Abstract
BACKGROUND:
The American Heart Association, in conjunction with the National Institutes of Health, annually reports the most up-to-date statistics related to heart disease, stroke, and cardiovascular risk factors, including core health behaviors (smoking, physical activity, diet, and weight) and health factors (cholesterol, blood pressure, and glucose control) that contribute to cardiovascular health. The Statistical Update presents the latest data on a range of major clinical heart and circulatory disease conditions (including stroke, congenital heart disease, rhythm disorders, subclinical atherosclerosis, coronary heart disease, heart failure, valvular disease, venous disease, and peripheral artery disease) and the associated outcomes (including quality of care, procedures, and economic costs).
METHODS:
The American Heart Association, through its Epidemiology and Prevention Statistics Committee, continuously monitors and evaluates sources of data on heart disease and stroke in the United States to provide the most current information available in the annual Statistical Update with review of published literature through the year before writing. The 2023 Statistical Update is the product of a full year’s worth of effort in 2022 by dedicated volunteer clinicians and scientists, committed government professionals, and American Heart Association staff members. The American Heart Association strives to further understand and help heal health problems inflicted by structural racism, a public health crisis that can significantly damage physical and mental health and perpetuate disparities in access to health care, education, income, housing, and several other factors vital to healthy lives. This year’s edition includes additional COVID-19 (coronavirus disease 2019) publications, as well as data on the monitoring and benefits of cardiovascular health in the population, with an enhanced focus on health equity across several key domains.
RESULTS:
Each of the chapters in the Statistical Update focuses on a different topic related to heart disease and stroke statistics.
CONCLUSIONS:
The Statistical Update represents a critical resource for the lay public, policymakers, media professionals, clinicians, health care administrators, researchers, health advocates, and others seeking the best available data on these factors and conditions.
Keywords: AHA Scientific Statements, cardiovascular diseases, epidemiology, risk factors, statistics, stroke
SUMMARY
Each year, the American Heart Association, in conjunction with the National Institutes of Health and other government agencies, brings together in a single document the most up-to-date statistics related to heart disease, stroke, and cardiovascular risk factors in the AHA’s Life’s Essential 8 (Figure),1 which include core health behaviors (smoking, physical activity, diet, and weight) and health factors (cholesterol, blood pressure, and glucose control) that contribute to cardiovascular health. The Statistical Update represents a critical resource for the lay public, policymakers, media professionals, clinicians, health care administrators, researchers, health advocates, and others seeking the best available data on these factors and conditions. Cardiovascular disease produces immense health and economic burdens in the United States and globally. The Statistical Update also presents the latest data on a range of major clinical heart and circulatory disease conditions (including stroke, congenital heart disease, rhythm disorders, subclinical atherosclerosis, coronary heart disease, heart failure, valvular heart disease, venous disease, and peripheral artery disease) and the associated outcomes (including quality of care, procedures, and economic costs). Since 2007, the annual versions of the Statistical Update have been cited >20 000 times in the literature.
Figure. AHA’s My Life Check—Life’s Essential 8.

Source: Reprinted from Lloyd-Jones et al.1 Copyright © 2022, American Heart Association, Inc.
Each annual version of the Statistical Update undergoes revisions to include the newest nationally representative available data, add additional relevant published scientific findings, remove older information, add new sections or chapters, and increase the number of ways to access and use the assembled information. This year-long process, which begins as soon as the previous Statistical Update is published, is performed by the AHA Statistics Committee faculty volunteers and staff and government agency partners. Below are a few highlights from this year’s Statistical Update. Please see each chapter for references, confidence intervals for statistics reported below, and additional information.
Cardiovascular Health (Chapter 2)
From 2013 to March 2020, the overall CVH score combining health scores of all 8 components of the Life’s Essential 8 was, on average, 73.6 for all US children between 16 and 19 years of age. The corresponding mean overall CVH score was 78.4 for NH Asian, 74.1 for NH White, and 71.3 for NH Black children. During the same period, the mean overall CVH score was 65.2 for all US adults, with a mean score of 69.6 for NH Asian, 66.0 for NH White, and 59.7 for NH Black adults.
A report based on data from the UK Biobank found that having ideal CVH over poor CVH attenuated the all-cause and cardiometabolic disease–related mortality for males and females and was associated with life expectancy gains of 5.50 years for males and 4.20 years for females, at an index age of 45 years, among participants with cardiometabolic diseases and correspondingly 4.55 years in males and 4.89 years in females for people without cardiometabolic diseases.
As of July 1, 2022, the cumulative number of COVID-19 (coronavirus disease 2019) deaths in the United States was 1 014 620, which equates to ≈306 deaths per 100 000 people. In metropolitan areas in the United States, the cumulative COVID-19 death rate was ≈292 deaths per 100 000 compared with ≈392 deaths per 100 000 in nonmetropolitan areas. In US counties with a high percentage (>17.3%) of the population in poverty, the cumulative COVID-19 death rate was ≈394 deaths per 100 000 compared with ≈248 deaths per 100 000 in counties with a low percentage (0.0%–12.3%) of the population that is living in poverty. As a result of the high COVID-19 mortality rates, life expectancy (at birth) in the United States decreased from 78.8 years in 2019 to 77.0 years in 2020 (−1.8 years) overall, and the corresponding life expectancy decreased from 76.3 to 74.2 years (−2.1 years) in males and decreased from 81.4 to 79.9 years (−1.5 years) in females.
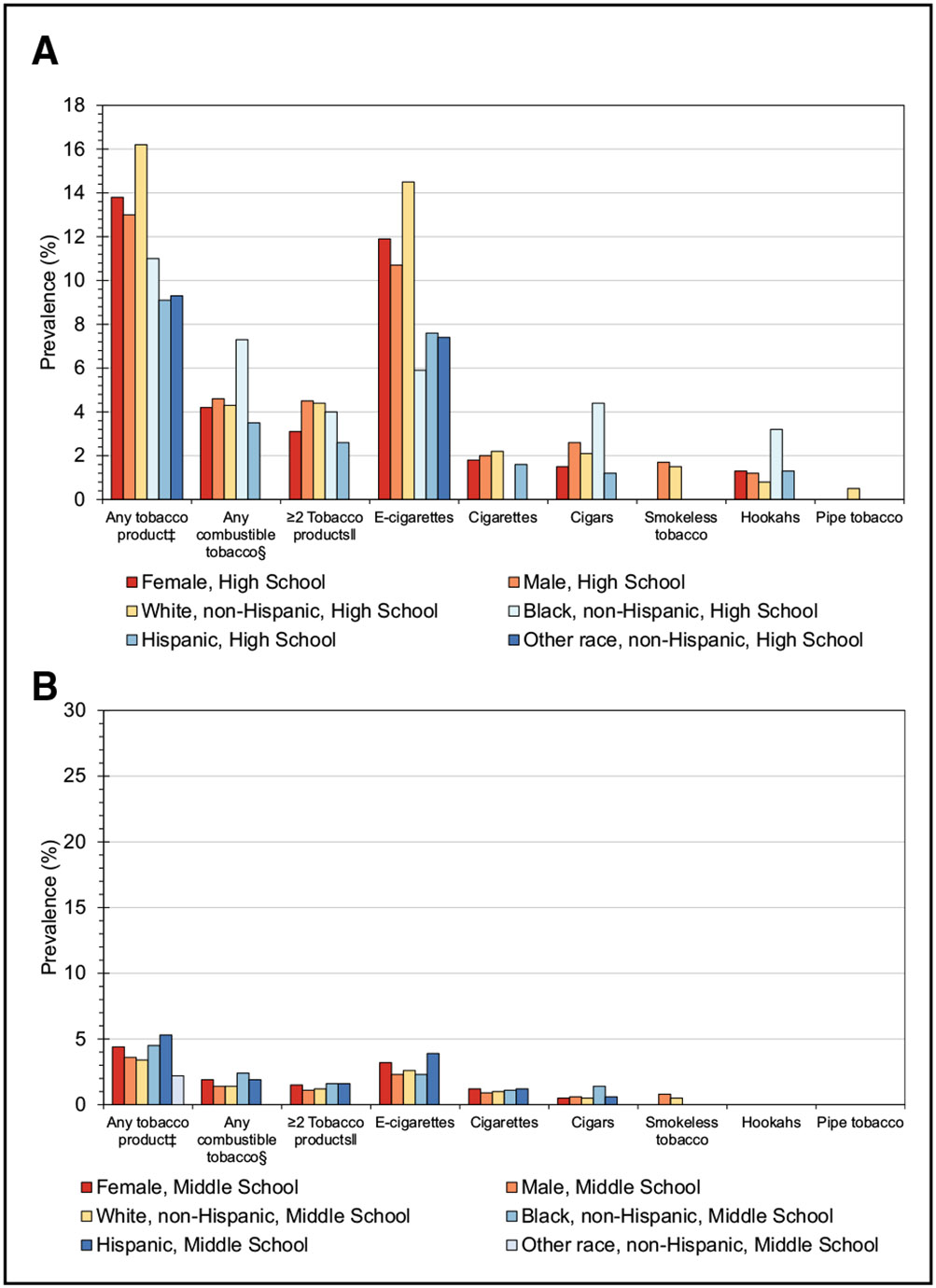
Smoking/Tobacco Use (Chapter 3)
The prevalence of cigarette use in the past 30 days among middle and high school students in the United States was 1.0% and 1.9%, respectively, in 2021.
Although there has been a consistent decline in adult and youth cigarette use in the United States in the past 2 decades, significant disparities persist. In 2020, substantially higher tobacco use prevalence rates were observed in American Indian/Alaska Native and lesbian, gay, and bisexual adults compared with White and heterosexual/straight adults (27.1% American Indian/Alaska Native versus 13.3% White; 16.1% lesbian, gay, and bisexual versus 12.3% heterosexual/straight adults).
Electronic cigarettes were the most commonly used tobacco product among adolescents in 2021; the prevalence of use in the past 30 days among middle and high school students in the United States was 2.8% and 11.3%, respectively, with the majority of adolescent users using flavored electronic cigarettes (85.8% of high school students and 79.2% of middle school students).
Physical Activity and Sedentary Behavior (Chapter 4)
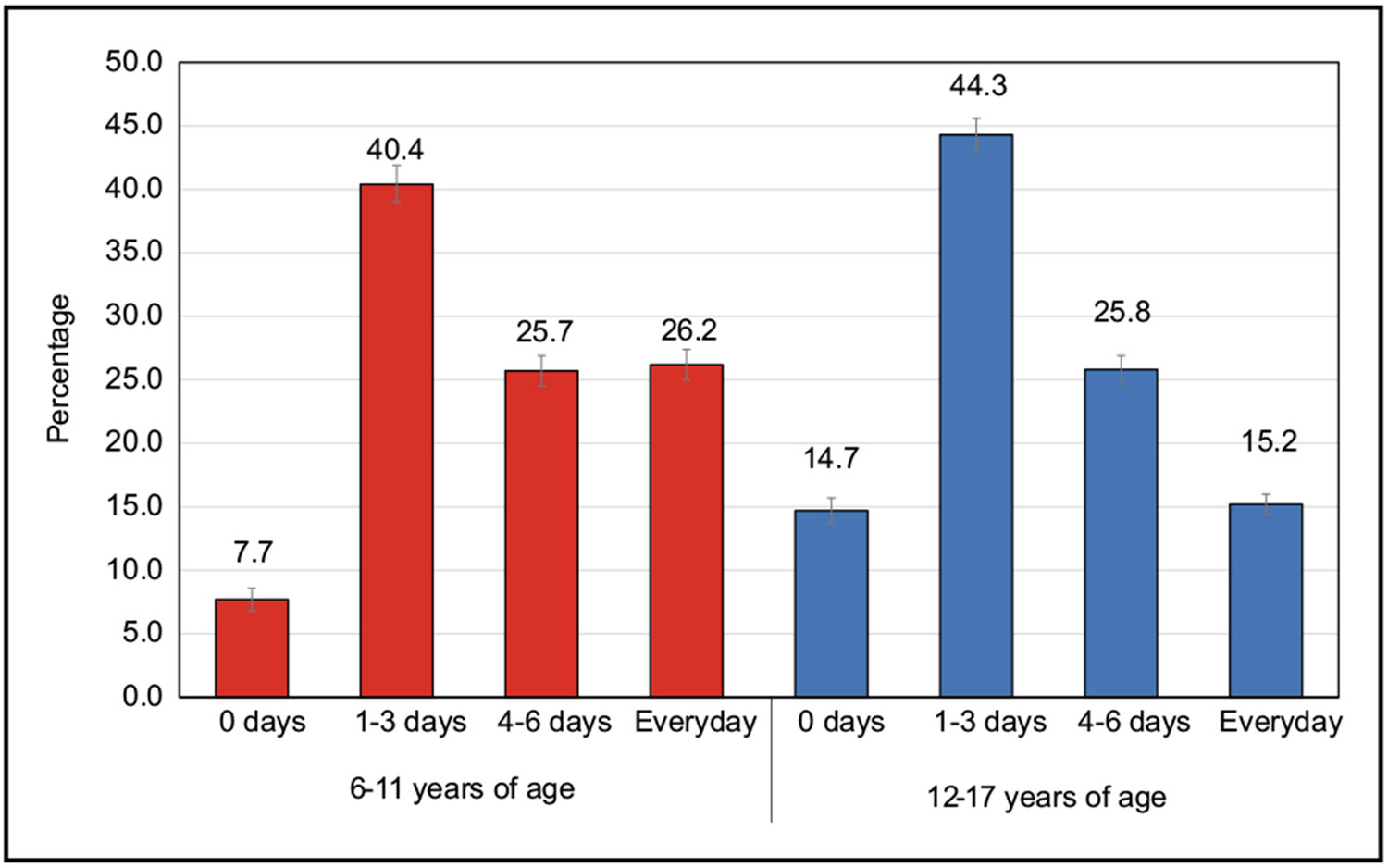
According to parental report in 2019 to 2020, the nationwide prevalence of youth 6 to 17 years of age who were active ≥60 minutes every day of the week was 20.6%.
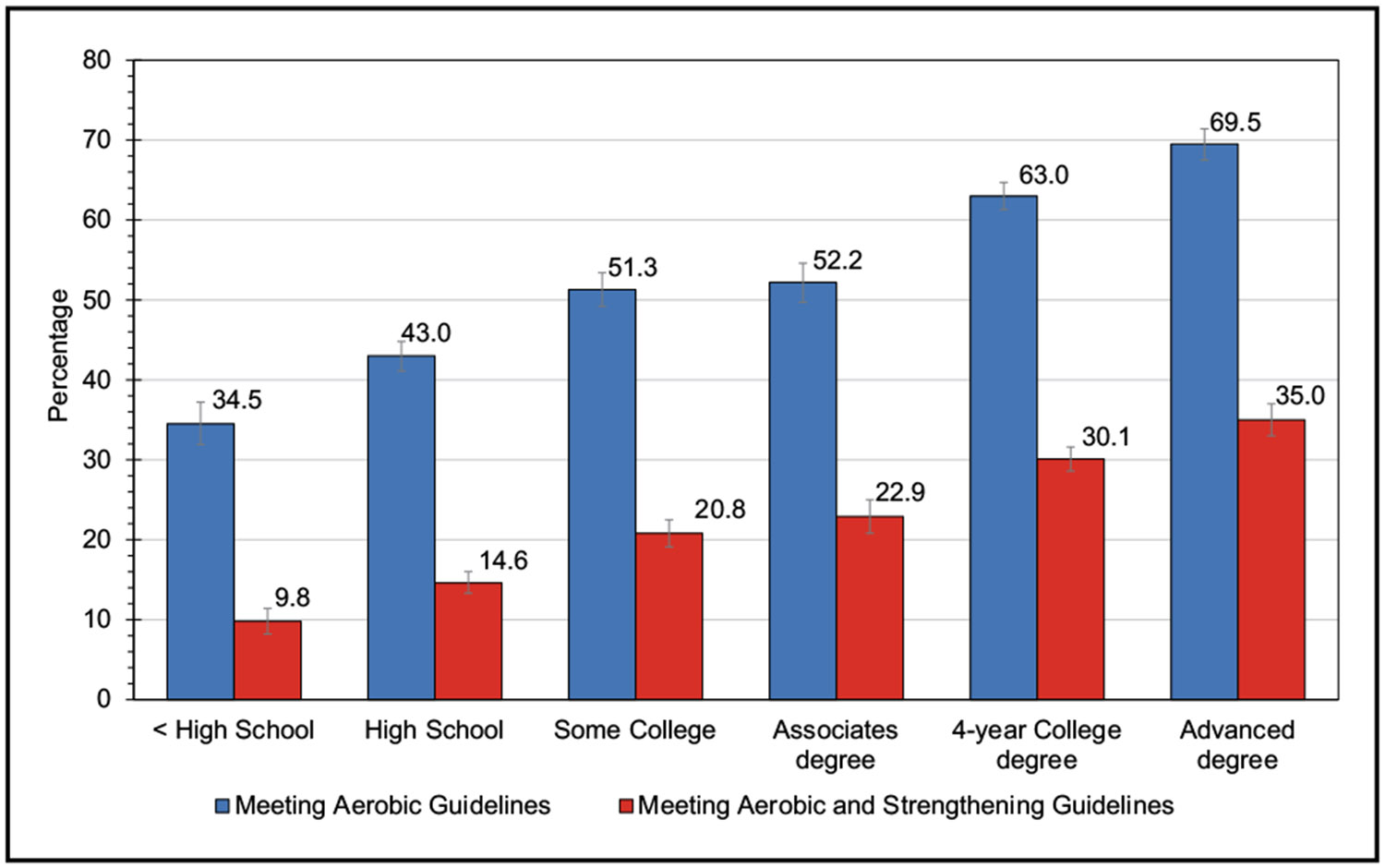
According to self-report in 2018, the age-adjusted proportion of adults who reported meeting the aerobic PA guidelines for Americans (≥150 min/wk of moderate PA, ≥75 min/wk of vigorous PA, or an equivalent combination of the two) through leisure-time activities was 54.2%.
Among 67 762 adults with >20 years of follow-up, 8.7% of all-cause mortality was attributed to a PA level of <150 min/wk of moderate-intensity PA.
Nutrition (Chapter 5)
The first study to use the AHA’s Life’s Essential 8 to quantify the CVH levels of adults and children in the United States included data from 23 409 individuals 2 through 79 years of age (13 521 adults and 9888 children) participating in NHANES (National Health and Nutrition Examination Survey). The adults in the study population represent 201 728 000 adults, and the children in the study represent 74 435 000 children. The composite CVH score ranges from 0 (lowest) to 100 (highest). Of the 8 metrics, diet was among the 4 with the lowest scores. The range of scores for diet across demographic groups was 23.8 to 47.7. Among children 2 to 5 years of age, a mean diet score of 61.1 was observed. The score for children 12 to 19 years of age was 28.5.
A meta-analysis of 38 prospective cohort studies showed that the relative risk (RR) for the highest versus the lowest categories of Mediterranean diet adherence was 0.79 for total CVD mortality, 0.73 for CHD incidence, 0.83 for CHD mortality, 0.80 for stroke incidence, 0.87 for stroke mortality, and 0.73 for myocardial infarction incidence.
Compared with a usual Western diet, a Dietary Approaches to Stop Hypertension–type dietary pattern with low sodium reduced systolic blood pressure (SBP) by 5.3, 7.5, 9.7, and 20.8 mm Hg in adults with baseline SBP <130, 130 to 139, 140 to 149, and ≥150 mm Hg, respectively.
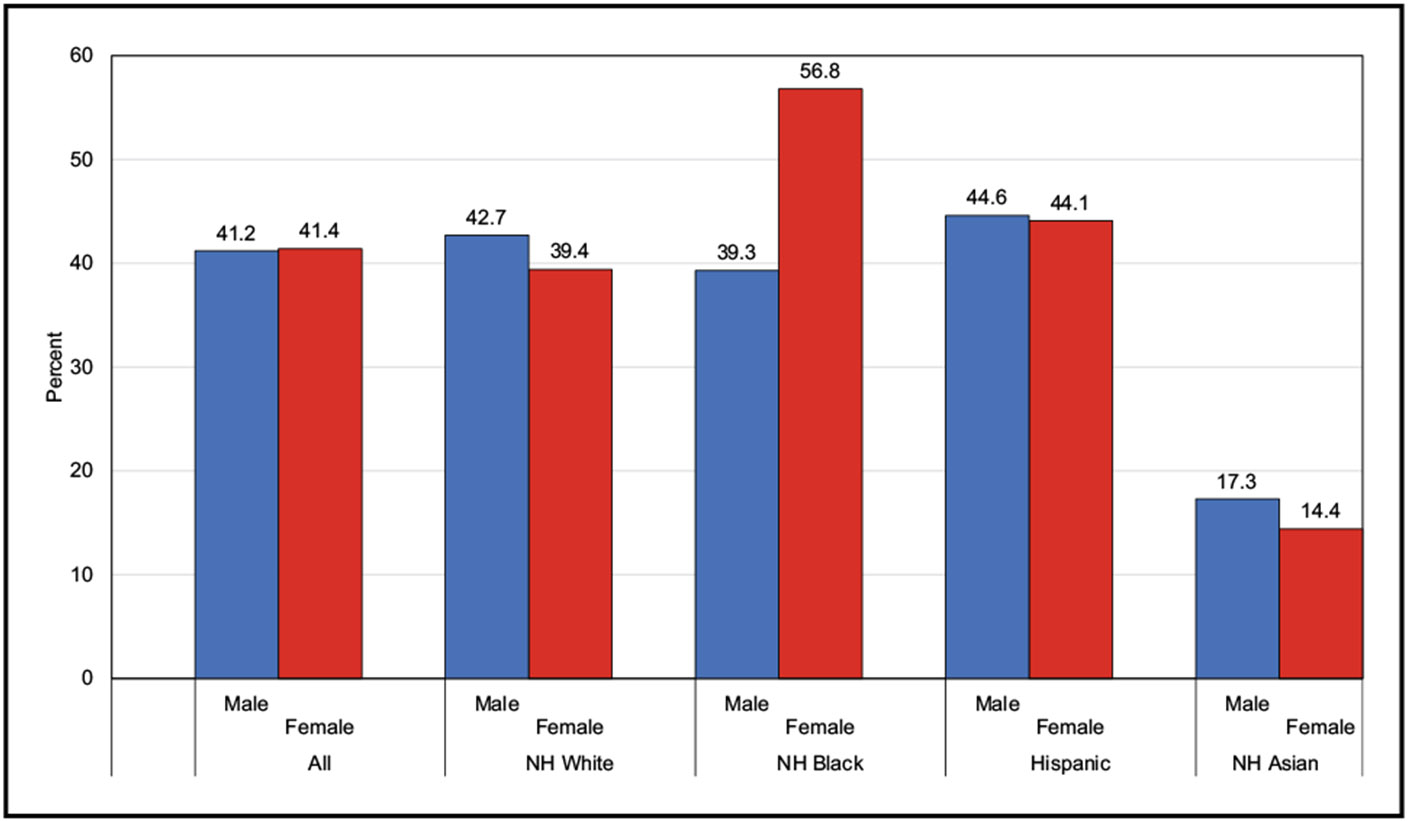
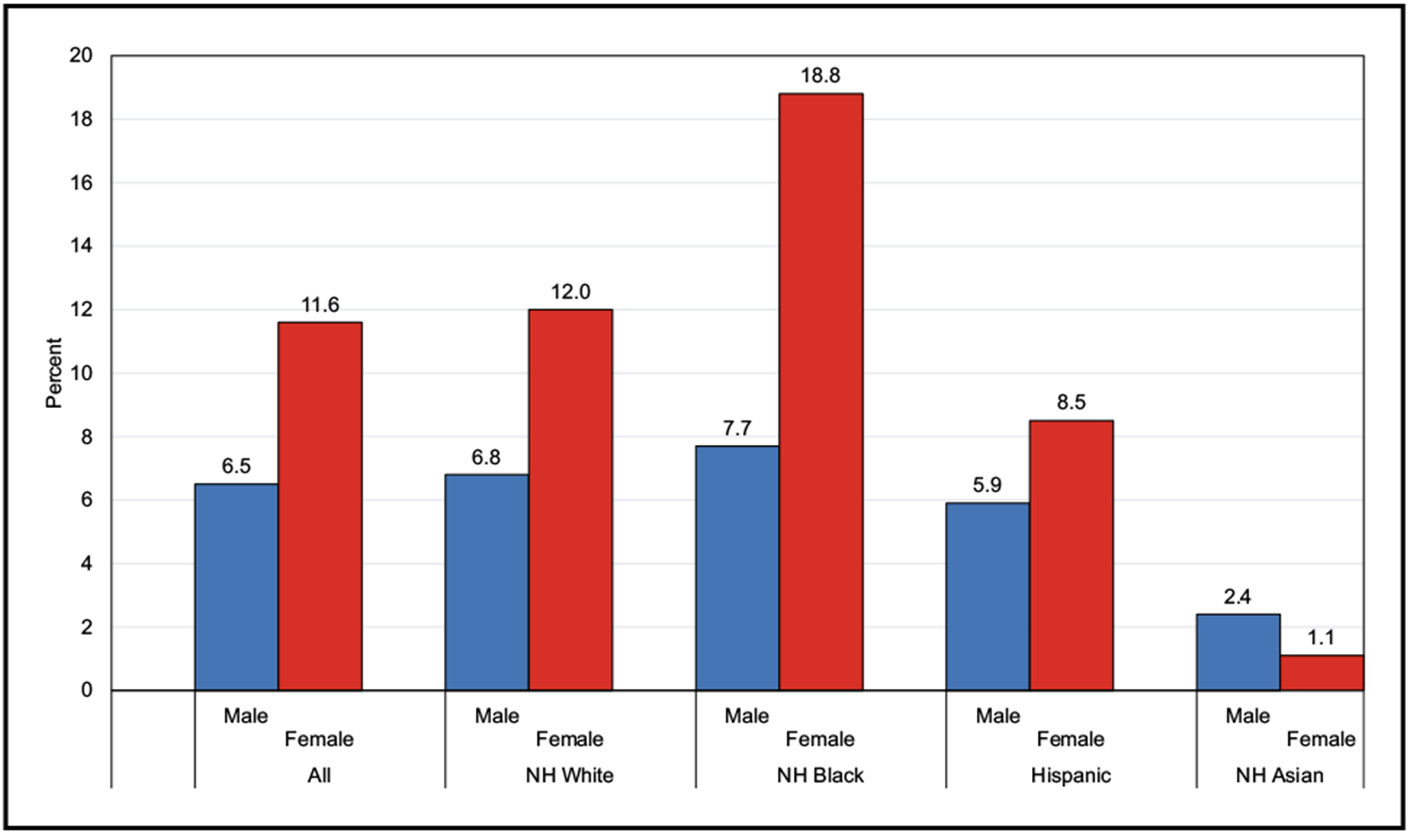
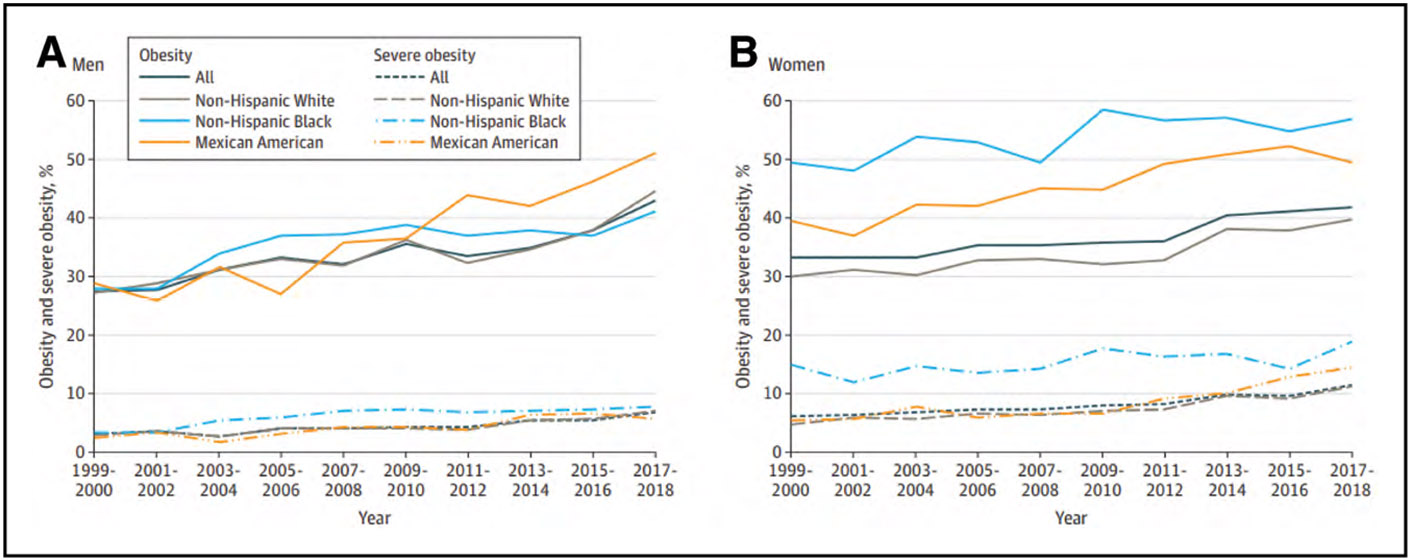
Overweight and Obesity (Chapter 6)
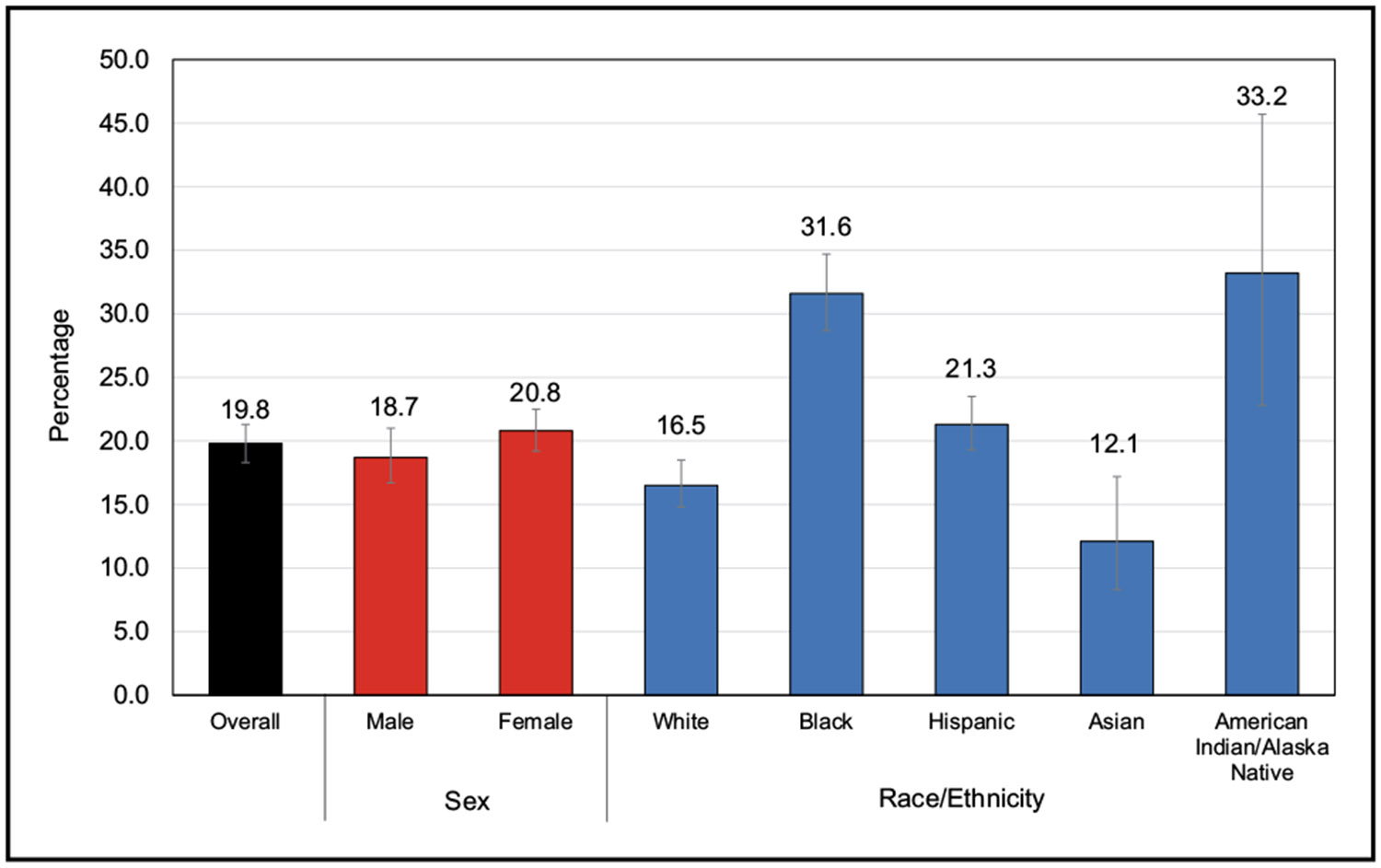
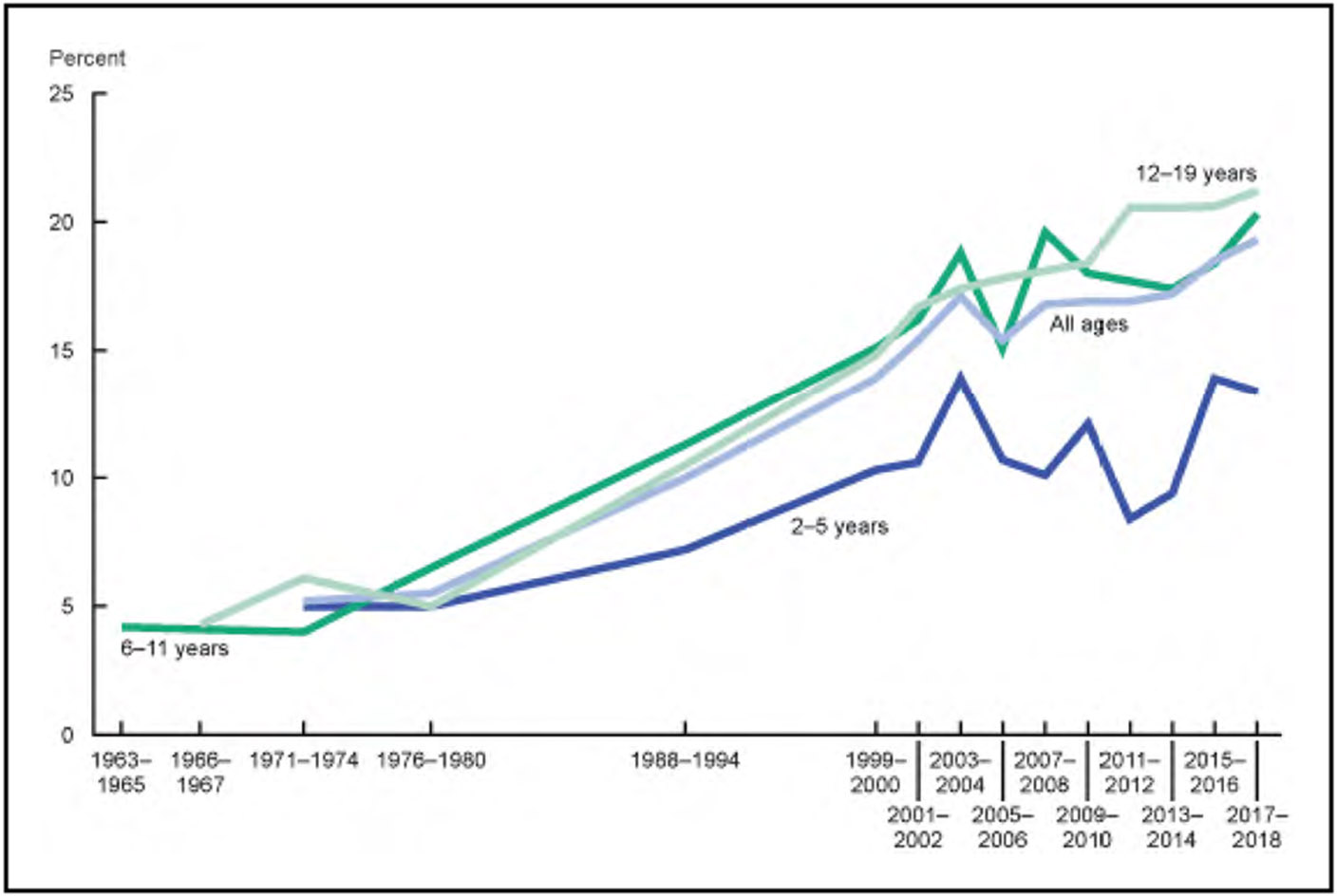
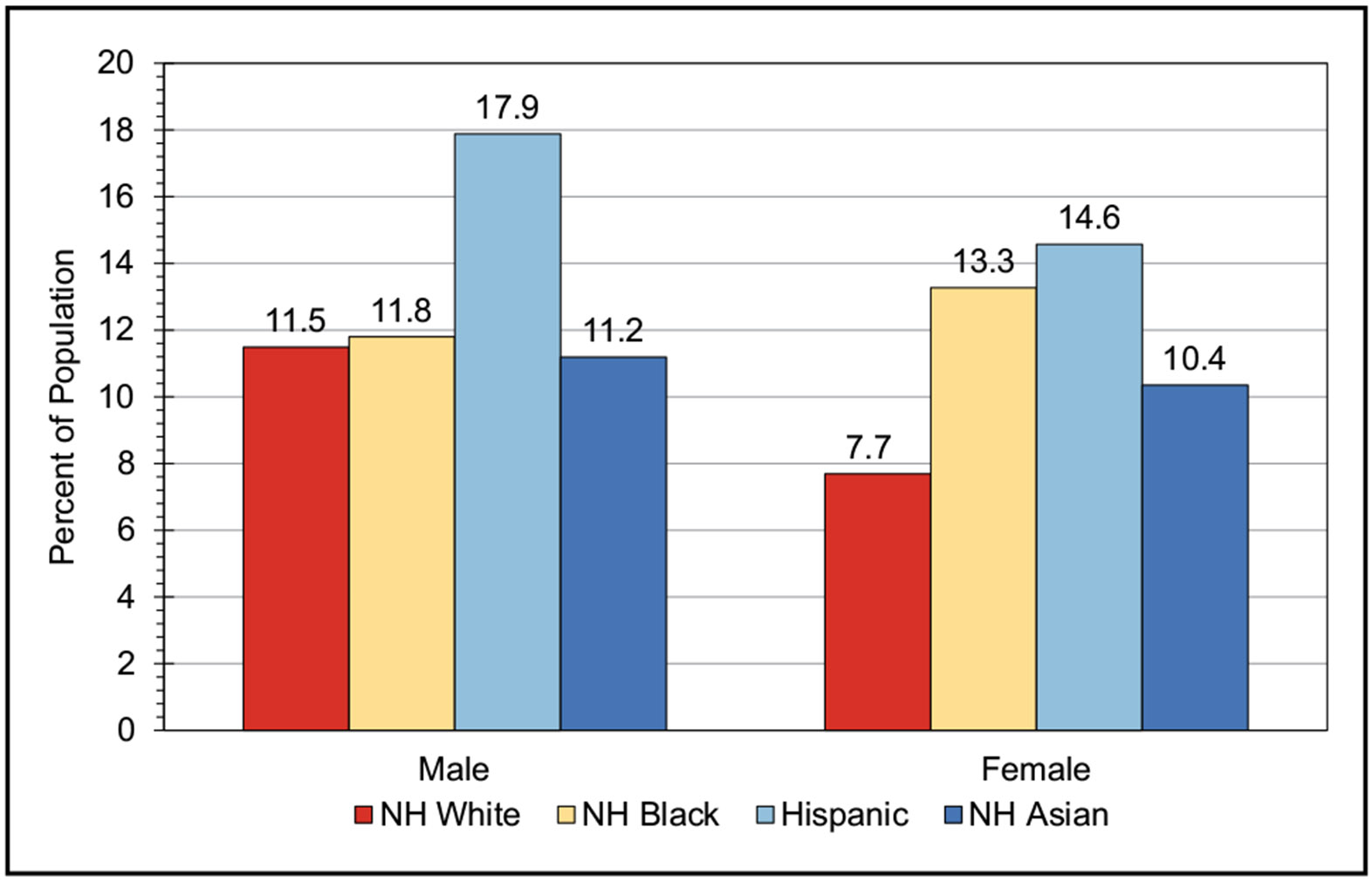
According to data from NHANES from 2017 until March 2020, among US children and adolescents 2 to 19 years of age, the prevalence of being either overweight or obese was 36.8%, with obesity prevalence of 19.8%. The highest prevalence of obesity was seen among Hispanic male and NH Black female youth.
