Our inclusion of the full set of effect sizes contributes to a more precise picture of the state of the literature for this intervention approach.
Limitations
As is the case in any analysis of coded variables, measurement error related to coding is an acknowledged risk, though this risk was minimized by the extensive discrepancy resolution procedures applied to all codes and high interrater reliability in the present study. Additionally, we lacked the power to run more complex models or test various interactions of interest, such as the potential interaction between intervention intensity and outcome boundedness. Similarly, the precision of summary estimates and moderator analyses is limited by the volume and quality of the primary literature on NDBIs. For some target outcomes, such as play, effect sizes were sourced from a single or a small handful of named interventions, which somewhat limits the degree to which we can be confident in generalizing the results from these studies to the broader category of NDBIs. Even so, we do believe the estimates we have calculated are informative. It is notable as well that we were unable to calculate summary effects of NDBIs on a number of outcomes of interest, including brain-based outcomes and indices of sensory and motor function, as such measures have been underrepresented in studies conducted to date. Inclusion of broader neural and behavioral outcome measures is necessary to determine whether NDBIs have the potential to influence the wider range of domains known to be impacted by autism.
Future Primary Research
Future primary research should not only include a robust representation of outcomes that span the continua of boundedness and proximity, but should also endeavor to monitor long-term outcomes to determine whether and to what extent NDBIs lead to downstream developmental gains that are detectable later in life. It is also important that future investigators register or pre-register their clinical trials whenever possible, and distinguish between primary and secondary outcome variable(s) in registrations and trial reports.
In addition, NDBIs are package interventions, and the key components of these packages have yet to be identified. In other words, which components of NDBIs are most crucial and how each of these components affect children with various demographic and behavioral characteristics is currently unknown. The Sequential Multiple Assignment Randomized Trial (SMART) study design, which was developed specifically to help develop adaptive interventions (Almirall, Nahum-Shani, Sherwood, & Murphy, 2014), has been used by prior autism researchers to investigate whether adaptations to intervention or increases in intervention intensity can provide added benefit to children who did not initially appear to benefit from an NDBI (Kasari et al., 2014). Similarly, this study design should be used in future research to investigate whether certain aspects of NDBIs differentially benefit children who do not initially reach intervention goals. Thoughtful research design, incorporating elements such as pre-treatment measurement of child and family characteristics that may predict a differential response to treatment and midpoint measurement of theorized mechanisms of action, in combination with advanced analytic approaches to moderation and mediation analysis, also have great potential to advance our understanding of the subgroups for whom, and the mechanisms by which NDBIs work.
Conclusions
On the whole, NDBIs have accrued a substantial body of supporting evidence for their effects on some, but not all, of the core and related characteristics associated with autism, including social communication, language, play, and cognition. This body of evidence is relatively methodologically rigorous compared to that of other common intervention approaches for children on the spectrum. However, this evidence is nonetheless limited by some methodological concerns, including a prevalence of outcomes subject to high detection bias and parent/teacher training CME. The results of this analysis also support the use of proximity and boundedness as important indicators of outcome quality. Future research should incorporate both distal and generalized outcomes, in order to obtain a more robust understanding of the extent to which NDBIs affect durable, meaningful, and developmentally important changes that benefit children with autism.
Supplementary Material
Footnotes
Though it is relatively standard in journals and professional settings to use person-first language, such as “children with autism,” many autistic individuals have endorsed identity-first language, which incorporates autism as a component of their identity. Recently, scholars have advocated for the flexible use of identity-first and person-first language, and for the avoidance of terms that invoke unnecessary medicalization (e.g., ‘disorder’), to accommodate the diversity of experiences and opinions of autistic persons and others in the broader autism community, while acknowledging that person-first language may be appropriate for children, who are still in the process of constructing and discovering their identities (Robison, 2019).
We elected to use the term ‘parent-reported sex’ in lieu of ‘gender’, because although it is likely that none of the primary studies included in our analyses verified the biological sex of participants, most primary studies used the term ‘sex’ rather than ‘gender’, and we reasoned that most parents were likely reporting the child’s sex assigned at birth. We recognize that sex represents a construct that is distinct from gender and gender identity, and that such distinctions are important to make. We opted to use the terms ‘girl’ and ‘boy’ in lieu of ‘male’ and ‘female’ in order to avoid what might be perceived as unnecessarily clinical language to describe children with autism
Contributor Information
Jenna Crank, Special Education Department, The University of Texas at Austin.