According to data from NHANES from 2017 until March 2020, the age-adjusted prevalence of overweight or obesity among adults ≥20 years of age in the United States was 71.2%, and the prevalence of obesity was 41.4%. The highest prevalence of obesity was among NH Black females.
A large umbrella review in 2021 found that every 5–kg/m2 increase in body mass index was associated with a 15% increased risk for CHD, 23% increased risk for atrial fibrillation (AF), 41% increased risk for HF, and 49% increased risk for hypertension.
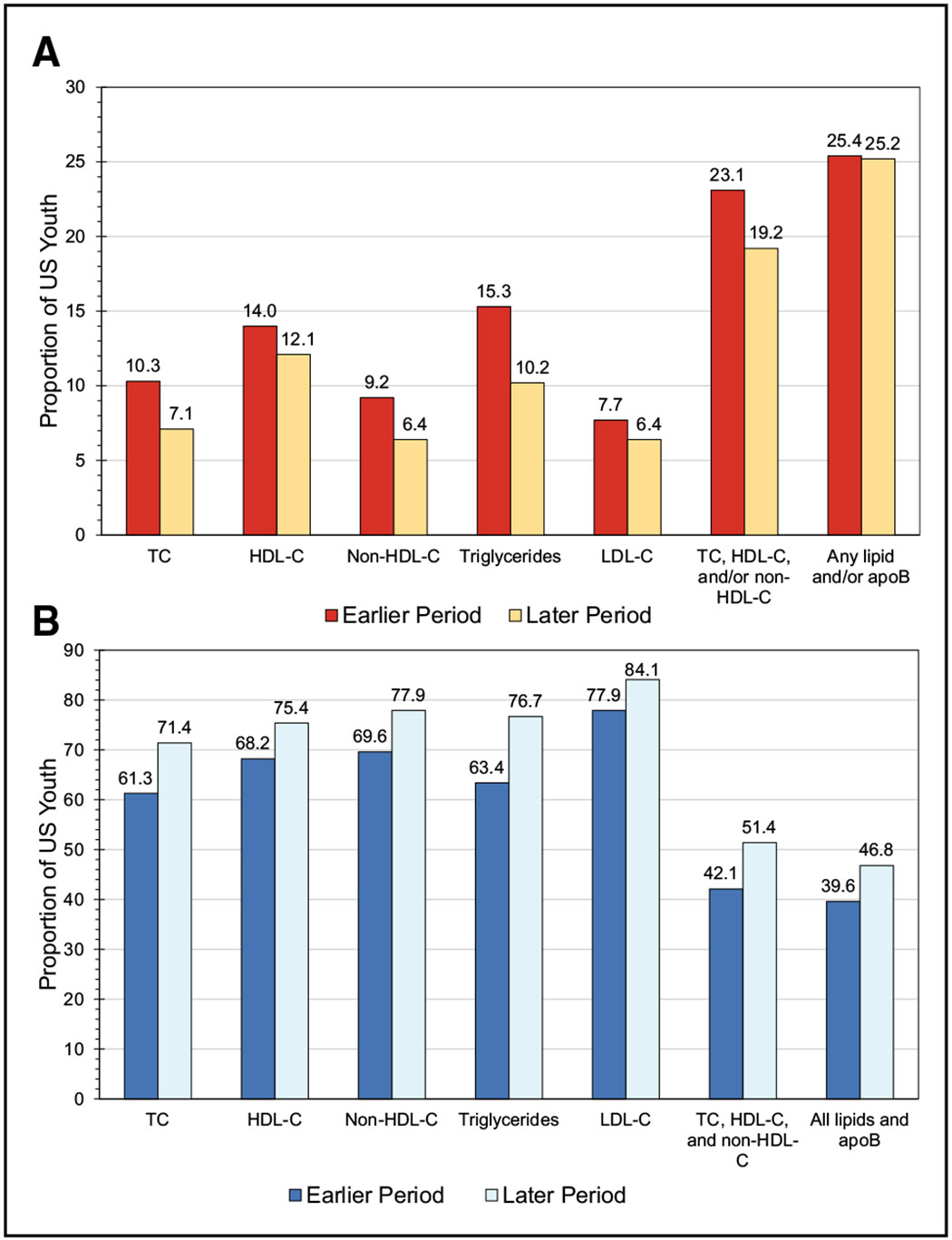
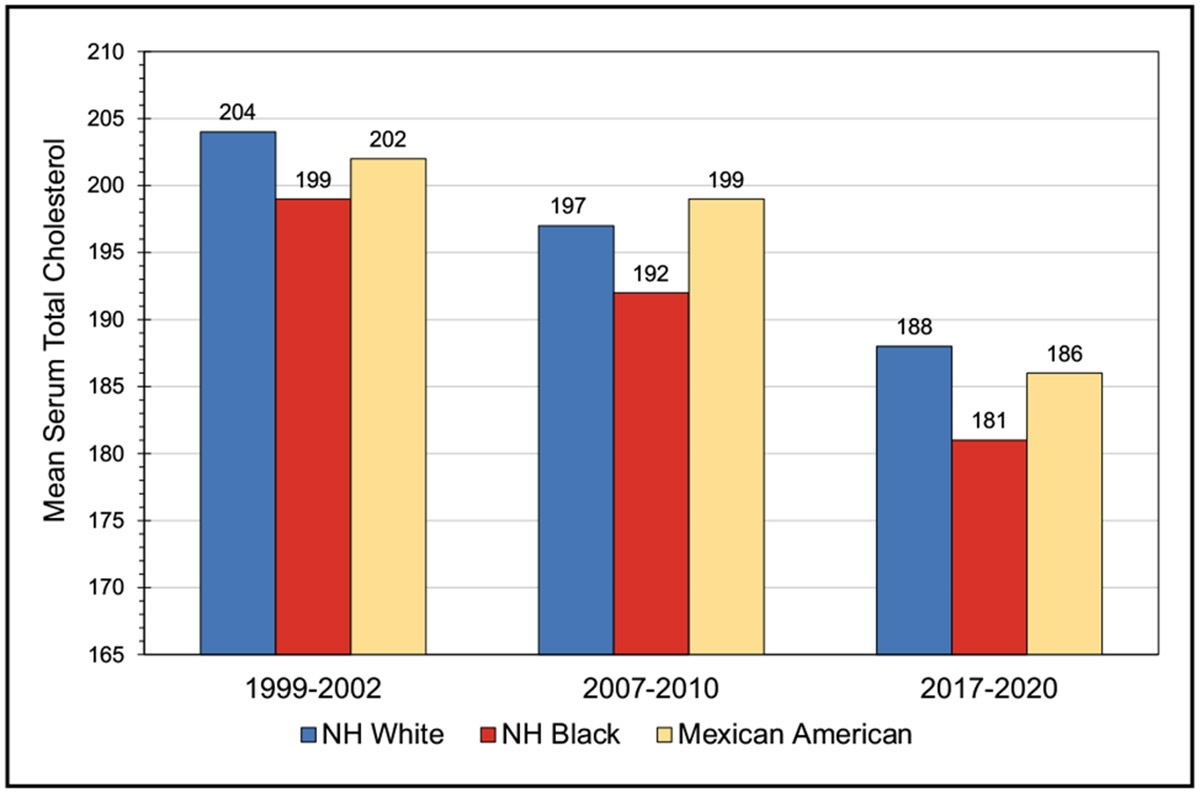
High Blood Cholesterol and Other Lipids (Chapter 7)
Among adolescents in 2017 to 2020, low-density lipoprotein cholesterol (LDL-C) levels ≥130 mg/dL occurred in 5.0% of male adolescents and 4.6% of female adolescents, LDL-C levels <40 mg/dL occurred in 19.3% of male adolescents and 8.6% of female adolescents, and triglycerides ≥130 mg/dL occurred in 7.2% of male adolescents and 6.2% of female adolescents.
In 2017 to 2020, among adults, total cholesterol ≥200 mg/dL occurred in 32.8% of males and 36.2% of females, LDL-C ≥130 mg/dL occurred in 25.6% of males and 25.4% of females, and high-density lipoprotein cholesterol <40 mg/dL occurred in 24.9% of males and 9.3% of females.
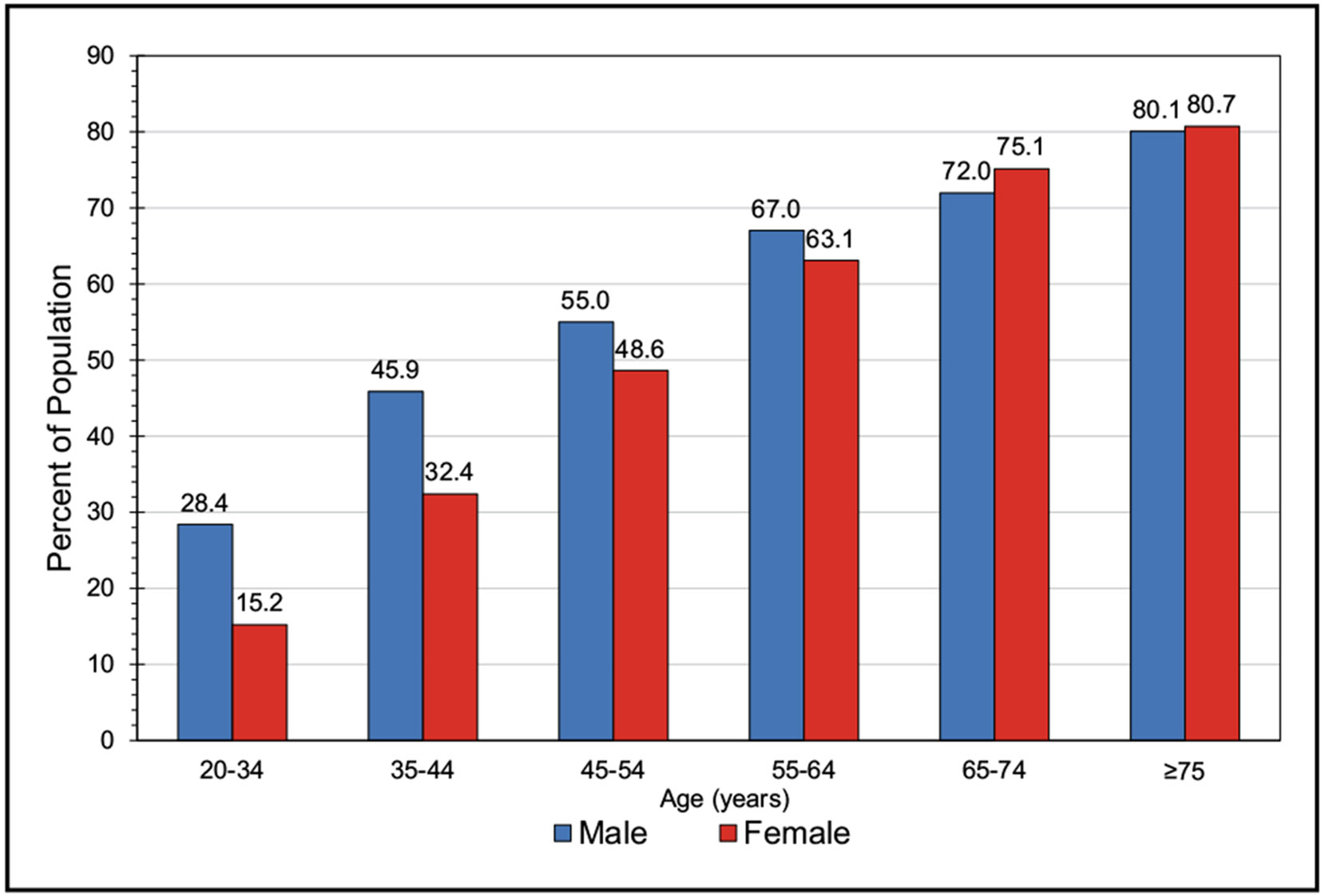
High Blood Pressure (Chapter 8)
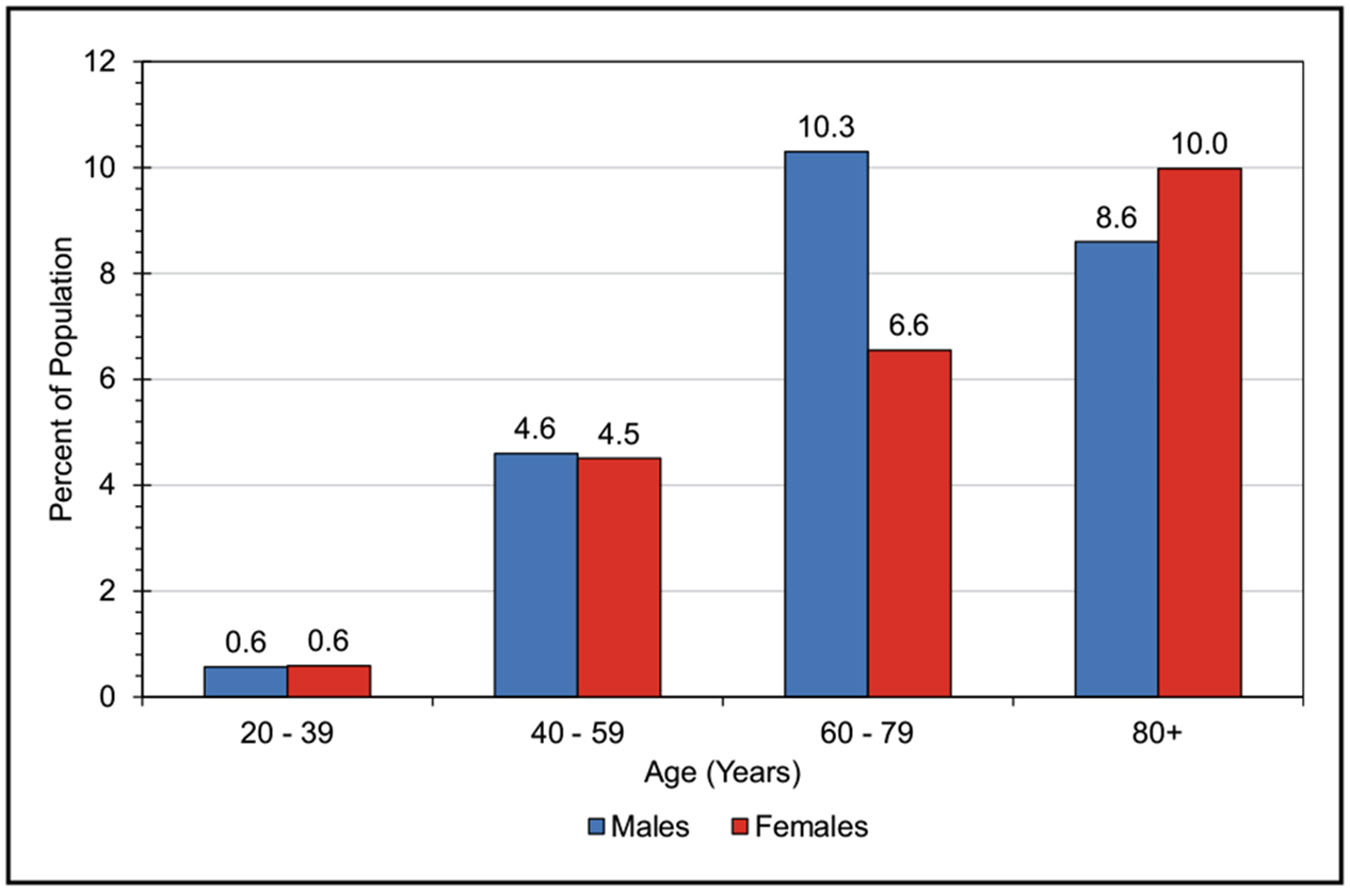
With the use of the most recent 2017 definition, the age-adjusted prevalence of hypertension among US adults ≥20 years of age was estimated to be 46.7% in NHANES in 2017 to 2020 (50.4% for males and 43.0% for females). This equates to an estimated 122.4 million adults ≥20 years of age who have high blood pressure (62.8 million males and 59.6 million females). A higher percentage of males than females had hypertension up to 64 years of age, but for those ≥65 years of age, the percentage of females with hypertension was higher than for males.
In an individual patient meta-analysis of 33 trials including 260 447 participants with 15 012 cancer events, no associations were identified between any antihypertensive drug class and risk of any cancer (hazard ratio [HR], 0.99 for angiotensin-converting enzyme inhibitors; HR, 0.96 for angiotensin receptor blockers; HR, 0.98 for β-blockers; HR, 1.01 for thiazides), except for calcium channel blockers (HR, 1.06). In a network meta-analysis comparing each drug class with placebo, no drug class was associated with an excess cancer risk (HR, 1.00 for angiotensin-converting enzyme inhibitors; HR, 0.99 for angiotensin receptor blockers; HR, 0.99 for β-blockers; HR, 1.04 for calcium channel blockers; HR, 1.00 for thiazides).
In an open-label, cluster-randomized trial involving 20995 individuals from 600 villages in rural China, the use of a salt substitute (75% sodium chloride and 25% potassium chloride by mass) compared with the use of regular salt (100% sodium chloride) resulted in a lower incidence of stroke (RR, 0.86), all-cause mortality (RR, 0.88), and major adverse cardiovascular event (RR, 0.87). There was no increase in rates of hyperkalemia with use of the salt substitute (RR, 1.04).
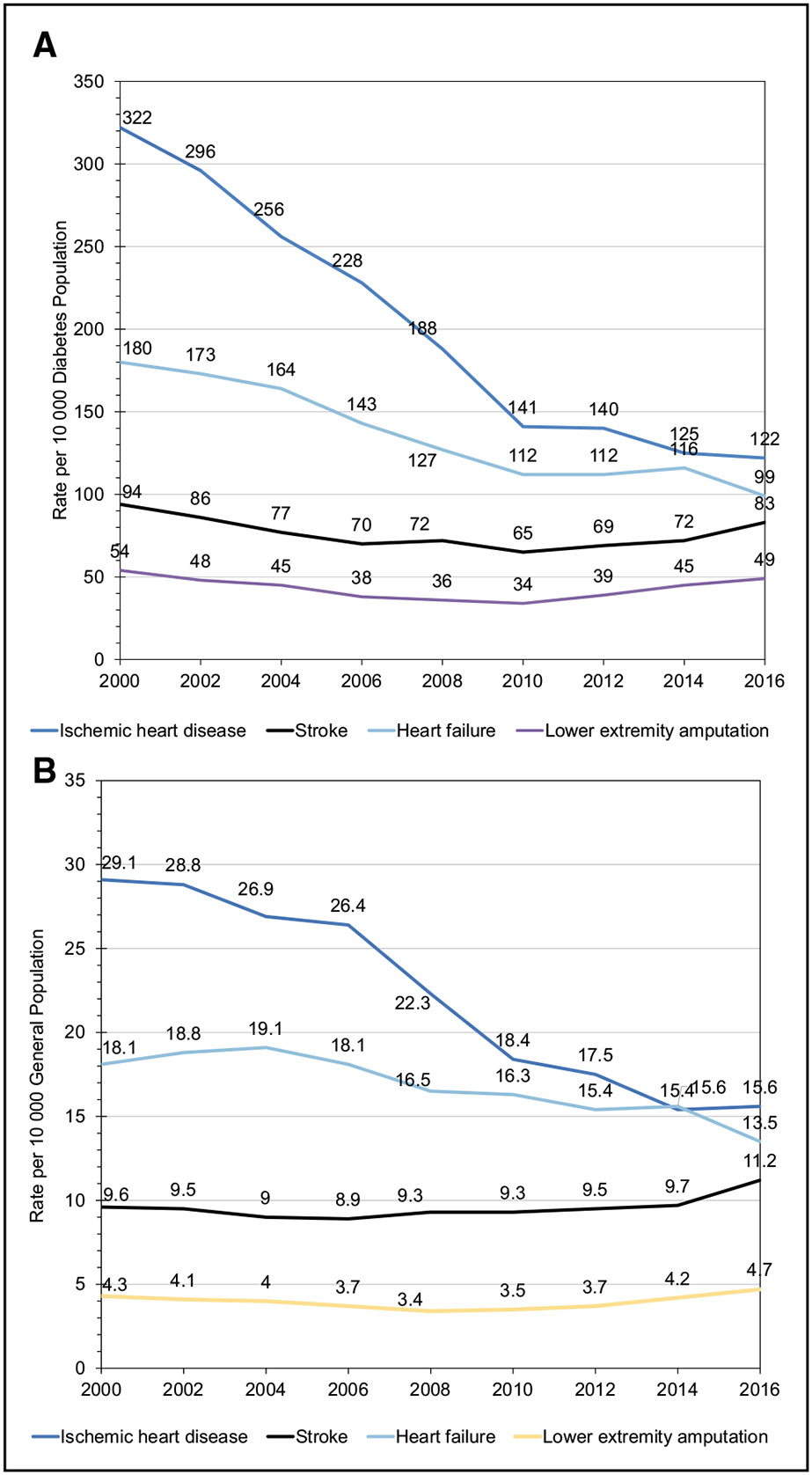
Diabetes (Chapter 9)
Overall, on the basis of 2017 to 2020 data, 29.3 million adults (10.6%) in the United States had diagnosed diabetes.
Data from the CALIBER UK cohort show the most common initial CVD complications for those with diabetes to be peripheral artery disease (16.2%) and HF (14.1%), followed by stable angina (11.9%), nonfatal myocardial infarction (11.5%), and stroke (10.3%).