Micheal Sandbank, Special Education Department, The University of Texas at Austin.
Kacie Dunham, Neuroscience Graduate Program, Vanderbilt University.
Shannon Crowley, Lynch School of Education and Human Development, Boston College.
Kristen Bottema-Beutel, Lynch School of Education and Human Development, Boston College.
Jacob I. Feldman, Department of Hearing and Speech Sciences, Vanderbilt University
Tiffany G. Woynaroski, Department of Hearing and Speech Sciences, Vanderbilt University Medical Center, Vanderbilt Brain Institute, Vanderbilt Kennedy Center, Frist Center for Autism and Innovation
References
* Indicates that studies were included in the meta-analysis
- Almirall D, Nahum-Shani I, Sherwood NE, & Murphy SA (2014). Introduction to SMART designs for the development of adaptive interventions: With application to weight loss research. Translational Behavioral Medicine, 4(3), 260–274. 10.1007/s13142-014-0265-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed). Arlington, VA: American Psychiatric Association. [Google Scholar]
- Antezana L, Factor RS, Condy EE, Strege MV, Scarpa A, & Richey JA (2019). Gender differences in restricted and repetitive behaviors and interests in youth with autism. Autism Research, 12(2), 274–283. [DOI] [PubMed] [Google Scholar]
- Baio J, Wiggins L, Christensen DL, Maenner MJ, Daniels J, Warren Z, … Yeargin-Allsopp M (2018). Prevalence of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveillance Summaries, 67(6), 6–13. 10.15585/mmwr.ss6513a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Begeer S, Mandell D, Wijnker-Holmes B, Venderbosch S, Rem D, Stekelenburg F, & Koot HM (2013). Sex differences in the timing of identification among children and adults with autism spectrum disorders. Journal of Autism and Developmental Disorders, 43(5), 1151–1156. [DOI] [PubMed] [Google Scholar]
- Ben-Itzchak E, & Zachor DA (2007). The effects of intellectual functioning and autism severity on outcomes of early behavioral intervention for children with autism. Research in Developmental Disabilities, 28(3), 287–303. [DOI] [PubMed] [Google Scholar]
- Ben-Sasson A, Hen L, Fluss R, Cermak S, Engel-Yeger B, & Gal E (2009). A meta-analysis of sensory modulation symptoms in individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 1–11. 10.1007/s10803-008-0593-3 [DOI] [PubMed] [Google Scholar]
- Bergen D (2002). The role of pretend play in children's cognitive development. Early Childhood Research & Practice, 4(1), 2–12. Retrieved from http://ecrp.uiuc.edu/v4n1/index.html. [Google Scholar]
- Bodfish JW, Symons FJ, Parker DE, & Lewis MH (2000). Varieties of repetitive behavior in autism: Comparisons to mental retardation. Journal of Autism and Developmental Disorders, 30(3), 237–243. 10.1023/A:1005596502855 [DOI] [PubMed] [Google Scholar]
- Bolton PF, Golding J, Emond A, & Steer CD (2012). Autism spectrum disorder and autistic traits in the Avon Longitudinal Study of Parents and Children: Precursors and early signs. Journal of the American Academy of Child & Adolescent Psychiatry, 51(3), 249–260. 10.1016/j.jaac.2011.12.009 [DOI] [PubMed] [Google Scholar]
- Bono MA, Daley T, & Sigman M (2004). Relations among joint attention, amount of intervention and language gain in autism. Journal of Autism and Developmental Disorders, 34(5), 495–505. [DOI] [PubMed] [Google Scholar]
- Bornstein MH, Hahn CS, & Haynes OM (2010). Social competence, externalizing, and internalizing behavioral adjustment from early childhood through early adolescence: Developmental cascades. Development and Psychopathology, 22(4), 717–735. 10.1017/S0954579410000416 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Boyd BA, Watson LR, Reszka SS, Sideris J, Alessandri M, Baranek GT, … & Belardi K (2018). Efficacy of the ASAP intervention for preschoolers with ASD: A cluster randomized controlled trial. Journal of Autism and Developmental Disorders, 48(9), 3144–3162. 10.1007/s10803-018-3584-z [DOI] [PubMed] [Google Scholar]