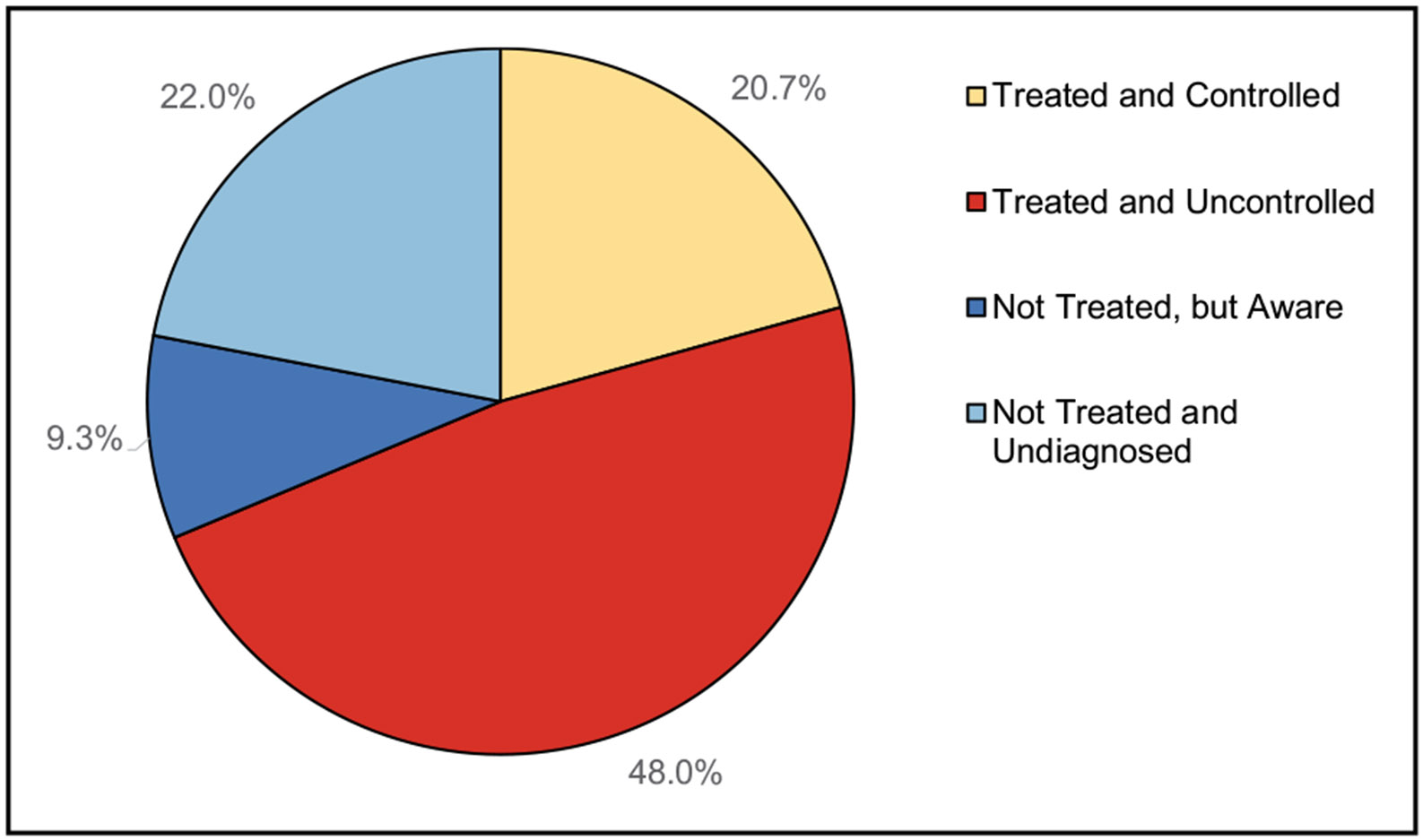
Data from the US Diabetes Collaborative Registry of 74 393 adults with diabetes demonstrate a prevalence of 74% with hemoglobin A1c <7%, 40% with blood pressure <130/80 mm Hg, and 49% with LDL-C <100 mg/dL (<70 mg/dL if with atherosclerotic cardiovascular disease), but only 15% at target for all 3 factors.
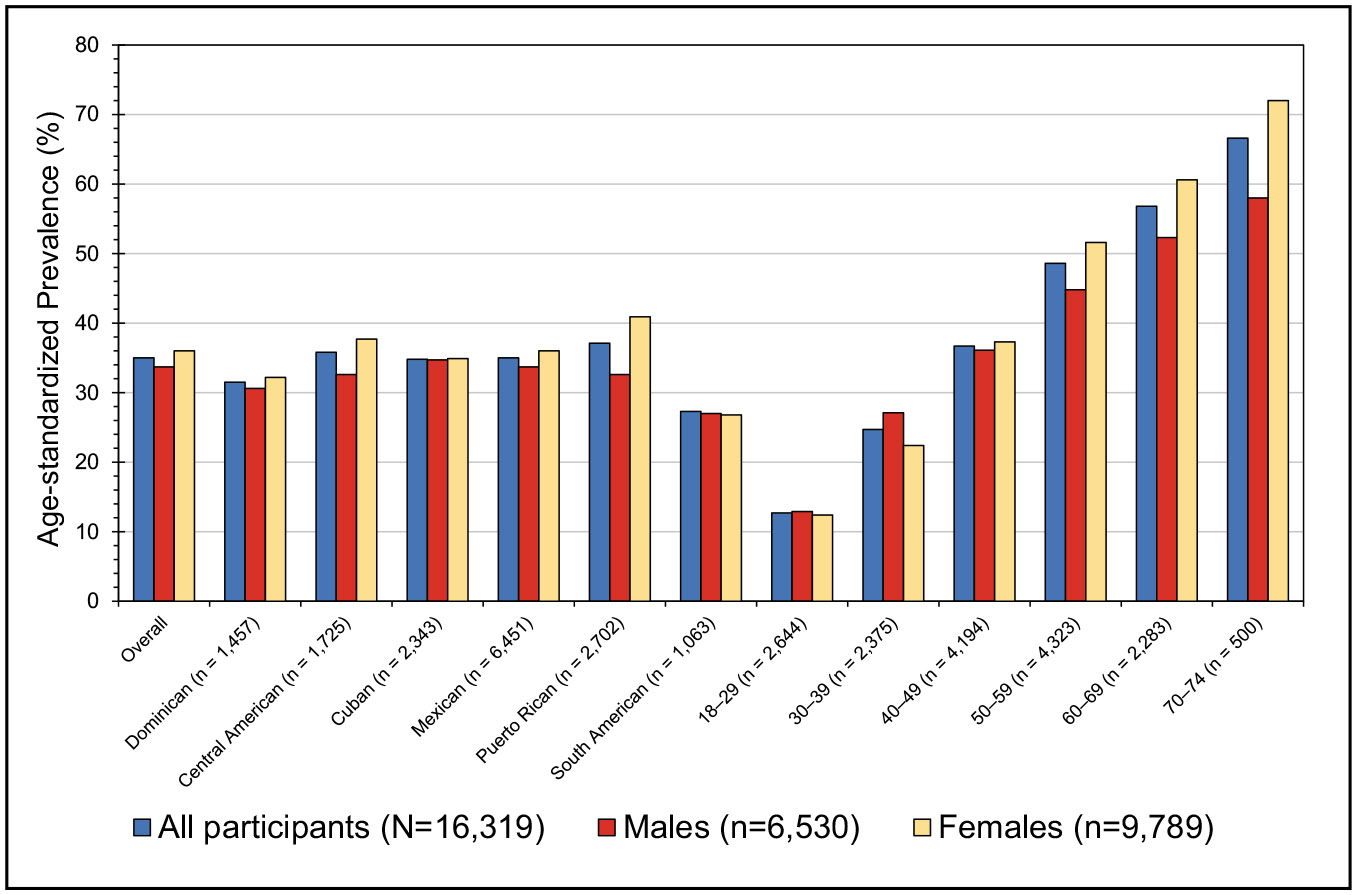
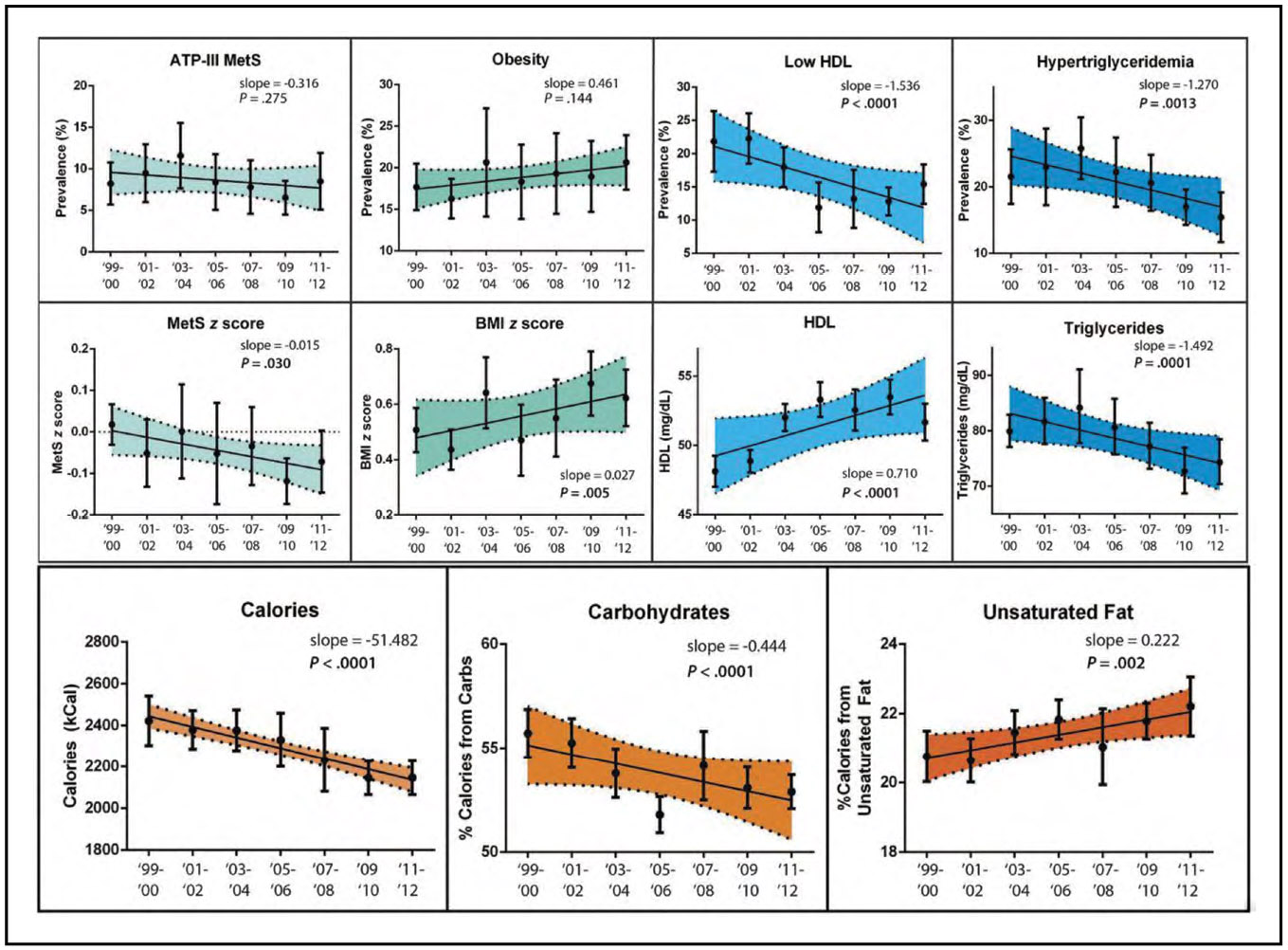
Metabolic Syndrome (Chapter 10)
From 1999 to 2018, the prevalence of metabolic syndrome among US youths remained stable at 4.36%. Among adults, the prevalence of metabolic syndrome increased from 36.2% to 47.3%.
According to the data from NHANES 1999 to 2018, the prevalence of metabolic syndrome among youths 12 to 19 years of age was 4.34% for NH White, 3.66% for NH Black, 7.70% for Mexican American, 4.84% for other Hispanic, and 1.84 for other race youths.
In 2017 to 2018, Mexican American adults generally had the highest prevalence of metabolic syndrome at 52.2%, whereas NH White adults had 46.6%, NH Black adults had 47.6%, other Hispanic adults had 45.9%, and Asian/other adults had 46.7%.
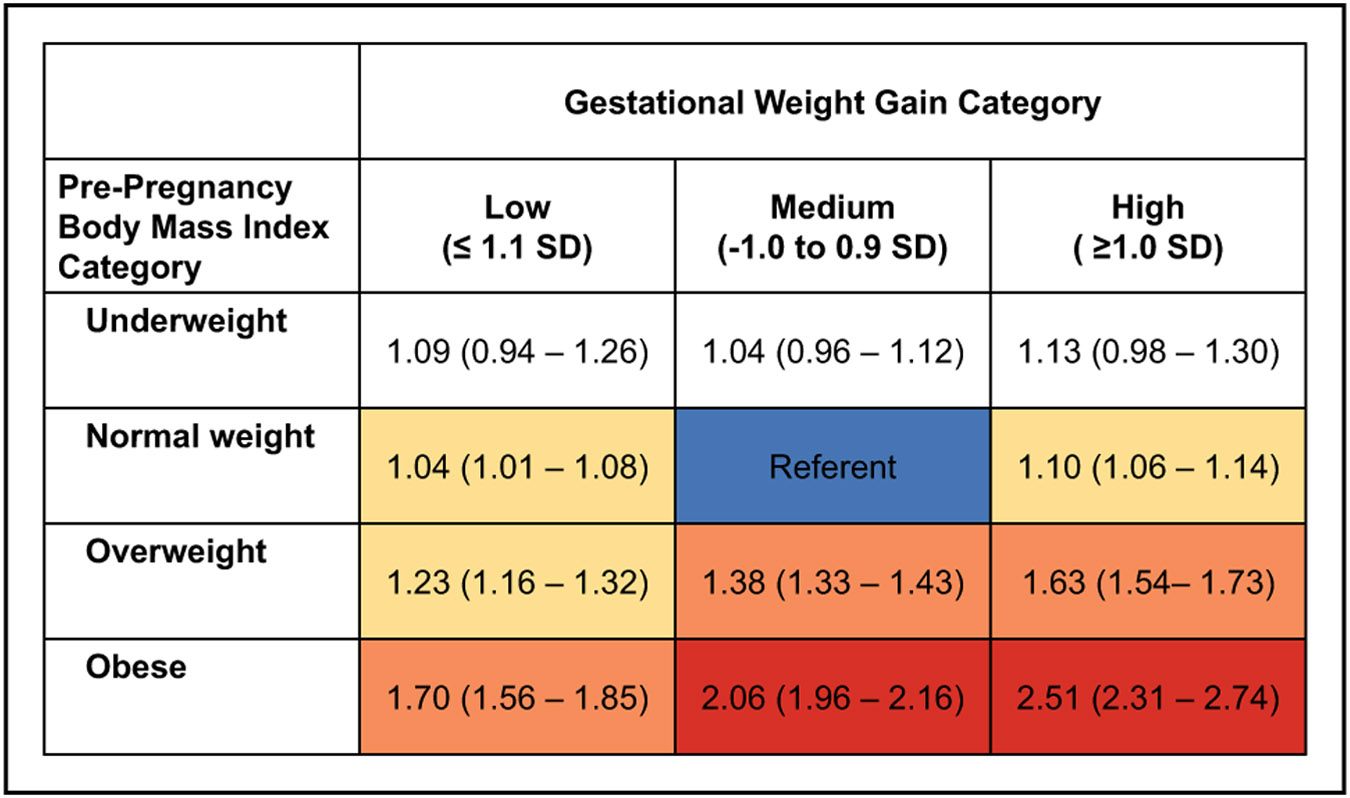
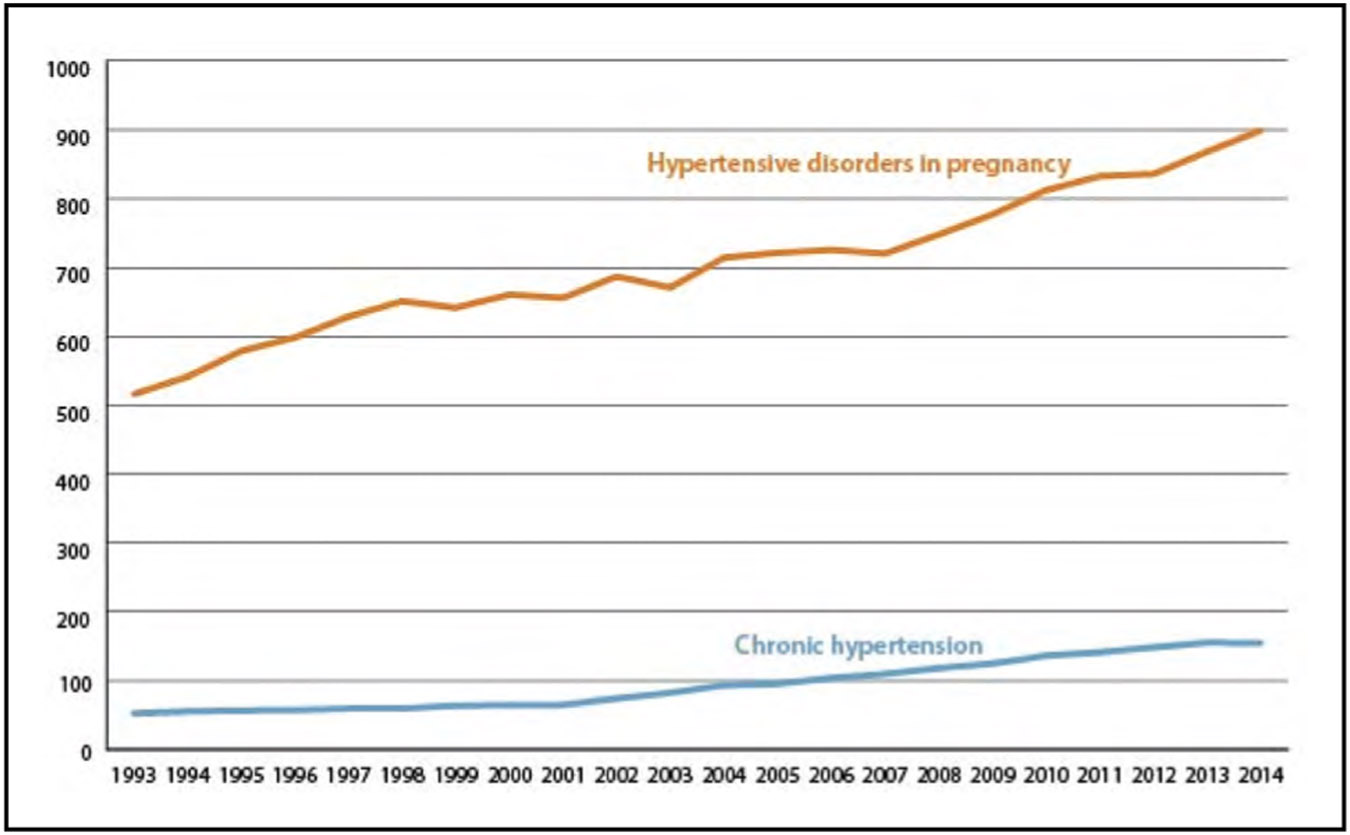
Adverse Pregnancy Outcomes (Chapter 11)
Rates of overall hypertensive disorders of pregnancy are increasing. Analysis of delivery hospitalizations from the National Readmission Database reported a rate of hypertensive disorders of pregnancy of 912.4 per 10 000 delivery hospitalizations in 2014 compared with 528.9 in 1993 in the United States.
Specific aspirin dosage and preeclampsia prevention were studied in 23 randomized trials (32 370 females). Females assigned at random to 150 mg experienced a 62% reduction in risk of preterm preeclampsia (RR, 0.38). Aspirin doses <150 mg produced no significant reductions. The number needed to treat with 150 mg of aspirin was 39. There was a maximum 30% reduction in risk of all gestational age preeclampsia at all aspirin doses.
In a cohort of 595 pregnant females in 4 US cities, perceived discrimination (self-reported as based on sex, race, income level or social status, age, and physical appearance) was associated with development of gestational diabetes. Gestational diabetes occurred in 12.8% of females in the top quartile of a self-reported discrimination scale versus 7.0% in all others (adjusted odds ratio [OR], 2.11, adjusted for age, income, parity, race and ethnicity, and study site); 22.6% of this association was statistically mediated by obesity.
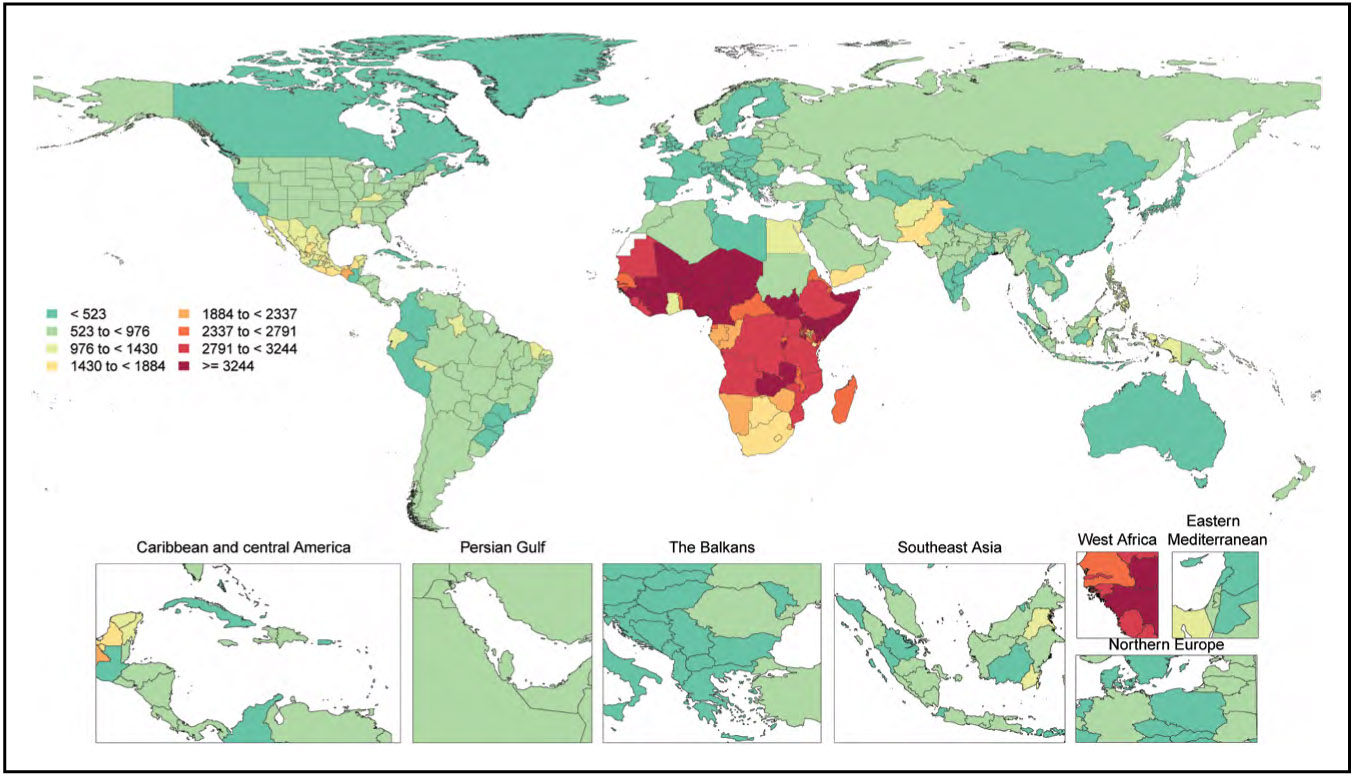
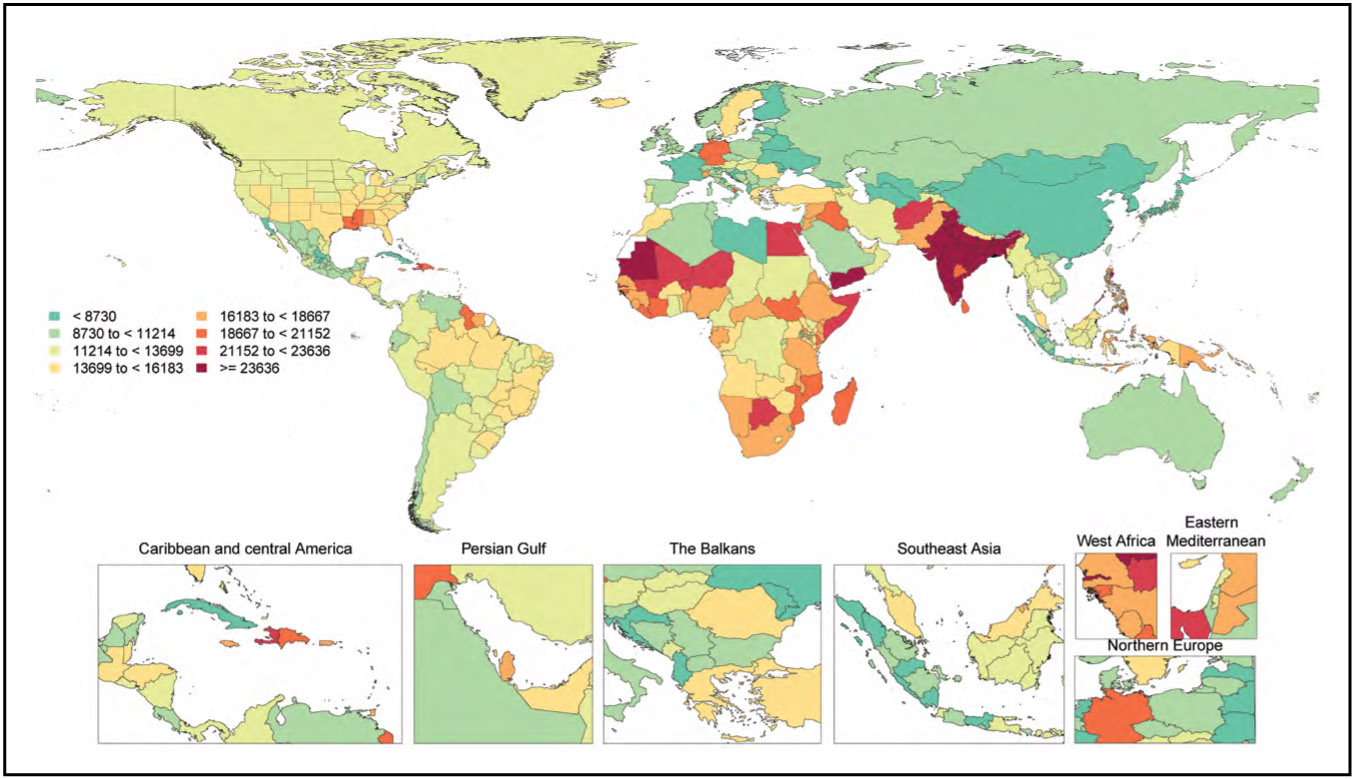
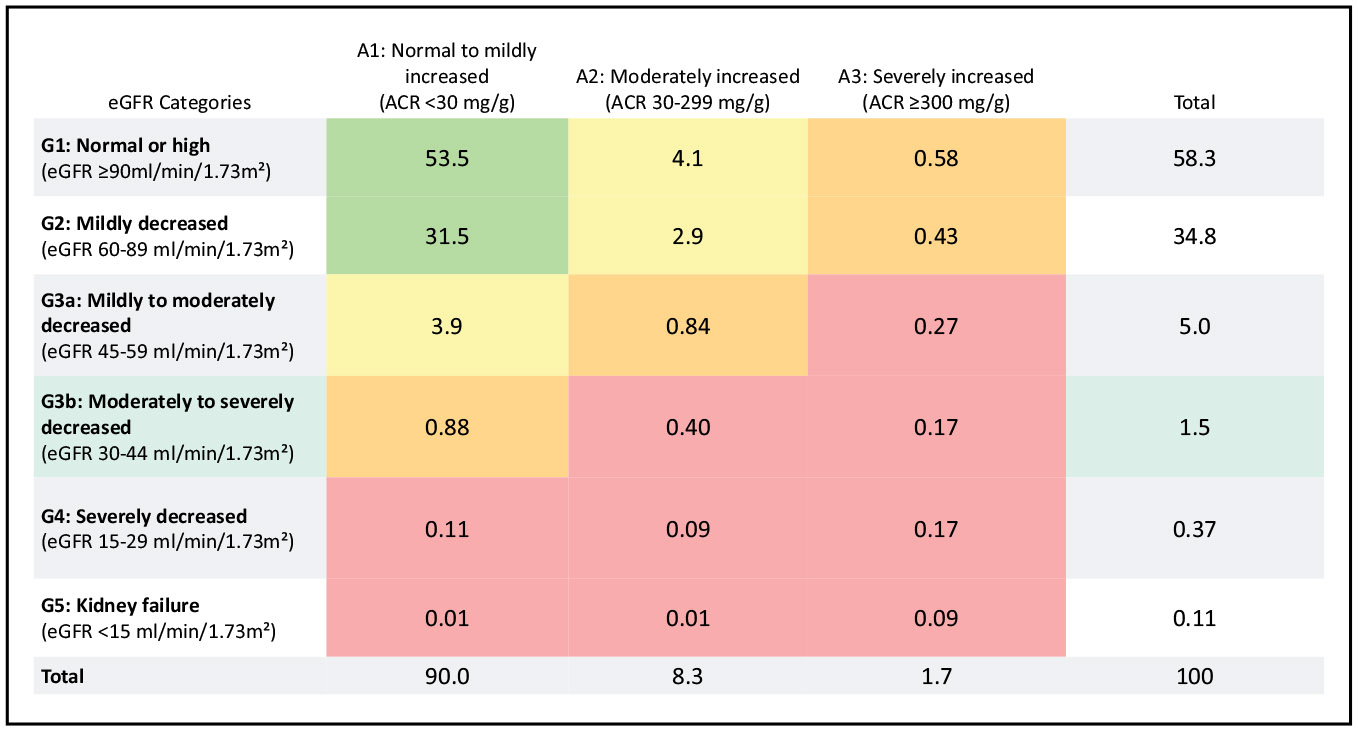
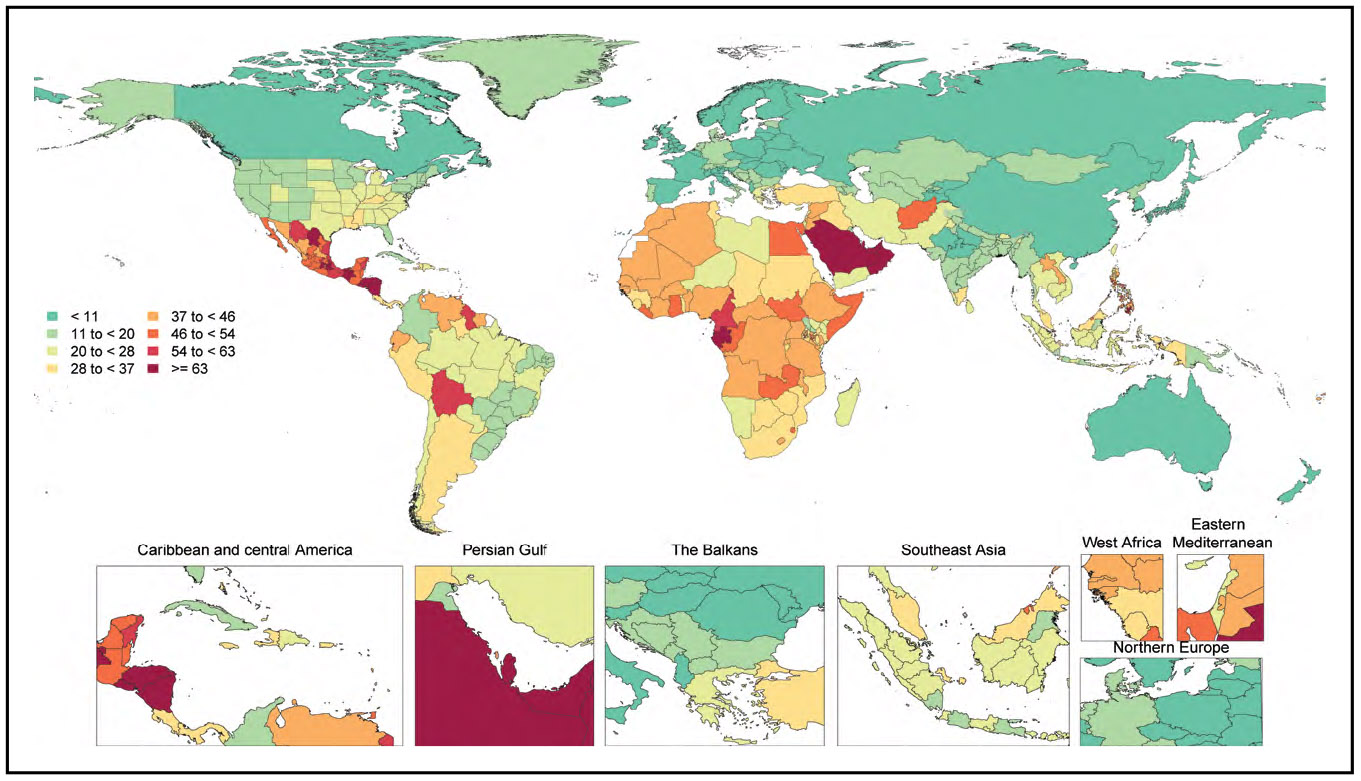
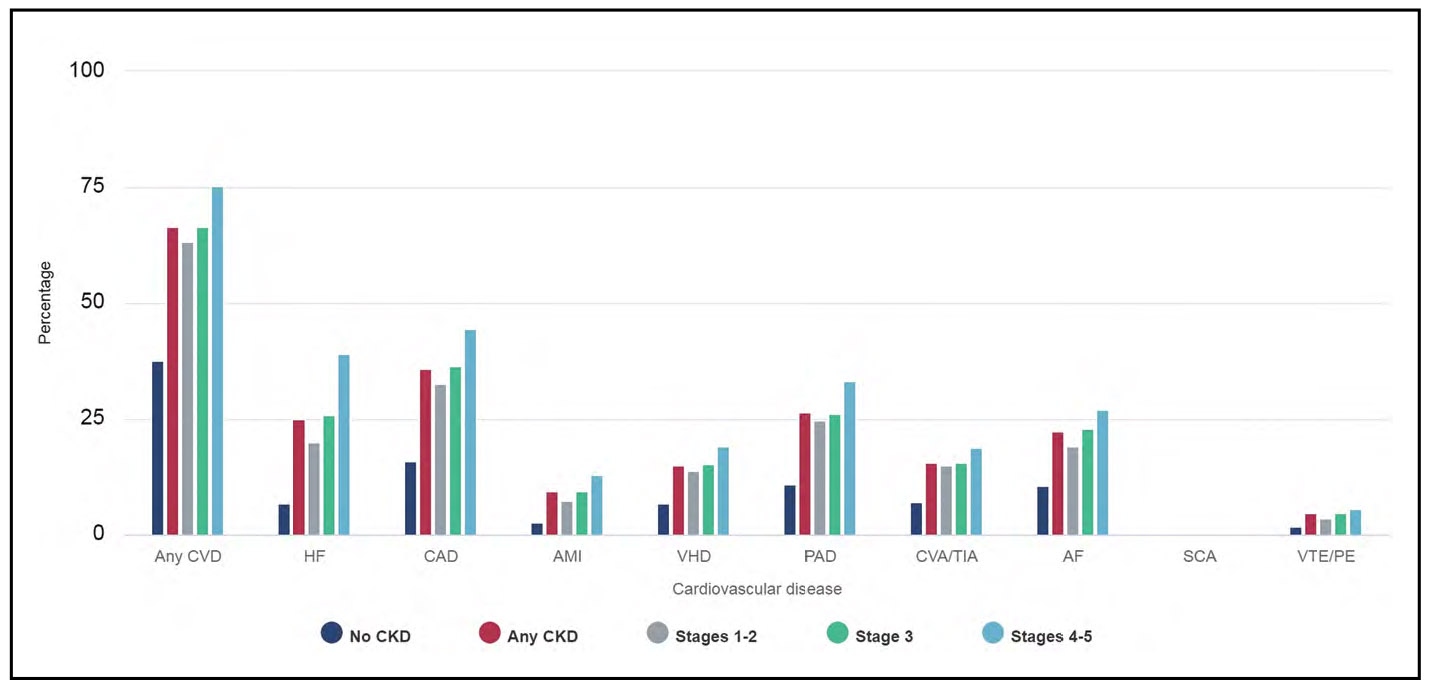
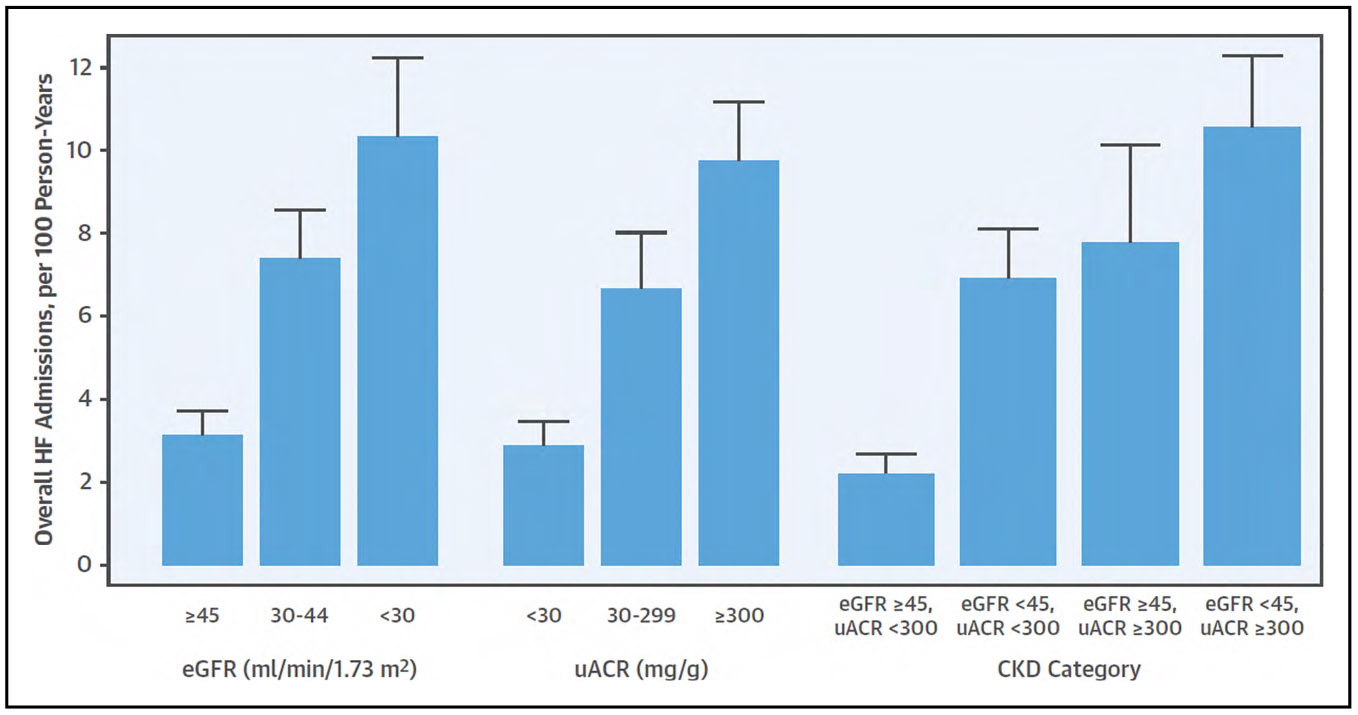
Kidney Disease (Chapter 12)
The overall prevalence of chronic kidney disease (estimated glomerular filtration rate <60 mL·min−1·1.73 m−2 or albumin-to-creatinine ratio ≥30 mg/g) in 2015 to 2018 was 14.9%.
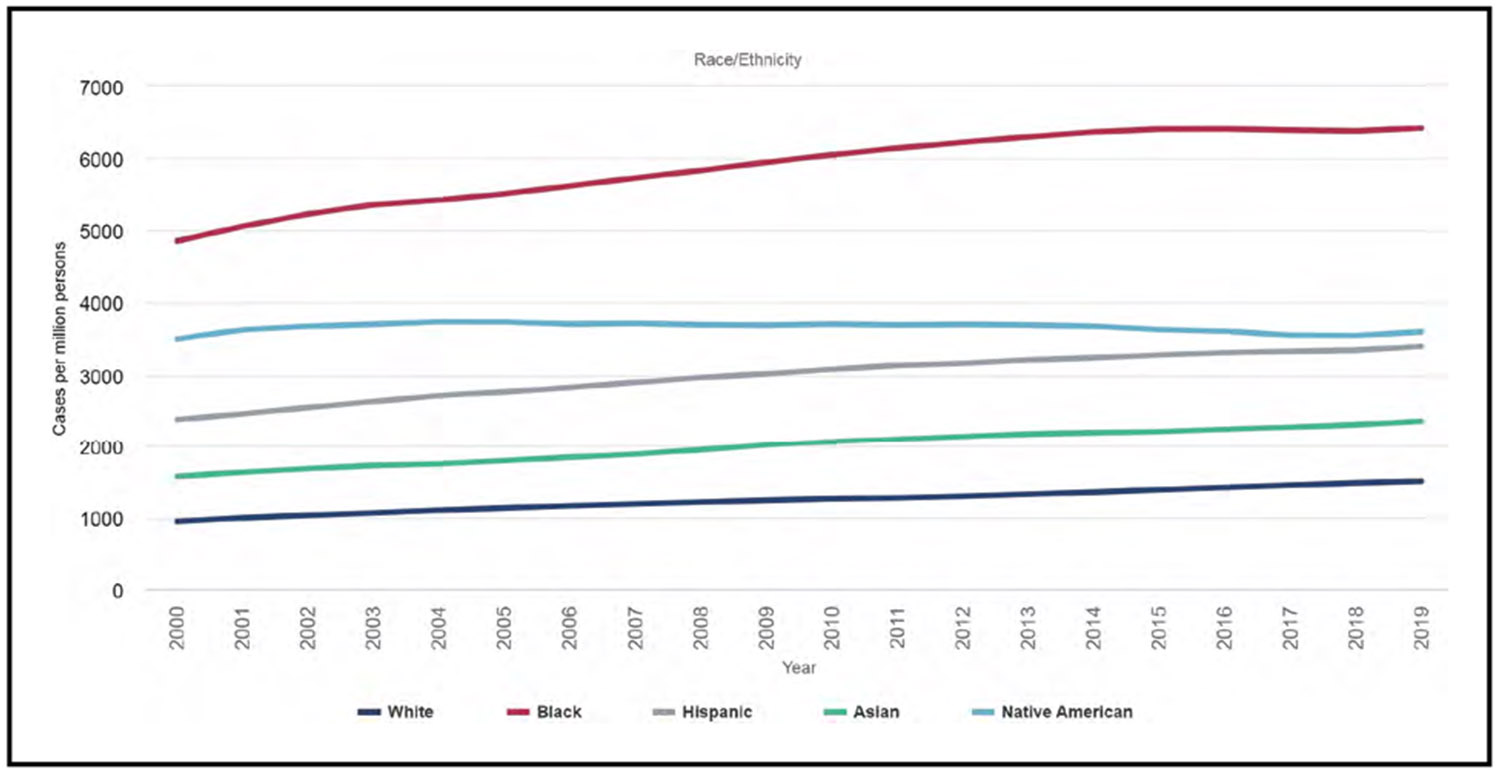
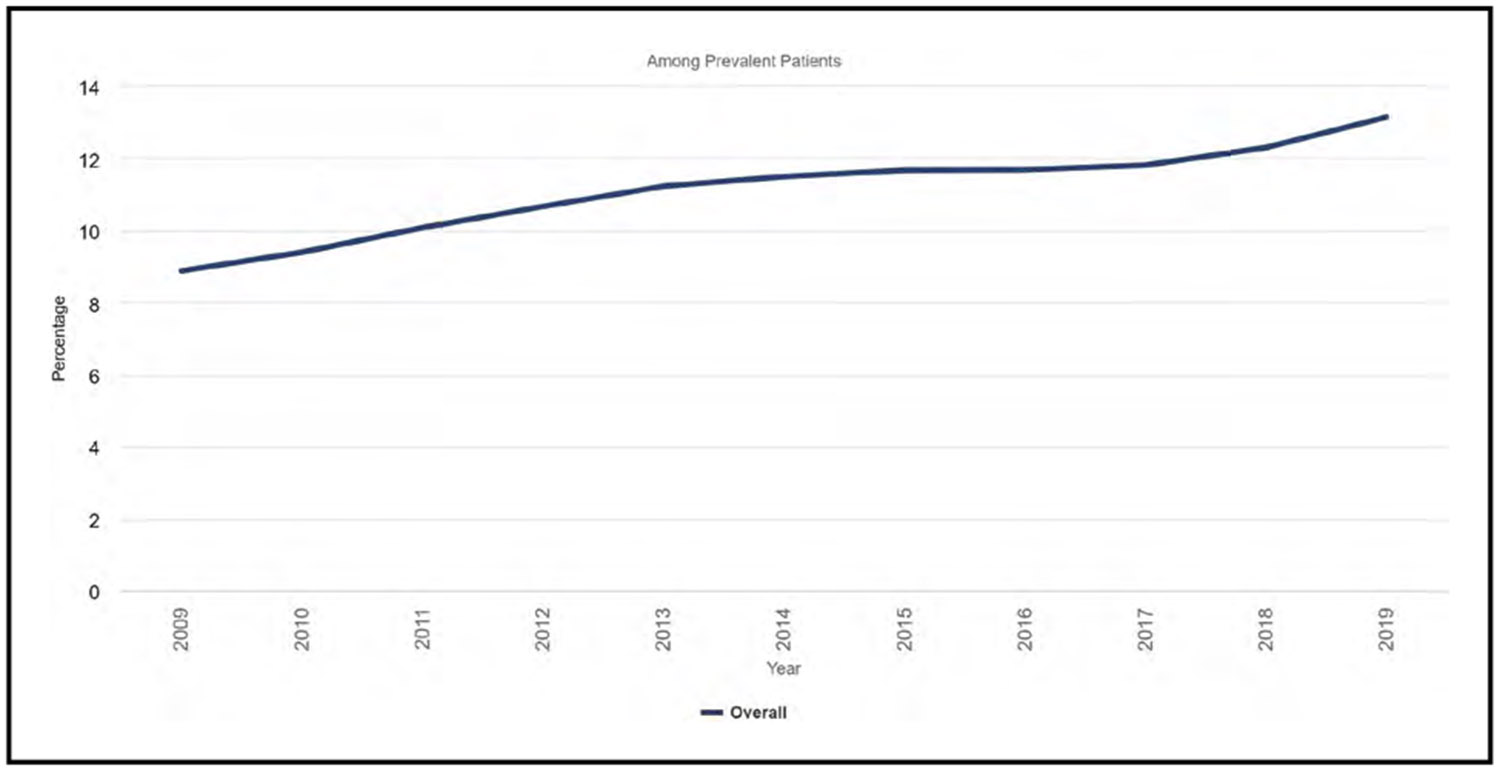
In 2019, the age-, race-, and sex-adjusted prevalence of end-stage renal disease in the United States was 2302 per 1 million people, an increase of 1.4% over 2018.
Total hospitalization expenditures in Medicare fee-for-service beneficiaries with end-stage renal disease was $12.2 billion in 2019, and outpatient spending was $13.1 billion in 2019.
Sleep (Chapter 13)
- The proportion of adults reporting insufficient sleep (<7 hours) in 2020 was 32.8%.
- Older adults, >65 years of age, report the lowest prevalence of insufficient sleep.
- NH Black adults had the highest percentage of respondents reporting sleeping <7 h/night (43.5%), whereas NH Asian adults (30.5%) and NH White adults (30.7%) had the lowest percentage of respondents reporting sleeping <7 hours.
Females report never or some of the days feeling well rested on awakening in the past days more frequently than males (46.9% versus 40.4%).
Data from the MIDUS study (Midlife in the United States) examined the association of a composite sleep health measure (sleep regularity, satisfaction, alertness, timing, efficiency, and duration) with risk of HD (yes/no to a question on diagnosis of HD). Each unit increase in the self-reported sleep health composite was associated with a 54% higher risk of HD, whereas the objectively measured actigraphy sleep health composite was associated with 141% higher risk.
Total Cardiovascular Disease (Chapter 14)
On the basis of NHANES 2017 to March 2020 data, the prevalence of CVD (comprising CHD, HF, stroke, and hypertension) in adults ≥20 years of age was 48.6% overall (127.9 million in 2020) and increases with age in both males and females.
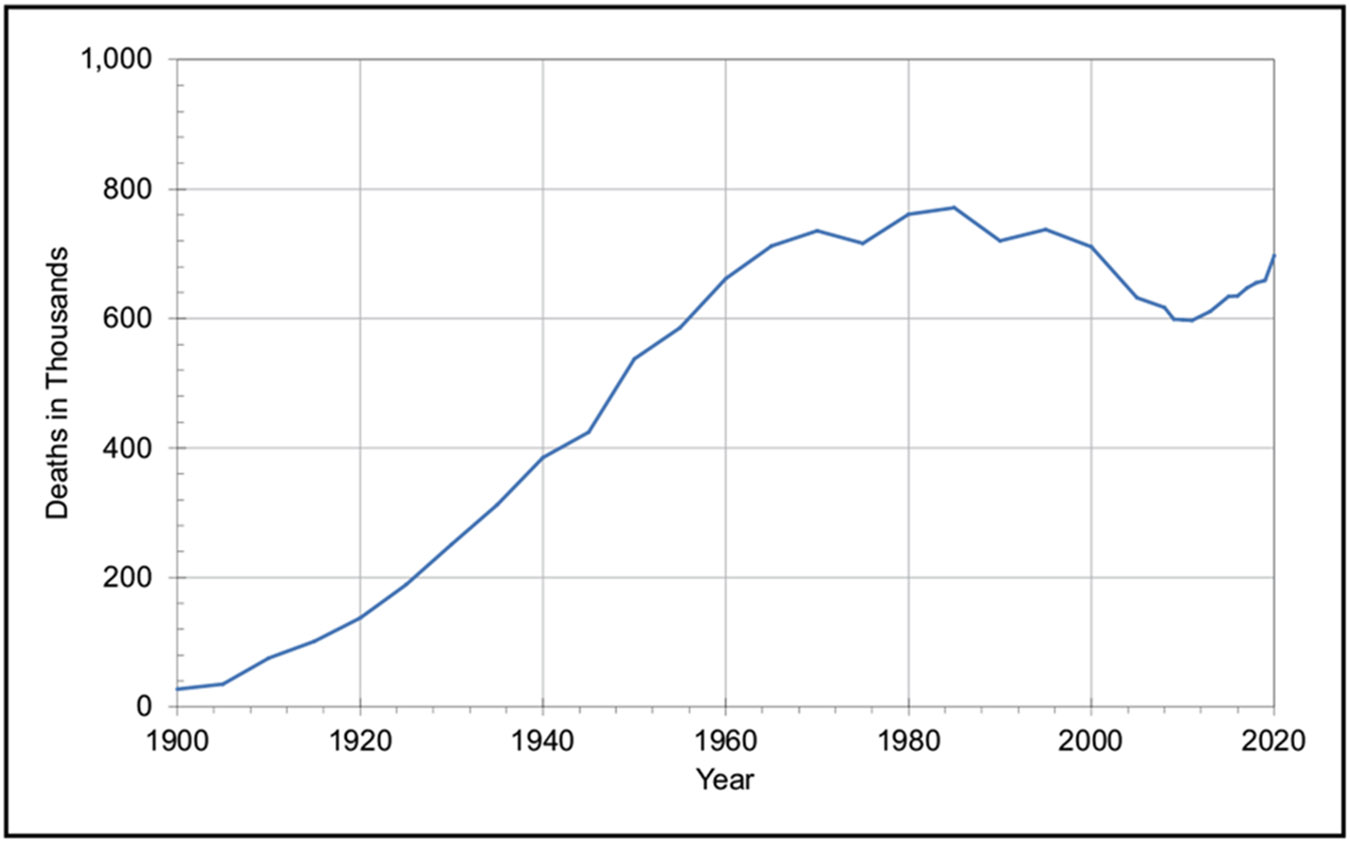
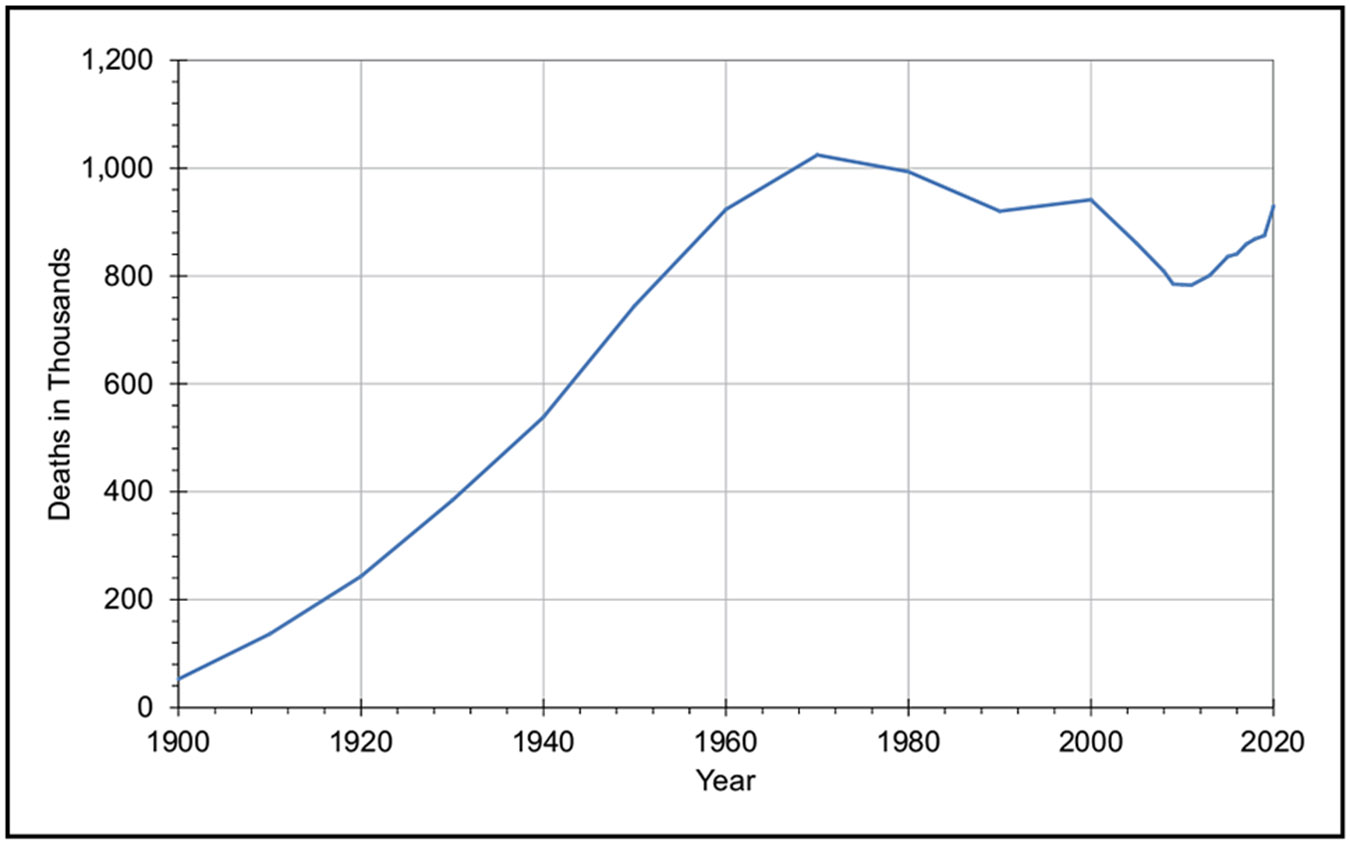
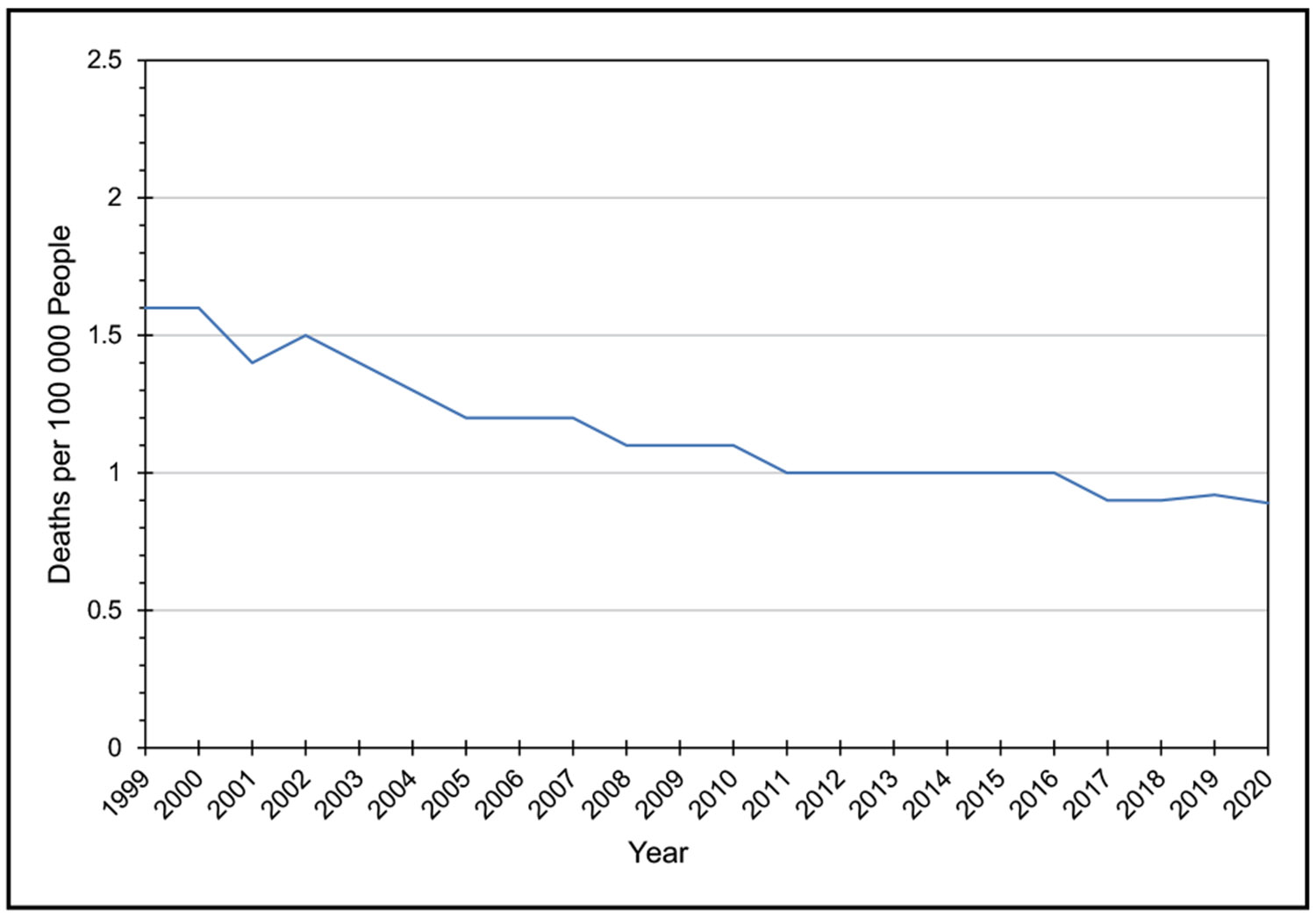
On the basis of 2020 mortality data, HD and stroke currently claim more lives each year than cancer and chronic lower respiratory disease combined. In 2020, 207.1 of 100 000 people died of HD and stroke.