- *Brian JA, Smith IM, Zwaigenbaum L and Bryson SE (2017). Cross-site randomized control trial of the Social ABCs caregiver-mediated intervention for toddlers with autism spectrum disorder. Autism Research, 10(10), 1700–1711. doi: 10.1002/aur.1818 [DOI] [PubMed] [Google Scholar]
- *Brian J, Bernardi K, Dowds E, Easterbrook R, MacWilliam S, & Bryson S (2017). Feasibility of training early childhood educators in a community child care setting using a caregiver-mediated intervention for toddlers with autism spectrum disorder. Journal of Education and Training Studies, 5(5), 93–102. doi: 10.11114/jets.v5i5.2345 [DOI] [Google Scholar]
- Carter AS, Messinger DS, Stone WL, Celimli S, Nahmias AS, & Yoder P (2011). A randomized controlled trial of Hanen’s ‘More Than Words’ in toddlers with early autism symptoms. Journal of Child Psychology and Psychiatry, 52(7), 741–752. 10.1111/j.1469-7610.2011.02395.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Chang YC, Shire SY, Shih W, Gelfand C, & Kasari C (2016). Preschool deployment of evidence-based social communication intervention: JASPER in the classroom. Journal of Autism and Developmental Disorders, 46(6), 2211–2223. 10.1007/s10803-016-2752-2 [DOI] [PubMed] [Google Scholar]
- Charman T, Pickles A, Simonoff E, Chandler S, Loucas T, & Baird G (2011). IQ in children with autism spectrum disorders: Data from the Special Needs and Autism Project (SNAP). Psychological Medicine, 41(3), 619–627. 10.1017/S0033291710000991 [DOI] [PubMed] [Google Scholar]
- Cicchetti D, & Gunnar MR (2008). Integrating biological measures into the design and evaluation of preventive interventions. Development and Psychopathology, 20(3), 737–743. 10.1017/S0954579408000357 [DOI] [PubMed] [Google Scholar]
- *Dawson G, Rogers S, Munson J, Smith M, Winter J, Greenson J, … Varley J (2010). Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics, 125(1), e17–e23. 10.1542/peds.2009-0958 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Drew A, Baird G, Baron-Cohen S, Cox A, Slonims V, Wheelwright S, … Charman T (2002). A pilot randomised control trial of a parent training intervention for pre-school children with autism. European Child & Adolescent Psychiatry, 11(6), 266–272. 10.1007/s00787-002-0299-6 [DOI] [PubMed] [Google Scholar]
- *Duifhuis EA, Den Boer JC, Doornbos A, Buitelaar JK, Oosterling IJ, & Klip H (2017). The effect of pivotal response treatment in children with autism spectrum disorders: A non-randomized study with a blinded outcome measure. Journal of Autism and Developmental Disorders, 47(2), 231–242. 10.1007/s10803-016-2916-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eaves LC, & Ho HH (2004). The very early identification of autism: Outcome to age 4 1/2–5. Journal of Autism and Developmental Disorders, 34(4), 367–378. 10.1023/B:JADD.0000037414.33270.a8 [DOI] [PubMed] [Google Scholar]
- *Estes A, Munson J, Rogers SJ, Greenson J, Winter J, & Dawson G (2015). Long-term outcomes of early intervention in 6-year-old children with autism spectrum disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 54(7), 580–587. 10.1016/j.jaac.2015.04.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fernell E, Hedvall Å, Westerlund J, Carlsson LH, Eriksson M, Olsson MB, … & Gillberg C (2011). Early intervention in 208 Swedish preschoolers with autism spectrum disorder. A prospective naturalistic study. Research in Developmental Disabilities, 32(6), 2092–2101. [DOI] [PubMed] [Google Scholar]
- Fink RS (1976). Role of imaginative play in cognitive development. Psychological Reports, 39(3), 895–906. 10.2466/pr0.1976.39.3.895 [DOI] [Google Scholar]
- Fombonne E (2009). Epidemiology of pervasive developmental disorders. Pediatric Research, 65(6), 591. 10.1203/PDR.0b013e31819e7203 [DOI] [PubMed] [Google Scholar]