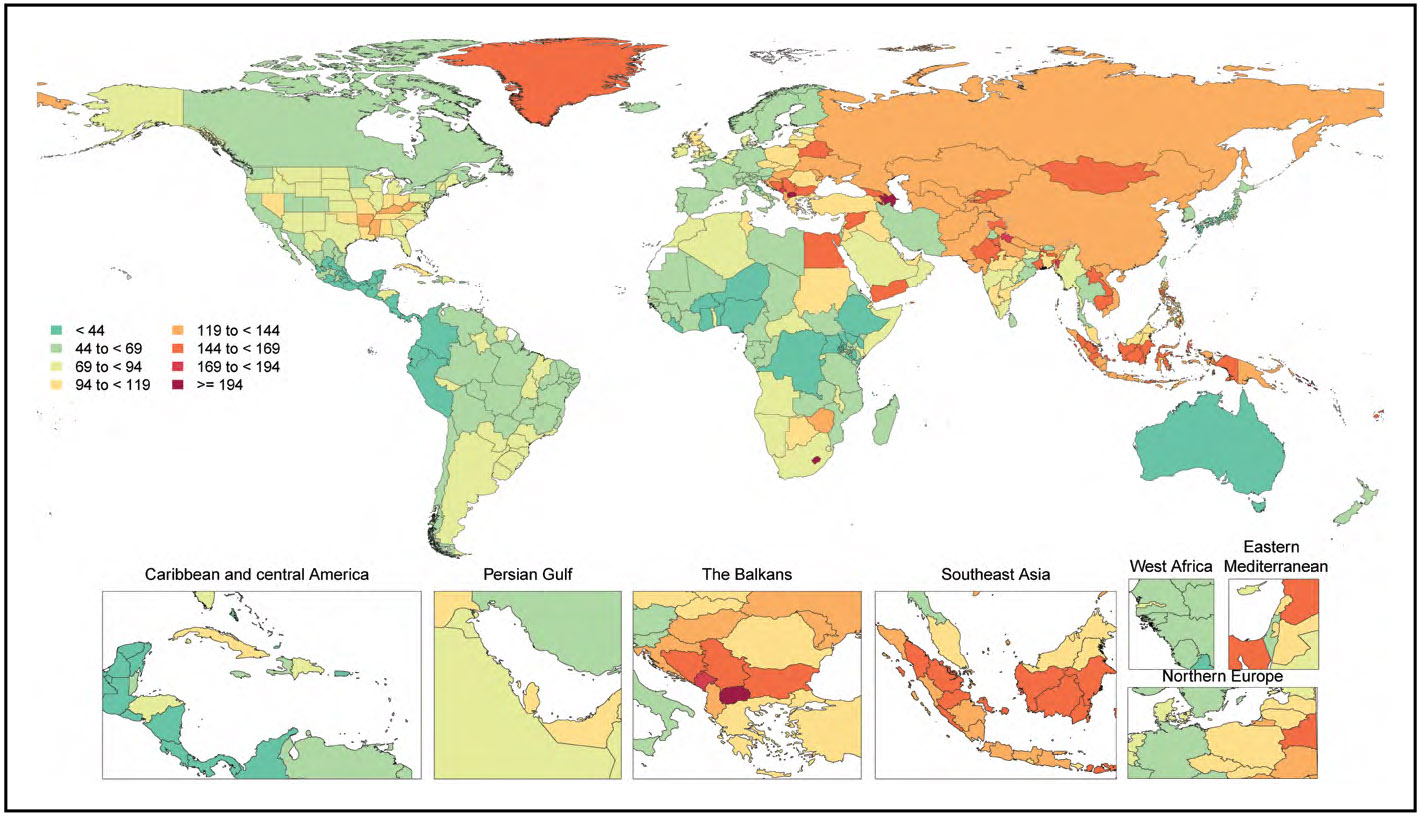
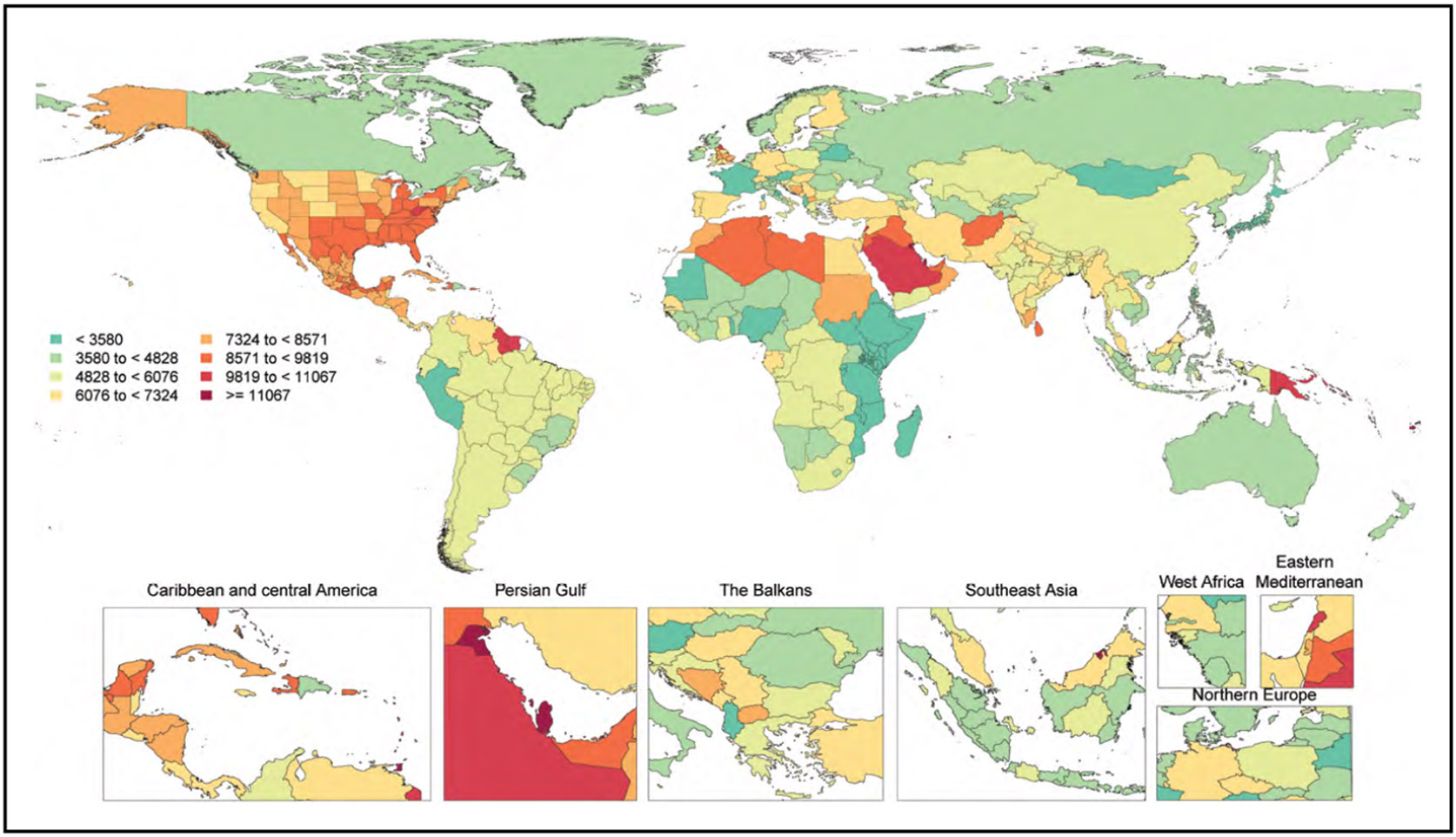
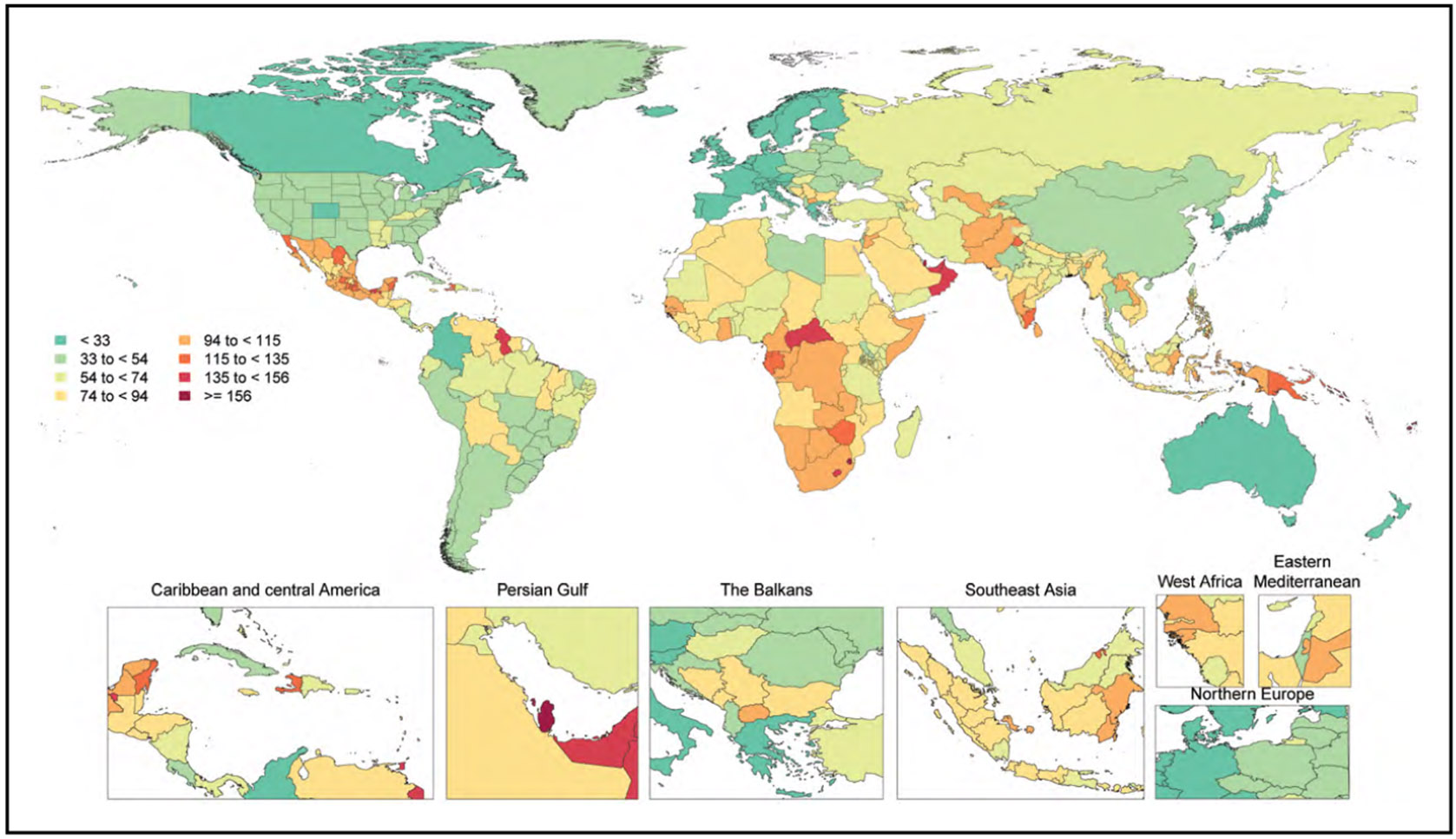
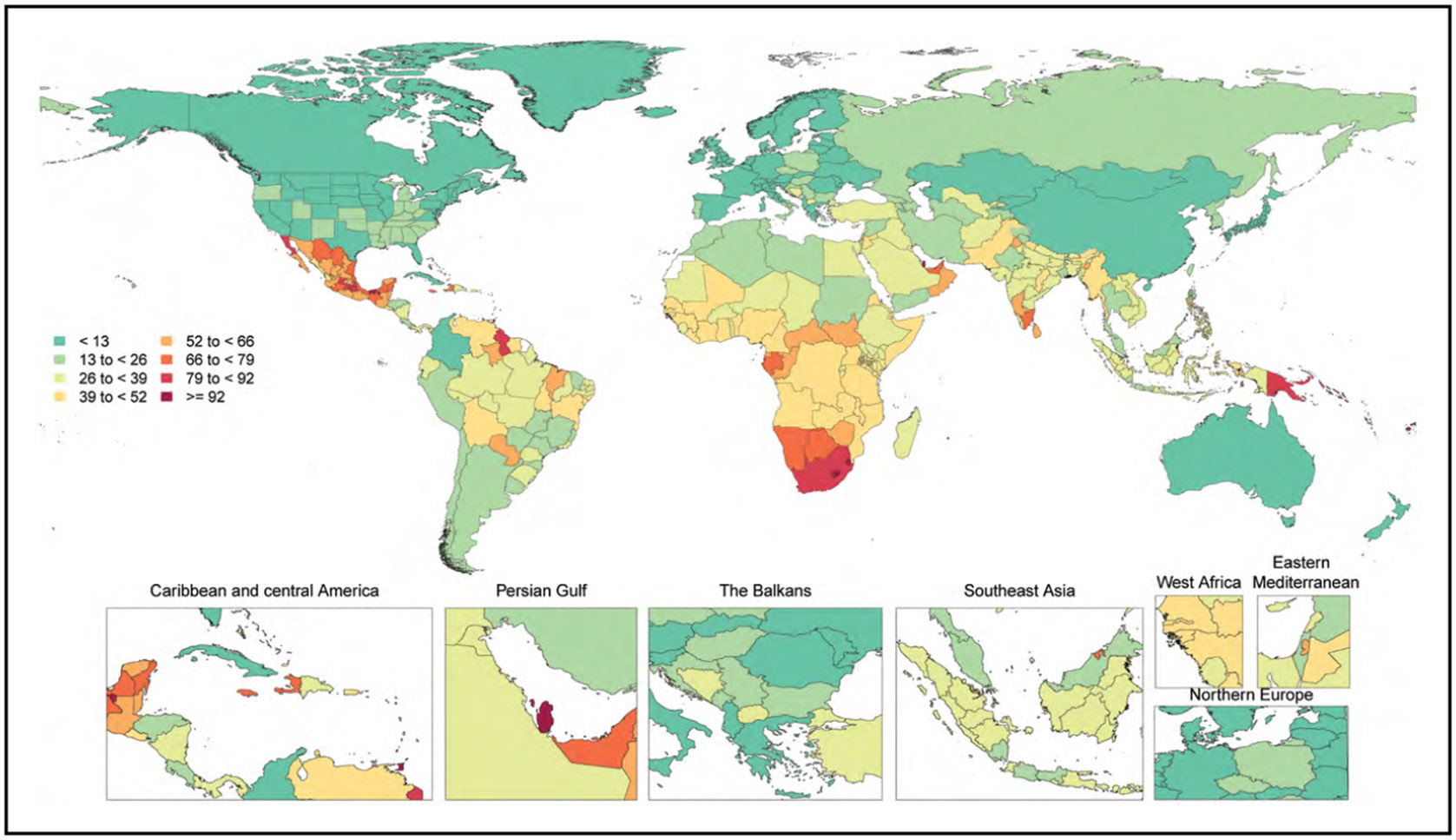
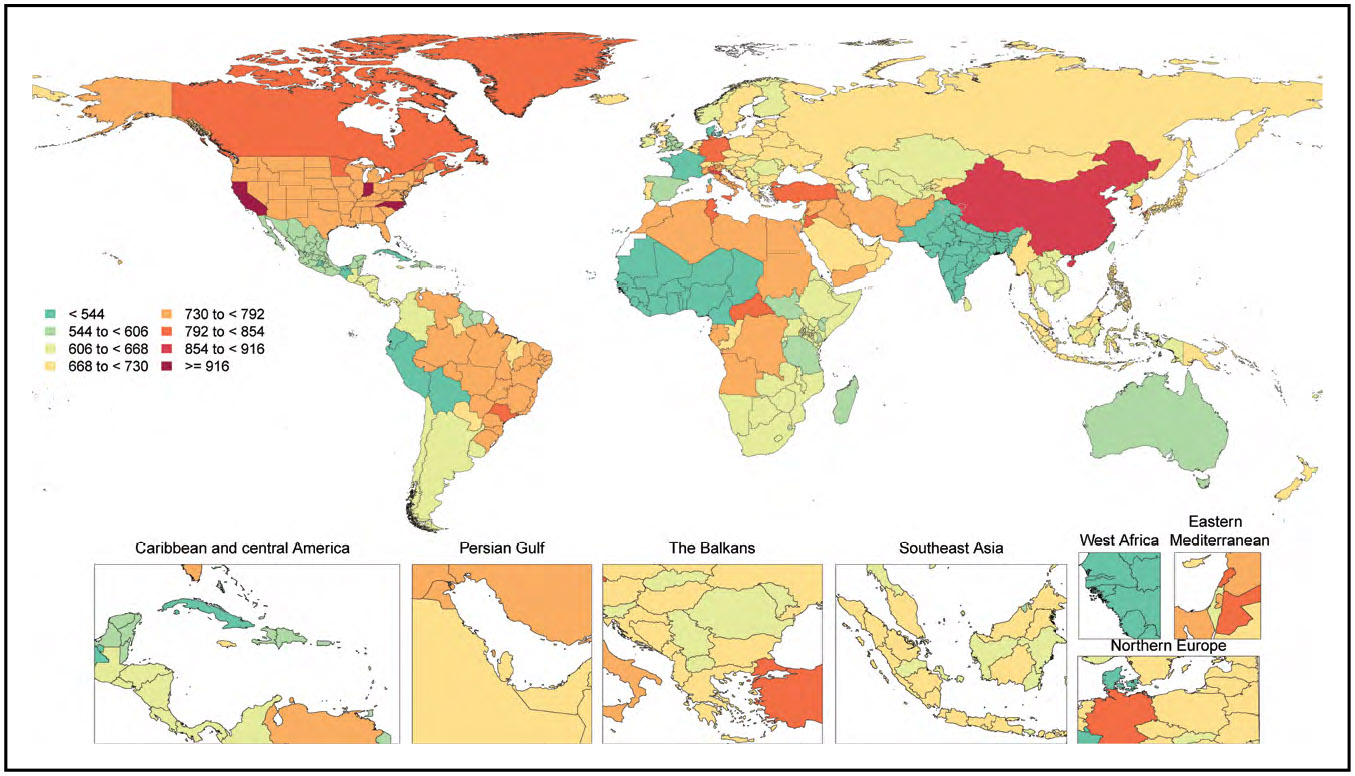
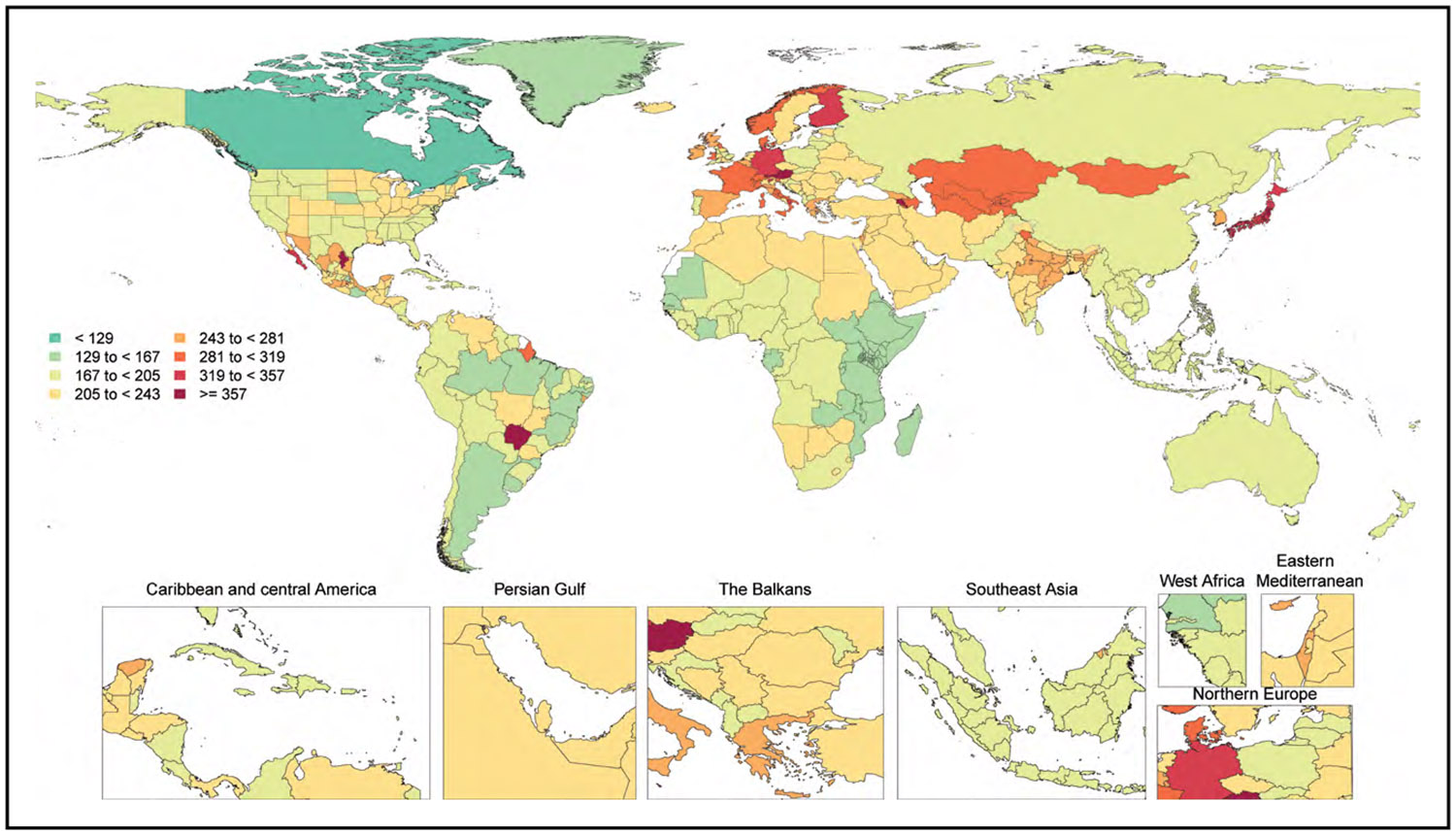
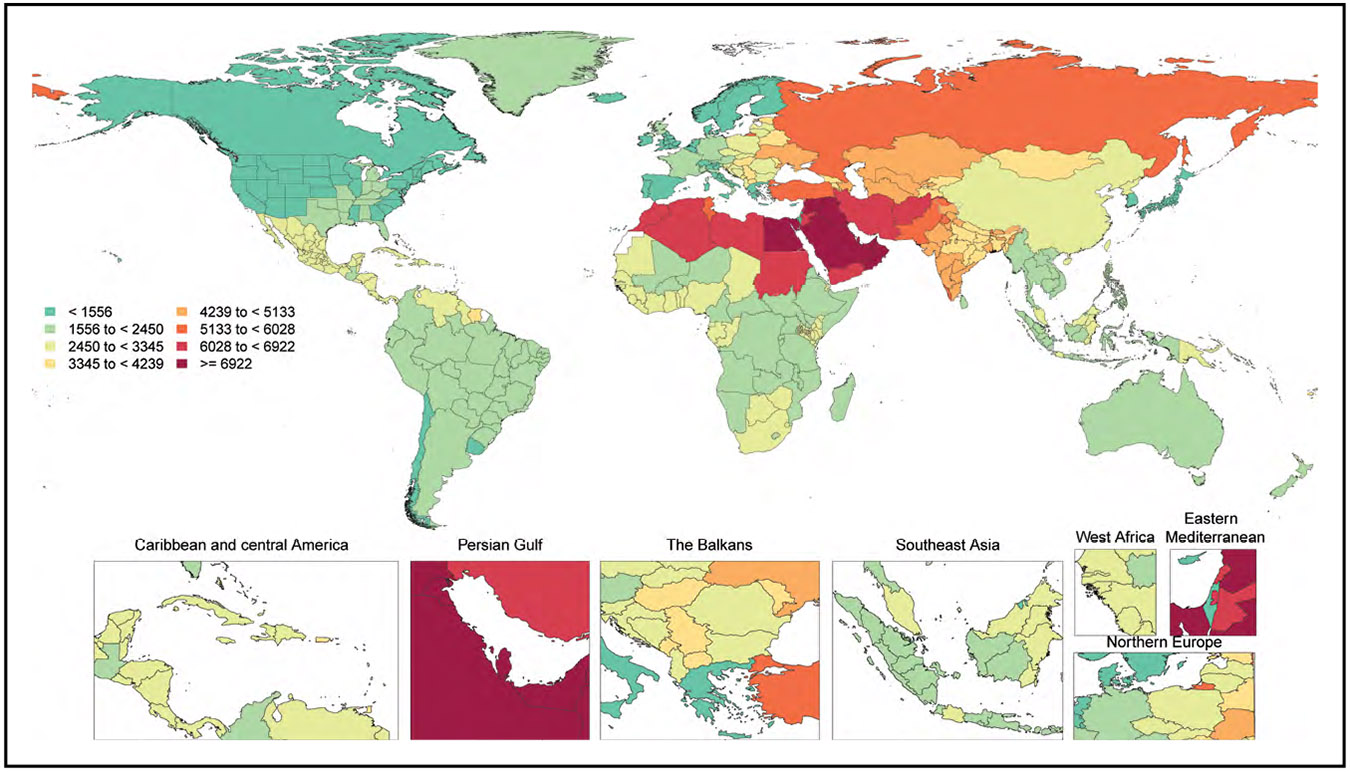
In 2020, 19.05 million deaths were estimated for CVD globally, which amounted to an increase of 8.71% from 2010. The age-standardized death rate per 100 000 population was 239.80, which represents a decrease of 12.19% from 2010. Overall, the crude prevalence of CVD was 607.64 million cases in 2020, an increase of 29.01% compared with 2010. However, the age-standardized prevalence rate was 7354.05 per 100 000, an increase of 0.73% from 2010.
Stroke (Cerebrovascular Diseases) (Chapter 15)
An analysis of data from the GBD 2019 study found that from 1990 to 2019, the absolute number of incident strokes increased by 70.0, whereas the age-standardized incidence rate for total stroke decreased by 17.0%. The age-standardized incidence rate for ischemic stroke decreased by 10% and intracerebral hemorrhage decreased by 29% during the same period.
A meta-analysis of 11 clinical trials from 1970 to 2021 with 20 163 patients with stroke found that intensive LDL-C–lowering statin-based therapies reduced the risk of recurrent ischemic stroke (RR, 0.88) compared with less intensive LDL-C–lowering statin-based therapies. This relationship was even stronger in populations with atherosclerosis (RR, 0.79).
In a meta-analysis of 66 trials of SBP-lowering interventions including 324 812 participants and 11 437 strokes over an average follow-up of 3.3 years, SBP lowering was associated with 21% lower odds of stroke compared with control. In meta-analyses of stroke types, SBP lowering was associated with 14% lower odds of ischemic stroke (6 trials), 28% lower odds of hemorrhagic stroke (6 trials), and 28% lower odds of fatal or disabling stroke (18 trials).
Brain Health (Chapter 16)
The GBD study estimated secular trends from 1990 to 2017 in dementia prevalence, incidence, disability-adjusted life-years (DALYs), and mortality globally and for high-income countries. Globally, prevalent cases increased by 119%, annual incident cases increased by 113%, DALYs increased by 115%, and annual deaths increased by 146%. However, global age-standardized prevalence decreased by 4%, age-standardized annual incidence decreased by 5%, age-standardized DALYs decreased by 6%, and age-standardized annual mortality decreased by 4%. For high-income countries, percent increases in absolute burden measures were smaller than globally: Prevalent cases increased by 93%, annual incident cases increased by 87%, DALYs increased by 90%, and annual deaths increased by 126%. The age-standardized prevalence in high-income countries decreased by 5%, age-standardized annual incidence rate decreased by 6%, age-standardized DALYs decreased by 7%, and age-standardized annual mortality rate decreased by 4%.
Among 229 976 participants in the UK Biobank, with 2143 cases of incident dementia over a median follow-up of 9 years, each 1-point increment in Life's Simple 7 score was associated with an 11% lower hazard of dementia (HR, 0.89). Each 1-point increment in the biological component score (based on blood pressure, cholesterol, and glucose) was associated with a 7% lower hazard of dementia (HR, 0.93). However, a 1-point increment in the lifestyle component score (based on smoking, body mass index, diet, and physical activity) was not associated with dementia (HR, 0.99).
In the HRS (Health and Retirement Study), cognitive impairment-free life expectancy at 55 years of age was estimated as 23.0 years for participants with no hypertension, HD, diabetes, or stroke; 21.2 years for those with any 1 of those conditions; 18.1 years for those with any 2 conditions; and 14.0 years for those with any 3 or all 4 conditions. The association of CVD burden with lower cognitive impairment-free life expectancy was also observed at 65, 75, and 85 years of age, with lower absolute life expectancies.
Congenital Cardiovascular Defects and Kawasaki Disease (Chapter 17)
2020 mortality related to congenital cardiovascular defects was 2817 deaths in the United States, an 11.9% decrease from the number of deaths in 2010.
Socioeconomic status (SES) is a major contributor to identified differences in infant mortality among infants with critical congenital cardiovascular defects, with greater mortality among socioeconomically deprived patients (OR, 1.7).
Since May 2020, the Centers for Disease Control and Prevention has been tracking reports of multisystem inflammatory syndrome in children. As of March 1, 2022, 7459 cases and 63 attributable deaths (0.84%) have been reported. Median age of cases was 9 years; 58% of cases have occurred in children who are Hispanic or Latino (1846 cases) or Black (2206 cases); 98% tested positive for SARS-2 (severe acute respiratory syndrome coronavirus 2; reverse transcriptase–polymerase chain reaction, serology, or antigen test); and 60% of reported patients were male.
Disorders of Heart Rhythm (Chapter 18)
An analysis of the Korea National Health Insurance Service (N=66 692) classified individuals by exercise status before and after AF diagnosis. Those who maintained exercise were significantly less likely to have ischemic stroke (HR, 0.86), HF (HR, 0.92), or mortality (HR, 0.61) than those who continued to abstain from exercise after AF diagnosis.
The study of social determinants and AF remains limited. In a limited-sized cohort (N=339) followed up for a median of 2.6 years (range, 0–3.4 years), individuals in the lowest income category (≤$19 999/y) had a 2.0-fold greater hospitalization risk (OR, 2.11) compared with those in the highest income category (≥$100 000/y).
A multicenter trial randomized individuals with at least 1 stroke risk factor and without AF in a 1:3 ratio to receive long-term rhythm monitoring with an implanted loop recorder (n=1501) or usual care (n=4503). Over a median follow-up of 64.5 months, those randomized to monitoring were 3-fold more likely to be diagnosed with AF (HR, 3.17).
Sudden Cardiac Arrest, Ventricular Arrhythmias, and Inherited Channelopathies (Chapter 19)
Recent data describing cardiac arrest or sudden cardiac death after an acute myocardial infarction suggest that contemporary short-term (3-month) risk is 0.29% or 116 per 100 000 person-years.
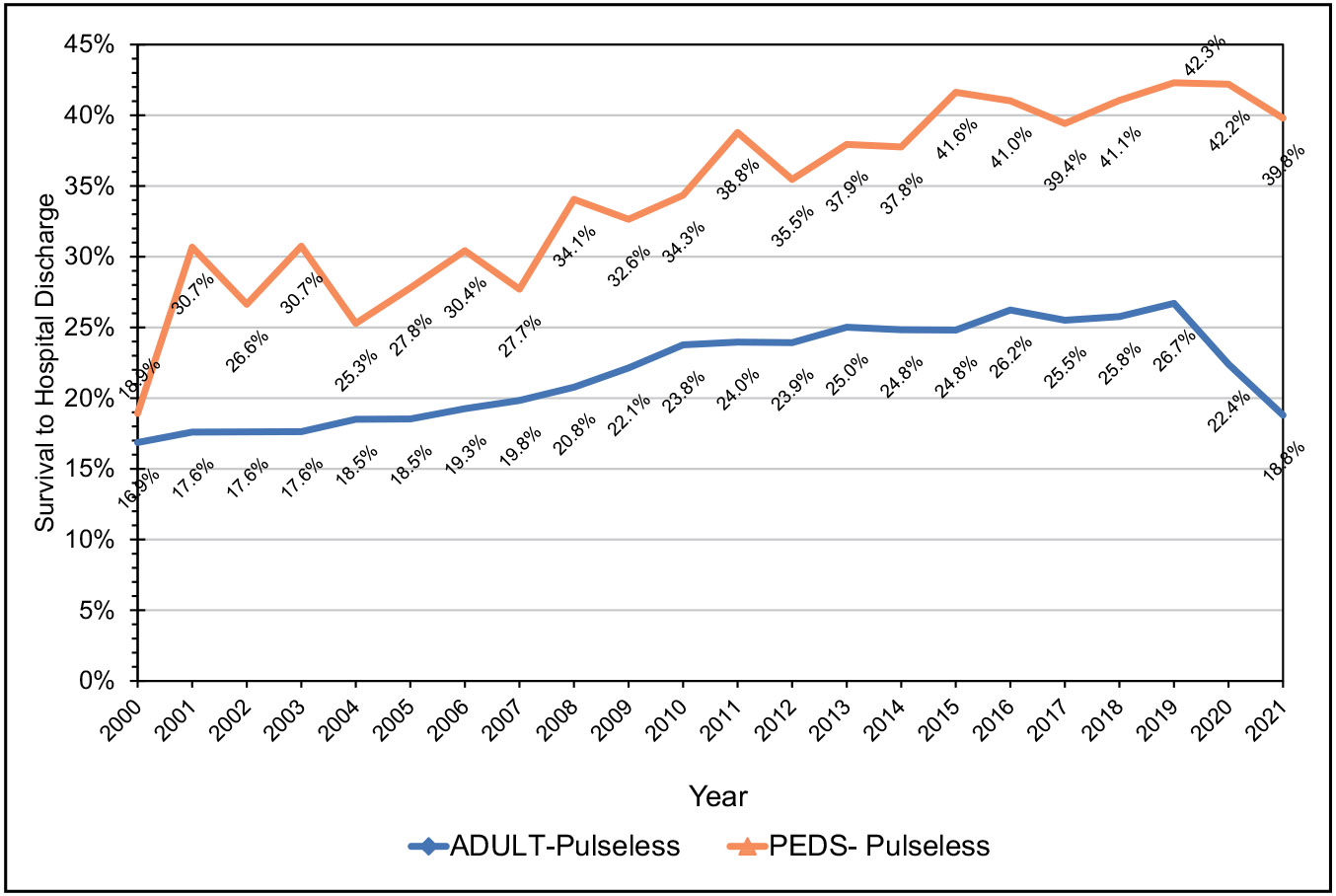
Laypeople in the United States initiated cardiopulmonary resuscitation in 40.2% of out-of-hospital cardiac arrests in 2021.
In the United States, individuals from underrepresented racial and ethnic groups are at substantially higher risk of sudden cardiac arrest and experience worse survival and neurological outcomes after sudden cardiac arrest compared with White individuals. In the ARIC study (Atherosclerosis Risk in Communities), the sex-adjusted HR for sudden cardiac death comparing Black with White participants was 2.12, and the fully adjusted HR was 1.38. In San Francisco, Black females had a 2.55 higher incidence of sudden arrhythmic death than White females.