- Fuller EA, & Kaiser AP (2020). The Effects of Early Intervention on Social Communication Outcomes for Children with Autism Spectrum Disorder: A Meta-analysis. Journal of Autism and Developmental Disorders, 50(5), 1683–1700. 10.1007/s10803-019-03927-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goods KS, Ishijima E, Chang YC, & Kasari C (2013). Preschool based JASPER intervention in minimally verbal children with autism: Pilot RCT. Journal of Autism and Developmental Disorders, 43(5), 1050–1056. 10.1007/s10803-012-1644-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gordon K, Pasco G, McElduff F, Wade A, Howlin P, & Charman T (2011). A communication-based intervention for nonverbal children with autism: What changes? Who benefits? Journal of Consulting and Clinical Psychology, 79(4), 447–457. [DOI] [PubMed] [Google Scholar]
- Green J, Charman T, McConachie H, Aldred C, Slonims V, Howlin P, & Barrett B (2010). Parent-mediated communication-focused treatment in children with autism (PACT): A randomised controlled trial. The Lancet, 375(9732), 2152–2160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green RM, Travers AM, Howe Y, & McDougle CJ (2019). Women and autism spectrum disorder: Diagnosis and implications for treatment of adolescents and adults. Current Psychiatry Reports, 21(4), 22. [DOI] [PubMed] [Google Scholar]
- Grelotti DJ, & Kaptchuk TJ (2011). Placebo by proxy. BMJ (Clinical research ed.), 343, d4345. 10.1136/bmj.d4345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halfon N, Shulman E, & Hochstein M (2001). Brain development in early childhood. New York, NY: Worth Publishers. [Google Scholar]
- Hampton LH, & Kaiser AP (2016). Intervention effects on spoken-language outcomes for children with autism: A systematic review and meta-analysis. Journal of Intellectual Disability Research, 60(5), 444–463. [DOI] [PubMed] [Google Scholar]
- *Hardan AY, Gengoux GW, Berquist KL, Libove RA, Ardel CM, Phillips J, … Minjarez MB (2015). A randomized controlled trial of Pivotal Response Treatment Group for parents of children with autism. Journal of Child Psychology and Psychiatry, 56(8), 884–892. 10.1111/jcpp.12354 [DOI] [PubMed] [Google Scholar]
- Harrop C, Jones D, Zheng S, Nowell S, Schultz R, & Parish-Morris J (2019). Visual attention to faces in children with autism spectrum disorder: Are there sex differences?. Molecular Autism, 10(1), 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hemmeter ML, & Kaiser AP (1994). Enhanced Milieu Teaching: Effects of parent-implemented language intervention. Journal of Early Intervention, 18(3), 269–289. 10.1177/105381519401800303 [DOI] [Google Scholar]
- Hinkka-Yli-Salomäki S, Banerjee PN, Gissler M, Lampi KM, Vanhala R, Brown AS, & Sourander A (2014). The incidence of diagnosed autism spectrum disorders in Finland. Nordic Journal of Psychiatry, 68(7), 472–480. 10.3109/08039488.2013.861017 [DOI] [PubMed] [Google Scholar]
- *Howlin P, & Rutter M (1989), Mothers' speech to autistic children: A preliminary causal analysis. Journal of Child Psychology and Psychiatry, 30(6) 819–843. doi: 10.1111/j.1469-7610.1989.tb00285.x [DOI] [PubMed] [Google Scholar]
- *Ingersoll B (2012). Brief report: Effect of a focused imitation intervention on social functioning in children with autism. Journal of Autism and Developmental Disorders, 42(8), 1768–1773. 10.1007/s10803-011-1423-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Ingersoll B, Wainer AL, Berger NI, Pickard KE, & Bonter N (2016). Comparison of a self-directed and therapist-assisted telehealth parent-mediated intervention for children with ASD: A pilot RCT. Journal of Autism and Developmental Disorders, 46(7), 2275–2284. 10.1007/s10803-016-2755-z [DOI] [PubMed] [Google Scholar]
- Ingersoll BR, Wainer AL, Berger NI, & Walton KM (2017). Efficacy of low intensity, therapist-implemented Project ImPACT for increasing social communication skills in young children with ASD. Developmental Neurorehabilitation, 20(8), 502–510. 10.1080/17518423.2016.1278054 [DOI] [PubMed] [Google Scholar]