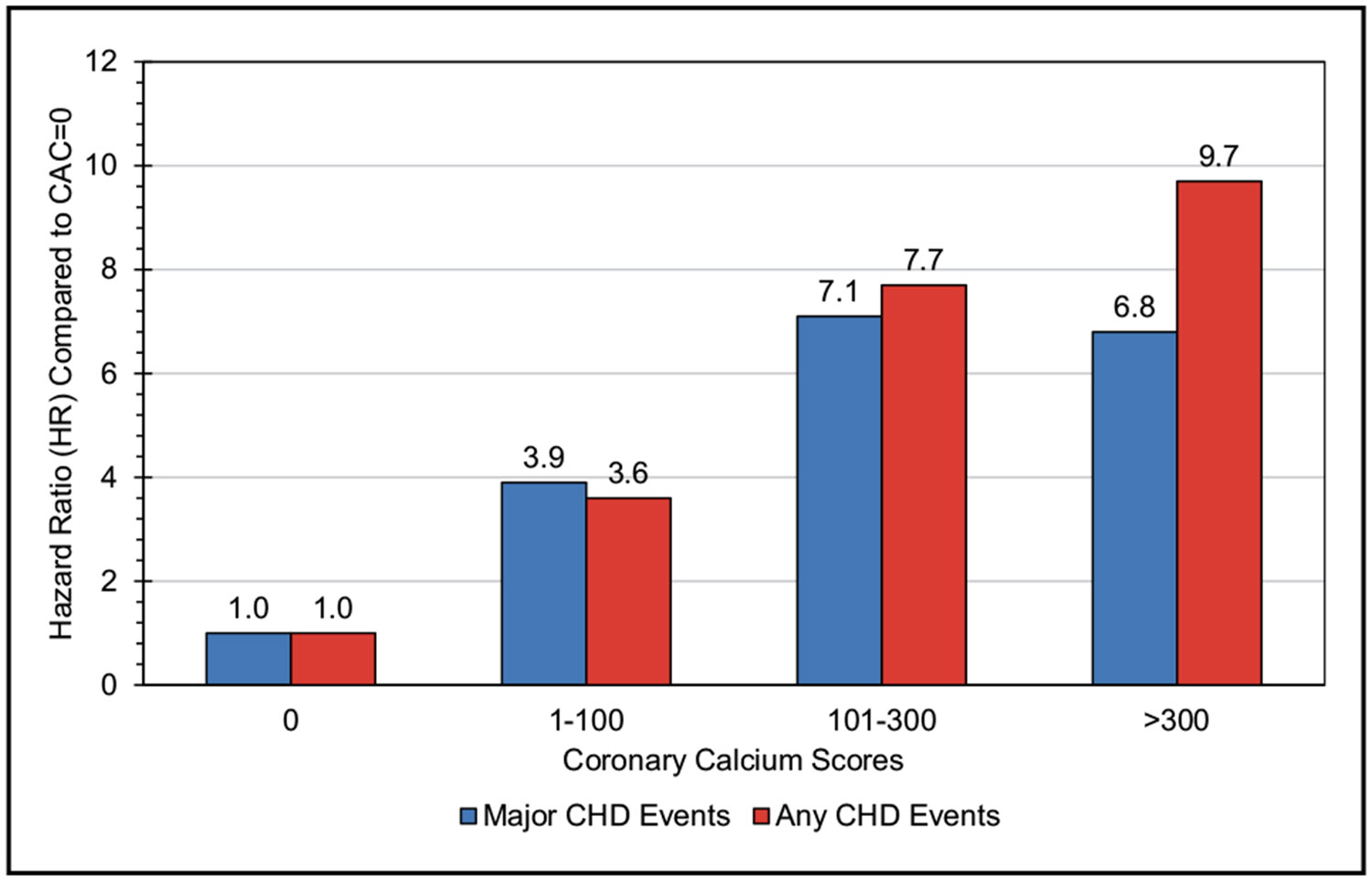
Subclinical Atherosclerosis (Chapter 20)
In a study-level meta-analysis involving 10 867 participants (6699 HIV positive, 4168 HIV negative; mean age, 52 years; 86% male; 32% Black), the prevalence of noncalcified plaque was 49% in HIV-positive individuals versus 20% in HIV-negative individuals (OR, 1.23).
In individuals without diabetes or CVD, higher hemoglobin A1c was associated with the extent of subclinical atherosclerosis assessed by intima-media thickness; atherosclerotic plaque of the carotids, abdominal aorta, and iliofemoral arteries; and coronary artery calcification (OR, 1.05, 1.27, 1.27, 1.36, 1.80, 1.87, and 2.47 for hemoglobin A1c 4.9%–5.0%, 5.1%–5.2%, 5.3%–5.4%, 5.5%–5.6%, 5.7%–5.8%, 5.9%–6.0%, and 6.1%–6.4%, respectively; reference hemoglobin A1c ≤4.8%).
In the Rotterdam Study of older adults, the presence of intraplaque hemorrhage (but not calcification or lipid-rich core) by high-resolution magnetic resonance imaging demonstrated an association with incident stroke and CHD (HR, 2.42 and 1.95, respectively).
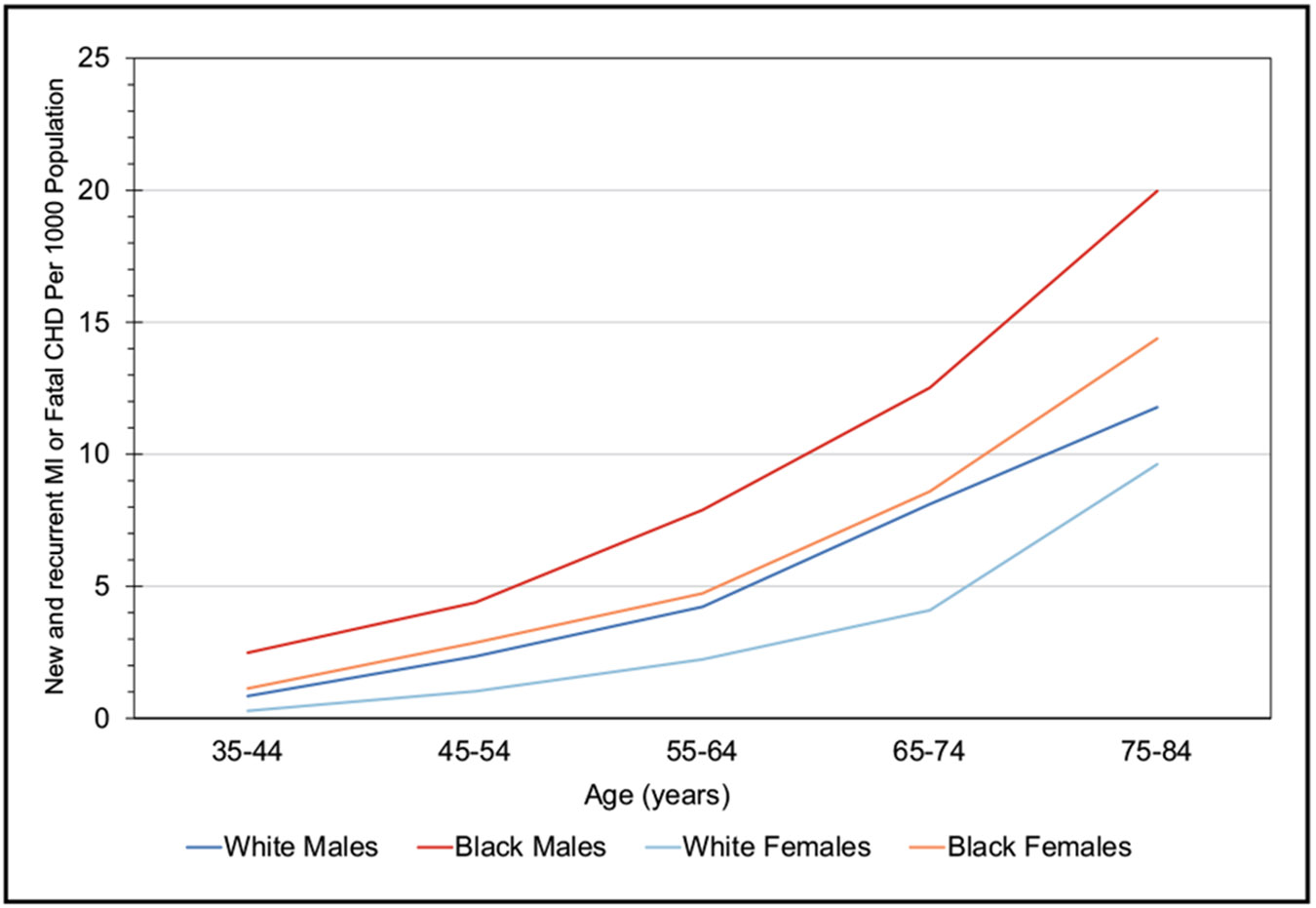
Coronary Heart Disease, Acute Coronary Syndrome, and Angina Pectoris (Chapter 21)
According to data from the 2005 to 2014 ARIC study, the estimated annual incidence of myocardial infarction is 605 000 new attacks and 200 000 recurrent attacks. Of these 805 000 first and recurrent events, it is estimated that 170 000 are silent.
An NIS (National Inpatient Sample) analysis of sex differences spanning 2004 to 2015 identified 7 026 432 hospitalizations for acute myocardial infarction. Compared with males, females were less likely to undergo coronary angiography (adjusted OR, 0.92) and percutaneous coronary intervention (adjusted OR, 0.82), Females had a higher risk of mortality (adjusted OR, 1.03) compared with males.
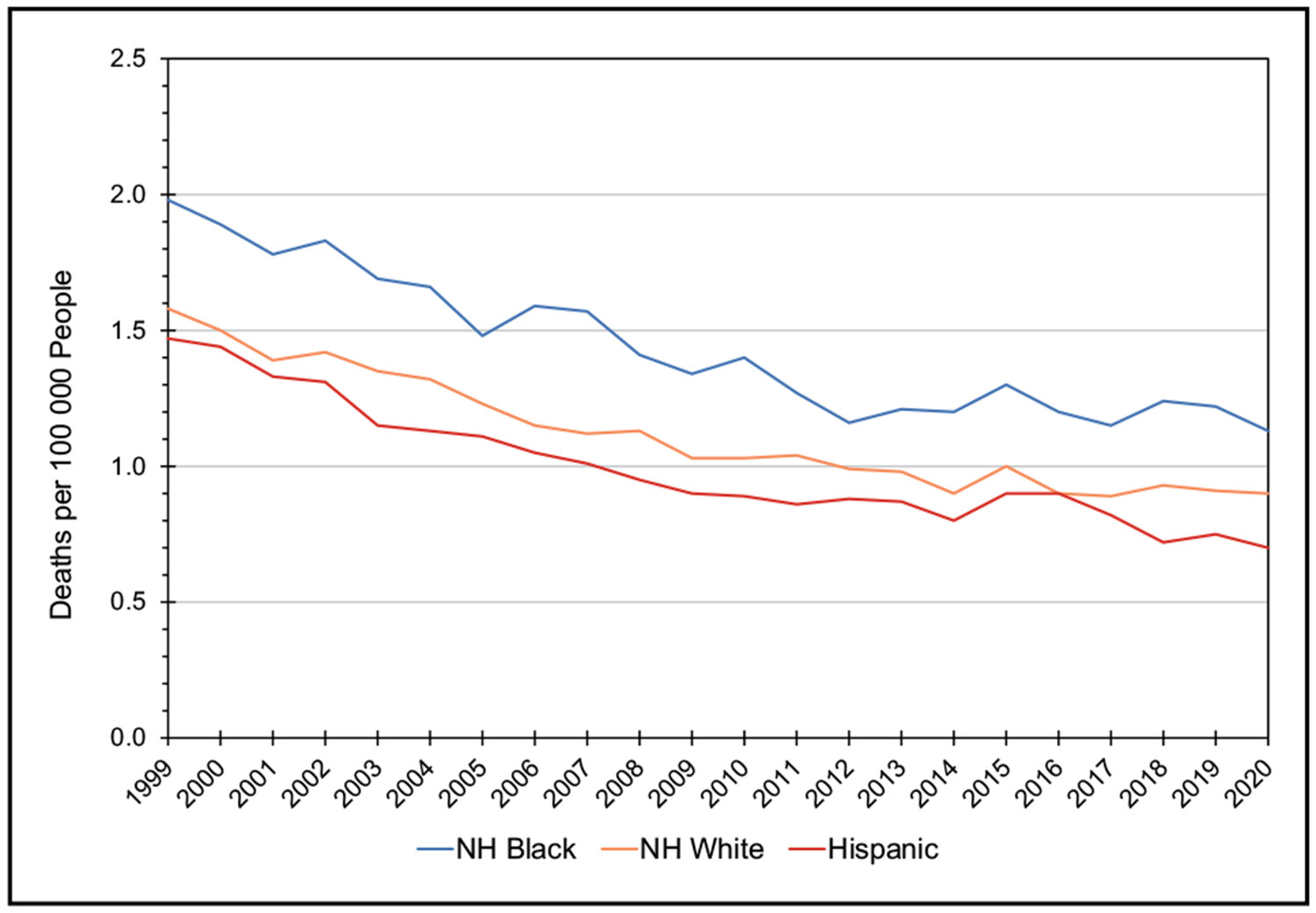
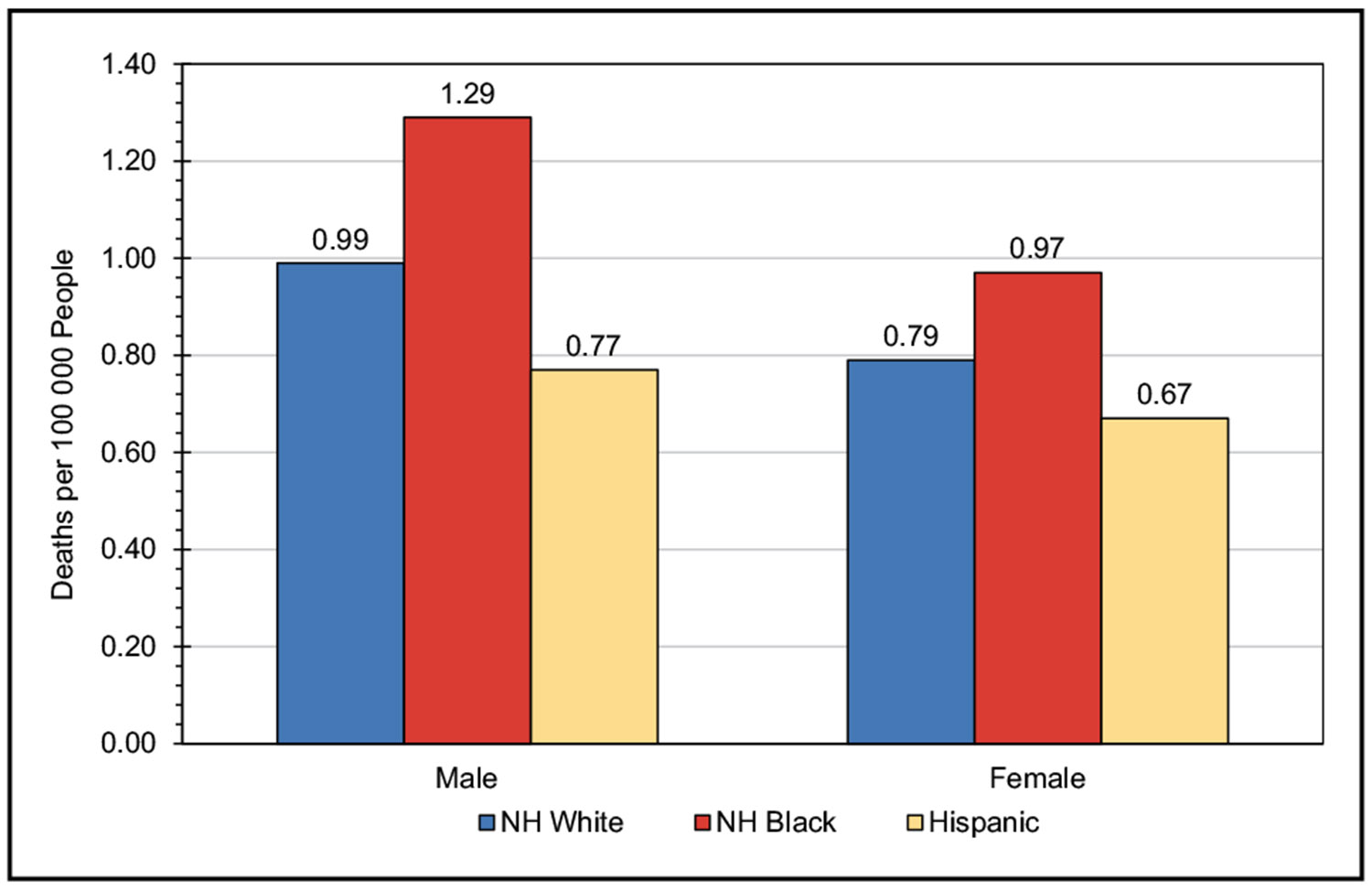
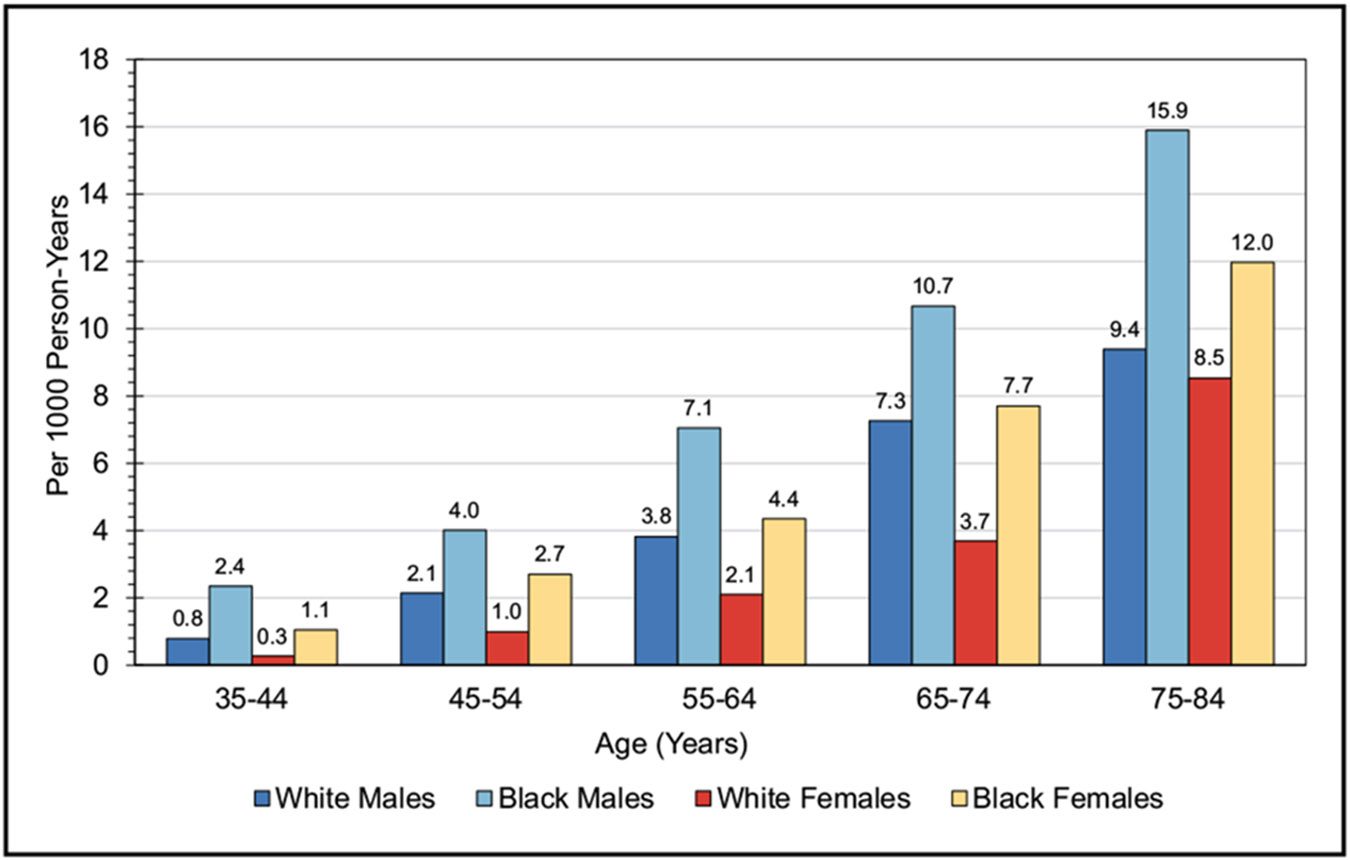
In 2020, CHD age-adjusted death rates per 100 000 were 128.5 for NH White males, 153.6 for NH Black males, and 102.2 for Hispanic males. For NH White females, the rate was 63.8; for NH Black females, it was 85.9; and for Hispanic females, it was 54.2.
Cardiomyopathy and Heart Failure (Chapter 22)
On the basis of data from NHANES 2017 to 2020, ≈6.7 million Americans ≥20 years of age had HF, which is increased from ≈6.0 million according to NHANES 2015 to 2018.
The lifetime risk of HF at 50 years of age increased among participants of the FHS (Framingham Heart Study) when comparing two 25-year epochs (1965–1989 versus 1990–2014) from 18.9% to 22.6% in females and 19.1% to 25.3% in males.
Some data suggest that improvements in survival in individuals with HF could be leveling off over time. Data from the Rochester Epidemiology Project in Olmsted County, Minnesota, showed improved survival after HF diagnosis between 1979 and 2000; however, estimated 5-year mortality for those with HF did not decline from 2000 to 2010 and remained high (52.6% overall; 24.4% for those 60 years of age; and 54.4% for those 80 years of age).
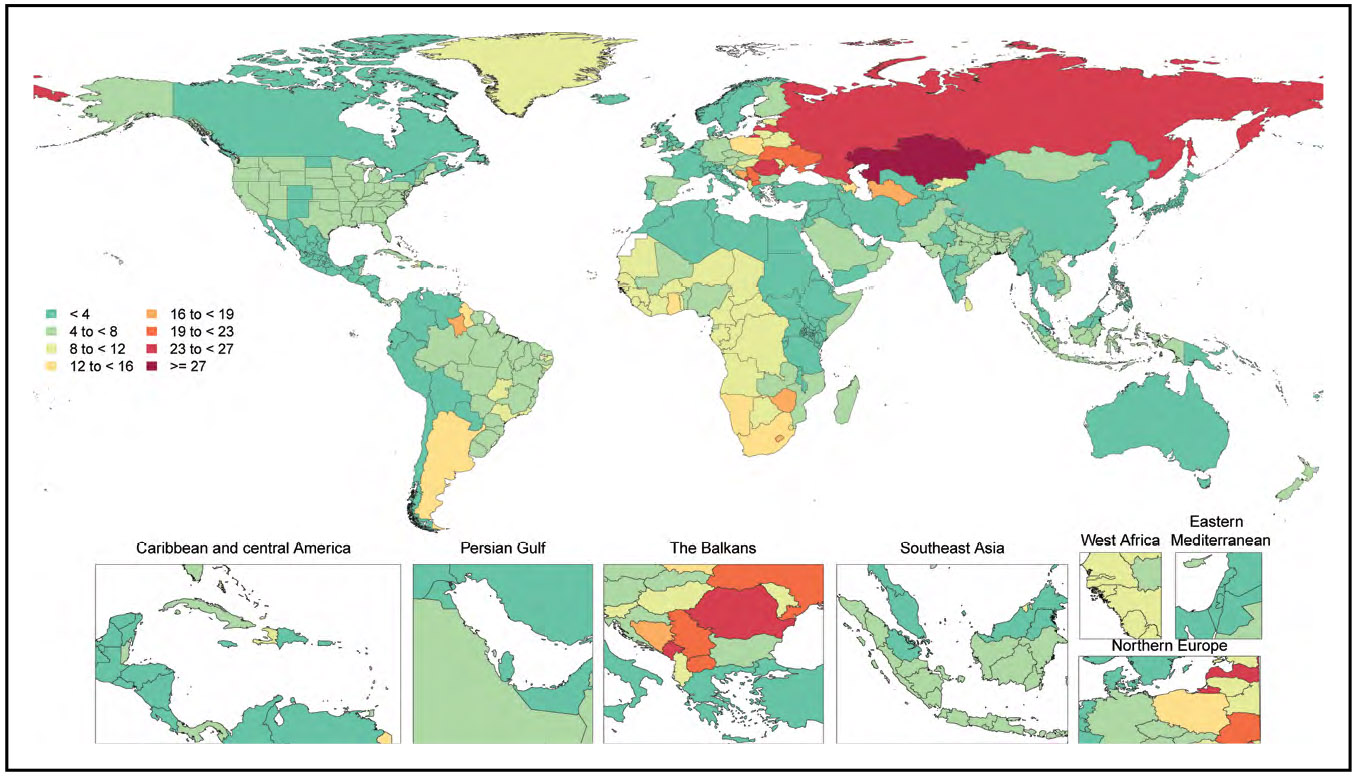
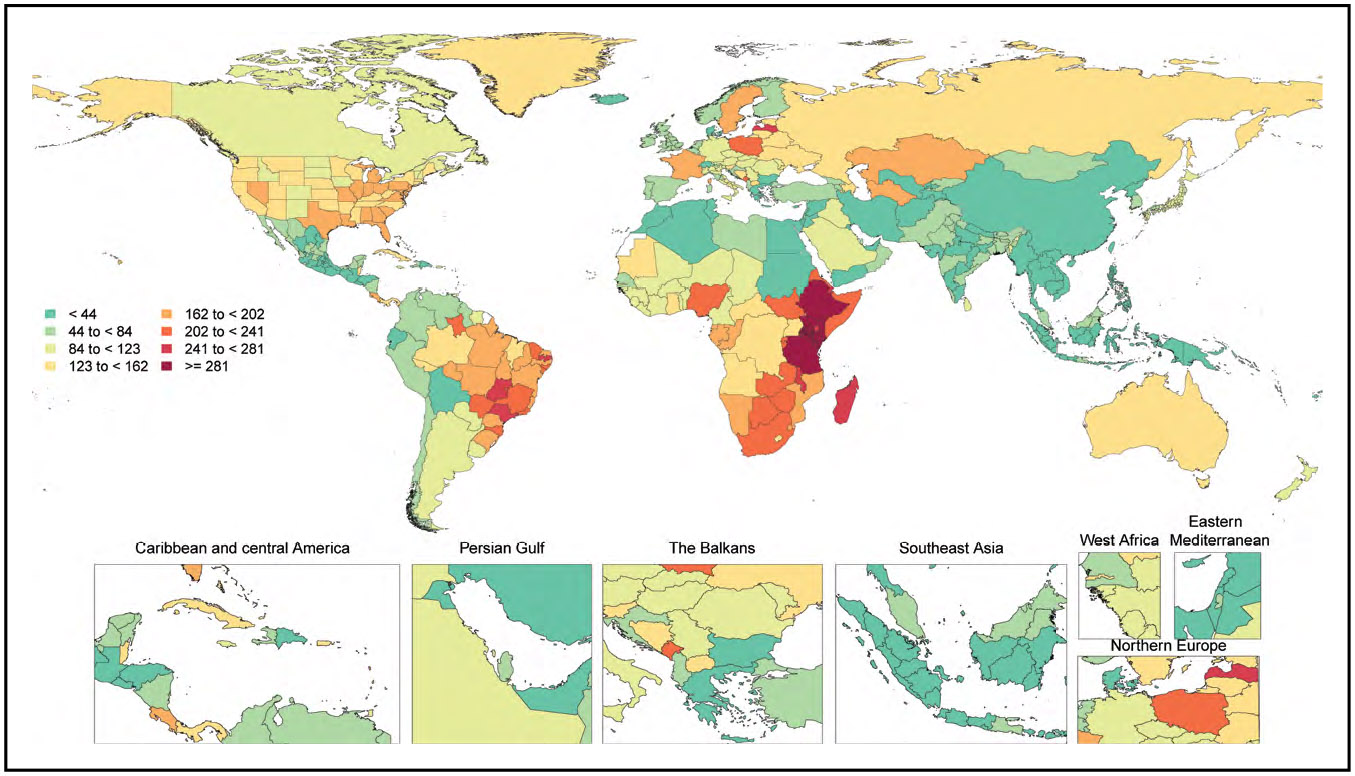
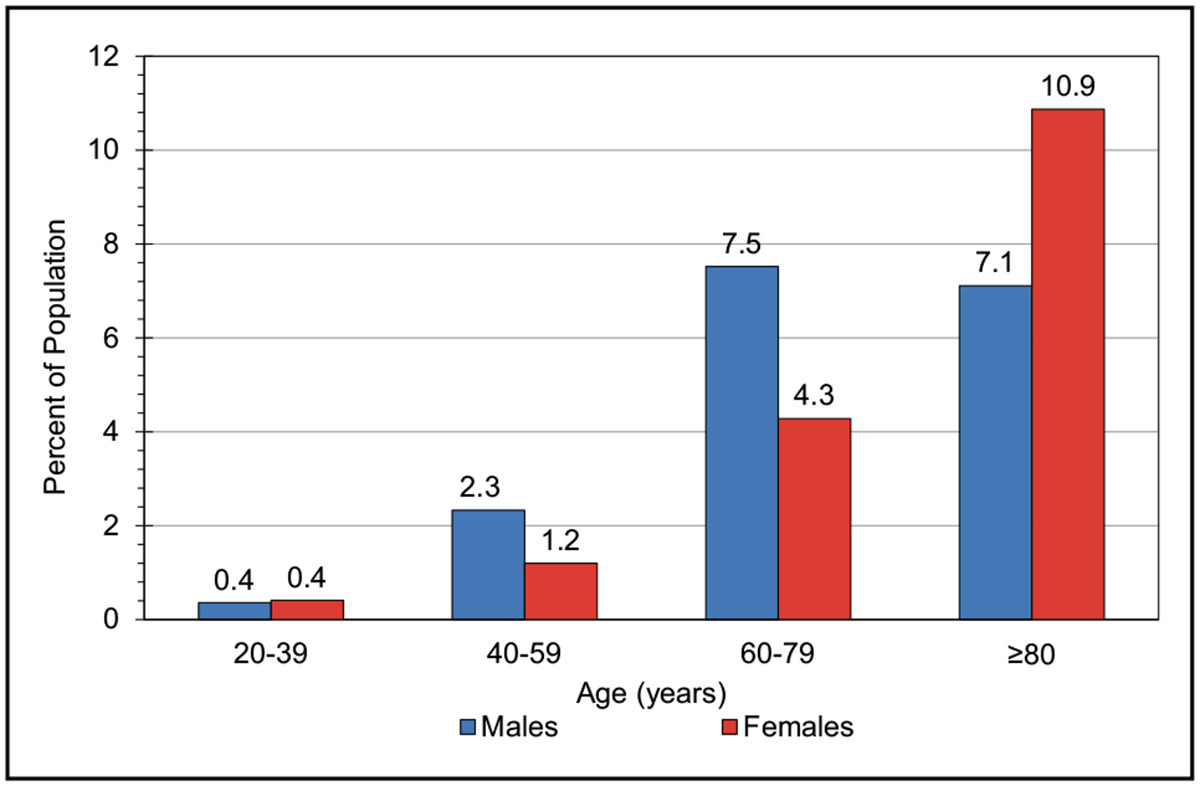
Valvular Diseases (Chapter 23)
The number of elderly patients with calcific aortic stenosis is projected to more than double by 2050 in both the United States and Europe according to a simulation model in 7 decision analysis studies. The pooled prevalence of all aortic stenosis in the elderly was 12.4%, and the prevalence of severe aortic stenosis was 3.4%.
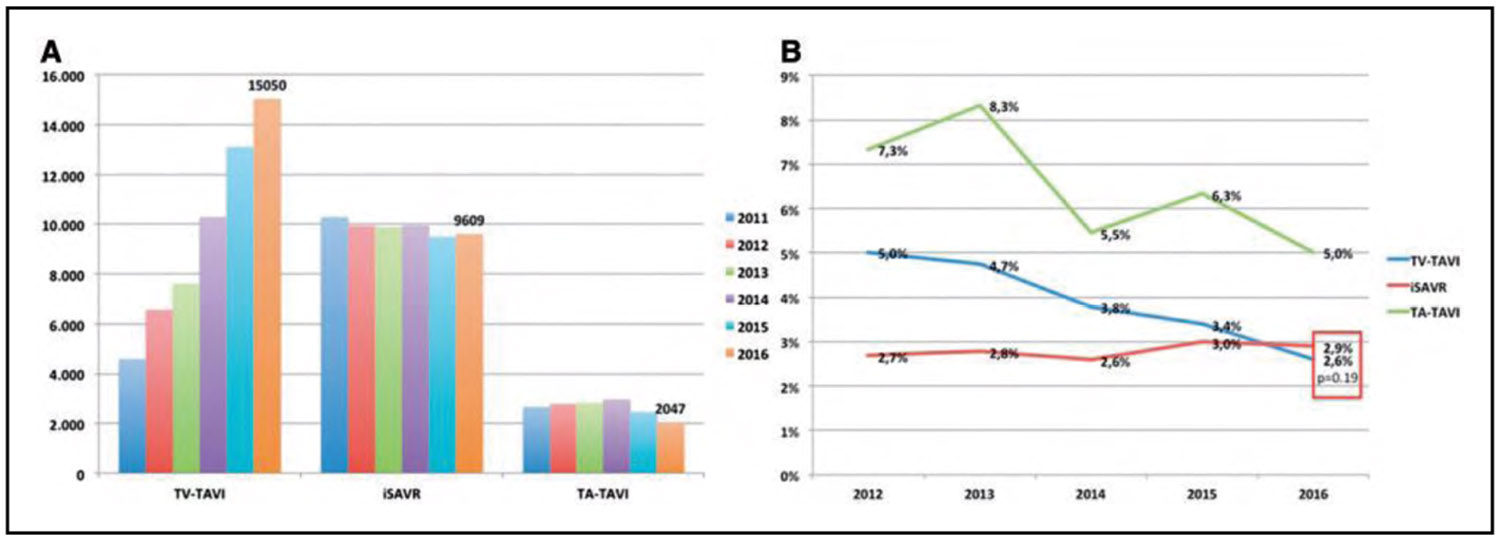
In 1000 patients with severe aortic stenosis at low surgical risk randomized in the PARTNER 3 trial (Placement of Aortic Transcatheter Valve 3) to either balloon-expandable transcatheter aortic valve replacement (TAVR) or surgical aortic valve replacement, the primary composite end point (death, stroke, or rehospitalization) rate was significantly lower in the TAVR versus surgical aortic valve replacement group (8.5% versus 15.1%; absolute difference, −6.6 percentage points for noninferiority; HR, 0.54). At 2 years, the primary end point was significantly reduced after TAVR compared with surgical aortic valve replacement (11.5% versus 17.4%; HR, 0.63), although TAVR valve thrombosis at 2 years was increased (2.6%; 13 events) compared with surgery (0.7%; 3 events).
Among 96 256 transfemoral TAVR procedures, adjusted 30-day mortality was higher at institutions with low procedural volume (3.19%) than at institutions with high procedural volume (2.66%; OR, 1.21).
Venous Thromboembolism (Deep Vein Thrombosis and Pulmonary Embolism), Chronic Venous Insufficiency, Pulmonary Hypertension (Chapter 24)
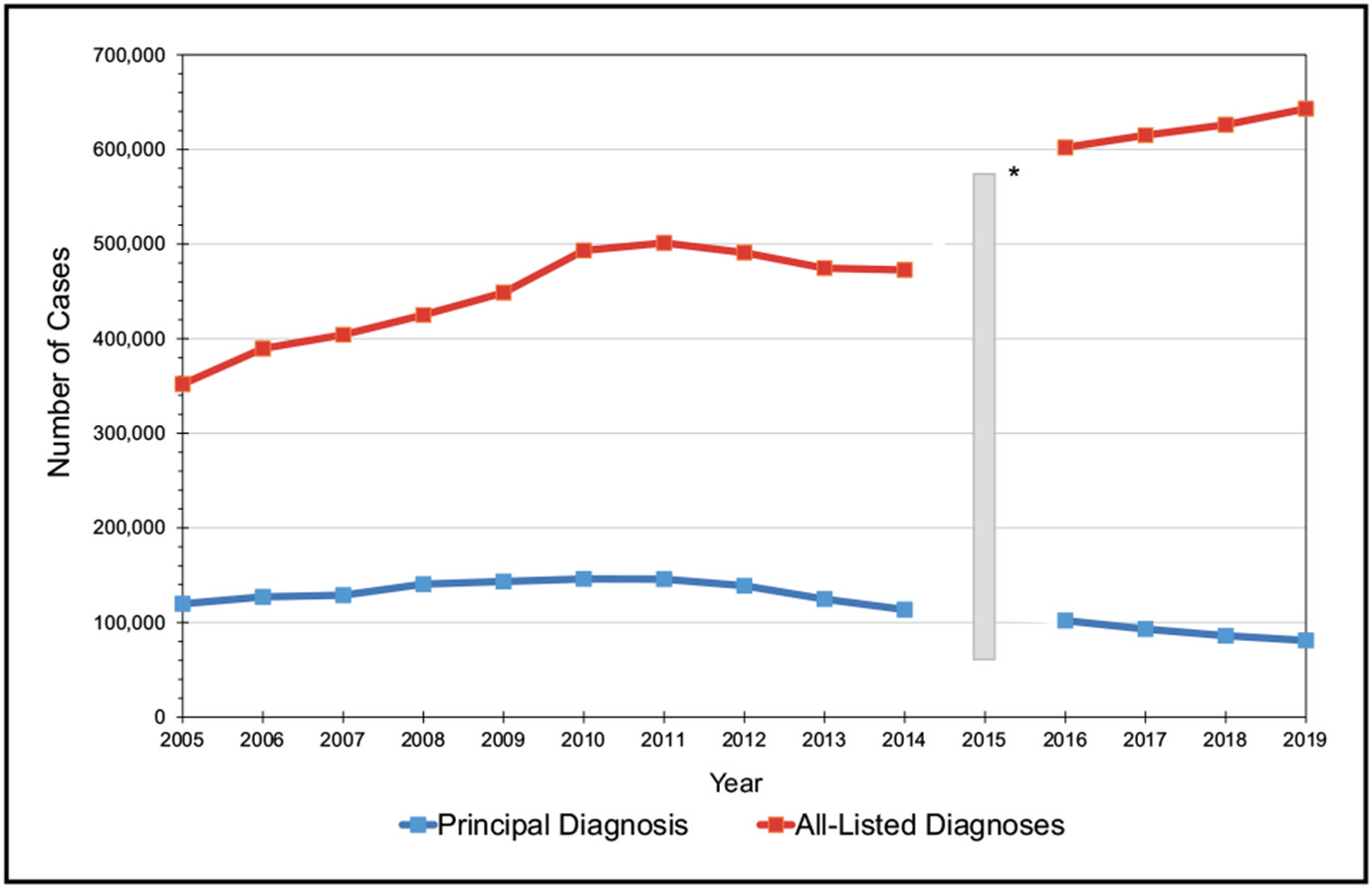
In 2019, there were an estimated ≈393 000 cases of pulmonary embolism, ≈643 000 cases of deep vein thrombosis, and ≈1 036 000 total venous thromboembolism cases in the United States.
In patients with COVID-19, there is a double risk of death after venous thromboembolism. In those admitted to the intensive care unit, this risk is 2.63 times higher, with a 3-fold increase in patients on mechanical ventilation.
In 2018, there were 578 000 outpatient visits for pulmonary hypertension as the principal diagnosis. In addition, there were 14 000 hospital discharges with pulmonary hypertension as the principal diagnosis.
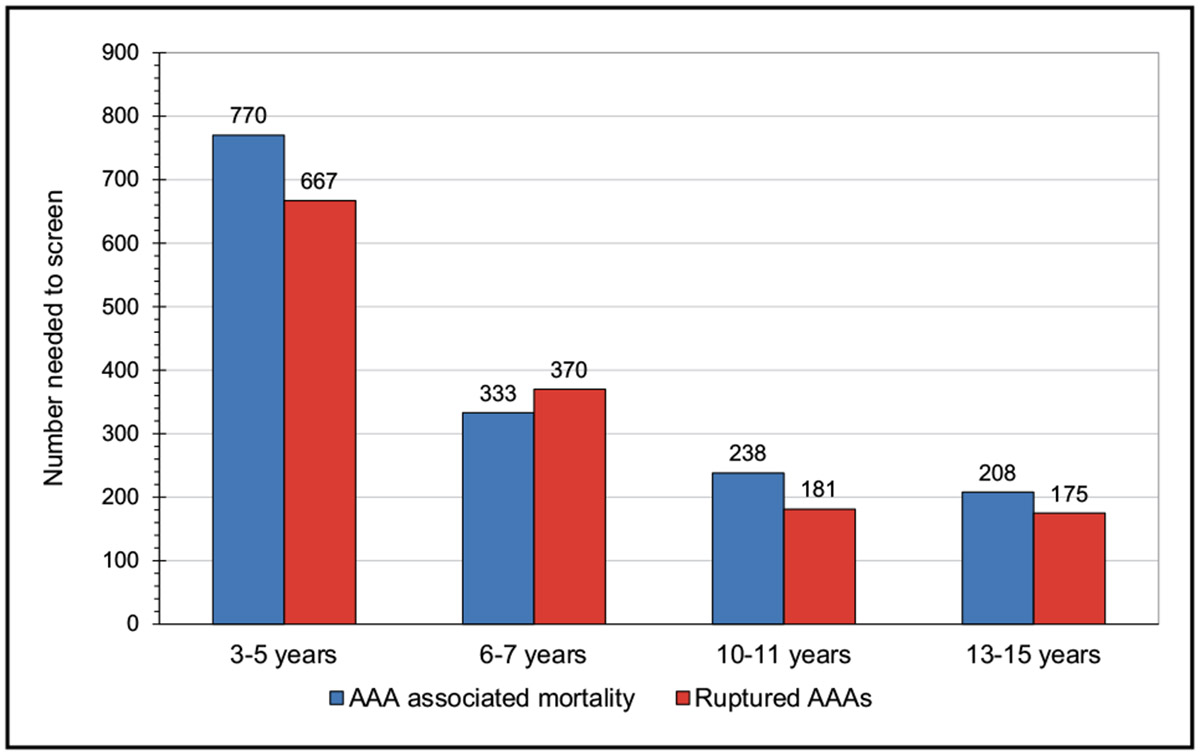
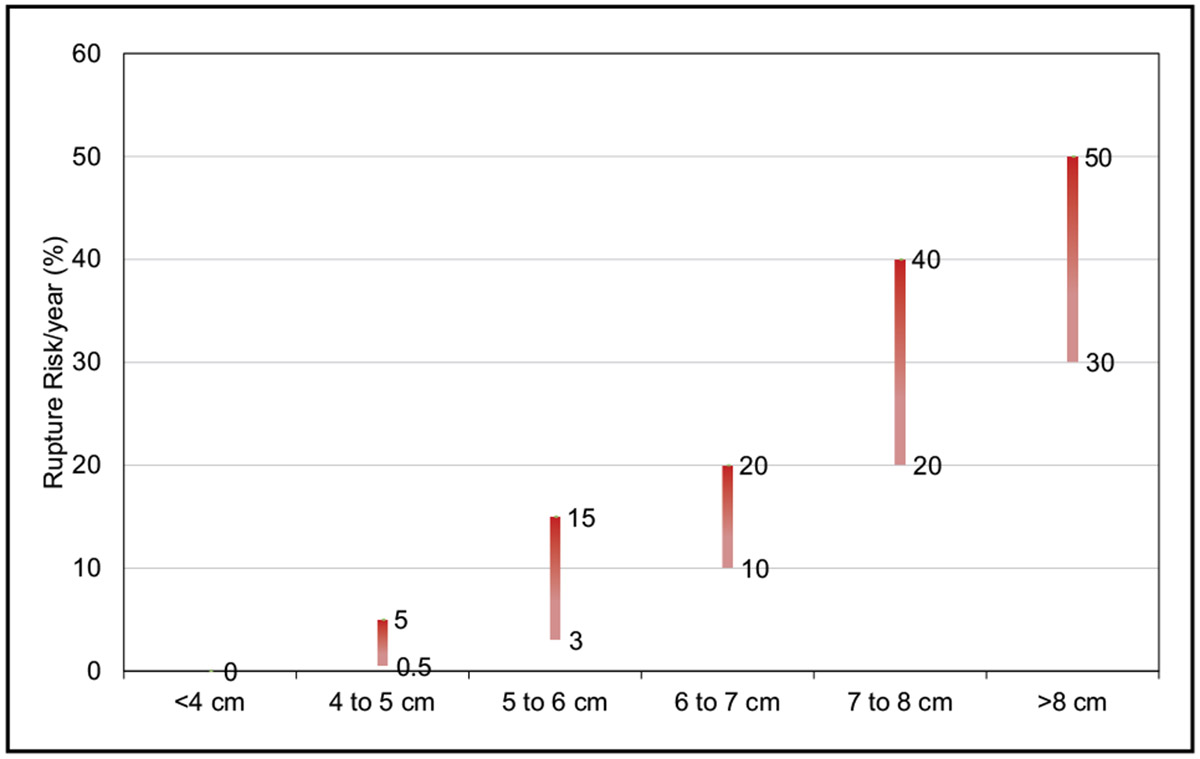
Peripheral Artery Disease and Aortic Diseases (Chapter 25)
Data from MarketScan and Medicare databases showed that only 33.9% of patients with peripheral artery disease were prescribed statins compared with 51.7% of patients with coronary artery disease, and only 24.5% of patients with peripheral artery disease in the MarketScan database achieved a target LDL-C <70 mg/dL.
Among Medicare beneficiaries, zip codes in the top quartile of amputation rates had a larger mean proportion of Black residents than zip codes in the bottom quartile (17.5% versus 4.4%).
In older individuals 60 to 74 years of age, male sex (OR, 1.9), hypertension (OR, 1.8), and family history (OR, 1.6) are the strongest contributors to risk of thoracic aortic aneurysm.
Quality of Care (Chapter 26)
Despite substantial disruptions to cardiovascular care delivery during the COVID-19 pandemic, among patients in the GWTG Registry (Get With The Guidelines) who were hospitalized for HF in 2021, 91.7% received angiotensin-converting enzyme inhibitors/angiotensin receptor blockers or angiotensin receptor-neprilysin inhibitors at discharge; 93.4% received evidence-based specific β-blockers; 99.2% had a measurement of left ventricular function; and 85.5% had a scheduled postdischarge appointment.
In 18 262 adults with hypertension, the age-adjusted estimated proportion with controlled blood pressure (blood pressure <140/90 mm Hg) improved from 31.8% in 1999 to 2000 to 48.5% in 2007 to 2008, was similar in 2013 to 2014 (53.8%), and then declined to 43.7% in 2017 to 2018.
In 390 692 patients receiving care at 586 hospitals from July 2008 to December 2013, patients residing in lower-SES neighborhoods had longer median arrival-to-angiography time (lowest quintile of SES, 8.0 hours; highest quintile of SES, 3.4 hours) and a higher rate of fibrinolysis (versus primary angioplasty) for ST-segment–elevation myocardial infarction (lowest quintile of SES, 23.1%; highest quintile of SES, 5.9%) compared with higher-SES neighborhoods. Patients from lower-SES neighborhoods had greater independent risk of in-hospital mortality and major bleeding and a lower quality of discharge care.
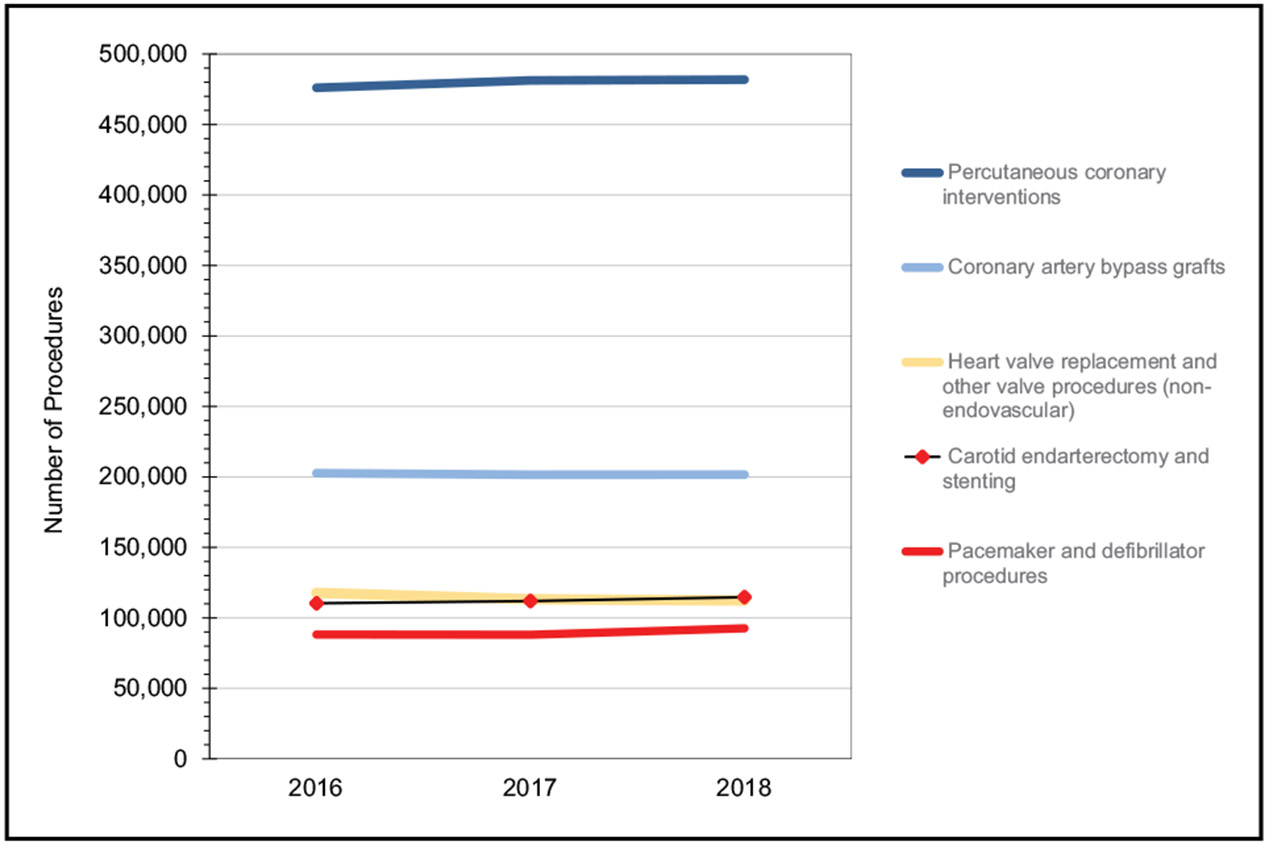
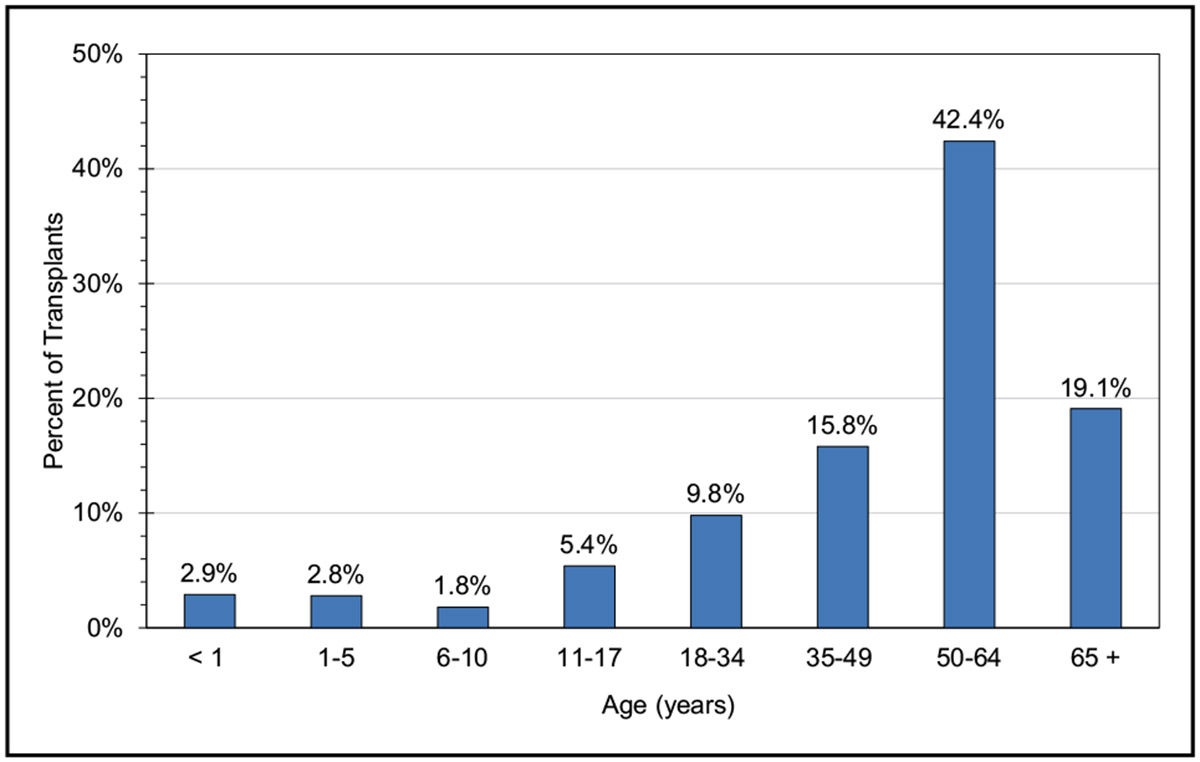
Medical Procedures (Chapter 27)
According to Healthcare Cost and Utilization Project data from the Agency for Healthcare Research and Quality for the year 2018, 481 780 percutaneous coronary interventions were performed on an inpatient basis in the United States.
Data from the Society of Thoracic Surgeons Adult Cardiac Surgery Database, which voluntarily collects data from ≈80% of all hospitals that perform coronary artery bypass grafts in the United States, indicate that a total of 161 816 procedures involved isolated coronary artery bypass graft in 2019.
In 2021, 3817 heart transplantations were performed in the United States, the most ever. The highest numbers of heart transplantations were performed in California (529), Texas (359), New York (307), and Florida (263).
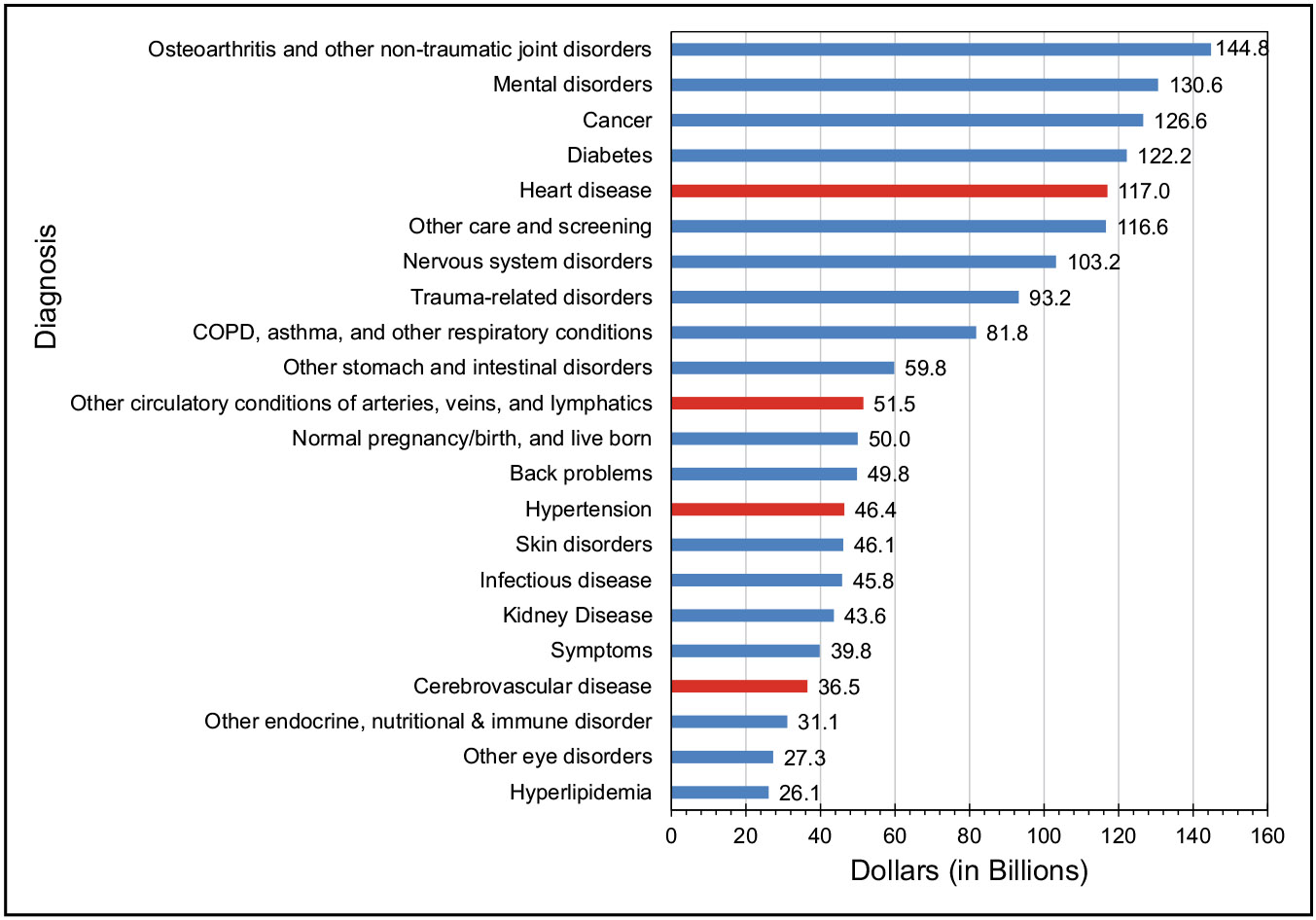
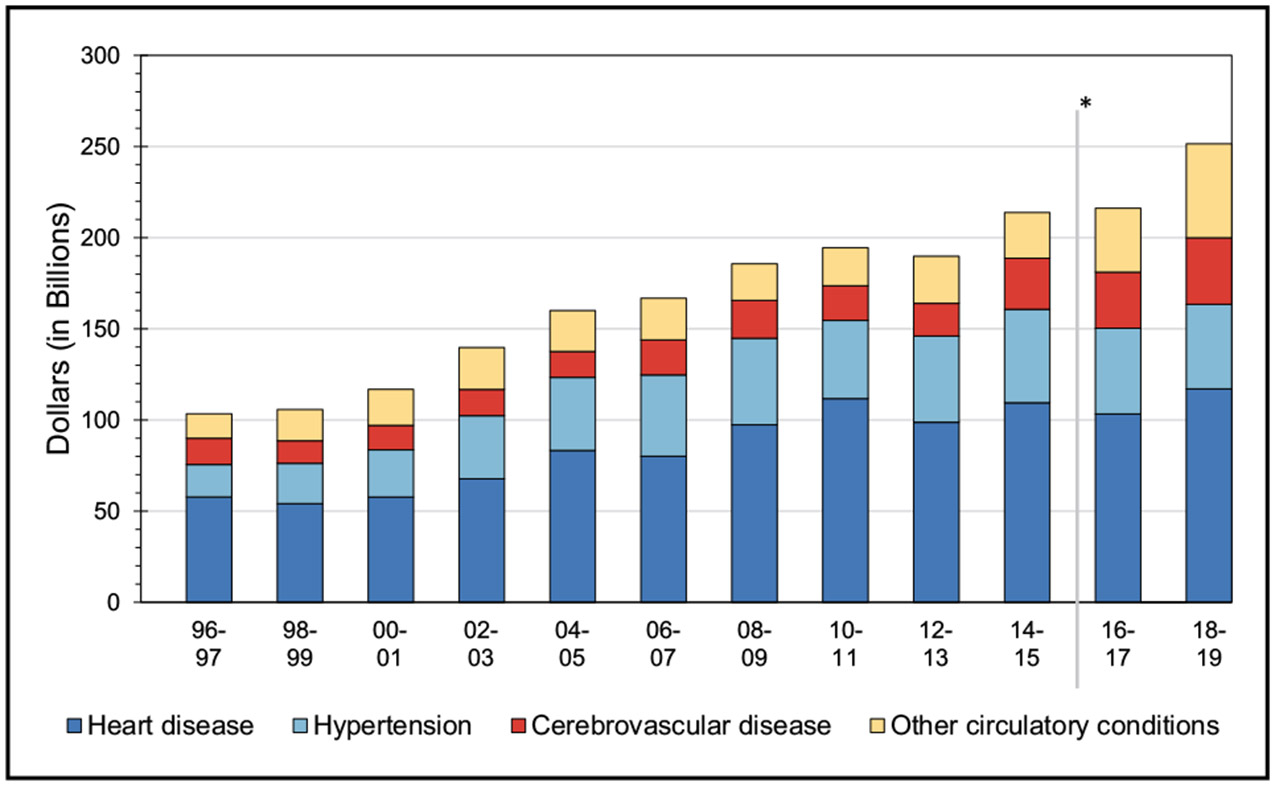
Economic Cost of Cardiovascular Disease (Chapter 28)
The average annual direct and indirect cost of CVD in the United States was an estimated $407.3 billion in 2018 to 2019.
The estimated direct costs of CVD in the United States increased from $103.5 billion in 1996 to 1997 to $251.4 billion in 2018 to 2019.
By event type, hospital inpatient stays accounted for the highest direct cost ($111.4 billion) in 2018 to 2019 in the United States.
Conclusions
The AHA, through its Epidemiology and Prevention Statistics Committee, continuously monitors and evaluates sources of data on heart disease and stroke in the United States to provide the most current information available in the Statistical Update. The 2023 Statistical Update is the product of a full year’s worth of effort by dedicated volunteer clinicians and scientists, committed government professionals, and AHA staff members, without whom publication of this valuable resource would be impossible. Their contributions are gratefully acknowledged.