- Itzchak EB, & Zachor DA (2011). Who benefits from early intervention in autism spectrum disorders?. Research in Autism Spectrum Disorders, 5(1), 345–350. [Google Scholar]
- Jarrold C, Boucher J, & Smith P (1993). Symbolic play in autism: A review. Journal of Autism and Developmental Disorders, 23(2), 281–307. 10.1007/BF01046221 [DOI] [PubMed] [Google Scholar]
- *Jocelyn LJ, Casiro OG, Beattie D, Bow J, & Kneisz J (1998). Treatment of children with autism: A randomized controlled trial to evaluate a caregiver-based intervention program in community day-care centers. Journal of Developmental and Behavioral Pediatrics, 19(5), 326–334. 10.1097/00004703-199810000-00002 [DOI] [PubMed] [Google Scholar]
- *Kaale A, Fagerland MW, Martinsen EW, & Smith L (2014). Preschool-based social communication treatment for children with autism: 12-month follow-up of a randomized trial. Journal of the American Academy of Child & Adolescent Psychiatry, 53(2), 188–198. 10.1016/j.jaac.2013.09.019 [DOI] [PubMed] [Google Scholar]
- Kaiser AP (1994). Enhanced Milieu Teaching: An analysis of applications by interventionists and classroom teachers. Paper presented at the Annual Meeting of the American Association on Mental Retardation, Boston, MA, 1994. [Google Scholar]
- Kanne SM, Gerber AJ, Quirmbach LM, Sparrow SS, Cicchetti DV, & Saulnier CA (2011). The role of adaptive behavior in autism spectrum disorders: Implications for functional outcome. Journal of Autism and Developmental Disorders, 41(8), 1007–1018. [DOI] [PubMed] [Google Scholar]
- *Kasari C, Lawton K, Shih W, Barker TV, Landa R, Lord C, … Senturk D (2014). Caregiver-mediated intervention for low-resourced preschoolers with autism: An RCT. Pediatrics, 134(1), e72–e79. 10.1542/peds.2013-3229 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Kasari C, Paparella T, Freeman S, & Jahromi LB (2008). Language outcome in autism: Randomized comparison of joint attention and play interventions. Journal of Consulting and Clinical Psychology, 76(1), 125–137. https://psycnet.apa.org/doi/10.1037/0022-006X.76.1.125 [DOI] [PubMed] [Google Scholar]
- Kim YS, Leventhal BL, Koh YJ, Fombonne E, Laska E, Lim EC, & Song DH (2011). Prevalence of autism spectrum disorders in a total population sample. American Journal of Psychiatry, 168(9), 904–912. [DOI] [PubMed] [Google Scholar]
- Koegel LK, Koegel RL, Harrower JK, & Carter CM (1999). Pivotal response intervention: Overview of approach. Journal of the Association for Persons with Severe Handicaps, 24(3), 174–185. 10.2511/rpsd.24.3.174 [DOI] [Google Scholar]
- Kreiser NL, & White SW (2014). ASD in females: Are we overstating the gender difference in diagnosis?. Clinical child and family psychology review, 17(1), 67–84. [DOI] [PubMed] [Google Scholar]
- Lai MC, Lombardo MV, Auyeung B, Chakrabarti B, & Baron-Cohen S (2015). Sex/gender differences and autism: Setting the scene for future research. Journal of the American Academy of Child & Adolescent Psychiatry, 54(1), 11–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Landa RJ, Holman KC, O’Neill AH, & Stuart EA (2011). Intervention targeting development of socially synchronous engagement in toddlers with autism spectrum disorder: A randomized controlled trial. Journal of Child Psychology and Psychiatry, 52(1), 13–21. 10.1111/j.1469-7610.2010.02288.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Lawton K, & Kasari C (2012). Brief report: Longitudinal improvements in the quality of joint attention in preschool children with autism. Journal of Autism and Developmental Disorders, 42(2), 307–312. 10.1007/s10803-011-1231-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lifter K (2000). Linking assessment to intervention for children with developmental disabilities or at-risk for developmental delay: The developmental play assessment (DPA) instrument. Play Diagnosis and Assessment, 2, 228–261. [Google Scholar]
- Lillard AS, Pinkham AM, & Smith E (2011). Pretend play and cognitive development. In Goswami U (Ed.), Handbook of cognitive development (296-303). Oxford, Oxon: Blackwell Publishing [Google Scholar]
- Lord C (1995). Follow-up of two-year-olds referred for possible autism. Journal of Child Psychology and Psychiatry, 36(8), 1365–1382. 10.1111/j.1469-7610.1995.tb01669.x [DOI] [PubMed] [Google Scholar]
- Lord C, Rutter M, DiLavore P, Risi S, Gotham K, & Bishop S (2012). Autism diagnostic observation schedule–2nd edition (ADOS-2). Los Angeles, CA: Western Psychological Corporation. [Google Scholar]
- Loveland KA (2005). Social-emotional impairment and self-regulation in autism spectrum. In Nadel J & Muir D (Eds.), Emotional development: Recent research advances, (365-370). New York, NY: Oxford University Press. [Google Scholar]
- Loveland KA, & Landry SH (1986). Joint attention and language in autism and developmental language delay. Journal of Autism and Developmental Disorders, 16(3), 335–349. 10.1007/BF01531663 [DOI] [PubMed] [Google Scholar]
- Makrygianni MK, & Reed P (2010). A meta-analytic review of the effectiveness of behavioural early intervention programs for children with autistic spectrum disorders. Research in Autism Spectrum Disorders, 4(4), 577–593. [Google Scholar]
- Mundkur N (2005). Neuroplasticity in children. The Indian Journal of Pediatrics, 72(10), 855–857. 10.1007/BF02731115 [DOI] [PubMed] [Google Scholar]
- National Institute of Child Health and Human Development. (2017). Early intervention for autism. https://www.nichd.nih.gov/health/topics/autism/conditioninfo/treatments/early-intervention#f7.
- National Research Council. (2001). Characteristics of effective interventions. In Lord C & Mcgee JP (Eds.), Educating children with autism (6). Washington, DC: National Academic Press. [Google Scholar]
- *Nefdt N, Koegel R, Singer G, & Gerber M (2010). The use of a self-directed learning program to provide introductory training in pivotal response treatment to parents of children with autism. Journal of Positive Behavior Interventions, 12(1), 23–32. 10.1177/1098300709334796 [DOI] [Google Scholar]
- Perry A, Cummings A, Geier JD, Freeman NL, Hughes S, Managhan T, … & Williams J (2011). Predictors of outcome for children receiving intensive behavioral intervention in a large, community-based program. Research in Autism Spectrum Disorders, 5(1), 592–603. [Google Scholar]
- Pickles A, Le Couteur A, Leadbitter K, Salomone E, Cole-Fletcher R, Tobin H, … Green J (2016). Parent-mediated social communication therapy for young children with autism (PACT): Long-term follow-up of a randomised controlled trial. The Lancet, 388(10059), 2501–2509. 10.1016/S0140-6736(16)31229-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reichow B, Hume K, Barton EE, & Boyd BA (2018). Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). The Cochrane Database of Systematic Reviews, 5(5), CD009260. doi: 10.1002/14651858.CD009260.pub3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reichow B, & Wolery M (2009). Comprehensive synthesis of early intensive behavioral interventions for young children with autism based on the UCLA young autism project model. Journal of Autism and Developmental Disorders, 39(1), 23. [DOI] [PubMed] [Google Scholar]
- Roberts MY, & Kaiser AP (2011). The effectiveness of parent-implemented language interventions: A meta-analysis. American Journal of Speech-Language Pathology, 20(3), 180–199. 10.1044/1058-0360(2011/10-0055) [DOI] [PubMed] [Google Scholar]
- *Roberts J, Williams K, Carter M, Evans D, Parmenter T, Silove N, … Warren A (2011). A randomised controlled trial of two early intervention programs for young children with autism: Centre-based with parent program and home-based. Research in Autism Spectrum Disorders, 5(4), 1553–1566. 10.1016/j.rasd.2011.03.001 [DOI] [Google Scholar]
- Rogers SJ, & Dawson G (2010). Early Start Denver Model for young children with autism: Promoting language, learning, and engagement. New York, NY: Guilford Press. [Google Scholar]