ABBREVIATIONS TABLE
| 3C | Three City Study |
| 4D Study | Deutsche Diabetes Dialyse Studie |
| 6MWD | 6-minute walk distance |
| AAA | abdominal aortic aneurysm |
| ABI | ankle-brachial index |
| ACC | American College of Cardiology |
| ACCORD | Action to Control Cardiovascular Risk in Diabetes |
| ACE | angiotensin-converting enzyme |
| ACR | albumin-to-creatinine ratio |
| ACS | acute coronary syndrome |
| ACTION | Acute Coronary Treatment and Intervention Outcomes Network |
| AD | Alzheimer disease |
| ADAMS | Aging, Demographics, and Memory Study |
| ADRD | Alzheimer disease and related dementia |
| AF | atrial fibrillation or atriofibrillation |
| AGES | Age, Gene/Environment Susceptibility |
| AHA | American Heart Association |
| AHEI | Alternative Health Eating Index |
| AHI | apnea-hypopnea index |
| aHR | adjusted hazard ratio |
| AHS-2 | Adventist Health Study 2 |
| AIM-HIGH | Atherothrombosis Intervention in Metabolic Syndrome With Low HDL/High Triglycerides and Impact on Global Health Outcomes |
| aIRR | adjusted incidence rate ratio |
| AIS | acute ischemic stroke |
| ALLHAT | Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial |
| AMI | acute myocardial infarction |
| ANP | atrial natriuretic peptide |
| aOR | adjusted odds ratio |
| AP | angina pectoris |
| APO | adverse pregnancy outcome |
| ARGEN-IAM-ST | Pilot Study on ST Elevation Acute Myocardial Infarction |
| ARIC | Atherosclerosis Risk in Communities |
| ARIC-NCS | Atherosclerosis Risk in Communities–Neurocognitive Study |
| ARIC-PET | Atherosclerosis Risk in Communities–Positron Emission Tomography |
| ARNI | angiotensin receptor-neprilysin inhibitor |
| aRR | adjusted relative risk |
| ARVC | arrhythmogenic right ventricular cardiomyopathy |
| ASB | artificially sweetened beverage |
| ASCVD | atherosclerotic cardiovascular disease |
| ASD | atrial septal defect |
| ASPECTS | Alberta Stroke Program Early CT Score |
| ASPIRE | Assessing the Spectrum of Pulmonary Hypertension Identified at a Referral Centre Registry |
| ASPREE | Aspirin in Reducing Events in the Elderly |
| ATP III | Adult Treatment Panel III |
| AUC | area under the curve |
| AVAIL | Adherence Evaluation After Ischemic Stroke Longitudinal |
| AWHS | Aragon Workers Health Study |
| BASIC | Brain Attack Surveillance in Corpus Christi |
| BEST | Randomized Comparison of Coronary Artery Bypass Surgery and Everolimus-Eluting Stent Implantation in the Treatment of Patients With Multivessel Coronary Artery Disease |
| BiomarCaRE | Biomarker for Cardiovascular Risk Assessment in Europe |
| BioSHaRe | Biobank Standardization and Harmonization for Research Excellence in the European Union |
| BMI | body mass index |
| BNP | B-type natriuretic peptide |
| BP | blood pressure |
| BRFSS | Behavioral Risk Factor Surveillance System |
| CABG | coronary artery bypass graft |
| CAC | coronary artery calcification |
| CAD | coronary artery disease |
| CAIDE | Cardiovascular Risk Factors, Aging and Dementia |
| CALIBER UK | Cardiovascular Research Using Linked Bespoke Studies and Electronic Health Records |
| CANHEART | Cardiovascular Health in Ambulatory Care Research Team |
| CARDIA | Coronary Artery Risk Development in Young Adults |
| CARDIoGRAM | Coronary Artery Disease Genome Wide Replication and Meta-Analysis |
| CARDIo- GRAMplusC4D |
Coronary Artery Disease Genome Wide Replication and Meta-Analysis (CARDIoGRAM) Plus the Coronary Artery Disease (C4D) Genetics |
| CARES | Cardiac Arrest Registry to Enhance Survival |
| CAS | carotid artery stenting |
| CASCADE FH | Cascade Screening for Awareness and Detection of Familial Hypercholesterolemia |
| CASQ2 | calsequestrin 2 |
| CCD | congenital cardiovascular defect |
| CDC | Centers for Disease Control and Prevention |
| CDC WONDER |
Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research |
| CEA | carotid endarterectomy |
| CERAD-TS | Consortium to Establish a Registry for Alzheimer’s Disease neuropsychological battery, total score |
| CHA2DS2- VASc |
clinical prediction rule for estimating the risk of stroke based on congestive heart failure, hypertension, diabetes, and sex (1 point each); age ≥75 years and stroke/transient ischemic attack/thromboembolism (2 points each); plus history of vascular disease, age 65 to 74 years, and (female) sex category |
| CHADS2 | clinical prediction rule for estimating the risk of stroke based on congestive heart failure, hypertension, age ≥75 years, diabetes (1 point each), and prior stroke/transient ischemic attack/thromboembolism (2 points) |
| CHAMP-HF | Change the Management of Patients With Heart Failure |
| CHAP | Chicago Health and Aging Project |
| CHARGE-AF | Cohorts for Heart and Aging Research in Genomic Epidemiology–Atrial Fibrillation |
| CHARM | Candesartan in Heart Failure–Assessment of Reduction in Mortality and Morbidity |
| CHD | coronary heart disease |
| CHS | Cardiovascular Health Study |
| CI | confidence interval |
| CICAT | Codi Ictus Catalunya Registry |
| CKD | chronic kidney disease |
| CKiD | Chronic Kidney Disease in Children |
| COAPT | Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients With Functional Mitral Regurgitation |
| COAST | Comparative Outcomes Services Utilization Trends |
| COMPASS | Cardiovascular Outcomes for People Using Anticoagulation Strategies |
| CONFIRM | Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter Registry |
| CORAL | Cardiovascular Outcomes in Renal Atherosclerotic Lesions |
| COVID-19 | coronavirus disease 2019 |
| CPAP | continuous positive airway pressure |
| CPR | cardiopulmonary resuscitation |
| CPVT | catecholaminergic polymorphic ventricular tachycardia |
| CREOLE | Comparison of Three Combination Therapies in Lowering Blood Pressure in Black Africans |
| CRIC | Chronic Renal Insufficiency Cohort |
| CROMIS-2 | Clinical Relevance of Microbleeds in Stroke |
| CRP | C-reactive protein |
| CRS | Cardiovascular Risk Survey |
| CRUSADE | Can Rapid Risk Stratification of Unstable Angina Patient Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines |
| CSA | community-supported agriculture |
| CSC | comprehensive stroke center |
| CT | computed tomography |
| CTEPH | chronic thromboembolic pulmonary hypertension |
| CVD | cardiovascular disease |
| CVD PREDICT | Cardiovascular Disease Policy Model for Risk, Events, Detection, Interventions, Costs, and Trends |
| CVH | cardiovascular health |
| CVI | chronic venous insufficiency |
| DALY | disability-adjusted life-year |
| DANISH | Danish Study to Assess the Efficacy of ICDs in Patients With Non-Ischaemic Systolic Heart Failure on Mortality |
| DASH | Dietary Approaches to Stop Hypertension |
| DBP | diastolic blood pressure |
| DCCT/EDIC | Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications |
| DCM | dilated cardiomyopathy |
| DHA | docosahexaenoic acid |
| DII | Dietary Inflammatory Index |
| DNA | deoxyribonucleic acid |
| DOAC | direct oral anticoagulant |
| DPP | Diabetes Prevention Program |
| DREAM-LDL | Diabetes (fasting blood glucose level), Rating (National Institutes of Health Stroke Scale), level of education, age, baseline Montreal Cognitive Assessment Scale score, and LDL-C level |
| DR’s EXTRA | Dose Responses to Exercise Training |
| DVT | deep vein thrombosis |
| EAGLES | Study Evaluating the Safety and Efficacy of Varenicline and Bupropion for Smoking Cessation in Subjects With and Without a History of Psychiatric Disorders |
| ECG | electrocardiogram |
| e-cigarette | electronic cigarette |
| ED | emergency department |
| EF | ejection fraction |
| eGFR | estimated glomerular filtration rate |
| ELSA | English Longitudinal Study of Ageing |
| EMPHASIS-HF | Eplere in Mild Patients Hospitalization and Survival Study in Heart Failure |
| EMS | emergency medical services |
| EPA | eicosapentaenoic acid |
| EPIC | European Prospective Investigation Into Cancer and Nutrition |
| ERICA | Study of Cardiovascular Risks in Adolescents |
| ERP | early repolarization pattern |
| ESRD | end-stage renal disease |
| EUCLID | Examining Use of Ticagrelor in PAD |
| EVEREST | Endovascular Valve Edge-to-edge Repair |
| EVEREST II HRS | Endovascular Valve Edge-to-Edge Repair High-Risk Study |
| EVITA | Effect of Vitamin D on Mortality in Heart Failure |
| EVITA | Evaluation of Varenicline in Smoking Cessation for Patients Post-Acute Coronary Syndrome |
| EXAMINE | Examination of Cardiovascular Outcomes With Alogliptin Versus Standard of Care |
| FDA | US Food and Drug Administration |
| FH | familial hypercholesterolemia |
| FHS | Framingham Heart Study |
| FIDELIO DKD | Finerenone in Reducing Kidney Failure and Disease Progression in Diabetic Kidney Disease |
| FINRISK | Finnish Population Survey on Risk Factors for Chronic, Noncommunicable Diseases |
| FMD | flow-mediated dilation |
| FOURIER | Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk |
| FPG | fasting plasma glucose |
| FRS | Framingham Risk Score |
| FUTURE | Follow-up of TIA and Stroke Patients and Unelucidated Risk Factor Evaluation |
| FVL | factor V Leiden |
| GARFIELD-VTE | Global Anticoagulant Registry in the Field–Venous Thromboembolism |
| GBD | Global Burden of Disease |
| GBD Study | Global Burden of Diseases, Injuries, and Risk Factors Study |
| GCNKSS | Greater Cincinnati/Northern Kentucky Stroke Study |
| GFR | glomerular filtration rate |
| GISSI-3 | Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico |
| GLORIA-AF | Global Registry on Long-term Oral Antithrombotic Treatment in Patients with Atrial Fibrillation |
| GLP1-RA | glucagon-like peptide 1 receptor agonist |
| GRS | genetic risk score |
| GWAS | genome-wide association study |
| GWTG | Get With The Guidelines |
| HANDLS | Healthy Aging in Neighborhoods of Diversity Across the Life Span |
| HAPIEE | Health, Alcohol and Psychosocial Factors in Eastern Europe |
| HAPO | Hyperglycemia and Adverse Pregnancy Outcome |
| HbA1c | hemoglobin A1c (glycosylated hemoglobin) |
| HBP | high blood pressure |
| HCHS/SOL | Hispanic Community Health Study/Study of Latinos |
| HCM | hypertrophic cardiomyopathy |
| HCUP | Healthcare Cost and Utilization Project |
| HD | heart disease |
| HDL | high-density lipoprotein |
| HDL-C | high-density lipoprotein cholesterol |
| HDP | hypertensive disorders of pregnancy |
| HEI | Healthy Eating Index |
| HELENA | Healthy Lifestyle in Europe by Nutrition in Adolescence |
| HF | heart failure |
| HF-ACTION | Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training |
| HFmrEF | heart failure with midrange ejection fraction |
| HFpEF | heart failure with preserved ejection fraction |
| HFrEF | heart failure with reduced ejection fraction |
| HIV | human immunodeficiency virus |
| HLHS | hypoplastic left-heart syndrome |
| HPFS | Health Professionals Follow-Up Study |
| HPS | Heart Protection Study |
| HR | hazard ratio |
| HRRP | Hospital Readmissions Reduction Program |
| HRS | Health and Retirement Study |
| HYVET | Hypertension in the Very Elderly Trial |
| ICD | International Classification of Diseases |
| ICD-9 | International Classification of Diseases, 9th Revision |
| ICD-9-CM | International Classification of Diseases, 9th Revision, Clinical Modification |
| ICD-10 | International Classification of Diseases, 10th Revision |
| ICD-10-CM | International Classification of Diseases, 10th Revision, Clinical Modification |
| ICE-PLUS | International Collaboration on Endocarditis–PLUS |
| ICH | intracerebral hemorrhage |
| ICU | intensive care unit |
| IE | infective endocarditis |
| IE After TAVI | Infective Endocarditis After Transcatheter Aortic Valve Implantation and SwissTAVI as Swiss Transcatheter Aortic Valve Implantation |
| IHCA | in-hospital cardiac arrest |
| IHD | ischemic heart disease |
| IMPACT | International Model for Policy Analysis of Agricultural Commodities and Trade |
| IMPROVE | Carotid Intima-Media Thickness (IMT) and IMT-Progression as Predictors of Vascular Events in a High-Risk European Population |
| IMT | intima-media thickness |
| INTER-CHF | International Congestive Heart Failure |
| INTERMACS | Interagency Registry for Mechanically Assisted Circulatory Support |
| IQR | interquartile range |
| IRAD | International Registry of Acute Aortic Dissection |
| IRR | incidence rate ratio |
| ISCHEMIA | International Study of Comparative Health Effectiveness With Medical and Invasive Approaches |
| IVIG | intravenous immunoglobulin |
| Iwate-KENCO | Iwate-Kenpoku Cohort |
| JHS | Jackson Heart Study |
| KD | Kawasaki disease |
| LAAO | Left Atrial Appendage Occlusion |
| LASI | Longitudinal Aging Study in India |
| LBW | low birth weight |
| LDL | low-density lipoprotein |
| LDL-C | low-density lipoprotein cholesterol |
| LEAD | Louisiana Experiment Assessing Diabetes |
| LEADER | Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results |
| LIBRA | Lifestyle for Brain Health |
| LOAD | late-onset Alzheimer disease |
| Look AHEAD | Look: Action for Health in Diabetes |
| LQTS | long QT syndrome |
| LTPA | leisure-time physical activity |
| LV | left ventricular |
| LVAD | left ventricular assist device |
| LVEF | left ventricular ejection fraction |
| LVH | left ventricular hypertrophy |
| MACE | major adverse cardiovascular event |
| MAP | Memory and Aging Project |
| MAPT | Multidomain Alzheimer Preventive Trial |
| MARS | Minority Aging Research Study |
| MCI | mild cognitive impairment |
| MDCS | Malmö Diet and Cancer Study |
| MEPS | Medical Expenditure Panel Survey |
| MESA | Multi-Ethnic Study of Atherosclerosis |
| MET | metabolic equivalent |
| MetS | metabolic syndrome |
| MHAS | Mexican Health and Aging study |
| MHO | metabolically healthy obesity |
| MI | myocardial infarction |
| MIDA | Mitral Regurgitation International Database |
| MIDAS | Myocardial Infarction Data Acquisition System |
| MIDUS | Midlife in the United States |
| MIMS | Monitor Independent Movement Summary |
| MIND-China | Multimodal Interventions to Delay Dementia and Disability in Rural China |
| MIS-C | multisystem inflammatory syndrome in children |
| MITRA-FR | Percutaneous Repair With the MitraClip Device for Severe Functional/Secondary Mitral Regurgitation |
| MMSE | Mini-Mental State Examination |
| MONICA | Monitoring Trends and Determinants of Cardiovascular Disease |
| MR | mitral regurgitation |
| MRI | magnetic resonance imaging |
| MTF | Monitoring the Future |
| MUSIC | Muerte Súbita en Insuficiencia Cardiaca |
| NAFLD | nonalcoholic fatty liver disease |
| NAMCS | National Ambulatory Medical Care Survey |
| NCDR | National Cardiovascular Data Registry |
| NCHS | National Center for Health Statistics |
| NH | non-Hispanic |
| NHAMCS | National Hospital Ambulatory Medical Care Survey |
| NHANES | National Health and Nutrition Examination Survey |
| NHDS | National Hospital Discharge Survey |
| NHIS | National Health Interview Survey |
| NHLBI | National Heart, Lung, and Blood Institute |
| NIH-AARP | National Institutes of Health–American Association of Retired Persons |
| NIHSS | National Institutes of Health Stroke Scale |
| NINDS | National Institutes of Neurological Disorders and Stroke |
| NIPPON DATA | National Integrated Project for Prospective Observation of Noncommunicable Disease and Its Trends in Aged |
| NIS | National (Nationwide) Inpatient Sample |
| NNT5 | number needed to treat for 5 years |
| NOMAS | Northern Manhattan Study |
| NOTION | Nordic Aortic Valve Intervention |
| NSDUH | National Survey on Drug Use and Health |
| NSHDS | Northern Sweden Health and Disease Study |
| NSTEMI | non–ST-segment–elevation myocardial infarction |
| NT-proBNP | N-terminal pro-B-type natriuretic peptide |
| nuMoM2b | Nulliparous Pregnancy Outcomes Study: Monitoring Mothers-to-Be |
| NVSS | National Vital Statistics System |
| NYTS | National Youth Tobacco Survey |
| ODYSSEY Outcomes | Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment With Alirocumab |
| OHCA | out-of-hospital cardiac arrest |
| ONTARGET | Ongoing Telmisartan Alone and in Combination With Ramipril Global Endpoint Trial and to Telmisartan Randomized Assessment |
| OPACH | Objectively Measured Physical Activity and Cardiovascular Health |
| OR | odds ratio |
| ORBIT-AF | Outcomes Registry for Better Informed Treatment of Atrial Fibrillation |
| OSA | obstructive sleep apnea |
| OVER | Open Versus Endovascular Repair |
| PA | physical activity |
| PAD | peripheral artery disease |
| PAF | population attributable fraction |
| PAGE | Placental Abruption Genetic Epidemiology |
| PAH | pulmonary arterial hypertension |
| PALM | Patient and Provider Assessment of Lipid Management Registry |
| PAPE | Peruvian Abruptio Placentae Epidemiology |
| PAR | population attributable risk |
| PARADIGM | Progression of Atherosclerotic Plaque Determined by Computed Tomographic Angiography Imaging |
| PARTNER | Placement of Aortic Transcatheter Valve |
| PATH | Population Assessment of Tobacco and Health |
| PATH-BP | Regular Acetaminophen Use and Blood Pressure in People With Hypertension |
| PCE | Pooled Cohort Equations |
| PCI | percutaneous coronary intervention |
| PCSK9 | proprotein convertase subtilisin/kexin type 9 |
| PE | pulmonary embolism |
| PESA | Progression of Early Subclinical Atherosclerosis |
| PHC | Pulmonary Hypertension Connection |
| PHIRST | Pulmonary Arterial Hypertension and Response to Tadalafil Study |
| PINNACLE | Practice Innovation and Clinical Excellence |
| PM2.5 | fine particulate matter <2.5-μm diameter |
| POINT | Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke |
| PPCM | peripartum cardiomyopathy |
| PPSW | Prospective Population Study of Women in Gothenburg |
| PR | prevalence ratio |
| PRECOMBAT | Premier of Randomized Comparison of Bypass Surgery Versus Angioplasty Using Sirolimus Stents in Patients With Left Main Coronary Artery Disease |
| PREDIMED | Prevención con Dieta Mediterránea |
| PreDIVA | Prevention of Dementia by Intensive Vascular Care |
| PREMA | Prediction of Metabolic Syndrome in Adolescence |
| PREMIER | Lifestyle Interventions for Blood Pressure Control |
| PREVEND | Prevention of Renal and Vascular End-Stage Disease |
| PRODIGY | Progress in Diabetes Genetics in Youth |
| PROFESS | Prevention Regimen for Effectively Avoiding Second Stroke |
| PRS | polygenic risk score |
| PTB | preterm birth |
| PTS | postthrombotic syndrome |
| PUFA | polyunsaturated fatty acid |
| PURE | Prospective Urban Rural Epidemiology study |
| PWV | pulse-wave velocity |
| QALY | quality-adjusted life-year |
| QTc | corrected QT interval |
| RCT | randomized controlled trial |
| REACH | Reduction of Atherothrombosis for Continued Health |
| REDINSCOR | Red Española de Insuficiencia Cardiaca |
| REGARDS | Reasons for Geographic and Racial Differences in Stroke |
| REMEDY | Global Rheumatic Heart Disease Registry |
| RENIS-T6 | Renal Iohexol Clearance Survey in Tromsø 6 |
| REPLACE | Riociguat Replacing PDE5i Therapy Evaluated Against Continued PDE5i Therapy |
| REVEAL | Registry to Evaluate Early and Long-term PAH Disease Management |
| RIETE | Registro Informatizado de Enfermedad Tromboembólica |
| ROC | Resuscitation Outcomes Consortium |
| ROS | Religious Orders Study |
| RR | relative risk |
| RSMR | risk-standardized mortality rate |
| RV | right ventricular |
| RYR2 | ryanodine receptor 2 |
| S.AGES | Sujets AGÉS–Aged Subjects |
| SADHS | South African Demographic Health and Surveillance Study |
| SAFEHEART | Spanish Familial Hypercholesterolemia Cohort Study |
| SAGE | Study on Global Ageing and Adult Health |
| SAH | subarachnoid hemorrhage |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| SAVE | Sleep Apnea Cardiovascular Endpoints |
| SAVR | surgical aortic valve replacement |
| SBP | systolic blood pressure |
| SCA | sudden cardiac arrest |
| SCD | sudden cardiac death |
| SCORE | Systematic Coronary Risk Evaluation |
| SD | standard deviation |
| SDB | sleep-disordered breathing |
| SE | standard error |
| SEARCH | Search for Diabetes in Youth |
| SEMI-COVID-19 | Sociedad Española de Medicina Interna Coronavirus Disease 2019 |
| SES | socioeconomic status |
| SFA | saturated fatty acid |
| SGA | small for gestational age |
| SGLT-2 | sodium-glucose cotransporter 2 |
| SHIP | Study of Health in Pomerania |
| SHIP AHOY | Study of Hypertension in Pediatrics, Adult Hypertension Onset in Youth |
| SHS | Strong Heart Study |
| SILVER-AMI | Comprehensive Evaluation of Risk Factors in Older Patients With Acute Myocardial Infarction |
| SNAC-K | Swedish National Study on Aging and Care in Kungsholmen |
| SND | sinus node dysfunction |
| SNP | single-nucleotide polymorphism |
| SPRINT | Systolic Blood Pressure Intervention Trial |
| SSB | sugar-sweetened beverage |
| START | South Asian Birth Cohort |
| STEMI | ST-segment–elevation myocardial infarction |
| STEP 1 | Research Study Investigating How Well Semaglutide Works in People Suffering From Overweight or Obesity |
| STEP 3 | Research Study to Look at How Well Semaglutide Is at Lowering Weight When Taken Together With an Intensive Lifestyle Program |
| STROKE-AF | Rate of Atrial Fibrillation Through 12 Months in Patients With Recent Ischemic Stroke of Presumed Known Origin |
| STS | Society of Thoracic Surgeons |
| SUN | Seguimiento Universidad de Navarra |
| SURMOUNT-1 | Efficacy and Safety of Tirzepatide Once Weekly Versus Placebo in Participants Who Are Either Obese or Overweight With Weight-Related Comorbidities |
| SURTAVI | Surgical Replacement and Transcatheter Aortic Valve Implantation |
| SVT | supraventricular tachycardia |
| SWAN | Study of Women’s Health Across the Nation |
| SwissTAVI | Swiss Transcatheter Aortic Valve Implantation |
| SYNTAX | Synergy Between PCI With Taxus and Cardiac Surgery |
| TAA | thoracic aortic aneurysm |
| TAVI | transcatheter aortic valve implantation |
| TAVR | transcatheter aortic valve replacement |
| TC | total cholesterol |
| TdP | torsade de pointes |
| TECOS | Trial Evaluating Cardiovascular Outcomes With Sitagliptin |
| TGA | transposition of the great arteries |
| TGF | transforming growth factor |
| TIA | transient ischemic attack |
| TIMI | Thrombolysis in Myocardial Infarction |
| TODAY | Treatment Options for Type 2 Diabetes in Adolescents and Youth |
| TOF | tetralogy of Fallot |
| TOPCAT | Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist |
| tPA | tissue-type plasminogen activator |
| TRIUMPH | Treprostinil Sodium Inhalation Used in the Management of Pulmonary Arterial Hypertension |
| TVT | transcatheter valve therapy |
| UI | uncertainty interval |
| USRDS | US Renal Data System |
| VF | ventricular fibrillation |
| VITAL | Vitamin D and Omega-3 Trial |
| VOYAGER | Efficacy and Safety of Rivaroxaban in Reducing the Risk of Major Thrombotic Vascular Events in Subjects With Symptomatic Peripheral Artery Disease Undergoing Peripheral Revascularization Procedures of the Lower Extremities |
| VSD | ventricular septal defect |
| VT | ventricular tachycardia |
| VTE | venous thromboembolism |
| WC | waist circumference |
| WHI | Women’s Health Initiative |
| WHICAP | Washington Heights–Hamilton Heights-Inwood Community Aging Project |
| WHO | World Health Organization |
| WHS | Women’s Health Study |
| WIC | Special Supplemental Nutrition Program for Women, Infants, and Children |
| WMD | weighted mean difference |
| WMH | white matter hyperintensity |
| WPW | Wolff-Parkinson-White |
| YLD | years of life lived with disability or injury |
| YLL | years of life lost to premature mortality |
| YRBS | Youth Risk Behavior Survey |
Abbreviations used only in charts and tables do not appear in this table.
Supplementary Material
Acknowledgments
The writing group thanks its colleagues Lucy Hsu and Michael Wolz at the National Heart, Lung, and Blood Institute; the team at the Institute for Health Metrics and Evaluation at the University of Washington; Bryan McNally and Rabab Al-Araji at the CARES (Cardiac Arrest Registry to Enhance Survival) program; Hongyan Ning and Donald Lloyd-Jones at Northwestern University; and Christina Koutras and Fran Thorpe at the American College of Cardiology for their valuable contributions and review.
Footnotes
Disclosures
| Writing group member |
Employment | Research grant | Other research support |
Speakers’ bureau/ honoraria |
Expert witness |
Ownership interest |
Consultant/ advisory board |
Other |
|---|---|---|---|---|---|---|---|---|
| Connie W. Tsao | Beth Israel Deaconess Medical Center | NIH† | None | None | Smith Haughey Rice & Roegge* | None | Abiomed† | None |
| Seth S. Martin | Johns Hopkins University School of Medicine | None | None | None | None | Corrie Health* | Amgen*; AstraZeneca*; Kaneka*; Sanofi* | None |
| Aaron W. Aday | Vanderbilt University Medical Center | None | None | None | None | None | None | None |
| Zaid I. Almarzooq | Brigham and Women’s Hospital | None | None | None | None | None | None | None |
| Cheryl A.M. Anderson | University of California, San Diego | NHLBI†; McCormick Science Institute† | None | None | None | None | None | None |
| Pankaj Arora | University of Alabama at Birmingham | NIH† | None | None | None | None | None | None |
| Christy L. Avery | University of North Carolina | None | None | None | None | None | None | None |
| Carissa M. Baker-Smith | Nemours-Alfred I. Dupont Hospital for Children Cardiac Center | INBRE*; Nemours Pilot*; Regeneron* | None | Cardiometabolic* | None | None | None | None |
| Andrea Z. Beaton | The Heart Institute, Cincinnati Children’s Hospital Medical Center | AHA*; Thrasher Pediatric Research Fund* | None | None | None | None | None | None |
| Amelia K. Boehme | Columbia University | None | None | None | None | None | None | None |
| Alfred E. Buxton | Beth Israel Deaconess Medical Center/Harvard Medical School | None | None | None | None | None | None | None |
| Yvonne Commodore-Mensah | Johns Hopkins School of Public Health & Nursing | None | None | None | None | None | None | None |
| Mitchell S.V. Elkind | Columbia University | BMS-Pfizer Alliance for Eliquis†; Roche Diagnostics† | None | None | None | None | None | AHA (officer)*; UpTo-Date (royalties for chapters on stroke)* |
| Kelly R. Evenson | University of North Carolina | NIH†; North Carolina Governor’s Highway Safety Program*; US Department of Transportation†; World Bank* | None | None | None | None | None | None |
| Chete Eze-Nliam | Cleveland Clinic | None | None | None | None | None | None | None |
| Setri Fugar | Medical College of Wisconsin | None | None | None | None | None | None | None |
| Giuliano Generoso | University Hospital, University of Sao Paulo | None | None | None | None | None | None | None |
| Debra G. Heard | American Heart Association | None | None | None | None | None | None | None |
| Swapnil Hiremath | University of Ottawa | Hecht Foundation* (no payment received) | None | None | None | None | None | None |
| Jennifer E. Ho | Beth Israel Deaconess Medical Center | NIH† | None | None | None | Pfizer† (immediate family members) | None | Cytel† (husband is employee) |
| Rizwan Kalani | University of Washington | None | None | None | None | None | None | None |
| Dhruv S. Kazi | Beth Israel Deaconess Medical Center, Harvard Medical School | Boston Scientific* | None | None | None | None | None | None |
| Darae Ko | Boston University | Boston Scientific† | None | None | None | None | Eagle Pharmaceuticals* | None |
| Deborah A. Levine | University of Michigan | NIH† | None | None | None | None | NIH* | None |
| Junxiu Liu | Icahn School of Medicine at Mount Sinai | None | None | None | None | None | None | None |
| Jun Ma | University of Illinois, Chicago | NIH†; Veterans Administration† | None | None | None | None | Health Mentor, Inc (San Jose) * | None |
| Jared W. Magnani | University of Pittsburgh | NIH/NHLBI† | None | None | None | None | None | None |
| Erin D. Michos | Johns Hopkins University School of Medicine | None | None | None | None | None | AstraZeneca*; Bayer*; Boehringer Ingelheim*; Esperion*; Novartis†; Novo Nordisk†; Pfizer* | None |
| Michael E. Mussolino | National Heart, Lung, and Blood Institute | None | None | None | None | None | None | None |
| Sankar D. Navaneethan | Baylor College of Medicine | None | None | None | None | None | Astra Zeneca*; Bayer†; Boehringer Ingelheim/Lilly†; ACI Clinical†; Vertex*; Vifor* | None |
| Nisha I. Parikh | University of California, San Francisco | None | None | None | None | None | None | None |
| Remy Poudel | American Heart Association | None | None | None | None | None | None | None |
| Mary Rezk-Hanna | University of California, Los Angeles | NIH†; Tobacco-Related Disease Research Program† | None | None | None | None | None | None |
| Gregory A. Roth | University of Washington | None | None | None | None | None | None | None |
| Nilay S. Shah | Northwestern University Feinberg School of Medicine | NHLBI† | None | None | None | None | None | None |
| Marie-Pierre St-Onge | Columbia University | None | None | None | None | None | None | None |
| Evan L. Thacker | Brigham Young University | None | None | None | None | None | None | None |
| Salim S. Virani | Baylor College of Medicine, Michael E. DeBakey VA Medical Center Health Services Research and Development Center for Innovations, The Aga Khan University | Department of Veteran Affairs†; NIH†; Tahir and Jooma† | None | None | None | None | None | None |
| Jenifer H. Voeks | Medical University of South Carolina | None | None | None | None | None | None | None |
| Nae-Yuh Wang | Johns Hopkins University School of Medicine | NIH† | None | None | None | None | None | None |
| Nathan D. Wong | University of California, Irvine | Novartis†; Novo Nordisk† | None | None | None | None | I-Health*; Novartis* | None |
| Sally S. Wong | American Heart Association | None | None | None | None | None | None | None |
| Kristine Yaffe | University of California, San Francisco | None | None | None | None | None | Alpha Cognition*; Eli Lilly*; Esia* | None |
The views expressed in this manuscript are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute; the National Institutes of Health; the US Department of Health and Human Services; or the US Department of Veterans Affairs.
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
The expert peer review of AHA-commissioned documents (eg, scientific statements, clinical practice guidelines, systematic reviews) is conducted by the AHA Office of Science Operations. For more on AHA statements and guidelines development, visit https://professional.heart.org/statements. Select the “Guidelines & Statements” drop-down menu, then click “Publication Development.”
The 2023 AHA Statistical Update uses language that conveys respect and specificity when referencing race and ethnicity. Instead of referring to groups very broadly with collective nouns (eg, Blacks, Whites), we use descriptions of race and ethnicity as adjectives (eg, Asian people, Black adults, Hispanic youths, Native American patients, White females).
As the AHA continues its focus on health equity to address structural racism, we are working to reconcile language used in previously published data sources and studies when this information is compiled in the annual Statistical Update. We strive to use terms from the original data sources or published studies (mostly from the past 5 years) that may not be as inclusive as the terms used in 2023. As style guidelines for scientific writing evolve, they will serve as guidance for data sources and publications and how they are cited in future Statistical Updates.
Supplemental Materials are available with this article at https://www.ahajournals.org/doi/suppl/10.1161/CIR.0000000000001123
REFERENCE
- 1.Lloyd-Jones DM, Allen NB, Anderson CAM, Black T, Brewer LC, Foraker RE, Grandner MA, Lavretsky H, Perak AM, Sharma G, et al. ; on behalf of the American Heart Association. Life’s Essential 8: updating and enhancing the American Heart Association’s construct of cardiovascular health: a presidential advisory from the American Heart Association. Circulation. 2022;146:e18–e43. doi: 10.1161/CIR.0000000000001078 [DOI] [PMC free article] [PubMed] [Google Scholar]