- Rogers SJ, & DiLalla DL (1991). A comparative study of the effects of a developmentally based instructional model on young children with autism and young children with other disorders of behavior and development. Topics in Early Childhood Special Education, 11(2), 29–47. 10.1177/027112149101100205 [DOI] [Google Scholar]
- *Rogers SJ, Estes A, Lord C, Vismara L, Winter J, Fitzpatrick, … Dawson G (2012). Effects of a brief Early Start Denver Model (ESDM)–based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 51(10), 1052–1065. 10.1016/j.jaac.2012.08.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Rogers SJ, Hayden D, Hepburn S, Charlifue-Smith R, Hall T, & Hayes A (2006). Teaching young nonverbal children with autism useful speech: A pilot study of the Denver model and PROMPT interventions. Journal of Autism and Developmental Disorders, 36(8), 1007–1024. 10.1007/s10803-006-0142-x [DOI] [PubMed] [Google Scholar]
- Rogers SJ, & Lewis HAL (1989). An effective day treatment model for young children with pervasive developmental disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 28(2), 207–214. 10.1097/00004583-198903000-00010 [DOI] [PubMed] [Google Scholar]
- Ruben RJ (1997). A time frame of critical/sensitive periods of language development. Acta Oto-laryngologica, 117(2), 202–205. 10.3109/00016489709117769 [DOI] [PubMed] [Google Scholar]
- Saemundsen E, Magnússon P, Georgsdóttir I, Egilsson E, & Rafnsson V (2013). Prevalence of autism spectrum disorders in an Icelandic birth cohort. BMJ Open, 3(6), e002748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sallows GO, & Graupner TD (2005). Intensive behavioral treatment for children with autism: Four-year outcome and predictors. American Journal on Mental Retardation, 110(6), 417–438. [DOI] [PubMed] [Google Scholar]
- Sandall S, McLean ME, & Smith BJ (2000). Recommended practices in family-based practices. In DEC recommended practices in early intervention/early childhood special education (39-44). Longmont, CO: Sopris West. [Google Scholar]
- Sandbank M, Bottema-Beutel K, Crowley S, Cassidy M, Dunham K, Feldman JI, … Woynaroski TG (2020a). Project AIM: Autism intervention meta-analysis for studies of young children. Psychological Bulletin, 146(1), 1–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sandbank M, Bottema-Beutel K, Crowley S, Cassidy M, Feldman JI, Canihuante M, & Woynaroski T (2020b). Intervention Effects on Language in Children With Autism: A Project AIM Meta-Analysis. Journal of Speech, Language, and Hearing Research, 63, 1537–1560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sandbank M, Bottema-Beutel K, & Woynaroski T (2020). Intervention recommendations for children with autism in light of a changing evidence base. JAMA Pediatrics. 10.1001/jamapediatrics.2020.4730 [DOI] [PubMed] [Google Scholar]
- Schreibman L, Dawson G, Stahmer AC, Landa R, Rogers SJ, McGee GG, … Halladay A (2015). Naturalistic developmental behavioral interventions: Empirically validated treatments for autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(8), 2411–2428. 10.1007/s10803-015-2407-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schreibman LE, Dufek S, & Cunningham AB (2011). Identifying moderators of treatment outcome for children with autism. In Matson JL & Sturmey P (Eds.), International handbook of autism and pervasive developmental disorders (295-305). New York, NY: Springer. [Google Scholar]
- Schreibman L, & Koegel RL (1996). Fostering self-management: Parent-delivered pivotal response training for children with autistic disorder. In Hibbs ED & Jensen PS (Eds.), Psychosocial treatments for child and adolescent disorders: Empirically based strategies for clinical practice (525–552). Washington, DC: American Psychological Association. 10.1037/10196-020 [DOI] [Google Scholar]
- *Schreibman L, & Stahmer AC (2014). A randomized trial comparison of the effects of verbal and pictorial naturalistic communication strategies on spoken language for young children with autism. Journal of Autism and Developmental Disorders, 44(5), 1244–1251. 10.1007/s10803-013-1972-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Shire SY, Chang YC, Shih W, Bracaglia S, Kodjoe M, & Kasari C (2017). Hybrid implementation model of community-partnered early intervention for toddlers with autism: A randomized trial. Journal of Child Psychology and Psychiatry, 58(5), 612–622. 10.1111/jcpp.12672 [DOI] [PubMed] [Google Scholar]
- Surén P, Bakken IJ, Aase H, Chin R, Gunnes N, Lie KK, … & Stoltenberg C (2012). Autism spectrum disorder, ADHD, epilepsy, and cerebral palsy in Norwegian children. Pediatrics, 130(1), e152–e158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tiede G, & Walton KM (2019). Meta-analysis of naturalistic developmental behavioral interventions for young children with autism spectrum disorder. Autism, 23(8), 2080–2095. 10.1177/1362361319836371 [DOI] [PubMed] [Google Scholar]
- Ungerer JA, & Sigman M (1981). Symbolic play and language comprehension in autistic children. Journal of the American Academy of Child Psychiatry, 20(2), 318–337. [DOI] [PubMed] [Google Scholar]
- Virués-Ortega J (2010). Applied behavior analytic intervention for autism in early childhood: Meta-analysis, meta-regression and dose–response meta-analysis of multiple outcomes. Clinical Psychology Review, 30(4), 387–399. 10.1016/j.cpr.2010.01.008 [DOI] [PubMed] [Google Scholar]
- *Vivanti G, Paynter J, Duncan E, Fothergill H, Dissanayake C, Rogers SJ, & Victorian ASELCC Team. (2013). Effectiveness and feasibility of the Early Start Denver Model implemented in a group-based community childcare setting. Journal of Autism and Developmental Disorders, 44(12), 3140–3153. 10.1007/s10803-014-2168-9 [DOI] [PubMed] [Google Scholar]
- Vivanti G, Prior M, Williams K, & Dissanayake C (2014). Predictors of outcomes in autism early intervention: Why don’t we know more?. Frontiers in Pediatrics, 2, 58. doi: 10.3389/fped.2014.00058 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Wetherby AM, & Woods JJ (2006). Early social interaction project for children with autism spectrum disorders beginning in the second year of life: A preliminary study. Topics in Early Childhood Special Education, 26(2), 67–82. 10.1177/02711214060260020201 [DOI] [Google Scholar]
- Wolff JJ, Botteron KN, Dager SR, Elison JT, Estes AM, Gu H, … IBIS Network (2014). Longitudinal patterns of repetitive behavior in toddlers with autism. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 55(8), 945–953. doi: 10.1111/jcpp.12207 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yoder P, & Stone WL (2006). Randomized comparison of two communication interventions for preschoolers with autism spectrum disorders. Journal of Consulting and Clinical Psychology, 74(3), 426–435. [DOI] [PubMed] [Google Scholar]
- Yoder PJ, Bottema-Beutel K, Woynaroski T, Chandrasekhar R, & Sandbank M (2013). Social communication intervention effects vary by dependent variable type in preschoolers with autism spectrum disorders. Evidence-based Communication Assessment and Intervention, 7(4), 150–174. 10.1080/17489539.2014.917780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yoder PJ, Estes A, Warren Z & Rogers S (November, 2018). More treatment is better only for children with mild autism symptoms. Paper given at American Speech Language Hearing Association, Boston, MA. [Google Scholar]
- Yoder PJ, Warren Z, Estens A, McEachin J & Rogers S (May, 2019). Evidence that more treatment is better only for children with mild autism symptoms. Poster given at the International Society for Autism Research, Montreal, CA. [Google Scholar]
- Zwaigenbaum L, Bauman ML, Stone WL, Yirmiya N, Estes A, Hansen RL, … Kasari C (2015). Early identification of autism spectrum disorder: Recommendations for practice and research. Pediatrics, 136(1), S10–S40. 10.1542/peds.2014-3667C [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.